Embed Size (px)
Citation preview

ANRV317-BE09-12 ARI 7 June 2007 18:44
Magnetic Resonance–Compatible Robotic andMechatronics Systems forImage-Guided Interventionsand Rehabilitation:A Review StudyNikolaos V. Tsekos,1 Azadeh Khanicheh,2
Eftychios Christoforou,1
and Constantinos Mavroidis2
1Cardiovascular Imaging Laboratory, Mallinckrodt Institute of Radiology,Washington University, St. Louis, Missouri 63110; email: [email protected] and Mechatronics Laboratory, Department of Mechanical & IndustrialEngineering, Northeastern University, Boston, Massachusetts 02115;email: [email protected]
Annu. Rev. Biomed. Eng. 2007. 9:351–87
First published online as a Review in Advance onApril 17, 2007
The Annual Review of Biomedical Engineering isonline at bioeng.annualreviews.org
This article’s doi:10.1146/annurev.bioeng.9.121806.160642
Copyright c© 2007 by Annual Reviews.All rights reserved
1523-9829/07/0815-0351$20.00
Key Words
medical robotics, MR-compatible actuators, MR-compatiblesensors, functional MRI
AbstractThe continuous technological progress of magnetic resonance imag-ing (MRI), as well as its widespread clinical use as a highly sensi-tive tool in diagnostics and advanced brain research, has broughta high demand for the development of magnetic resonance (MR)-compatible robotic/mechatronic systems. Revolutionary robotsguided by real-time three-dimensional (3-D)-MRI allow reliable andprecise minimally invasive interventions with relatively short recov-ery times. Dedicated robotic interfaces used in conjunction withfMRI allow neuroscientists to investigate the brain mechanisms ofmanipulation and motor learning, as well as to improve rehabili-tation therapies. This paper gives an overview of the motivation,advantages, technical challenges, and existing prototypes for MR-compatible robotic/mechatronic devices.
351
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
Contents
INTRODUCTION. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 352Advantages of MRI in Image-Guided Interventions . . . . . . . . . . . . . . . . . . 352Advantages of MRI/fMRI in Neuroscience
and Rehabilitation Therapies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 353Motivation for MR-Compatible Interventional Robotic Systems . . . . . . 354Motivation for MR-Compatible Robotic Rehabilitation Systems . . . . . . 355
THE MRI TECHNOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 356MR-Scanners, MR-Safety, and MR-Compatibility. . . . . . . . . . . . . . . . . . . . 356MR-Compatible Materials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 358MR-Compatible Actuators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 358MR-Compatible Sensors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 361Testing the MR Compatibility of Mechatronic Systems . . . . . . . . . . . . . . . 361
MR-COMPATIBLE ROBOTIC AND MECHATRONIC SYSTEMS . . 362Research and Development in MR-Compatible Interventional
Robotic Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 362Research and Development in MR-Compatible Rehabilitation
Robotic Devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 367Procedure Planning and Guidance of MR-Compatible Interventional
Robotic Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 376DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 377
INTRODUCTION
Magnetic resonance imaging (MRI) is one of the most versatile modalities in mod-ern diagnostic medicine and an indispensable tool in a wide range of clinical andbasic science research. Among the emerging biomedical engineering areas of cur-rent development in MRI are the performance of image-guided interventions (IGI),the mapping of brain activity in neuroscience studies, and the monitoring of theprogress of rehabilitation therapies (1–7). Within the field of interventional MRI, anew direction is the use of remotely actuated and controlled devices to assist in theperformance of interventions (8–25). The use of MRI in IGI, neuroscience studies,and monitoring of rehabilitation procedures shares common benefits and challenges,both originating from the inherent properties of this modality. The MRI scanneremploys extreme magnetic fields, rapidly changing magnetic field gradients, and ra-diofrequency pulses. As a result, the commonly used robotic and mechatronic systemsare not suitable for MRI applications, resulting in a need for a new generation of de-vices: the MR-compatible systems.
Advantages of MRI in Image-Guided Interventions
The gold standard modalities in interventional medicine are the X-ray-based flu-oroscopy and computer tomography (CT) and ultrasound. Compared with those
352 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
modalities, MRI provides several benefits that make it attractive for guiding inter-ventions. First, MRI offers a plethora of soft-tissue contrast mechanisms that allowthe assessment of both anatomical morphology and function. Among the morphologymethods is the high-quality magnetic resonance angiography (MRA) using exogenousMR contrast agents or even the tissue water as an endogenous contrast agent. Regard-ing function, the modality offers methods such as the assessment of tissue perfusionand blood oxygen level–dependent (BOLD) (26, 27) and water tissue diffusion (28,29). As a result, MRI provides the methods for a comprehensive diagnosis and char-acterization of tissue pathophysiology, as well as the delineation of targets for biopsiesand therapeutic interventions. In addition, contrast mechanisms, such as MR perfu-sion and thermometry, allow for monitoring the effects of procedures, such as thermaland cryo-ablations (e.g., 30–34). Second, MRI is an intrinsically three-dimensional (3-D) modality that allows unrestricted selection of oblique 3-D or multislice imaging.Such capability may better suit the visualization of a procedure, without constraintsor the need to manually reposition the patient or the imaging instrument as in thecase of X-ray fluoroscopy. Recent technological advancements in modern MR scan-ners allow the dynamic “on-the-fly” adjustment of the imaging planes and volumes, acapability that has been exploited in interventional MRI (35–40). This feature can beused to dynamically follow the movement of a MR-compatible interventional roboticdevice, thereby allowing a freehand dynamic guidance and control of the procedure,in a similar way with handheld ultrasound (11). Third, MRI does not use ionizingradiation and therefore is safer for the patient and medical staff. Another feature ofMRI is that the quality of images is independent of the expertise of the operator, as isthe case of ultrasound. In principle, MRI provides the means for single-modality andsingle-session-based procedures that integrate (a) diagnosis for identification of tissuepathophysiology and delineation of the targeted lesion; (b) guidance of the appropriateintervention, including positioning the tool and monitoring tissue-properties alter-ing procedures, such as thermal ablations; and (c) assessment of the results of theinterventional procedure. In view of the above benefits offered by MRI, major effortis devoted to the development and assessment of its clinical potential and merit inguiding interventional procedures (1–4, 41–43).
Advantages of MRI/fMRI in Neuroscienceand Rehabilitation Therapies
The recent discovery that MRI can be used to map changes in brain hemodynam-ics that correspond to mental operations extends traditional anatomical imaging toinclude maps of human brain function. A new technique called functional magneticresonance imaging (fMRI) allows observation of the structures and determinationof which structures participate in specific functions. This technique provides sev-eral benefits that make it an attractive tool in neuroscience and the investigation ofthe neurobiological changes occurring during rehabilitation therapy. First, fMRI canmeasure the brain anatomy and blood flow simultaneously. The most commonly usedfMRI technique measures brain activation over the BOLD effect. BOLD imagingrelies on sensitivity to changes in oxygen levels within the circulating blood. These
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 353
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
changes presumably reflect changes in neural activity that are accompanied by changesin blood flow. fMRI has particular spatial and temporal advantages over other imagingmodalities. fMRI offers imaging with temporal resolution on the order of seconds.The spatial resolution of BOLD and other fMRI methods is typically 1–4 mm, whichis better than most functional imaging methods, such as positron emission tomog-raphy (PET) and single photon emission computerized tomography (SPECT) (44).Second, fMRI can record brain signals noninvasively and without risks of radiationinherent in other scanning methods, such as CT scans. Also, the signal does not re-quire injections of radioactive isotopes, such as PET. Noninvasiveness and relativesafety of the technique allow repeated studies to be carried out within a given subjectso that important questions, such as the ability of the brain to adapt with time, can beaddressed (45). In studies of how a motor skill is learned, for example, fMRI followsthe way the brain changes functionally over time, contributing to an understandingof which brain circuits are involved in developing the skills (46). This approach hasbeen used to investigate both how healthy subjects learn new complex tasks (47) andalso to understand how people with initially disabling neurological disease, such asa stroke, improve functionally over time (48). The clinical relevance of fMRI alsohas been strengthened by recent experiments that have explored the neurobiologicalbasis of specific rehabilitation strategies associated with the recovery of function (49).Third, BOLD fMRI is a relative technique in that it must compare images takenduring one state with another (or a control condition) to create a meaningful picture.As images are acquired very rapidly, one can acquire enough images to measure therelative differences between two states to perform a statistical analysis within a singleindividual. BOLD-fMRI paradigms generally have several periods of rest alternatingwith several periods of activation. Images are then compared over the entire activationwith the rest periods. Therefore, one can make statistical statements in comparingdifferent states within an individual in a single session.
Motivation for MR-Compatible Interventional Robotic Systems
Despite the aforementioned advantages, MRI presents an important impediment inthe practice of IGI: limited access to the patient. Patient accessibility depends onthe particular design of the employed magnet. The open-type scanners offer thebest access to the patient. With a vertical arrangement of the magnet poles, thesesystems offer sideways or all-around accessibility to the patient, even though thevertical distance between the poles is in the range of 40 to 45 cm. However, theirlow magnetic fields, in the range of 0.02–0.7 Tesla, result in a lower available sig-nal and slower speeds of image acquisition (a new commercial open system is a 1.0Tesla). Although it is not commercially available anymore, a special 0.5 Tesla MRscanner known as double-donut or split bore offers a vertical 50-cm-wide gap inbetween two facing superconductive magnets for direct access to the patient. Themost widely used, the cylindrical scanners are based on superconductive magnetsthat have a horizontal bore with typical diameters of 60 cm and lengths 1.20 to 2.0 m(a new commercial system offers 70 cm). Although access to the patient throughthe openings of the gantry is exceptionally limited, these scanners use magnetic field
354 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
strengths of 1.0 to 3.0 Tesla, offering the best available signal and magnetic fieldhomogeneity.
