Embed Size (px)
Citation preview

CONTROVERSY
Ramon M. Esclamado, MD, Section Editor
MALIGNANT CAROTID BODY TUMOR
Consultants: William Carroll, MD1 Kerstin Stenson, MD2 Scott Stringer, MD3
1 Division of Otolaryngology, University of Alabama, Birmingham, Alabama2 Department of Otolaryngology, University of Chicago, Chicago, Illinois3 Department of Otolaryngology, University of Mississippi Medical Center, Jackson, Mississippi
CASE PRESENTATION
A 38-year-old woman initially presented with a
3-week history of decreased hearing in the left ear.
Evaluationrevealedaleftserousotitismedia,withno
evidenceofanasopharyngealmass.Shewastreated
forallergicrhinitis,withsubsequentresolutionofher
serous effusion. During the third trimester of her
subsequent pregnancy, she noted a progressive
globussensationandleft-sidedintermittentotalgia.
A CT scan after her pregnancy showed a 2- � 2-cm
enhancing mass at the left carotid bifurcation. In
addition, prominent soft tissue was noted in the
nasopharynx and tongue base, with bilateral 1-cm
level II nodes. She was subsequently referred for
furtherevaluationandmanagement.Shehadhadan
upper respiratory infection 2 weeks before the CT
scanbutnofevers,chills,ornightsweats.Shesmoked
one pack of cigarettes per day for 20 years but
otherwisewasingoodhealth.
Physical examination at the time of referral
revealed an obese, anxious woman, with a slightly
hyponasal voice. There was a left-sided serous
middle ear effusion. No trismus was present, but
prominent Waldeyer’s ring lymphoid tissue was.
Fiberoptic nasolaryngoscopy revealed prominent
nasopharyngeal lymphoid tissue abutting the left
eustachian tube orifice with purulent exudate. A
laryngeal and hypopharyngeal examination was
unremarkable. A mildly tender, 2-cm mass was
detected at the left carotid bulb, and rubbery,
mobile small lymph nodes were found at level II
bilaterally. There were no cranial nerve deficits.
Question 1: What is your differential diagnosis
at this time?
Dr. Carroll: The salient features of the history
and physical examination of this patient include:
unilateral serous otitis in a smoker, neck mass,
fullness in Waldeyer’s ring, and progression of
symptoms with pregnancy. Initial diagnostic con-
siderations includenasopharyngealororopharyng-
eal neoplasm (epithelial or lymphoid). Progression
of symptoms with pregnancy could be due to be-
nign lymphoid hyperplasia, but an estrogen recep-
tor (+) malignancy such as metastatic breast
carcinoma could also be responsible, particularly
in a 38-year-old woman.
Dr. Stenson: Nasopharyngeal carcinoma with
metastatic lymphadenopathy should be the diag-
nosis of exclusion. Other diagnoses to consider
would be lymphoma as well as infection of the
adenoid tissue secondary to her recent upper
respiratory infection. The finding of an enhanced
Department of Otolaryngology and Communicative Disorders, TheCleveland Clinic Foundation, 9500 Euclid Avenue (A71), Cleveland, Ohio44195Head & Neck 26: 301–306Published online 12 February 2004 in Wiley InterScience(www.interscience.wiley.com). DOI: 10.1002/hed.20017
B 2004 Wiley Periodicals, Inc.
Malignant Carotid Body Tumor HEAD & NECK March 2004 301

mass at the carotid bifurcation raises the diagnosis
of carotid body tumor.
Dr. Stringer: At this point, my differential diag-
nosis includes lymphoma, a carotid body tumor,
a nasopharyngeal carcinoma, oropharyngeal car-
cinoma, eustachian tube dysfunction, adenoiditis,
and chronic rhinosinusitis. However, my level of
concern for anything other than adenoiditis, eusta-
chian tube dysfunction, and a carotid body tumor is
very low given the lack of any other findings on the
CT scan. Iwould continue to consider lymphoma as
a possibility, however.
