Embed Size (px)
Citation preview
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Recommendations of an Expert Panel
This activity is supported by an educational grant from Healthpoint.
This activity is sponsored by the North American Center for Continuing Medical Education.
June 2008 Supplement
Healthpoint Debrid Supp OWM 6/17/08 4:16 PM Page 1
Falanga.qxd 6/17/08 4:59 PM Page 8
Continuing EducationCompletion Time:Estimated time to complete this complimentary activity is 1 hour.Target Audience:Physicians and nurses who treat patients with woundsLearning Objectives:Upon completion of this educational activity, participants shouldbe able to:
• Describe the range of clinical and biological abnormalitiesin the wound bed that can inhibit wound healing
• Define initial and maintenance debridement and describethe primary goals of each
• Discuss the scientific and clinical rationale for initial andmaintenance debridement
• Name two tools that can be used to assess the adequacyof debridement and wound bed preparation in general
• Describe how to implement debridement within the con-text of an effective wound care strategy
• List several different methods of debridement.Method of Participation:Participants must read the journal supplement then take, submit,and pass the post-test by June 30, 2009. Participants must com-pletely fill out the answer/evaluation form and mail theanswer/evaluation form to NACCME at 83 General Warren Blvd.,Suite 100, Malvern, PA 19355 or fax it to 610-560-0502. Within60 days, the participant will be advised of passing or failing theexam. A score of or above 70% will comprise a passing grade. Acertificate will be awarded to participants who successfully com-plete the exam.Accreditation:MD/DO: This activity is sponsored by the North American Centerfor Continuing Medical Education (NACCME). NACCME isaccredited by the Accreditation Council for Continuing MedicalEducation to provide continuing medical education for physi-cians. NACCME designates this educational activity for a maxi-mum of 1 AMA PRA Category 1 Credit™. Physicians should onlyclaim credit commensurate with the extent of their participationin the activity. This activity has been planned and produced inaccordance with the ACCME Essential Areas and Policies.Nurses: ANCC: NACCME is an approved provider of continuingnursing education by the Pennsylvania State Nurses Association,an accredited approver by the American Nurses CredentialingCenter’s Commission on Accreditation. This continuing nursingeducation activity was approved by the PA State NursesAssociation for 1 contact hour (Provider Number 110-3-E-06).Provider approved by the California Board of Registered Nursing,Provider Number 13255, for 1 contact hour.Off-Label/Unapproved Usage Disclosure:This educational activity contains discussion of published and/orinvestigational uses of agents that are not indicated by the FDA.
NACCME does not recommend the use of any agent outside ofthe labeled indications. Please refer to the official prescribinginformation for each product for discussion of approved indica-tions, contraindications, and warnings.Faculty Disclosures:All those with control over the content of continuing educationprograms sponsored by NACCME are expected to disclosewhether they do or do not have any real or apparent conflict(s)of interest or other relationships related to the content of theirpresentation(s). It is not assumed that these relationships willhave an adverse impact on presentations; they are simply notedhere to fully inform participants.Planner and Faculty: Dr. Falanga has disclosed that he is a con-sultant to Organogenesis.Faculty: Dr. Brem has disclosed that he is a consultant toOrganogenesis. Dr. Ennis has disclosed that he is a consultant toCelleration and Accelecare Wound Centers. Dr.Ayello has disclosedthat she is a consultant to 3M Health Care, Smith & Nephew, Hill-Rom, KCI, IVIVI, Sage, Mölnlycke, Coloplast, and Ross. She is a mem-ber of the speakers’ bureau for Smith & Nephew, KCI, Ross, and Hill-Rom. She has received other financial or material support fromGaymar, Healthpoint, NJHA (3M Health Care, Sage, andHealthpoint), LWW, Hollister, and WUWHS. Dr. Gould has disclosedthat she has received grant/research support and is a scientific advi-sor to Diversified Clinical Services. She is a member of the speakers’bureau for KCI. Dr.Wolcott has disclosed that he has receivedgrant/research support from NIH. He is a member of the speakers’bureau for Cubist and Pfizer.Medical Writer: Amy Lindsay, PhD, has disclosed that she hasno significant financial relationships.Reviewer: Dr. Siegel has disclosed that he has no significantfinancial relationships.Commercial Support: This activity is supported by an educa-tional grant from Healthpoint.Conflict of Interest Resolution/Content Validation:In compliance with ACCME Standards for Commercial Supportand NACCME’s policy and procedure for resolving conflicts ofinterest, this continuing medical education activity was reviewedby Dr. Siegel in June 2008 for clinical content validity and toinsure that the activity’s materials are fair, balanced, and free ofbias toward the commercial supporters of the activity, that activ-ity materials represent a standard of practice within the profes-sion in the United States, and that any studies cited in the mate-rials upon which recommendations are made are scientificallyobjective and conform to research principles generally acceptedby the scientific community.Sponsor: This activity is sponsored by The North AmericanCenter for Continuing Medical Education.Release Date: Expiration Date:June 30, 2008 June 30, 2009
Supplement to OWM June 2008 1
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Falanga.qxd 6/17/08 3:53 PM Page 1
2 Supplement to OWM June 2008
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
IntroductionDifficult-to-heal and chronic
wounds, such as venous, diabetic, pres-sure, and arterial insufficiency ulcers,affect millions of people in the UnitedStates. Several reviews ofincidence/prevalence studies have beenpublished.Venous ulcers are estimatedto affect approximately 2.5 millionpeople in the United States.1,2
Approximately 6% (0.882 to 1.2 mil-lion) of the 14.7 to 20 million peoplewith diabetes in the United States areat risk of developing diabetic neuro-pathic ulcers over any given 3-yearperiod.3,4 Pressure ulcers afflict an addi-tional 1.3 to 3 million people,5 includ-ing an estimated 10%–18% of those inacute care and up to 28% of those inextended care facilities.6 The totaldirect annual cost incurred in the treat-ment of these wounds is estimated tobe in the tens of billions of dollars.7–9
Recent estimates suggest that com-plete wound closure is achieved in aslow as 25%–50% of chronic wounds,specifically venous and diabetic ulcers,following up to 20 weeks of treat-ment.10–12 The delayed healing of thesewounds has a significant negative
Maintenance Debridement in the Treatmentof Difficult-to-Heal Chronic WoundsRecommendations of an Expert PanelVincent Falanga, MD;1,2 Harold Brem, MD;3 William J. Ennis, DO;4 Randall Wolcott, MD;5 Lisa J. Gould, MD,PhD;6 Elizabeth A. Ayello, PhD, RN7
From 1Boston University, Departments of Dermatology and Biochemistry, Boston, MA; 2NIH Center of BiomedicalResearch Excellence, Roger Williams Medical Center, Providence, RI; 3Division of Wound Healing & RegenerativeMedicine, Department of Surgery, New York University School of Medicine, New York, NY; 4University of Illinois, Chicago,IL; 5Southwest Regional Wound Care Center, Lubbock, TX; 6James A. Haley Veterans’ Hospital, Department of Surgery,Tampa, FL; 7Excelsior College School of Nursing, Albany, NY
Address correspondence to: Vincent Falanga, MD, Roger Williams Medical Center, Dept. of Dermatology, 50 Maude Street, Providence,RI 02908; E-mail: [email protected]
Abstract
Introduction: Maintenance debridement has been proposed as a ther-apeutic intervention to address the problem of chronic wounds charac-terized by an adequate wound bed but absent or slow healing. A panelof experts convened to address the rationale and method of mainte-nance debridement.
Purpose: The goals of the panel were to summarize the scientific ration-ale for maintenance debridement, discuss the biochemical and cellularabnormalities in the wound bed, and provide a working algorithm forhow maintenance debridement should be used.
Methods: A multidisciplinary panel of wound healing and wound careexperts comprising the fields of nursing, dermatology, internal medicine,and surgery was assembled to address maintenance debridement fromdifferent points of view and offer a unified approach.
Findings: The chronic wound contains a number of microbial, biochem-ical, and cellular features and abnormalities that prevent or slow its pro-gression to healing despite a seemingly adequate wound bed. Underthese circumstances, maintenance debridement is proposed as a way toremove tissues that are colonized with an excessive bacterial burdenand diminish what can be described as a biochemical and cellular bur-den that impairs healing. A working clinical algorithm is proposed.
Conclusion: Maintenance debridement is a proactive way to “jump-start” the wound and keep it in a healing mode, even when traditionaldebridement may not appear necessary because of a seemingly“healthy” wound bed.
