Embed Size (px)
Citation preview

FETALFETAL MALPRESENTATIONMALPRESENTATION
andandMALPOSITIONMALPOSITION
Joni Jabez O. AreolaJoni Jabez O. AreolaUlysses E. Boglosa, Jr.Ulysses E. Boglosa, Jr.Jennifer P. SedilloJennifer P. Sedillo

Fetal Malpresentation
Fetal malpresentationFetal malpresentation refers to fetal presenting part other than vertex and includes breech, transverse, face, brow, and sinciput.
Malpresentations may be identified late in pregnancy or may not be discovered until the initial assessment during labor.

Related Factors
• The woman has had more than one pregnancy
• There is more than one fetus in the uterus
• The uterus has too much or too little amniotic fluid
• The uterus is not normal in shape or has abnormal growths, such as fibroids
• placenta previa
• The baby is preterm

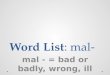
BREECHComplete (Flexed) Breech Presentation Footling Breech PresentationFrank (Extended) Breech PresentationKneeling Breech Presentation
VERTEXBrow Presentation Face PresentationSincipital Presentation
TRANSVERSE
Types of Malpresentation
The diagnosis of abnormal fetal presentations is commonly made with The diagnosis of abnormal fetal presentations is commonly made with a combination ofa combination of Leopold’s ManeuverLeopold’s Maneuver,, Vaginal examination Vaginal examination, , and and UltrasoundUltrasound

Types of Malpresentation
BREECHBREECH
Breech presentation means that either the buttocks or the feet are the first body parts that will contact the cervix.
Breech presentations occurs in approximately 3% of the births and are affected by fetal attitude.
Breech presentations can be difficult births, with the presenting point influencing the degree of difficulty.

Types of Breech Presentation
Frank breechFrank breech
The baby's bottom comes first, and the legs are flexed at the hip and extended at the knees (with feet near the ears).
65-70% of breech babies are in the frank breech position.
Complete BreechComplete Breech
The baby's hips and knees are flexed so that the baby is sitting crosslegged, with feet beside the bottom.

Types of Breech Presentation
Footling BreechFootling Breech
One or both feet come first, with the bottom at a higher position. This is rare at term but relatively common with premature fetuses.
Kneeling BreechKneeling Breech
The baby is in a kneeling position, with one or both legs extended at the hips and flexed at the knees. This is extremely rare.

Maternal Risks
Prolonged labor r/t decreased pressure exerted by the breech on the cervix.
PROM may expose client to infection.
Cesarean or forceps delivery.
Trauma to birth canal during delivery from manipulation and forceps to free the fetal head.
Intrapartum or postpartum hemorrhage.

Fetal Risks:
Compression or prolapse of umbilical cord.
Entrapment of fetal head in incompletely dilated cervix.
Aspiration and asphyxia at birth.
Birth trauma from manipulation and forceps to free the fetal head.

Management
If the woman is in early labor and the membranes are intact, attempt External Cephalic Version.
Tocolytics, such as Terbutaline 0.25 mg IM, can be used before ECV to help relax the uterus.
If ECV is successful, proceed with normal childbirth. If EVC fails or is not advisable, deliver by caesarean section.


Attempt external version if:Attempt external version if:
Breech presentation is present at or after 37 weeks (before 37 weeks, a successful version is more likely spontaneously revert back to breech presentation)
Vaginal delivery is possible
Membranes are intact and amniotic fluid is adequate;
There are no complications (e.g. fetal growth restriction, uterine bleeding, previous caesarean delivery, fetal abnormalities, twin pregnancy, HPN, fetal death).
Management

VAGINAL BREECH DELIVERYVAGINAL BREECH DELIVERY. A vaginal breech delivery by a skilled health care provider is safe and feasible under the following conditions:
- complete or frank breech- adequate clinical pelvimetry- fetus is not too large- no previous caesarean section for cephalopelvic disproportion- flexed head.
Management

CESAREAN SECTION for breech presentation. A cesarean section is safer than vaginal breech delivery and recommended in cases of:
Double footling breech
Small or malformed pelvis
Very large fetus
Previous cesarean section for cephalopelvic disproportion
Hyperextended or deflexed head.
Management


Types of Malpresentation
TRANSVERSEIn a transverse lie, a
fetus lies horizizontally in the pelvis so that the longest fetal axis is perpendicular to that of the mother.
The presenting part is usually one of the shoulders (acromion process), an iliac crest, a hand, or an elbow.