The current practice of performing MR-guided procedures with cylindrical scan-ners entails removing the patient from the scanner and using preoperative MRIroadmaps and fudicial markers for aiming the tool. This approach does not use real-time imaging for guidance, and as a result has certain drawbacks. First, the approachto the targeted lesion may not be accurate because as the interventional tool advancesit dislocates the tissue depending on the material properties of the tissue and thespeed of advancement (1, 16, 20–23). This alters the local anatomy and position ofthe target and the surrounding tissue, making these roadmaps “obsolete.” In additionto suboptimal accuracy, for example, when sampling tissue from small lesions, thisapproach may also induce undesirable trauma on healthy tissue or hemorrhage. Sec-ond, the practice may require longer procedures and induce additional discomfortto the patient. Specifically, after the insertion of the interventional tool using thepreoperative roadmaps, the patient should be reinserted into the MRI scanner andimaged to validate the accurate placement of the tool. Subsequently, the patient isremoved either to complete the procedure (if the placement is correct) or to adjustthe position of the tool by appropriate maneuvering, which may include its removaland reinsertion. This procedure may need to be repeated more than once, resultingin increased duration and cost of the procedure, surgical trauma, and chances forcomplications (4).
Access to the patient is not a problem with X-ray fluoroscopy and ultrasound,which allow real-time guidance. To address this critical limitation of MRI and fa-cilitate real-time guidance of IGI, remotely actuated and controlled MR-compatiblemanipulators have been introduced (8–10, 12–18, 20–25). With these devices, theentire or part of a procedure, such as the alignment of the tool with the desired inser-tion path, can be performed while the patient remains inside the MR scanner. Thisprovides real-time visualization of the procedures and, therefore, allows improvedtargeting while capitalizing on the improved contrast offered by the modality. Be-yond addressing the patient accessibility, manipulators offer general benefits such assteadiness and accuracy (13, 15, 21, 43, 50, 51). Currently, several examples of MR-compatible interventional robotic systems have been presented for brain biopsies (18),breast interventions (14, 17, 52), endoscope manipulation (15), prostate procedures(9, 22, 23), and general purpose systems for use with standard cylindrical MR scanners(13, 53).
Motivation for MR-Compatible Robotic Rehabilitation Systems
High-spatial-resolution images of neural activity in a noninvasive manner in fMRImake it possible to study cortical reorganization throughout the recovery process ofpatients with stroke, traumatic brain injury, and other neurological disorders. In thefield of human motor control, data on brain activation have confirmed and extendedthe findings of previous electrophysiological studies in animals and patients who un-derwent neurological surgery (54, 55). In recent years, the use of fMRI to explorebrain plasticity following neurological injury has continued to rise (56). Functional
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 355
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
activation tasks commonly utilized during fMRI include making a fist (57), fingertapping (58), wrist extension (59), wrist passive flexion–extension (60), arm flexion–extension (61), finger flexion–extension (49), sequential finger tapping with opposi-tion (57), and tracking a sine wave with the finger (62, 63). Unfortunately these tasksmay not provide optimally controlled studies within subjects whose motor functionis changing over the time of repeated tests or across subjects because normalizationand repeatability of each task in terms of speed, kinematics, forces, etc., are especiallydifficult to accomplish in impaired subjects. Additionally, in most cases fMRI stud-ies require MR-compatible devices to record and/or generate limb movements andforces. One way to address these shortcomings is to utilize robotic/mechatronic inter-faces capable of producing computer-controlled dynamics during movement. Thesedevices allow (a) the standardization of study condition, (b) the quantification of be-havioral outcomes, and (c) the simulation of movements and setups used in specificclinical training routines (64).
fMRI is commonly performed using gradient echo–echo planar imaging (GE-EPI)sequences, which are even more sensitive than anatomical MRI sequences as theymeasure heterogeneities of the magnetic field. Heterogeneities of the magnetic fieldcreated by the presence of a mechatronic device lead to time-varying image distortionand signal loss and can be falsely associated with neural activation. Additionally, thefast switching gradients and high static magnetic field required for functional imagingincrease electromagnetic compatibility constraints. It should be considered, wheninteracting with human subjects during functional imaging, that there is a limitedspace within the scanner bore (typical diameter of 60 cm) and the subject must becomfortable with the mechatronic device while performing the task. In addition, usingthe device should not create any movement artifacts. Despite all these difficultiesand challenges, several MR-compatible robotic/mechatronic interfaces for use infMRI studies have been introduced in the past few years. These devices that enableneurologists to investigate motor performance and the mechanisms of neural recoveryfollowing neurological injuries, such as stroke, can be distinguished in three types:(a) manipulandums with actuators (65–67), (b) force or/and motion sensing systems(68–71), and (c) tactile stimulators (72–74).
THE MRI TECHNOLOGY
MR-Scanners, MR-Safety, and MR-Compatibility
The development and use of MR-compatible devices are very challenging tasks owingto the nature of the modality, which uses high magnetic fields, fast-switching magneticfield gradients, and radiofrequency pulses, as well as being very sensitive to externalnoise. The MR scanner uses a strong static magnetic field to polarize the nuclear spinsof the observed nuclei; the higher the magnetic field, the higher the polarization ofthe spins, thus, the higher the available MR signal. As discussed previously, standardclinical MR scanners use magnetic field strengths as high as 3.0 Tesla. During thepast 15 years, to further improve signal-to-noise ratio (SNR) and better elucidateand explore contrast mechanisms, the trend has been toward even higher magnetic
356 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
fields, and we have witnessed the introduction of human systems for investigationalpurposes at 7.0 Tesla (75) and recently as high as 9.4 Tesla and beyond. These strongmagnetic fields result in extremely hazardous conditions: High forces can be exertedon ferrous apparatuses and interventional tools, making them harmful projectiles forthe patient, medical personnel, and the instruments (76–78). Beyond being hazardous,ferromagnetic materials inside the MR scanner also affect the homogeneity of themain magnetic field, resulting in substantial loss of the signal. Susceptibility artifactscan also be induced by paramagnetic materials when their susceptibility is differentfrom that of the tissue. In addition to the static main magnetic field, the MR scanneruses rapidly varying magnetic field gradients for spatial encoding during the imagingsequence. These gradient magnetic fields can induce electrical fields and currents(eddy-currents) inside conductive materials. These eddy-currents may alter the localhomogeneity of the main magnetic field and severely affect the quality and linearity ofMR images (78–82). Moreover, the MR scanners apply radiofrequency (RF) pulses toexcite and manipulate the polarized spins for the collection of the MR signal. TheseRF pulses, as well as the magnetic field gradients, can heat interventional tools thatcontain conductive elements, such as needles or catheters, and become an additionalrisk to the patient.
MRI is very sensitive to electromagnetic noise; to prevent deterioration of theimage SNR, the entire scanner rooms are highly shielded Faraday cages. Such elec-tromagnetic noise may originate from electronic equipment needed for the operationof mechatronic devices when they reside inside the MR scanner room. Even wiresthat pass from the outside to the inside of the scanner room can create problemsbecause wires act as antennas that radiate electric noise. These environmental con-ditions require the careful selection of construction materials, actuation assemblies,sensors, and shielding of electronics.
The literature agrees, in general terms, about the definitions of MR safety andcompatibility of an object or device (e.g., 10, 17, 25, 76–78, 82–84). A device is MRsafe inside the MR environment when it does not present any additional risk to thepatient. The MRI environment includes the space inside and outside the gantry ofthe scanner. This definition of MR safety does not refer to any potential effects ofthe device on the MR images, i.e., a MR-safe device may affect the quality of theimages. The effect of the device on the MR images is included in the definition of itsMR compatibility. A device is MR compatible when, in addition to being MR safe, itspresence and/or operation does not significantly affect the quality of the MR imagesand, inversely, its operation is not affected by the MR scanner. Reviews of the MRI-related safety issues can be found in References 76–78, 81–83. Of course, the relevanceof MR-compatibility and safety is not only limited to mechatronic systems but extendsto any device exposed to the MRI environment. For example, electronic devices usedin the MRI environment should be immune to the static magnetic field, the gradients,and the radiofrequency pulses of the scanner to avoid possible malfunctions, such asinduced activations, deactivations, and damage. Examples of such devices pertinent tothe patient safety are implantable cardiac pacemakers and drug infusion pumps (85).The MR compatibility of mechatronic devices was examined in Reference 86, andcertain types of materials and devices were experimentally evaluated. When an object
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 357
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
or device is characterized as MR safe or MR compatible, the exact conditions underwhich testing took place need to be clearly stated. It is likely that different behaviormay be exhibited under more extreme MR conditions, different types of scanners,etc.
MR-Compatible Materials
Materials most often used in the construction of conventional robotic and mecha-tronic systems are ferromagnetic (e.g., carbon steel) because of their desirable me-chanical properties, such as strength, rigidity, and machinability. However, these ma-terials are, in general, not suitable for the construction of MR-compatible devices.Ferromagnetic materials are subject to strong magnetic forces and can become po-tentially dangerous projectiles if they are placed close to the MR scanner withoutbeing securely attached to a fixed structure. Another source of MR-incompatibilityis the generation of eddy-currents inside conductive materials, such as aluminum,which may cause image artifacts. Eddy-currents may also cause unwanted heating ofthe materials, resulting in burns (81, 87).
Materials suitable for MR-compatible devices are nonmagnetic and nonconduc-tive. Combinations of plastic, ceramic, fiberglass, carbon fiber, and other compositeshave been extensively used for the development of MR-compatible systems. A maindrawback associated with many of these materials is their limited structural stiffness,which can have a negative effect on the manipulability and accuracy of robotic andmechatronic devices. In many robotic/mechatronic systems developed for MRI appli-cations, a limited number of metallic parts (such as aluminum, copper, and stainlesssteel) have often been incorporated into the otherwise MR-compatible structures(e.g., 14, 18, 23). MR compatibility studies have demonstrated that small parts, suchas screws, bearings, and gears, made of MR-incompatible materials do not presentsubstantial problems or image artifacts as long as they are of small size and appro-priately positioned relative to the imaged area. A comprehensive review of the MRcompatibility of materials was presented by Schenck (88) along with many pertinentreferences. Evaluating the available construction materials and the developed MRcompatible robotic systems, we observe that a combination of different materials ismost likely to be used for the construction of a system depending on the structuralneeds and the proximity to the area of imaging.