Falanga.qxd 6/17/08 3:53 PM Page 2

Supplement to OWM June 2008 3
impact on quality of life and is associ-ated with the risk of serious and cost-ly complications, such as recurringinfections and limb amputation.2,13–15
These treatment failures are devastat-ing to patients and add many morebillions of dollars to the overall eco-nomic burden of difficult-to-heal andchronic wounds (approximately $11billion for amputations alone).8,13
To promote greater uniformity ofcare and improve treatment outcomes,several professional societies and agen-cies have published evidence-baseddocuments that address the care ofchronic wounds. Most recently, theseinclude the series of guidelines on thebest care of chronic wounds publishedby the Wound Healing Society(WHS),3,5,16,17 the Centers forMedicare & Medicaid Services ExpertAdvisory Panel on the Usual Care ofChronic Wounds,18 and the Agencyfor Healthcare Research and Qualitytechnology assessment on usual carein the management of chronicwounds.19 Other important guide-lines, including those from theWound, Ostomy, and ContinenceNurses Society (WOCN), have beenreviewed as well.19 These guidelinesprovide a helpful foundation for thedevelopment of effective treatmentplans and discuss the importance ofeffective debridement in achievingthe goals of therapy. Admittedly,guidelines are evidence-based only upto a point and are by necessity worksin progress due to changes that occurin the understanding of the pathogen-esis of disease processes and the role oftherapeutic agents. Moreover, clini-cians can benefit from additionalguidance regarding the practicalimplementation of specific guidelinerecommendations within a compre-hensive treatment strategy. The needfor clearer recommendations for prac-tical implementation of debridement
procedures has become more pressingin light of recent concerns that greaterattention must be paid to the per-formance and documentation ofdebridement.20
In November 2007, an expert panelwas convened in Boston,Massachusetts, to discuss the princi-ples of maintenance debridement as acritical element in a successful woundcare strategy and develop practicalrecommendations for its implementa-tion. The expert, multidisciplinarypanel included clinicians from thefollowing fields: nursing, dermatol-ogy, internal medicine, and surgery.The panel members have had exten-sive experience in the care of diffi-cult-to-heal and chronic wounds andare actively involved in wound careresearch and/or education.The focuswas on maintenance debridementbecause of a growing body of evi-dence that demonstrates the deleteri-ous effects of an unchecked necrotic,cellular, and bacterial burden on theability of wounds to heal.21–31
Moreover, a direct relationship hasbeen demonstrated between healingrates and the efficiency and frequencyof debridement.32–35 The panel mem-bers reviewed the available guidelinesthat have been published mostrecently3,16,17 and analyzed the scientif-ic evidence for bacterial, biochemical,and cellular abnormalities in chronicwounds.22–31 All authors of this manu-script were panel members.
MAINTENANCEDEBRIDEMENT IN THECONTEXT OF WOUND BEDPREPARATION: GLOBAL VIEW
Truly active and effective treat-ments for chronic wounds haveemerged only recently, within the last10 years. First, topically appliedrecombinant human platelet-derivedgrowth factor (rhPDGF) was
approved for the treatment of diabet-ic neuropathic foot ulcers. Shortlythereafter, a living bilayered skin con-struct received regulatory approvalfor treating venous and diabeticulcers.23,34,36 With the emergence ofthese sophisticated products, whichwere the result of many decades ofresearch and technological advances,came the expectation that the clinicaloutcome for chronic wounds wouldbe dramatically improved. However,panel members believe that threeobstacles became apparent shortlyafter these and other advanced prod-ucts were approved for clinical use.Admittedly, complete published dataon these obstacles and how theyaffect clinical care in a measurableway are not available.Two rather pre-dictable obstacles were reimburse-ment and acceptance by clinicians.The reimbursement issues have nowbeen largely dealt with satisfactorily,at least for some tissue skin substi-tutes. Moreover, in response to edu-cational efforts, clinical evidence, andguidelines, clinicians are now increas-ingly using these advanced therapeu-tic agents. A more interesting obsta-cle to the success of advanced thera-pies, however, was unexpected. Itbecame clear that even experiencedclinicians were not paying closeenough attention to the state of thewound bed and what would berequired for advanced products todisplay their optimal efficacy. Thishad become clear during therhPDGF trials34 and after the approvalof living skin substitutes.22
As a result, the concept of woundbed preparation was developed toaddress the overall state of the woundand the steps necessary to optimizeboth the endogenous process of heal-ing and the effectiveness of advancedtherapeutic agents. After its first for-mulation,22 the concept was expanded
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Falanga.qxd 6/17/08 3:53 PM Page 3

4 Supplement to OWM June 2008
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
in other publications.23–25 The con-cept of wound bed preparation stim-ulated the field of chronic woundcare in important and beneficialways. It helped clinicians focus oncontrol of wound exudate, removalof necrotic tissue, attention to biolog-ical events that occur duringimpaired healing, and the properguidelines for conventional treat-ment.As part of wound bed prepara-tion, another concept with importantpractical ramifications was born:maintenance debridement.22,23,37 Thisconcept was based on early evidenceaccumulated from clinical trials,22
biochemical and cellular features ofchronic wounds,25,28,30,31,38 and thedetermination of increased bacterialburden and biofilm presence.16,26,39 Inlight of these findings, maintenancedebridement represents the need torestore the healing mode by a pro-gram of debriding the wound bedeven when the wound bed mayappear clinically adequate.
SCIENTIFIC RATIONALE FORDEBRIDEMENT
The importance of debridementwas observed as a secondary out-come in a randomized, double-blind, placebo-controlled, multicen-ter trial of the safety and efficacy oftopically applied rhPDGF in thetreatment of chronic diabeticulcers.34 In that trial, all ulcers werethoroughly debrided (wound bed
and callus) at the beginning of thestudy, and the investigators wereallowed to perform additionaldebridements during follow-upwhen they deemed the procedureappropriate. The study achieved itsprimary goal by demonstrating thatthe rate of wound closure was high-er among ulcers treated withrhPDGF than those treated withplacebo. An important and unex-pected finding, however, was that thecenters performing the most fre-quent debridements had the highestwound closure rates in both therhPDGF and placebo treatmentgroups. Similarly, the centers thatperformed the least frequentdebridements had the lowest healingrates.34 These findings suggest thatdebridement can lead to improvedclinical outcomes. This conclusiongains considerable support fromresults showing that frequentdebridement of chronic wounds canhelp reduce amputation rates.40
As previously discussed, the needfor initial and repeated debridementof a clearly necrotic or nonviablewound bed in diabetic neuropathicfoot ulcers was quite evident fromthe findings of Steed et al.34 Later, asless clinically evident abnormalitiespresent in the wound bed becamemore apparent, the concept of main-tenance debridement evolved.22 Theimportance of maintenance debride-ment gains further support from the
recognition that in difficult-to-healand chronic wounds there are manybiochemical, cellular, and bacteriolog-ical abnormalities that will interferewith healing and increase the risk ofinfection if not frequently or continu-ally controlled.22–24 Therefore, woundsthat clinically show a seemingly ade-quate wound bed may benefit fromdebridement if healing has stalled.35
There are now promising tools thatcan be used to assess the effectivenessof debridement and wound bedpreparation.Two such studies show acorrelation between the efficacy ofdebridement and healing rates.32,33
The Debridement PerformanceIndex,32 which evaluates the adequa-cy of debridement, has been shownto directly correlate with the likeli-hood of wound closure by Week 12.This was demonstrated in a valida-tion study that found that theDebridement Performance Index,which is based on the removal of cal-lus, undermined edges, and necrotictissues, was an independent predictorof wound closure in diabetic footulcers that had been treated witheither standard therapy or a bioengi-neered skin construct.32 More recent-ly, the Wound Bed Score (WBS),which provides a broader and moreglobal assessment of the wound andreflects the adequacy of wound bedpreparation in general, has beenshown to be a predictor of ultimatewound closure in venous ulcers.33,37
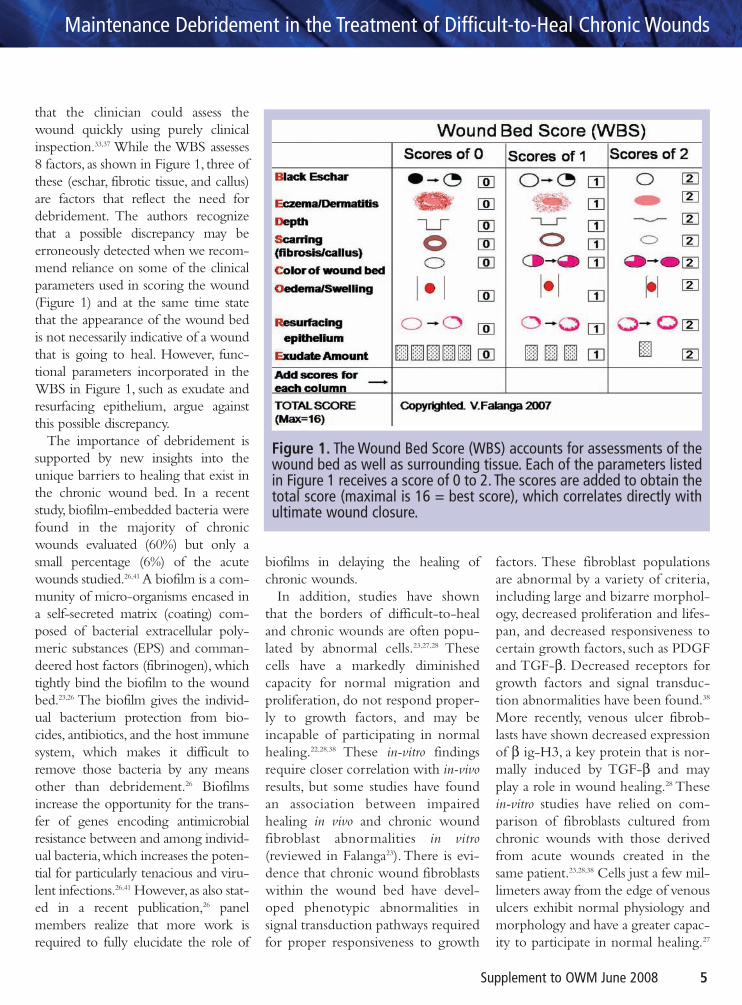
The WBS includes assessments of thepresence of eschar, fibrotic tissue, andcallus — all factors that reflect theadequacy or need for debridement.37
Figure 1 shows how the WBS isdetermined. The WBS relies entirelyon critical parameters that are impor-tant in wound closure and can beanalyzed at the bedside without theneed for laboratory tests. Indeed, theWBS was developed with the goal
The removal of nonfunctional cells within thewound bed and at the wound edge, removal ofnecrotic tissue, or elimination of biofilms maypromote healing in wounds that are stuck in anonhealing mode.
