Embed Size (px)
Citation preview
Making the most out of the CBCMaking the most out of the CBC and peripheral blood smear
May 2011
John D’Orazio, M.D., Ph.D.Pediatric Hematology-Oncologygy gy
University of Kentucky College of [email protected]
objectivesobjectives
• Understand the clinical information that a complete blood
objectivesobjectives
• Understand the clinical information that a complete blood count (CBC) contains and how to get the most information out of it.
• Appreciate the importance of the peripheral blood smear in the interpretation of hematologic conditions.the interpretation of hematologic conditions.
• Reinforce concepts through cases via audience participation.
I have no relevant financial admissions or conflicts of
interest to disclose .
Complete Blood Count (CBC)“hemogram”
• One of the most commonly ordered testsy
• UK hospital runs about 700 hemograms a day
– 15,000‐20,000 a month
– 40% outpatient 60% inpatient
(Compared to ~1,000 chemistry panels per day)
p p
• Directed test for blood disorders
• Screening test for systemic diseases
Advia 2120 Hematology Analyzer
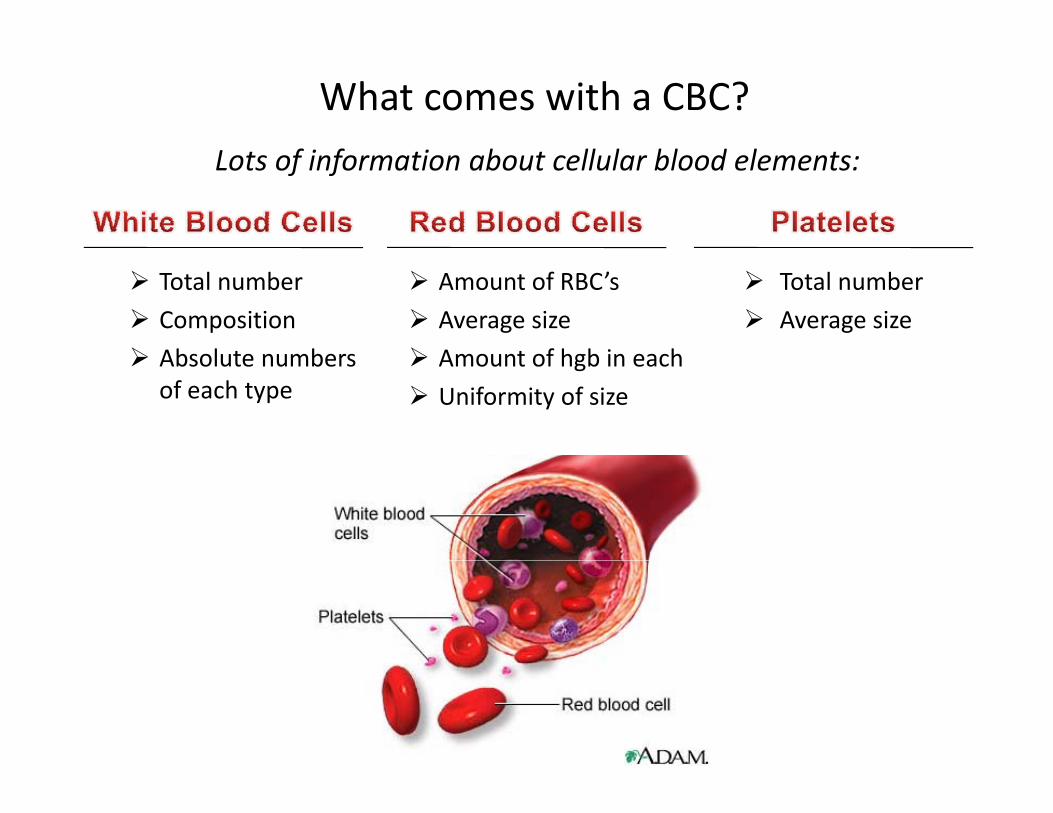
What comes with a CBC?L f i f i b ll l bl d lLots of information about cellular blood elements:
Total number
Composition
Absolute numbers
Total number
Average size
Amount of RBC’s
Average size
Amount of hgb in each Absolute numbers of each type
Amount of hgb in each
Uniformity of size
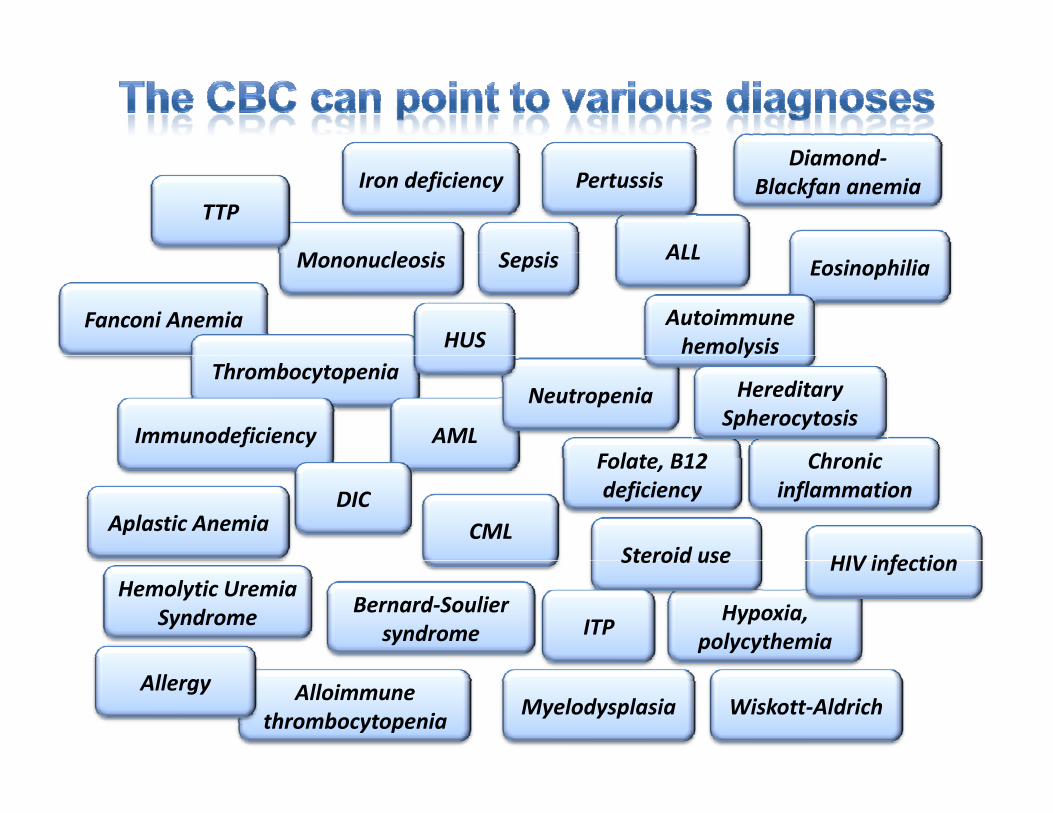
Di d
M l i
Diamond‐Blackfan anemia
TTPIron deficiency
S i ALL
Pertussis
Mononucleosis
Fanconi Anemia
Eosinophilia
Autoimmune hemolysis
Sepsis ALL
HUSThrombocytopenia
AMLFolate B12
Neutropenia
y
ImmunodeficiencyChronic
Hereditary Spherocytosis
CML
Folate, B12 deficiency
Steroid use HIV infection
Aplastic Anemia
Chronic inflammationDIC
Bernard‐Souliersyndrome
Hemolytic Uremia Syndrome Hypoxia,
polycythemia
Steroid use HIV infection
ITP
Alloimmunethrombocytopenia
Wiskott‐AldrichMyelodysplasiaAllergy
The CBC is one of the most commonly used i i di iscreening tests in medicine

Procedure• Blood is collected, usually venous
– capillary, arterial blood are o.k.
• Purple (lavender)‐topped tube
– Contains EDTA, an anticoagulant that works by chelating calcium
– Clotting is Ca‐dependent
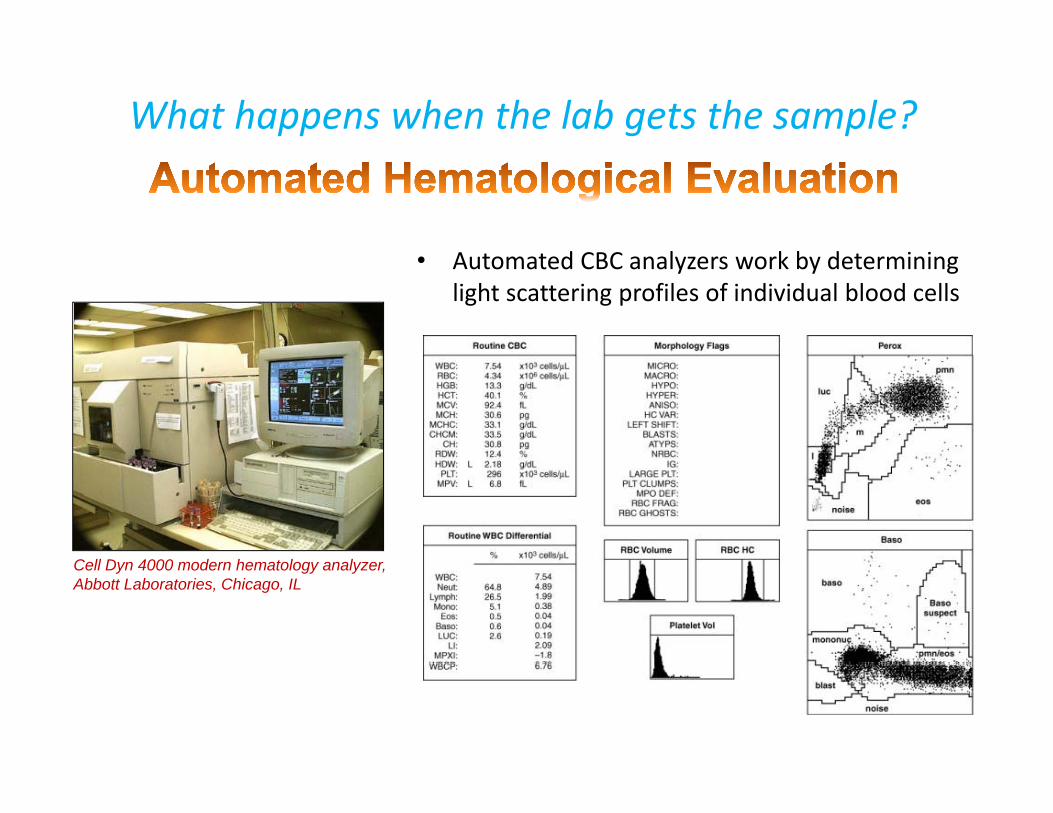
What happens when the lab gets the sample?
A d CBC l k b d i i• Automated CBC analyzers work by determining light scattering profiles of individual blood cells
C ll D 4000 d h t l lCell Dyn 4000 modern hematology analyzer, Abbott Laboratories, Chicago, IL

Hemoglobin (Hgb)g ( g )
• The oxygen‐carrying molecule in RBC’s
• Measured as grams per deciliter (g/dL) of whole blood.
d f l b• Tetramer comprised of 4 globin proteins and an iron‐containing heme moiety.
Hemoglobin Alpha globin Beta globin
Hgb A (adult) 2 22 2
Hgb A2 2 δ2
H b F (f t l)Hgb F (fetal) 2 γ2

Almost all analyzers calculate hemoglobin by thehemoglobin by the
cyanomethemoglobin method.
Drabkin’s reagentDrabkin’s reagent
Hgb Cyanmet‐Hgb
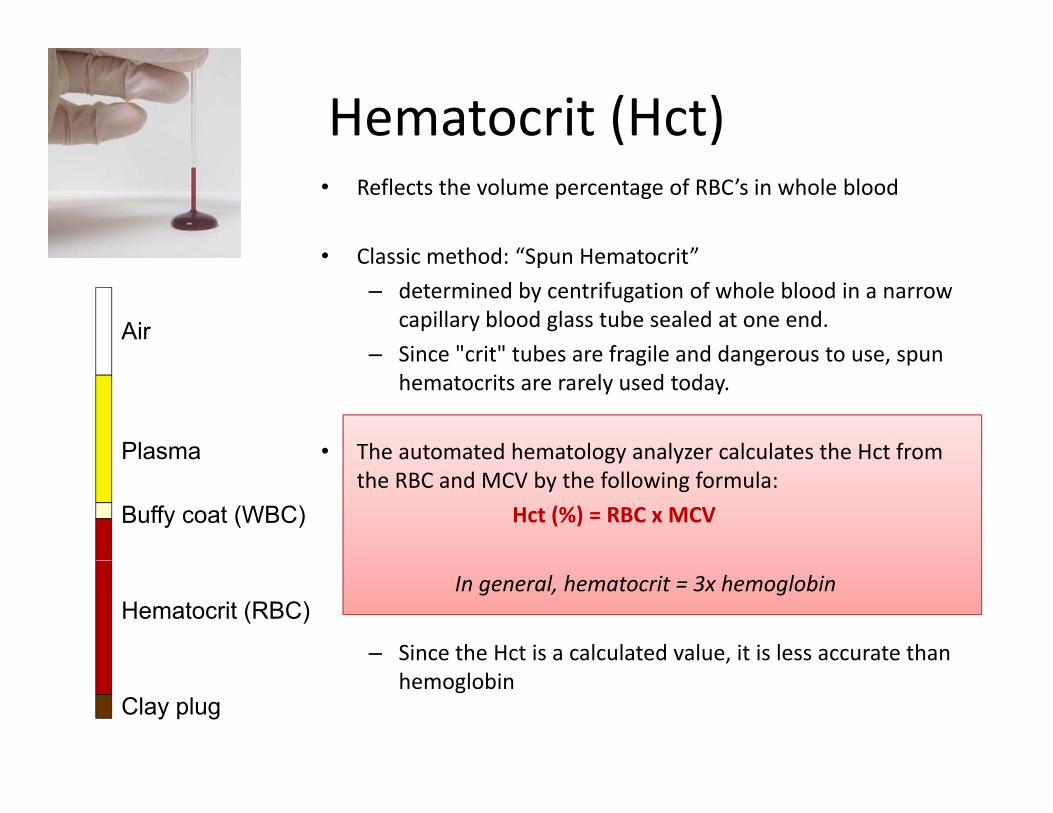
Hematocrit (Hct)• Reflects the volume percentage of RBC’s in whole blood
• Classic method “Spun Hematocrit”• Classic method: “Spun Hematocrit”
– determined by centrifugation of whole blood in a narrow capillary blood glass tube sealed at one end.
– Since "crit" tubes are fragile and dangerous to use spunAir
– Since crit tubes are fragile and dangerous to use, spun hematocrits are rarely used today.
• The automated hematology analyzer calculates the Hct fromPlasma The automated hematology analyzer calculates the Hct from the RBC and MCV by the following formula:
Hct (%) = RBC x MCV
Plasma
Buffy coat (WBC)
In general, hematocrit = 3x hemoglobin
– Since the Hct is a calculated value, it is less accurate than
Hematocrit (RBC)
,hemoglobin
Clay plug
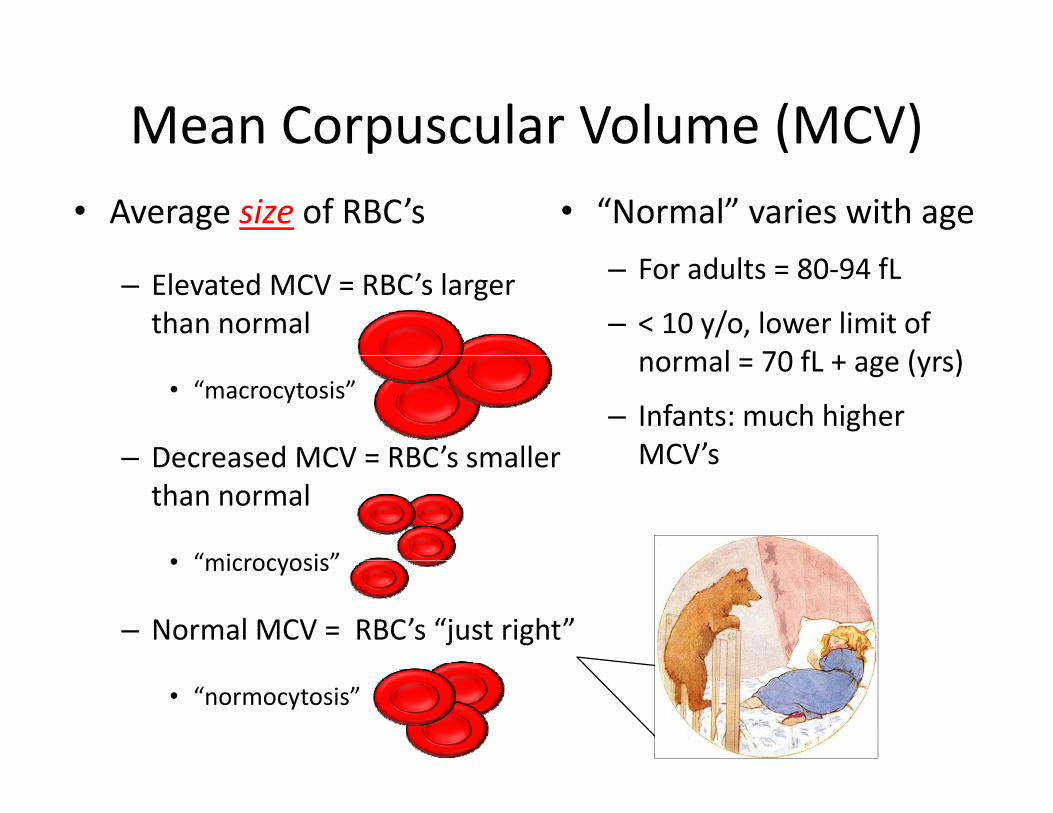
Mean Corpuscular Volume (MCV)p ( )• Average size of RBC’s • “Normal” varies with age
– Elevated MCV = RBC’s larger than normal
– For adults = 80‐94 fL
– < 10 y/o, lower limit of l 70 fL + ( )
• “macrocytosis”
– Decreased MCV = RBC’s smaller
normal = 70 fL + age (yrs)
– Infants: much higher MCV’s– Decreased MCV = RBC s smaller
than normal
• “microcyosis”
MCV s
• microcyosis
– Normal MCV = RBC’s “just right”
• “normocytosis”
Key yConcept
To make a proper RBC, there must be coordination p p ,between proliferation of RBC precursor cells and hemoglobinization of maturing RBC’s
Hematopoeitic Mature
- - - cell division - - - differentiation - - -
HematopoeiticStem cell
Matureerythrocytes

Cell division occurs relatively normally but Hgb production is defective. The cytoplasm can’t “fill up” properly with hemoglobin before the cells divide, so daughter cells are small.
Hgb production is fine but there is a problem with DNA synthesis. RBC precursors divide slowly, allowing more time to accumulate Hgb which makes the cells large.
Problems withProblem with DNA
Problems with HemoglobinProduction
Synthesis
Iron
B12 deficiencyMarrow failure
Iron Deficiency
↓ Globin(thalassemia) Folate
deficiencyHydroxyurea yHydroxyurea,Chemo
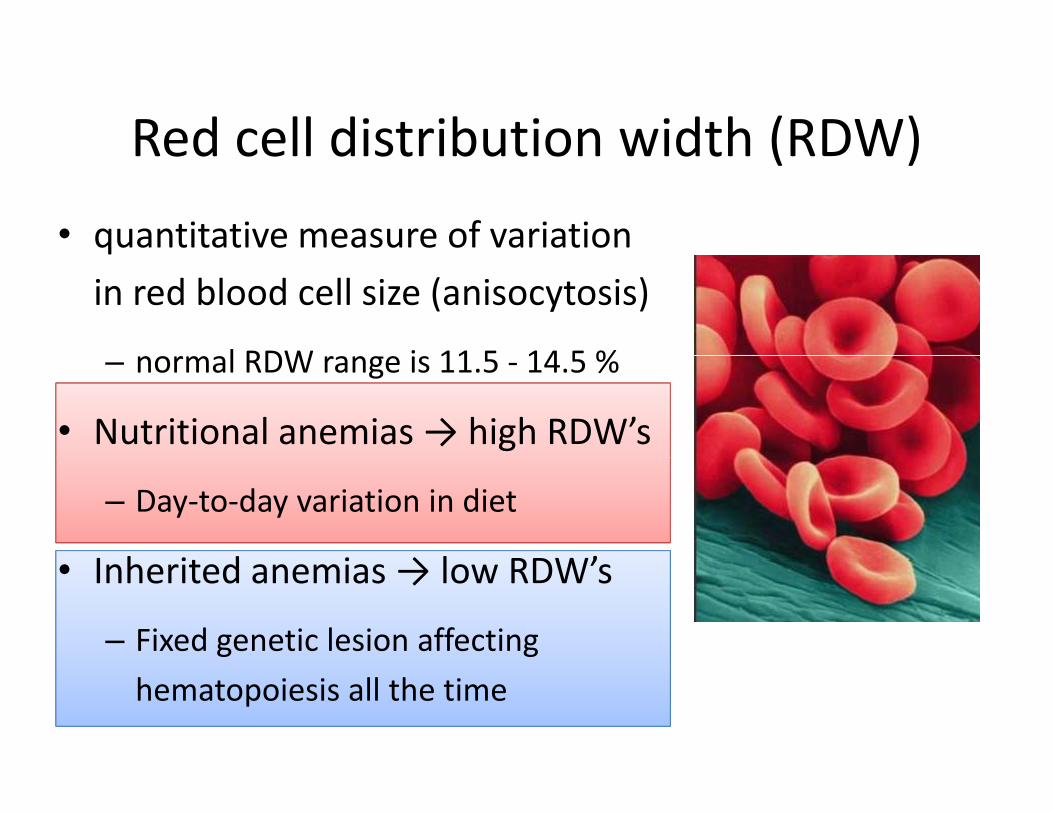
Red cell distribution width (RDW)Red cell distribution width (RDW)
• quantitative measure of variation q
in red blood cell size (anisocytosis)
l RDW i 11 5 14 5 %– normal RDW range is 11.5 ‐ 14.5 %
• Nutritional anemias → high RDW’s
– Day‐to‐day variation in diet
I h it d i → l RDW’• Inherited anemias → low RDW’s
– Fixed genetic lesion affecting
hematopoiesis all the time

MCV and RDWNormal NormalMicrocytosis Microcytosis
(cel
ls)
(cel
ls)
o aMicrocytosisLow RDW
(Thalassemia)
MicrocytosisHigh RDW
(Fe deficiency)
Even
ts
Even
ts
RBC Size RBC Size
ells
)
Normal
ells
)
Normocytosis Macrocytosis(Folate or B12)
Normal
Even
ts (c
e
Even
ts (c
e
RBC Size RBC Size

“Mentzer Index”Mentzer IndexWilliam Mentzer, M.D.Pediatric Hematology/OncologyProfessor Emeritus, UCSF
• helps differentiate whether microcytic anemia is caused from iron deficiency or from thalassemia
Professor Emeritus, UCSF
caused from iron deficiency or from thalassemia.
Mentzer Index = MCV RBC countMentzer Index MCV RBC count
< 11 > 13
Mentzer WC, 1973, "Differentiation of iron deficiency from thalassaemia trait". Lancet 1 (7808): 882.
thalassemia Fe deficiency

production destruction
Circulating red cell mass represents a balance between cellular production and destruction
To determine whether there is impaired RBC production or
cellular production and destruction.
premature RBC destruction… always order a reticulocyte count in your anemia work‐up!
Low retic count = RBC production problem
High retic count = RBC destruction
The reticulocyte count is not part of the CBC.

