Embed Size (px)
Citation preview

Magnitude of Benefit of Endovascular Thrombectomy 6-24 Hours after Onset in Acute Ischemic Stroke Patients with Clinical-Core Mismatch
Saver Jl, Nogueira RG, Jadhav AP, Haussen DC, BonafeA, BudzikRF, Bhuva P, Yavagal DR, Ribo R, Cognard C, Haenl RA, Sila CA, Hassan AE, Liebeskind DS, Smith WS, Jovin TG, for the DAWN Investigators
Disclosures
• JLS, APJ, DCH, AB, RFB, PB, DRY, RR, CC, RA, CAS, AEH, DSL, WSS: consulting fees and
travel expenses for work advising on rigorous trial design and conduct
• RGN, TGJ: travel expenses only for work advising on rigorous trial design and conduct

Background: Patient Selection for Mechanical Thrombectomy
• Initial MT RCTs of highly effective devices generally
time-focused patient selection
• Pooled analysis - benefit rapidly decays, may be lost by 7.3 hours1
• National AHA+ESO guidelines endorsed only <6 hr window as IA
evidence2,3
• Physiologic, rather than purely time-based, selection
may identify patients >6 hr from LKW who benefit
• ~40% of AIS-LVO
• Wake-up onset
• Unclear onset time
• Witness late onset, slow progressorsunclear onset, wunclear onset time AIS-LVO
• Clinical-Core Mismatch - substantial deficits but limited infarct4
• DAWN tested this approach
1 Saver et al, JAMA. 2016 2 Powers et al, Stroke 2015 3 Wahlgren Int J Stroke 2016 et.al, 4 Jovin et.al, Stroke 2011
Outcomes = Collaterals
Time

Background: Indices of Treatment Benefit Magnitude
• DAWN
• Primary endpoint: Utility-Weighted modified Rankin Scale
• Group-level, average benefit directly interpretable
• Health-related utility, from 0% (death) to 100% (optimum health)
• Average patient xx% improvement

Background: Indices of Treatment Benefit Magnitude
• DAWN
• Primary endpoint: Utility-Weighted modified Rankin Scale
• Group-level, average benefit directly interpretable
• Health-related utility, from 0% (death) to 100% (optimum health)
• Average patient xx% improvement
• Patient-level indices of benefit also would be helpful,
for patients, physicians, policy-makers
• Benefit per hundred (BPH): among 100 patients, how many benefit?
• Number needed to treat (NNT): How many need to be treated for 1 to
benefit?
Background: Indices of Treatment Benefit Magnitude
• DAWN
• Primary endpoint: Utility-Weighted modified Rankin Scale
• Group-level, average benefit directly interpretable
• Health-related utility, from 0% (death) to 100% (optimum health)
• Average patient xx% improvement
• Patient-level indices of benefit also would be helpful,
for patients, physicians, policy-makers
• Benefit per hundred (BPH): among 100 patients, how many benefit?
• Number needed to treat (NNT): How many need to be treated for 1 to
benefit?
• Current study to derive BPH and NNT values
• Overall and in 6-12 and 12-24h time windows

