Embed Size (px)
Citation preview

MALABSORPTION SYNDROME AS A CAUSE OF TREATMENT FAILURE IN TB PATIENTS
www.uf.ua/int
STOPTB

II
MALABSORPTION OF DRUGS – ONE OF THE CAUSES OF INEFFECTIVE
TREATMENT OF TUBERCULOSIS
• diseases of the pancreas• cholestasis syndrome of any etiology• inflammatory bowel disease• Crohn's disease• autoimmune enteropathy• diabetes mellitus• amyloidosis• systemic sclerosis• autonomic neuropathy• hyperthyroidism• Zollinger-Ellison syndrome• atrophic gastritis
DISEASES AND CONDITIONS THAT OCCUR WITH MALABSORPTION SYNDROME:
• neurofibromatosis• resection of the pancreas, stomach• infectious and parasitic gastrointestinal
lesions• HIV / AIDS• TB• alcoholism• aging
is a clinical syndrome that is characterized by impaired absorption of nutrients, vitamins, minerals and drugs from the gastrointestinal tract.
MALABSORPTION SYNDROME

III
ONE OF THE MOST SERIOUS CONSEQUENCES OF MALABSORPTION SYNDROME IN TB PATIENTS IS POOR ABSORPTION OF ORAL ANTI-TB DRUGS, WHEREUPON PATIENTS DO NOT REACH THEIR REQUIRED CONCENTRATION IN BLOOD AND FOCI OF INFECTION, WHICH LEADS TO TREATMENT FAILURE AND DEVELOPMENT OF MDR-TB
Malabsorption syndrome is a common comorbid condition in most TB patients, which is associated with a specific impairment of transport in the intestines caused both by an infection, and the negative impact of anti-TB drugs in the lining of the stomach and intestines. The result is a vicious circle:
MALABSORPTION SYNDROME AND TUBERCULOSIS
PROGRESSION OFTUBERCULOSIS
MALABSORPTION SYNDROME
DECREASED ABSORPTIONOF ANTI-TB DRUGS

IV
Serum concentration of anti-TB drugs in patients with MDR-TB is further reduced.²
HIV-infected patients have malabsorption of anti-TB drugs even in the absence of symptoms of the gastrointestinal tract dysfunction.³
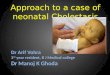
IN THE MAJORITY OF TB PATIENTS RECEIVING ORAL TREATMENT CONCENTRATION OF ANTI-TB DRUGS IN PLASMA IS EXTREMELY LOW
Presumably, this is caused by the decrease of functional intestinal absorption zone in TB patients. New ways of improving the bioavailability of anti-TB drugs are required.¹
!
per os per os
The minimum normal level (8 mcg/ml)
The maximum normal level (24 mcg/ml)
The maximum normal level (6 mcg/ml)
The minimum normal level (3 mcg/ml)
Tuberculosis Tuberculosis
The
conc
entr
atio
n of
rifa
mpi
cin
in th
e se
rum
(mcg
/ml)
Ison
iazi
d co
ncen
trat
ion
in s
erum
(mcg
/ml)
КThe
con
cent
ratio
n of
rifa
mpi
cin
in th
e se
rum
(mcg
/ml)
Maximum therapeutically significant level (6 mcg/ml)
The minimum therapeutically significant levels (3 mcg/ml)
The minimum therapeutically significant level (8 mcg/ml)
MDR-TB Susceptible TB Healthy
1. MDR-TB vs. healthy people / 2. Susceptible TB vs. healthy people / 3. MDR-TB vs. susceptible TB
Ison
iazi
d co
ncen
trat
ion
in s
erum
(mcg
/ml)
Maximum therapeutically significant level (24 mcg/ml)
per os per os
MDR-TB Susceptible TB Healthy
1. Valéria G. F. et al., Intestinal Permeability and Malabsorption of Rifampin and Isoniazid in Active Pulmonary Tuberculosis - The Brazilian Journal of Infectious Diseases 2006;10(6):374-379
2. Elizabeth C. Barroso et al.,Serum Concentrations of Rifampin, Isoniazid, and Intestinal Absorption, Permeability in Patients with Multidrug Resistant Tuberculosis - Am. J. Trop. Med. Hyg., 81(2), 2009, pp. 322–329
3. Mehta JB et al., Utility of rifampin blood levels in the treatment and follow-up of active pulmonary tuberculosis in patients who were slow to respond to routine directly observed therapy. Chest 2001;120:1520–4

