Embed Size (px)
Citation preview
Make sure you’ve got the right bus driver and the “right people on the bus”.
-Jim Collins
Good to Great
Dr. Robert Laskowski, President & CEO sends his greetings to the attendees, and he wants everyone to know that he strongly believes that effective leadership & teamwork matters “a whole bunch”.
Quality leadership always leads to better quality outcomes.
What we have in common with other healthcare systems & hospitals
Physician practices & Private physician issues Increasing organizational complexity Credential vertically & practice horizontally Limited sources of profitability Increasing costs, competition, quality & pt. safety stds Ongoing capacity challenges Residency review committee rules & regs Sustaining viable research funding & structure
What is quality health care & safety?
Care that maximizes the probability of desired outcomes– Effective, efficient, timely, patient-centered,
equitable, and safe
Absence of complicationsRef: Alex Hover, MD, FACP (CareScience)
DOING THE RIGHT THING RIGHT! Patient Safety – 1st Do No Harm!
“Hospitals & Physicians more aware of “Public Reporting” on Quality & Safety
Government & other– CMS, AHRQ, NQF, State…
Regulatory Agencies– JCAHO, CMS…
Purchasing Consortia– Leapfrog, NBCH…
HIT Companies– CareScience, HealthGrades..
Lay Press– US News & World Report…
Objectives & targets differ ● Some agreement on best & worst ● Poor overall agreement ● Aren’t changing patients’ behavior-yet
List of National Report Card Agencies