• If an infant is preterm and smaller than usual, an attempt to turn the fetus to a horizontal lie may be made.
• Most infants in transverse lie must be born by cesarean birth, however, because they cannot be turned and cannot be born normally form this “wedged” position.
Management

Types of Malpresentation
SINCIPUTSINCIPUT
The sinciput presentation occurs when the larger diameter of the fetal head is presented. Labor progress is slowed with slower descent of the fetal head.
FACEFACE
The face presentation is caused by hyper-extension of the fetal head so that neither the occiput nor the sinciput is palpable on vaginal examination.

Management
In the chin-anteriorchin-anterior position prolonged labor is common. Descent and delivery of the head by flexion may occur.
In the chin-posterior chin-posterior position, however, the fully extended head is blocked by the sacrum. This prevents descent and labor is arrested.

ManagementChin-Anterior PositionChin-Anterior Position
If the cervix is fully dilated: Allow to proceed with
normal childbirth; If there is slow progress
and no sign of obstruction, augment labor with oxytocin;
If descent is unsatisfactory, deliver by forceps.
If the cervix is not fully dilated and there are no signs of obstruction: augment labor with
oxytocin.
Chin-Posterior PositionChin-Posterior Position
If the cervix is fully dilated: Deliver by caesarean
section.
If the cervix is not fully dilated Monitor descent, rotation
and progress. If there are signs of obstruction, deliver by caesarean section.
*Do not perform vacuum Do not perform vacuum extraction for face extraction for face presentation.presentation.

Types of Malpresentation
BROWBROW
The brow presentation is caused by partial extension of the fetal head so that the occiput is higher than the sinciput.
MGTMGT: If the fetus is alive or dead, deliver by caesarean section.
*Do not deliver brow presentation by vacuum extraction, outlet forceps or symphysiotomy.

Nursing Care of Clients with Malpresentations
• Observe closely for abnormal labor patterns.• Monitor fetal heart beat and contractions
continuously.• Anticipate forceps-assisted birth.• Anticipate cesarean birth for incomplete breech or
shoulder presentation.• Be prepared for childbirth emergencies such as
cesarean section, forceps-assisted delivery, and neonatal-resuscitation.
• Position pt. in Trendelenburg or knee-chest position.• Manually raise the presenting part aseptically

Fetal Malpresentation Fetal Malpresentation PathophysiologyPathophysiology


Anxiety Provide client and family teaching,Be available to client for listening and talkingProvide client support and encouragement.Encourage client to acknowledge and express feelings.Encourage breathing exercises to relieve anxiety.
Fear Provide client and family teaching,Note for degree of incapacitation.Stay with the client or make arrangements to have someone else be there.Provide opportunity for questions and answer honestly.Explain procedures within level of client’s ability to understand and handle.

Risk for InjuryObserve closely for abnormal labor patterns.Monitor fetal heart beat and contractions continuouslyBe prepared for childbirth emergencies such as cesarean section, forceps-assisted delivery, and neonatal-resuscitation.Maintain sterility of equipments Anticipate forceps-assisted birth.Anticipate cesarean birth for incomplete breech or shoulder presentation.
Risk for infectionStress proper hand washing techniques of all caregivers.Maintain sterile technique.Cleanse incision site daily and prn.Change dressings as needed.Encourage early ambulation, deep breathing, coughing, and position change.

Fetal MalpositionFetal Malposition
Refers to positions other than an occipitoanterior occipitoanterior positionposition.
Malpositions include occipitoposterior occipitoposterior and occipitotransverseoccipitotransverse positions of fetal head in relation to maternal pelvis.
It is usually seen in multipara or those with lax abdominal wall. Fetal malpositions are assessed during labor.

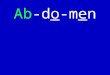
Left Occipitoanterior Left Occipitoanterior RotationRotation
• (A)(A) A fetus in cephalic presentation, LOA position. View is from outlet. The fetus rotates 90 degrees from this position. (B)(B) Descent and flexion (C)(C) Internal rotation complete. (D). (D) Extension; the face and chin are born

Types of Fetal Malposition
Occipitoposterior PositionOccipitoposterior Position
Arrested labor may occur when the head does not rotate and/or descend. Delivery may be complicated by perineal tears or extension of an episiotomy.
Occipitotransverse PositionOccipitotransverse Position
It is the incomplete rotation of OP to OA results in the fetal head being in a horizontal or transverse position (OT).