Question 2: She was treated with a 10-day
course ofAugmentin (GlaxoSmithKline,U.K.), and
re-evaluation at 2 weeks revealed resolution of the
purulent exudate and about 50% regression of the
nasopharyngeal soft tissue. Results of her neck
examination remained unchanged. What would be
your next step in evaluation?
Dr. Stenson: In terms of the nasopharyngeal
abnormality and lymphadenopathy, one should
consider performing a biopsy of the nasopharyn-
geal tissue (after evaluation for vascular anom-
aly), performing fine-needle aspiration (FNA) of
the cervical lymphadenopathy, or both. These low-
risk procedures can be done in the clinic setting.
Significant information about the diagnosis of the
nasopharyngeal abnormality and ultimate further
testing (if and when) for the carotid body tumor
can be acquired. If the index of suspicion for
malignancy were low or if biopsy and FNA as
outlined above were negative for malignancy, the
surgeon could counsel the patient about treatment
for her carotid body tumor. The surgeon would
then order a four-vessel angiogram to assess
patency of circle of Willis and cross-filling of the
cerebral hemispheres. The carotid body tumor
should then be embolized, and surgery planned
1–3 days thereafter.
Dr. Stringer: Assuming that there was no
evidence of deep infiltration in the nasopharynx
or oropharynx on the CT scan, I would proceed
with planning excision of the carotid body tumor.
My suspicion for lymphoma or a nasopharyngeal
carcinoma has become even lower given the res-
ponse to antibiotics. However, I have occasionally
observed an apparent response of malignant tu-
mors to antibiotics due to a decrease in associated
infection. Therefore, I would consider a nasopha-
ryngeal examination under anesthesia, with a
possible biopsy, depending on the status of the
serous effusion at this point. It will also be pos-
sible to access the lymphadenopathy directly at
the time of excision of the carotid body tumor.
Were it not for the lymphoid hypertrophy in Wal-
deyer’s ring, I would not be overly concerned
about bilateral, stable, 1-cm level II lymph nodes
in this patient.
Dr. Carroll: Most carotid body tumors are
strongly suspected on the basis of examination
and CT. The physical findings of carotid body
tumor are distinctive and alone raise suspicion. A
2-cm carotid body tumor is typically much more
fixed to the bifurcation and is firmer and more
pulsatile than is a metastatic node of the same
size. When coupled with typical CT findings of a
mass splaying the carotid bifurcation, the sur-
geon is alerted that the case is more than a neck
mass of unknown primary. The usual workup for
persistent neck mass of unknown primary is
staging endoscopy followed by excision node
biopsy. If carotid body tumor is not suspected
before this stage, the results can be disastrous.
The persistence of multiple small nodes and
fullness in Waldeyer’s ring following antibiotics
in this case does warrant examination under
anesthesia and biopsy to exclude concurrent
lymphoma or carcinoma.
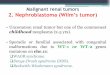
Question 3: A bilateral carotid angiogram was
obtained (Figure 1) because the patient refused
MRI. No other vascular lesions are noted in the
head and neck, and the circle of Willis is patent.
Are any other diagnostic studies indicated?
Dr. Stringer: If the patient has a positive family
history for paragangliomas, I would counsel her in
regard to genetic testing. If possible, I would also
obtain MR images to be sure there are no other
undetected paragangliomas that would alter my
treatment planning. Without a positive family his-
tory, I believe that the CT alone is an adequate
examination. Isolated carotid body tumors are
rarely catecholamine-secreting, so, absent any
other symptoms, I would not order a urine cate-
cholamine analysis. I do not routinely order angio-
grams for diagnosis of carotid body tumors. I
obtain an angiogram only if I plan to embolize the
tumor preoperatively, and the benefit of emboliza-
tion is controversial.