• JCAHO – EB meds/procedures & safety
• CMS – EB meds/procedures & safety
• Leapfrog – EB systems/practices, M & M
• US News & World Report – Reputation, AHA survey data, M & M
• Solucient – M & M and Operating Margin
• Healthgrades – M & M for specific surgical procedures and diseases
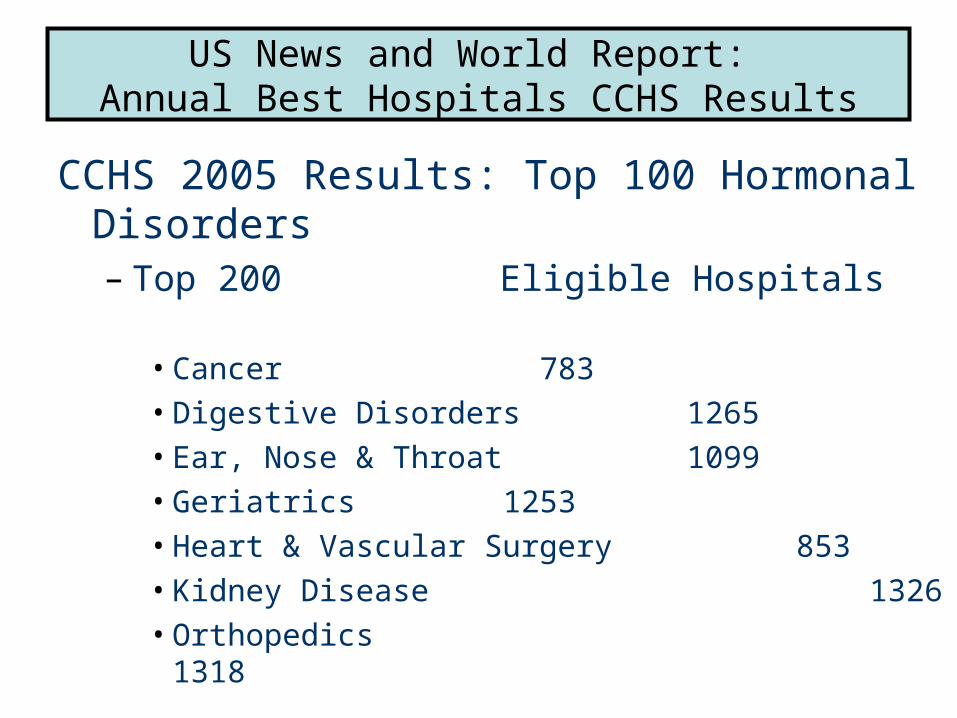
US News and World Report: Annual Best Hospitals CCHS Results
CCHS 2005 Results: Top 100 Hormonal Disorders– Top 200 Eligible Hospitals
• Cancer 783 • Digestive Disorders 1265 • Ear, Nose & Throat 1099• Geriatrics 1253• Heart & Vascular Surgery 853• Kidney Disease 1326• Orthopedics 1318
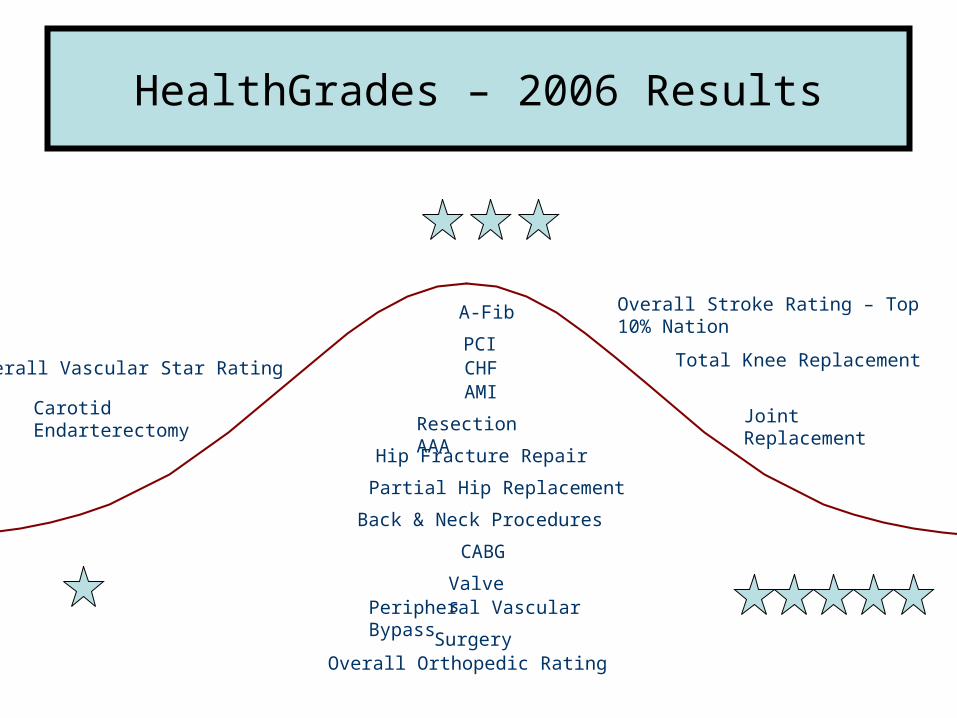
HealthGrades – 2006 Results
Total Knee Replacement
Joint Replacement
Partial Hip Replacement
Hip Fracture Repair
Back & Neck Procedures
SurgeryOverall Orthopedic Rating
Resection AAA
Carotid Endarterectomy
Peripheral Vascular Bypass
Overall Vascular Star Rating
Overall Stroke Rating – Top 10% Nation
CABG
Valves
PCI
AMICHF
A-Fib
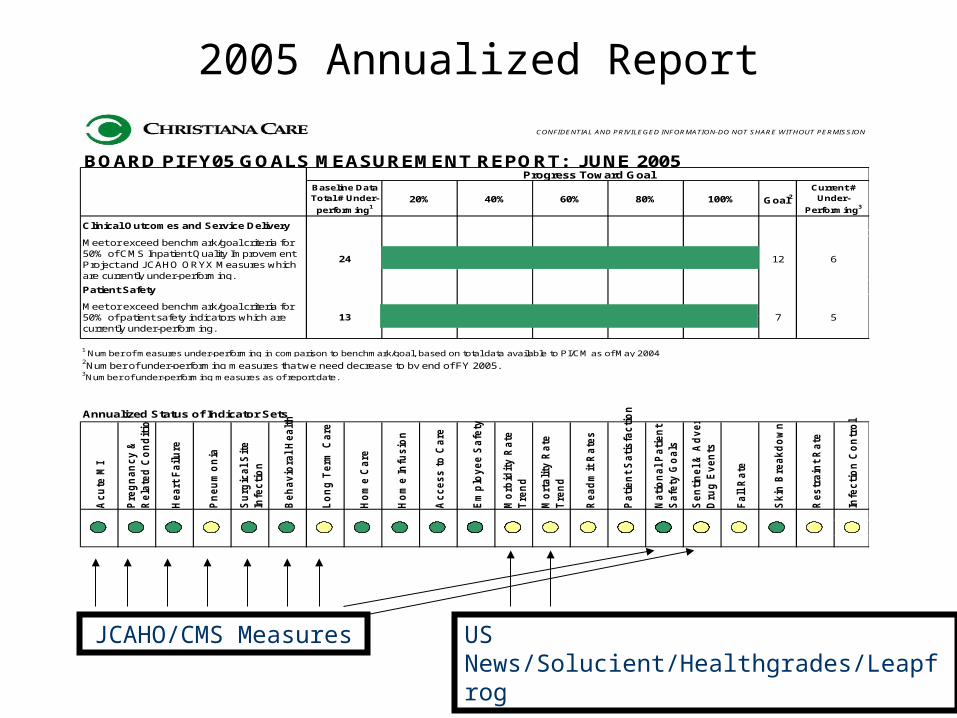
2005 Annualized ReportCONFIDENTIAL AND PRIVILEGED INFORMATION-DO NOT SHARE WITHOUT PERMISSION
BOARD PI FY05 GOALS MEASUREMENT REPORT: JUNE 2005
Goal2
Clinical Outcomes and Service Delivery
Patient Safety
1 Number of measures under-performing in comparison to benchmark/goal, based on total data available to PI/CM as of May 2004 2Number of under-performing measures that we need decrease to by end of FY 2005.3Number of under-performing measures as of report date.