V
In patients receiving optimal anti-TB treatment per os, in which clinical, radiological or microbiological improvements are not achieved in the DOT regimen it is necessary to suspect the malabsorption syndrome⁴
• 100% bioavailability• quick achieving the high concentrations of the drug
in the foci of infection regardless of the state of the digestive tract, the characteristics of the diet and comorbidities
• reducing the number of side effects• possibility to intensify treatment• reduction of cases of interruption of therapy
(100% control)• accurate dosing
BENEFITS OF INTRAVENOUS ADMINISTRATION OF ANTI-TB DRUGS
4. Mehta JB et al., Chest, 2001; Kimerling ME et al., Chest, 1998; McIlleron H, Antimicrob Agents Chemother, 2006; Peloquin CA, N Engl J, 1993; Patel KB, Belmonte R, Crowe HM, N Engl J Med, 1995; Peloquin CA, Drugs 2002
5. Treatment of Tuberculosis. - American Thoracic Society, CDC, and Infectious Diseases Society of America
TO RESOLVE THIS PROBLEM IN THE GUIDELINE ON TREATMENT OF TUBERCULOSIS THE AMERICAN THORACIC SOCIETY, CDC, AND INFECTIOUS DISEASES SOCIETY OF AMERICA STATE: PARENTERAL THERAPY IS INDICATED FOR SEVERELY ILL PATIENTS WHO CANNOT TAKE ORAL THERAPY AND PATIENTS FOR WHOM POOR ABSORPTION HAS BEEN DOCUMENTED. PREPARATIONS OF ISONIAZID, RIFAMYCINS AND MOST FLUOROQUINOLONES ARE AVAILABLE FOR INTRAVENOUS ADMINISTRATION5
!

VI
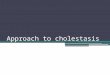
The concentrations of anti-TB drugs in the blood and the foci of infection in patients of intravenous treatment group was almost 5 times higher than in the group of oral chemotherapy, which was accompanied by an increase in the frequency of sputum conversion in the intensive phase of treatment (94.7% vs. 79.0%, respectively) and shortening time of healing cavities from 3.9 to 3.0 months (p = 0.05 ).
CLINICAL EFFICACY OF THE MODIFIED TREATMENT REGIMEN IN PATIENTS WITH NEWLY DIAGNOSED PULMONARY TB6
Patients of the main group in the intensive phase of treatment as part of chemotherapy received isoniazid, rifamycin SV sodium and ethambutol intravenously, in the control group the same drugs in similar doses patients received orally.
rifamycin SV sodium intravenously
rifampicin per os
DYNAMICS OF THE BLOOD CONCENTRATION AFTER RIFAMYCIN ADMISSION PER OS AND IV
20
15
10
5
01 2 3 4 5 6
mcg/ml
hours
6. M.M. Kuzhko. - Proceedings of the 5th International Scientific and Practical Conference on Tuberculosis and Lung Diseases, October 20-22, 2011, Baku, the Azerbaijan Republic

VII
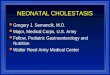
Our case is a 15-year-old male student, previously healthy and who presented with a 5-month history of cough, sputum, anorexia and weight loss (10 kg). He presented no vomits and his bowel history was normal, with no diarrhoea. He was taking no medication. He was non-smoker and had no alcohol or drug addiction. Clinical, radiological and microbiological evaluation supported the diagnosis of respiratory TB. Daily oral weight-adjusted standard combination therapy (isoniazid (INH):300 mg, rifampicin (RIF): 600 mg, pyrazinamide (PZA): 1500 mg and ethambutol (EMB): 1200 mg) was started. Patient’s HIV status was negative. Sputum-culture exam confirmed Myco-bacterium tuberculosis sensitive for all first-line drugs in use. Nevertheless, patient failed to improve (clinical and radiologically) and monthly repeated sputum smear during first 4 months of treatment showed persistence of acid-fast bacilli (AFB). Assuming the possibility of malabsorption of anti-TB drugs, patient was prescribed with intravenous INH, RIF and streptomycin (SM) while continuing intake of daily oral PZA and EMB. Meanwhile, patient began to improve clinically, 1 month after mycobacterial charge was signifi-cantly reduced and 2 months after he was asymptomatic and gaining weight. By that time chest X-ray was improving and since then sputum smear became persistently AFB negative. Cultural exams turned to negative only after the third month of treatment. This patient had good tolerance to intravenous treatment and no side effects.
Chest X-ray (after 4 months of initial treatment). Worsening radiological pattern: more exuberant bilateral lung infiltrate and larger cavitary lung
lesion on the left
MALABSORPTION OF ANTIMYCOBACTERIAL DRUGS AS A CAUSE OF TREATMENT FAILURE IN TUBERCULOSIS7
Chest X-ray (after complete treatment). Almost complete chest X-ray abnormalities resolution
7. Joro Bento. Malabsorption of antimycobacterial drugs as a cause of treatment failure in tuberculosis – BMJ Case Reports 2010; doi: 10.1136/bcr.12.2009.2554
Case report

YURiA-PHARM ltd10 Amosova str., Kiev, Ukraine, 03680phone/fax: +38 (044) 275-01-08 +38 (044) 275-92-42www.uf.ua/int
ISONIAZID (100 mg/5ml syrup)
• Accurate dosing• Convenient administration• Pleasant taste and smell• Lower risk of side effects
RIFONAT (30 mg/ml rifamycin concentrate for preparation of infusion solution)
• One of the most effective antituberculosis drugs• Infusion administration provides for the highest effectiveness of treatment• Lower risk of gastric side effects• Overcome resistance of МTB
INBUTOL (ethambutol hydrochloride, 10% infusion solution)
• 100% controllable therapy• Maximal efficiency• Maximal safety
PASKONAT (paraaminosalicylic acid, 3% infusion solution)
• Long history of use in tuberculosis treatment• Low development of MTB resistance• Increases effect of other antituberculosis drugs
CON
TRO
LLA
BIL
ITY
EFF
ECTI
VEN
ESS!
&