Dr. Carroll: Once the diagnosis of carotid body
tumor, or anymass in the parapharyngeal space, is
entertained, we recommend MRI/MRA. The clas-
sic splaying of the internal and external carotid
arteries is usually seen clearly on MRI. Flow voids
within the tumor raise the suspicion of a para-
ganglioma. With MRA, the course or the great
vessels, the feeding vessels to the mass, and any
significant tortuosity or luminal narrowing of the
great vessels are often evident.
HEAD & NECK March 2004302 Malignant Carotid Body Tumor

Once the diagnosis of carotid body tumor is
strongly suspected, multicentric tumors need to
be excluded. MRI is an excellent screening tool
for this purpose. Carotid body tumors can be
associated concurrently with paraganglioma in
any of the head and neck sites. With this patient’s
history of middle ear disease and ear pain, the
possibility of a co-existent glomus jugulare or
glomus tympanicum should not be ignored. Most
carotid body tumors are not vasoactive (1–5%).We
typically screen, however, for elevated urine
catecholamines. Blood pressures should also be
checked, and symptoms of flushing and tachycar-
dia discussed.
The final diagnostic study that we typically ob-
tain for a carotid body tumor is a cerebral angio-
gram. This is scheduled the day before surgery so
that the tumor can be embolized if indicated. Most
tumors at our institution are embolized preoper-
atively. Small tumors with limited vascularity are
an exception.
Dr. Stenson: The treating physician should or-
der either a serum or 24-h urine studies for vanil-
lylmandelic acid (VMA) and metanephrines to
determine if the tumor is catecholamine-secreting.
Question 4: What are your indications for
preoperative test occlusion of the carotid artery?
Dr. Carroll: Balloon occlusion of the internal
carotid artery and cerebral perfusion using radio-
nuclide-enhanced SPECT are used on all pa-
tients. One of our neuroradiologists, Dr. Joe
Horton, was part of the team at Pittsburgh in
the late 1980s that demonstrated the value of this
technique for establishing safety of sacrifice of the
internal carotid artery. About 5% of patients
develop neurological symptoms in the radiology
suite with balloon occlusion alone. These patients
do not have nuclear medicine imaging and are
very high risk if the carotid artery is sacrificed or
clamped for an extended period. Of the remaining
patients, approximately 14% show a significant
focal decrease in the cerebral blood flow on
SPECT imaging. The risk of cerebrovascular
accident (CVA) is greater than 90% if carotid
sacrifice or extended clamping of the carotid is
necessary for these patients. For those patients
with minimal or no impairment of cerebral per-
fusion, the risk of CVA is 2–3% with carotid
occlusion. Symptomatic complication rates for
these studies are less than 1%. We believe this
clinical information is valuable. Given the diffi-
culty of surgical resection of these tumors and the
possibility of having to apply clamps to the carotid
arteries to gain control or replace the segment of
the artery with a graft, we believe that these
studies are justified.
Dr. Stenson: Shamblin1 describes three differ-
ent types or stages of carotid body tumors. Type I
consists of a small tumor that is easily dissected
from the adjacent vessels in a periadventitial
plane. Type II tumors are larger and more adhe-
rent and partially surround the vessel. Type III
tumors are large and completely surround the ca-
rotid bifurcation. As described, types II and III
tumors aremost likely to require carotid resection.
One should determine via CT scanning if the
tumor encases the common and/or internal carotid
artery. If there appears to be a type II or III tumor,
preparation for carotid replacement, including
test balloon occlusion with electroencephalogram
monitoring (during the test occlusion as well as
during resection) should be arranged. The subse-
quent intraoperative expertise of our vascular col-
leagues is critical for the carotid shunting and
replacement aspects of this operation.
Dr. Stringer: I no longer use any preoperative
carotid artery blood flow analysis, including pre-
FIGURE 1. Carotid angiogram.
Malignant Carotid Body Tumor HEAD & NECK March 2004 303

operative test occlusion. The relationship between
this test and patient outcome in terms of stroke is
not reliable enough for planning purposes. The
size of the tumor would not affect my decision in
this regard.
Question 5: What are your treatment recom-
mendations?