• Supravital staining that identifies ribosomesin the cytoplasm of RBC’sin the cytoplasm of RBC s
• Ribosomes persist in RBC’s for 24‐48h after leaving the marrowg
– ongoing Hgb synthesis
• Reticulocytes are young red blood cells onlyReticulocytes are young red blood cells only 1‐2 days removed from the marrow.
• Why is the retic count normally ~1%?y y
– Normal RBC life‐span ~ 120d
– Each day the body must replace 1 ÷ 120 = ~1%Each day the body must replace 1 120 1% of the red cell mass
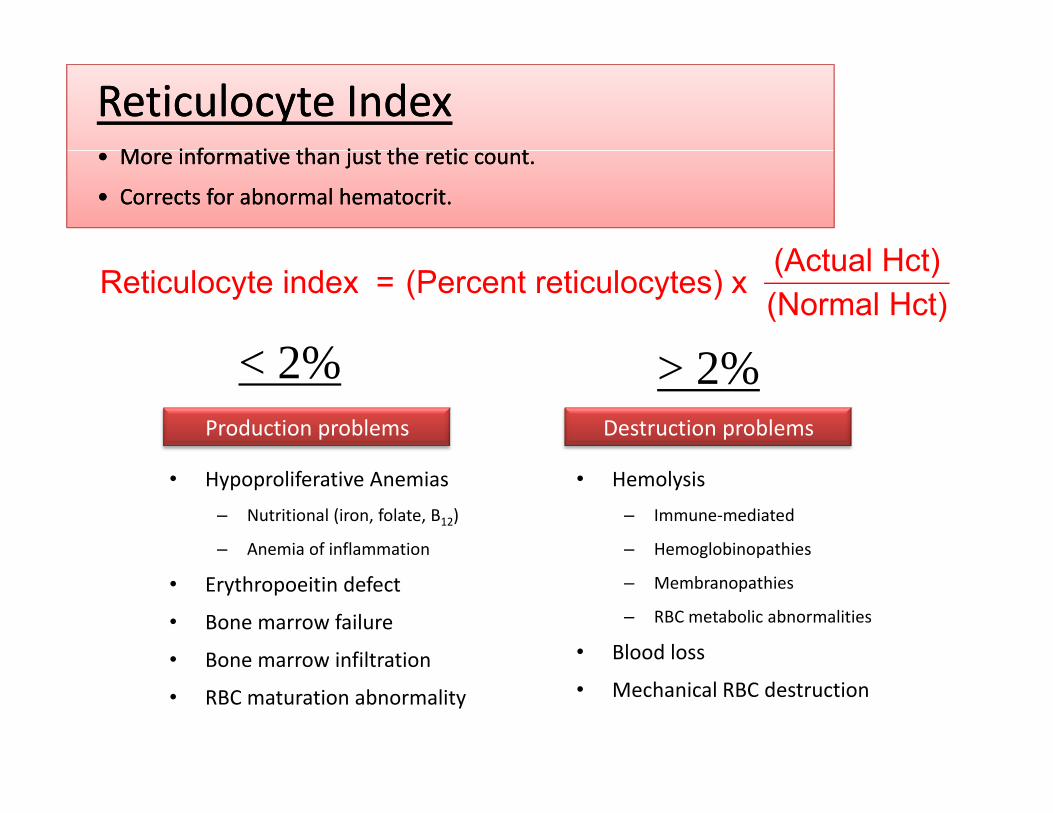
Reticulocyte IndexReticulocyte IndexM i f ti th j t th ti tM i f ti th j t th ti t• More informative than just the retic count.
• Corrects for abnormal hematocrit.
• More informative than just the retic count.
• Corrects for abnormal hematocrit.
(A t l H t)
< 2% 2%
=Reticulocyte index (Percent reticulocytes) x(Actual Hct)(Normal Hct)
< 2% > 2%Production problems Destruction problems
• Hypoproliferative Anemias
– Nutritional (iron, folate, B12)
– Anemia of inflammation
• Hemolysis
– Immune‐mediated
– Hemoglobinopathies
• Erythropoeitin defect
• Bone marrow failure
• Bone marrow infiltration
– Membranopathies
– RBC metabolic abnormalities
• Blood lossBone marrow infiltration
• RBC maturation abnormality • Mechanical RBC destruction

Clues to reticulocytosis on a CBC
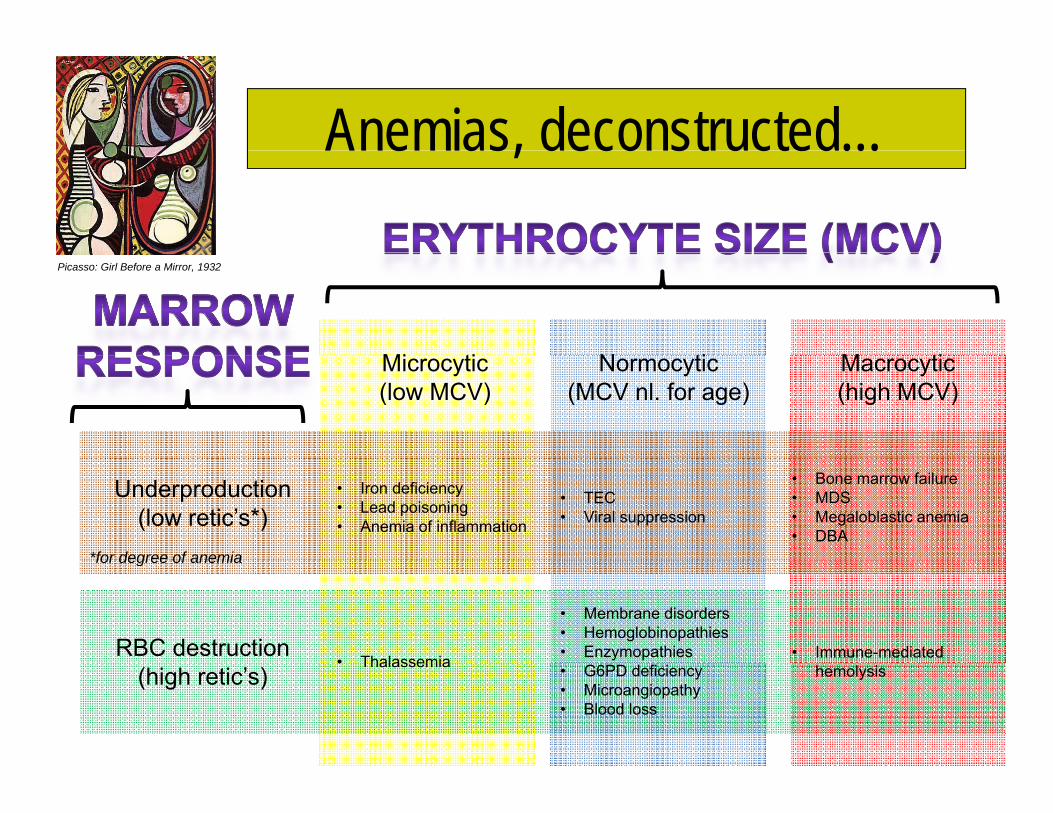
Anemias, deconstructed…Anemias, deconstructed…
Mi ti N ti M ti
Picasso: Girl Before a Mirror, 1932
Microcytic(low MCV)
Normocytic(MCV nl. for age)
Macrocytic(high MCV)
Underproduction(low retic’s*)
*for degree of anemia
• Iron deficiency• Lead poisoning• Anemia of inflammation
• TEC• Viral suppression
• Bone marrow failure• MDS• Megaloblastic anemia• DBA
for degree of anemia
RBC destruction• Thalassemia
• Membrane disorders• Hemoglobinopathies• Enzymopathies • Immune-mediated
(high retic’s)• Thalassemia • G6PD deficiency
• Microangiopathy• Blood loss
hemolysis


Automated WBC Differential
• Histogram analysis of WBC’s
• each "dot" represents data from a single cell.
• Each type of WBC displays a ll si
ze) monocytes
neutrophils
y ycharacteristic size and granularity
• In this case:
• 65 6% Neutrophilsscat
ter (
ce
• 65.6% Neutrophils
• 26.2% Lymphocytes
• 5.6% Monocytes Forw
ard
s eosinophilsbasophils
lymphocytes y
• 2.2% Eosinophils
• 0.4% Basophils Side scatter (cellular complexity)
lymphocytes
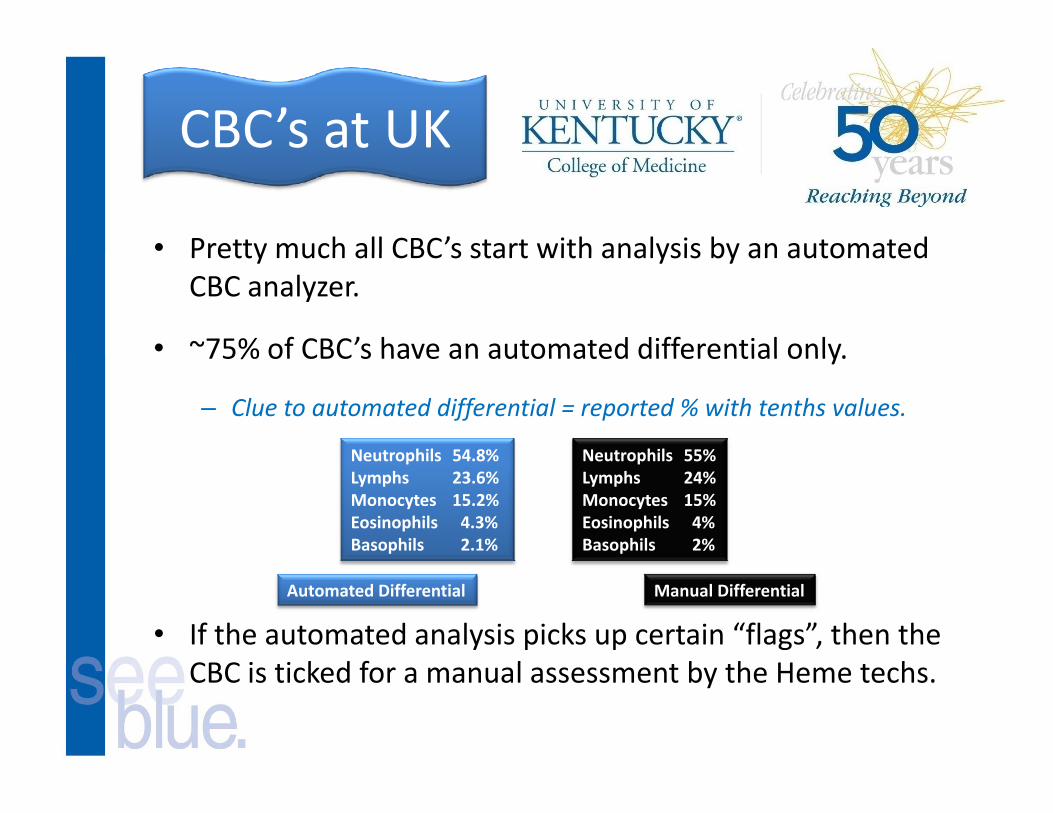
CBC’s at UK
• Pretty much all CBC’s start with analysis by an automatedPretty much all CBC s start with analysis by an automated CBC analyzer.
• ~75% of CBC’s have an automated differential only.75% of CBC s have an automated differential only.
– Clue to automated differential = reported % with tenths values.
Neutrophils 54 8% Neutrophils 55%Neutrophils 54.8%Lymphs 23.6%Monocytes 15.2%Eosinophils 4.3%Basophils 2.1%
Neutrophils 55%Lymphs 24%Monocytes 15%Eosinophils 4%Basophils 2%
• If the automated analysis picks up certain “flags”, then the CBC i i k d f l b h H h
Automated Differential Manual Differential
CBC is ticked for a manual assessment by the Heme techs.
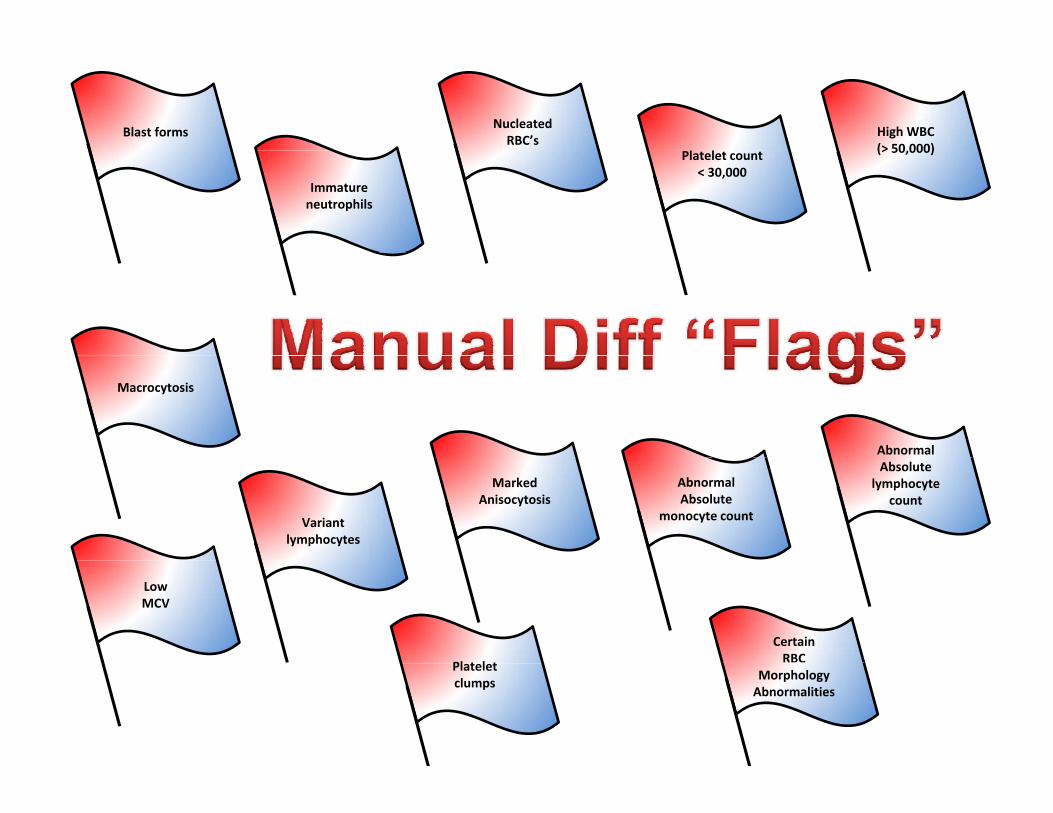
Nucleated RBC’s
Blast forms High WBC(> 50 000)Platelet count
< 30,000Immature neutrophils
(> 50,000)
Abnormal
Macrocytosis
Abnormal Absolute
monocyte count
Absolute lymphocyte
count
Variant lymphocytes
MarkedAnisocytosis
Certain RBC Pl t l t
LowMCV
Morphology Abnormalities
Platelet clumps
Bottom lineBottom line…
• Today’s automated hematology analyzers are very good for most routine applications, but they’re not perfect.
A d CBC’ ’ li bl d ib h l h l f• Automated CBC’s can’t reliably describe the actual morphology of WBC’s or RBC’s
– Machines can “flag” certain RBC or WBC abnormalities (e.g. 2+ anisocytosis)g ( g y )
• If the diagnosis that you are considering correlates with a specific WBC or RBC morphology, then order a manual slide review.
– Leukemia (blasts)
– RBC membrane disorder (spherocytes)
Lik i if th CBC d ’t “fit” ith th li i l i t th• Likewise, if the CBC doesn’t “fit” with the clinical picture, then more information might be obtained by examining a peripheral blood smear.
CBC’s and Manual Diff’s• Only when a manual differential is performed will anyone from
the lab physically look at the peripheral blood smear.p y y p p
• Remains the “gold standard” for blood interpretation
• Clinical Lab’s Heme techs are excellent and reliable• Clinical Lab s Heme techs are excellent and reliable
• Exceptional smears are also reviewed by hematopathologists
• The practitioner has the option of requesting a manual differential right from the start (on the general lab order form)the start (on the general lab order form).
• For now, but the lab may evaluate this policy (labor‐intensive)
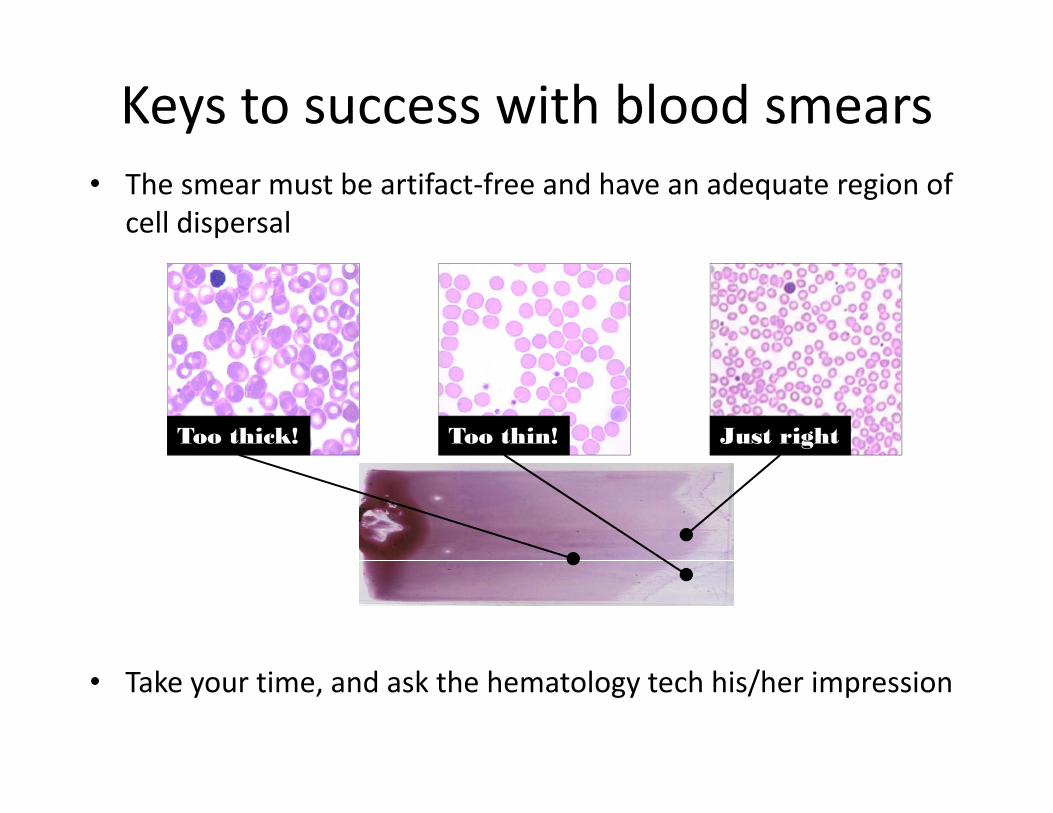
Keys to success with blood smears• The smear must be artifact‐free and have an adequate region of
cell dispersal
Too thick! Too thin! Just right
• Take your time, and ask the hematology tech his/her impression
Warm-up slides
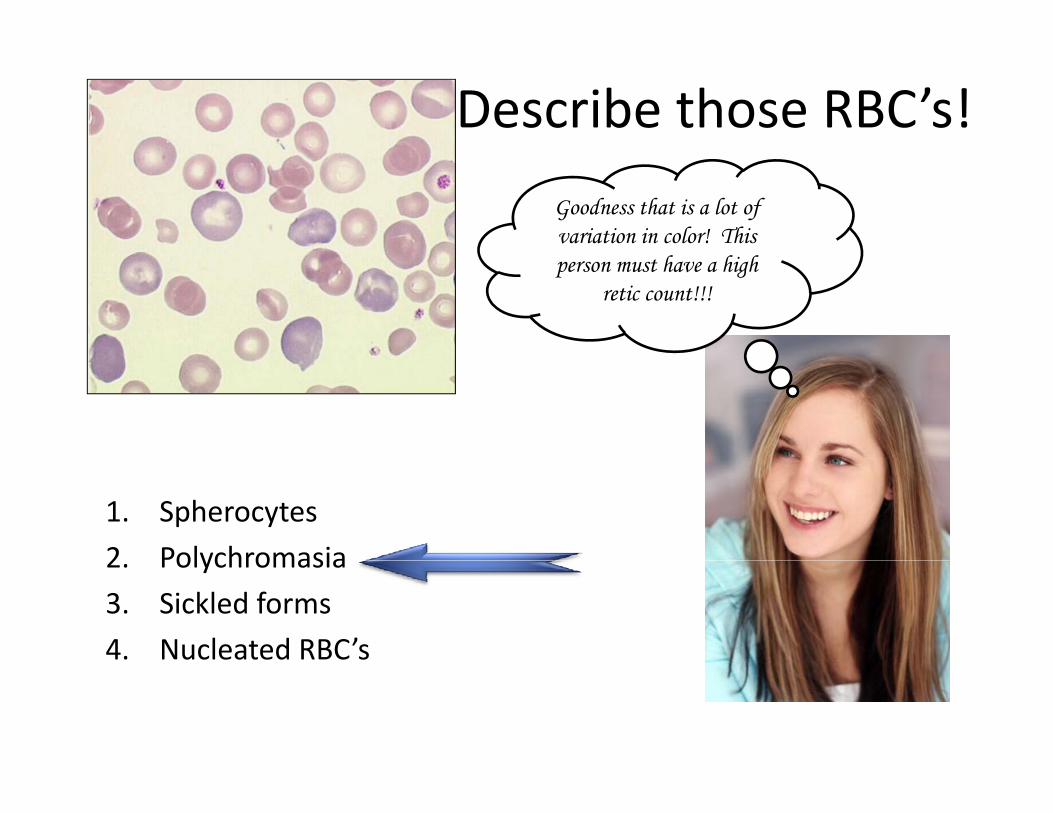
Describe those RBC’s!
Goodness that is a lot of variation in color! This person must have a high
retic count!!!
1. Spherocytes
2 Polychromasia2. Polychromasia
3. Sickled forms
4. Nucleated RBC’s