Falanga.qxd 6/17/08 3:53 PM Page 4
Supplement to OWM June 2008 5
that the clinician could assess thewound quickly using purely clinicalinspection.33,37 While the WBS assesses8 factors, as shown in Figure 1, three ofthese (eschar, fibrotic tissue, and callus)are factors that reflect the need fordebridement. The authors recognizethat a possible discrepancy may beerroneously detected when we recom-mend reliance on some of the clinicalparameters used in scoring the wound(Figure 1) and at the same time statethat the appearance of the wound bedis not necessarily indicative of a woundthat is going to heal. However, func-tional parameters incorporated in theWBS in Figure 1, such as exudate andresurfacing epithelium, argue againstthis possible discrepancy.
The importance of debridement issupported by new insights into theunique barriers to healing that exist inthe chronic wound bed. In a recentstudy, biofilm-embedded bacteria werefound in the majority of chronicwounds evaluated (60%) but only asmall percentage (6%) of the acutewounds studied.26,41 A biofilm is a com-munity of micro-organisms encased ina self-secreted matrix (coating) com-posed of bacterial extracellular poly-meric substances (EPS) and comman-deered host factors (fibrinogen), whichtightly bind the biofilm to the woundbed.23,26 The biofilm gives the individ-ual bacterium protection from bio-cides, antibiotics, and the host immunesystem, which makes it difficult toremove those bacteria by any meansother than debridement.26 Biofilmsincrease the opportunity for the trans-fer of genes encoding antimicrobialresistance between and among individ-ual bacteria,which increases the poten-tial for particularly tenacious and viru-lent infections.26,41 However,as also stat-ed in a recent publication,26 panelmembers realize that more work isrequired to fully elucidate the role of
biofilms in delaying the healing ofchronic wounds.
In addition, studies have shownthat the borders of difficult-to-healand chronic wounds are often popu-lated by abnormal cells.23,27,28 Thesecells have a markedly diminishedcapacity for normal migration andproliferation, do not respond proper-ly to growth factors, and may beincapable of participating in normalhealing.22,28,38 These in-vitro findingsrequire closer correlation with in-vivoresults, but some studies have foundan association between impairedhealing in vivo and chronic woundfibroblast abnormalities in vitro(reviewed in Falanga23).There is evi-dence that chronic wound fibroblastswithin the wound bed have devel-oped phenotypic abnormalities insignal transduction pathways requiredfor proper responsiveness to growth
factors. These fibroblast populationsare abnormal by a variety of criteria,including large and bizarre morphol-ogy, decreased proliferation and lifes-pan, and decreased responsiveness tocertain growth factors, such as PDGFand TGF-β. Decreased receptors forgrowth factors and signal transduc-tion abnormalities have been found.38
More recently, venous ulcer fibrob-lasts have shown decreased expressionof β ig-H3, a key protein that is nor-mally induced by TGF-β and mayplay a role in wound healing.28 Thesein-vitro studies have relied on com-parison of fibroblasts cultured fromchronic wounds with those derivedfrom acute wounds created in thesame patient.23,28,38 Cells just a few mil-limeters away from the edge of venousulcers exhibit normal physiology andmorphology and have a greater capac-ity to participate in normal healing.27
Figure 1. The Wound Bed Score (WBS) accounts for assessments of thewound bed as well as surrounding tissue. Each of the parameters listedin Figure 1 receives a score of 0 to 2. The scores are added to obtain thetotal score (maximal is 16 = best score), which correlates directly withultimate wound closure.
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Falanga.qxd 6/17/08 3:53 PM Page 5

6 Supplement to OWM June 2008
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Chronic wounds also have beenshown to have elevated levels ofmatrix metalloproteinases, which havebeen associated with poor healing.29–31
Debridement may help by removingabnormal cells and excess matrix met-alloproteinases and help in the recruit-ment of normal cells to the wound.22
DEFINITION OF TERMSGenerally, terms are defined before
one addresses the issues that thoseterms represent. However, the panelthought it would be more helpful tofirst discuss the background that led tothe evolution and formulation ofmaintenance debridement.
The distinction between initial (orrepeated) debridement and mainte-nance debridement is not necessarilyin the method used but rather in boththe temporal sequence and the ration-ale.Thus, unlike the initial (and some-times repeated) debridement, mainte-nance debridement may be requiredeven in the context of an adequatewound bed when the wound showscontinued impaired healing.22,23
Traditionally, the term debridementhas been used to address the removalof necrotic, damaged, or infected tis-sue.3,22 Therefore, debridement may
need to be repeated periodically (typ-ically once or twice a week for chron-ic wounds) as long as the wound beddisplays the features of necrotic, dam-aged, and/or infected tissue. This iswhat was done in previous studies inwhich debridement was found to cor-relate with faster wound closure. Inthose studies, the presence of a newlyformed callus around the neuropathicdiabetic foot ulcer could be consideredevidence of damaged, and certainlyreactive, tissue surrounding thewound.34 As shown in Table 1, initialdebridement refers to the first debride-ment performed on a wound follow-ing the initial evaluation by the clini-cian.This may or may not, however, bethe first debridement performed dur-ing the life cycle of a particularwound. Patients with difficult-to-healand chronic wounds may have manycomorbidities and may transitionbetween multiple clinicians and sites ofcare before complete healing isachieved. Nonetheless, the first timeany clinician sees a patient for woundcare, the wound should always be re-evaluated and an independent decisionmade about the need for debridement.
Maintenance debridement, on theother hand, can be defined as ongoing
wound debridement to keep thewound free of impediments to heal-ing in addition to the removal ofnonviable, damaged, and/or infectedtissue.22,23 Maintenance debridementwas first described in the context of anovel approach to make the woundmore permissive to healing, the con-cept of wound bed preparation.22,23 Theexpert panel and authors of the pres-ent manuscript agree that a woundmay need maintenance debridementto restore and sustain a healing mode.Thus, in a wound that is resistant tohealing, the clinician must recognizethat other factors that are not clini-cally detectable upon inspection maybe present in the wound bed. Suchfactors include a high bacterial bur-den or biofilm, a disequilibrium oftissue metalloproteinases, and woundcells that have become phenotypical-ly abnormal (the cellular burden).22,23
The panel suspects that, in time, someof these parameters may becomemore easily measurable and provide agreater rationale for therapeuticintervention.
