Embed Size (px)
Citation preview
MALABSORPTION
Dr. Gehan M. Osman
MBBS, MD Pediatrics
Jaffar Ibn Auf Specialized Hospital
National University
Faculty of Medicine
Definition
Malabsorptive disorders are conditions that cause insufficient assimilation of ingested nutrients as a result of either maldigestion or malsbsorption.
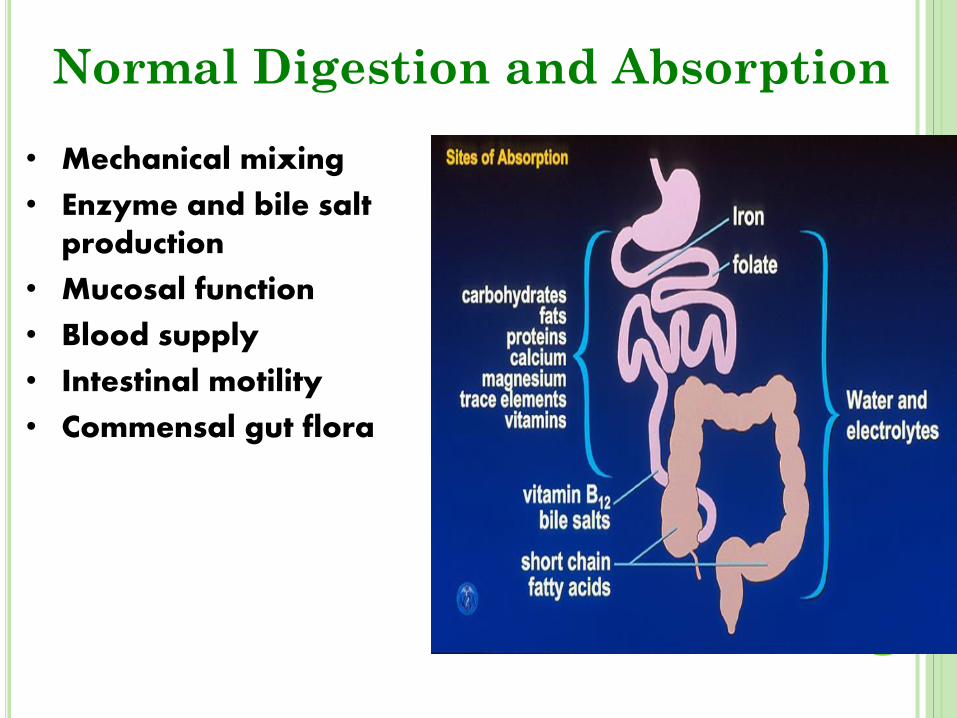
Normal Digestion and Absorption
• Mechanical mixing
• Enzyme and bile salt production
• Mucosal function
• Blood supply
• Intestinal motility
• Commensal gut flora
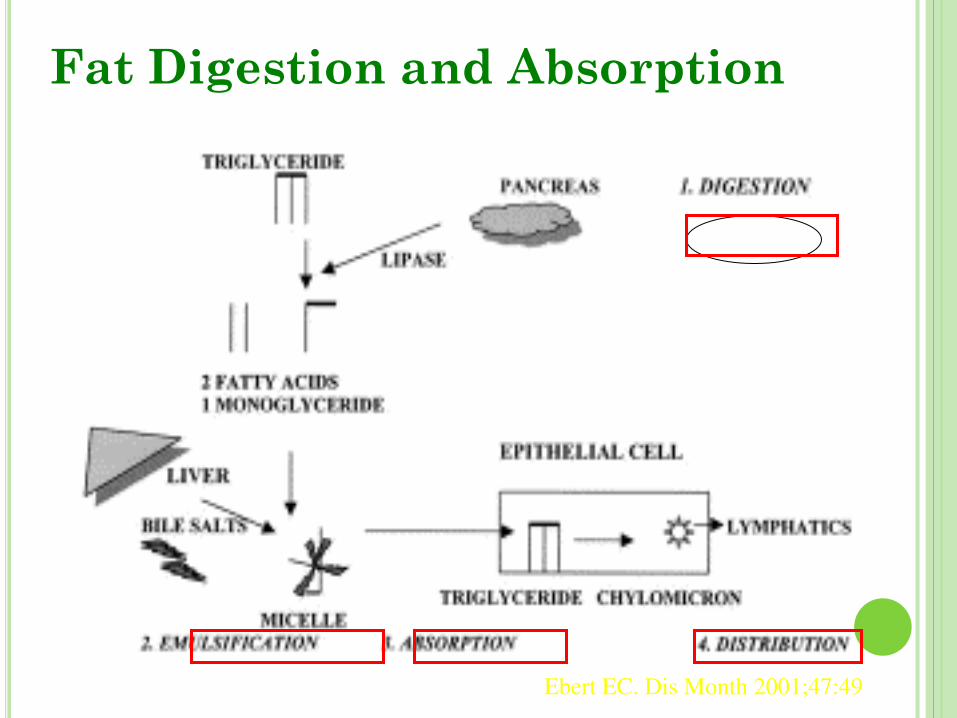
Fat Digestion and Absorption
Ebert EC. Dis Month 2001;47:49
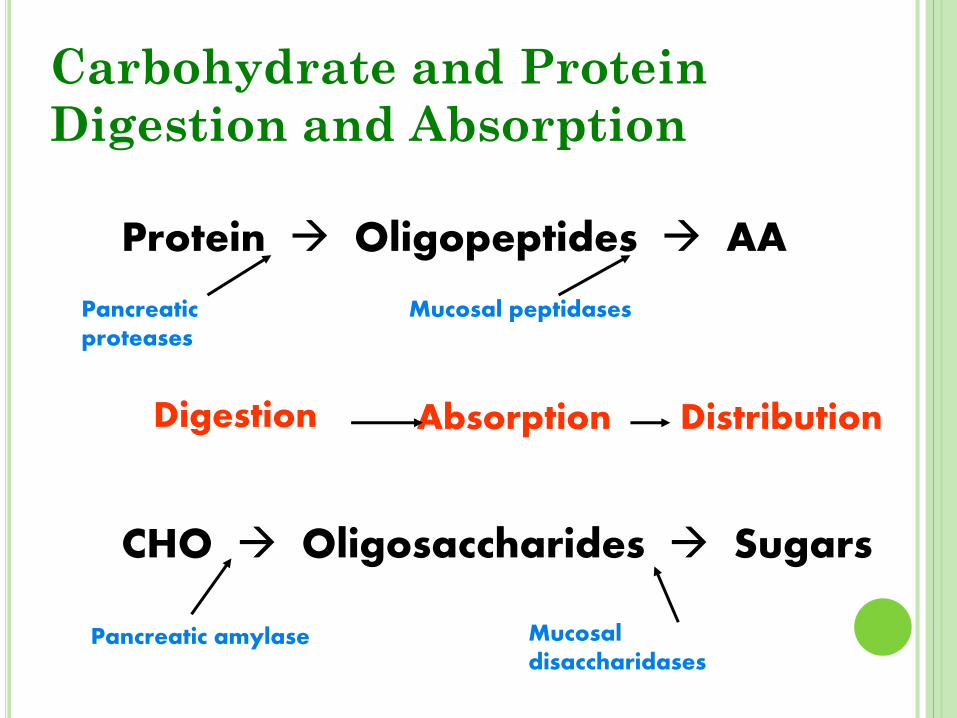
Carbohydrate and Protein
Digestion and Absorption
Protein Oligopeptides AA
CHO Oligosaccharides Sugars
Pancreatic amylase Mucosal disaccharidases
Pancreatic proteases
Mucosal peptidases
Digestion Absorption Distribution
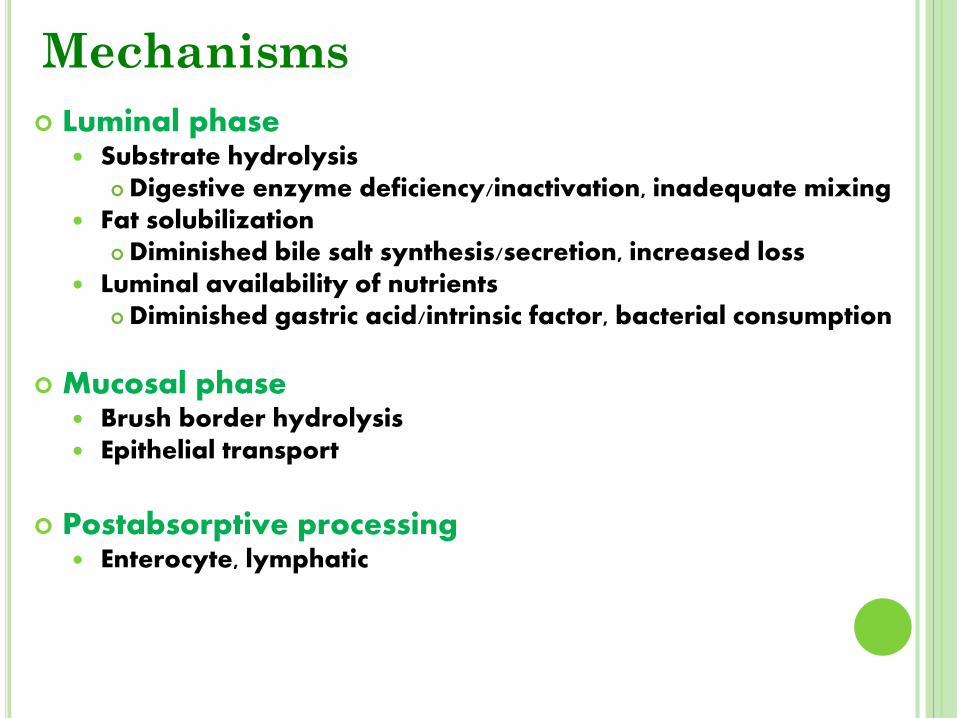
Mechanisms
Luminal phase Substrate hydrolysis
Digestive enzyme deficiency/inactivation, inadequate mixing Fat solubilization
Diminished bile salt synthesis/secretion, increased loss Luminal availability of nutrients
Diminished gastric acid/intrinsic factor, bacterial consumption
Mucosal phase Brush border hydrolysis Epithelial transport
Postabsorptive processing Enterocyte, lymphatic
Causes Exocrine pancreatic insufficiency
