Embed Size (px)
Citation preview
Making the Church A Safe Place For Victims of Trauma
Philip G. Monroe, PsyDBiblical SeminaryGlobal Trauma Recovery Institute
Objectives
• Identify the common struggles of trauma survivors in faith communities.
• Identify three ways to make churches safer for trauma survivors.
• Learn effective trauma healing support techniques.
[email protected] www.wisecousel.wordpress.com
• If you need a break, take one!• Consider your neighbors when you speak
– Avoid unnecessary trauma details– Remember who may be in the room
Care for yourself and others
What is trauma?
• Overwhelming experience disrupting life as you know it
• Alters view of self, other, and God• Most toxic? Betrayal forms of trauma• Response continues on after event(s)
Anything that exceeds one’s capacity to cope
What is trauma?
More specifically:
Overwhelming experience; demands placed upon the
physiological system that result in a profound felt sense of
vulnerability and/or loss of control
Posttraumatic Stress Disorder
• Traumatic experience• Intrusive symptoms• Attempts to shut down intrusions• Negative feelings about life and
self
Trauma turns complex when:
• Terror goes beyond typical PTSD• Stressors are interpersonal, premeditated,
planned and caused by humans• Stressors are repeated and chronic in
nature• Victims are exploited by “caregivers”
PTSD on steroids: Complex PTSD
• Mood and impulses• Attention and consciousness• Self-perceptions; perceptions of abuser• Relationships• Physical symptoms• Meaning and values
In addition to the conditioned physiological and emotional responses to reminders characteristic of PTSD complexly traumatized children develop a view of the world that incorporates their betrayal and hurt. They anticipate and expect the trauma to recur and respond with hyperactivity, aggression, defeat or freeze responses to minor stresses.
Their cognition is affected by reminders: they tend to become confused, dissociated and disoriented when faced with stressful stimuli. They easily misinterpret events in the direction of a return of trauma and helplessness which causes them to be constantly on guard, frightened and over- reactive. Finally, expectations of a return of the trauma permeate their relationships. This is expressed as negative self-attributions, loss of trust in caretakers and loss of the belief that some somebody will look after them and making feel safe. They tend to lose the expectation that they will be protected and act accordingly. As a result, they organize their relationships around the expectation or prevention of abandonment or victimization. This is expressed as excessive clinging, compliance, oppositional defiance and distrustful behavior, and they may be preoccupied with retribution and revenge
Not Marked list of symptoms
• Sexual problems• Emotional problems• Relational problems• Daily life problems• Health problems• Identity problems
Intense fear, paralysis/helplessness, inability to effect any change, threat of annihilation, leading to experience of,
Loss of voice, control, connection, and meaning, resulting in,
Disorganized physical, cognitive, and emotional response system thereby increasing,
Relational pain, distrust, self-contempt, overwhelming anxiety, evidenced as,
Running from the past…afraid of the future
DepressionAnxiety
Trauma
• Shame– I am dirty.
• Dissociation– Adaptive disconnecting, becomes chronic.
• Relational/emotional dysregulation
Three other consequences of CSA
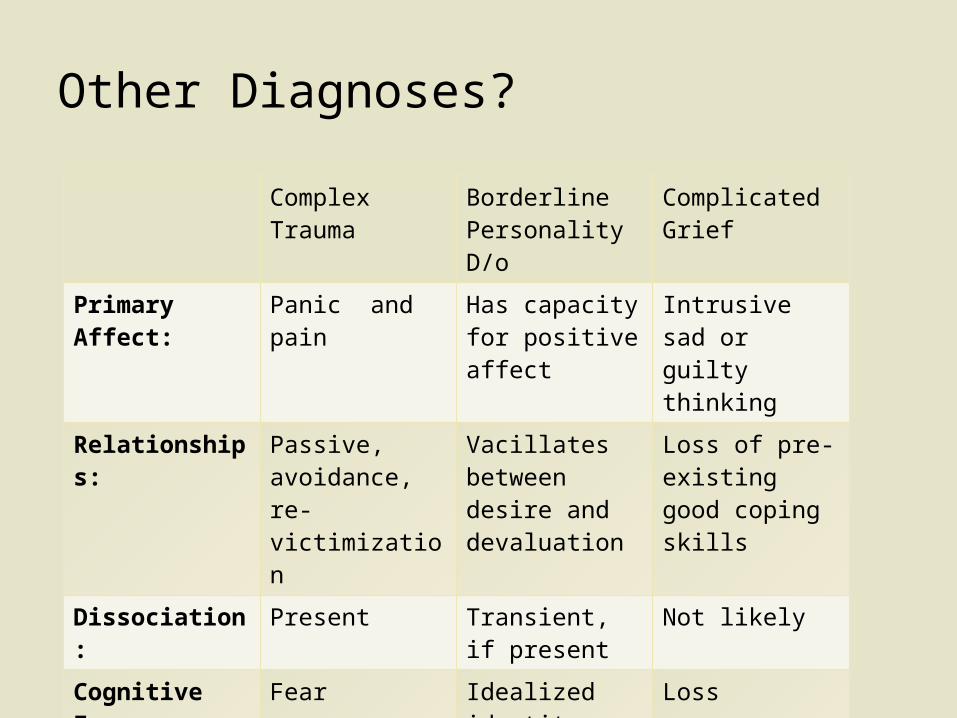
Other Diagnoses?