Table 1 defines both initialdebridement and maintenancedebridement, as agreed upon by thepanel. There was discussion amongpanel members about what consti-tutes a lack of wound closure or,perhaps even more challenging,inadequate wound closure. This hasimportant ramifications when dis-cussing at what point to institutemaintenance debridement andwhen to terminate it (Figure 2).Improvement in the wound, specifi-cally its depth and surface area, haslong been used as a clinical parame-ter. However, short of no improve-ment at all, the critical issue is howmuch of an improvement is neededto regard the wound as closing in atimely manner.There was consensusthat this should remain an active
Table 1. Definition of terms and goals of debridement
Initial Debridement: The removal of necrotic, damaged, and/orinfected tissue from the wound bed. Removal of periwound callus isincluded in this definition. The debridement needs to be repeated aslong as those clinical parameters persist or recur.
Maintenance Debridement: Ongoing debridement to help main-tain the wound in a healing mode. The debridement intervention isdictated not only by clinically evident parameters but also by theneed to achieve optimal wound bed preparation. Therefore, mainte-nance debridement is performed even in the face of a seeminglyhealthy wound bed if the wound is not showing evidence of closure.
Falanga.qxd 6/17/08 3:53 PM Page 6
Supplement to OWM June 2008 7
area of investigation and testing.One possibility is to use the rate of0.75 mm/week of wound edgeadvancement (to be discussed later),which is about 80% sensitive andspecific for ultimate wound closure.However, an easier way that doesnot require calculating the healingrate is to use the WBS (Figure 1).Studies are needed to explore thevalidity of this recommendation.
GOALS OF INITIAL AND MAINTENANCE DEBRIDEMENT
Some chronic wound care guidelineshave adopted these definitions ofdebridement and maintenancedebridement, but in most cases, thetwo either have not been crisply sepa-rated or have been merged. For exam-ple, in some chronic wound careguidelines, debridement is listed as akey element of both infection control
and wound bed preparation.The WHSguidelines state that debridement “isrequired to remove the obviousnecrotic tissue, excessive bacterial bur-den, and cellular burden of dead andsenescent cells”3,5,16,17 and that mainte-nance debridement “is needed tomaintain the appearance and readinessof the wound bed for healing.”3,5,16
These two statements may lead to con-fusion. Indeed, this discussion is meant
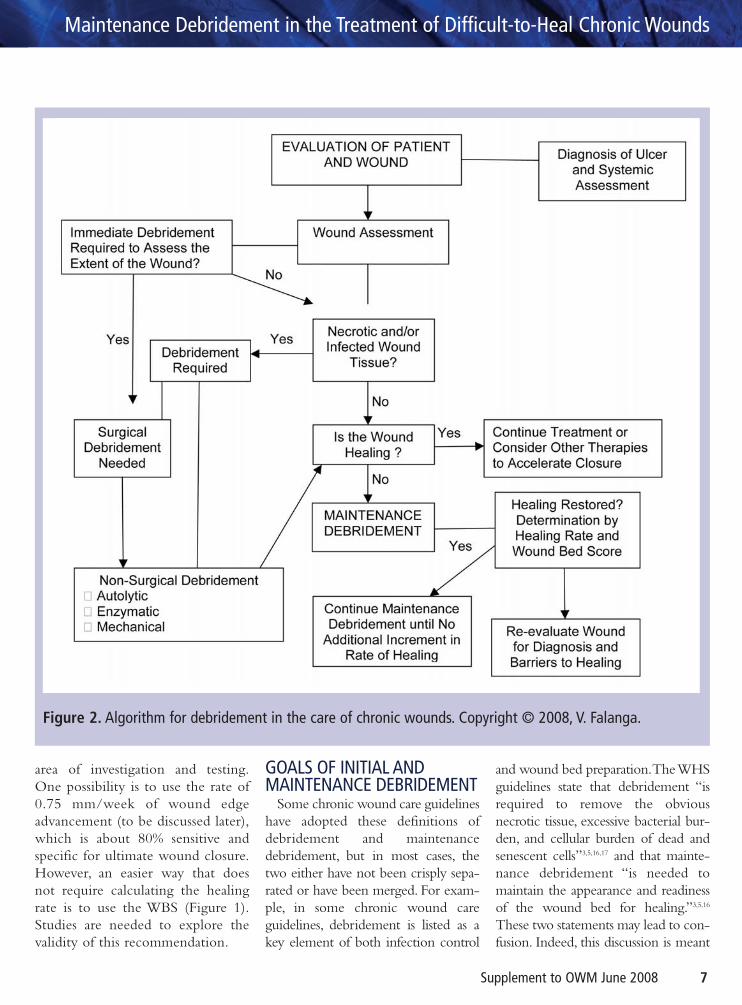
Figure 2. Algorithm for debridement in the care of chronic wounds. Copyright © 2008, V. Falanga.
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Falanga.qxd 6/17/08 3:53 PM Page 7
8 Supplement to OWM June 2008
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
to clarify those statements regardingmaintenance debridement. Table 1defines more clearly the goals ofdebridement, re-emphasizing the dis-tinction between initial and mainte-nance debridement. This point isaddressed further in the discussion onthe algorithm for debridement (Figure2) in the next section.
It is essential to emphasize thatcomplete and timely wound closureis the overriding objective of allaspects of wound care, includingdebridement, because the latter cor-relates with wound closure rates.32–34
One can acknowledge that circum-stances exist in which patient com-fort and wound stabilization, ratherthan complete wound closure, maybe the primary goals of wound care.However, this approach should applyto only a small percentage of cases,such as in those patients for whomtreatment is simply not possible orpractical because of their unique and
underlying comorbidities.42 Terminalor serious illness, per se, generally isnot considered sufficient cause toabandon efforts to promote healing.On the other hand, the exclusiveemphasis on complete wound clo-sure for all types of wounds, ratherthan additional focus on decreasedwound size, pain control, and quality-of-life improvements, may have madeit more difficult for new therapies toreach regulatory approval.
IMPLEMENTATION OFDEBRIDEMENT WITHIN THECONTEXT OF AN EFFECTIVEWOUND CARE STRATEGY
The role of debridement within acomprehensive wound care strategyis highlighted in the algorithmshown in Figure 2, which was agreedupon by panel members. Discussionof all components of effective woundcare is beyond the scope of this arti-cle. However, it is important to
emphasize that decisions aboutdebridement can only be made aftera thorough evaluation of all aspects ofthe patient’s condition (includingnutritional and vascular status).Therefore, debridement is mosteffectively implemented within thecontext of a therapeutic regimen thataddresses all of the wound’s needs.Some topical therapies may interferewith one another or with the use ofcertain therapeutic agents. For exam-ple, concomitant use of heavy metalsand antiseptics, particularly those thatare not slow-release, needs to beapproached with caution in the con-text of living skin substitutes andgrowth factors.23,24
The evaluation process involvesclose attention to systemic issues (ie,presence of diabetes, heart failure, useof immunosuppressive agents) as wellas wound assessment. As shown inFigure 2, checkpoints prompt the cli-nician to make important decisionsregarding the need for immediatesurgical debridement, the type ofdebridement to adopt, and the needfor maintenance debridement.
The recommendations for debride-ment and which type of debridementprovided in this section stem from theopinions and experience of the expertpanel. This is also by necessity, forthere is general lack or paucity of clin-ical research trials addressing thesebasic wound care topics. Particularly,there are no large and reliable studiescomparing different approaches andmethods of debridement. The panelrecognizes that this is a fertile area ofinvestigation, which may have beenlagging behind other evidence-basedtopics because of the lack of agreedupon endpoints.