Annualized Status of Indicator Sets
Acu
te M
I
Pre
gn
an
cy &
Rela
ted
Co
nd
itio
ns
Heart
Failu
re
Pn
eu
mo
nia
Su
rgic
al S
ite
Infe
cti
on
Beh
av
iora
l H
ealt
h
Lo
ng
Term
Care
Ho
me C
are
Ho
me In
fusio
n
Acce
ss t
o C
are
Em
plo
ye
e S
afe
ty
Mo
rbid
ity R
ate
Tre
nd
Mo
rtali
ty R
ate
Tre
nd
Read
mit
Rate
s
Pati
en
t S
ati
sfa
cti
on
Nati
on
al P
ati
en
t
Safe
ty G
oa
ls
Sen
tin
el
& A
dvers
e
Dru
g E
ven
ts
Fall R
ate
Skin
Bre
akd
ow
n
Restr
ain
t R
ate
Infe
cti
on
Co
ntr
ol
Meet or exceed benchmark/goal criteria for 50% of CMS Inpatient Quality Improvement Project and JCAHO ORYX Measures which are currently under-performing.
Meet or exceed benchmark/goal criteria for 50% of patient safety indicators which are currently under-performing.
60% 80%
13
24
Baseline DataTotal # Under-
performing1
Progress Toward Goal
612
20% 40% 100%
57
Current # Under-
Performing3
US News/Solucient/Healthgrades/LeapfrogJCAHO/CMS Measures
Performance Improvement: Major Areas of Activities – Proactive & Reactive
Patient Safety– Sentinel Events, FMEA– JCAHO Patient Safety Goals– AHRQ Safety Plan– Leapfrog compliance (ICU, eICU)– IHI’s Rapid Response Teams
Accreditation Compliance– JCAHO, NCQA, CMS– ACS – Trauma – Cancer
Improving Care Delivery– Guideline & PI Teams– Staff Competency & JCAHO Standards
Quality/Performance Measures– CMS/JCAHO, Patient Safety, Clinical Registries
Example – Sentinel Event - Leadership at all levels involved
Fire in the EP Cath Lab – patient with significant burns on chest, face, airway was transferred to Crozer’s Burn Unit
Family support by Patient Relations Dept. Staff support by Psych Crisis Team Duraprep immediately suspended from use Root Cause Team convened Tool to identify fire risk and other risk reduction strategies
developed & implemented Outside consultant trained over 400 staff members
Patient Safety – Failure Mode & Effects Analysis
Proactive analysis and improvement of high risk procedures and processes, examples include:
Response to ventilator alarms Telephone system failure Prevention of patient elopement in LTC Patients at risk for suicide or harm in non-psychiatric
settings
Improving Care Delivery – Standards of Care
Continuous review of clinical, performance improvement and patient safety literature to identify what improves care and outcomes
Feedback from Medical Staff and other clinical staff leaders in all areas on new and tested ways to improve care delivery and outcomes
Leapfrog/CMS/JCAHO and others driving to standardize care delivery nationally
Improving Care Delivery – Example Development of Sepsis Protocol
USA sepsis mortality = 30 -50%; CCHS = 26% International Sepsis Forum published treatment
guidelines a few months ago – reduces mortality rates by 25-50%
Interdisciplinary Team formed at CCHS to develop implementation plan
Protocol focuses on antibiotics/fluids within 1 hour of presenting in the ED or diagnosis on a Nursing Unit
CCHS implemented “Sepsis Alert Protocol” Compliance with protocol & M & M rates—tracked
Performance Measurements in as close to real time as possible
Twenty databases utilized for benchmarking Clinical areas – detailed benchmark data Results publicly available
– CMS– JCAHO– Leapfrog– Healthgrades– US News & World Report
KEEP IT SIMPLE…MAKE SURE IT’S USEFUL INFORMATION
Chief Medical Officer: Primary Function at CCHS
The CMO as the leader of the Medical Affairs functions, will have responsibility for strategic planning, clinical services, quality, professional performance, business performance, medical education, clinical research and physician practice and network development. As part of the Sr. Exec. Team, the CMO participates in the development of system-wide medical & administrative policies and procedures, acts as liaison between the medical staff, Sr. Mgmt, Board of Directors, and reports directly to the President & CEO.