Background: Indices of Treatment Benefit Magnitude
• DAWN primary results: ESOC (5/17), NEJM (11/17)
• Primary endpoint: Utility-Weighted modified Rankin Scale, 5.5 vs 3.4
• Abs diff 2.0 (95CrI 1.1-3.0), post p > 0.999
• Group-level, average benefit directly interpretable
• Health-related utility, from 0% (death) to 100% (optimum health)
• Average patient 20% improvement
• Patient-level indices of benefit also would be helpful,
for patients, physicians, policy-makers
• Benefit per hundred (BPH): among 100 patients, how many benefit?
• Number needed to treat (NNT): How many need to be treated for 1 to
benefit?
• Current study to derive BPH and NNT values
• Overall and in 6-12 and 12-24h time windows
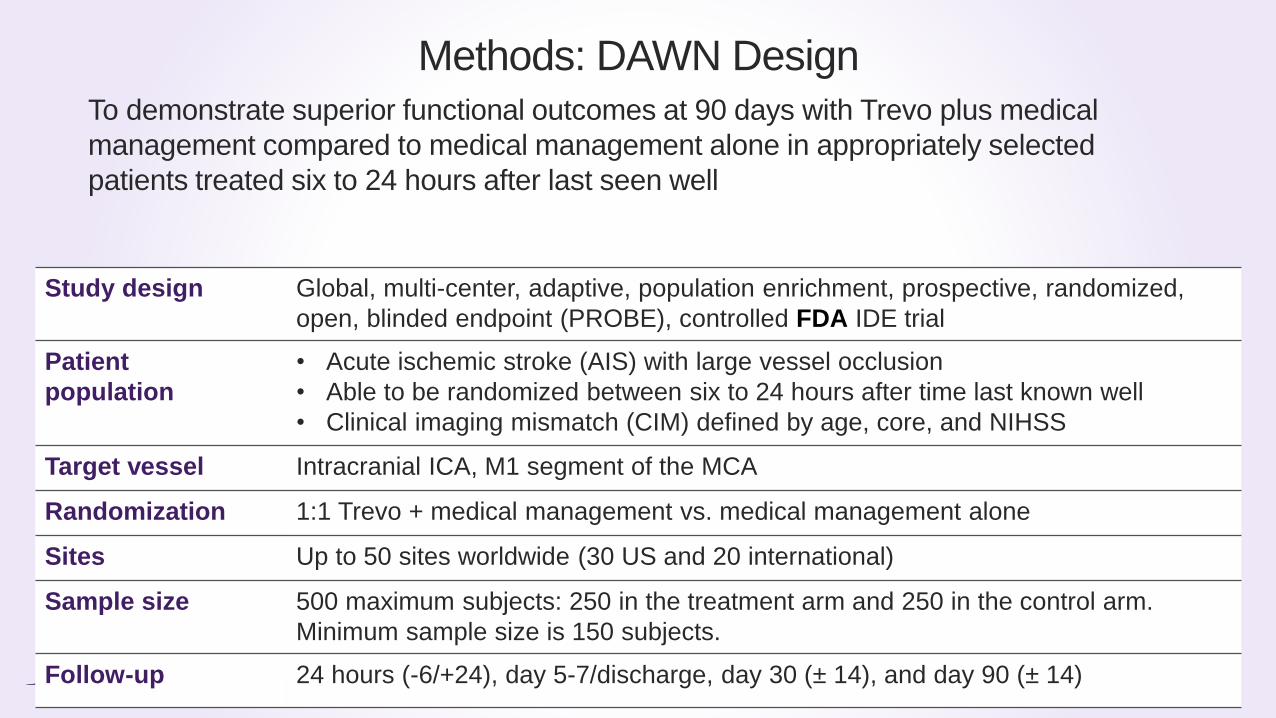
Study design Global, multi-center, adaptive, population enrichment, prospective, randomized,
open, blinded endpoint (PROBE), controlled FDA IDE trial
Patient
population
• Acute ischemic stroke (AIS) with large vessel occlusion
• Able to be randomized between six to 24 hours after time last known well
• Clinical imaging mismatch (CIM) defined by age, core, and NIHSS
Target vessel Intracranial ICA, M1 segment of the MCA
Randomization 1:1 Trevo + medical management vs. medical management alone
Sites Up to 50 sites worldwide (30 US and 20 international)
Sample size 500 maximum subjects: 250 in the treatment arm and 250 in the control arm.
Minimum sample size is 150 subjects.
Follow-up 24 hours (-6/+24), day 5-7/discharge, day 30 (± 14), and day 90 (± 14)
Methods: DAWN DesignTo demonstrate superior functional outcomes at 90 days with Trevo plus medical
management compared to medical management alone in appropriately selected
patients treated six to 24 hours after last seen well