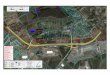
Left Occipitoposterior Left Occipitoposterior RotationRotation
• (A)(A) Fetus in cephalic presentation LOP position. View is from outlet. The fetus rotates 135 degrees from this position. (B)(B) Descent and flewion. (C)(C) In ternal rotation beginning. Because of the posterior position, the head will rotate in a longer arc than if it were in an anterior position. (D)(D) Internal rotation complete. (E) (E) Extension; the face and the chin are born. (F)(F) External rotation; the fetus rotates to place the shoulder in an anteroposterior position

Diagnosis:Diagnosis:Abdominal examinationAbdominal examination – the lower part of the abdomen is flattened, fetal limbs are palpable anteriorly and the fetal flank. Vaginal examinationVaginal examination – the posterior fontanelle is toward the sacrum and the anterior fontanelle may be easily felt if the head is deflexed
UltrasoundUltrasound
Maternal risks:Maternal risks: • prolonged labor• potential for operative
delivery• extension of
episiotomy, • 3rd or 4th degree
laceration of the perineum.
Maternal symptomsMaternal symptoms:: • Intense back pain in
labor• Dysfunctional labor
pattern• prolonged active phase • secondary arrest of
dilatation• arrest of descent

Nursing MGTEncourage the mother to lie on her side from the fetal back, which may help with rotation.Pelvic – rocking may Knee – chest position
help with rotation. may facilitate rotation.
Apply sacral counter – pressure with heel of hand to relieve back pain.Continue support and encouragement:Keep client and family informed progress.Praise client’s efforts to maintain control.

Management
• If there are signs of obstruction or the fetal If there are signs of obstruction or the fetal heart rate is abnormal at any stageheart rate is abnormal at any stage, deliver by caesarean section.
• If the membranes are intactIf the membranes are intact, rupture the membranes with an amniotic hook or a Kocher clamp.
• If the cervix is not fully dilated and there are If the cervix is not fully dilated and there are no signs of obstructionno signs of obstruction, augment labor with oxytocin.
• If the cervix is fully dilated but there is no If the cervix is fully dilated but there is no descent in the expulsive phasedescent in the expulsive phase, assess for signs of obstruction.

Management
If the cervix is fully dilated and if:
• the leading bony edge of the head is above -2 station, perform caesarean section;
• the leading bony edge of the head is between 0 station and -2 station, Delivery by Vacuum Extraction and Symphysiotomy
• If the operator is not proficient in symphysiotomy, perform caesarean section;
• If the bony edge of the fetal head is at 0 station, deliver by vacuum extraction or forceps.

Management
SYMPHYSIOTOMY A surgical procedure in
which the cartilage of the symphysis pubis is divided to widen the pelvis allowing childbirth when there is a mechanical problem. Currently the procedure is rarely performed in developed countries, but is still routine in developing countries where cesarean section is not always an option.

ManagementForceps - provides traction or
a means of rotating the fetal head.
Risks: fetal ecchymosis or edema of the face, transient facial paralysis, maternal lacerations, or episiotomy extensions.
Vacuum extraction - Provides traction to shorten the second stage of labor.
Risks: newborn cephalhematoma, retinal hemorrhage and intracranial hemorrhage.

Nursing Diagnoses:Impaired gas exchange
Encourage the mother to lie on her side from the fetal back, which may help with rotation.Knee – chest position may facilitate rotation.Pelvic – rocking may help with rotation.Monitor FHB appropriatelyBe prepared for childbirth emergencies such as cesarean section, forceps-assisted delivery, and neonatal-resuscitation.
Pain Encourage relaxation with contractions. Apply sacral counter – pressure with heel of hand to relieve back pain.Provide comfortable environment.Teach breathing exercises for use during early labor until client receives pharmacologic relief.Monitor physical response for example, palpitations/rapid pulse

Fatigue Assess psychological and physical factors that may affect reports of fatigue levelMonitor physical response for example, palpitations/rapid pulseMonitor fetal heart beat and contractions continuously.Refraining from intervening with client during contraction.
Anxiety Keep client and family informed progress.Provide support during labor through personal touch and contact. These methods convey concern.Continue support and encouragement.Make the client feel she is somewhat in control of her situation.Provide client and family teaching.Identify client’s perception of the threat presented by the situation.
Nursing Diagnoses:

Fetal Malposition Fetal Malposition PathophysiologyPathophysiology


QUIZ TIME!!!!!!!!!!!!