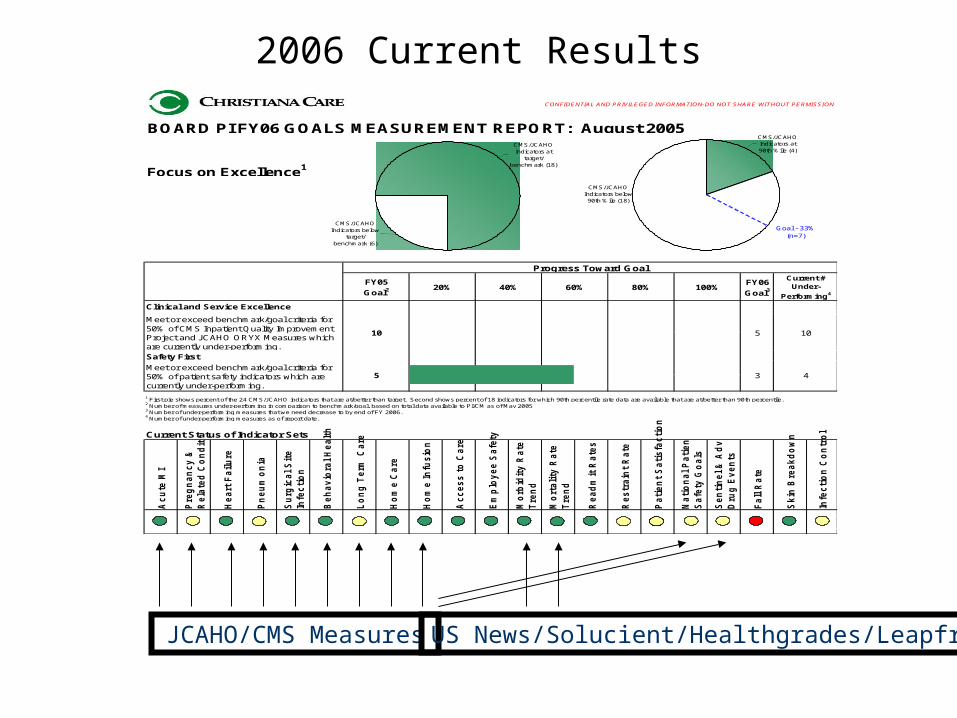
2006 Current ResultsCONFIDENTIAL AND PRIVILEGED INFORMATION-DO NOT SHARE WITHOUT PERMISSION
BOARD PI FY06 GOALS MEASUREMENT REPORT: August 2005
Focus on Excellence1
FY06
Goal3
Clinical and Service Excellence
Safety First
Current Status of Indicator Sets
Acu
te M
I
Pre
gn
an
cy &
Rela
ted
Co
nd
itio
ns
Heart
Failu
re
Pn
eu
mo
nia
Su
rgic
al S
ite
Infe
cti
on
Beh
avio
ral H
ealt
h
Lo
ng
Term
Care
Ho
me C
are
Ho
me In
fusio
n
Acce
ss t
o C
are
Em
plo
ye
e S
afe
ty
Mo
rbid
ity R
ate
Tre
nd
Mo
rtali
ty R
ate
Tre
nd
Read
mit
Rate
s
Restr
ain
t R
ate
Pati
en
t S
ati
sfa
cti
on
Nati
on
al P
ati
en
t
Safe
ty G
oa
ls
Sen
tin
el
& A
dvers
e
Dru
g E
ven
ts
Fall R
ate
Skin
Bre
akd
ow
n
Infe
cti
on
Co
ntr
ol
2 Number of measures under-performing in comparison to benchmark/goal, based on total data available to PI/CM as of May 2005 3 Number of under-performing measures that we need decrease to by end of FY 2006.4 Number of under-performing measures as of report date.
1 First pie shows percent of the 24 CMS/JCAHO indicators that are at/better than target. Second shows percent of 18 indicators for which 90th percentile rate data are available that are at/better than 90th percentile.
Meet or exceed benchmark/goal criteria for 50% of CMS Inpatient Quality Improvement Project and JCAHO ORYX Measures which are currently under-performing.
Meet or exceed benchmark/goal criteria for 50% of patient safety indicators which are currently under-performing.