ch. Pancreatitis pancreatic CA cystic fibrosis
Inactivation of pancreatic lipase Gastrinoma (ZES)
drugs (orlistat) bile acid (impaired micelle
formation) cholestatic liver dis
Bacterial overgrowth Anatomic stasis (blind loop,stricture,fistula) Functional stasis (DM, scleroderma)
Interrupted enterohepatic circulation of bile acid (ileal resection, Crohn’s )
Drugs (bind or precipitate b. salt) neomycin, chlestyramine
Impaired mucosal absorbtion/ mucosal loss or defect
intestinal resection or bypass inflammation/infiltration/infct (celiac, tropical sprue, lymphoma, scleroderma, Crohn’s
Impaired nutrient transport lymphatic obstruction
(lymphoma, lymphangectasia) CHF
Genetic disorders disacharidase defficiency Agamaglobulinemia
Endocrine/Metabolic disorders DM
Hyperthyroidism adrenal insufficiency
carcinoid syndrome
Malabsorption Causes Generalized Defect:
Present with similar signs and symptoms; abdominal distention; pale, foul smelling, bulky stools; muscle wasting; poor weight gain or weight loss; and growth retardation.
A. Exocrine pancreas: cystic fibrosis, chronic pancreatitis, chronic protein calorie malnutrition, Shwachmann-Diamond syndrome.
B. Liver: biliary atresia, familial neonatal hepatitis, other cholestatic states.
C. Intestine: massive resection, giardiasis, celiac disease, cow milk protein intolerance, immune deficiency, tropical sprue.