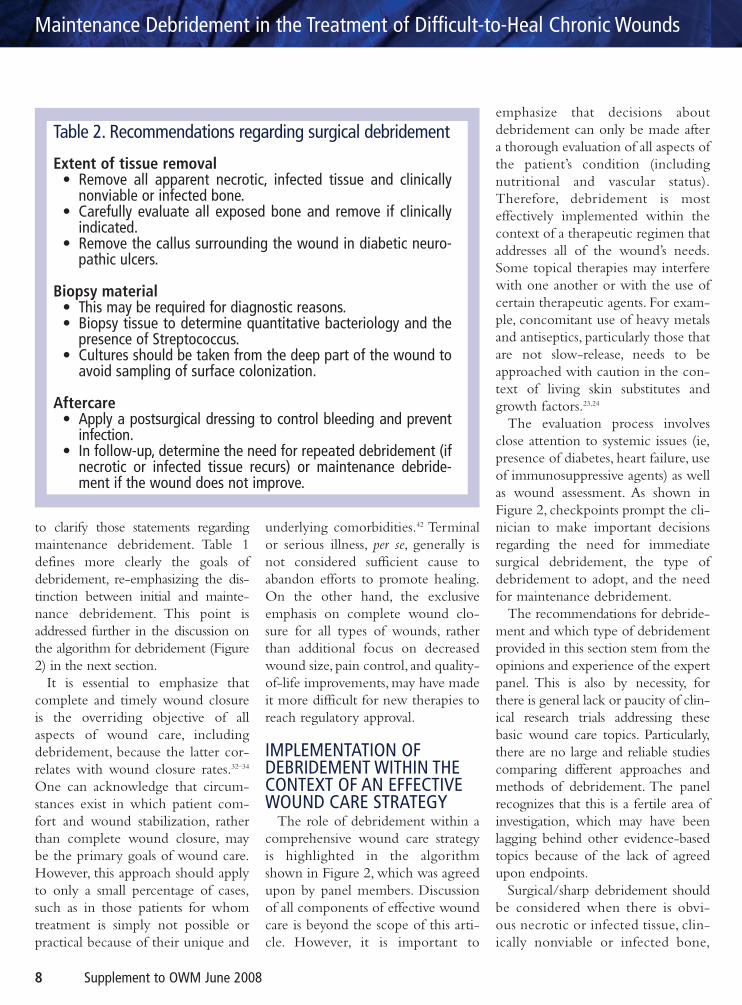
Surgical/sharp debridement shouldbe considered when there is obvi-ous necrotic or infected tissue, clin-ically nonviable or infected bone,
Table 2. Recommendations regarding surgical debridement
Extent of tissue removal• Remove all apparent necrotic, infected tissue and clinically
nonviable or infected bone.• Carefully evaluate all exposed bone and remove if clinically
indicated.• Remove the callus surrounding the wound in diabetic neuro-
pathic ulcers.
Biopsy material• This may be required for diagnostic reasons.• Biopsy tissue to determine quantitative bacteriology and the
presence of Streptococcus.• Cultures should be taken from the deep part of the wound to
avoid sampling of surface colonization.
Aftercare• Apply a postsurgical dressing to control bleeding and prevent
infection.• In follow-up, determine the need for repeated debridement (if
necrotic or infected tissue recurs) or maintenance debride-ment if the wound does not improve.
Falanga.qxd 6/17/08 3:53 PM Page 8

Supplement to OWM June 2008 9
undermining or tunneling, or callus(Table 2).The panel considered under-mining of a wound to be a criticalproblem that affects both the properevaluation of the extent of the woundand the possibility that underminingcreates a dead space immediatelybeneath the surrounding skin thatmight facilitate bacterial overgrowth.However, it also was recognized thatin certain clinical situations, eg, inpressure ulcers and when the under-mining is not judged to be extensive,one need not immediately proceed tosurgical/sharp debridement. The dis-advantages of surgical debridementare its invasiveness and that healthy tis-sue is removed.An important consid-eration for surgical debridement alsois based on proper wound assessment.This situation typically arises in thecontext of diabetic foot ulcers wherethe extent of the ulceration, tunnel-ing, and the possibility of an abscessmay not be clinically evident and mustbe explored immediately (Figure 2).The patient’s vascular status, however,must always be considered before sur-gical/sharp debridement is performed.
Practical recommendations for sur-gical/sharp debridement are summa-rized in Table 2.
All exposed bone should be evalu-ated and removed if clinically indi-cated. It is also particularly importantto remove callus in diabetic neuro-pathic ulcers due to the possibilitythat the callus causes additional pres-sure to the wound edges.
During surgical debridement, itmay be appropriate to obtain tissuefor histological and microbial evalua-tion.This is usually done to exclude amalignancy, to help in the diagnosisof an inflammatory ulcer (ie, due tovasculitis), or to rule out an unusualwound infection. A rare but impor-tant difficulty is encountered whenfaced with pyoderma gangrenosum,
an inflammatory condition that canbe idiopathic or most commonlyassociated with rheumatoid arthritisand ulcerative colitis. If this conditionis suspected (biopsy is not diagnos-tic), dermatological consultation ishelpful. Pyoderma gangrenosum,through a process known as pathergy,can worsen and enlarge dramaticallyupon surgical debridement.43
A critical checkpoint in Figure 2 isthe decision of whether the wound isnot healing, even when the woundbed seems adequate and free of obvi-ously necrotic and infected tissue. Ifthe wound shows signs of healing,such as decreased depth and overallsize or wound edges that havemigrated over the wound bed, onemay opt to continue the treatmentstrategy that is being carried out atthat time. However, additionaland/or more advanced treatmentmodalities may be used at this pointto further accelerate wound closure.
In the absence of satisfactory signsof healing, even when the woundbed seems adequate, maintenancedebridement should be strongly con-sidered. Falanga22,23 previously dis-cussed the rationale for initiatingmaintenance debridement at thatpoint. Biochemical and cellularabnormalities, as well as excessivebacterial burden, may cause impairedhealing and may be helped byremoving what falsely appears to benormal granulation tissue. For main-tenance debridement, nonsurgicalmeans may be tried first, but oneshould also consider surgical tissueremoval if no improvement is noted.
Initial debridement. Initialdebridement may be surgical/sharp,mechanical, enzymatic, biological(larval therapy), or autolytic, depend-ing on the condition of the wound.The merits of each approach are dis-cussed briefly in Table 3 and in
review articles.37,44–46 A key issue forinitial debridement is when tochoose surgical/sharp debridement,which requires specific personnel,facilities, and expertise, over otheravailable techniques.
The previous section discussed sur-gical debridement. As indicated inFigure 2, depending on the clinicalfindings and circumstances, the clini-cian may decide to use nonsurgicalmeans of debridement. These othertypes of debridement and theiradvantages and disadvantages also arediscussed in Table 3 and reviewedelsewhere.44–49 It must be appreciatedthat overlaps exist in the way differ-ent debriding interventions work.For example, absorbent agents(including dressings) may overlapwith slow-release antiseptic prepara-tions that incorporate an antisepticwithin a release vehicle (Table 3).Another difficulty is how to discuss afeature of a debriding agent thatcomes into play immediately beforeor after debridement begins. Forexample, occlusive dressings often aresaid to cause painless debridement.Yet, their removal can be associatedwith considerable pain. For this rea-son, the last column in Table 3 refersto an overall assessment of thepatient’s comfort rather than painalone.Yet another difficulty encoun-tered by the panel in definingdebriding agents and in formulatingTable 3 was whether to include slow-release antiseptics. However, clinicalstudies have shown that effectivedebridement can be achieved withthis approach.50
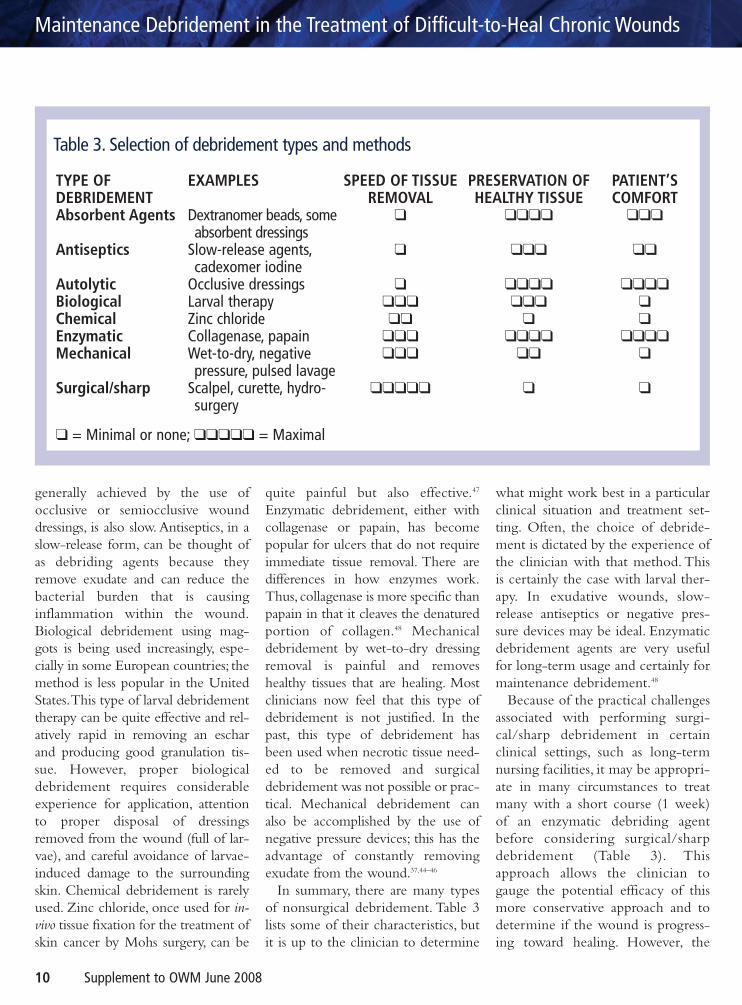
There are specific advantages anddisadvantages to all classes of debrid-ing approaches, as summarized inTable 3. Absorbent agents, such asbeads (less commonly used now) andnewer absorbing dressings tend to beslow in action.Autolytic debridement,
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Falanga.qxd 6/17/08 3:53 PM Page 9
10 Supplement to OWM June 2008
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
generally achieved by the use ofocclusive or semiocclusive wounddressings, is also slow. Antiseptics, in aslow-release form, can be thought ofas debriding agents because theyremove exudate and can reduce thebacterial burden that is causinginflammation within the wound.Biological debridement using mag-gots is being used increasingly, espe-cially in some European countries; themethod is less popular in the UnitedStates.This type of larval debridementtherapy can be quite effective and rel-atively rapid in removing an escharand producing good granulation tis-sue. However, proper biologicaldebridement requires considerableexperience for application, attentionto proper disposal of dressingsremoved from the wound (full of lar-vae), and careful avoidance of larvae-induced damage to the surroundingskin. Chemical debridement is rarelyused. Zinc chloride, once used for in-vivo tissue fixation for the treatment ofskin cancer by Mohs surgery, can be
quite painful but also effective.47