Dr. Stenson: If the patient has not already had
a biopsy of the nasopharyngeal tissue, this step
should be completed. If nasopharyngeal malig-
nancy is ruled out, the patient should be prepared
for resection of her carotid body tumor. Preopera-
tive four-vessel angiogram with embolization of
the tumor should be completed at this time. Sched-
ules permitting, surgery should occur 1–3 days
thereafter to minimize post-embolic neovascular-
ization and inflammation. As a routine part of the
surgical approach, the level II and III lymph nodes
are removed via a selective neck dissection. This
not only enhances exposure but also allows for
pathologic analysis of the lymph nodes for meta-
static paraganglioma. Surgical technique involves
early identification of cranial nerves, ligation of
the external carotid artery, and meticulous peri-
adventitial dissection of the tumor from the carotid
bifurcation and internal carotid artery with liberal
use of the bipolar cautery.
Dr. Stringer: I recommend excision of the
carotid body tumor and nasopharyngeal and oro-
pharyngeal examination with possible biopsy, de-
pending on the findings. If after upper endoscopy
I noted abnormal lymph nodes upon entering the
neck, I would excise them and send one or more for
frozen section analysis in this particular case,
primarily because of the nasopharyngeal abnor-
malities described. If it returned as squamous cell
carcinoma, I would proceed with a full, modified
neck dissection. Otherwise, I would proceed with
excision of the carotid body tumor. If I were in-
formed intraoperatively of paraganglioma cells
being present in the nodes, I would complete a
selective neck dissection encompassing levels
II–IV. However, it is not my normal practice in
the course of carotid body tumor surgery to send
lymph nodes for frozen section analysis unless
they are clearly abnormal. As described in the
answer to Question 6, I send the immediate peri-
carotid bulb lymph nodes, if present, for perma-
nent section analysis.
The likelihood of having to sacrifice the internal
carotid artery in this case would be very low given
the small size of the lesion. However, it is my
practice to have a vascular surgeon on standby in
some fashion for all carotid body tumors for
medicolegal purposes and in case of the unantici-
pated need for vascular bypass and saphenous vein
grafting. I do not routinely have the vascular
surgeon present in the room during the case.
Dr. Carroll: The natural history of these tumors
is often slow, steady growth. A recent publication2
from The Netherlands estimated the tumor-
doubling time at 4.2 years. This slow growth rate
certainly allows time to weigh options. A rushed
decision for surgical resection is rarely needed. In
the index case, the patient is 38 years old with a
small tumor and no documented cranial nerve
deficit. There are no multifocal lesions. We would
usually recommend surgical therapy—particu-
larly in the case when the neck will be violated
for a node biopsy. A wait-and-watch approach with
repeat scanning on a yearly basis is not unreason-
able, and we give patients this option. We are
careful to explain that these tumors typically grow
slowly over time and gradually become more
difficult to remove without accompanying cranial
nerve damage. Collateral cerebral profusion may
diminish with age as well, making risk of carotid
occlusion for significant. The option of primary
radiation is discussed as well. Our preference is to
reserve radiation for very large lesions and for
those who are elderly or infirm.
We approach carotid body tumors in a multi-
disciplinary fashion. The neuroradiologist is in-
volved, as discussed above. The Vascular Surgery
service is also involved in all cases. For small
tumors, the vascular surgeons may simply be on
stand-by status and are called if needed. For large
tumors with a high likelihood of carotid resection,
the vascular surgeons arrange their surgery
schedules to be immediately available. This team
approach allows aggressive and complete resection
of large tumors with a reasonable margin of safety
for the patients.
The patient underwent nasal endoscopy with
biopsy of the nasopharyngeal soft tissue revealing
acute and chronic inflammation of lymphoid tis-
sue. She then underwent neck exploration with
excision of left level IIa and IIIa nodes, which
showed no evidence of lymphoma or other malig-
nancy. Her carotid body tumor was then removed
uneventfully, with the plane of dissection readily
established just deep to the loose carotid adven-
titia. Her postoperative course was uncompli-
cated. One week after surgery, the final pathologic
analysis revealed that the neck mass was consist-
ent with paraganglioma, but there was a micro-
scopic focus of paraganglioma cells in an excised
lymph node.