60% 80%
5
10
FY05
Goal2
Progress Toward Goal
105
20% 40% 100%
43
Current # Under-
Performing4
CMS/JCAHO Indicators below 90th %ile (18)
CMS/JCAHO Indicators at 90th %ile (4)
Goal - 33%(n=7)
CMS/JCAHO Indicators below
target/ benchmark (6)
CMS/JCAHO Indicators at
target/ benchmark (18)
JCAHO/CMS Measures US News/Solucient/Healthgrades/Leapfrog
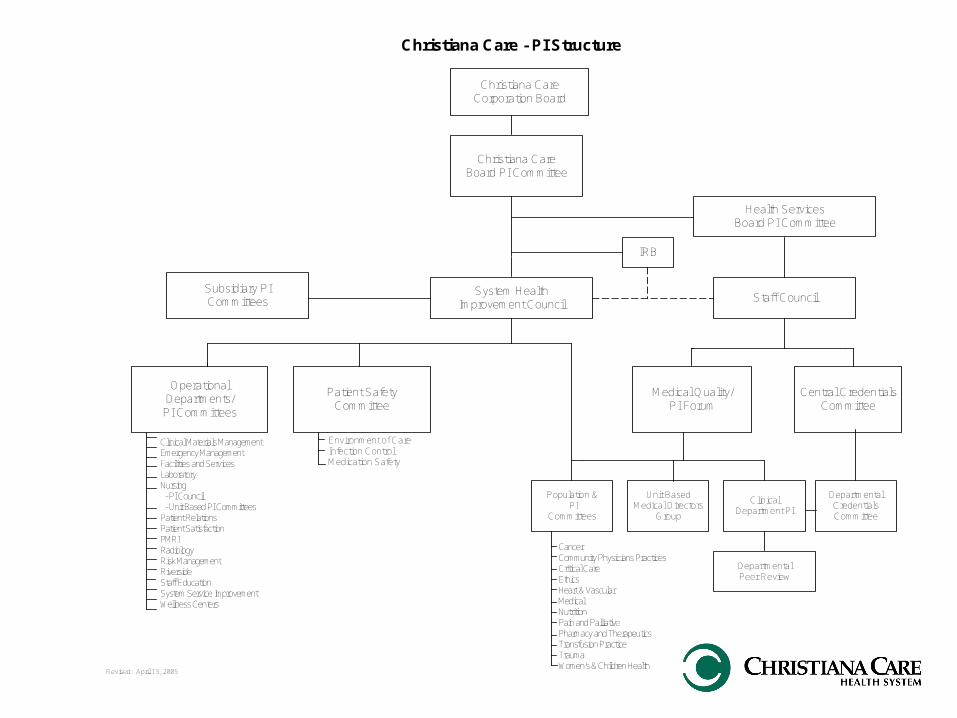
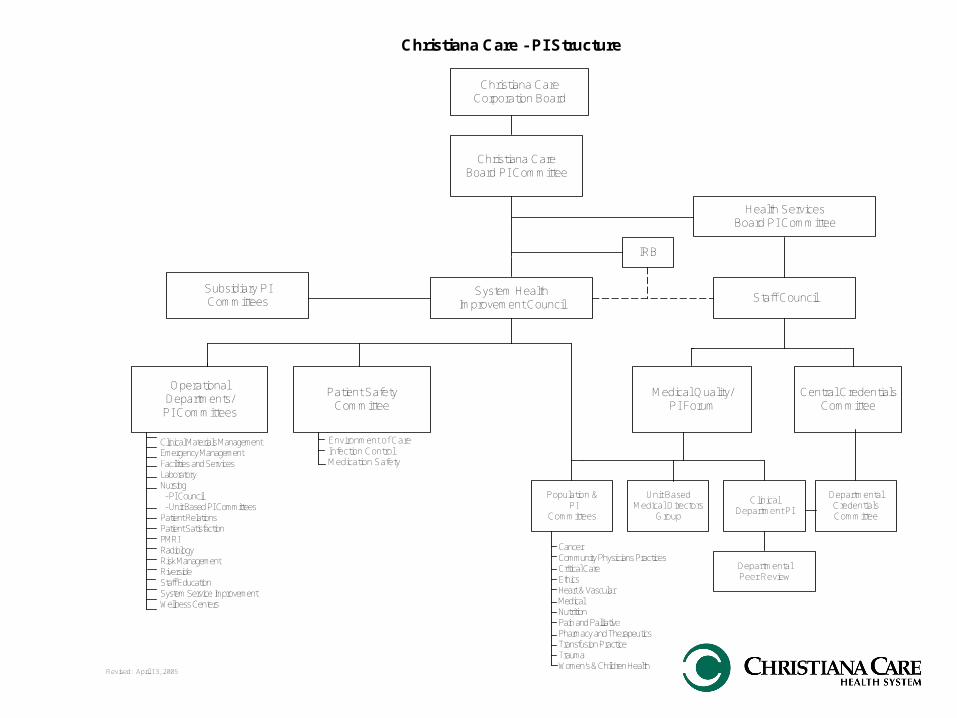
Christiana CareCorporation Board
System HealthImprovement Council
Christiana CareBoard PI Committee
CancerCommunity Physicians PracticesCritical CareEthicsHeart & VascularMedicalNutritionPain and PalliativePharmacy and TherapeuticsTransfusion PracticeTraumaWomen's & Children Health
Christiana Care - PI Structure
OperationalDepartments/PI Committees
Medical Quality/PI Forum
Central CredentialsCommittee
DepartmentalCredentialsCommittee
Staff CouncilSubsidiary PICommittees
Health ServicesBoard PI Committee
ClinicalDepartment PI
DepartmentalPeer Review
Population & PI
Committees
Unit BasedMedical Directors
Group
Patient SafetyCommittee
Clinical Materials ManagementEmergency ManagementFacilities and ServicesLaboratoryNursing - PI Council - Unit Based PI CommitteesPatient RelationsPatient SatisfactionPMRIRadiologyRisk ManagementRiversideStaff EducationSystem Service ImprovementWellness Centers
Environment of CareInfection ControlMedication Safety
IRB
Revised: April 13, 2005
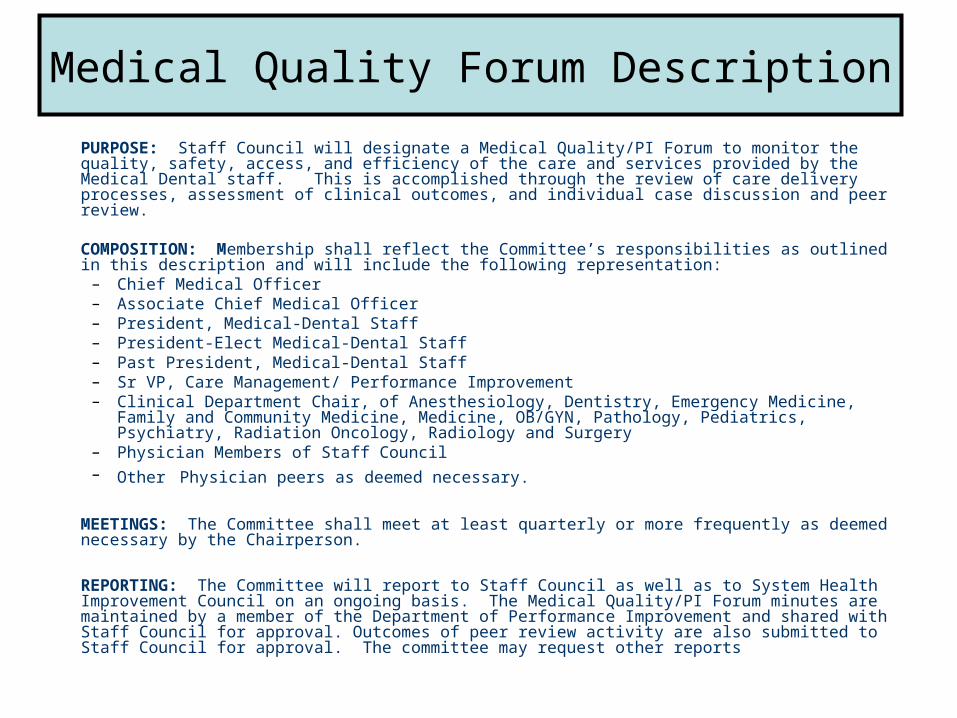
PURPOSE: Staff Council will designate a Medical Quality/PI Forum to monitor the quality, safety, access, and efficiency of the care and services provided by the Medical Dental staff. This is accomplished through the review of care delivery processes, assessment of clinical outcomes, and individual case discussion and peer review.
COMPOSITION: Membership shall reflect the Committee’s responsibilities as outlined in this description and will include the following representation:
– Chief Medical Officer– Associate Chief Medical Officer– President, Medical-Dental Staff – President-Elect Medical-Dental Staff– Past President, Medical-Dental Staff– Sr VP, Care Management/ Performance Improvement– Clinical Department Chair, of Anesthesiology, Dentistry, Emergency Medicine, Family and
Community Medicine, Medicine, OB/GYN, Pathology, Pediatrics, Psychiatry, Radiation Oncology, Radiology and Surgery