Describe those RBC’s!Describe those RBC s!
Just look at all that variation in
red cell size!
1. Poikilocytosis
2 Polychromasia2. Polychromasia
3. Anisocytosis
4. Target Formsg
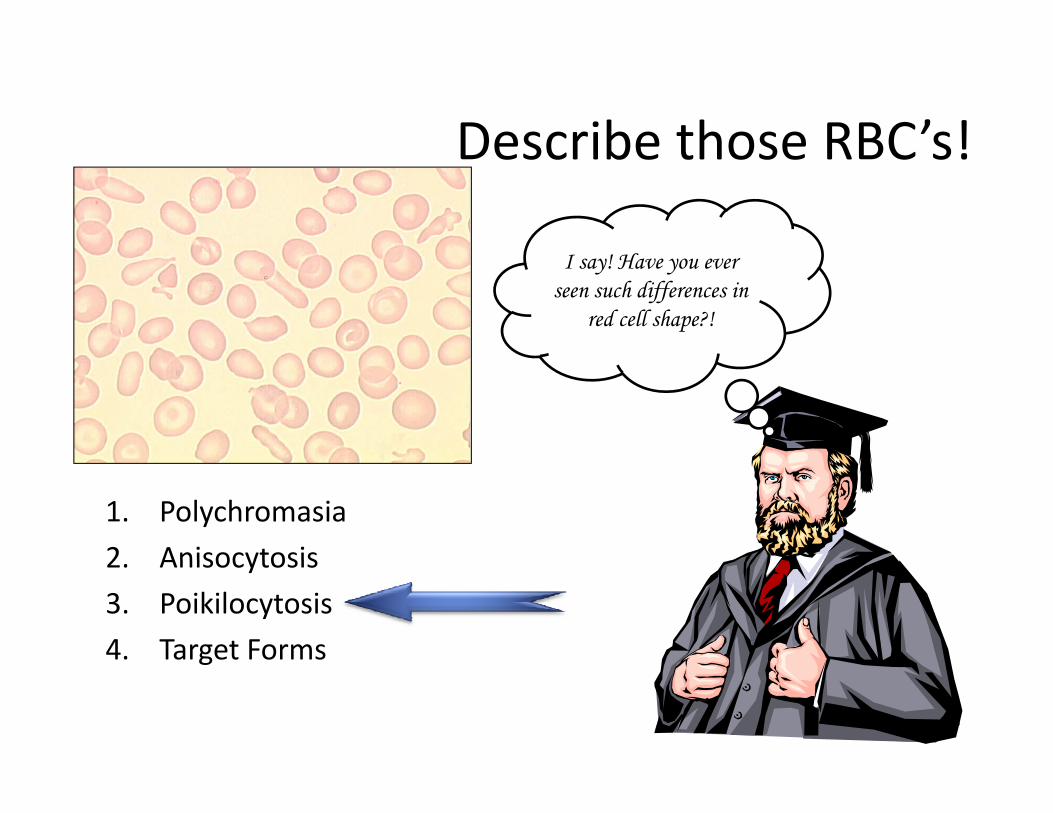
Describe those RBC’s!Describe those RBC s!
I say! Have you ever seen such differences in
red cell shape?!
1. Polychromasia
2 Anisocytosis2. Anisocytosis
3. Poikilocytosis
4. Target Formsg
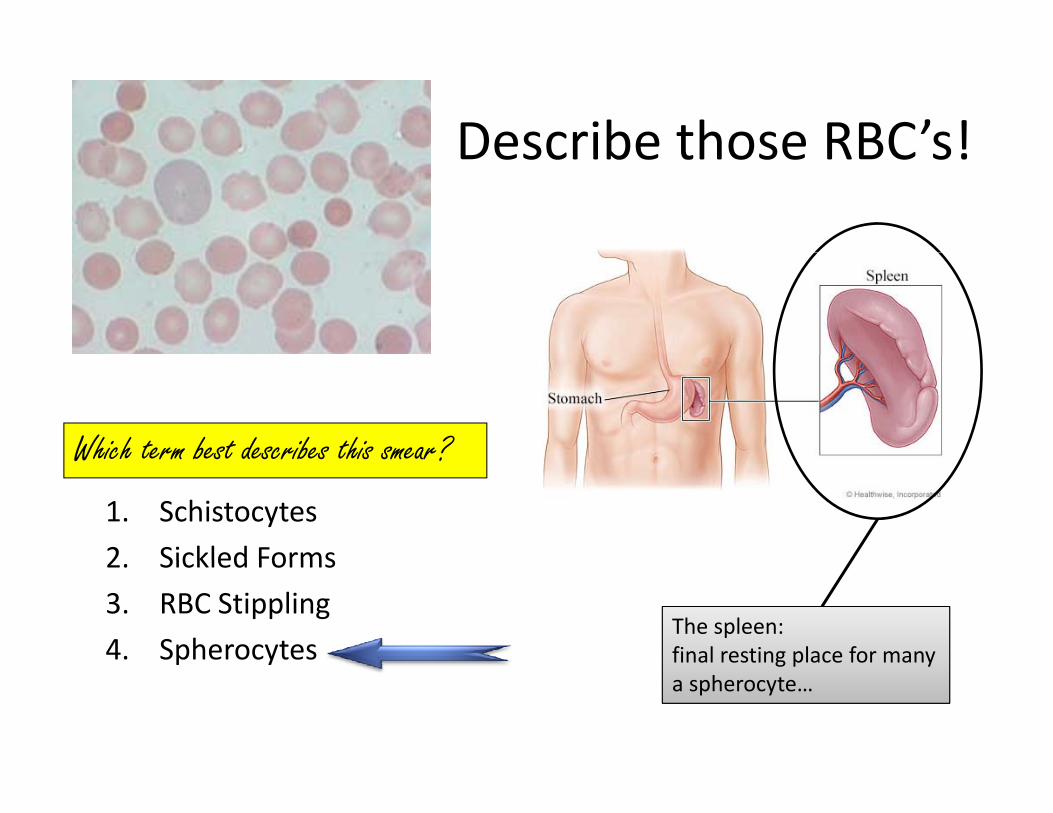
Describe those RBC’s!Describe those RBC s!
Which term best describes this smear?Which term best describes this smear?
1. Schistocytes
2 Sickled Forms2. Sickled Forms
3. RBC Stippling
4. SpherocytesThe spleen: final resting place for many p y g p ya spherocyte…
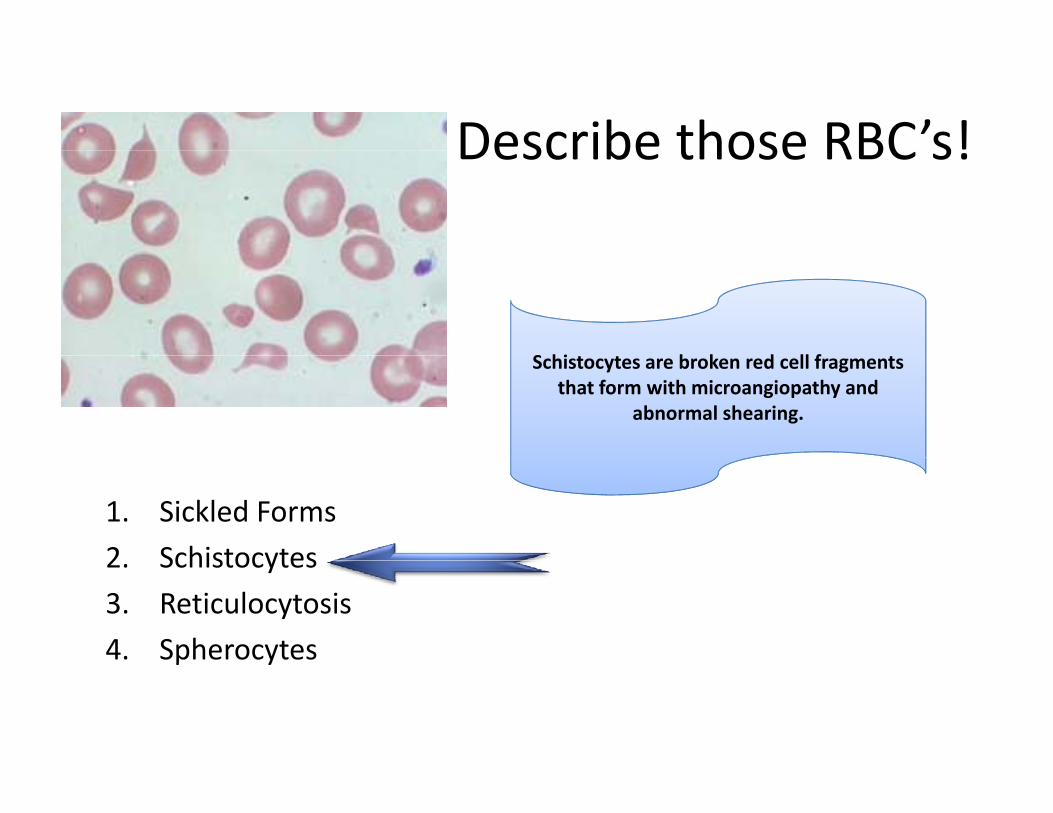
Describe those RBC’s!Describe those RBC s!
S hi b k d ll fSchistocytes are broken red cell fragments that form with microangiopathy and
abnormal shearing.
1. Sickled Forms
2 Schistocytes2. Schistocytes
3. Reticulocytosis
4. Spherocytesp y
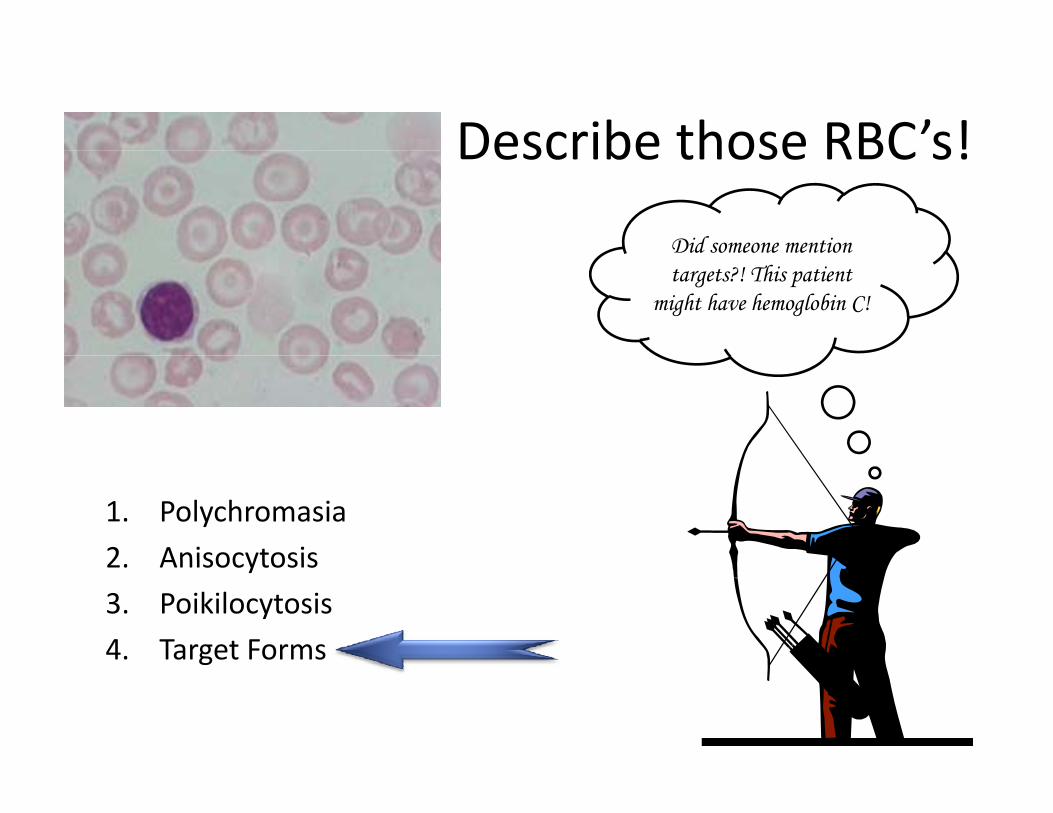
Describe those RBC’s!Describe those RBC s!
Did someone mention targets?! This patient
might have hemoglobin C!
1. Polychromasia
2 Anisocytosis2. Anisocytosis
3. Poikilocytosis
4. Target Formsg
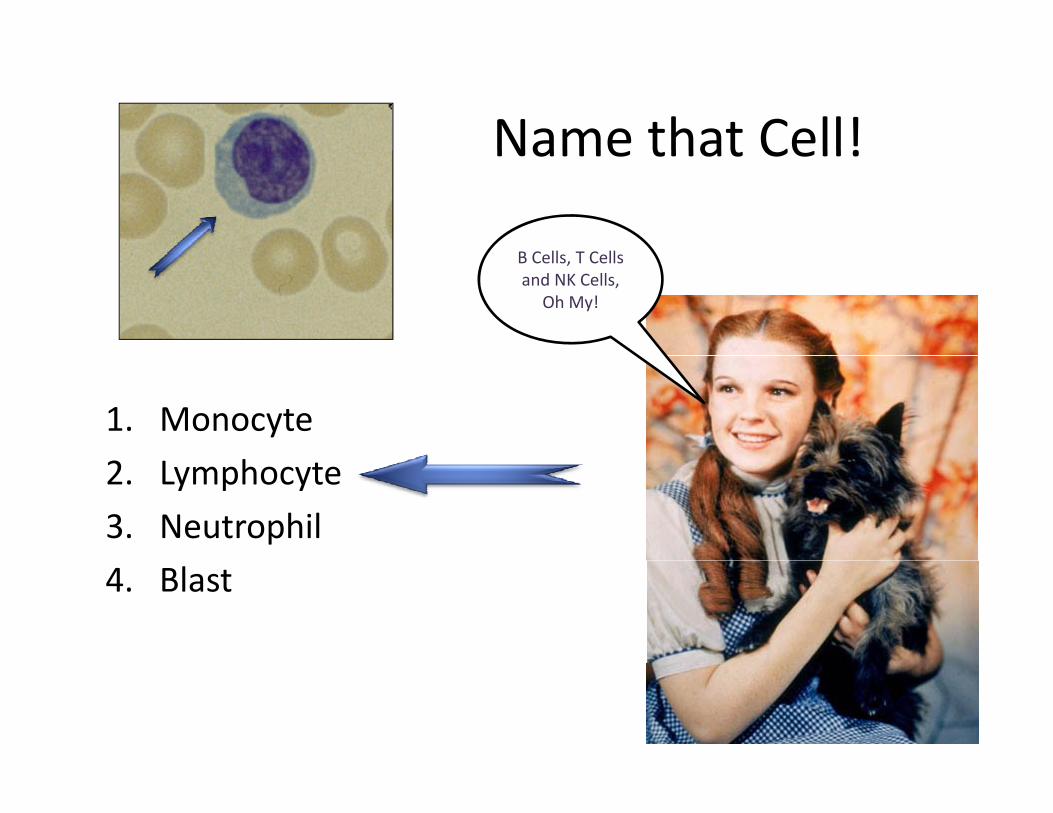
Name that Cell!Name that Cell!
B C ll T C llB Cells, T Cells and NK Cells,
Oh My!
1. Monocyte
2. Lymphocyte
3. Neutrophil
4. Blast
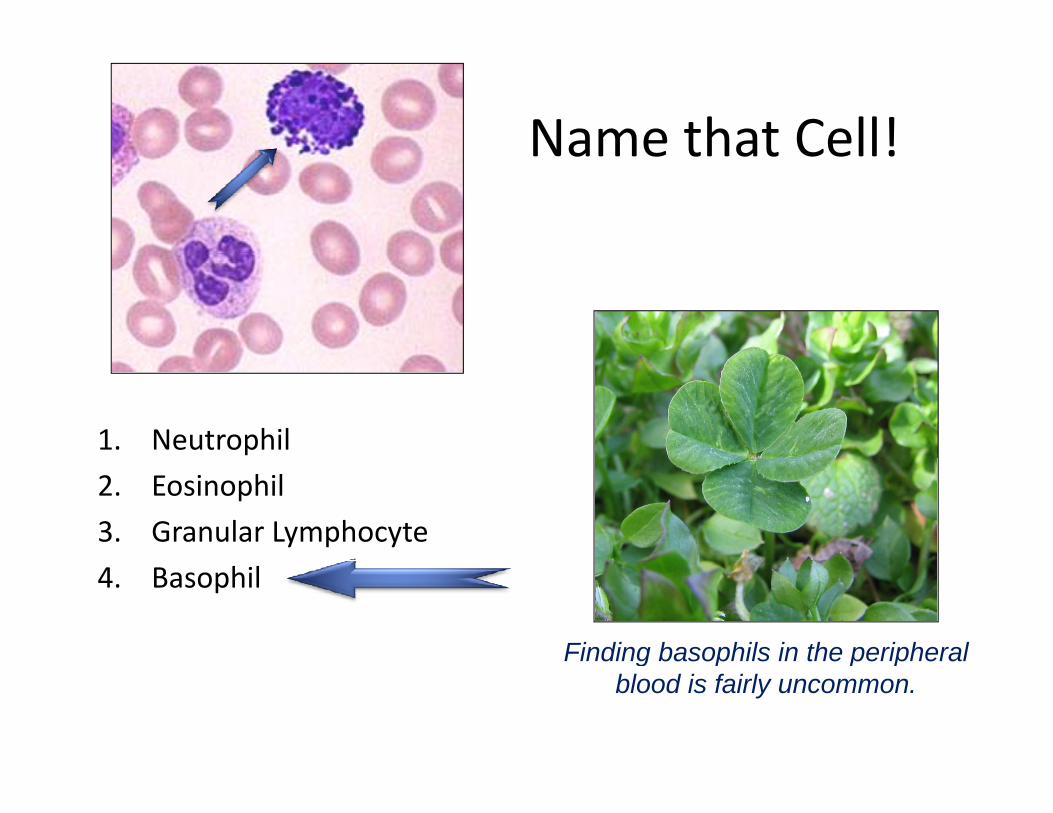
Name that Cell!Name that Cell!
1. Neutrophil
2. Eosinophil
3. Granular Lymphocyte
4. Basophil
Finding basophils in the peripheral g p p pblood is fairly uncommon.
Name that Cell!Name that Cell!
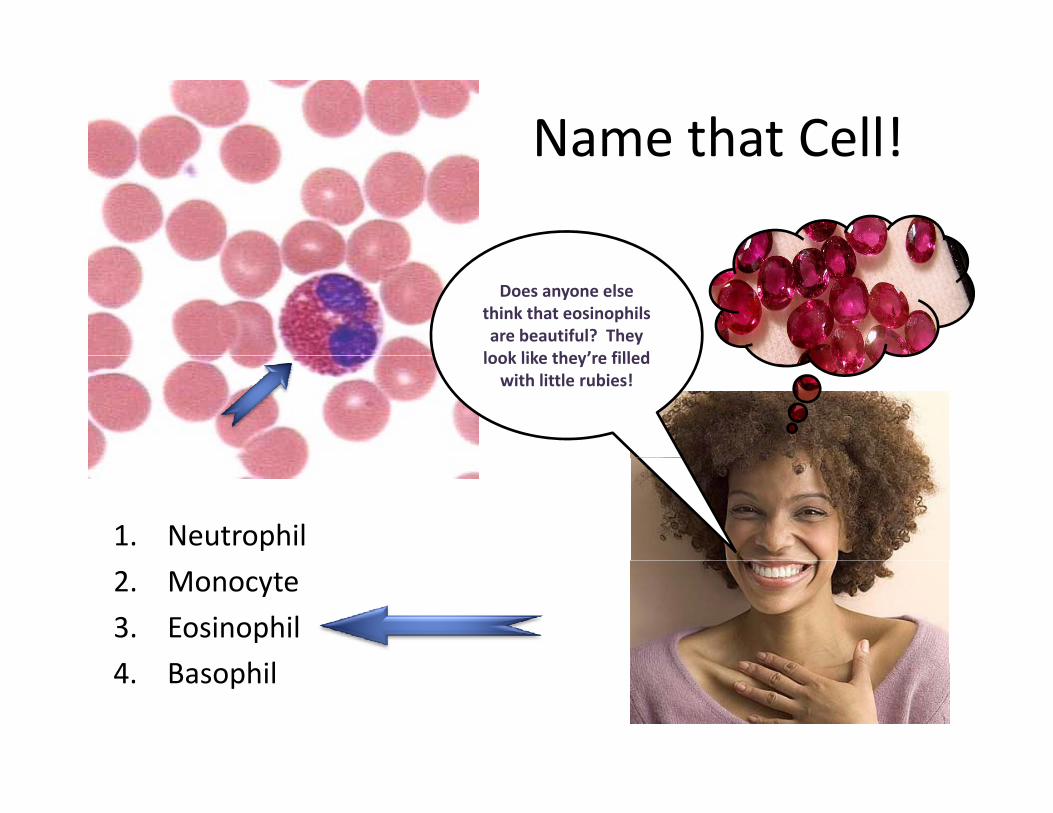
Does anyone else think that eosinophilsare beautiful? They look like they’re filledlook like they’re filled with little rubies!
1. Neutrophil
2. Monocyte
3. Eosinophil
4 hil4. Basophil
Name that Cell!Name that Cell!
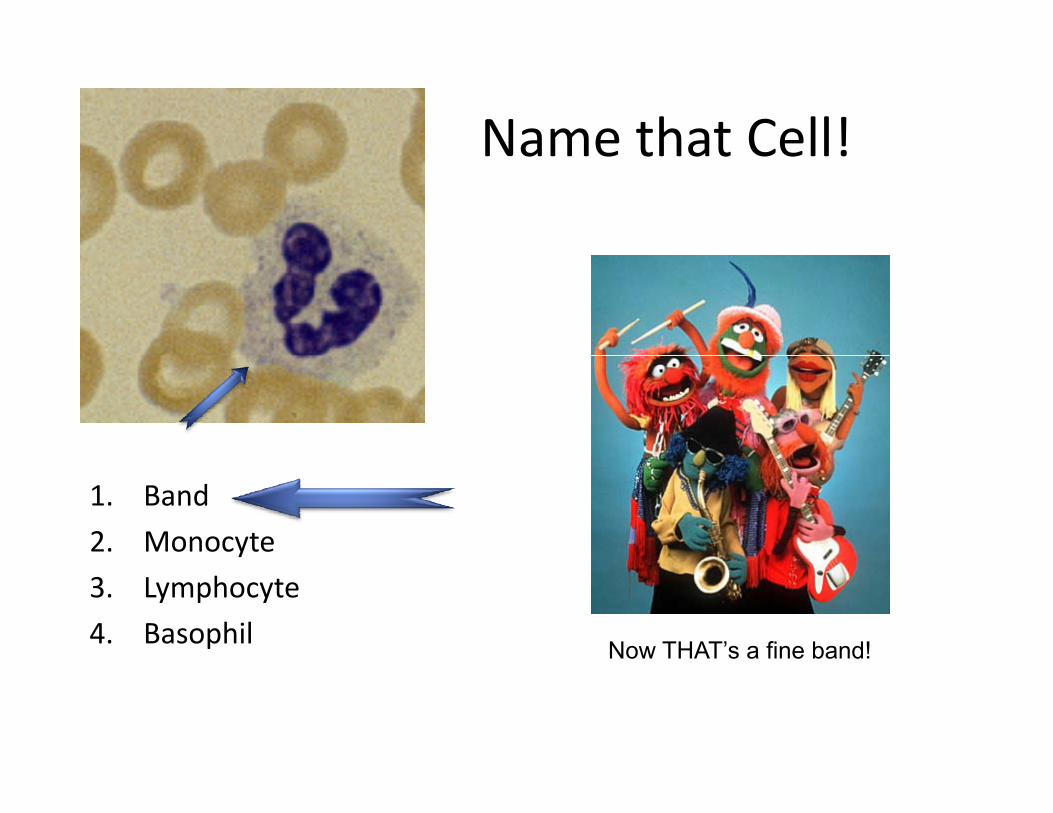
1. Band
2. Monocyte
3. Lymphocyte
4. Basophil Now THAT’s a fine band!
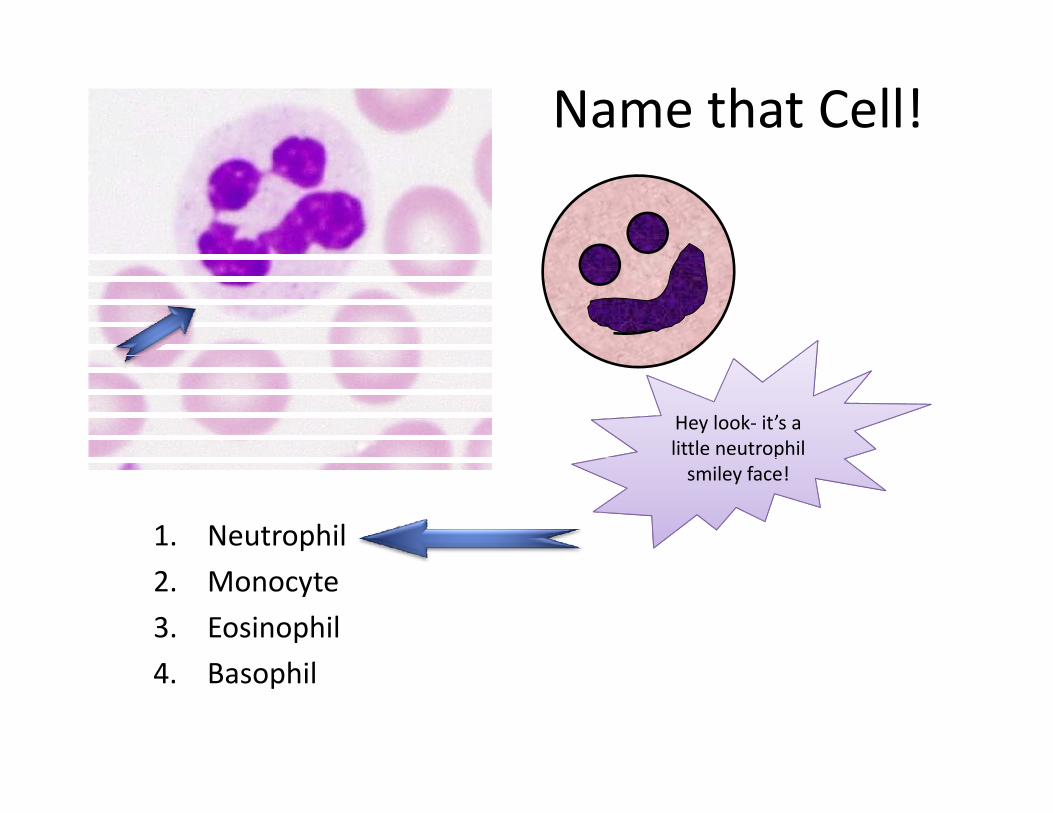
Name that Cell!
Hey look‐ it’s a little neutrophil
1. Neutrophil
psmiley face!
2. Monocyte
3. Eosinophil
4 hil4. Basophil

Name that Cell!Name that Cell!
Prepare to be phagocytized!
1. Neutrophil
2. Monocyte
3. Lymphocyte
4. Basophil
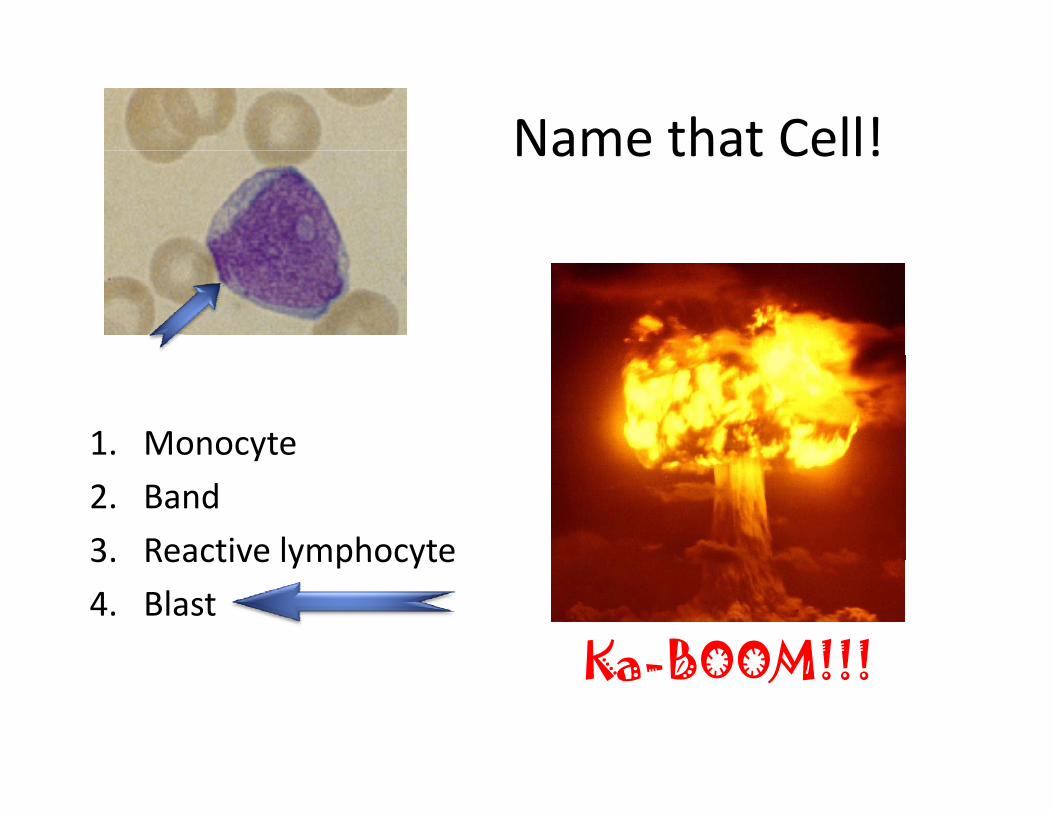
Name that Cell!Name that Cell!
1. Monocytey
2. Band
3. Reactive lymphocyte3. Reactive lymphocyte
4. Blast
Ka BOOM!!!Ka-BOOM!!!