MR-Compatible Actuators
The MR-compatible interventional systems require appropriate forms of actua-tion. The commonly used electromagnetic actuators are, in general, not compatiblewith the MRI environment owing to their principle of operation. Therefore, alterna-tive types of actuation have been considered and novel ones have been proposed forMR compatible applications. Manual actuation is the simplest choice and an exampleof such actuation is an interventional device designed to assist in prostate-relatedprocedures (16, 23). Another possible option is hydraulic actuation given the appro-priate selection of hydraulic fluid and components (power generators, accumulators,
358 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
hydraulic cylinders, valves, etc.). Hydraulic power can be transferred through hosesand produce large forces at distant locations. This form of actuation was used ona six-degree-of-freedom (DOF) manipulator presented by Kim et al. (89) for use inminimally invasive liver surgery performed inside open MR scanners. Ultrasonic mo-tors were used for generating the hydraulic power and the associated unit was kept ata distance from the MR scanner to address compatibility issues. Sterilized saline wasused for the transmission of power to the hydraulic cylinders. The main problemsreported relevant to that form of actuation were leakages of fluid as well as entranceof air bubbles into the pressurized system. Furthermore, a study by Moser et al. (90)investigated the use of a hydraulic master-slave system for MRI related applicationsfocusing on the dynamics of the system.
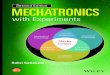
Pneumatics is another form of actuation used with MR devices that eliminatesproblems associated with hydraulic systems. Pneumatic systems are cleaner and op-erate at higher speeds compared with hydraulic systems. However, they are suitableonly for relatively low-force applications and have limited stiffness owing to thecompressibility of the air. Recently, a highly efficient and controllable pneumaticmotor called PneuStep (91, 92) was introduced that is suitable for MR applications.PneuStep uses a stepper motor principle to achieve precise motion on the order of0.050 mm, is simple in design and construction, and its operation is safe and fully MRcompatible (Figure 1). This new motor uses pneumatics for actuation and optics forencoding, which are both decoupled from electromagnetism. The motor was success-fully tested in MR scanners of up to 7 Tesla without imager interference, artifacts, orloss of motion accuracy. Pneumatic actuators are also used with one of the currently
ba
MC
P/C
OE
Figure 1MR compatible motors. (a) Commercial rotary ultrasonic motor (Shinsei, Japan) showntogether with its motor controller (MC) and the power/control (P/C) and the opticalencoder (OE) wiring. These motors contain certain conductive components and the powersupplies and controllers may introduce image artifacts. (b) Fully MR-compatible pneumaticmotor developed at the Urology Robotics Group of The Johns Hopkins University. Thismotor provides accuracy on the order of 0.050 mm and has been successfully tested for MRcompatibility up to 7 Tesla without being affected by the MR scanner or inducing noise inthe images. (Printed by permission of Dr. Dan Stoianovici, The Johns Hopkins University,Baltimore, Maryland.)
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 359
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
commercially available systems, the robotic assistance system InnoMotionTM (In-nomedic GmbH, Herxheim, Germany).
Other nonconventional types of MR-compatible actuation include the elec-trostrictive polymer actuators investigated by Vogan et al. (93) who examinedtheir application in reconfigurable imaging coils. The use of electrostatic linear-motion motors for MR applications was theoretically and experimentally studied byYamamoto et al. (94). Electrorheological fluids (ERFs) have provided an alternativeway for generating resistive forces inside a MR scanner (95–97). After demonstratingexperimentally the MR compatibility of ERFs, the authors of References 95–97 de-veloped and tested in a MR scanner an ERF-powered rehabilitation device that canapply controllable resistive forces on a person’s hand.
Another type of actuation that has been used in MR devices is electromagneticactuation that utilizes the large static magnetic field of the MR scanner (64). Applyingcurrents to coils inside the magnetic field of the MR scanner induces Lorentz forcesthat can serve to generate loads and movements. To generate larger forces, eitherhigher currents, which affect the MR images, or larger coil diameters, which makethe device bulky and inconvenient to use, are necessary.
With most of the systems developed so far, the favorite actuators have been theultrasonic, piezoelectric motors (USM) (8, 14, 15, 18, 25, 53) (Figure 1). Their opera-tion is based on the piezoelectric phenomenon and the fact that motion is produced bythe ultrasonic vibration of a piezoelectric ceramic when high-frequency voltage is ap-plied. They are suitable for MRI applications because they are magnetically immuneand they do not produce any magnetic fields either. Relevant MR-compatibility testswere performed by Chinzei et al. (86) to examine the effect of the motor on the imagesfor different operating conditions and distances from the isocenter of the scanner.Ultrasonic motors are bidirectional with a high torque-to-weight ratio, small size, andcompact shape. A special feature of the USM is their high breaking torque, whichallows a robotic system to maintain its current position and support its own weightwhen not actuated. However, this can also be considered a drawback given that thejoints of the actuated device cannot be moved manually if necessary, for example, inthe case of a medical emergency or failure of the actuation system. A solution to thisproblem is the use of mechanical clutches that disengage the motor from the rest ofthe motion system, an approach implemented by Chinzei & Miller (10) and Kosekiet al. (15).
Many types of actuators are only MR compatible when they are away from theimaging area, such as the commercially available USM. To address the compatibilityissue in most systems using this form of actuation, the motors remain outside thescanner and a motion transmission system is used to transfer the motion to the dis-tant actuated points. Remote actuation can be implemented using drive shafts, belt orchain drive systems, cable-driven systems, linkages, etc. Performance limitations aretypically associated with robotic/mechatronic systems with remotely actuated jointsthat are known to suffer from joint flexibility, backlash, and friction, as demonstratedin Christoforou & Tsekos (98). Examples of remotely actuated MR-compatible ma-nipulators can be found in the literature (8, 15, 25, 53) and are discussed in moredetail in the following sections.
360 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
MR-Compatible Sensors
The safe and accurate operation of any robotic/mechatronic device, including thosefor MRI applications, requires the use of position and/or force feedback signals forclosed-loop control. In this section, we review sensors that have been used in MR-compatible systems.
A charge-coupled device (CCD) laser micrometer system was implemented byKoseki et al. (99) and used for testing the positioning repeatability of a MR-compatiblemanipulator inside the scanner. Custom-designed incremental encoders for transla-tional as well as rotational measurements have been proposed, which use glass gratingpatterns for counting motion and fiber-optic cables for the transfer of signals to the re-motely placed optical components and circuitry (8). Innomedic (Herxheim, Germany)has developed both rotary and linear optical encoders based on fiber-optic technology.
A six-axis force sensor for MRI applications was developed by Takahashi et al. (100)using fiber optic components and a similar sensor was also used on a MR-compatiblehaptic device presented by Gassert et al. (101). In both cases, light was transmittedthrough a fiber cable to the remotely located, MR-compatible part of the sensor andcontinued through a returning cable. A physical displacement of the sensing elementowing to the applied force affected the passage of the light between the two cables.By measuring the intensity of the returning light the size of the applied force can bederived. Another example is the force sensor based on optical micrometry developedand tested by Tada & Kanade (102). Several papers have reported the use of loadcells within a MR environment (68, 95, 103). These sensors are made of conductivematerials, such as aluminum, and require a small size, appropriately positioned relativeto the imaged area, and MR compatibility testing.
A sensing issue related to MR image guidance of interventional procedures is thevisualization and tracking of interventional devices and tools, which in general aremade of MR inert materials and are invisible in the images. Localization and trackingof the manipulator should be available when the device is both idle and in motion,the latter requiring fast measurements. A solution for the localization of devicesinside a MR scanner is based on active MR-visible markers. These markers are smallcontainers filled with MR contrast agents and surrounded by a miniature RF antennathat is connected to one of the data acquisition channels of the scanner dedicated tothis marker (13, 104). Projection imaging can then be performed, which allows forfast spatial localization of the markers (105). With the use of dedicated channels perantenna, their position can be determined in space fast and as reliably as allowed bythe inherent limitations of the MR scanner technology (i.e., linearity of the magneticfield gradients).
Testing the MR Compatibility of Mechatronic Systems
Studies of the MR compatibility of robotic/mechatronic devices entail the inves-tigation of their presence and/or operation on the MR images. These studies as-sess global and local susceptibility effects, secondary to eddy-currents on conductivecomponents and impurities, and the possible image quality deterioration owing tothe powering of electronics and the operation of the device actuators. In general,
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 361
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
different imaging pulse sequences and protocols have different degrees of sensitivityto the sources of such artifacts (8, 10, 86, 106). Therefore, such studies usually eval-uate spin-echo-based sequences, such as the conventional spin-echo and the turbospin-echo or half-Fourier turbo spin-echo HASTE, as well as gradient-echo-basedones, such as the standard gradient recalled echo (GRE) and true fast imaging withsteady precession (TrueFISP).
Quantitative measurements include the linewidth of the proton signal from simplesingle-pulse acquisitions (8, 86) and the SNR as well as the contrast-to-noise ratio(CNR) from images. The image quality is assessed primarily by measuring the SNRand, to a lesser degree, by the CNR of regions of interest (ROI) traced on the MRimages. To assess the different sources of image artifacts, MR compatibility testsmost often entail studying the effect of the robotic/mechatronic device on the MRimages collected at four conditions. (a) The device is not present, which correspondsto the reference condition versus which the others are compared. (b) The device is inplace but not powered. This condition is used for the investigation of the effects ofthe passive presence of the device in regard to image artifacts originating from eddy-currents on conductive material and bulk or local susceptibility effects, and secondaryto the presence of small ferromagnetic parts and/or impurities in the constructionmaterials. (c) The device is in place, the electronics are powered but the device isnot actuated. This condition is used for the assessment of the effect of RF emissionsfrom the electronic component of the device that may reside inside the scannerroom to the MR images. Such components can be power supplies, motor drivers,or other electronic devices. (d) The device is in place, the electronics are powered,and the device is actuated. This condition is investigated to evaluate the effect of theoperation of the device. It should be noted that, even when ignoring the operationof the motors, when the electronics are activated they may produce different RFemissions as compared to when they are just powered on.