Enzymatic debridement, either withcollagenase or papain, has becomepopular for ulcers that do not requireimmediate tissue removal. There aredifferences in how enzymes work.Thus, collagenase is more specific thanpapain in that it cleaves the denaturedportion of collagen.48 Mechanicaldebridement by wet-to-dry dressingremoval is painful and removeshealthy tissues that are healing. Mostclinicians now feel that this type ofdebridement is not justified. In thepast, this type of debridement hasbeen used when necrotic tissue need-ed to be removed and surgicaldebridement was not possible or prac-tical. Mechanical debridement canalso be accomplished by the use ofnegative pressure devices; this has theadvantage of constantly removingexudate from the wound.37,44–46
In summary, there are many typesof nonsurgical debridement. Table 3lists some of their characteristics, butit is up to the clinician to determine
what might work best in a particularclinical situation and treatment set-ting. Often, the choice of debride-ment is dictated by the experience ofthe clinician with that method. Thisis certainly the case with larval ther-apy. In exudative wounds, slow-release antiseptics or negative pres-sure devices may be ideal. Enzymaticdebridement agents are very usefulfor long-term usage and certainly formaintenance debridement.48
Because of the practical challengesassociated with performing surgi-cal/sharp debridement in certainclinical settings, such as long-termnursing facilities, it may be appropri-ate in many circumstances to treatmany with a short course (1 week)of an enzymatic debriding agentbefore considering surgical/sharpdebridement (Table 3). Thisapproach allows the clinician togauge the potential efficacy of thismore conservative approach and todetermine if the wound is progress-ing toward healing. However, the
Table 3. Selection of debridement types and methods
TYPE OF DEBRIDEMENTAbsorbent Agents
Antiseptics
AutolyticBiologicalChemicalEnzymaticMechanical
Surgical/sharp
EXAMPLES
Dextranomer beads, someabsorbent dressings
Slow-release agents,cadexomer iodine
Occlusive dressingsLarval therapyZinc chlorideCollagenase, papainWet-to-dry, negativepressure, pulsed lavage
Scalpel, curette, hydro-surgery
SPEED OF TISSUEREMOVAL
❑
❑
❑❑❑❑❑❑
❑❑❑❑❑❑
❑❑❑❑❑
PRESERVATION OFHEALTHY TISSUE
❑❑❑❑
❑❑❑
❑❑❑❑❑❑❑
❑❑❑❑❑
❑❑
❑
PATIENT’SCOMFORT
❑❑❑
❑❑
❑❑❑❑❑❑
❑❑❑❑❑
❑
❑ = Minimal or none; ❑❑❑❑❑ = Maximal
Falanga.qxd 6/17/08 3:53 PM Page 10

Supplement to OWM June 2008 11
safety and welfare of the patient mustnot be compromised because of dif-ficulties with the clinical setting; theclinician needs to follow the optimalprinciples of wound care. Differenttypes of enzymatic agents are avail-able, and some are able to digestthick eschars in certain cases.Collagenase- and papain-basedenzymatic agents are available forthis purpose.48 Enzymatic treatment,which can be considered a milderand slower approach to debride-ment, is not appropriate whenadvancing necrosis is present.
Maintenance debridement. Inthe face of impaired or slow healing,the clinician should strongly considerinstituting maintenance debridementto improve wound bed prepara-tion.22,23,37 Although surgical debride-ment may be used even for mainte-nance debridement, a more gentleapproach is often used (Table 3). Acritical issue with regard to mainte-nance debridement is deciding howlong to continue it and when todebride again if not choosing amethod that is ongoing (enzymes,chemicals, etc.). The only way toensure that the goal of maintenancedebridement (keeping the woundfree of barriers to healing) is beingmet is to evaluate the wound for evi-dence of healing.Although this is nota primary focus of our discussion, theactual healing rate, representing thespeed at which wound edges moveinward within the first 3 to 4 weeksof therapy, has been shown to be avalid endpoint.51 Using the healingrate in clinical trials could lead tomore efficient screening of experi-mental treatments and could acceler-ate the regulatory approval of newand useful therapies. In previousreports, it has been shown that thehealing rate, measurable at 4 weeks oftherapy, is approximately 80% sensi-
tive and specific for predicting ulti-mate wound closure in venous (by 24weeks; n = 136) and diabetic (by 12weeks; n = 96) ulcers.36 Interestingly,in the same studies, it was found thata critical threshold of the healing ratefor predicting wound closure was0.75 mm/week of inward movementof the wound edges for both types ofvenous and diabetic neuropathicwounds.The implication is that thereis a certain keratinocyte speed limitcommon to chronic wounds.23,51
The goal of maintenance debride-ment is to keep the wound progress-ing toward healing with minimalinterruption, but there may be cost-effectiveness benefits as well.A proac-tive strategy may reduce the need formore aggressive (and potentially moretraumatic and costly) debridement inresponse to wound deterioration.
Some wounds may need only mild,ongoing debridement, while othersmay require more potent treatments.The available options are describedin Table 3.
During maintenance debridement,the methods used from Table 3 mayvary during follow-up, depending onthe clinical findings and necessities.The effectiveness of maintenancedebridement should be monitoredregularly and adjusted as needed toensure that the wound continues toprogress toward healing.The WBS, asin Figure 1, can be useful in thisregard, because optimal wound bed
preparation should be the result of aneffective maintenance debridementstrategy.36,37 Absence of healing, slowhealing, or an increase in the size ofthe wound is sufficient to signal thatthe patient should be re-evaluated. Ifno explanation can be found for thefailure to heal (ie, infection or exces-sive bacterial burden, systemic fac-tors, lack of compliance with offload-ing), a more aggressive method ofdebridement may be chosen (Table3). Of course, debridement is onlypart of wound bed preparation. Itmay be necessary to intervene withother treatment modalities to jump-start the healing process.
It is important to keep in mind thatonce maintenance debridement hasbeen instituted, it should not be dis-continued just because the wound“looks good”; the ultimate goal is toachieve complete closure. A woundbed that “looks good” to a clinician(even an experienced one) does notnecessarily mean that it is adequatefrom a microbial, biochemical, and cel-lular standpoint. In discussing and con-structing the algorithm shown inFigure 2, the panel also considered atwhat point maintenance debridementshould be discontinued when thewound is showing evidence of healing.Hence, as emphasized with theapproach of wound bed prepara-tion,22,23,37 one needs to rely on func-tional parameters that show evidenceof healing. However, this needs further
Clinical inspection alone cannot determinewhether the wound bed is adequate from amicrobial, biochemical, and cellular standpoint.Hence, one must rely on functional parametersthat show evidence of healing.
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Falanga.qxd 6/17/08 3:53 PM Page 11
12 Supplement to OWM June 2008
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
study.As shown in Figure 2, the panelproposes that maintenance debride-ment should be continued as long asfurther increments in healing occur,which could be characterized as anincreasing healing rate or animprovement in the WBS (Figure 1).