- Age 18
- NIHSS ≥10
- Pre-mRS 0-1
- TLSW to
Randomization:
6-24h
RAPID CTP/DWI CIM:
A. 80 y/o:
1. NIHSS 10 + core <21cc
B. <80 y/o:
2. NIHSS 10 + core <31cc
3. NIHSS 20 + core <51cc
1:1
Randomization:- CIM subgroup
- ICA-T vs M1
- 6-12 vs 12-24h
Control
Thrombectomy
90-day
mRS
Study Methods: Workflow
NCCT/DWI:
<1/3 MCA Territory
CTA/MRA:
ICA-T and/or MCA-M1(Tandem Occlusions Allowed)
Informed
Consent
- U-W mRS
- mRS 0-2
6-24h

TRIAL STOPPED FOR AT FIRST INTERIM EFFICACY ANALYSIS:
OVERWHELMING EFFICACY IN 1ST 200 PATIENTS

DAWN Trial Utility-Weighted mRS
Utility weighted mRS
• Better captures health state transitions across the entire spectrum
• Patient-centered outcomes analysis
Minimal Clinically Important Difference (MCID)
• MCID for health-related utility is well-established: 0.31
• 5 transitions on the mRS are clinically valuable
– 1 transition not clinically valuable, from mRS 6 to mRS 5
mRS 0 1 2 3 4 5 6
Weight 10 9.1 7.6 6.5 3.3 0 0
1 Kaplan et al, Health Serv Res 1976;11:478-507; Kaplan, COPD 2005;2:91-7 (0.3 value is scaled to 0-10 range of UW-mRSversion used in DAWN)

BPH and NNT Derivations
• Analyzed age, NIHSS, and core-adjusted 90d distributions
• For all dichotomized cutpoints of the mRS
• NNT and BPH values by calculating inverse of absolute risk difference
• For improvements on the UW-mRS (= improvements by 1 or
more levels across all steps of the 6 level mRS)
• NNT and BPH values by automated joint outcome table resampling
• R function “xsample” used to randomly sample values of the vector “x” from all possible joint
outcome table solutions
• Using the mirror algorithm, 3000 samples were taken from the large population of all possible
solutions, without replacement.
• Mean and range NNTB values were calculated for these random samples from all possible NNTB
values under the constraints
Endo
0 1 2 3 4 5+6
0 20 20
1 39 39
No Endo 2 19 19
3 208 208
4 317 317
5+6 397 397
20 39 19 208 317 397
Endo
0 1 2 3 4 5+6
0 40 40
1 11 40 51
No Endo 2 5 28 7 40
3 24 78 46 14 162
4 10 69 99 85 80 343
5+6 4 9 16 32 51 252 364
94 224 168 131 131 252
Endo
0 1 2 3 4 5+6
0 40 40
1 3 48 51
No Endo 2 4 6 30 40
3 22 63 35 42 162
4 17 85 85 64 92 343
5+6 8 22 18 25 39 252 364
94 224 168 131 131 252
Automated joint outcome table multiple resampling

Results

DAWN Treatment Group-Level Differences
Entire DAWN Cohort
mRS (6 level)Stacked Bar Chart

DAWN Treatment Group-Level Differences
Entire DAWN Cohort
mRS (6 level)Stacked Bar Chart
UW-mRSUtility Staircase Plot

mRS Outcomes – Entire DAWN Cohort
Outcome mRS BPH
Dichotomized
Asymptomatic 0 5
Freedom from Disability 0-1 23
Functional Independence 0-2 36
Ambulatory 0-3 32
Not Requiring Constant Care 0-4 11

mRS Outcomes – Entire DAWN Cohort
Outcome mRS BPH NNT
Dichotomized
Asymptomatic 0 5 19
Freedom from Disability 0-1 23 4
Functional Independence 0-2 36 3
Ambulatory 0-3 32 3
Not Requiring Constant Care 0-4 11 9