The degree of image deterioration depends on the type of actuators, the associatedelectronics, and their shielding. Compatibility tests of most manipulation systemsactuated using piezoelectric actuators have consistently demonstrated signal intensityartifacts and deterioration of the SNR at the aforementioned conditions (c) and (d ).In Tsekos et al. (53), based on these findings the motor drivers were enclosed insidea Faraday cage, the cables were shielded using aluminum sheath, and the relevantproblems were considerably eliminated. In addition to experimental evaluation ofthe MR compatibility of robotic manipulators, the use of numerical simulations forpredicting the MR compatibility characteristics of objects was proposed by Chinzei(107) and simulation results were compared with experimental ones.
MR-COMPATIBLE ROBOTIC AND MECHATRONIC SYSTEMS
Research and Development in MR-Compatible InterventionalRobotic Systems
Over the past decade, several groups worldwide have developed MR-compatible in-terventional robotic systems. These works demonstrated the feasibility as well as the
362 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
challenges associated with the development of such devices. Anatomy-specific systemshave been introduced for MR-guided procedures in the brain (18), breast (14, 17, 25),and prostate (16, 22, 23). Purpose-specific systems include a robot for MR-guidedendoscope manipulation (15) and a needle-guiding robot for MR-guided microwavethermotherapy (12). Two devices were also introduced as general purpose systems,designed for access to the upper part of the body (13, 53). A scanner-specific generalpurpose system was also introduced to exploit the vertical gap of the double-donutMR scanner (8). These systems use different kinematic structures and actuation mech-anisms depending on the targeted applications and the available space in the scanner.
One of the pioneering works in the field of MR-compatible interventional roboticsis that of Masamune et al. (18), who developed a MR-compatible manipulator ded-icated to neurosurgical applications. The device was designed to be mounted onthe patient couch and above the head of the subject, providing six DOF for MR-guided stereotactic needle biopsies. The frame of the system was primarily madeof the MR-inert polyethylene terephthalate, incorporated a small number of non-magnetic metallic small-sized parts and it was actuated with ultrasonic motors. Thiswork assessed the mechanical properties, MR compatibility, and operational accuracyof the system. It also provided the first insights into the challenges associated withMR-compatible mechatronics. Specifically, even though polyethylene terephthalatewas proved a suitable construction material in regard to MR compatibility, its ratherlow structural stiffness was found unsuitable for the effective manipulation of heavyinterventional instruments. Systematic assessment of the mechanical errors associ-ated with each DOF, as well as investigation of MR-guided targeting on phantoms,demonstrated an overall positioning accuracy of less than 3 mm. MR-compatibilitystudies in a 0.5 Tesla scanner revealed that when actuated, the ultrasonic motors sub-stantially deteriorated the image quality and it was required to power off the motordrivers during MR scanning.
A MR-compatible robotic system specifically designed for operation inside thevertical gap of the 0.5 Tesla double-donut MR scanner was presented by Chinzei et al.(8, 10). The design of the system is optimized for assisting an interventionalist whostands in the limited space between the two magnets. Its end-effector is linked to twolong members, which are rigidly attached to a remotely located motion mechanism,mounted on a supporting structure located above the scanner. The end-effector of thesystem allows the positioning of an axisymmetric tool using the available five DOF,which are actuated with ultrasonic motors. With only the two long and slim membersentering the area between the two pieces of the magnet, this configuration resultsin minimal occupancy in the already limited workspace of the surgeon. In addition,placing the actuators and the motion mechanism away from the sensitive area of theimager contributes to its overall good MR compatibility.
A robotic system was developed by Koseki et al. (15) dedicated to MR-guidedmanipulation of endoscopes for use in transnasal neurosurgical procedures. Thisfour-DOF device was specifically designed for use with open MR scanners and ittook advantage of the available horizontal space between the vertical poles of suchscanners. The kinematic structure of this robot incorporates a five-bar linkage mech-anism for the transfer of motion to the remotely actuated joints. Like most of the
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 363
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
Figure 2The MR-compatible manipulator for MR-guided procedures in the prostate developed at theDepartment of Radiology of The Johns Hopkins University. (Printed by permission of Drs.Axel Krieger and Ergin Atalar, The Johns Hopkins University, Baltimore, Maryland.)
MR-compatible devices, the system is driven by ultrasonic motors. To improve struc-tural stiffness as well as reduce the construction cost, the system also includes MR-incompatible materials. However, their size and location in relation to the imagingvolume of the scanner were carefully considered to achieve MR compatibility. In thiswork, the accuracy, repeatability, and stiffness of the prototype system were examinedexperimentally. MR-compatibility studies inside a 0.3 Tesla open scanner confirmedthat the scanner had no effect on the operation of the robotic system, and SNR phan-tom studies demonstrated that the presence of the manipulator had little effect on theimage quality. However, the operation of the ultrasonic motors was found to causeconsiderable noise in the images and the manipulator was not actuated during MRimaging.
A MR-compatible device for image-guided biopsy and therapeutic procedures inthe prostate was developed by Susil et al. (22, 23) and further improved by Kriegeret al. (16) (Figures 2 and 3). The system is manually positioned and actuated and itscompact size, which originated from its anatomy-specific design, allows its use in bothopen and cylindrical high-field MRI scanners. The device was mainly constructed ofplastic materials, while metallic small parts were kept to a minimum. To facilitateMR guidance, the system incorporates active fiducial markers made of small RF coilsplaced at known areas of the device. Connected to dedicated channels of the MRscanner, these coils allow for MR-based tracking of the device position and guidanceof the procedure. Its accuracy and operation were investigated with in vitro and invivo studies on a canine model, which demonstrated accuracy in placing a needlewithin 2 mm of the desired target lesion. The device is one of the few that have beentested on humans in a 1.5 Tesla cylindrical scanner (22). Testing of that system alsoincluded intraprostatic injections using MR contrast agent as well as image-guidedbrachytherapy seed placement.
364 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
Figure 3MR-guided procedures with the prostate manipulator. (a) Sagittal T2-weighted MR imagecontaining rectal sheath and prostate. (b) Axial T2-weighted MR image containing prostateand rectal sheath with selected target. (c) Axial T1-weighted image after insertion of theneedle, verifying accurate targeting, thus a small displacement between target point and thevoid is created by the needle tip. (Printed by permission of Drs. Axel Krieger and ErginAtalar, The Johns Hopkins University, Baltimore, Maryland.)
A robot specifically developed for MR-guided microwave thermotherapy of livertumors was presented by Hata et al. (12). The design of the device is based on a remotecenter of motion approach and was controlled in a semiactive manner. Specifically,it consists of a three-DOF Cartesian stage, which is activated with ultrasonic motorsand a passive end-effector with two unconstrained rotational DOF monitored byMR-compatible sensors. After the target is identified from MR images, the interven-tionalist manually adjusts the orientation of the needle insertion path. At the sametime, the Cartesian stage maintains the remote center of motion at the predefinedtumor site. The main structure is made of aluminum and is installed on the side of thepatient couch so that it does not interfere with the operation of the interventionalist.Targeting accuracy, as well as MR compatibility tests, was performed inside a low-field 0.5 Tesla scanner on a phantom. The testing confirmed that the presence ofthe robot next to the scanner had little effect on the quality of the images. However,when one or more motors were actuated, considerable noise was induced on the MRimages.
ROBITOM, the first MR-compatible robotic system dedicated to MR-guidedbreast biopsies, was presented by Kaiser et al. (14). The system, which was specifi-cally designed to use the cylindrical space inside a closed scanner, consists of a MR-compatible plastic rack that hosts two piezoelectric motors that drive an extensionarm along two Cartesian directions. The distal end of the extension arm, which facesthe patient, carries a tilting housing that can be loaded with different instrumentadapters for different applications, such as delivery of local anesthesia, performanceof skin incision, and insertion of a trocar. In this system, the patients are placed inthe prone position on a specially designed support device that is mounted on thepatient couch and provides plates for the fixation and moderate compression of thebreasts. A patient study using this device inside a 1.5 Tesla scanner was presented by
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 365
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
Pfleiderer et al. (21). In response to the results of those studies, a second prototype,the ROBITOM II, was presented in Pfleiderer et al. (20). The latest version avoidsthe problem of lesion shifting and target missing observed at the first version of thesystem owing to the slow insertion of the trocar into the breast. In the new system, ahigh-speed trocar unit was implemented. This latest version was also equipped witha dedicated double breast biopsy coil, which allows better imaging and access to thebreasts to facilitate interventions. In vitro phantom experiments inside a 1.5 Teslascanner were used to assess the precision of the device, and in vivo human tests insidea cylindrical scanner resulted to the successful harvest of biopsy specimens.
Another breast-dedicated MR-compatible robotic system was developed by Tsekoset al. (25) and further improved by Larson et al. (17) for biopsies and breast conservingtherapies of breast cancer. Compared with previous designs (14), the system allowsaccess to the breast from any desired orientation. This is achieved by incorporating anactuated rotating base with two compression plates, which allows setting the orienta-tion of breast compression and thus one of axes of insertion. The device has five DOFremotely actuated with ultrasonic motors and a motion transmission system consist-ing of shafts and universal joints. This system is used to set the degree of compression,the insertion path, and the depth of insertion of an interventional probe. Experimentalstudies on breast phantoms demonstrated the procedure of MR-guided compression,stabilization, and needle insertion. These studies were performed at 4.0 Tesla, thestrongest field at which MR robotic devices have been tested so far.