The clinical features of these disorders typically differ from those of generalized malabsorptive disorders, some present without gastrointestinal disorders.
A. Intestinal: abetalipoproteinemia, Hartnup disease, disaccharidase deficiency, vit.B12 malabsorption, glucose - galactose malsbsorption, Chloride losing diarrhea, acrodermatitis enteropathica.
B. Drug induced: sulfasalazine(folate), phenytoin (Calcium)
C. Pancreatic: Specific enzyme deficiency like lipase, trypsinogen.
Malabsorption Causes Speclized Defect:
1) Impaired fat absorption:
i) Pancreatic lipase is necessary for triglyceride hydrolysis in duodenum.
Pancreatic enzyme deficiency leads to fat malabsorption.
ii) Inactivation of pancreatic lipase by low gastric luminal pH – fat malabsorption.
iii) Interruption of enterohepatic circulation of bile salt – impaired micelle formation – fat malabsorption.
Absorption of fat soluble vitamins may be impaired as well.
3) Impaired protein absorption:
Hydrolysis of polypeptides occurs mainly in small intestine by action of pancreatic enzyme trypsin,
chymotrypsin.
Deficiency of pancreatic proteases – impaired
protein absorption.
Diseases like:
Chronic pancreatitis
Cystic fibrosis
Ca. pancreatic resection
- Protein malnutrition
Clinical features
Depend on the cause and severity
Global
Diffuse mucosal- involvement
Impaired absorption of all nutrients
Classic manifestation Diarrhea(steatorrhea) weight loss
Majority – sub clinical
E.g.. Celiac disease
Partial (isolated)
2° to diseases that interfere with absorption of specific nutrients E.g. Pernicious Anemia Lactase deficiency
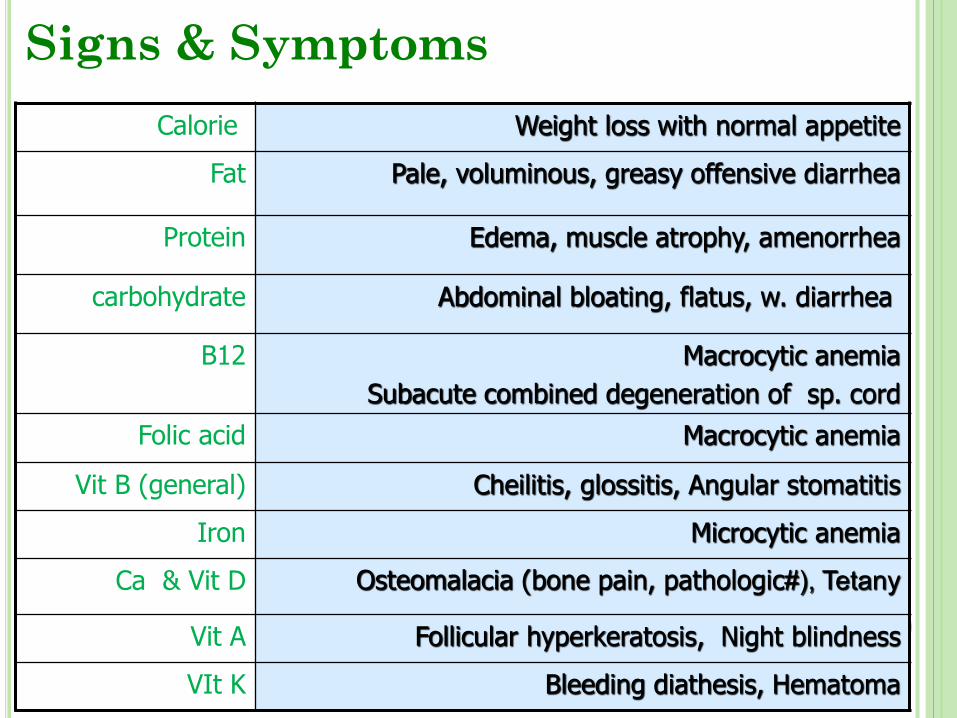
Signs & Symptoms
Calorie Weight loss with normal appetite
Fat Pale, voluminous, greasy offensive diarrhea
Protein Edema, muscle atrophy, amenorrhea
carbohydrate Abdominal bloating, flatus, w. diarrhea
B12 Macrocytic anemia Subacute combined degeneration of sp. cord
Folic acid Macrocytic anemia
Vit B (general) Cheilitis, glossitis, Angular stomatitis
Iron Microcytic anemia
Ca & Vit D Osteomalacia (bone pain, pathologic#), Tetany
Vit A Follicular hyperkeratosis, Night blindness
VIt K Bleeding diathesis, Hematoma
History and Exam
• Prior GI surgery
• h/o chronic pancreatitis
• h/o liver, GI disorder
• h/o CTD, diabetes
• h/o radiation therapy
• Diet and medications
• Alcohol/drugs
• h/o chronic sinus or respiratory infections
• Recent travel history
• Timing of onset
• Bowel habits/stool characteristics
• Associated GI and systemic complaints
• Evidence of malnutrition or micronutrient deficiencies on exam
General:
- CBC: microcytosis, macrocytosis, lymphopenia
- RFT: low urea & creatinine, hypokalemia
- hypocalcemia, low s. albumin
- prolonged PT
- low s. Fe, vit B12, folate
- low s. carotene, cholesterol
History and Exam
Specific:
Tests of fat absorption:
Quantitative fecal fat
Patient should be on daily diet containing 80-100 grams of fat.
Fecal fat estimated on 72 h collection.
6 grams or more of fat/day is abnormal.