mRS Outcomes – Entire DAWN Cohort
Outcome mRS BPH NNT
Dichotomized
Asymptomatic 0 5 19
Freedom from Disability 0-1 23 4
Functional Independence 0-2 36 3
Ambulatory 0-3 32 3
Not Requiring Constant Care 0-4 11 9

mRS Outcomes – Entire DAWN Cohort
Outcome mRS BPH NNT
Dichotomized
Asymptomatic 0 5 19
Freedom from Disability 0-1 23 4
Functional Independence 0-2 36 3
Ambulatory 0-3 32 3
Not Requiring Constant Care 0-4 11 9
Entire Range
Lower Disability 0/1/2/3/4/5+6 50 2

mRS Outcomes – Entire DAWN Cohort
Outcome mRS BPH NNT
Dichotomized
Asymptomatic 0 5 19
Freedom from Disability 0-1 23 4
Functional Independence 0-2 36 3
Ambulatory 0-3 32 3
Not Requiring Constant Care 0-4 11 9
Entire Range
Lower Disability 0/1/2/3/4/5+6 50 2

mRS Outcomes – Entire DAWN Cohort
Outcome mRS BPH NNT
Dichotomized
Asymptomatic 0 5 19
Freedom from Disability 0-1 23 4
Functional Independence 0-2 36 3
Ambulatory 0-3 32 3
Not Requiring Constant Care 0-4 11 9
Entire Range
Lower Disability 0/1/2/3/4/5+6 50 2
For every 100 DAWN-like patients treated, thrombectomy yields improved
disability-related quality of life in 50, including functional independence in 36.