Recently, Tajima et al. (24) introduced the first MR robotic system that incorpo-rates two six-DOF robotic manipulators. This unique prototype master-slave systemis designed for use with the all-around open scanners. Each manipulator has threetranslational DOF that are located on its base and three DOF on its arm component,which approaches the surgical site inside the scanner. The base of the manipulator isprimarily made of aluminum and the arm of plastic materials. The presented studiesincluded assessment of its manipulability as well as its MR compatibility by perform-ing SNR studies on a phantom placed inside the head coil of a 0.3 open scanner.With the manipulator touching the phantom, a slight artifact and minor effect onthe image were observed, as well as approximately 10% reduction in SNR when themanipulator was in motion.
The only currently commercially available MR-compatible interventional roboticsystem is InnoMotionTM (Innomedic GmbH, Herxheim, Germany) (Figures 4 and5). The system is a robotic arm that can assist in percutaneous interventions insideMR scanners. It has six DOF and was developed for a variety of applications, includ-ing spinal procedures for pain therapy, tumor therapy, and biopsies. The system ismounted on the patient couch and moves along an arc-shaped support base. Its ac-tuation was based on specially developed pneumatic actuators. This system was usedby Bock et al. (13, 104) who presented an animal study on image-guided targetingwith a needle inside a 1.5 Tesla cylindrical MR scanner.
Another general purpose MR-compatible interventional system was recently de-veloped by Tsekos et al. (53) and further improved by Christoforou et al. (11)(Figure 6). The device has seven DOF and consists of a Cartesian positioner withthree orthogonal DOF located in front of the MR scanner and a robotic arm that is
366 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
a b
Figure 4(a) The MR-compatible robotic assistance system InnoMotionTM (Innomedic GmbH,Herxheim, Germany) developed for MR-guided procedures. (b) Patient positioning for spinalprocedures. (Printed by permission of Dr. M. Bock et al., Department of Medical Physics inRadiology, German Cancer Research Center, Heidelberg, Germany.)
deployed inside the scanner. The arm has three rotational DOF and a linear one forthe insertion of interventional tools. For MR compatibility, actuators are placed atthe proximal end of the arm, i.e., outside the scanner, and motion is transferred to thedistant joints using a system of drive shafts and universal joints for the through-jointtransmission (98). MR-compatibility studies included the assessment of the SNR andCNR of MR images on phantoms and in vivo inside a 1.5 Tesla cylindrical scanner.The phantom studies demonstrated that the noise induced by the operation of theultrasonic motors can be substantially reduced by enclosing the electronics inside aFaraday cage and shielding the wires. In vivo studies on animals demonstrated thatthe SNR and CNR were sufficient for in vivo real-time MRI guidance even while therobotic device is in motion.
Research and Development in MR-Compatible RehabilitationRobotic Devices
Within the past 5 years, several groups worldwide have proposed differentrobotic/mechatronic systems for fMRI studies in neuroscience or aided rehabili-tation. These systems can be categorized in three different groups: (a) force or/andmotion measuring systems, (b) tactile stimulators, and (c) computer-controlled forcegenerating systems. In most systems, actuation and control takes place outside theMR scanning room and the energy is transferred to the subject placed inside thescanner room via different mechanical transmissions, such as pneumatic, hydraulic,or mechanical (pulleys and ropes, etc.). These systems are usually complex and sufferfrom long transmission lines accompanied by dissipative and delay effects. To avoidthese problems, some groups have developed systems where the actuators are locateddirectly at the end-effector inside the scanner room. All these works demonstrated
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 367
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
a
84.0 mm
x
b
d
c
e
x
Figure 5Results from a MR-guidedintervention with theInnoMotionTM roboticassistance device simulatingpain therapy on a pig modelinside a cylindrical1.5 T MR scanner. (a) Animage used for trajectoryplanning identifying theinsertion (blue cross) and thetarget point (red cross) nearthe plexus coeliacus.(b, c) Two images during theneedle insertion collectedwith a TrueFISP MRI fastpulse sequence. The greenarrows point to the two MRvisible markers. (d, e) Imagesused to validate theplacement of the needlecollected with aT1-weighted FLASH pulsesequence. After the needleplacement, Gd-DTPAcontrast agent is locallyinfused and accumulates atthe targeted site (whitearrow). (Printed bypermission of Dr. M. Bocket al., Department ofMedical Physics inRadiology, German CancerResearch Center,Heidelberg, Germany.)
the feasibility as well as the challenges associated with the development of fMRIcompatible devices.
Different groups have developed fMRI-compatible force sensing systems to quan-tify forces exerted by subjects in their upper extremities for motor function studies.Liu et al. (70) presented a fMRI-compatible system that was designed to measure handgrip force and surface electromyograms (EMGs) of finger flexor and extensor muscles.The force measurement system consists of a handgrip device, a pressure transducer,nylon tube, and a water reservoir. The grip force applied to a hand grip device istransmitted to a pressure transducer, which is placed outside the scanner room by awater-filled nylon tube. The quality of the fMRI brain images was maintained while
368 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
Figure 6The MR-compatiblerobotic device developed atWashington University inSt. Louis, MO. (a) Thesystem with its coversremoved showing theCartesian base and thefour-DOF arm. (b) The armand the end-effector of thesystem.
using the device in a 1.5 Tesla MR scanner. A custom MR-compatible dynamometerthat quantifies hand grip force during fMRI testing was used by Cramer et al. (68).The grip dynamometer consists of a force transducer that is fitted into plastic han-dles. The transducer was held in the palm, with squeezing performed by four fingerson the top handle of the transducer and the thumb on the bottom handle. The devicewas used in a 3 Tesla MR scanner, allowing for brain activation patterns to be quanti-fied at varying effort levels. A fMRI-compatible wrist device that measures isometricforces and joint moments generated at the wrist was presented by Hidler et al. (69,103) to study mechanisms of neural recovery following neurological injuries. Thedevice consists of a six-axis load cell, which measures the forces and moments exertedby test subjects on a handle. The load cell and handle are mounted on a wedge and theelbow is flexed slightly during testing to improve comfort. Four padded, adjustablebumpers are used to stabilize the forearm during testing and isolate the brain activa-tion areas that are responsible for activating the wrist muscles (Figure 7). The devicewas tested in a 3 Tesla MR scanner and did not introduce noise or movement artifactsin the fMRI data and was not influenced by the magnetic fields. A MR-compatiblefinger motion sensing device for measuring angular velocity of one segment of each ofthe 10 fingers during fMRI was presented by Schaechter (71). The device uses micro-electromechanical system (MEMS) sensors that are secured to the wrist by a Velcro
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 369
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
Figure 7MR-compatible forcesensing wrist module.(Printed by permission ofDr. Joseph Hidler, Centerfor Applied Biomechanicsand RehabilitationResearch, NationalRehabilitation Hospital,Washington, DC.)
watchband. The use of the device in a 3 Tesla MR scanner did not cause artifacts andthe environment did not interfere with the finger motion measurements.
In most of the experiments conducted to date, manually controlled tactile per-ception tasks, such as tactile objection recognition, have been performed (108, 109).However, such setups have the disadvantage of being static during the acquisitiontime, and thus no interactive changes or vibrating stimuli can be applied. The de-mand for a dedicated device to deliver distinct, reproducible, and passive tactilestimuli in a fMRI environment gave rise to recent developments on this issue. Sev-eral groups have developed vibrotactile stimulators for fMRI experiments. A fMRI-compatible piezoceramic vibrotactile stimulator was presented by Harrington et al.(73). Piezoceramics are nonmagnetic materials that can produce displacements underapplied voltage. The vibrotactile stimulator consists of a piezoceramic wafer and apower source to apply a square wave signal to create an abrupt voltage change thatcauses more distinct mechanical displacements in the wafer. The vibrotactile stimu-lator was used inside a 1.5 Tesla MR scanner and did not create any artifact to theimages.
A fMRI-compatible magnetomechanical vibrotactile device was proposed byGraham et al. (72) for the investigation of somatosensory neuronal activation. Thedevice utilizes the magnetic field of the MRI scanner to produce a mechanical force.The resulting Lorentz forces can be oriented to generate large vibrations that are eas-ily converted to translational motions. fMRI experiments were conducted using a 1.5Tesla MR scanner. Usage of the device did not generate any noise to the fMRI images.
A vibrotactile stimulator was presented by Golaszewski et al. (110) to map thecortical areas that show activation during a vibration paradigm in fMRI studies. Thevibrotactile consists of a direct current (DC) motor, flexible shaft, and a vibration head.The DC motor is placed outside the MR room and is connected to the vibration headwith a flexible shaft. The vibration head contains a gear-driven excenter and can beaffixed to various regions of human body. The device was tested inside a 1.5 Teslascanner and did not interfere with fMRI images.
370 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
Figure 8MR-compatible,pneumatically driven tactilestimulator. (Printed bypermission of Dr. KarlheinzMeier, Electronic VisionGroup, Kirchhoff Institutefor Physics, Heidelberg,Germany.)
A fMRI-compatible pneumatic vibration device was reported by Golaszewski et al.(111). The vibration device consists of a dual membrane pump that is driven by a DCmotor. The oscillating air pressure is controlled with a commercially available bloodpressure cuff. The vibration amplitude can be selected and controlled with a pneu-matic by-pass line. The vibration device produces oscillating air that is transferredinto the magnet room via plastic tubes to the vibration head. The vibration head isa latex tube, which can be affixed to the patient with Velcro straps. All experimentswere performed with a 1.5 Tesla MR-scanner and showed that the device does notinterfere with fMRI images.
A pneumatic vibrotactile stimulation device for fMRI experiments was reportedby Briggs et al. (112). The tactor consists of a latex rubber diaphragm mounted ona semirigid plastic holder. A plastic tube delivers pulses of pressurized air from themanifold in the control box containing solenoid valves that control the airflow to thetactors. The vibrotactile stimulator was used in a 3 Tesla MR scanner and did notproduce any artifact in fMRI images.