May be due to: - Pancreatic dis
- Small intestinal dis
- Hepatobiliary disease
Fecal Fat Determination
Qualitative
• Random spot sample
– Qualitative (Sudan stain)
– Semi-quantitative (#/size of droplets)
– Acid steatocrit
• Less sensitive for mild-moderate steatorrhea
• Variable reproducibility
• Helpful only if abnormal
D-xylose Test
• Indicates malabsorption secondary to mucosal dysfunction
• Oral load with 25 g D-xylose
– 5 hr urine collection (normal > 4 g)
– 1 hr and 3 hr serum samples (normal > 20 mg/dl at 1 hr, > 18.5 mg/dl at 3 hr)
• Numerous factors affect results
• Role in clinical practice controversial
– ? Use in special populations
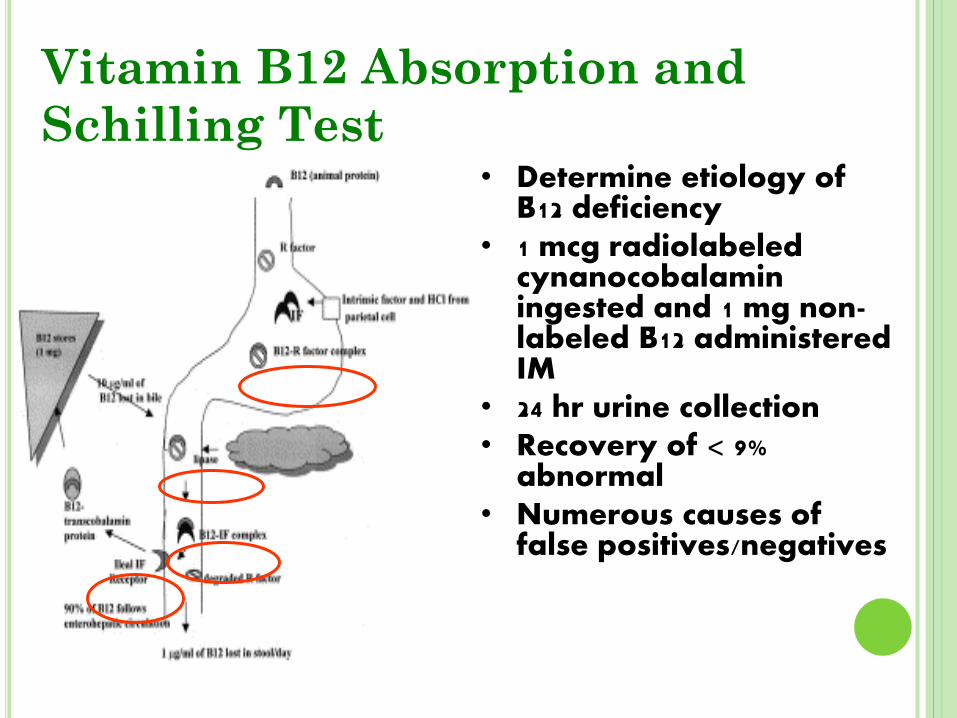
Vitamin B12 Absorption and
Schilling Test • Determine etiology of
B12 deficiency • 1 mcg radiolabeled
cynanocobalamin ingested and 1 mg non-labeled B12 administered IM
• 24 hr urine collection • Recovery of < 9%
abnormal • Numerous causes of
false positives/negatives
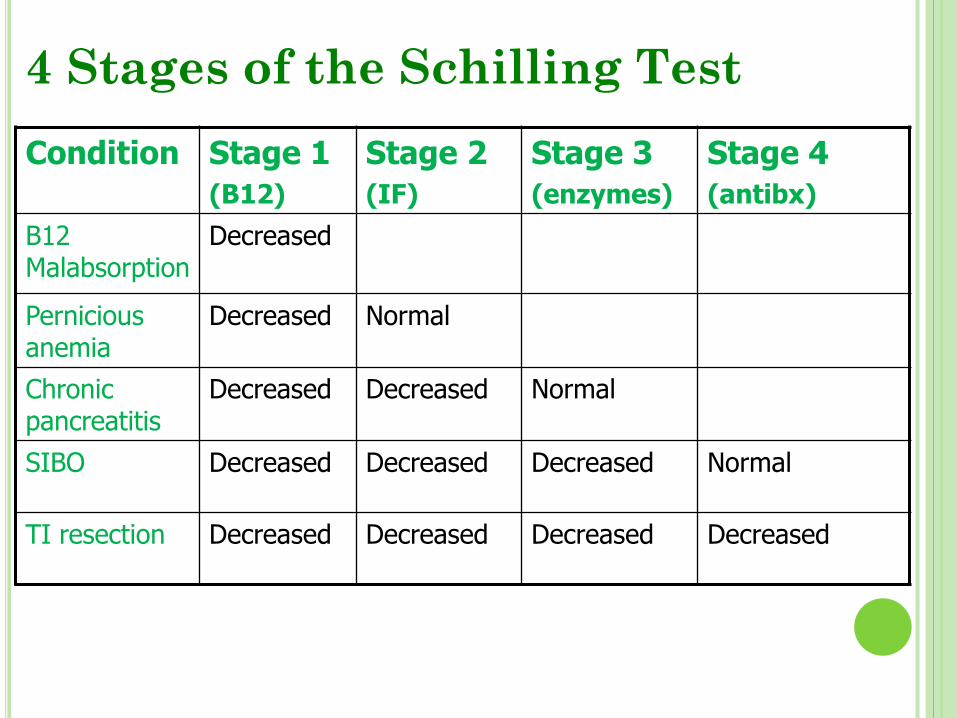
4 Stages of the Schilling Test
Condition Stage 1
(B12)
Stage 2
(IF)
Stage 3
(enzymes)
Stage 4
(antibx)
B12 Malabsorption
Decreased
Pernicious anemia
Decreased Normal
Chronic pancreatitis
Decreased Decreased Normal
SIBO Decreased Decreased Decreased Normal
TI resection Decreased Decreased Decreased Decreased
Direct Pancreatic Function Tests
• Gold standard
• Quantitative stimulation tests using either secretin or CCK or test (Lundh) meal
• Requires Dreiling tube placed into duodenum with collection of contents for an hour
• Analyzed for bicarbonate (secretin) or amylase/lipase/trypsin (CCK)
• Low concentrations (< 80-90 mEq/L HCO3; < 780 IU/L lipase) consistent with pancr. insuff.