– Physician Members of Staff Council– Other Physician peers as deemed necessary.
MEETINGS: The Committee shall meet at least quarterly or more frequently as deemed necessary by the Chairperson.
REPORTING: The Committee will report to Staff Council as well as to System Health Improvement Council on an ongoing basis. The Medical Quality/PI Forum minutes are maintained by a member of the Department of Performance Improvement and shared with Staff Council for approval. Outcomes of peer review activity are also submitted to Staff Council for approval. The committee may request other reports
Medical Quality Forum Description
Give Information—not just data, and make it personal
ACUTE MI: By Dept, Section, & Group D/Cs LOS $Tot Chgs Severity AMI
CompCCHSFMMedSurgCardIMGrp 1Grp 2
Christiana CareCorporation Board
System HealthImprovement Council
Christiana CareBoard PI Committee
CancerCommunity Physicians PracticesCritical CareEthicsHeart & VascularMedicalNutritionPain and PalliativePharmacy and TherapeuticsTransfusion PracticeTraumaWomen's & Children Health
Christiana Care - PI Structure
OperationalDepartments/PI Committees
Medical Quality/PI Forum
Central CredentialsCommittee
DepartmentalCredentialsCommittee
Staff CouncilSubsidiary PICommittees
Health ServicesBoard PI Committee
ClinicalDepartment PI
DepartmentalPeer Review
Population & PI
Committees
Unit BasedMedical Directors
Group
Patient SafetyCommittee
Clinical Materials ManagementEmergency ManagementFacilities and ServicesLaboratoryNursing - PI Council - Unit Based PI CommitteesPatient RelationsPatient SatisfactionPMRIRadiologyRisk ManagementRiversideStaff EducationSystem Service ImprovementWellness Centers
Environment of CareInfection ControlMedication Safety
IRB
Revised: April 13, 2005
Unit Based Medical DirectorsPhysicians & Nurses Working as a Team
Communication & Engagement
– Vital to success of the program
100% participation is necessary– Monthly Meeting– Monthly Summary Report
UNIT BASED MEDICAL DIRECTOR MONTHLY REPORT(TO BE COMPLETED IF YOU ARE UNABLE TO ATTEND THE MONTHLY MEETING)
1) Nursing Unit rounding and support.Unit-based operational issues and clinical issues addressed this month:
2) Involvement in PI/Patient Safety initiatives on the unit.
