Embed Size (px)
Citation preview

Using information technology for
resistance containment: Malaria
surveillance in the future moving toward elimination strategy • By
Wichai Satimai MD.,MA.,DTM&H
Bureau of Vector Borne diseases
Department of Disease Control
Ministry of Public Health Thailand


2.181.110.24 0
2
4
6
8
10
12
14
16
0
2
4
6
8
10
12
14
16
ABER SPR API
ABER & SPR / 100 pop. API / 1,000 pop.
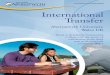
Annual Blood Examination Rate (ABER), Slide PositivityRate (SPR) and
Annual Parasite Incidence (API/1,000), Thailand FY 1965 - 2011
Fiscal Year

38.2
60.8
0
20
40
60
80
100
1965 1968 1971 1974 1977 1980 1983 1986 1989 1992 1995 1998 2001 2004 2007 2010
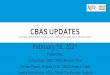
P.falciparum P.vivax
Percentage
Fiscal Year
Proportion of malaria parasite species, Thailand, FY 1965-2011
P. falciparum
P. vivax

5

0
20
40
60
80
100
1965 1968 1971 1974 1977 1980 1983 1986 1989 1992 1995 1998 2001 2004 2007 2010
P.falciparum P.vivax
Percentage
Fiscal Year
CHL SP2 SP3 QT MSP M
2005 M+ATS whole country in 2005 (2days)
M
Proportion of malaria parasite species
in relation to the National drug policy, Thailand, FY 1965-2010
1973 SP 1985
MSP
1982
QT
1990 M
1995 M+ATS ; only in Trat, Chantaburi, Tak
1965
CHL
2008 M+ATS 3 days

7
1.Mae Hong Son
2.Tak
3.Kanchanaburi
4.Ratchaburi
5.Ranong
6.Ubon Ratchathania
7.Chanthaburi
8.Trat
9.Yala
9
5
4
1
2
3 6
8
7
Nine Provinces as Sentinel sites for monitoring of
drug resistance

Tak
2004 1997
Mef 25 mg/kg + Art 12 mg/kg for 2 days N ACPR% LTF% ETF% 1997: 38 89.5 10.5 0 2002: 39 92.3 5.4 2.6 2003: 71 96.6 3.4 0 2004: 47 86.5 13.5 0 2006: 46 89 11 0
2002 2003 2006

2003
2003 2002 1997 2004
2005 2004 1997 2002 2003 2006
TAK
2003 2002 1997 2004 2002
KB
2003 2002 2004 2005 2006
RB
2003 2002 1997 2004 1998 2000
RN
MHS CHM
2002
2005
2004
2003
1998
1997
TR
2004
2002
2003
CHB
2003
2002
1997
2004
1998
1999
UB
M3 M5A12 M3A12 2006

Result 3: Efficacy of CQ, 2009-2010
MH CB YL KN
No. recruited 56 55 53 48
Lost 6 5 0 0
Withdrawn) 2 0 0 0
No. analyzed 48 50 53 48
% Parasitaemia
Day 3 8.3 30 0 31.3
% ACPR 100 96 100 93.8
% ETF 0 0 0 0
% LCF 0 0 0 0
% LPF 0 4 0 6.2

11
Implementation Areas
Only Zone 1 areas use
Atovaquone/Proguanil
The rest follows the
national drug policy
Zone 1
Sakaeo
Srisaket
Chanthaburi
Trat
Burirum
Ubonratchathani
Surin

Table 2 Primer pairs and specific restriction enzymes for detecting 3 polymorphisms at codon 268
Primer pairs and specific restriction enzymes for detecting 3 polymorphisms
Codon 268 Type Primer pair Restriction Enzyme
Product size
(base pair)
Outer primer
CYTB1+CYTB2 939
TAT Wild type CYTB3+CYTB5 NsiI 359+25
TCT Y268S CYTB2+CYTB6 AlwNI 147+24
AAT Y268N CYTB2+CYTB7 SspI 150+24
NsiI cuts TAT; AlwNI cuts TCT; SspI cuts TAT and TCT, but not AAT
DNA Sequencing