Complex Trauma
Borderline Personality D/o
Complicated Grief
Primary Affect: Panic and pain Has capacity for positive affect
Intrusive sad or guilty thinking
Relationships: Passive, avoidance, re-victimization
Vacillates between desire and devaluation
Loss of pre-existing good coping skills
Dissociation: Present Transient, if present
Not likely
Cognitive Focus:
Fear Idealized identity
Loss
Self: Consistent self loathing
Confused Compare/ contrast with self prior to loss
• When you hear these real impacts– Where does your mind go?
• Self-blaming?• Hopelessness?
Reflect:
• Some numbers– 1:4 women; 1:6 men with sexual assaults– Adverse childhood experiences (ACEs)
• 30% with physical abuse• 12% witnessed domestic violence• 11% with emotional abuse• 20% sexual abuse• PHL receives higher than national average rates
So…how many hidden in your church?
How common is trauma?
CAVEAT: Don’t argue backwards
Don’t assume symptoms predicts abuse!
Correlation Causation
Hint: It has NOTHING to do with the victim.
Secret ingredient to trauma
• Traumatic events do not always lead to traumatic reactions. Only 25-35% end up with traumatic symptoms. Why?
– Social support? Continuing isolation? Community response?
– Active, successful reaction?
Why aren’t MORE traumatized?
Factors involved
• Type and origin of exposure• Age/developmental stage during exposure• Public versus private• Chronicity• Lasting impact• Social support• Other resources and resiliencies• Other vulnerabilities• Individual differences (coping style, cognitive,
temperament)
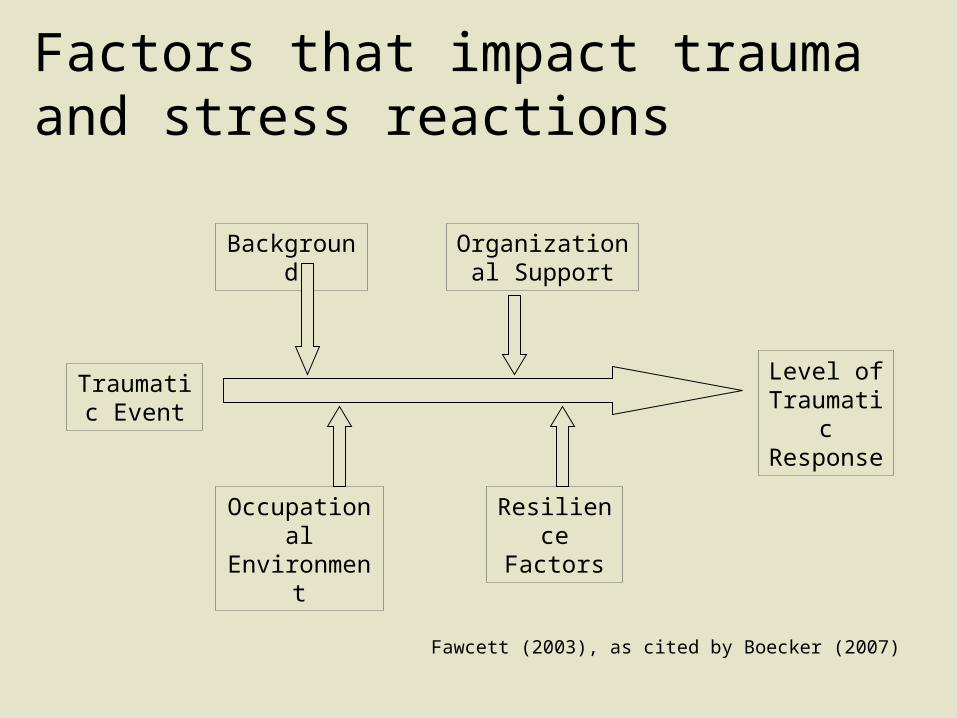
Factors that impact trauma and stress reactions