PI/Patient Safety activities addressed this month:
3) Educational sessions for the nursing/ancillary staff.
Monthly didactic program provided:
Unit Based Medical Director Evaluation Summary
• Rounds/Operational Issues – Average score – 2.4 (out of 3.0)
• PI/Patient Safety Activities– Average score – 2.2 (out of 3.0)
• Monthly Didactic Education– Average score – 1.8 (out of 1.8)
Monthly didactic education – lowest score
Scores < 2 are unacceptable

- Safety First
- Great Place to Work
- Clinical Service Excellence
-Think of Yourself as the Patient
Dr. Robert Laskowski, President & CEO trusts that everyone is a believer that leadership, quality, safety, and teamwork matter “a whole bunch”!
Focus on Excellence is the CCHS way.
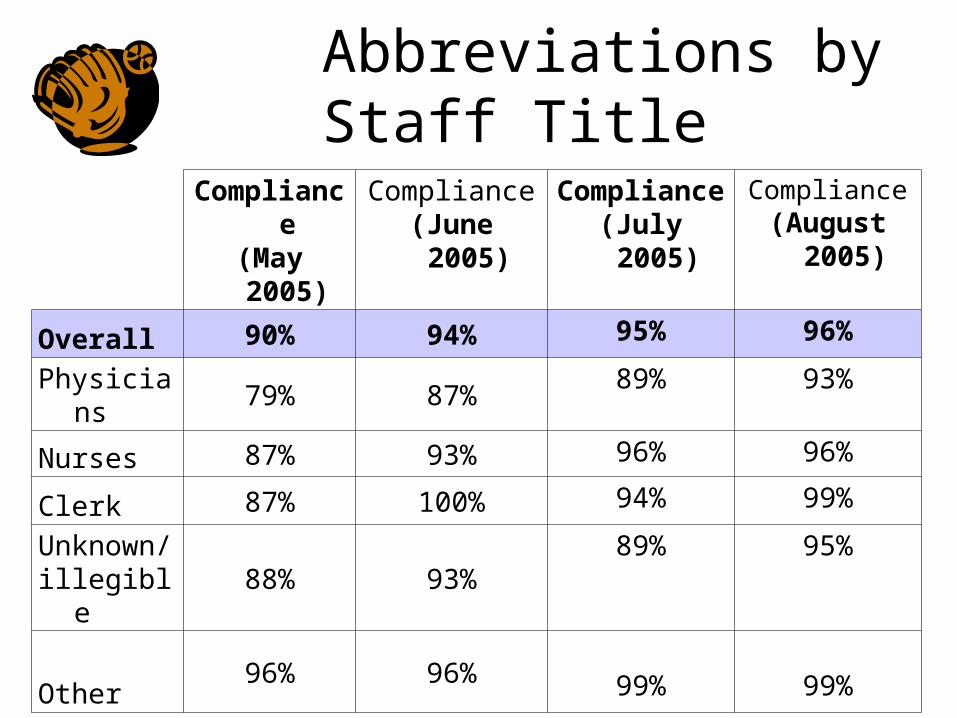
Abbreviations by Staff Title
Compliance(May 2005)
Compliance(June 2005)
Compliance(July 2005)
Compliance(August
2005)
Overall 90% 94% 95% 96%
Physicians 79% 87% 89% 93%
Nurses 87% 93% 96% 96%
Clerk 87% 100% 94% 99%
Unknown/illegible
88% 93%89% 95%
Other96% 96% 99% 99%
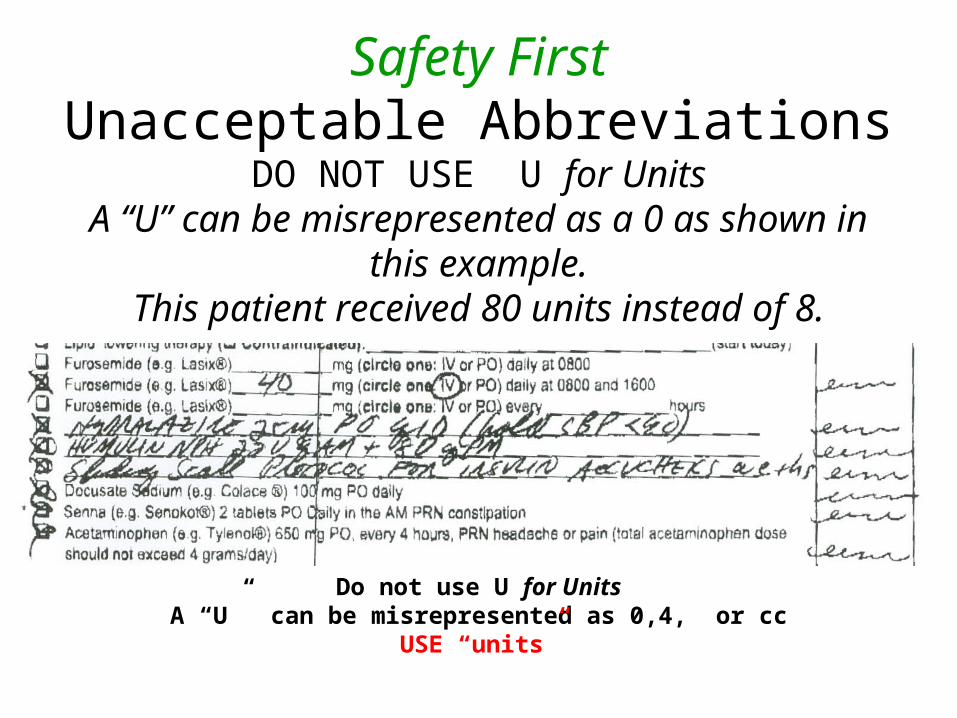
Safety FirstUnacceptable Abbreviations