A fMRI-compatible, pneumatically driven tactile device was presented by Zappeet al. (74). The device establishes tactile contact with the skin by a compressed air–driven piston (Figure 8). An electropneumatic interface located several meters awayfrom the center of the magnet regulates the pressure timing. The compressor thatprovides the required working pressure is placed outside of the MR room. The deviceis capable of stimulating the skin using arbitrary time sequences that consist of 2-Dtactile images. The device was tested in a 2 Tesla MR scanner and operates withoutgenerating artifacts.
Actuated robotic systems have been used to investigate motor control.Robotic/mechatronic interfaces can dynamically interact with humans, deliver forces,and perform movements to study neuromuscular response. A robotic/mechatronicinterface in conjunction with fMRI would enable neuroscientists to view and investi-gate the brain mechanisms involved in performing tasks under variable dynamic en-vironments and to investigate the neural basis of motor control. A fMRI-compatibleone-DOF haptic interface for wrist motion was presented by Moser et al. (90) andfurther improved by Gassert et al. (101) to investigate the brain mechanisms of hu-man motor control. This system consists of a master part and a slave part linkedover a hydrostatic transmission (Figure 9). The actuator (rotary direct drive motor)
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 371
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
Controlcomputer
ab
MR compatibleslave actuator
Rotary output withtorque sensor
Masteractuator
Emergencybuttons
Hydrostatictransmission
Figure 9One-DOF MR-compatible haptic interface. (Printed by permission of Dr. Roger Gassert,Medical Robotics Group, Laboratory of Robotic Systems, Ecole Polytechnique Federale deLausanne, Lausanne, Switzerland.)
is placed outside the scanner room and drives the master piston via a transmissionstage and a belt and pulley mechanism. The master cylinder is connected to a MR-compatible slave cylinder, which is placed inside the MR scanner via 10 m of flexiblehydraulic conducts to transmit force and motion of the actuator. An optical forcesensor, based on reflected light intensity measurement over optical fibers, is used tomeasure interaction forces with the human subject (113). The MR-compatibility testswere performed inside a 1.5 Tesla scanner. Using similar actuation and force-sensingprinciple, Gassert et al. (66) presented a two-DOF haptic interface to investigate theneural control of multijoint arm movements. fMRI compatibility was demonstratedthrough phantom tests as well as a functional study with a human subject.
A MR-compatible, computer-controlled, variable-resistance hand device with oneDOF was proposed by Khanicheh et al. (95–97) for fMRI studies of motor control.A novel feature of the device is the use of ERFs to achieve resistive force generation.ERFs are fluids that experience dramatic changes in rheological properties, such asviscosity or yield stress, in the presence of an electric field. The first prototype isdesigned and utilizing an ERF rotary brake with pincer handle motion and consistsof four major subsystems: (a) an ERF rotary brake; (b) a gearbox; (c) handles; and(d) two sensors, one optical encoder, and one force sensor (aluminum strain gaugetype) to measure the patient induced motion and force (Figure 10). The secondprototype is utilizing an ERF linear damper with linear handle motion and alsoincludes two sensors for linear position and force measurements (Figure 11). Thedevice is designed to resist up to 50% of the maximum level of gripping force of ahuman hand and be controlled in real time. The device was tested inside a 3 Tesla MR
372 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
a
Force sensor
Gear box
Stationaryhandle thumb
Finger handle
Encoder
Transmissionbracket
EMF resistiveelement
b
Figure 10MR-compatible hand-rehabilitation device with pincer handle motion and rotary ERF brake.
scanner. Detailed testing demonstrates that there is neither an effect from the MRenvironment on the ERF properties and performance of the device nor significantdegradation on MR images by the introduction of the device in the MR scanner.
A MR-compatible, one-DOF haptic interface device for fMRI studies was pre-sented by Riener et al. (64). The device uses two coils that produce a Lorentz forceinduced by the large static magnetic field of the MR scanner, which are mountedon a movable axis (Figure 12). An optical encoder and a force sensor are integratedwith a handle. To increase the resolution of the angular measurements, rotationalmovements of the handle are converted to the encoder via a small gear transmission.The force sensor is comprised of three optical fibers, two fibers measure the lightintensities emitted by one opposing fiber. To make the system less sensitive to dif-fused light and absorption within the fibers, the force is determined by relative ratherthan absolute intensity changes. The device could interact with the user and causeisometric, active, or passive interactions depending on the controller. The device wastested in a 3 Tesla scanner and with a constant current flow below 1A. There were noelectromagnetic interferences that affected the MR image quality.
A fMRI-compatible parallel link manipulandum was presented by Diedrichsenet al. (65) to study brain regions involved in processing reach errors. The manipulan-dum allows free 2-D movements in horizontal plane and is capable of applying forceto the hand. The robotic system uses two-way, air-driven cylinders that house pis-tons, servo valves, and linkages. Forces are applied via air pistons supplied with an airpressure of 100 psi from a compressor outside the MR room. The force produced bythe pistons is bidirectional. This force is transmitted to the joint of the robot througha linkage (Figure 13). Optical encoders were used to measure the position of the
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 373
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
a
Fixedhandle
Forcesensor
Returnelastic
Linear ERdamper
EncoderMovinghandle
Adjustablecollar
b
Figure 11MR-compatiblehand-rehabilitation devicewith linear handle motionand linear ERF damper.
robot’s links. The device was utilized in a 3 Tesla MR scanner and pilot functionalstudies were performed on human subjects.
A fMRI-compatible manipulandum system for finger movements was presentedby Izawa et al. (67) to investigate the neural correlates for motor control. The system iscomposed of a two-DOF parallel link arm actuated by two ultrasonic motors equippedwith rotary encoders. Two ultrasonic motors align vertically to the parallel linksarm. Motors connect to the links directly to drive the links without a gearbox. Themanipulandum produced the target force that is computed from impedance controlto make the subject feel the virtual impedance in his/her finger. The force of the tipof the manipulandum is determined by the torques of ultrasonic motors. The subjectsmanipulate the end-effector of the maniulandum by the index finger. The device was
374 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
Figure 12MR-compatibleelectromagnetic hapticinterface. (Printed bypermission of Dr. RobertRiener, ETH Zurich,Zurich, Switzerland.)
installed inside a 1.5 Tesla MR scanner and it was shown that the device did notinterfere with the fMRI scanner and was suitable to use in fMRI studies.
A fMRI-compatible virtual reality system that included a data glove equipped withtactile feedback was developed in References 114 and 115 for fMRI investigations ofthe somatosensory system. The data glove is composed of position-tracking sensorsthat were mounted on the hand and a vibrotactile device that was attached to the
Figure 13MR-compatible robotic arm. (Printed by permission of Dr. Reza Shadmehr, The JohnsHopkins University, Baltimore, Maryland.)
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 375
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
distal, palmer surface of the index finger. Shape TapeTM (Measured Inc.), an array offiber-optic bend-and-twist sensors mounted on a flexible ribbon, is used for trackingthe hand position and posture. The tape is mounted with Velcro straps along theindex finger and thumb of the data glove. This allows simple pointing and pinchingmotions to be captured and translated to movements on a computer display. A smallmagnetomechanical vibrotactile device, which uses the scanner’s large static magneticfield to present controlled, reproducible somatosensory stimuli, is mounted under-neath the Velcro strap on the index finger of the data glove. The virtual environment(VE) consists of a virtual block and a detailed graphical representation of the subject’svirtual hand. fMRI experiments were performed inside a 3 Tesla MR scanner and thetactile data glove was found to be MR compatible and did not introduce any signalintensity artifacts or noise increases during functional scanning.
A MR-compatible stationary cycle was presented by Cheng et al. (116) for flowquantification in large arteries during lower limb exercise inside a 0.5 Tesla openmagnet. The cycle consists of six major parts: (a) a crank tower that pivots aroundthe flywheel center through a range of angles and can be locked in place with quick-release clamps; (b) a power transmission system that comprises a crank sprocket, asmaller flywheel sprocket, and a belt that connects tow sprockets; (c) a freewheelmechanism that transmits torque to the flywheel when the cycle is driven forwardand allows freewheeling when the cycle is driven backward or the subject stops pad-dling; (d ) frictional torque generation, which comprises a pendulum whose deflectioncorresponds to the flywheel friction force and can be preadjusted for a higher loadwork; (e) supports and guide rails that provide stability for the cycle during exercise;and ( f ) a light sensor that measures the angular speed of the flywheel and thereforeinstantaneous workload. The system was capable of producing smooth, repeatablelower limb exercise while phase contrast MRI was performed in the abdominal aorta,and image artifact was not observed.
Procedure Planning and Guidance of MR-Compatible InterventionalRobotic Systems
Performance of IGI with MR-compatible manipulators is often based on a stereotacticsemiautomated approach, which entails the inspection of preoperative MR images toprescribe a path for the insertion of the interventional tool. In a stereotactic approach,the operator can do all planning using preoperative images combined with anatomicalmaps and other patient-specific information. The robotic system can then executethe preprogrammed tasks while the operator monitors the procedure and intervenesif necessary. In a needle-targeting procedure, for example, an image-guided biopsyor an ablation, the operator can examine a set of 2-D or 3-D images and definethe insertion point as well as the target, i.e., define the insertion vector (Figure 5).The robotic system can then solve the inverse kinematics problem and automaticallyalign its end-effector with the desired insertion vector. This option is available onthe InnoMotionTM system, and another implementation example can be found inOzcan et al. (19). The success of this stereotactic method depends on the accurateregistration of the patient and the robotic system to the MRI scanner’s reference
376 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
frame. The registration procedure can be performed using localization of specialmarkers placed at known locations of the manipulation system (11, 53).