Fawcett (2003), as cited by Boecker (2007)
Traumatic Event
Organizational Support
Background
Level of Traumatic Response
Resilience Factors
Occupational Environment
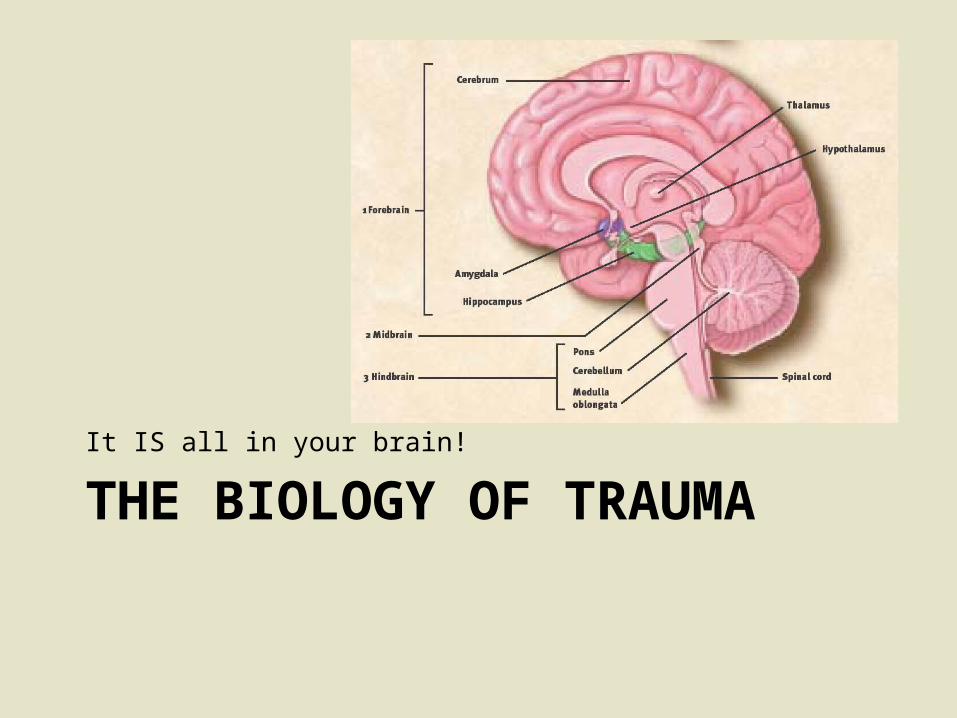
THE BIOLOGY OF TRAUMAIt IS all in your brain!
Your brain is:
• Adaptable• Use-dependent
The brain develops efficient ways to cope with and respond to daily experience!!!
Experience processing• Three types of experience processing
– Cognitive (frontal cortex)– Emotional (limbic systems)– Reactive (brainstem)
• Overactive limbic system (amygdala) seems to shut down prefrontal cortex (used for activation, assessment, etc.)– Disconnects cognition from affect
Prefrontal activity? One study:
• PTSD sufferers showed decreased prefrontal cortex activity when asked to remember or think about former traumatic events.
– Hypothesis: PTSD victims re-experience their trauma rather than recall from their present position.
How the brain responds to memories of trauma:
– Activation of the survival response: • Heightened amygdala and other limbic activity
– Not just a memory--Seeing and feeling• Activation of sensory areas
– Inability to speak:• Decreased activation of Broca’s area
– Emotions are more salient than language:• Marked Rt. hemisphere lateralization
2 overlapping systems
• Amygdala + Hippocampus + Cingulate– Arousal + Evaluate + Decide– Michael Lyles: accelerator, no brakes, no steering
• Hypothalamus + pituitary + adrenal– Cortisol/stress feedback loop
• low cortisol but more frequent “radar” results in overreaction to weak “signals” and no correction back to norm
Impact of chronic stress?