• Limited by availability, invasiveness, expense
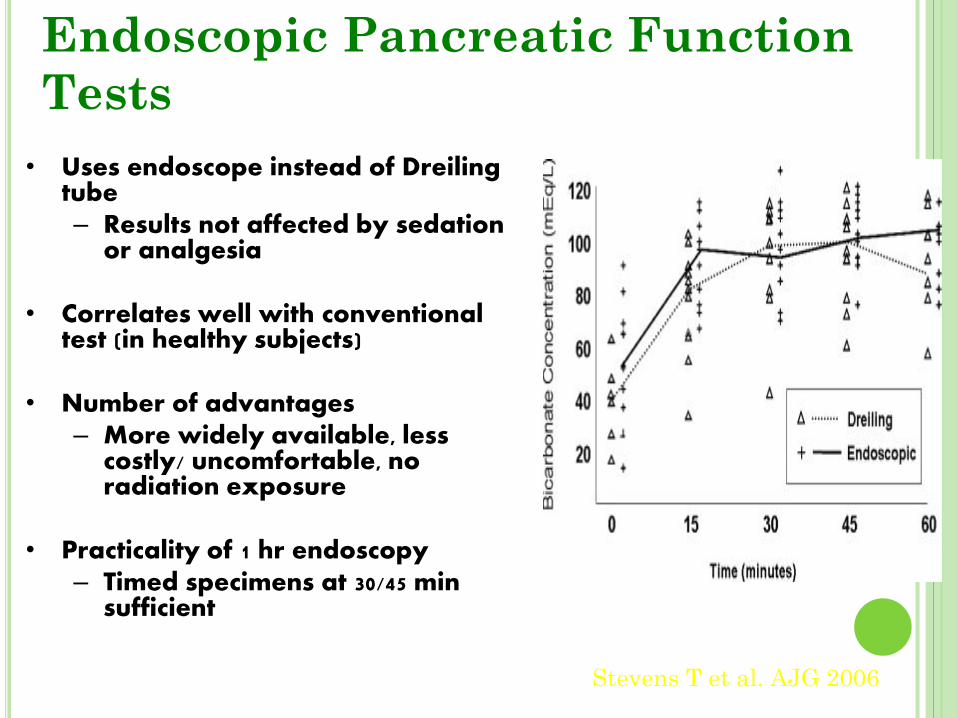
Endoscopic Pancreatic Function
Tests
• Uses endoscope instead of Dreiling tube – Results not affected by sedation
or analgesia
• Correlates well with conventional test (in healthy subjects)
• Number of advantages
– More widely available, less costly/ uncomfortable, no radiation exposure
• Practicality of 1 hr endoscopy
– Timed specimens at 30/45 min sufficient
Stevens T et al. AJG 2006
Indirect Pancreatic Function Tests
• Serum trypsinogen/trypsin
• Fecal chymotrypsin
• Fecal elastase-1
• Pancreolauryl test
• Bentiromide test
• Trial of pancreatic enzymes
“Tubeless tests”
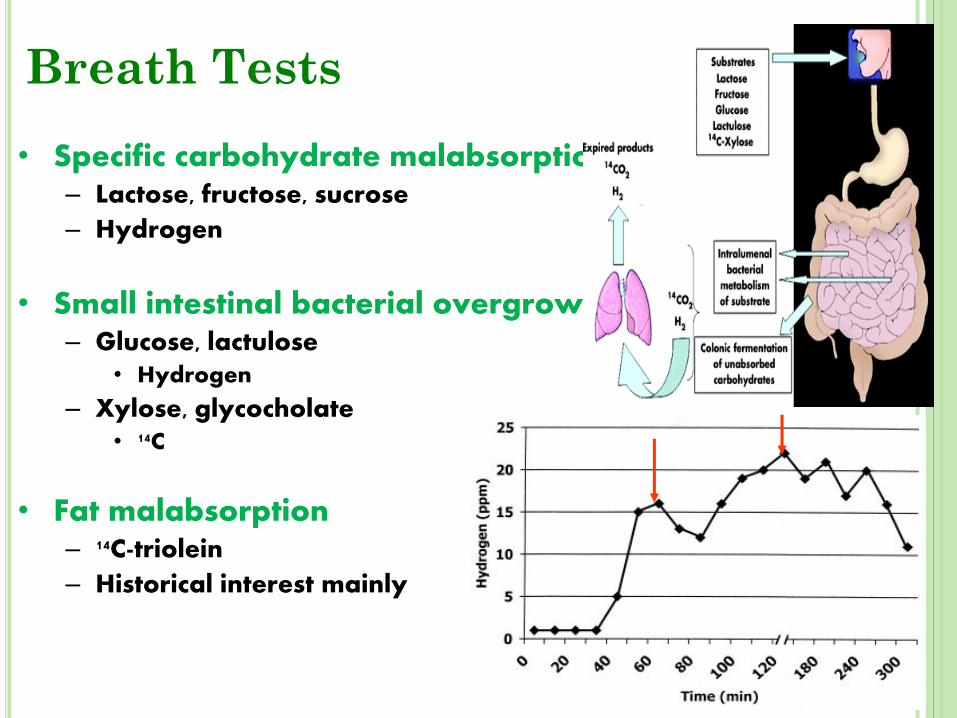
Breath Tests
• Specific carbohydrate malabsorption – Lactose, fructose, sucrose
– Hydrogen
• Small intestinal bacterial overgrowth – Glucose, lactulose
• Hydrogen
– Xylose, glycocholate
• 14C
• Fat malabsorption – 14C-triolein
– Historical interest mainly
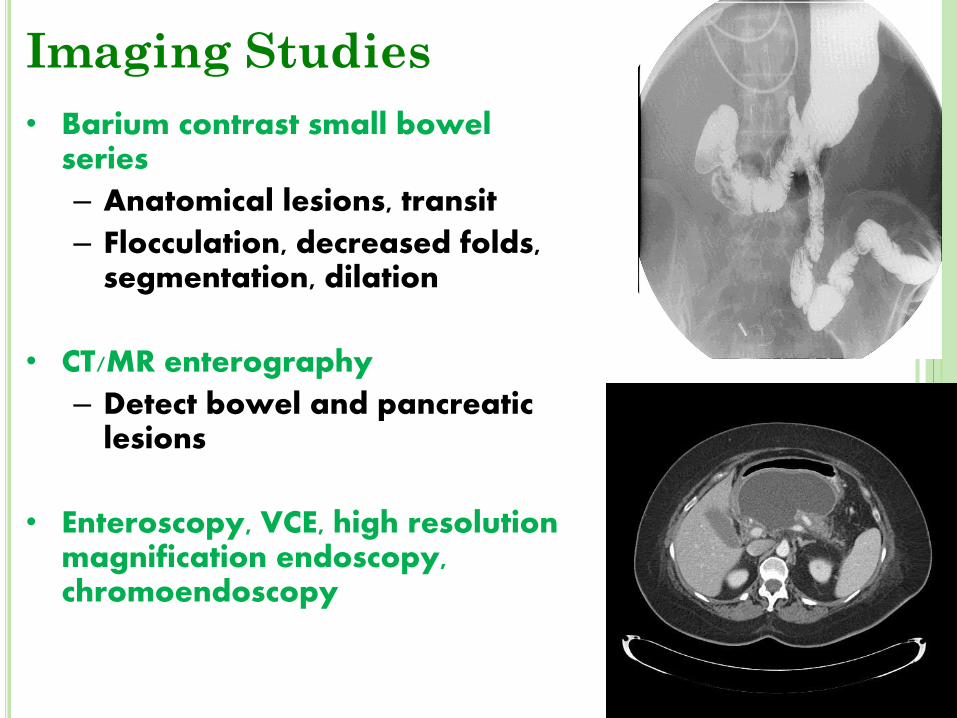
Imaging Studies
• Barium contrast small bowel series
– Anatomical lesions, transit
– Flocculation, decreased folds, segmentation, dilation
• CT/MR enterography
– Detect bowel and pancreatic lesions
• Enteroscopy, VCE, high resolution magnification endoscopy, chromoendoscopy
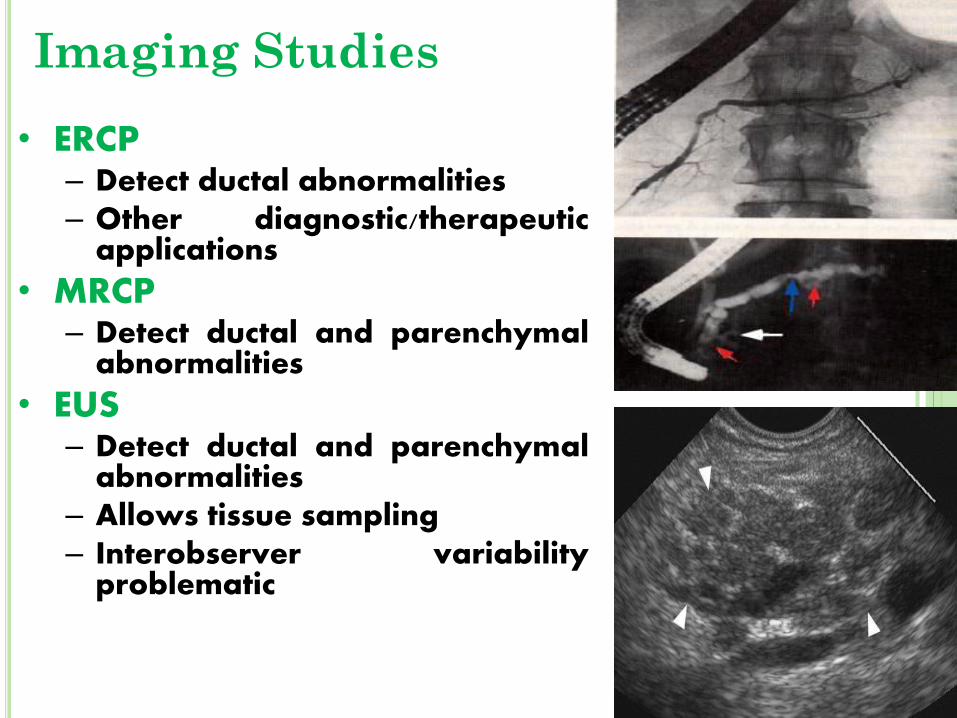
Imaging Studies
• ERCP – Detect ductal abnormalities – Other diagnostic/therapeutic
applications
• MRCP – Detect ductal and parenchymal
abnormalities
• EUS – Detect ductal and parenchymal
abnormalities – Allows tissue sampling – Interobserver variability
problematic
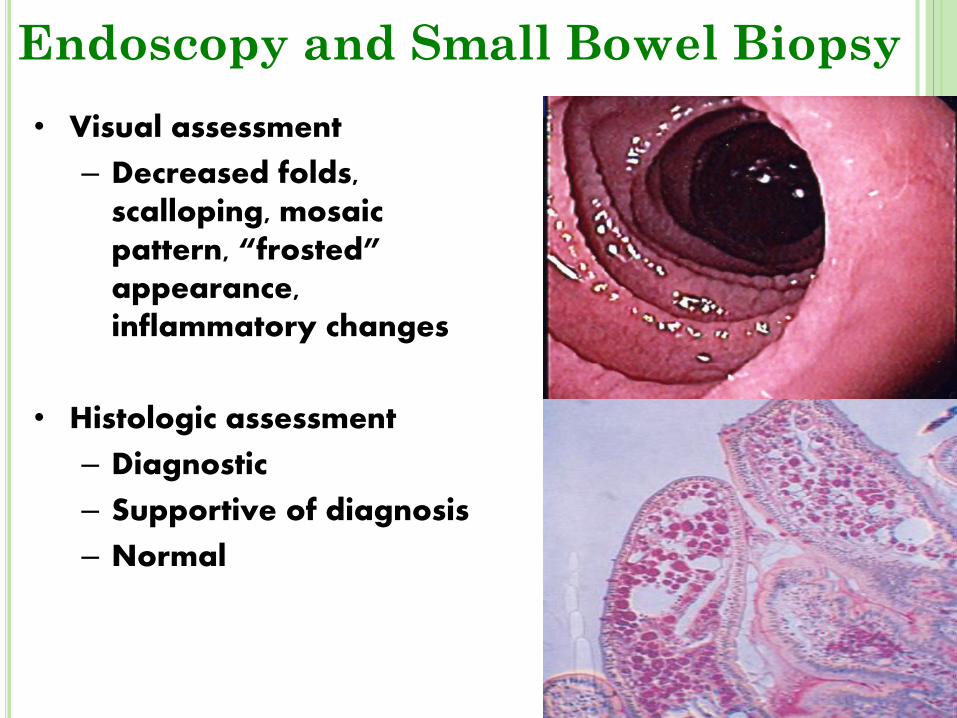
Endoscopy and Small Bowel Biopsy
• Visual assessment
– Decreased folds, scalloping, mosaic pattern, “frosted” appearance, inflammatory changes
• Histologic assessment
– Diagnostic
– Supportive of diagnosis
– Normal
Tests of Fat Malabsorption
• Fecal fat collection
• Spot fecal fat
• 14C-triolein, 13C-triglyceride breath tests
• Near infrared reflectance analysis (NIRA)
– Can measure fecal fat, nitrogen and CHO
– As accurate but less time consuming then 72 hr fecal fat collection
– Not widely available
Tests of Carbohydrate