DO NOT USE U for UnitsA “U” can be misrepresented as a 0 as shown in
this example.This patient received 80 units instead of 8.
Do not use U for UnitsA “U” can be misrepresented as 0,4, or cc
USE “units”
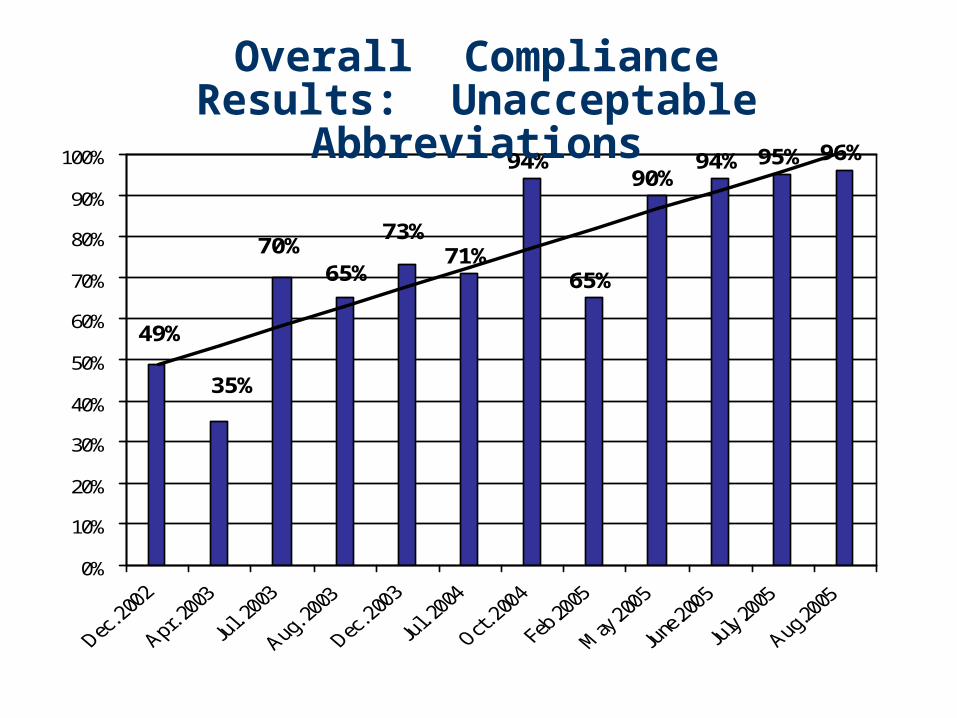
71%
94%
65%
90%94% 95% 96%
73%
65%70%
35%
49%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Overall Compliance Results: Unacceptable Abbreviations
Summary
Effective Leadership Skills Can Be Learned Invest in Leadership and Choose Your Medical Staff
Leaders Carefully Manage Relationships Keep Things as Simple and as Focused as Possible
– Results Orientated, Peered & Personal in real time National Report Cards (e.g., JCAHO) are useful
measures of what should already be being done Stay Positive and Have Fun!!
Questions & Comments










![BUS BUS BUS BUS BUS BUS BUS BUS BUS · Sunday 15 May 2016 Liverpool Street to Colchester, Ipswich, Norwich and branches BUS BUS BUS BUS BUS BUS BUS BUS BUS] 1 1 1 1 1 1 1 1 1 1 1](https://img.pdfslide.us/doc/110x75/5fab4ce2477d2d3adf21016a/bus-bus-bus-bus-bus-bus-bus-bus-sunday-15-may-2016-liverpool-street-to-colchester.jpg)