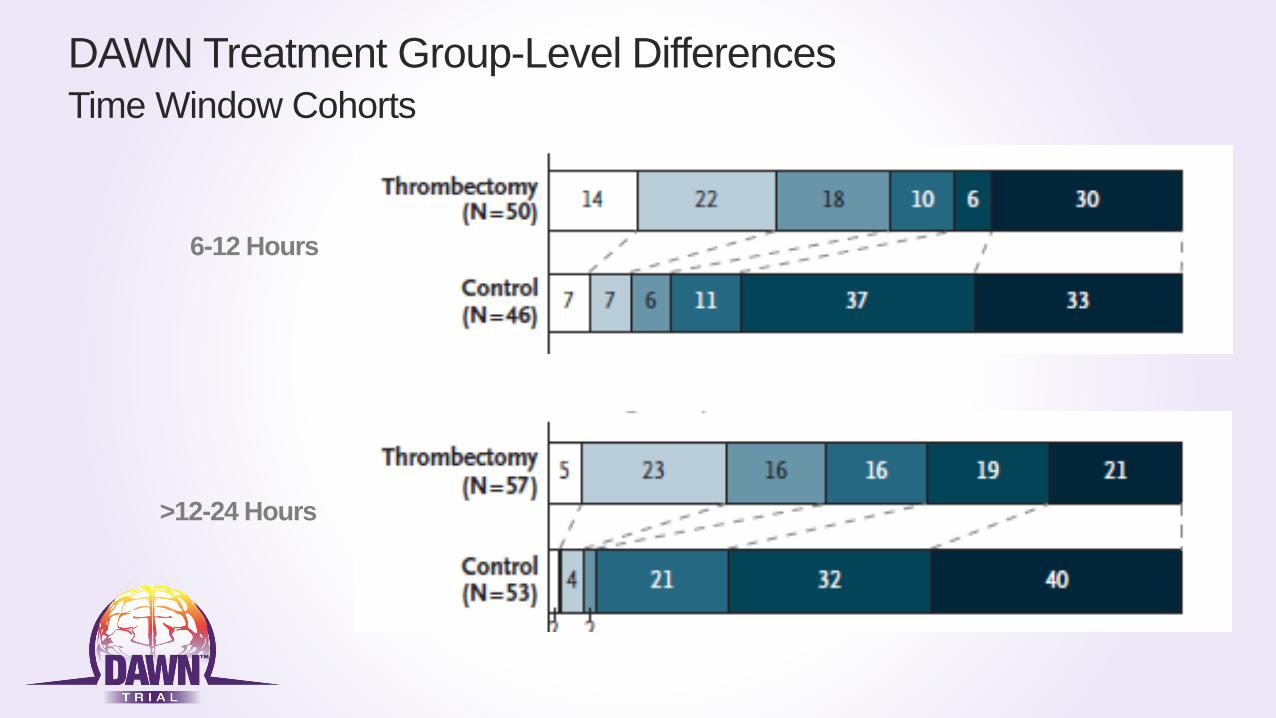
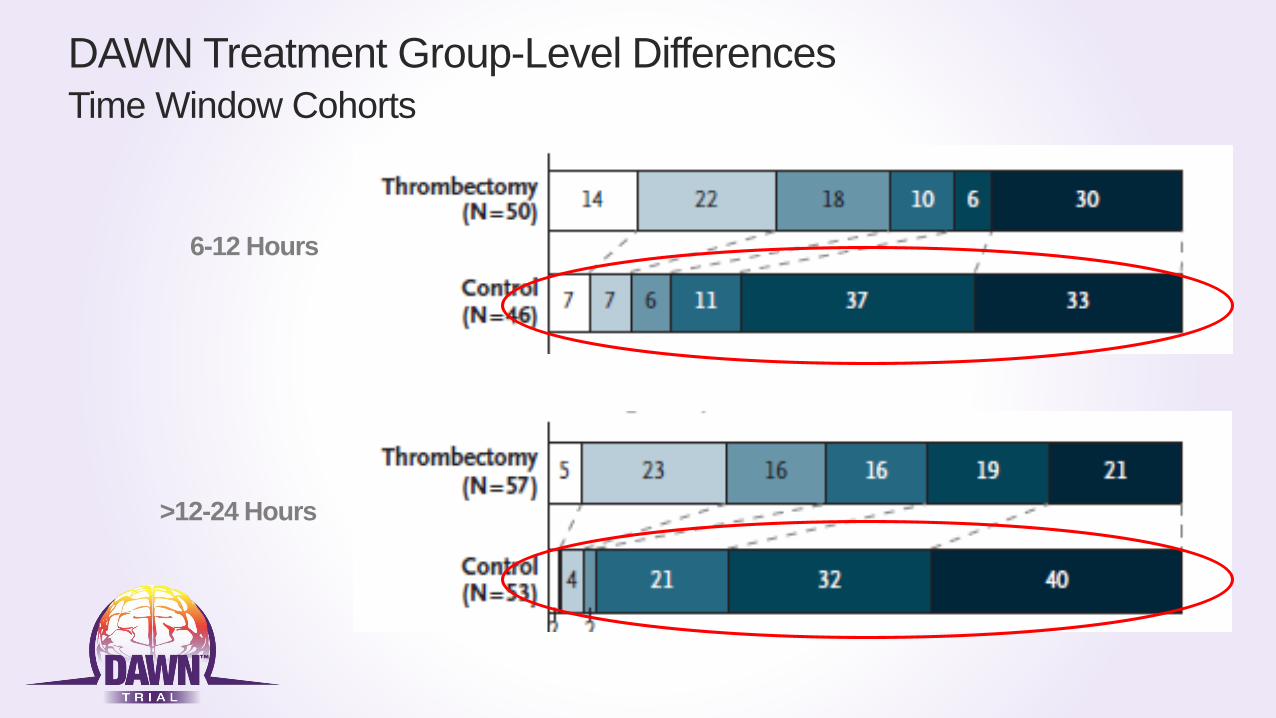
DAWN Treatment Group-Level Differences
Time Window Cohorts
6-12 Hours
>12-24 Hours

mRS Outcomes – DAWN Time Window Cohorts
6-12 Hrs >12 – 24 Hrs
Outcome mRS BPH BPH
Dichotomized
Asymptomatic 0 7 3
Freedom from Disability 0-1 22 22
Functional Independence 0-2 33 36
Ambulatory 0-3 33 31
Not Requiring Constant Care 0-4 2 19