Malabsorption
• Oral breath tests
• Quantitative analysis of fecal CHO
• Stool pH
• Oral tolerance tests
• Direct assay of mono- and disaccharidases
Tests of Protein Malabsorption
• Nutrient balance studies with fecal nitrogen measurement
• Radioisotopic methods
– 51Cr-labeled albumin
– 99mTc-labeled transferrin
– 125I-labeled albumin
• Indirect methods
– Fecal -1 antitrypsin clearance (> 25 mg/d)
Celiac disease Gluten sensitive
enteropathy
• Environmental, genetic, and immunologic factors, some of which are clear and others that are only now beginning to come into focus, are important in the pathogenesis of celiac disease.
• The disease activating proteins in wheat, rye, and barely widely termed Glutens.
• Celiac disease is strongly associated with HLA class II genes on DQ locus. DQ2 &DQ8.
Celiac disease Clinical features
Most children show symptoms between nine and 24 months , but the condition may occur at any age. Malabsorption causing diarrhea, failure to thrive, abdominal distention, and muscle wasting is the classic presentation.
Also seen are vomiting, anorexia, irritability, isolated abdominal distention, short stature, unexplained iron deficiency anemia, rickets, glossitis and angular stomatitis,delayed puberty,infertlity .
Celiac disease
Diagnosis
• Serological screening: antiendomyseal IgA and IgG antibodies are recommended. Antigliadin and Antireticulin antibodies can also be of help.
• If serological screening is positive a small bowel biopsy should be performed.
Demonstration of inflammation, villous atrophy and crypt hyperplasia is consistent with the diagnosis. ”Marsh classification”
Celiac disease
Therapy • Dietary: Life long provision of gluten free diet. All
wheat, rye, and barely should be eliminated from the diet.
• Initially while small intestinal mucosa heal, restriction of lactose as well as vitamin and iron supplementation may be necessary.
• Improvement of mood and appetite is followed by lessening of diarrhea usually within 1 week of starting therapy.
Celiac disease
Prognosis
• Diabetes mellitus, IgA deficiency, and other autoimmune disease have high incidence among celiac patients.