• Excess stress slows– Down-regulation (calming)
• Chronic stress– Immune system breakdown
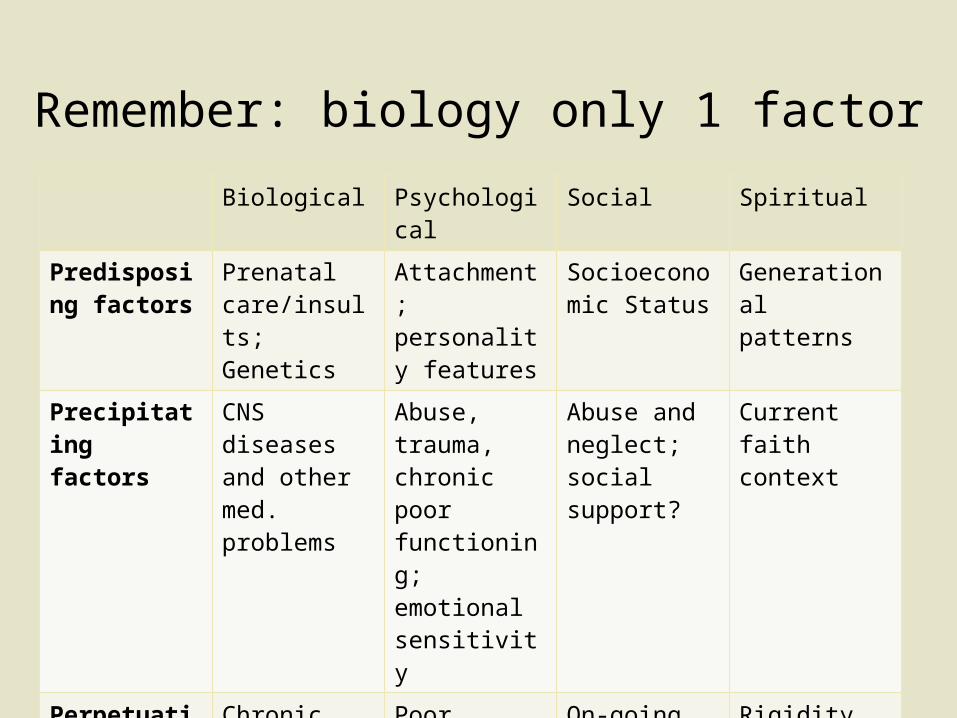
Remember: biology only 1 factor
Biological Psychological Social Spiritual
Predisposing factors
Prenatal care/insults;Genetics
Attachment; personality features
Socioeconomic Status
Generational patterns
Precipitating factors
CNS diseases and other med. problems
Abuse, trauma, chronic poor functioning; emotional sensitivity
Abuse and neglect; social support?
Current faith context
Perpetuating factors
Chronic disease
Poor adjustment to change
On-going lack of resources
Rigidity
Your brain is STILL adaptable and can change!
Remember:
• Military related trauma• Domestic violence
What about job-loss, mis-carriage, adoption?
One note about other traumas
THE CHURCH AS THREATTo Traumatized Parishioners
What are the dangers of having invisible wounds in the church?
Question:
• Trust given to authority• Culture of intimate sharing• Beloved narratives
– Redemption and restoration– Suffering well– Changed lines
Normal expectations in church?
• Spiritual forms of abuse– Prayer manipulation– Bible used to condone victimization or silence– Over-focus on sex and family ideals– “Get over it” theology
When the church hurts victims
AGENTS OF HEALING IN THE CHURCH
Leaders, Parishioners, & Counselors
Church as Refuge
• Teaching– Normalize brokenness
• Speak about shame but also “beauty for ashes”
– Encourage corporate lament– Paint a true picture of restoration
• Highlight courage over idyllic endings• Highlight hope
Leaders setting the foundation
An oppressing spiritual force– Opposes love, the true picture of God and
church– Paints a false picture
• Abuse of power immobilizing fear• Deception moral and relational confusion• Failure to protect chaotic choices• Objectification distorted view of self/bodies• Forced false worship Enslaved to false gods
The spiritual damage of abuse
• Naming evils, oppressions, injustices, losses• Expressing sorrow and despair• Asking God to act• Waiting/entrusting oneself to God
Lament as worship
• Offender repentance? Accountability?