CONCLUSION AND FUTURE NEEDS
This report relied on the collectiveexpertise of a group of experts fromdifferent fields to arrive at an agree-ment with regard to maintenancedebridement and a clinical algorithmthat clinicians can use when evaluat-ing a chronic wound. The clinicaland scientific rationale for mainte-nance debridement was discussedbased on the panel’s understanding ofbacterial burden and biofilms, bio-chemical abnormalities, and pheno-typic changes in cells persisting (cel-lular burden) in from the wound bedand at the edge of nonhealingwounds.As a result, an important con-clusion is that maintenance debride-ment may be required when thewound is not healing and even whenthe wound bed appears to be satisfac-tory upon clinical inspection. Implicitin these conclusions is that there canbe a strong dissociation between theclinical appearance of the wound bedand satisfactory healing. Clinical
research, combined with in-vitro stud-ies and biomarkers, may providestronger evidence for these state-ments and recommendations.
The efficacy of debridement strate-gies could be improved by the devel-opment of simple markers or assess-ment tools that could be used at thebedside to determine quickly if addi-tional debridement is necessary.Therefore, an important consensusstatement from this expert panel isthat, at least in chronic wounds, theeffectiveness of debridement canonly be determined by how thedebridement improves wound heal-ing. The recommendations made inthis report, which are to use the heal-ing rate and the WBS, follow thispremise. However, the panel realizesthat additional and larger trials willbe needed to fully determine thevalidity of these recommendationsregarding debridement and whichassessments of debridement (ie,WBSor healing rate) most accurately pre-dict healing.There is also a great andincreasing demand for on-site educa-tional programs focusing on thepractical implementation of bestpractice paradigms.There is a partic-ular need for a greater understandingof the strengths, limitations, and mosteffective use of different methods ofdebridement. Comparative studies of
different types of debridement, per-haps using the algorithm proposed inthis report, could bring about acogent approach to these difficultissues regarding basic wound care.
The human and economic impactof difficult-to-heal and chronicwounds, such as venous, diabetic,pressure, and arterial insufficiencyulcers, is large and growing. Theoverall healing rates for these woundscan be improved with the aid ofclear, evidence-based guidelines forcomprehensive care.3,5,16–19 Theseguidelines outline the importance ofan effective debridement strategy inpreventing infection and preparingthe wound bed to heal.
A growing body of evidence showsthat effective and frequent debride-ment can improve healing rates.Debridement aids healing by remov-ing and keeping the wound free ofnecrotic tissue and excessive bacteriaas well as the dead and senescent cellsthat can interfere with healing.22,23,37
An effective debridement strategywill consist of an initial debridementcombined with a customized main-tenance debridement plan.Maintenance debridement is likely tobe most effective as a proactiveapproach to prevent the build-up ofnecrotic or denatured tissues and cel-lular abnormalities.
There are still many unmet needsin the treatment of difficult-to-healand chronic wounds. Rates of com-plete wound closure remain unac-ceptably low,10 and far too manypatients suffer from complicationsresulting from nonhealing wounds.The conscientious implementation
ACKNOWLEDGMENTSDr. Falanga’s work was supported in part by NIH grant DK067836, the Wound Biotechnology Foundation, and Award NumberP20RR018757 from the National Center For Research Resources. The content is solely the responsibility of the authors and doesnot necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
A growing body of evidence shows that effective and frequent debridement can improve healing rates.
Falanga.qxd 6/17/08 3:53 PM Page 12
Supplement to OWM June 2008 13
of an effective maintenance debride-ment strategy within a comprehen-sive wound care plan may help in sig-nificantly improving these outcomes.
References 1. Phillips T, Stanton B,Provan A,Lew R.A study
of the impact of leg ulcers on quality of life:financial, social, and psychologic implications. JAm Acad Dermatol. 1994;31(1):49–53.
2. Brem H, Kirsner RS, Falanga V. Protocol forthe successful treatment of venous ulcers. Am JSurg. 2004;188(1A Suppl):1–8.
3. Steed DL, Attinger C, Colaizzi T, et al.Guidelines for the treatment of diabetic ulcers.Wound Repair Regen. 2006;14(6):680–692.
4. Centers for Disease Control and Prevention.Diabetes Data & Trends. Available at:www.cdc.gov/diabetes/statistics/prev/nation-al/figpersons.htm. Accessed February 14,2006.
5. Whitney J, Phillips L, Aslam R, et al.Guidelines for the treatment of pressure ulcers.Wound Repair Regen. 2006;14(6):663–679.
6. Pressure ulcers in America: prevalence, inci-dence, and implications for the future. Anexecutive summary of the National PressureUlcer Advisory Panel monograph. Adv SkinWound Care. 2001;14(4):208–215.
7. Olin JW, Beusterien KM, Childs MB, SeaveyC, McHugh L, Griffiths RI. Medical costs oftreating venous stasis ulcers: evidence from aretrospective cohort study. Vasc Med.1999;4(1):1–7.
8. Gordois A, Scuffham P, Shearer A, Oglesby A,Tobian JA. The health care costs of diabeticperipheral neuropathy in the US. DiabetesCare. 2003;26(6):1790–1795.
9. Kumar RN, Gupchup GV, Dodd MA, et al.Direct health care costs of 4 common skinulcers in New Mexico Medicaid fee-for-serv-ice patients. Adv Skin Wound Care.2004;17(3):143–149.
10. Margolis DJ,Allen-Taylor L,Hoffstad O,BerlinJA. Healing diabetic neuropathic foot ulcers:are we getting better? Diabet Med.2005;22(2):172–176.
11. Franks PJ, Moffatt CJ. Health related quality oflife in patients with venous ulceration: use ofthe Nottingham health profile. Qual Life Res.2001;10(8):693–700.
12. Thomas DR, Diebold MR, Eggemeyer LM.Acontrolled, randomized, comparative study of aradiant heat bandage on the healing of stage 3-4 pressure ulcers: a pilot study. J Am Med DirAssoc. 2005;6(1):46–49.
13. Cali TJ, Bruce M. Pressure ulcer treatment:examining selected costs of therapeutic failure.Adv Wound Care. 1999;12(Suppl 2):8–11.
14. Iglesias CP, Birks Y, Nelson EA, Scanlon E,Cullum NA. Quality of life of people withvenous leg ulcers: a comparison of the dis-criminative and responsive characteristics oftwo generic and a disease specific instruments.Qual Life Res. 2005;14(7):1705–1718.
15. Shukla D,Tripathi AK,Agrawal S,Ansari MA,Rastogi A, Shukla VK. Pain in acute andchronic wounds: a descriptive study. Ostomy
Wound Manage. 2005;51(11):47–51.16. Robson MC, Cooper DM, Aslam R, et al.
Guidelines for the treatment of venous ulcers.Wound Repair Regen. 2006;14(6):649–662.
17. Hopf HW, Ueno C,Aslam R, et al. Guidelinesfor the treatment of arterial insufficiencyulcers. Wound Repair Regen.2006;14(6):693–710.
18. Centers for Medicare & Medicaid Services.Medicare Coverage Database. Available at:http://www.cms.hhs.gov/mcd/viewmcac.asp?where=index&mid=28. Accessed March 17,2008.
19. Lau J,Tatsioni A, Balk E, et al. Usual Care in theManagement of Chronic Wounds:A Review of theRecent Literature. Rockville, Md: Agency forHealthcare Research and Quality; 2005.
20. Office of Inspector General. Medicare pay-ments for surgical debridement services in2004. Office of Inspector General, 2007.Available at:http://oig.hhs.gov/oei/reports/oei-02-05-00390.pdf.Accessed May 5, 2008.
21. Moore J, Jensen P. Assessing the role andimpact of enzymatic debridement. PodiatryToday. 2004;17(7):54–61.
22. Falanga V. Classifications for wound prepara-tion and stimulation of chronic wounds.Wound Repair Regen. 2000;8(5):347–352.
23. Falanga V.The chronic wound: impaired heal-ing and solutions in the context of wound bedpreparation. Blood Cells Mol Dis.2004;32(1):88–94.
24. Falanga V. Wound healing and its impairmentin the diabetic foot. Lancet.2005;366(9498):1736–1743.
25. Schultz GS, Sibbald RG, Falanga V, et al.Wound bed preparation: a systematic approachto wound management. Wound Repair Regen.2003;11(Suppl 1):S1–S28.
26. James GA, Swogger E, Wolcott R, et al.Biofilms in chronic wounds. Wound RepairRegen. 2008;16(1):37–44.
27. Brem H,Stojadinovic O,Diegelmann RF,et al.Molecular markers in patients with chronicwounds to guide surgical debridement. MolMed. 2007;13(1-2):30–39.
28. Cha J, Kwak T, Butmarc J, et al. Fibroblastsfrom non-healing human chronic woundsshow decreased expression of beta ig-h3, aTGF-beta inducible protein. J Dermatol Sci.2008;50(1):15–23.