HEAD & NECK March 2004304 Malignant Carotid Body Tumor

Question 6: Would you recommend any other
additional treatment for her malignant carotid
body tumor?
Dr. Stenson: The principles of carotid body
tumor resection include early operative manage-
ment, adequate lymph node sampling, and com-
plete tumor resection. These techniques apply to
both benign and malignant carotid body tumors.
Carotid body tumors are known to be slow growing
and generally thought of as radioresistant. One
might consider postoperative radiotherapy for a
large malignant tumor with positive margins and
several positive lymph nodes. If, however, as in
this young patient’s case, there is only one positive
node, the surgeon should consider complete neck
dissection and/or close observation without adju-
vant postoperative therapy. In either situation,
routine follow-up CT may help detect subclini-
cal recurrences that will facilitate timely opera-
tive management.
Dr. Stringer: Absent an extremely aggressive
appearance of the tumor or abnormally enlarged
nodes, the role of routine intraoperative nodal
sampling is not established. It is difficult to obtain
necessary data owing to the rarity of carotid body
tumors and the even more rare incidence of
malignancy. Therefore, we do not know the true
incidence of paraganglioma cells being inciden-
tally present in lymph nodes with a relatively
normal appearance. It is my usual practice to
excise all lymph nodes encountered in the imme-
diate region of the carotid body tumor for perma-
nent histopathologic analysis. As in the present
case, frozen section analysis is not always diag-
nostic of the presence of paraganglioma cells in the
lymph nodes.
I would recommend moderate-dose radiation
therapy postoperatively and reserve neck dissec-
tion for a treatment failure. As discussed above, I
would perform a selective neck dissection only if I
knew of the diagnosis of a malignant lesion
intraoperatively, but I do not think the morbidity
of a secondary neck dissection 1 week later is
justified given our limited knowledge of the benefit
of neck dissection for these tumors and given the
success of moderate-dose radiation in stopping the
growth of paragangliomas.
Dr. Carroll: Malignancy in carotid body tumors
is rare. There are no distinguishing histologic
features of malignancy, and the diagnosis is
confirmed only by finding the tumor in adjacent
lymph nodes or distant sites. For documented me-
tastases in regional nodes with no evidence of
systemic spread, node dissection with postopera-
tive radiation is reasonable. I am aware of no defi-
nitive studies supporting this position.
COMMENTARY
The clinical presentation of this patient is similar
to many patients seen in a general otolaryngology
practice, but the salient features of this history
and physical examination that warrant formula-
tion of a careful differential diagnosis and evalua-
tion are outlined by Dr. Carroll in Question 1. All
of the consultants outline the important diagnostic
considerations, which highlights a key pitfall to
avoid: theCT findingof a carotidbody tumor should
not distract one from considering other pathologic
processes in cases inwhich the clinical picture does
not ‘‘fit’’ the typical presentation of a carotid body
tumor, because more than 90% of carotid body
tumors are benign and slow growing and its treat-
ment may be deferred. As stated by Dr. Stringer,
the most likely etiology of the nasopharyngeal
mass and serous otitis in this patient was adenoi-
ditis, and a trial of antibiotics can be safely given.
When there was incomplete resolution of the
nasopharyngeal abnormality and lymphadenop-
athy, all of the consultants recommended naso-
pharyngeal biopsy either in the clinic or under
general anesthesia. The importance of sampling
lymph nodes to exclude lymphoma is noted by Drs.
Carroll and Stringer. Once the possibility of a con-
current malignancy is ruled out, the carotid body
tumor can be addressed.