• Forgiveness?
• Restoration and reconciliation?
True picture of restoration
• Honest admission• Sacrificial efforts to repair• Accepts and requires discipline/accountability
True Repentance?
• Policy development– prevention policies; train– response policies to abuse/violence– Engagement with mental health services
Leaders setting the foundation
• Train– Lay care teams to support and encourage victims
and their families
Leaders setting the foundation
• Listen and learn– Be a student more than a teacher!
• Understand what encourages safety
– Bear witness• Identify losses and resiliencies
Individual efforts for change
• Don’t talk too much, become pushy• Watch out for rubber-necking
– But don’t avoid difficult subjects• Pay attention to your body language• Validate• Use question to keep the conversation going• Listen at 3 levels
Counselor 101 skills
• Validating• Not looking for an
explanation
Listening means
• Safe, predictable boundaries heal• Avoid all control or coercion• Speak the truth• Allow for brokenness• Notice incremental change
Remember!
• Validate (again)• Gentle reframes
– Ex: Noting all/nothing thinking– Ex: Finding the good without discounting the bad
• Validate (again)
When you do speak
– Medications?– Counseling models?
• Safety memory processing reconnection
– Counseling interventions• Mindfulness; narrative work; Exposure
desensitization response change
Understand their therapies
• Awareness of the moment• Focus on being (vs. doing and reacting)• Waking up from life on automatic• Non-judgmental attitude
What is mindfulness?
• Intention, attention, attitude• Not grasping at judgments• Observing, noticing, describing, labeling• Attending to sensations; Acting with
awareness
Mindful activities
• Naming the rumination; accepting• Focusing on the present with senses• Repeating a verse• “What do you want me to be doing in the next
5 minutes?”
What might it look like?
• Increased patience, decreased stress response
• Processing of emotions• Present rather than withdrawing• Increases curiosity, openness, acceptance
and love
Benefits?
Narrative work: Good story telling•Tells story at own pace, no pressure•Chooses when not to tell a part of the story•Listener silence and body language to show interest•Storytelling without words•Difficult stories start and end at safe points•Good coping skills before starting story telling•Notes resiliency and strength in the midst of trauma•Story told from the present rather than reliving the story
• Frequent interruptions• Forcing the story• Reliving the story• Avoiding painful emotions• Exhorting the person to get over
the feelings; telling them how to feel
• Only talking about the trauma, ignoring strengths and other history
• Ending a session without talking about the present or a safe place
– Fishing for memories– Re-birthing– Imagery and some forms of healing prayer– Enmeshed therapists
Recognize dangerous interventions
• Friend, support, prayer partner, ear• Watch out for splitting
Remember your role
• Does the heavy lifting of therapy• Encourages healthy boundaries and safe
spaces• Collaborative efforts/goals• Teaches/trains lay helpers• Gives voice to common pit-falls and
roadblocks
Counselors as agents of change
• Distancing from the church and other social supports; Criticizing lay efforts
• Assuming church is healthy• Forgetting permission to collaborate• Failing to connect trauma and faith
First, some pit-falls of our own
• Advise clients how to use their voice; give space for making choices
• Increase empathy for self and other (orgs) for failings and disconnects
• Avoid all/nothing responses to faith/church
Support the client voice
• Find mutual goals where possible• Identify how counseling fits into big picture• Speak the native language!• Be gentle with errors
With permission…engage leaders
Remember to listen first!
• Be willing to consult and encourage leaders• Be willing to teach on counseling topics• Connect trauma recovery to faith
Give back to the church
SARAA Case Study of a 27 year old married woman
• Abused at 5 by uncle• Abused as teen by brother• Marries at 18• Involved at conservative hierarchical church• Marital sex problems• Self-despising; distrustful
Her history
• Church leader helps?• Lay supporter helps• Counselor helps?• Collaborative efforts?
Making church safe?
• The Long Journey Home (Schmutzer, A. ed.)• Counseling Survivors of Sexual Abuse; • On the Threshold of Hope (Langberg)
– Group workbook now available• Rid of My Disgrace (Holcomb)
Book resources:
• www.dianelangberg.com• www.globaltraumarecovery.org
– Free videos by Diane Langberg on abuse, trauma, and narcissistic systems and leaders
• www.netgrace.org
Web resources:





