Cases
CBC and peripheral blood smear can clinch the
diagnosis.diagnosis.

d l k ’ fHands on clickers… it’s time for audience participation fun!p p
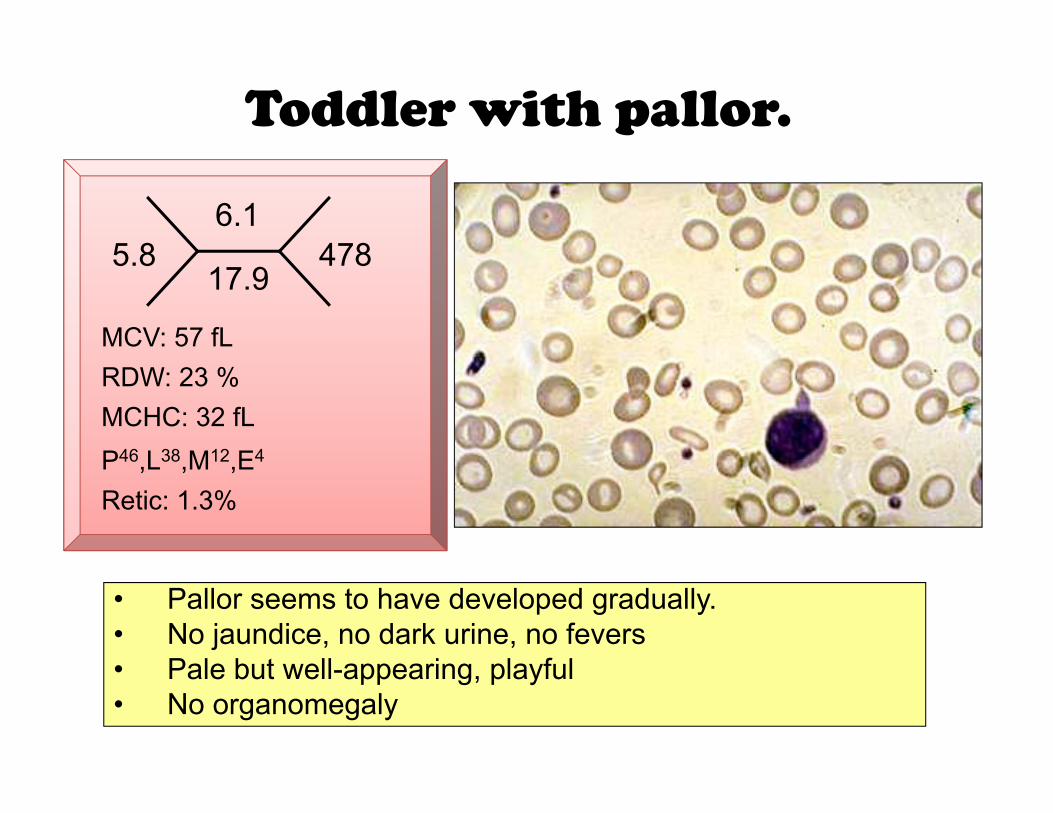
Toddler with pallor.
5 86.1
4785.817.9
478
MCV: 57 fL
P46 L38 M12 E4
RDW: 23 %MCHC: 32 fLP46,L38,M12,E4
Retic: 1.3%
• Pallor seems to have developed gradually.• No jaundice, no dark urine, no fevers
P l b t ll i l f l• Pale but well-appearing, playful• No organomegaly
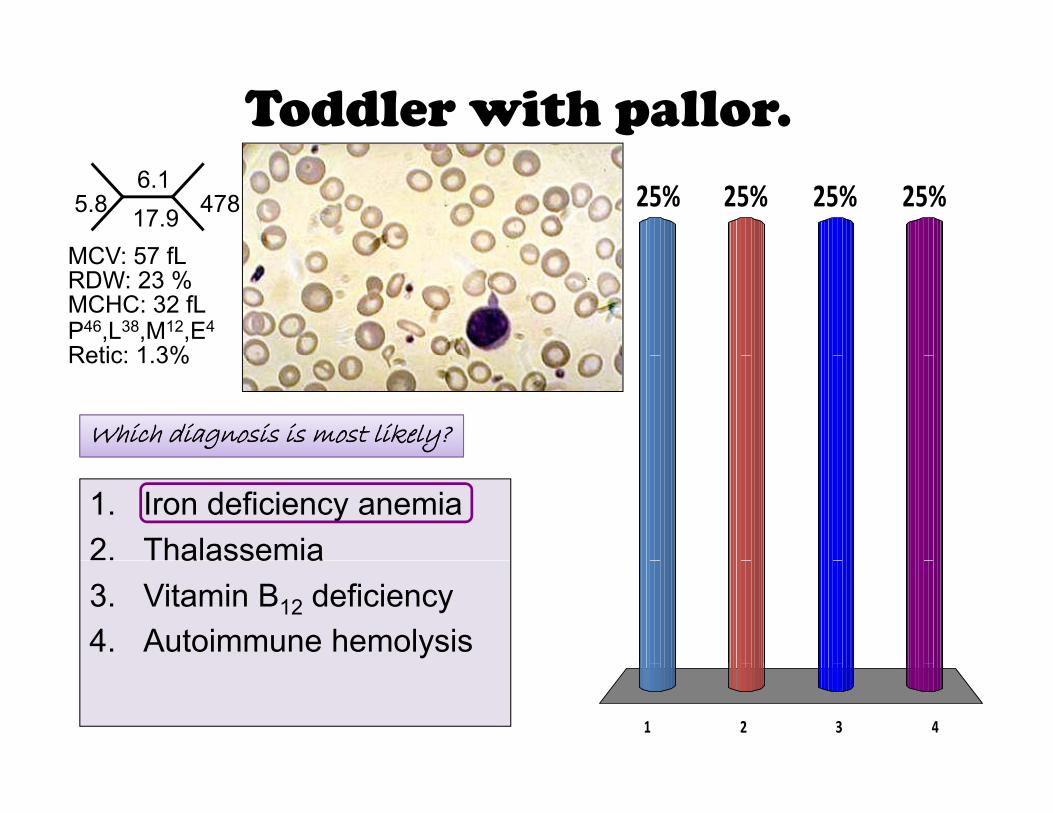
Toddler with pallor.
5.86.117.9 478
MCV: 57 fL
25% 25%25%25%
P46,L38,M12,E4
MCV: 57 fL
Retic: 1 3%
RDW: 23 %MCHC: 32 fL
Retic: 1.3%
Which diagnosis is most likely?
1. Iron deficiency anemia2. Thalassemiaa asse a3. Vitamin B12 deficiency4. Autoimmune hemolysis
1 2 3 4

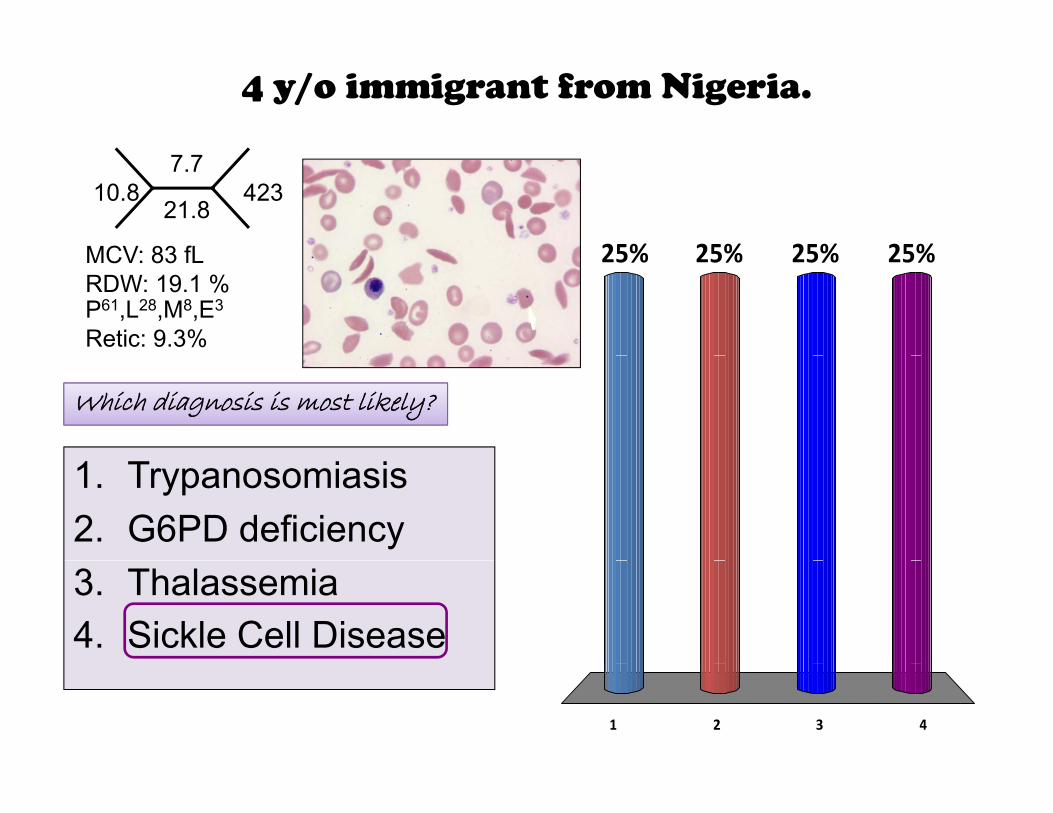
4 y/o immigrant from Nigeria.
7.710.8
21.8423
MCV 83 fL
P61,L28,M8,E3
MCV: 83 fLRDW: 19.1 %
Retic: 9.3%
• Not previously known to be anemic.
• Bloodwork on his initial “well-child” check.
• 4-5 cm firm spleen felt on examination.
• Muddy sclerae
• II/VI systolic murmur left sternal border
4 y/o immigrant from Nigeria.
10.87.7
21.8423
MCV: 83 fL 25% 25%25%25%
P61,L28,M8,E3
MCV: 83 fL
Retic: 9.3%
RDW: 19.1 %25% 25%25%25%
Which diagnosis is most likely?
1. Trypanosomiasis2. G6PD deficiency3. Thalassemia4. Sickle Cell Disease
1 2 3 4
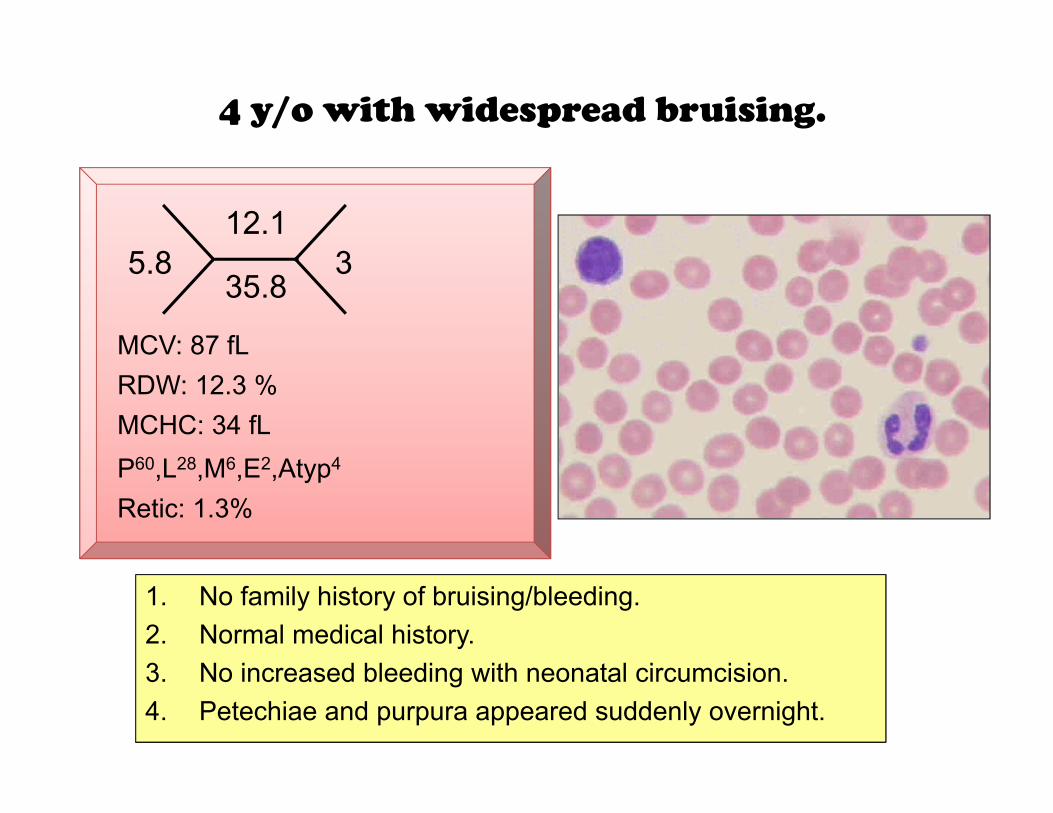
4 y/o with widespread bruising.
5 812.1
35.835.8
3
MCV: 87 fL
60 28 6 2 4
RDW: 12.3 %MCHC: 34 fLP60,L28,M6,E2,Atyp4
Retic: 1.3%
1. No family history of bruising/bleeding.2. Normal medical history.3 N i d bl di i h l i i i3. No increased bleeding with neonatal circumcision.4. Petechiae and purpura appeared suddenly overnight.

4 y/o with widespread bruising.
5.812.135.8 3
25% 25%25%25%
P60,L28,M6,E2,Atyp4
MCV: 87 fL
R ti 1 3%
RDW: 12.3 %MCHC: 34 fL
25% 25%25%25%
Retic: 1.3%
Which diagnosis is most likely?g y
1. Acute Leukemia2. Idiopathic Aplastic Anemia3. Child abuse4. ITP (Primary autoimmune
thrombocytopenia)
1 2 3 4
y p )