An alternative to the stereotactic planning and semiautomated control is one basedon a “freehand” interactive control of the manipulator. Direct control is a methodused in robotic surgeries (e.g., 117, 118). Such an approach becomes more relevant inMRI with the advent of new technical advancements. State-of-the-art MRI scannersallow the adjustment of imaging parameters on the fly from an external source ofinstructions. This capability allows almost instantaneous adjustment of parameters,such as the number, position, and orientation of the imaging slice(s) or volume,as well as the type of contrast of the collection pulse sequence. This offers a newopportunity in visualizing and even planning a procedure. Recently, Christoforouet al. (11) demonstrated the integration of a MR-compatible robotic device with aMRI scanner in a way that the transient position of the robot is sent to the MRI, which,in turn, adjusts the position and orientation of the imaging plane to always visualize theend-effector of the system. In this work, using manual control either with a graphicsuser interface or a manual control handle, the MRI scanner “followed” the motionof the manipulator providing a “manipulator-driven” approach. The ability for man-in-the-loop direct control of the interventional tool combined with the on-the-flyupdate of the imaging plane corroborate to a simple and intuitive image guidancein a way similar to this with the gold-standard ultrasound-guided interventions IGIor with endoscopy-based surgical robots (e.g., 117, 118). The manipulator-drivenreal-time imaging provides for scouting the subject, identifying a target, and settingthe path of the interventional tool to clear for obstacles and align it to the target.Man-in-the-loop image-guided control may also provide the means of practice forcompensation of needle bending, a major source of error observed in previous studieswith MR-compatible systems (21–23), because the operator can use dynamic imagingto appropriately react and correct the bending. The feature of having the tool alwaysat the same position and orientation relative to the field of view (FOV) provides astraight-forward way of directing the tool, while a simple software routine can placea line-of-sight on any frame without any special image processing.
DISCUSSION
MR-compatible mechatronics is an emerging and exciting field in biomedical engi-neering that uses multidisciplinary expertise from a wide range of engineering, basicscience, and clinical fields. The literature includes several MR-compatible roboticdevices developed during the past decade, since the first work by Masamune et al.(18). The presented systems include a wide variety of kinematic structures, methodsof actuation and transmission, and utilization purpose representative to the needs andchallenges of the field. Anatomy-specific systems include devices especially designedto conform to the specific anatomical needs for interventions in the brain (18), breast(14, 17, 25), and prostate (16, 22, 23). Purpose-specific devices include a system forMR-guided endoscope manipulation (15) and hepatic ablations (12), and also includea stationery cycle for flow quantification in large arteries during lower limb exercise(116). Another example is a magnet-specific system for use with the double-donut
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 377
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
MR scanner (8). Two devices were also introduced as general purpose systems (13,53). Functional brain imaging-specific systems for fMRI studies in neuroscience andneuron rehabilitation include devices designed to measure forces exerted by sub-jects in their limb (68, 70, 103), tactile stimulators to produce somatonsensory cortexactivation (72–74, 110–112), and computer-controlled force-generating systems toinvestigate the neural correlates for motor control under variable dynamic environ-ment (64–66, 90, 95, 96, 101).
From the standpoint of clinical practice, there are several reasons why MR-compatible interventional robotic systems would be desirable. First, interventionalprocedures could be performed with excellent contrast visualization not only of thetarget tissue but of the neighboring tissues and along the trajectory of the interven-tional tool. This is potentially a great advantage, as the trajectory of the tool mayneed to be adjusted so as to avoid passing through other organs where injury can beinflicted, such as blood vessels, isolated nerves or nerve plexuses, or solid organs, forexample, the kidneys (11, 13, 16, 17). In addition, in the case of procedures where aninjection is to be made in a certain area of the body, the spread of the injected liquidcould be visualized with the technology (13, 119). Targeting of the tool by a me-chanical system can potentially be more accurate and smooth compared with needlemovement by the human hand. However, this may not necessarily be an advantage atthe phase of insertion, as sometimes a clinician’s experience in doing certain proce-dures is invaluable and the intuitive perception or “feel” that often guides cliniciansmay not be reproducible by a motorized system. Finally, the use of MRI technologyconfers, in addition to excellent oblique 3-D or multislice visualization and localiza-tion, the advantage that there is no radiation exposure for the patient or the physician.Therefore, even though MR-compatible interventional systems are not proven yet,it is worthwhile pursuing further development in this area as the potential benefitscan be substantial.
fMRI-compatible robotic/mechatronic systems have several advantages in a clin-ical setting. First, these systems are equipped with linear/angular position encodersand force/torque sensors to produce a record of motor output during fMRI that areuseful for postimaging analysis of motor performance. Measuring the force of move-ment offers certain advantages, such as enabling a direct comparison between forceexerted and features of brain activation. Careful monitoring of subject performanceduring brain mapping is important in studies of brain functions and plasticity andmay have particular importance in patients with stroke, multiple sclerosis, and otherneurological disorders. In addition, these systems can dynamically interact with hu-mans and deliver distinct, accurate, and reproducible tactile stimuli, movements, andforces to the human body. Interactive changes can be applied by computer controlsand the corresponding brain activities can be located by fMRI. Finally, using fMRIand robotic devices during rehabilitation could provide a better understanding ofbrain function, pathological analysis, and regeneration process in nerve lesion, whichcan assist in the development of optimal rehabilitation devices and exercise protocols.
Looking toward the future of MR-compatible robotic systems in IGI and reha-bilitation there are several issues that need to be addressed. The most critical one isthat of the clinical merit of this technology. The development of these systems was
378 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
primarily driven by the desire to utilize the high-quality diagnostic information of-fered by MRI to guided biopsies and therapeutic interventions, as well as to addressthe limited accessibility in high-field MR scanners. Although both of those reasonsare, in principal, clinically meritorious, they are rather general objectives. However,the clinical merit of this technology can only be verified within the realm of daily prac-tice. Although technical challenges are still to be addressed with optimal methods, thetechnical feasibility of such devices has been proven. Identification of clinically viableapplications for MR-compatible interventional robotic systems has already startedwith clinical studies in the breast (20, 21), spine (13, 104), and prostate (16, 22). Inaddition, fMRI-compatible robotic devices have already found their place in clinicalstudies of stroke patients (68). Considering the clinical merit of this technology, animportant factor that is not often considered during the initial phases of technical fea-sibility and demonstration is cost. The financial aspect encompasses different levelsfrom the acquisition of a system, training of personnel, maintenance, and operation.The high cost of MRI scanners adds two parameters that need to be consideredwhen developing such systems: ease of installing the system and duration of theprocedure.
Technical challenges are obvious, and we believe that as more groups are involvedin the field not only will they be addressed but may result in new concepts. One im-portant technical challenge is the development of “true” MRI compatible actuators.Along this line is the recent development of a pneumatic actuator that is based onthe step-motor operation principle that provides very high resolution (91, 92). Suchmotors belong to a new generation of actuators that can operate inside the MR scan-ner and thus eliminate or reduce the need for remote transmission and the associatedmechanical complexity and errors (98). Another aspect that requires further investiga-tion concerns the construction materials. New materials, most probably composites,that are MR inert and have appropriate mechanical properties are in need. Alwayshaving the end-user as the primary determinant of a design, an additional aspect thatneeds careful evaluation is the human machine interface.
Another aspect of this technology is the appropriate integration of the imagingmodality with the operation and control of the device. Stereotactic approaches cantake advantage of the fact that MRI offers unparallel 3-D and multislice capabilitiesand a wide range of contrast mechanisms. However, too much information may notserve in favor of planning and guiding a procedure because it may increase the workload of the operator beyond that necessary. Therefore, together with the developmentof the mechatronic technology, it is important to expand research in the imagingprotocols needed for assessing the pathophysiology of the targeted tissue; imageprocessing and display need to be incorporated in the control software to simplifyrather than perplex the workload of the operator. Previous studies have illustratedthat MRI with different contrast can be segmented and overlaid to define pathwaysand avoid sensitive structures (such as vessels) and healthy tissue (43).
In conclusion, the literature in MR-compatible interventional and rehabilitationrobotic systems clearly shows highly promising results. The next step is at two fronts.One is to bring this technology to the clinical practice and evaluate its clinical merit.The other is to address the technical challenges in a way that is clinically relevant.
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 379
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
DISCLOSURE STATEMENT
Coauthor Nikolaos V. Tsekos is the principal investigator in two funding grants fromthe National Institutes of Health (NIH) that are related to parts of the work reviewedin this manuscript (grant numbers CA81817 and HL067924).
ACKNOWLEDGMENTS
The Washington University team was supported by the National Institutes of Healthgrant HL067924 (N.V.T). The Northeastern University team was supported by asubcontract from the Massachusetts General Hospital in Boston, MA, from the Na-tional Institutes of Health grant 5R21EB004665-02.
LITERATURE CITED
1. Debatin G, Adam JF, ed. 1998. Interventional Magnetic Resonance Imaging. Berlin:Springer Verlag
2. Jolesz F, Kahn T, Lufkin R. 1998. Genesis of interventional MRI. J. Magn.Reson. Imaging 8:2
3. Jolesz FA. 1998. Interventional and intraoperative MRI: a general overview ofthe field. J. Magn. Reson. Imaging 8:3–7
4. Lufkin RB, ed. 1999. Interventional MRI. St. Louis, MO: Mosby5. Blanco RT, Ojala R, Kariniemi J, Perala J, Niinimaki J, Tervonen O. 2005.