29. Wysocki AB.Wound fluids and the pathogen-esis of chronic wounds. J Wound OstomyContinence Nurs. 1996;23(6):283–290.
30. Ladwig GP, Robson MC, Liu R, Kuhn MA,Muir DF, Schultz GS. Ratios of activatedmatrix metalloproteinase-9 to tissue inhibitorof matrix metalloproteinase-1 in wound fluidsare inversely correlated with healing of pres-sure ulcers. Wound Repair Regen.2002;10(1):26–37.
31. Mwaura B, Mahendran B, Hynes N, et al.Theimpact of differential expression of extracellu-lar matrix metalloproteinase inducer, matrixmetalloproteinase-2, tissue inhibitor of matrixmetalloproteinase-2 and PDGF-AA on thechronicity of venous leg ulcers. Eur J VascEndovasc Surg. 2006;31(3):306–310.
32. Saap LJ, Falanga V. Debridement performanceindex and its correlation with complete clo-sure of diabetic foot ulcers. Wound Repair
Regen. 2002;10(6):354–359.33. Falanga V, Saap LJ, Ozonoff A. Wound bed
score and its correlation with healing ofchronic wounds. Dermatol Ther.2006;19(6):383–390.
34. Steed DL, Donohoe D,Webster MW, LindsleyL. Effect of extensive debridement and treat-ment on the healing of diabetic foot ulcers. JAm Coll Surg. 1996;183(1):61–64.
35. Ennis WJ, Meneses P. Issues impacting woundhealing at a local level: the stunned wound.Ostomy Wound Manage. 2000;46(1ASuppl):39S–48S.
36. Falanga V,Sabolinski ML.Prognostic factors forhealing of venous and diabetic ulcers.WOUNDS. 2000;12(5 Suppl A):42A–46A.
37. Panuncialman J, Falanga V. The science ofwound bed preparation. Clin Plast Surg.2007;34(4):621–632.
38. Kim BC, Kim HT, Park SH, et al. Fibroblastsfrom chronic wounds show altered TGF-beta-signaling and decreased TGF-beta Type IIreceptor expression. J Cell Physiol.2003;195(3):331–336.
39. Stoodley P,Sauer K,Davies DG,Costerton JW.Biofilms as complex differentiated communi-ties. Annu Rev Microbiol. 2002;56:187–209.
40. Wolcott RD, Rhoads DD.A study of biofilm-based wound management in subjects withcritical limb ischaemia. J Wound Care.2008;17(4):145–155.
41. Donlan RM, Costerton JW. Biofilms: survivalmechanisms of clinically relevant microorgan-isms. Clin Microbiol Rev. 2002;15(2):167–193.
42. Ferris FD, Al Khateib AA, Fromantin I, et al.Palliative wound care: managing chronicwounds across life’s continuum: a consensusstatement from the International PalliativeWound Care Initiative. J Palliat Med.2007;10(1):37–39.
43. Panuncialman J, Falanga V. Basic approach toinflammatory ulcers. Dermatol Ther.2006;19(6):365–376.
44. Kirshen C, Woo K, Ayello EA, Sibbald RG.Debridement: a vital component of woundbed preparation. Adv Skin Wound Care.2006;19(9):506–517.
45. Ayello EA, Cuddigan JE. Debridement: con-trolling the necrotic/cellular burden. Adv SkinWound Care. 2004;17(2):66–75.
46. Steed DL. Debridement. Am J Surg.2004;187(5A):71S–74S.
47. Falanga V, Iriondo M. Zinc chloride paste forthe debridement of chronic leg ulcers. JDermatol Surg Oncol. 1990;16(7):658–661.
48. Falanga V.Wound bed preparation and the roleof enzymes: a case for multiple actions of ther-apeutic agents. WOUNDS. 2002;14(2):47–57.
49. Bradley M, Cullum N, Sheldon T. Thedebridement of chronic wounds: a systematicreview. Health Technol Assess. 1999;3(17 Pt1):1–78.
50. Brem H, Balledux J, Sukkarieh T, Carson P,Falanga V. Healing of venous ulcers of longduration with a bilayered living skin substitute:results from a general surgery and dermatologydepartment. Dermatol Surg.2001;27(11):915–919.
51. Donohue K, Falanga V. Healing rate as a prog-nostic indicator of complete healing: a reap-praisal. WOUNDS. 2003;15(3):71–76.
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Falanga.qxd 6/17/08 3:53 PM Page 13
14 Supplement to OWM June 2008
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
1) What are the recent estimates of the percentage of chron-ic wounds that achieve complete closure after 20 weeks oftreatment?
a) 80%–90%b) 5%–10%c) 25%–50%d) 100%
2) What factors within the wound bed can contribute to poorhealing?
a) The presence of clinically necrotic and infected tissueb) Excessive wound exudate c) The presence of biofilm within the woundd) Abnormal and unresponsive cells at the wound edgee) All of the abovef) none of the above
3) What was the effect of debridement frequency in a clinicaltrial of the safety and efficacy of recombinant humanplatelet-derived growth factor in the treatment of chronicdiabetic ulcers?
a) There was no effectb) Centers performing the most frequent debridements had
the highest healing ratesc) Centers performing the least frequent debridements had
the lowest healing ratesd) b and c
4) True or false: There is no evidence that more frequentdebridement can help reduce amputation rates.
a) Trueb) False
5) True or false: Wounds that show a clinically adequatewound bed but are not progressing toward healing may ben-efit from debridement.
a) Trueb) False
6) Approximately what percentage of chronic wounds con-tain biofilm-embedded bacteria?
a) 100%b) 5%c) 60%d) 0%
7) What is not a method of debridement?a) Mechanical b) Magnetic c) Surgicald) Enzymatice) Biologicalf) None of the above
8) What is the primary goal of maintenance debridement?a) To keep the wound free of barriers to healingb) To maintain the size of the woundc) To control itchingd) To determine the cause of the wound
9) How long should maintenance debridement be continued?a) As long as it is effective and the wound is progressing
toward healingb) Until the wound is clear of necrotic tissuec) Until there is no sign of infectiond) All of the abovee) None of the above
10) What is a sign that the wound should be re-evaluated?a) Nonhealingb) Slow healingc) Increase in the size of the woundd) All of the abovee) None of the above
Post-Test Questions
CME Test-Small.qxd 6/17/08 3:56 PM Page 14

Supplement to OWM June 2008 15
Maintenance Debridement in the Treatment of Difficult-to-Heal Chronic Wounds
Supplement to June 2008 Ostomy Wound Management
Please print clearly: Certificate will be mailed to this address within 6–8 weeks.
Name:________________________________Degree:___________Position/Title:____________________
Organization/Institution:__________________________________________________________________
Department:___________________________________________________________________________
Mailing Address for Certificate: CHECK ONE: _____WORK _____HOME
Street:_______________________________________________________________________________
City:__________________________________________State:_______Zip Code:____________________
E-mail Address:________________________________________________________________________
Phone:______________________________________Fax:______________________________________
What other topics would be of interest to you?________________________________________________
All tests/evaluation forms must be received by June 30, 2009.
Return via fax or mail to: NACCME-Princeton CME300 Rike Drive, Suite AMillstone Township, NJ 08535Fax: 610-560-0502
Answer and Evaluation Form
Please answer the following questions by circling the appropriate rating:
5 = Strongly Agree 4 = Agree 3 = Neutral 2 = Disagree 1 = Strongly Disagree
The stated learning objectives were met 5 4 3 2 1
Faculty was knowledgeable on the subject matter 5 4 3 2 1
Content was objective 5 4 3 2 1
Content was balanced 5 4 3 2 1
Met my educational needs 5 4 3 2 1
Content was scientifically rigorous 5 4 3 2 1
Content avoided commercial bias or influence 5 4 3 2 1
Content was timely and related to my practice 5 4 3 2 1
Content will assist me in enhancing patient care 5 4 3 2 1
Information presented will improve my practice/patient outcomes 5 4 3 2 1
Answers: Refer to post-test. CircleALL that apply for each question.
1.) A B C D
2.) A B C D E F
3.) A B C D
4.) A B
5.) A B
6.) A B C D
7.) A B C D E F
8.) A B C D
9.) A B C D E
10.) A B C D E
CME Test-Small.qxd 6/17/08 3:56 PM Page 15

Falanga.qxd 6/17/08 4:59 PM Page 8

Falanga.qxd 6/17/08 4:59 PM Page 8

300 Rike Drive, Suite AMillstone Township, NJ 08535
Healthpoint Debrid Supp Cover4 6/17/08 4:00 PM Page 1