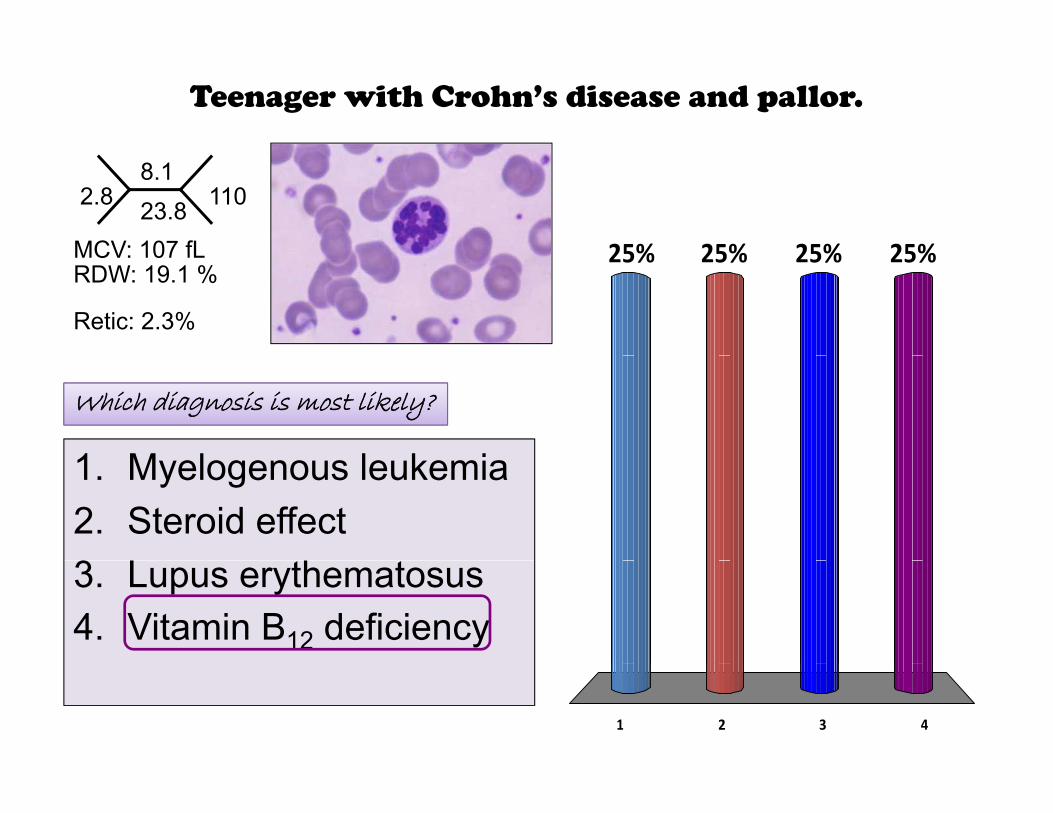
Teenager with Crohn’s disease and pallor.
2 86.7
1102.819.8
110
MCV: 107 fL
P41,L48,M9,E2
Retic: 2 3%
RDW: 19.1 %
• Diagnosed 4 years prior with IBD
Retic: 2.3%
Diagnosed 4 years prior with IBD
• Hospitalized a few times with Crohn’s exacerbations.
• Pallor seems to have come on gradually.
• Symptoms include some weakness and dizziness.
Teenager with Crohn’s disease and pallor.
2.88.123.8 110
MCV: 107 fL 25% 25%25%25%MCV: 107 fL
Retic: 2.3%
RDW: 19.1 %25% 25%25%25%
Which diagnosis is most likely?
1 M l l k i1. Myelogenous leukemia2. Steroid effect3 L h3. Lupus erythematosus4. Vitamin B12 deficiency
1 2 3 4
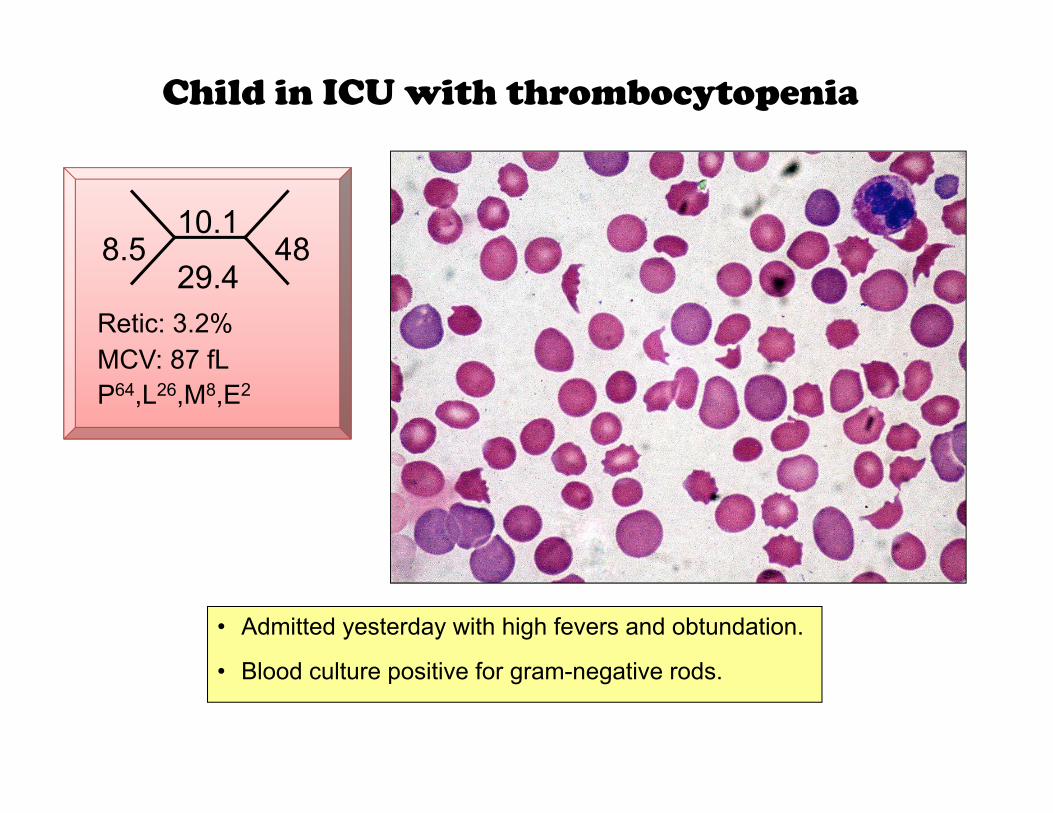
Child in ICU with thrombocytopenia
8 510.1
488.529.4
48
MCV: 87 fLRetic: 3.2%
P64,L26,M8,E2MCV: 87 fL
• Admitted yesterday with high fevers and obtundation.
Bl d lt iti f ti d• Blood culture positive for gram-negative rods.
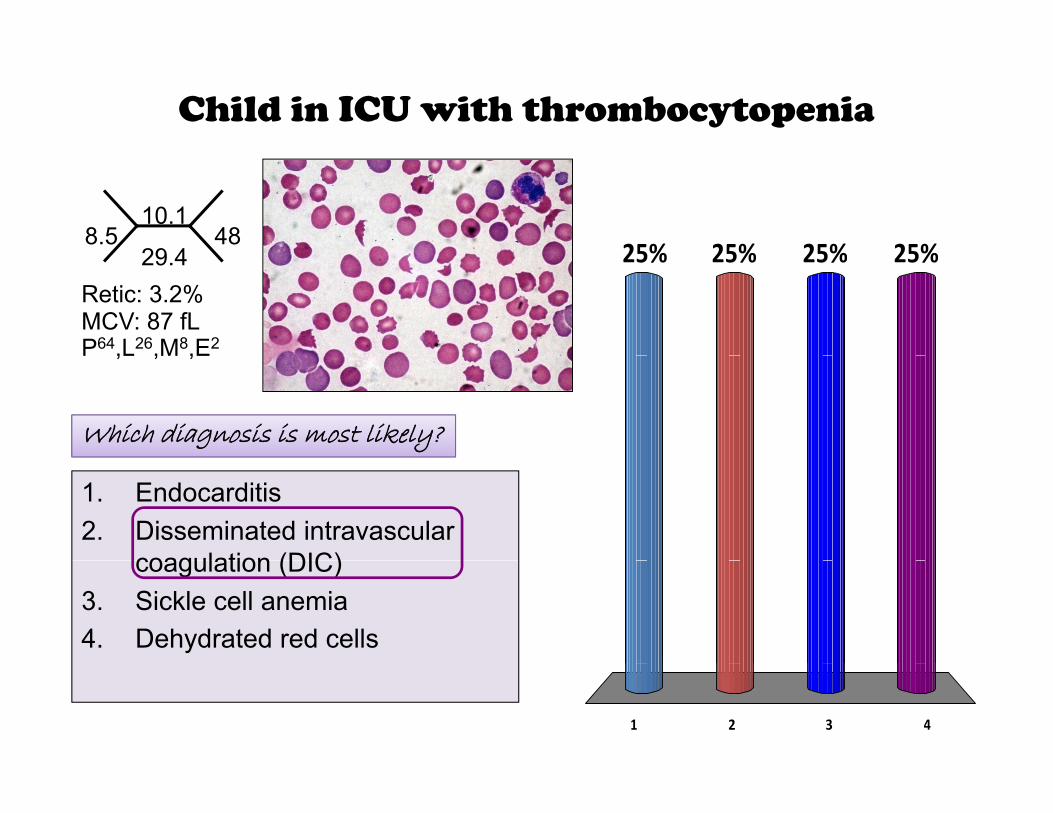
Child in ICU with thrombocytopenia
8.510.1
29 448
25% 25%25%25%29.4
P64,L26,M8,E2MCV: 87 fLRetic: 3.2%
25% 25%25%25%
P ,L ,M ,E
Which diagnosis is most likely?
1. Endocarditis2. Disseminated intravascular
coagulation (DIC)coagulation (DIC)3. Sickle cell anemia4. Dehydrated red cells
1 2 3 4
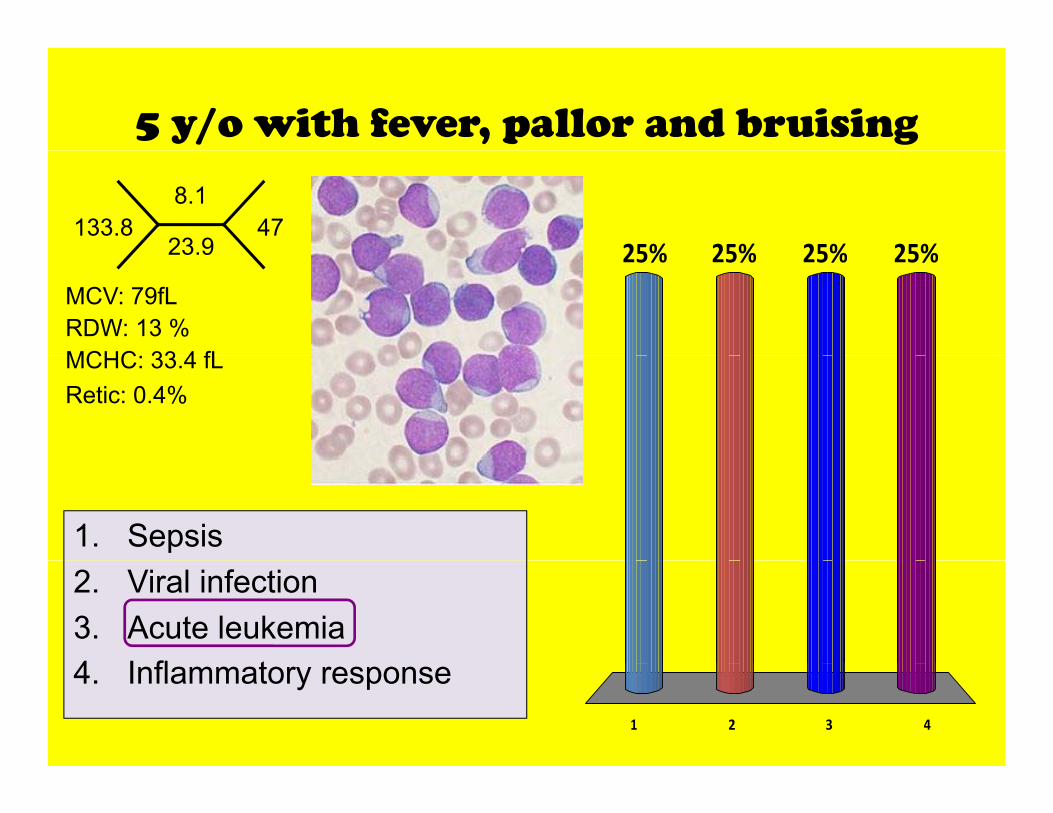
5 y/o with fever, pallor and bruising
133.88.1
23.947
25% 25%25%25%23.9
MCV: 79fLRDW: 13 %MCHC 33 4 fL
25% 25%25%25%
Retic: 0.4%MCHC: 33.4 fL
1. Sepsis2. Viral infection3. Acute leukemia4 I fl t
1 2 3 4
4. Inflammatory response
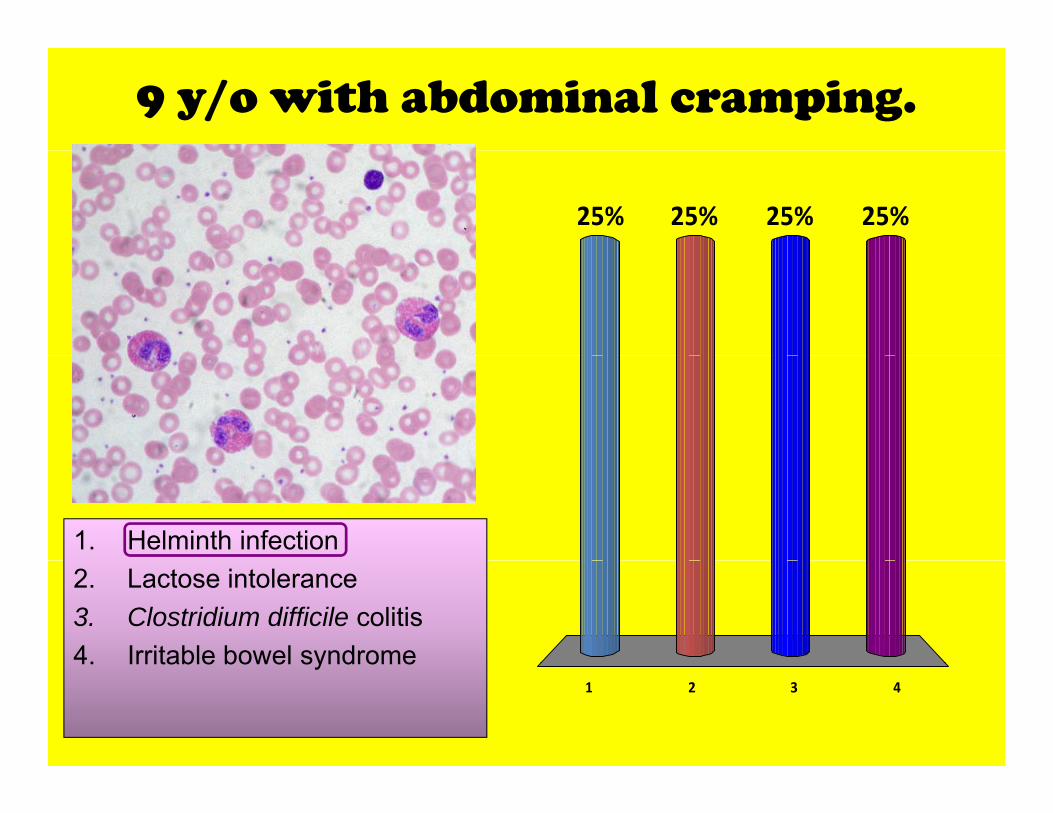
9 y/o with abdominal cramping.
25% 25%25%25%
1. Helminth infection2. Lactose intolerance3. Clostridium difficile colitis4. Irritable bowel syndrome
1 2 3 4
4. Irritable bowel syndrome
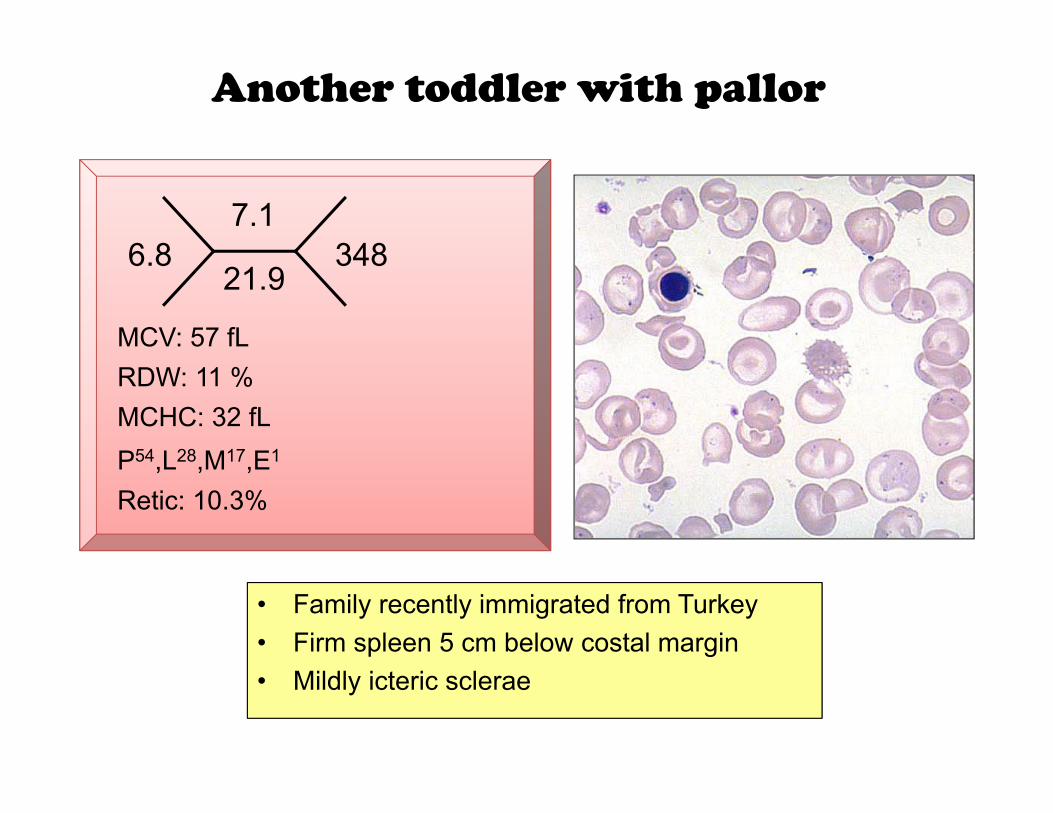
Another toddler with pallor
6 87.1
3486.821.9
348
MCV: 57 fL
P54 L28 M17 E1
RDW: 11 %MCHC: 32 fLP54,L28,M17,E1
Retic: 10.3%
• Family recently immigrated from Turkey• Firm spleen 5 cm below costal margin• Mildly icteric sclerae
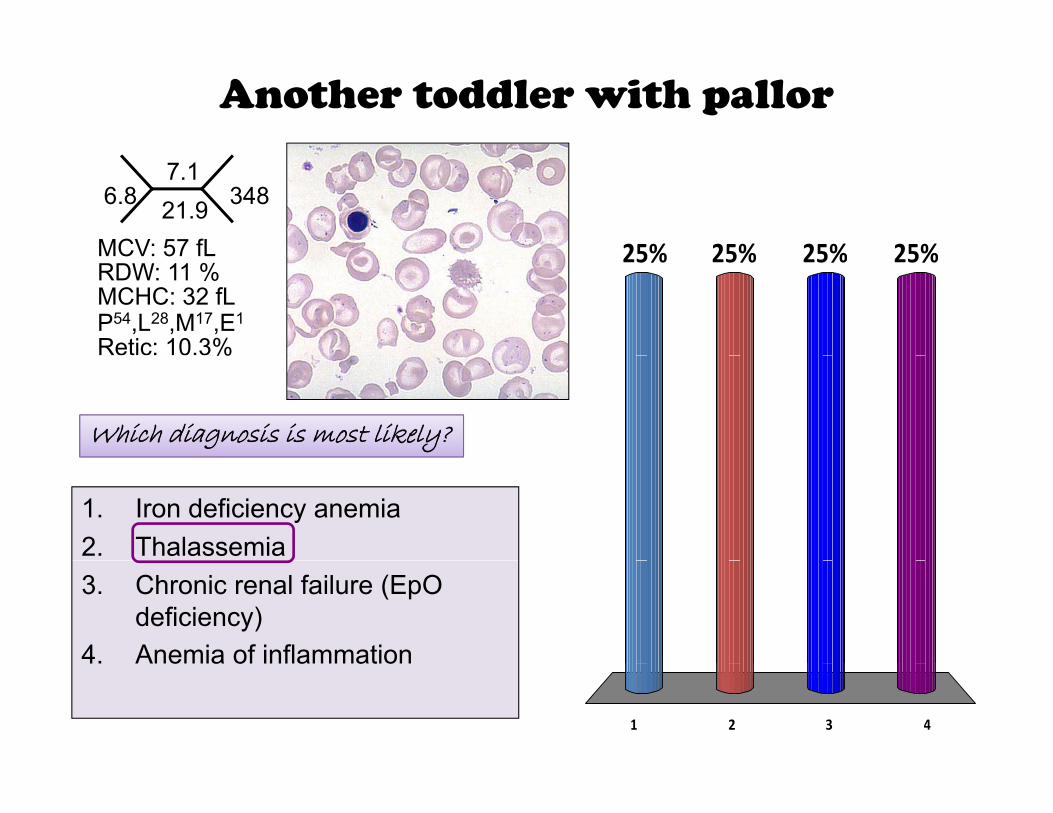
Another toddler with pallor
6.87.121.9 348
MCV: 57 fL 25% 25%25%25%
P54,L28,M17,E1
MCV: 57 fL
Retic: 10.3%
RDW: 11 %MCHC: 32 fL
25% 25%25%25%
%
Which diagnosis is most likely?
1. Iron deficiency anemia2. Thalassemia3. Chronic renal failure (EpO
deficiency)4. Anemia of inflammation
1 2 3 4
4. Anemia of inflammation
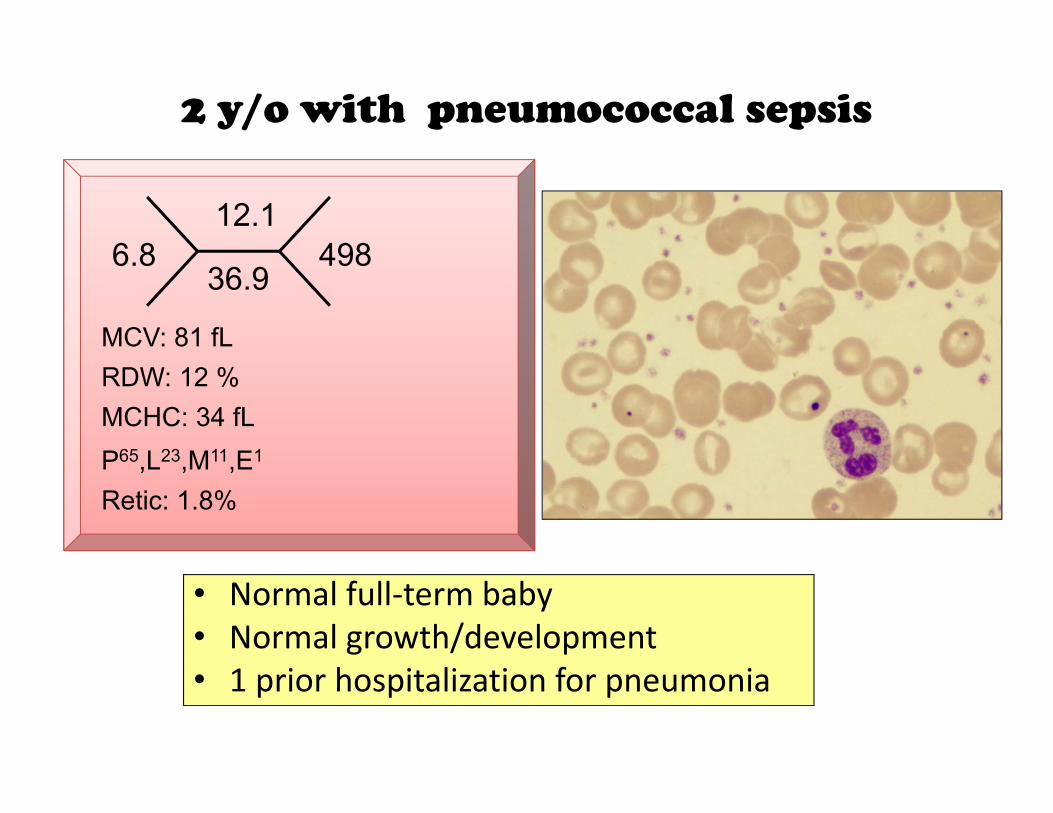
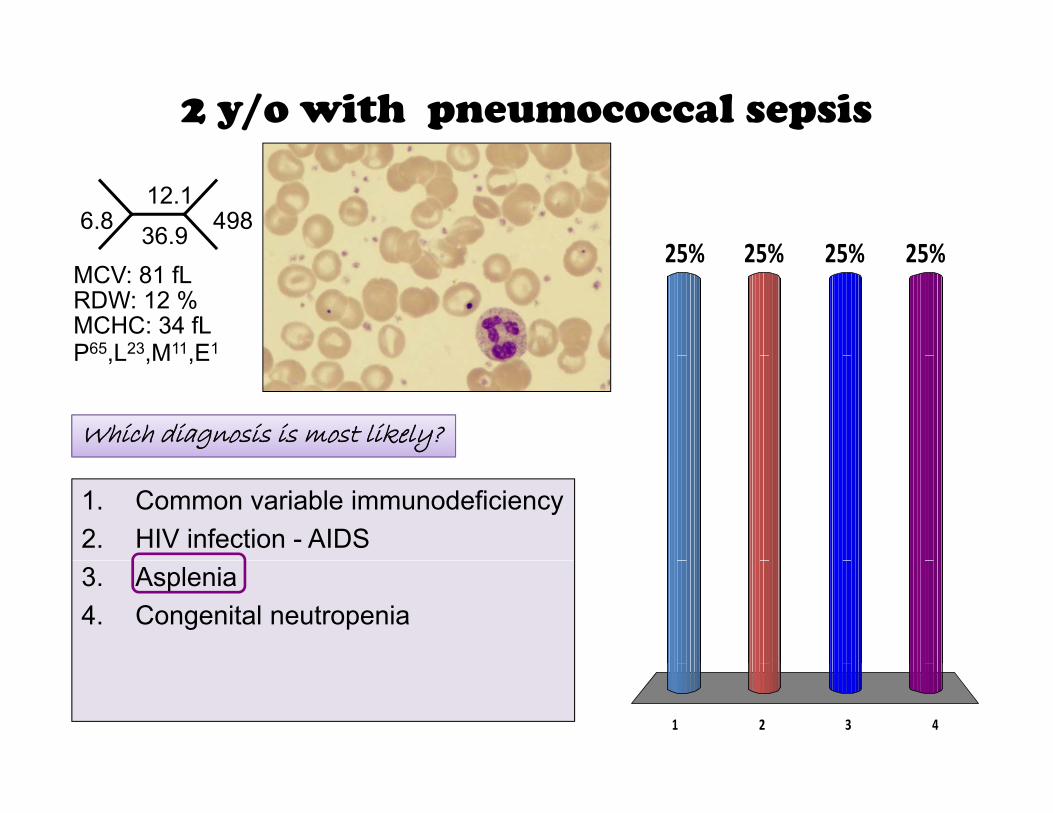
2 y/o with pneumococcal sepsis
6 812.1
4986.836.9
498
MCV: 81 fL
P65 L23 M11 E1
RDW: 12 %MCHC: 34 fLP65,L23,M11,E1
Retic: 1.8%
• Normal full‐term baby• Normal growth/development• 1 prior hospitalization for pneumonia
2 y/o with pneumococcal sepsis
6.812.1
36.9 49825% 25%25%25%
P65 L23 M11 E1
MCV: 81 fLRDW: 12 %MCHC: 34 fL
25% 25%25%25%
P ,L ,M ,E
Which diagnosis is most likely?
1. Common variable immunodeficiency2. HIV infection - AIDS3. Asplenia4. Congenital neutropenia
1 2 3 4
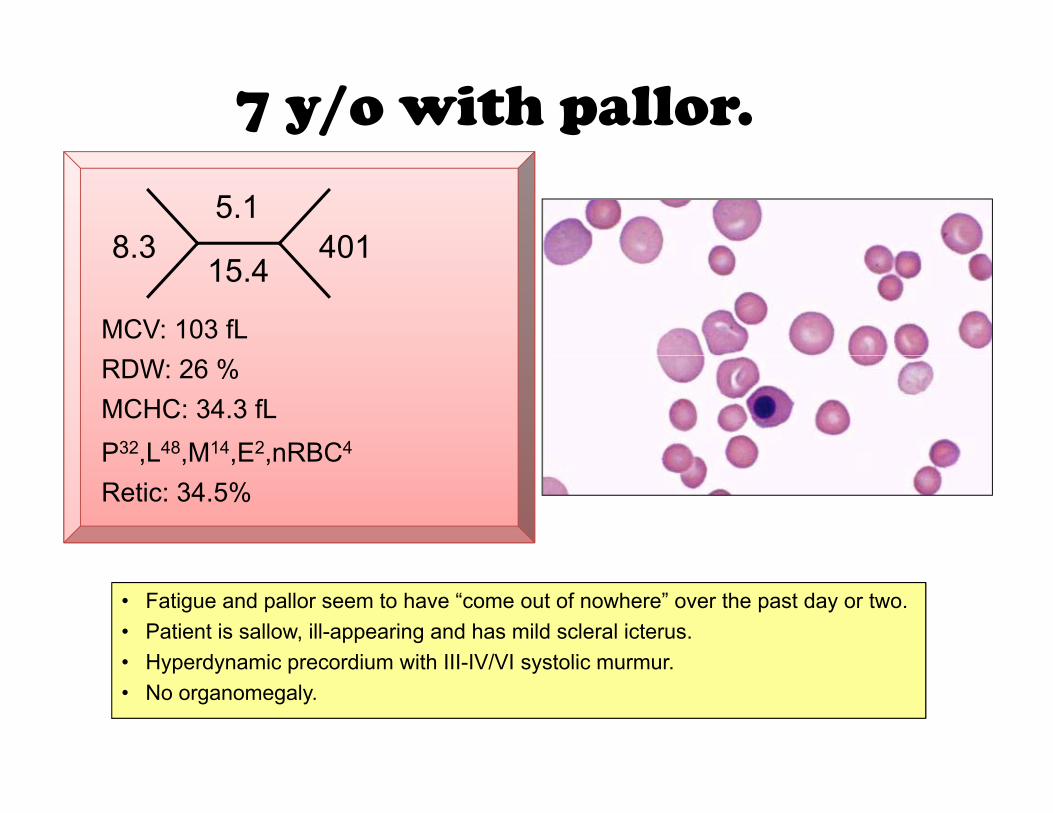
7 y/o with pallor.
8 35.1
4018.315.4
401
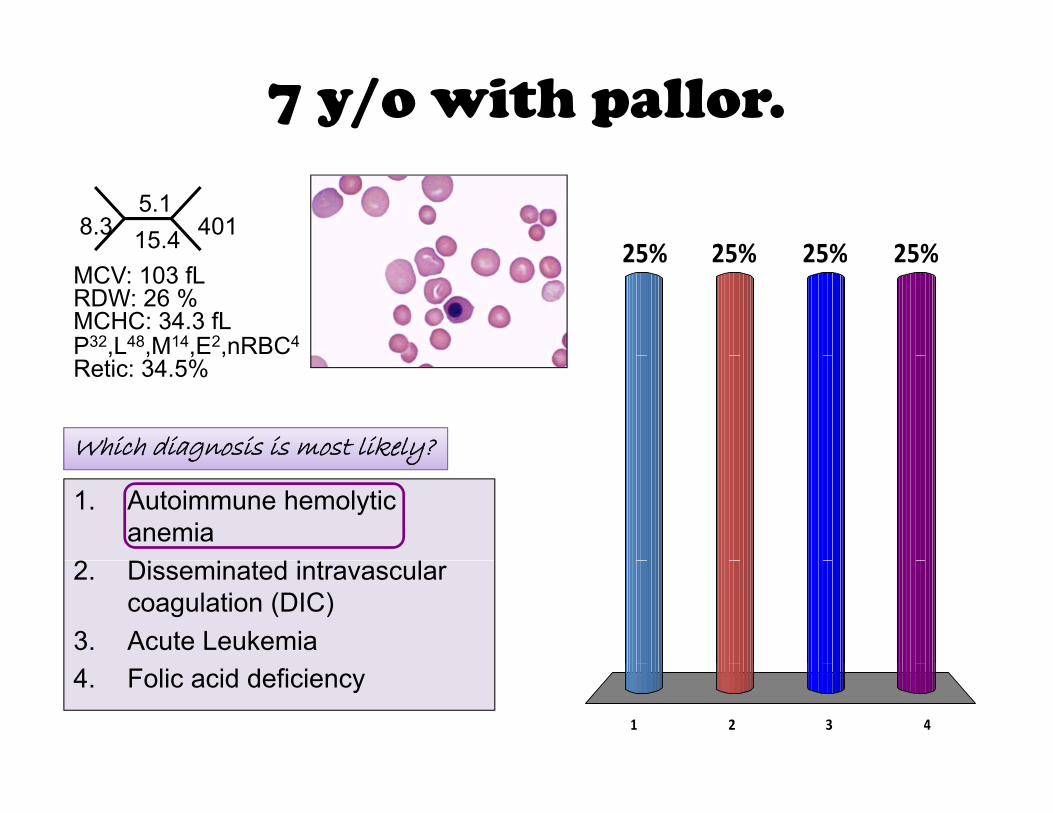
MCV: 103 fL
P32 L48 M14 E2 nRBC4
RDW: 26 %MCHC: 34.3 fLP ,L ,M ,E ,nRBCRetic: 34.5%
• Fatigue and pallor seem to have “come out of nowhere” over the past day or two.• Patient is sallow, ill-appearing and has mild scleral icterus.• Hyperdynamic precordium with III-IV/VI systolic murmur• Hyperdynamic precordium with III-IV/VI systolic murmur.• No organomegaly.
7 y/o with pallor.
8.35.115.4 401
25% 25%25%25%
P32,L48,M14,E2,nRBC4
MCV: 103 fLRDW: 26 %MCHC: 34.3 fL
25% 25%25%25%
, , , ,Retic: 34.5%
Which diagnosis is most likely?g y
1. Autoimmune hemolytic anemia
22. Disseminated intravascular coagulation (DIC)
3. Acute Leukemia
1 2 3 4
4. Folic acid deficiency
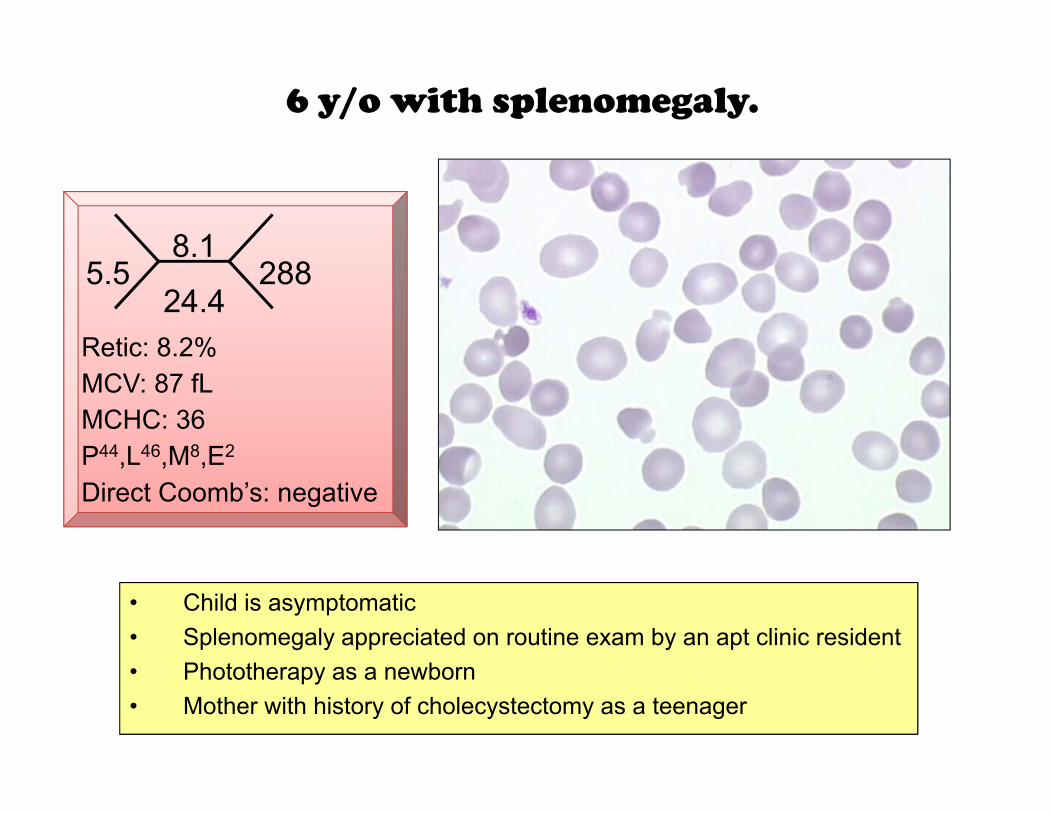
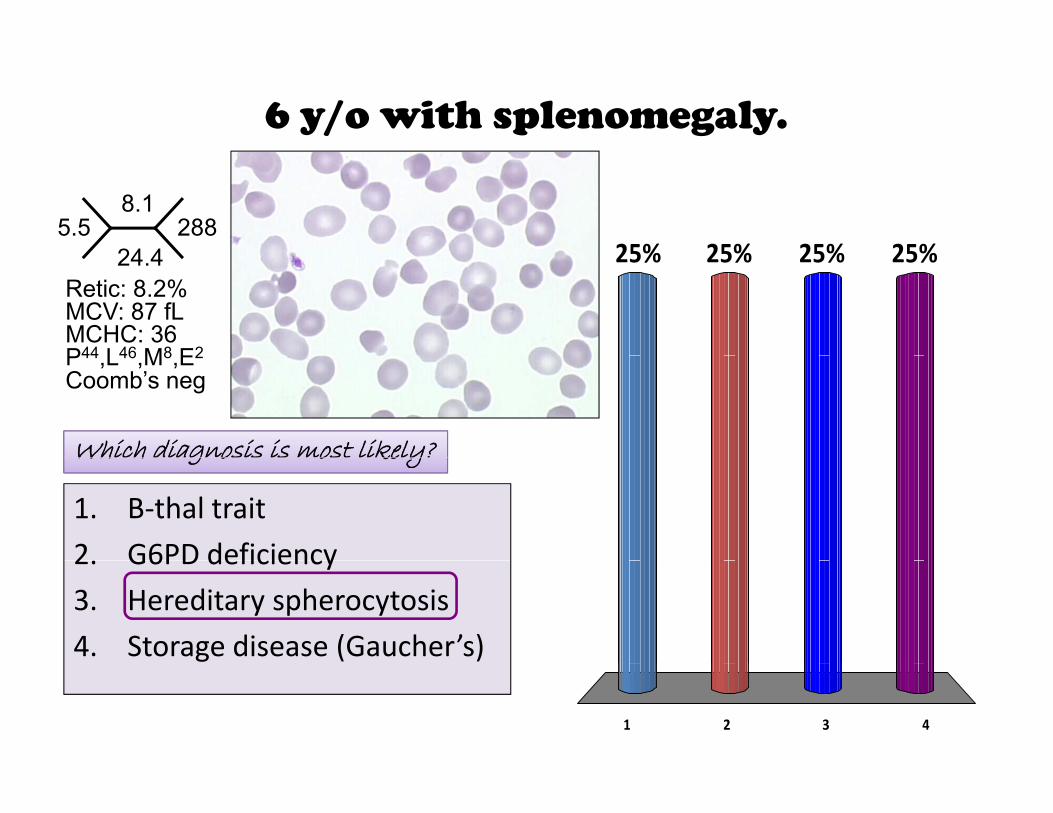
6 y/o with splenomegaly.
8 15.5
8.1
24.4288
Retic: 8.2%
P44 L46 M8 E2
MCV: 87 fLRetic: 8.2%
MCHC: 36
Direct Coomb’s: negativeP ,L ,M ,E
• Child is asymptomatic• Splenomegaly appreciated on routine exam by an apt clinic resident
Ph t th b• Phototherapy as a newborn• Mother with history of cholecystectomy as a teenager
6 y/o with splenomegaly.
5.58.1
24 4288
25% 25%25%25%24.4
P44 L46 M8 E2
MCV: 87 fLRetic: 8.2%
MCHC: 36
25% 25%25%25%
Coomb’s negP44,L46,M8,E2
Which diagnosis is most likely?Wh h g o o ke y
1. B‐thal trait
2 G6PD deficiency2. G6PD deficiency
3. Hereditary spherocytosis
4. Storage disease (Gaucher’s)
1 2 3 4
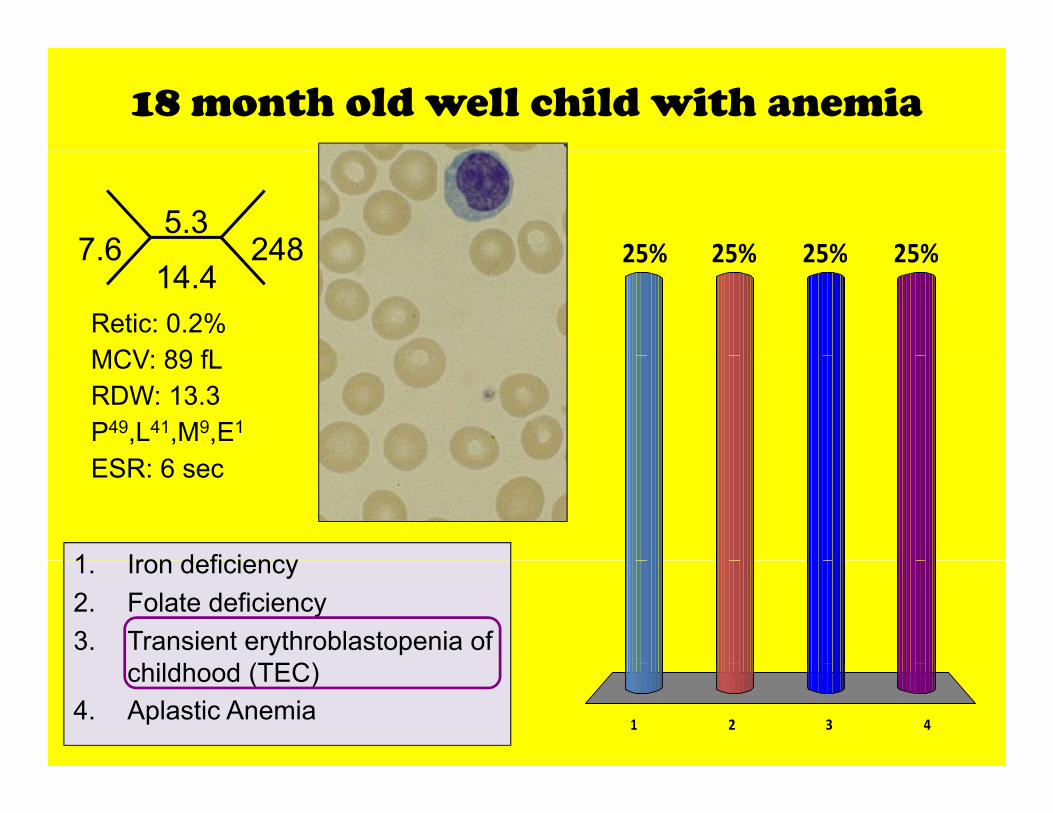
18 month old well child with anemia
7 65.3
248 25% 25%25%25%7.614.4
248
MCV: 89 fLRetic: 0.2%
25% 25%25%25%
P49,L41,M9,E1
MCV: 89 fLRDW: 13.3
ESR: 6 sec
1 Iron deficiency1. Iron deficiency2. Folate deficiency3. Transient erythroblastopenia of
hildh d (TEC)
1 2 3 4
childhood (TEC)4. Aplastic Anemia
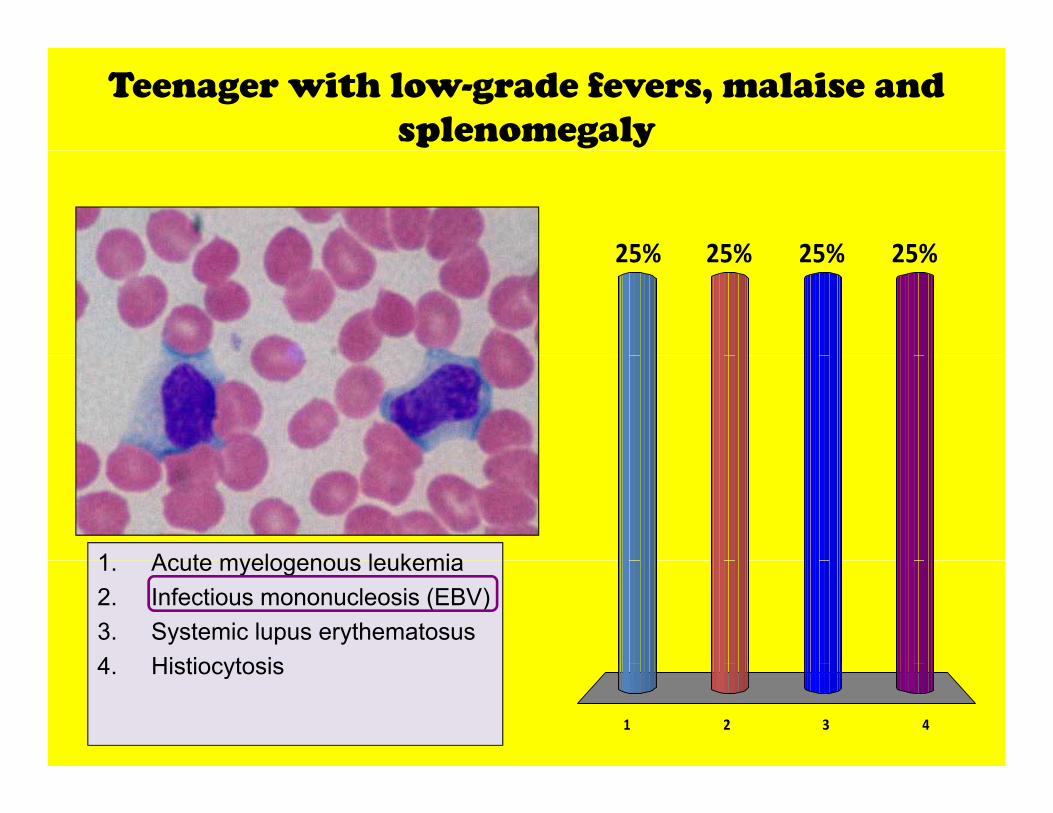
Teenager with low-grade fevers, malaise and splenomegaly
25% 25%25%25%25% 25%25%25%
1 Acute myelogenous leukemia1. Acute myelogenous leukemia2. Infectious mononucleosis (EBV)3. Systemic lupus erythematosus4 Histiocytosis
1 2 3 4
4. Histiocytosis
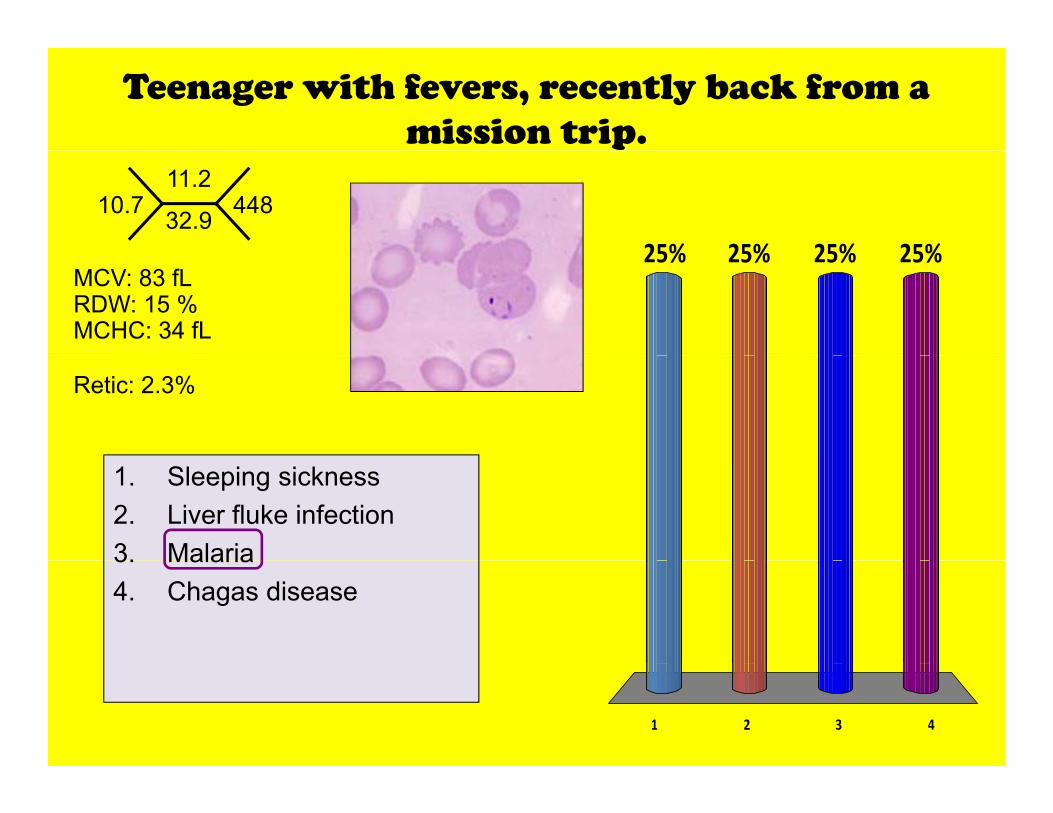
Teenager with fevers, recently back from a mission trip.
10.711.2
32.9 448
25% 25%25%25%MCV: 83 fLRDW: 15 %MCHC: 34 fL
25% 25%25%25%
Retic: 2.3%
1. Sleeping sickness2. Liver fluke infection3. Malaria3. Malaria4. Chagas disease
1 2 3 4