• The late development of bowel lymphoma in long standing cases with poor adherence to diet is possible.
• No complications from long term gluten free diet treatment are recognized.
Cow milk protein allergy
• The precise mode by which cow’s milk protein cause disease is unknown. Sensitization may occur de novo or after a bout of acute infectious enteritis.
Variable mucosal abnormalities may be found in the stomach, small bowel, and colon.
Infants who are sensitive to cow’s milk protein may also be sensitive to soy protein.
Cow milk protein allergy
Clinical features
• Most symptoms develop in the first 3 months of life.
1. Diarrhea and vomiting are the most common and if prolonged lead to failure to thrive.
2. Rectal bleeding may be seen if allergic colitis occur.
3. Edema secondary to protein losing enteropathy, often associated with anemia.
4. Wheezing, rhinorrhea, and eczema may occur.
Cow milk protein allergy
• Diagnosis
is usually made empirically once symptoms resolve after elimination of cow’s milk.
• Therapy:
elimination of cow’s milk from the diet is usually curative although severely affected infants may take weeks or months to recover and may require IV alimentation until the intestinal mucosa heals.
Lactose intolerance
Lactase deficiency
Lactose enzyme located on the brush border membrane of the small bowel epithelial cells, hydrolyses lactose into glucose and galactose before their absorption.
If this hydrolysis is incomplete the sugar will accumulate in the distal intestinal lumen where organic acids and hydrogen gas are produced by bacteria.
Lactose intolerance
Lactase deficiency
The excess intraluminal sugar and organic acids draw water into the lumen leading to osmotic diarrhea.
• Lactase deficiency is a common cause of diarrhea in childhood. Congenital absence of lactase is rare while acquired lactase deficiency is usually secondary to a diffuse mucosal disease like infectious diarrhea or celiac disease.
Lactose intolerance
Clinical manifestations
In response to ingestion of lactose (milk) Explosive watery diarrhea is associated with abdominal distention, borborygmi, flatulence, cramping abdominal pain, and an excoriated diaper area.