mRS Outcomes – DAWN Time Window Cohorts
6-12 Hrs >12 – 24 Hrs
Outcome mRS BPH NNT BPH NNT
Dichotomized
Asymptomatic 0 7 14 3 33
Freedom from Disability 0-1 22 5 22 5
Functional Independence 0-2 33 3 36 3
Ambulatory 0-3 33 3 31 3
Not Requiring Constant Care 0-4 2 44 19 5

mRS Outcomes – DAWN Time Window Cohorts
6-12 Hrs >12 – 24 Hrs
Outcome mRS BPH NNT BPH NNT
Dichotomized
Asymptomatic 0 7 14 3 33
Freedom from Disability 0-1 22 5 22 5
Functional Independence 0-2 33 3 36 3
Ambulatory 0-3 33 3 31 3
Not Requiring Constant Care 0-4 2 44 19 5
Entire Range
Lower Disability 0/1/2/3/4/5+6 45 2 56 2
DAWN Treatment Group-Level Differences
Time Window Cohorts
6-12 Hours
>12-24 Hours
DAWN Treatment Group-Level Differences
Time Window Cohorts
6-12 Hours
>12-24 Hours

DAWN Treatment Group-Level Differences
Time Window Cohorts
6-12 Hours
>12-24 Hours

Discussion: Comparison with Other Thrombectomy Trials
DAWN
Disability-Related QoL(UW-mRS)
Level of Disability (mRS shift analysis)
Benefit Per Hundred*(Shift+Fxn Ind)
49 (36 /14)
*In comparative analyses, BPH values were calculated using the algorithmic min-max joint outcome table method (rather than the multiple resampling joint outcome table method)

Discussion: Comparison with Other Thrombectomy Trials – 1A
DAWN
HERMES 2H
Disability-Related QoL(UW-mRS)
Level of Disability (mRS shift analysis)
Benefit Per Hundred*(Shift+Fxn Ind)
49 (36 /14)
51 (32 /18)
*In comparative analyses, BPH values were calculated using the algorithmic min-max joint outcome table method (rather than the multiple resampling joint outcome table method)

Discussion: Comparison with Other Thrombectomy Trials – 1B
Disability-Related QoL(UW-mRS)
Level of Disability (mRS shift analysis)
Benefit Per Hundred*(Shift+Fxn Ind)
DAWN
HERMES 5H
49 (36 /14)
33 (14 /19)
*In comparative analyses, BPH values were calculated using the algorithmic min-max joint outcome table method (rather than the multiple resampling joint outcome table method)

Discussion: Comparison with Other Thrombectomy Trials - 2
Disability-Related QoL(UW-mRS)
Level of Disability (mRS shift analysis)
Benefit Per Hundred*(Shift+Fxn Ind)
49 (36 /14)
48 (29 /19)
*In comparative analyses, BPH values were calculated using the algorithmic min-max joint outcome table method (rather than the multiple resampling joint outcome table method)

Conclusions
• Endovascular thrombectomy with the Trevo device at 6-24h in patients with
clinical-core mismatch confers benefit of substantial magnitude, improving 90 day
disability levels in one-half of patients, including conferring functional
independence in one-third.
• Benefit is substantial in both the 6-12h and >12-24h time windows, with about half
of patients benefitting in both periods. But earlier patients do better in both the
thrombectomy and control groups.
• The proportion of patients benefitting in DAWN is similar in magnitude to that
observed in broadly screened patients selected for treatment at 2h, and
substantially higher than that seen for broadly selected patients at 5h.