School-age child with bruising and low-grade fevergrade fever
28 48.3
52 25% 25%25%25%28.424.7
52
MCV: 91 fLRDW: 13 %
25% 25%25%25%
Retic: 1.7%MCHC: 33.4 fL
1. Acute myelogenous leukemiay g2. Reactive left shift3. ITP4 Listeria infection
1 2 3 4
4. Listeria infection
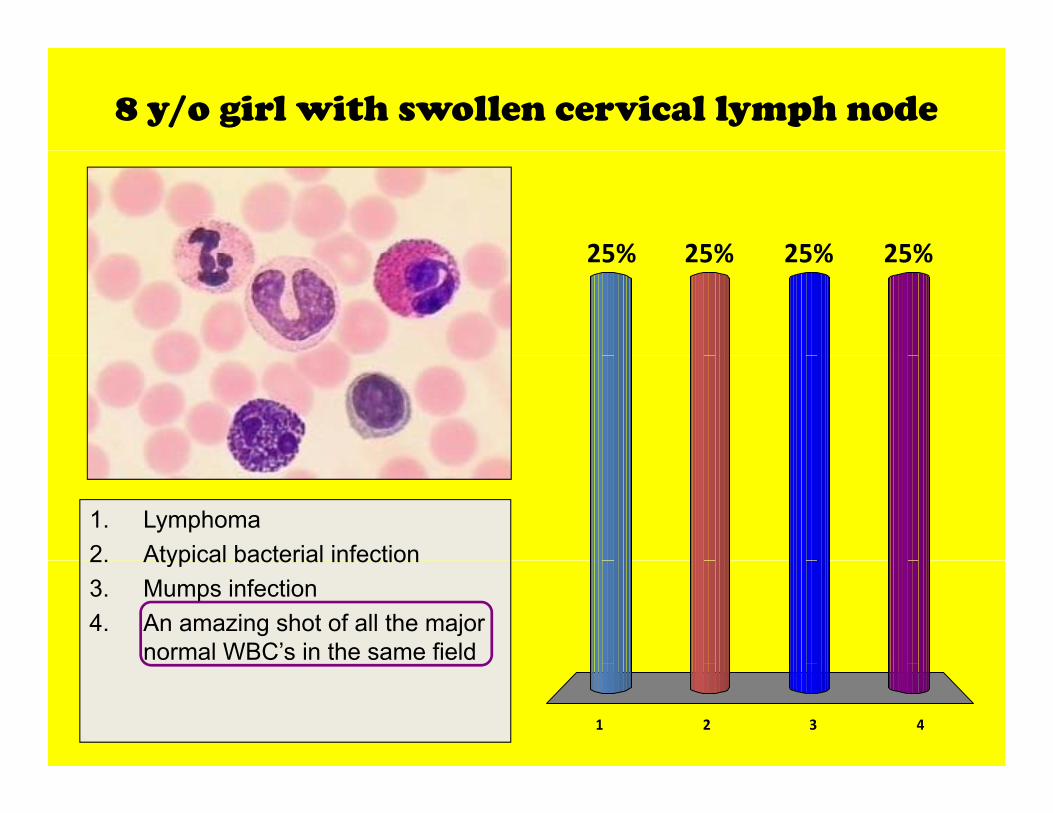
8 y/o girl with swollen cervical lymph node
25% 25%25%25%25% 25%25%25%
1. Lymphoma2. Atypical bacterial infection2. Atypical bacterial infection3. Mumps infection4. An amazing shot of all the major
normal WBC’s in the same field
1 2 3 4
Take home• The CBC and peripheral blood smear offer a wealth of information regarding g gpathophysiology.– Heme/onc diagnoses
– Atopy, Rheumatology
– Infectious disease“John always review the
– Others
Th i b fit t i i bl d
John, always review the primary data yourself…”
• There is benefit to reviewing blood smears yourself, especially in difficult or challenging casesor challenging cases.
Howard Weinstein, MDChief, Pediatric Hematology/Oncology, MGH
Or ask your friendly hematologist for help!
[email protected]; 323‐6238

What the !@#$ are they talking about?
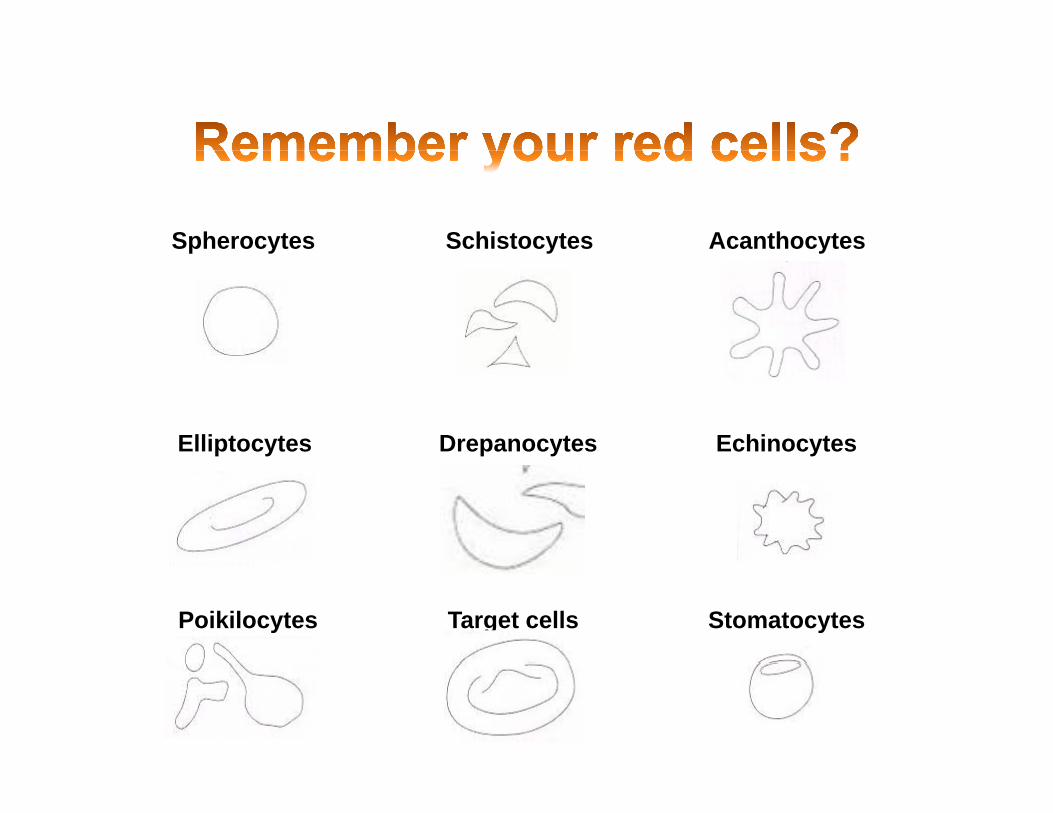
• Polychromasia, Polychromatophilia
RBC’s of different staining color, implies reticulocytosisy p
• PoikilocytosisRBC’s of different shape, mixed population (old + transfused cells)
RBC’s of different size;• Anisocytosis
• Schistocytosis
RBC s of different size; reticulocytosis, high RDW
RBC fragments, microangiopathic processes (DIC), shearing
• Elliptocytes, Ovalocytosis
• Drepanocytosis
RBC’s look elliptical, membranopathy
Sickle cell forms Hgb S disease• Drepanocytosis
• Spherocytosis
Sickle cell forms, Hgb S disease
No central pallor in rbc’s; HS or AIHA
• Howell‐Jolly bodies Functional asplenia
Acanthocytes SchistocytesSpherocytes yyp y
Echinocytes Elliptocytes Drepanocytes
Target cells Stomatocytes Poikilocytes

Decreased Increased
Neutrophils • Kostmann’s syndrome• Cyclic neutropenia
• Infections• Tissue destructiony p
• Bone marrow failure• Leukemia• Autoimmune neutropenia• Benign neutropenia of childhood
• Corticosteroids• Leukemoid reaction• GCSF administration
g p• Infection/sepsis• Drug‐induced (Bactrim, chemotherapy)• Myelodysplasia
Lymphocytes • Congenital immunodeficiency• Severe infection• Drugs (Corticosteroids alkylating)
• Viral infection (e.g. EBV)• Some fungal, parasitic infections• Rare bacterial infection (Pertussis)Drugs (Corticosteroids, alkylating)
• GI disease• Acquired Immunodeficiency
Rare bacterial infection (Pertussis)• Allergic reactions/drug sensitivities• Immunologic disease
Monocytes • Corticosteroids • Inflammatory responses• Recovery phase of neutropenia• Myeloproliferative disorders
Eosinophils • Bacterial infection• ACTH administration
• Parasitic infections• Allergic conditionsACTH administration Allergic conditions• Drug therapy
Basophils • Corticosteroids • Bone marrow failure• Myeloproliferative syndromes
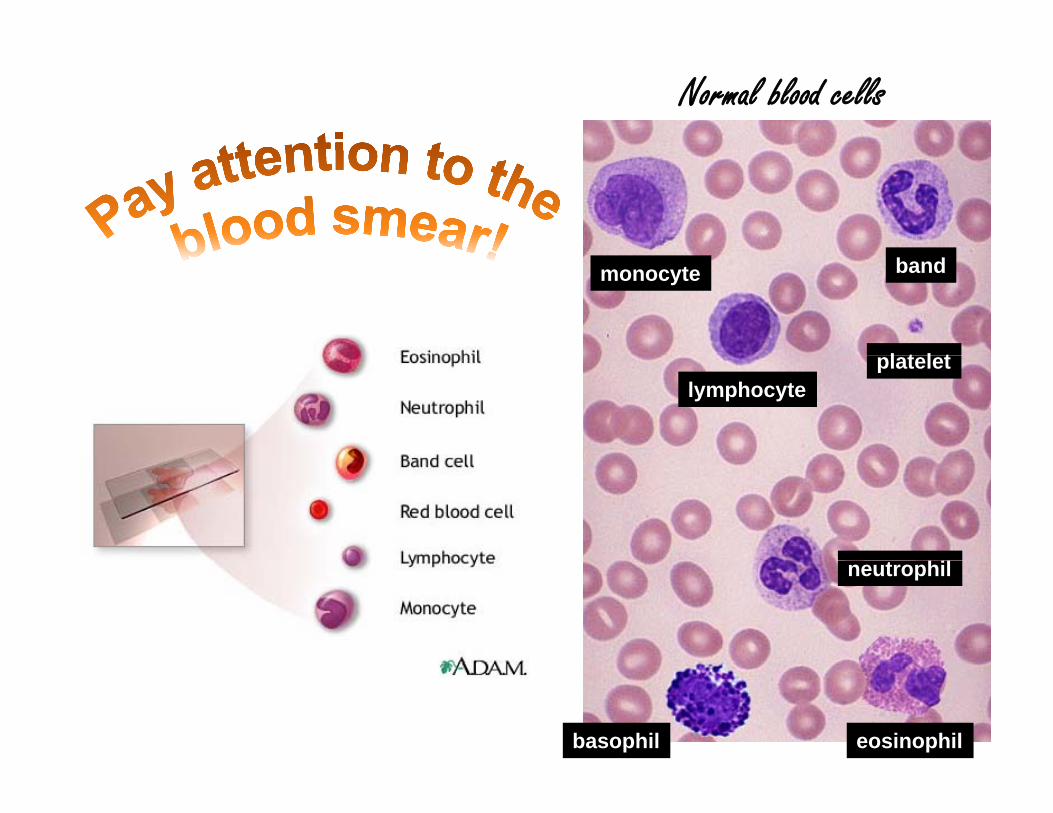
Normal blood cells
bandmonocyte
l t l tlymphocyte
platelet
neutrophil
eosinophilbasophil
Anemia‐ a suggested approach• Does the child look anemic?
• Does the child act anemic?
• Key physical exam parameters:
– Look at the conjunctiva under the lower eye lid
– Splenomegaly? Tachycardia? Petechiae/purpurae?
• The lab tests to order will be dictated by:
The degree of pallor presence of symptoms– The degree of pallor, presence of symptoms
– Physical findings (jaundice, HSM, adenopathy, etc)
– Apparent pace of the anemiapp p
– What diagnoses are being considered
• Start out with a CBC, but always order a reticulocyte count too!
– The retic count distinguishes between RBC destruction and underproduction

Red blood cells
Mean corpuscular hemoglobin (MCH)Mean corpuscular hemoglobin (MCH)
• Average amount of Hgb inside each RBCg g
• High MCH’s go along with large (macrocytic) RBC’s
• Low MCH’s correlate with microcytosis and anemias caused by impaired Hgb
th isynthesis.