Web-based malaria surveillance: Malaria surveillance in the future moving toward
malaria elimination in Thailand

Original System: Forms are recorded, and summarized on paper

Detected cases are plotted on household walking map

To provide effective management information
system capable of coordination at operational
staff to enable rapid and high quality
implementation of malaria elimination strategy
Objective

3 out of 6 Core Modules in Vector-Borne Disease Control
have been implemented
Epidemiology Module
Vector
Control Module
BCC
Module

Key Features • Case Management (Real time – Village V.S. household level
traceable) • Case detection
• Case Investigation
• Case Follow up
• Vector Control (Effectively distributed/controlled) • The most up-to-date population survey cover any risk areas
• LLIN /LLIHN distribution
• IRS action
• Impregnated Bed Net Distribution
• Behavioral Change Communication (Individual Home Visit
information can be sent to the center for evaluating the awareness of
residences within the target areas)
• Different type of reports displayed in different presentation format
(table, graph,GIS,etc.)
• Integrate into public heath routine tasks
• Simple and easy to interpret, and user friendly

Technologies
• Web-based synchronization technology
• capable of switching between offline / online mode of data entry. This
terminology is benefit for the low resources area. Users can still operate
in case of internet link has difficulties. Then data can be later
transferred when internet is back to normal.
• Mobile Computing
• simply disseminated or received information to/from different devices in
other platforms i.e. Mobile/ Tablet
• Geographical Information System (GIS) ready
• ability to toggle GIS in key element of indicators for better understanding of the situation in short term

Work & Data Flow
EP 1
EP 3 EP 1
Not Infected
Infected
• Case
investigation • Treatment
Day 0
• Drug compliance • Case follow-up
Day 1,2,3
Pf : Day 7,14,21,28,35,42 Pv: Day 7,14,21,28,60,90
• Case follow-up
• Case Detection
MIS
VIVO
EP 1 FU

Data Capturing for Case Management
Active Case/Passive Case Detection
Location Information
Diagnosis
Treatment

Infected Cases Follow Up Schedule generated automatically

Cases Follow Up can be done through Tablet 7 inches Device

Epidemiology Summary Report

Epidemiology Reports can be displayed in different format (Table, Bar Chart, Pie, or Line), and different time frame (monthly, Weekly)

Day 0 alert will be sent using SMS
on a daily basis and
Summary on a weekly basis

Maps in Malaria GIS (http://gis.biophics.org) 1. Number of Malaria Cases
2. Malaria Incidence
3. Proportion of PF Malaria Receiving ACT
4. Proportion of PV Malaria Receiving chloroquine and
primaquine
5. Percent of PF Malaria Receiving ACT and have DOT
6. Percent of PF Malaria Receiving ACT, DOT but Day 3
Positive
7. PF Cases Receiving ACT, DOT but Day 3 Positive (by
Patient)
8. Percent of malaria cases who got investigate
9. Indigenous Case
10. Malaria Stratification Area

GIS can display number of Malaria Cases classified by administrative level up to village level

March 18, 2010
Cases Investigation captured cases which
have possible same source of infection

2009 = 54 cases
Day 3 Positive Cases (ACT) 2009-2012
2010 = 33 Cases 2011 = 14 cases 2012=81 cases

Conclusions
• New technology can become one of a major strategy to fight
against Vector-Borne Disease
• Knowledge sharing/transferring should be strengthened among
regional countries in order to exchange information across
different territories
• Regional and Global Collaborations or networking across public
health units should be initialized for the purpose of
joining/sharing disease control tasks, and lead to practical integration between working units across barriers

Thank you





![KevinMilligan MichaelSmart August2017 · Results: Ordinaryleastsquaresestimates (1) (2) (3) VARIABLES Log1%share Log1%share Log1%share Owntaxrate -2.31** -2.18*** -2.18*** [0.93]](https://img.pdfslide.us/doc/110x75/5fc2036594954800f423d29b/kevinmilligan-michaelsmart-results-ordinaryleastsquaresestimates-1-2-3-variables.jpg)