Enrolling CentersNorth America
1. Abington Memorial, PA
2. Baptist Jacksonville, FL
3. Buffalo, NY
4. Capital Health Trenton, NJ
5. Christiana Delaware, DE
6. CPMC San Francisco, CA
7. Erlanger ,Chattanooga, TN
8. Florida Hospital, FL
9. Grady Atlanta, GA
10. JFK, Edison, NJ
11. Kaiser LA
12. Kennestone, Marietta GA
13. KUMC Kansas City, KA
14. Lexington Memorial, KY
15. Riverside, OH
16. Rush, IL
17. St. Joseph Mercy MI
18. Texas Stroke Institute TX
19. Toronto Western, ON
20. UCLA, CA
21. UH Cleveland, OH
22. University of Miami, FL
23. UPMC, PA
24. Valley Baptist, TX
Europe
26. Bellvitge Barcelona
27. Germans Trias Barcelona
28. Gui de Chauliac Montpellier
29. Hopital Purpan Toulouse
30. Hospital Clinic Barcelona
31. Vall d'Hebron Barcelona
Australia
32. Royal Melbourne Hospital
0
0
0
0
1
1
1
1
1
1
2
2
2
3
5
5
5
5
5
7
7
7
7
7
9
10
14
14
38
46
0 5 10 15 20 25 30 35 40 45 50 55 60
Lexington (PI: GIven, ATE 08/29/16) - 0 SPM
Kennestone (PI: Gupta, ATE 09/01/16) - 0 SPM
UCLA (PI: Starkman, ATE 11/21/16) - 0 SPM
Hospital Clinic (PI: Urra, ATE 02/22/17) - 0 SPM
JFK (PI: Kirmani, ATE 02/15/17) - 1.9 SPM
Capital (PI: Vez, ATE 07/01/14) - 0 SPM
Florida Hospital (PI: Hellinger, ATE 11/09/15) - 0.1…
Kaiser LA (PI: Feng, ATE 11/19/15) - 0.1 SPM
KUMC (PI: Abraham, ATE 02/01/16) - 0.1 SPM
Bellvitge (PI: Cardona, ATE 01/31/17) - 1 SPM
Erlanger (PI: Devlin, ATE 06/05/15) - 0.1 SPM
Memorial Regional (PI: Mehta, ATE 02/26/16) - 0.2…
Toronto Western (PI: Silver, ATE 08/26/16) - 0.3 SPM
Abington (PI: Shah, ATE 10/29/15) - 0.2 SPM
CPMC (PI: English/Barazangi, ATE 05/05/15) - 0.2…
Rush (PI: Chen, ATE 05/07/15) - 0.2 SPM
Royal Melbourne (PI: Mitchell, ATE 11/12/15) - 0.3…
Buffalo (PI: Levy, ATE 12/01/15) - 0.3 SPM
Germans Trias I Pujol Badalona (PI: Millán Torné ,…
Valley Baptist (PI: Hassan, ATE 03/31/15) - 0.3 SPM
UH Cleveland (PI: Sila, ATE 05/04/15) - 0.3 SPM
Baptist Jacksonville (PI: Hanel, ATE 01/21/16) - 0.5…
Hopital Purpan Toulouse (PI: Cognard, ATE…
Vall d'Hebron Barcelona (PI: Ribo, ATE 05/19/16) -…
University of Miami (PI: Yavagal, ATE 09/01/16) -…
Texas Stroke Institute (PI: Bhuva, ATE 04/10/15) -…
Gui de Chauliac Montpellier (PI: Bonafe, ATE…
Riverside (PI: Budzik, ATE 08/28/14) - 0.5 SPM
Grady (PI: Nogueira/Hassen, ATE 11/25/14) - 1.4 SPM
UPMC (PI: Jadhav, ATE 10/31/14) - 1.6 SPM

SPECIAL ACKNOWLEDGEMENTS STRYKER NEUROVASCULAR DAWN CLINICAL TEAM
• Alice Lin, CRA, Lead Clinical Research Associate
• Patricia Morgan, BSN, RN, Lead Clinical Research Associate
• Ryan Shields, MSc, Sr. Manager, Data Management and Biostatistics
• Christine Toruno MSc, DAWN Project Manager

Thank youto all DAWN investigators, patients and families





