Mean corpuscular hemoglobin i (MCHC)concentration (MCHC)
• Average concentration of hemoglobin inside a red cell.
• Takes red cell volume into account
• Decreased MCHC values (hypochromia) seen in conditions where Hgb is abnormally diluted inside RBC’s
• Iron deficiency anemia
• Thalassemia
• Increased MCHC values (hyperchromia) seen when Hgb is abnormally concentrated inside RBC’sconcentrated inside RBC s
• Spherocytosis
• Abnormal Hgb (S, C)If MCHC 35 fL thi k h t !
g ( , )
• Severe burns If MCHC > 35 fL, think spherocytes!
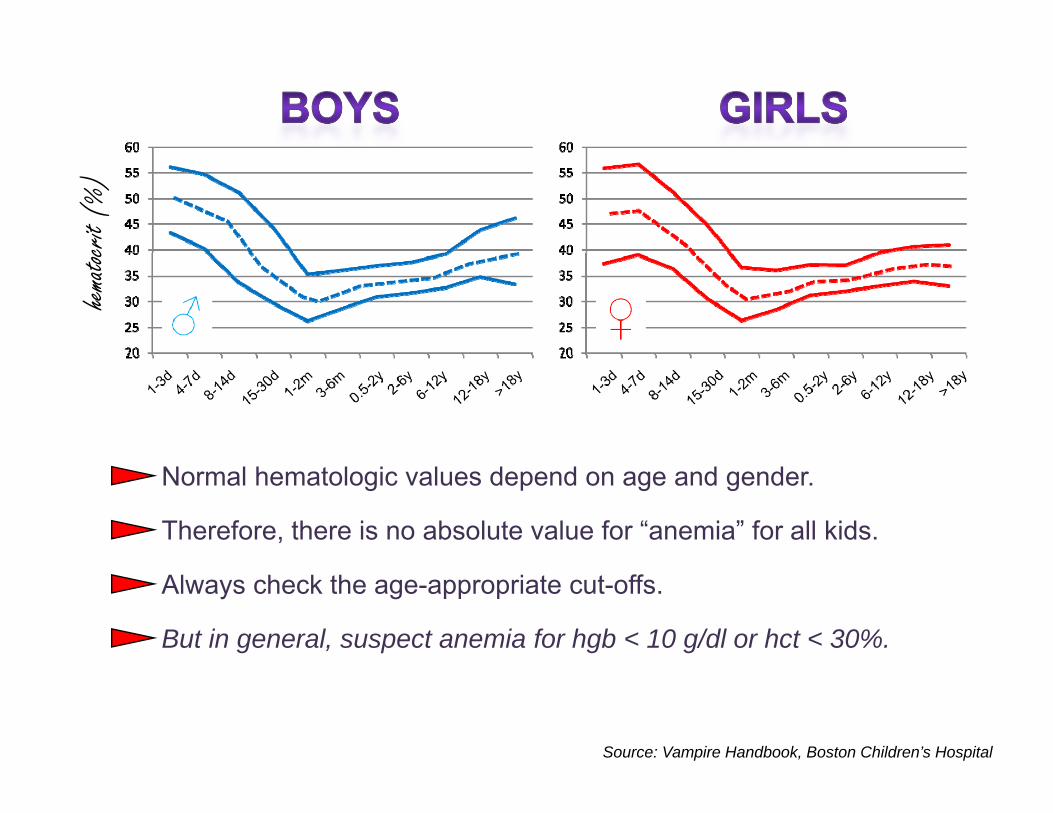
crit (
%)
hemato
c
Normal hematologic values depend on age and gender.
Therefore, there is no absolute value for “anemia” for all kids.
Always check the age-appropriate cut-offs.
But in general, suspect anemia for hgb < 10 g/dl or hct < 30%.
Source: Vampire Handbook, Boston Children’s Hospital

1 y/o with pallor1 y/o with pallor
8 28.2
351 25% 25%25%25%8.2 23.9 351
MCV: 71 fLRDW: 18.4 %
25% 25%25%25%
Retic: 2.6%
1. Lead poisoning2 Malaria2. Malaria3. Babesiosis4. Hemoglobin C disease
1 2 3 4
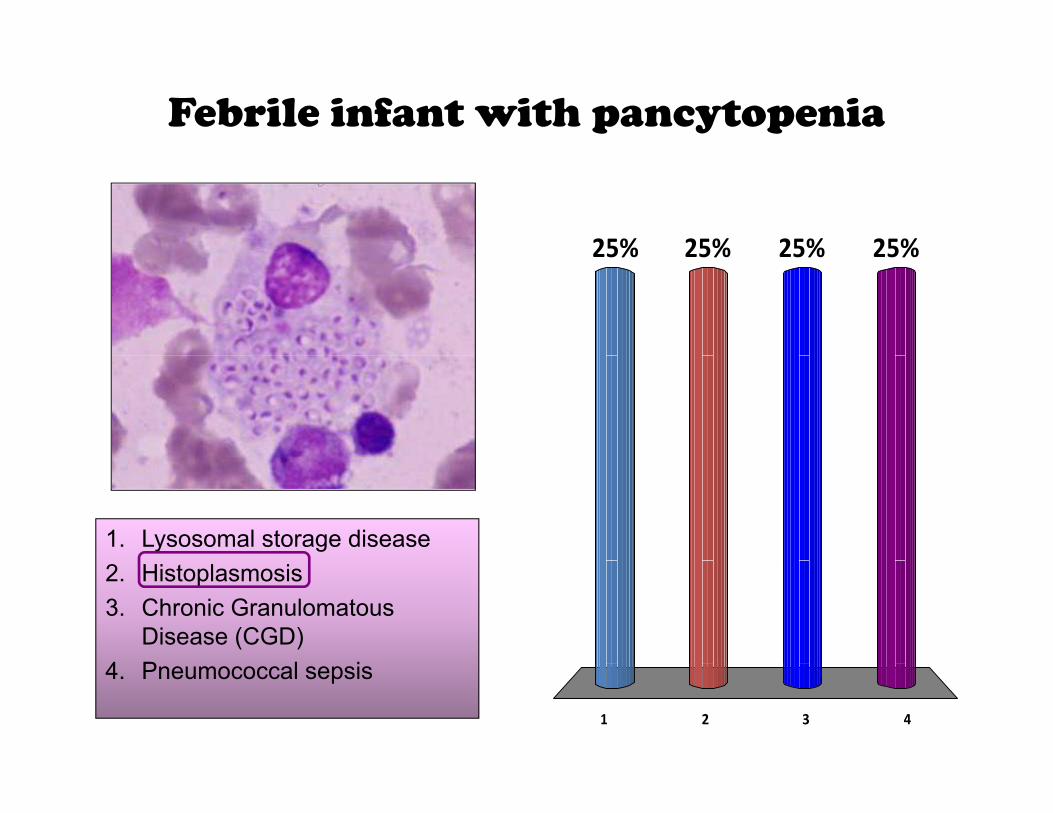
Febrile infant with pancytopenia
25% 25%25%25%25% 25%25%25%
1. Lysosomal storage disease2. Histoplasmosis3. Chronic Granulomatous
Disease (CGD)4 P l i
1 2 3 4
4. Pneumococcal sepsis
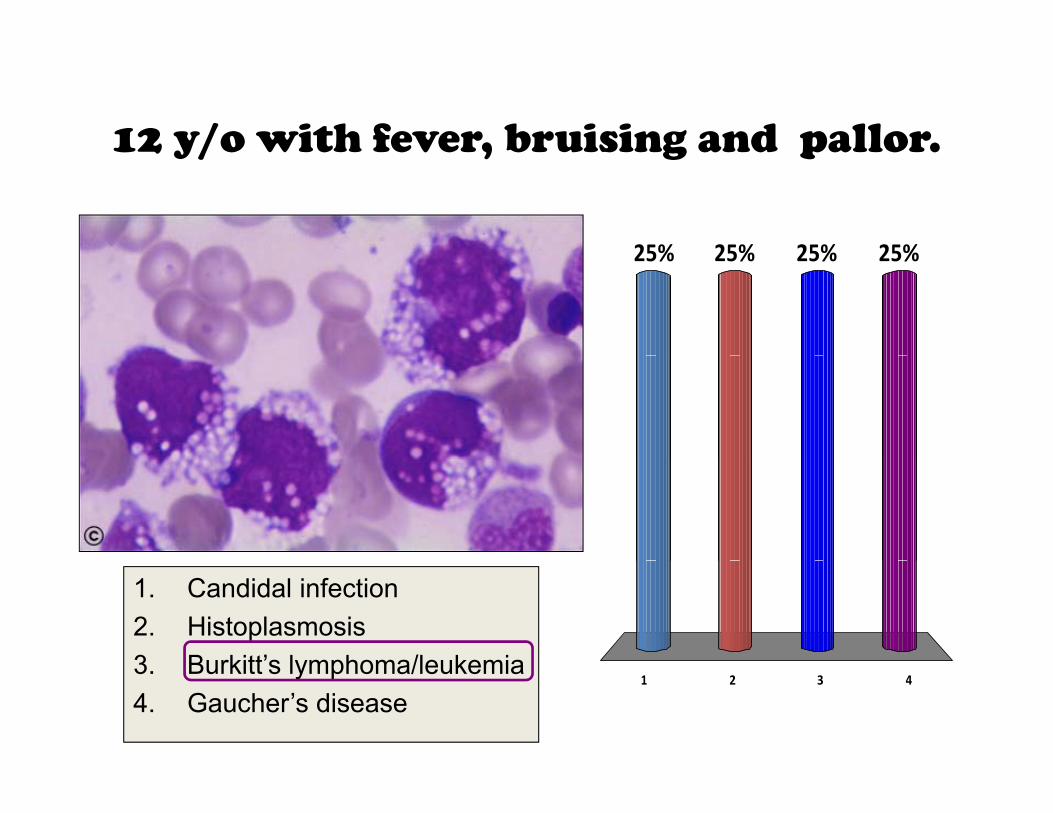
12 y/o with fever, bruising and pallor.12 y/o with fever, bruising and pallor.
25% 25%25%25%25% 25%25%25%
1. Candidal infection2. Histoplasmosis3 Burkitt’s lymphoma/leukemia
1 2 3 43. Burkitt s lymphoma/leukemia4. Gaucher’s disease
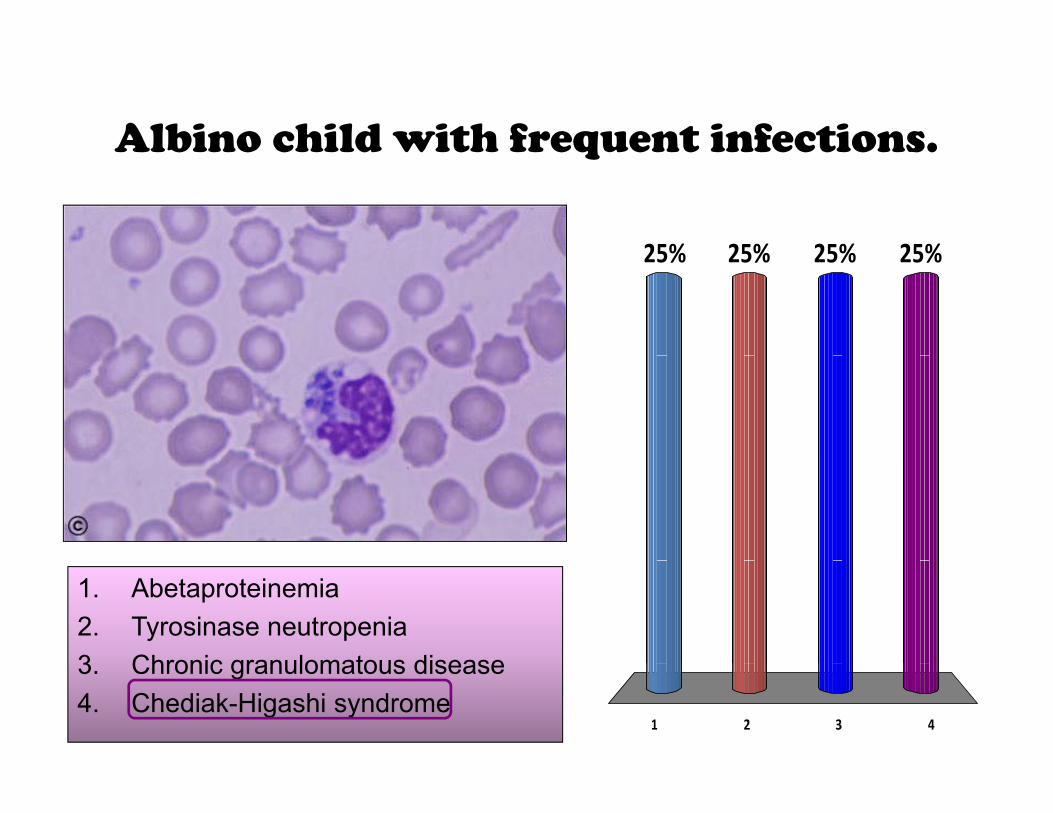
Albino child with frequent infections.Albino child with frequent infections.
25% 25%25%25%25% 25%25%25%
1. Abetaproteinemia2. Tyrosinase neutropenia3 Chronic granulomatous disease
1 2 3 4
3. Chronic granulomatous disease4. Chediak-Higashi syndrome