Lactose intolerance
Diagnosis
1. Breath hydrogen testing; is the most accurate
diagnostic test.
2. Stool PH; less than 5.6 and presence of reducing substance + 2 and more suggest carbohydrate malabsorption.
3. Intestinal biopsy; Direct assay of brush border enzyme activity.
Lactose intolerance
Therapy
1. Elimination of cow’s milk and substitution by lactose free milk.
2. Lactaid is a lactase preparation when added to milk it allows asymptomatic consumption of modest quantities of milk incubated with the added enzyme.
Malabsorption due to bacteral
over growth of small bowel
Normal small intestine is bacterial sterile due to:
– Acid
– Int. peristalsis (major)
– Immunoglobulin
Cause of bacterial growth.
e.g.
– Small intestinal diverticuli
– Blind loop
– Strictures
– DM/ Scleroderma
Pathophysiology
1) Bacterial over growth: Metabolize bile salt resulting in deconjugation of bile salt Bile Salt Impaired intraluminal micelle formation
Malabsorption of fat.
2) Intestinal mucosa is damaged by
Bacterial invasion Toxin Metabolic products Damage villi may cause total villous atrophy.
Clinically: Steatorrhea Anaemia B12 def. Reversed of symptom after antibiotic treatment. Diagnosis: Breath test Cxylose test Culture of aspiration (definitive) Treatment: Antibiotic Tetracyclin Ciproflexacin Metronidazole Amoxil
Protein-Losing Enteropathy
• Characterized by excessive loss of serum proteins into the gut
– Hypoproteinemia, hypoalbuminemia, edema, muscle atrophy
• May occur as isolated phenomenon or part of global malabsorption
• Need to r/o malnutrition, nephrosis, liver
disease
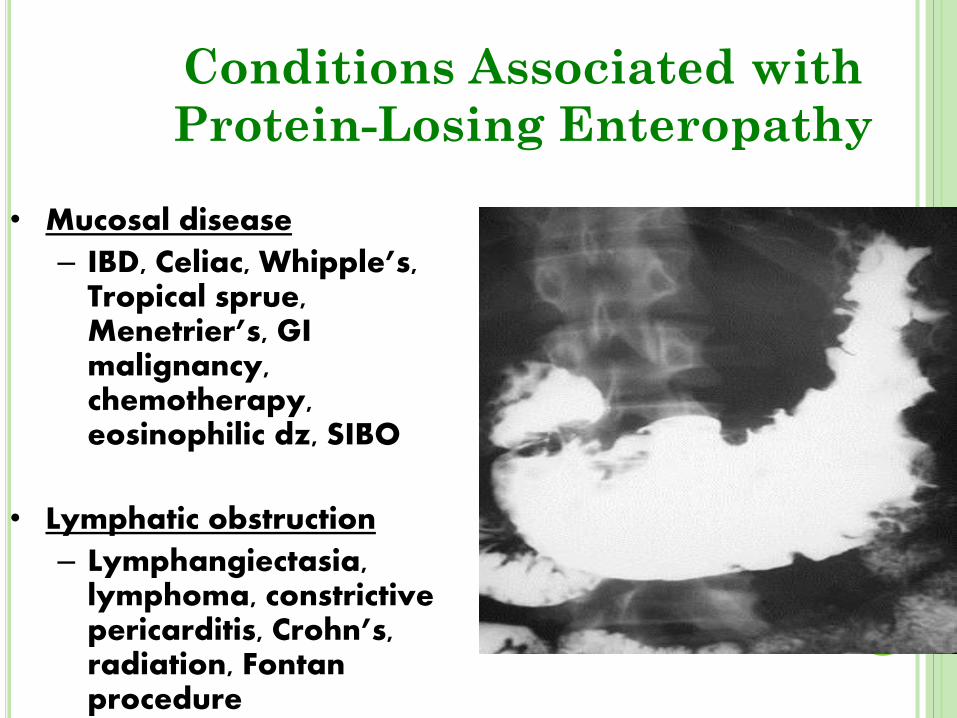
Conditions Associated with
Protein-Losing Enteropathy
• Mucosal disease
– IBD, Celiac, Whipple’s, Tropical sprue, Menetrier’s, GI malignancy, chemotherapy, eosinophilic dz, SIBO
• Lymphatic obstruction
– Lymphangiectasia, lymphoma, constrictive pericarditis, Crohn’s, radiation, Fontan procedure
Postgastrectomy malabsorption
the risk is greatest after total gastrectomy and progressively decreases after partial gastrectomy and gastrojejunal anastomoses (Billroth II), antrectomy and gastric- duodenal
anastomoses (Billroth I)
Mechanism Several mechanisms, the most common is the
"poor mixing and poor timing." Rapid gastric emptying coupled with decreased release of secretin and cholecystokinin results in suboptimal exposure of the nutrient bolus to both bile salts and pancreatic enzymes as it traverses the small intestine.
Intestinal lymphoma
Primary lymphoma usually not
associated with malabsorption.
Enteropathy-associated T-cell
lymphoma (EATL) and Small
Intestinal Immuo-Proliferative
Disease (IPSID): both cause
malabsorption.
PSID
IPSID is common in young in Middle East, cause diffuse infiltration of mucosa and submucosa with B lymphocytes and plasma cells:
Abdominal pain, anorexia, diarrhea, wt loss, and as disease progresses: ascites and hepatosplenomegaly
Dx: serum protein electrophoresis
Rx: prolonged course antibiotics(6 m): tetracycline, metro esp. in early disease, but once frank lymphoma is established: combination chemotherapy± radiotherapy
Take Home Points Approach to Suspected
Malabsorption • History
• Physical exam
• Routine “screening” labs
• Stool analysis
• Selective tests based on above findings
• Treat based on underlying disease or type of malabsorption
H2 breath tests, Celiac Abs, Abd imaging, EGD w/bx, Colon
w/bx, PFT, ERCP/MRCP/EUS, Angio, Fecal 1-AT, Fat pad
aspirate
Thanks …. Any question