Appropriate preoperative evaluation of a car-
otid body tumor centers around three issues:
(1) screening for multiple paragangliomas, (2)
imaging of the cerebral circulation, and (3) use of
preoperative embolization. The 24-h urine screen-
ing for VMAandmetanephrine is recommended by
Drs. Carroll and Stenson but not by Dr. Stringer.
Because the incidence of vasoactive carotid body
tumors is low, this may not be necessary in the
absence of hypertension, tachycardia, and flush-
ing. MRI is the diagnostic study of choice, both for
establishing the diagnosis of carotid body tumor
and for screening for multiple paragangliomas.
Screening MRI is performed routinely by Dr.
Carroll, but Dr. Stringer recommends this only in
case of a positive family history of paragangliomas.
The consultants’ approaches to imaging the ce-
rebral circulation and test occlusion of the carotid
artery are widely divergent. Preoperative carotid
blood flow analysis is no longer used by Dr. Stri-
nger, regardless of size of the tumor, because he
believes test occlusion is not a reliable predictor of
Malignant Carotid Body Tumor HEAD & NECK March 2004 305

stroke. Dr. Stenson uses test balloon occlusion
with EEG monitoring if the carotid body tumor is
large and partially or completely surrounds the
carotid artery. Dr. Carroll uses balloon occlusion
and SPECT imaging of the cerebral perfusion in all
patients and outlines his rationale for obtaining
this information, which he believes is valuable.
While this area remains controversial, preopera-
tive cerebral perfusion testing is warranted in the
unusual patient with large tumors, in which case
obtaining distal control of, or sewing a graft to, the
internal carotid artery near the skull base may
be difficult.
Preoperative embolization is performed by Dr.
Stenson 1–3 days before surgery in all patients
and by Dr. Carroll the day before surgery in all
patients except those with small tumors. This
again is controversial, since preoperative emboli-
zation can cause inflammation, whichmay obscure
the surgical plane of dissection. It is possible to
resect these tumors with minimal blood loss
without embolization by first circumferentially
ligating and dividing all feeding vessels to the
tumor prior to dissection off the carotid artery. The
only vessel that is difficult to control because it is
usually not accessible until the end of the dis-
section is a small artery that routinely arises from
the posterior aspect of the carotid bulb and enters
the base of the tumor near its attachment to the
carotid bifurcation.
All of the consultants agree that this tumor
should be surgically treated because of the pa-
tient’s young age, small tumor, and natural his-
tory of slow, progressive growth (doubling time of
4.2 years, as noted by Dr. Carroll). There is
unanimity in the need for having vascular sur-
gery colleagues available and/or present if there
is a high likelihood of carotid sacrifice. In this
patient, excisional biopsy of level II and III lymph
nodes to rule out lymphoma is also planned by
the consultants.
The finding of paraganglioma cells with sur-
rounding lymph nodes is one of the hallmarks for
malignant carotid body tumor. Unfortunately, this
was seen only on permanent, not frozen, sections;
this leaves a dilemma as to appropriate additional
treatment. The consultants all recognize that
there is very little information in the medical
literature to strongly support a particular ap-
proach. Dr. Stenson suggests completion neck dis-
section or close observation with serial CT scans,
Dr. Stringer recommends postoperative radiation
therapy, whereas Dr. Carroll suggests neck dis-
section with postoperative radiation.
This patient illustrates many of the nuances
and unanswered questions that arise in the
management of carotid body tumors. Careful
review of the clinical experience by institutions
with large cohorts of patients with this entity may
help address some of these questions.
REFERENCES
1. Shamblin WR, ReMine WH, Sheps SG, Harrison EG.Carotid body tumor (chemodectoma): clinicopathologicanalysis of ninety cases. Am J Surg 1971;122:732–739.
2. Jansen JC, van den Berg R, Kuiper A, van der Mey AG,Zwinderman AH, Cornelisse CJ. Estimation of growth ratein patients with head and neck paragangliomas influencesthe treatment proposal. Cancer 2000;88:2811–2816.
HEAD & NECK March 2004306 Malignant Carotid Body Tumor