This is not a staining artifact!This is not a staining artifact!
25% 25%25%25%25% 25%25%25%
1 Obstructive liver disease1. Obstructive liver disease2. Abetalipoproteinemia3. Thalassemia
1 2 3 4
4. Severe burns
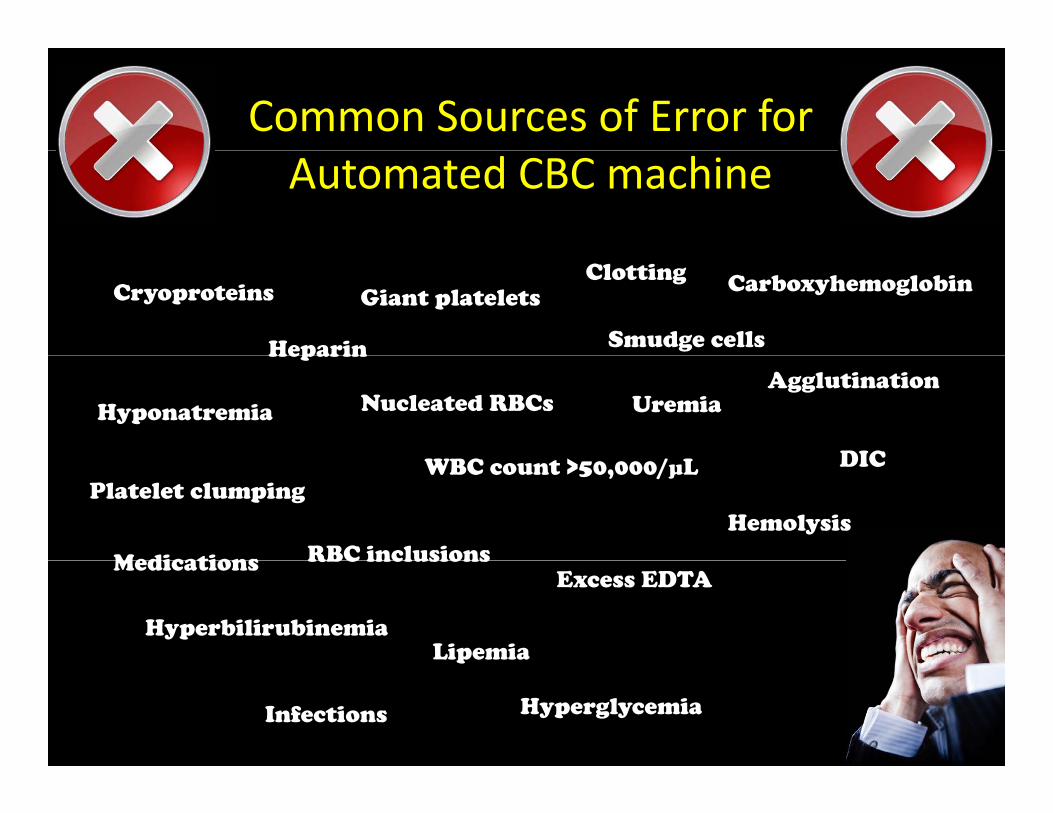
Common Sources of Error for Automated CBC machine
Cryoproteins
Heparin
Giant plateletsClotting
Smudge cells
Carboxyhemoglobin
Heparin
Nucleated RBCs Uremia HyponatremiaAgglutination
DICPlatelet clumping
WBC count >50,000/μL
Hemolysis
Medications RBC inclusions
DIC
Medications
HyperbilirubinemiaLipemia
RBC inclusionsExcess EDTA
p
Hyperglycemia Infections
Anemia: not enough red cells.
I d t i h l bi itInadequate oxygen-carrying hemoglobin capacity
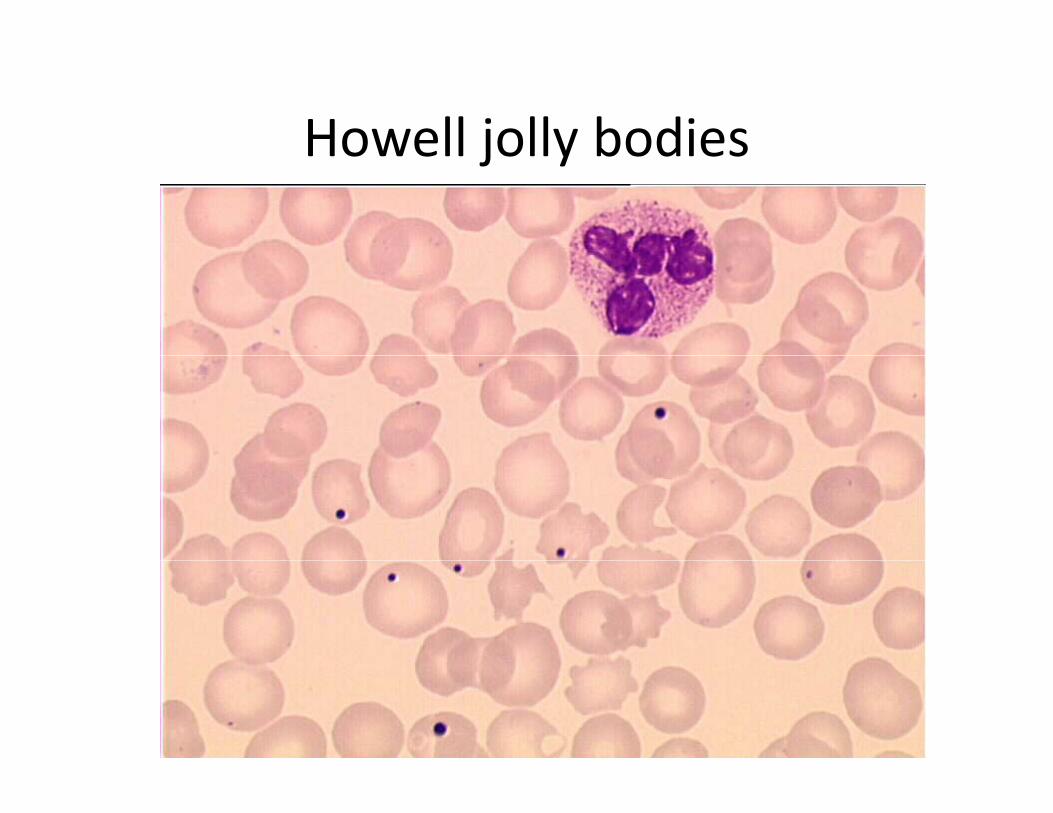
Howell jolly bodiesHowell jolly bodies
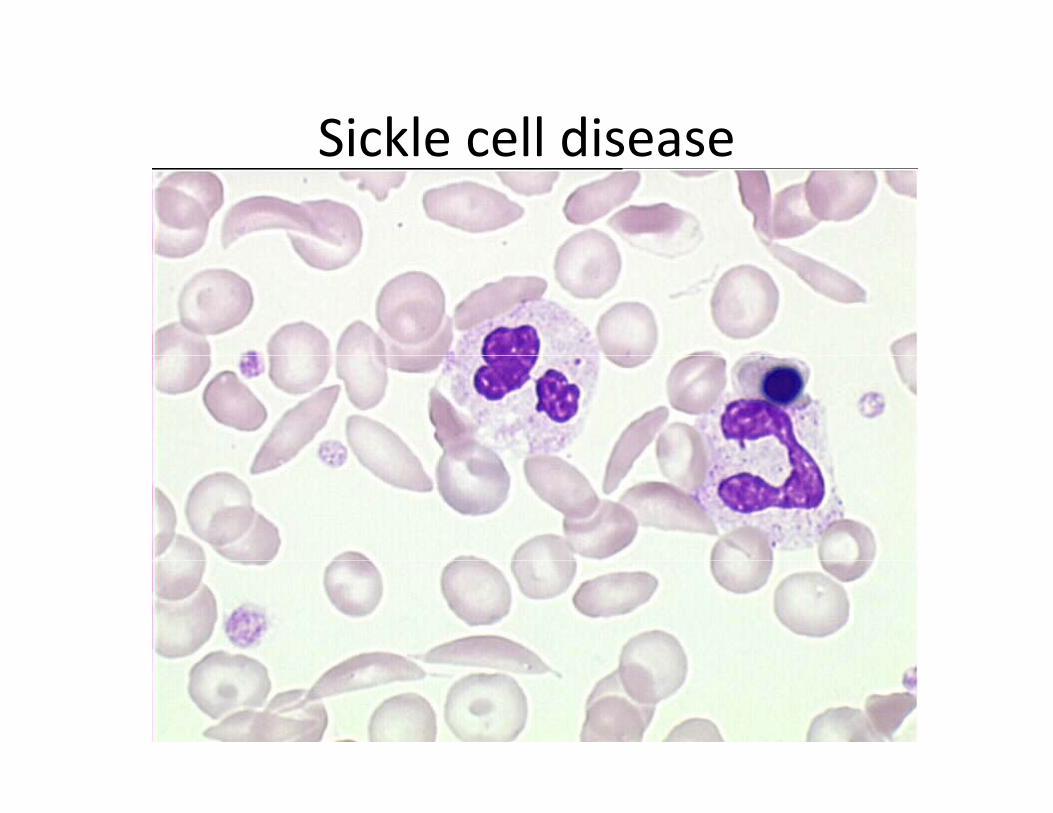
Sickle cell diseaseSickle cell disease
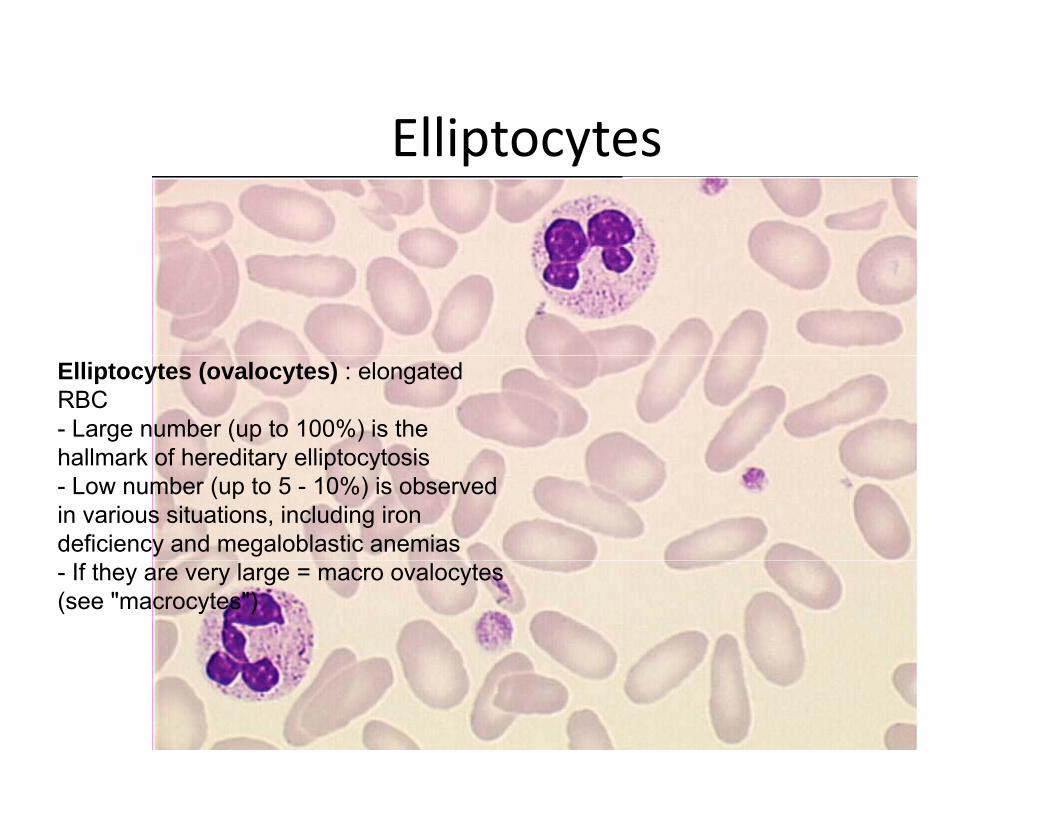
ElliptocytesElliptocytes
Elliptocytes (ovalocytes) : elongated RBC- Large number (up to 100%) is the hallmark of hereditary elliptocytosishallmark of hereditary elliptocytosis- Low number (up to 5 - 10%) is observed in various situations, including iron deficiency and megaloblastic anemias- If they are very large = macro ovalocytes (see "macrocytes")
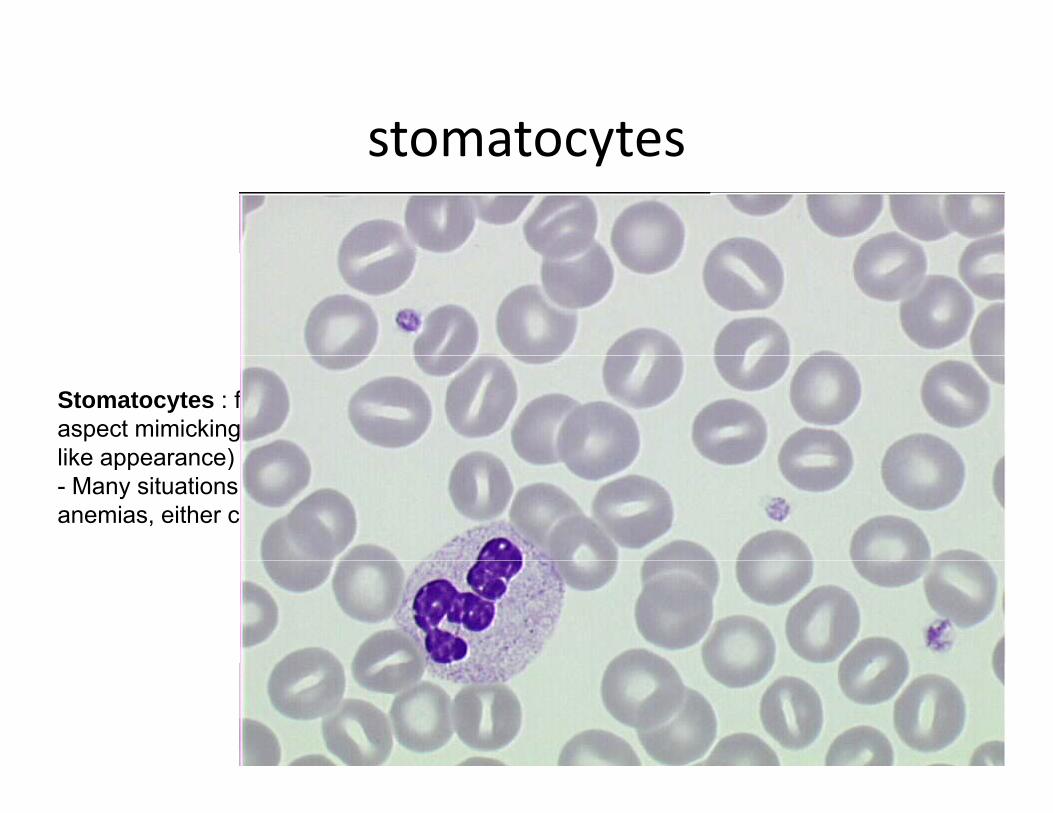
stomatocytesstomatocytes
Stomatocytes : folded RBC leading to an aspect mimicking a mouth and its lips (slit-like appearance)like appearance)- Many situations, including hemolytic anemias, either constitutive or acquired
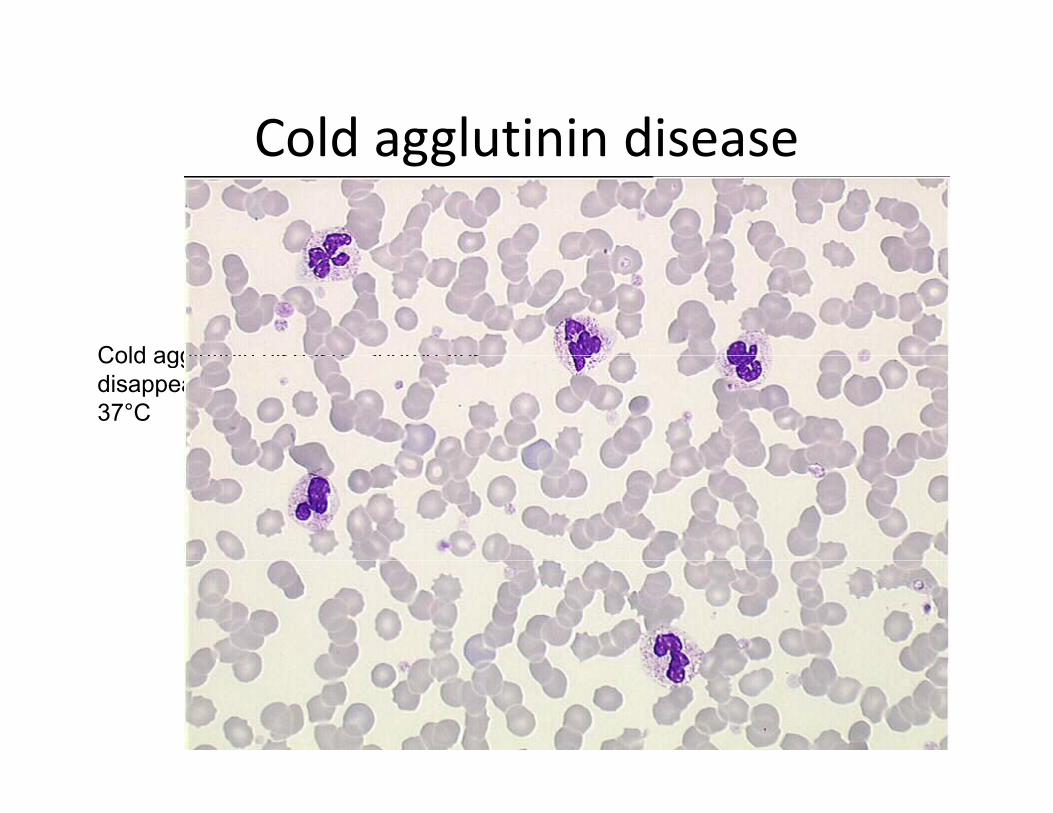
Cold agglutinin diseaseCold agglutinin disease
Cold agglutinin disease ; aggregatesCold agglutinin disease ; aggregates disappear after the sample is warmed at 37°C

echinocytesechinocytes
Echinocytes or crenated or contractedEchinocytes or crenated or contracted cells : up to 50 protrusions (spines or spurs) may be observed- They correspond usually to an artifact (glass slides, old samples, saline solutions)- Excess in lipids (not diet fed samples)- Various congenital haemoglobin and enzymatic disordersenzymatic disorders- Acute renal failure
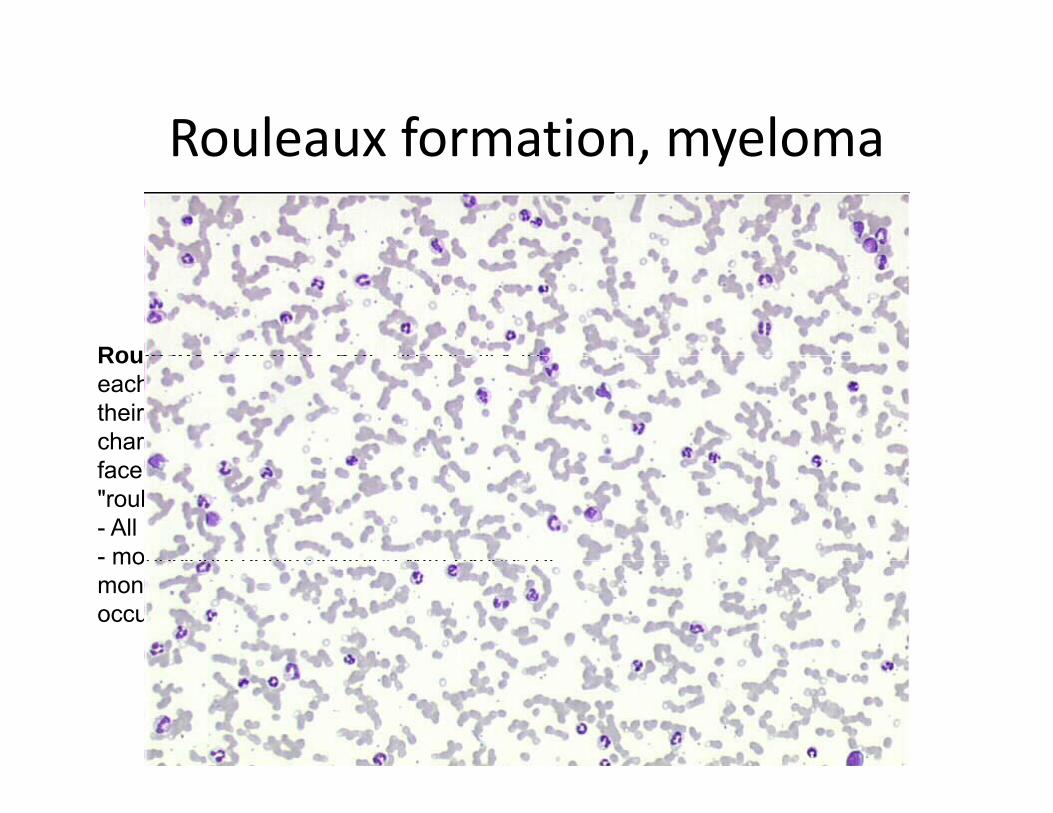
Rouleaux formation, myelomaRouleaux formation, myeloma
Rouleaux formation: RBC do not stick toRouleaux formation: RBC do not stick to each other in normal conditions because their external membrane is negatively charged; if neutralization occurs, RBC stick face to face, leading to the so-called "rouleaux formation"- All inflammatory disorders (slide)- monoclonal gammopathies with excess ofmonoclonal gammopathies with excess of monoclonal immunoglobulin (does not occur in light chain myeloma)

Acanthocytes : crenation is limited (3 to 12 i )12 spines or spurs)Hereditary acanthocytosis (abetalipoproteinemia) Liver diseases (cirrhosis) with dyslipidemia(c os s) t dys p de aAs a part of artefact, mixed to echinocytes
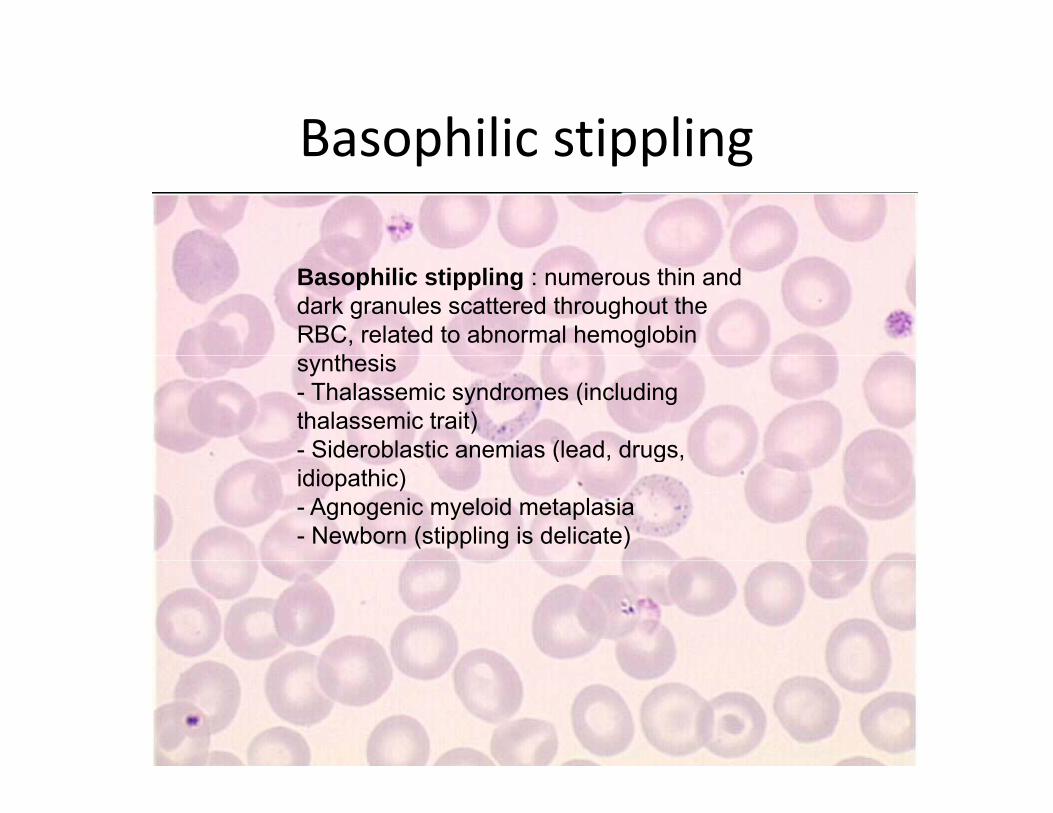
Basophilic stipplingBasophilic stippling
Basophilic stippling : numerous thin and dark granules scattered throughout the RBC, related to abnormal hemoglobin
th isynthesis- Thalassemic syndromes (including thalassemic trait)- Sideroblastic anemias (lead, drugs, ( , g ,idiopathic)- Agnogenic myeloid metaplasia- Newborn (stippling is delicate)
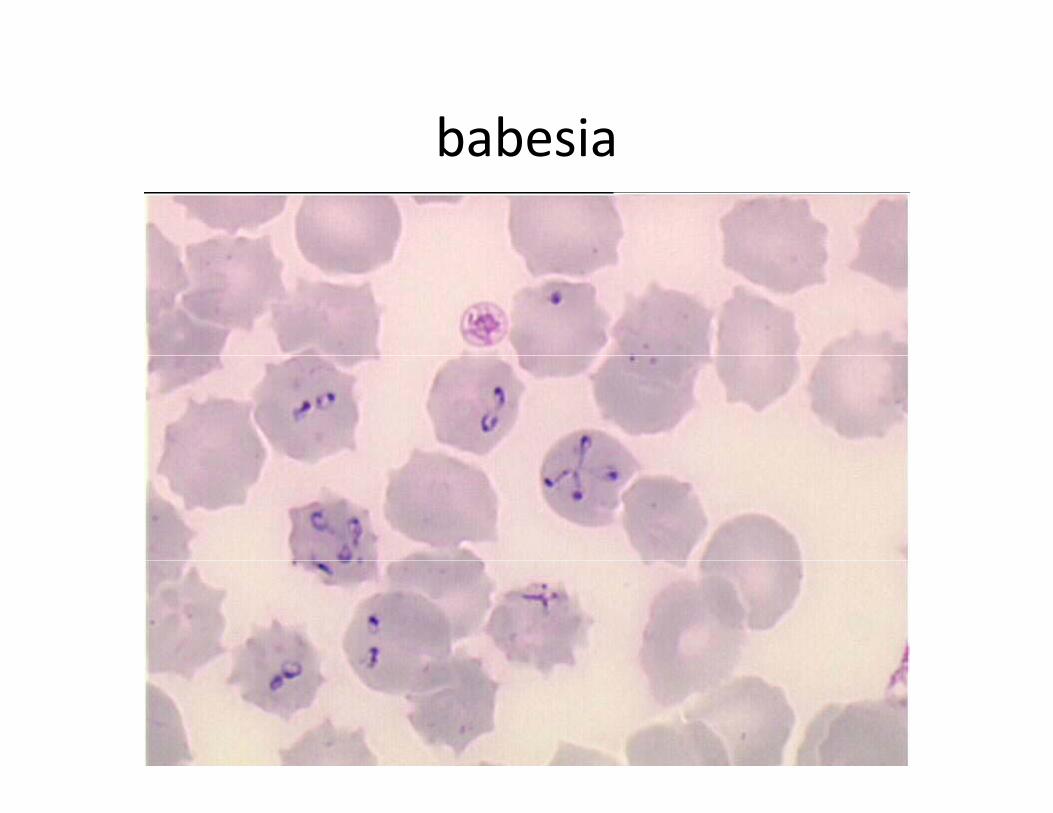
babesiababesia
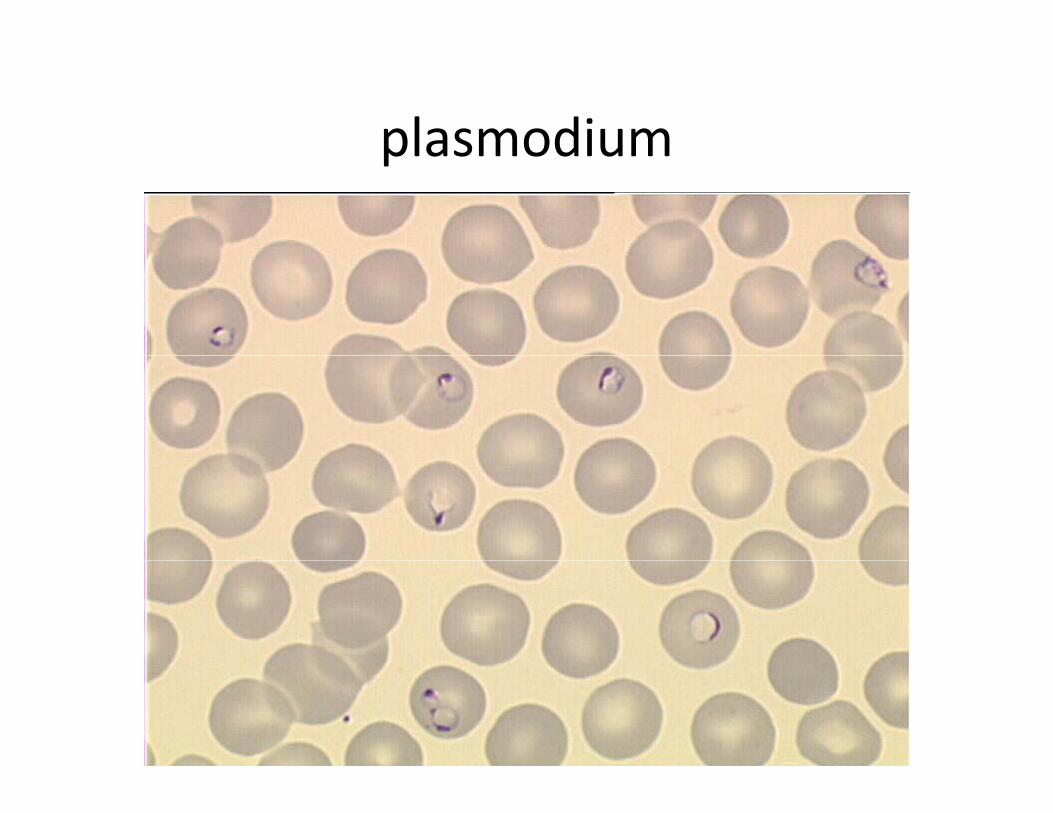
plasmodiumplasmodium
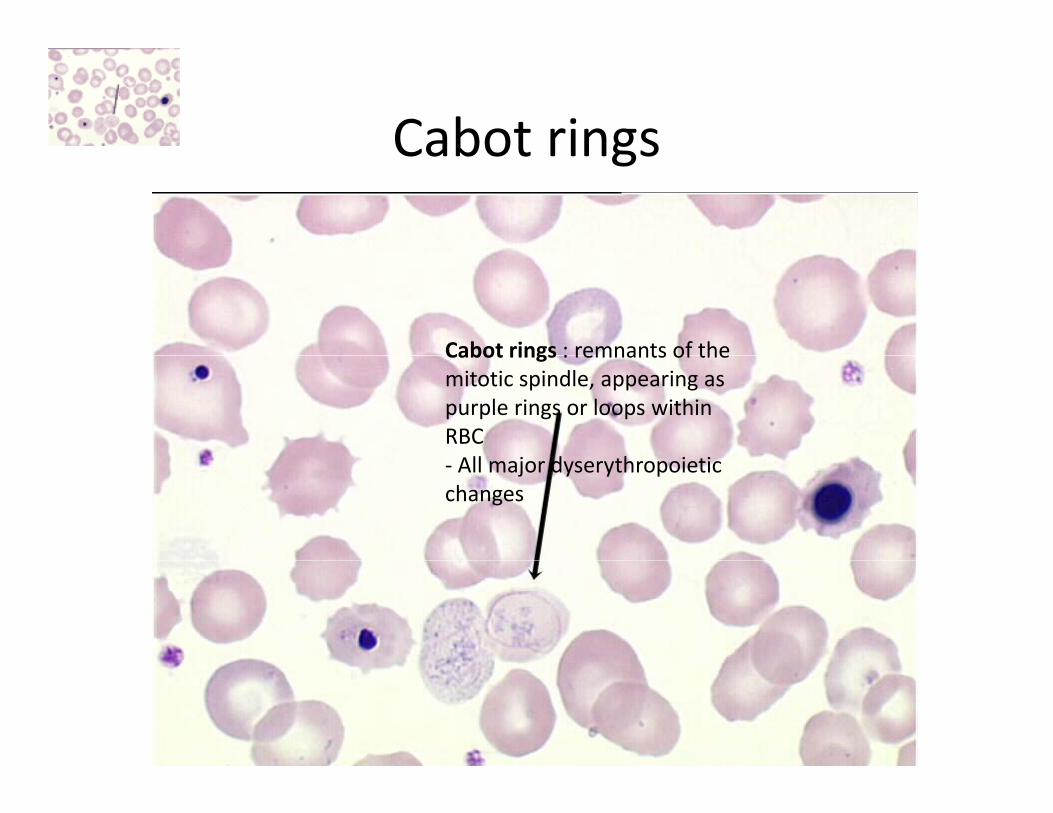
Cabot ringsCabot rings
Cabot rings : remnants of theCabot rings : remnants of the mitotic spindle, appearing as purple rings or loops within RBCAll j d h i i‐ All major dyserythropoietic
changes

Papenheimer bodiesPapenheimer bodies
Pappenheimer bodies : small dark RBC inclusions ; usually one to three within the ; ycell, they are located near the periphery of the cytoplasm- All dyserythropoietic states lead to their production and number may raise sharplyproduction, and number may raise sharply (up to 100% of RBC) in splenectomized or asplenic patients