Interventional and intraoperative MRI at low field scanner—a review. Eur. J.Radiol. 56:130–42
6. Cramer SC, Nelles G, Benson RR, Kaplan JD, Parker RA, et al. 1997. A func-tional MRI study of subjects recovered from hemiparetic stroke. Stroke 28:2518–27
7. Dobkin BH, Firestine A, West M, Saremi K, Woods R. 2004. Ankle dorsiflexionas an fMRI paradigm to assay motor control for walking during rehabilitation.Neuroimage 23:370–81
8. Chinzei K, Hata N, Jolesz F, Kikinis R. 2000. MR compatible surgical assistrobot: system integration and preliminary feasibility study. Proc. Med. ImageComput. Comput.-Assisted Intervention, pp. 921–30. Pittsburgh, PA: Springer
9. Chinzei K, Miller K. 2001. Towards MRI guided surgical manipulator. Med.Sci. Monit. 7:153–63
10. Chinzei K, Miller K. 2001. MRI guided surgical robot. Austr. Conf. RoboticsAutomation, pp. 50–5. Sydney: Springer
11. Christoforou E, Akbudak E, Ozcan A, Karanikolas M, Tsekos NV. 2006. Perfor-mance of interventions with manipulator-driven real-time MR-guidance: im-plementation and initial in vitro tests. Magn. Reson. Imaging 25(1):69–77
12. Hata N, Hashimoto R, Tokuda J, Morikawa S. 2005. Needle guiding robot forMR-guided microwave thermotherapy of liver tumor using motorized remote-center-of-motion constraint. Proc. IEEE Int. Conf. Robotics Automation, pp. 1664–68. Barcelona, Spain: IEEE
380 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
13. Hempel E, Fischer H, Gumb L, Hohn T, Krause H, et al. 2003. An MRI-compatible surgical robot for precise radiological interventions. Comput. AidedSurg. 8:180–91
14. Kaiser WA, Fischer H, Vagner J, Selig M. 2000. Robotic system for biopsyand therapy of breast lesions in a high-field whole-body magnetic resonancetomography unit. Invest. Radiol. 35:513–19
15. Koseki Y, Washio T, Chinzei K, Iseki H. 2002. Endoscope manipulator fortrans-nasal neurosurgery, optimized for and compatible to vertical field openMRI. Proc. Med. Image Comput. Comput.-Assisted Intervention, pp. 114–21. Tokyo,Jpn: Springer
16. Krieger A, Susil RC, Menard C, Coleman JA, Fichtinger G, et al. 2005. Designof a novel MRI compatible manipulator for image guided prostate interventions.IEEE Trans. Biomed. Eng. 52:306–13
17. Larson BT, Erdman AG, Tsekos NV, Yacoub E, Tsekos PV, Koutlas IG. 2004.Design of an MRI-compatible robotic stereotactic device for minimally invasiveinterventions in the breast. J. Biomech. Eng. 126:458–65
18. Masamune K, Kobayashi E, Masutani Y, Suzuki M, Dohi T, et al. 1995. De-velopment of an MRI-compatible needle insertion manipulator for stereotacticneurosurgery. J. Image Guid. Surg. 1:242–48
19. Ozcan A, Christoforou E, Brown D, Tsekos NV. 2006. Fast and efficient ra-diological interventions via a graphical user interface commanded magneticresonance compatible robotic device. Annu. Int. Conf. IEEE Eng. Med.Biol. Soc.,28th. New York: IEEE
20. Pfleiderer SO, Marx C, Vagner J, Franke RP, Reichenbach JR, Kaiser WA.2005. Magnetic resonance-guided large-core breast biopsy inside a 1.5-T mag-netic resonance scanner using an automatic system: in vitro experiments andpreliminary clinical experience in four patients. Invest. Radiol. 40:458–63
21. Pfleiderer SO, Reichenbach JR, Azhari T, Marx C, Malich A, et al. 2003. Amanipulator system for 14-gauge large core breast biopsies inside a high-fieldwhole-body MR scanner. J. Magn. Reson. Imaging 17:493–98
22. Susil RC, Camphausen K, Choyke P, McVeigh ER, Gustafson GS, et al. 2004.System for prostate brachytherapy and biopsy in a standard 1.5 T MRI scanner.Magn. Reson. Med. 52:683–87
23. Susil RC, Krieger A, Derbyshire JA, Tanacs A, Whitcomb LL, et al. 2003.System for MR image-guided prostate interventions: canine study. Radiology228:886–94
24. Tajima F, Kishi K, Nishizawa K, Kan K, Ishii H, et al. 2004. A prototypemaster-slave system consisting of two MR-compatible manipulators with inter-changeable surgical tools. Proc. IEEE Int. Conf. Robotics Automation, pp. 2505–10.New Orleans, LA: IEEE
25. Tsekos NV, Shudy J, Yacoub E, Tsekos PV, Koutlas IG. 2001. Developmentof a robotic device for MRI-guided interventions in the breast. Proc. IEEE Int.Symp. Bioinform. Bioeng., pp. 201–8. Washinghton, DC: IEEE
26. Harel N, Ugurbil K, Uludag K, Yacoub E. 2006. Frontiers of brain mappingusing MRI. J. Magn. Reson. Imaging 23:945–57
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 381
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
27. Ogawa S, Menon RS, Tank DW, Kim SG, Merkle H, et al. 1993. Functionalbrain mapping by blood oxygenation level-dependent contrast magnetic reso-nance imaging. A comparison of signal characteristics with a biophysical model.Biophys. J. 64:803–12
28. LeBihan D. 1990. IVIM method measures diffusion and perfusion. Diagn. Imag-ing 12:133, 136
29. Le Bihan D, Urayama S, Aso T, Hanakawa T, Fukuyama H. 2006. Direct andfast detection of neuronal activation in the human brain with diffusion MRI.Proc. Natl. Acad. Sci. USA 103:8263–68
30. Aschoff AJ, Rafie N, Jesberger JA, Duerk JL, Lewin JS. 2000. Thermal le-sion conspicuity following interstitial radiofrequency thermal tumor ablationin humans: a comparison of STIR, turbo spin-echo T2-weighted, and contrast-enhanced T1-weighted MR images at 0.2 T. J. Magn. Reson. Imaging 12:584–89
31. Boaz TL, Lewin JS, Chung YC, Duerk JL, Clampitt ME, Haaga JR. 1998. MRmonitoring of MR-guided radiofrequency thermal ablation of normal liver inan animal model. J. Magn. Reson. Imaging 8:64–69
32. McDannold NJ, Jolesz FA. 2000. Magnetic resonance image-guided thermalablations. Top Magn. Reson. Imaging 11:191–202
33. Merkle EM, Shonk JR, Duerk JL, Jacobs GH, Lewin JS. 1999. MR-guided RFthermal ablation of the kidney in a porcine model. Am. J. Roentgenol. 173:645–51
34. Tacke J, Speetzen R, Adam G, Sellhaus B, Glowinski A, et al. 2001. ExperimentalMR imaging-guided interstitial cryotherapy of the brain. Am. J. Neuroradiol.22:431–40
35. Atalar E, Kraitchman DL, Carkhuff B, Lesho J, Ocali O, et al. 1998. Catheter-tracking FOV MR fluoroscopy. Magn. Reson. Med. 40:865–72
36. Hillenbrand CM, Elgort DR, Wong EY, Reykowski A, Wacker FK, et al. 2004.Active device tracking and high-resolution intravascular MRI using a novelcatheter-based, opposed-solenoid phased array coil. Magn. Reson. Med. 51:668–75
37. Zhang Q, Wendt M, Aschoff AJ, Zheng L, Lewin JS, Duerk JL. 2000. ActiveMR guidance of interventional devices with target-navigation. Magn. Reson.Med. 44:56–65
38. Zhang Q, Wendt M, Aschoff AJ, Lewin JS, Duerk JL. 2001. A multielementRF coil for MRI guidance of interventional devices. J. Magn. Reson. Imaging14:56–62
39. Karmarkar PV, Kraitchman DL, Izbudak I, Hofmann LV, Amado LC, et al.2004. MR-trackable intramyocardial injection catheter. Magn. Reson. Med.51:1163–72
40. Wacker FK, Hillenbrand CM, Duerk JL, Lewin JS. 2005. MR-guided endovas-cular interventions: device visualization, tracking, navigation, clinical applica-tions, and safety aspects. Magn. Reson. Imaging Clin. N. Am. 13:431–39
41. Ladd ME, Zimmermann GG, Quick HH, Debatin JF, Boesiger P, et al. 1998.Active MR visualization of a vascular guidewire in vivo. J. Magn. Reson. Imaging8:220–25
42. Lewin JS, Nour SG, Duerk JL. 2000. Magnetic resonance image-guided biopsyand aspiration. Top Magn. Reson. Imaging 11:173–83
382 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
43. Jolesz FA, Nabavi A, Kikinis R. 2001. Integration of interventional MRI withcomputer-assisted surgery. J. Magn. Reson. Imaging 13:69–77
44. Posse S, Muller-Gartner HW, Dager SR. 1996. Functional magnetic resonancestudies of brain activation. Semin. Clin. Neuropsychiatr. 1:76–88
45. Doyon J. 1997. Skill learning. Int. Rev. Neurobiol. 41:273–9446. Toni I, Ramnani N, Josephs O, Ashburner J, Passingham RE. 2001. Learning ar-
bitrary visuomotor associations: temporal dynamic of brain activity. Neuroimage14:1048–57
47. Karni A, Meyer G, Rey-Hipolito C, Jezzard P, Adams MM, et al. 1998. The ac-quisition of skilled motor performance: fast and slow experience-driven changesin primary motor cortex. Proc. Natl. Acad. Sci. USA 95:861–68
48. Pineiro R, Pendlebury S, Johansen-Berg H, Matthews PM. 2001. FunctionalMRI detects posterior shifts in primary sensorimotor cortex activation afterstroke: evidence of local adaptive reorganization? Stroke 32:1134–39
49. Johansen-Berg H, Dawes H, Guy C, Smith SM, Wade DT, Matthews PM.2002. Correlation between motor improvements and altered fMRI activity afterrehabilitative therapy. Brain 125:2731–42
50. Gronemeyer DH, Seibel RM, Schmidt A, Melzer A, Dell M. 1996. Two- andthree-dimensional imaging for interventional MRI and CT guidance. Stud.Health Technol. Inform. 29:62–76
51. Scholz M, Deli M, Wildforster U, Wentz K, Recknagel A, et al. 1996. MRI-guided endoscopy in the brain: a feasability study. Minim. Invasive Neurosurg.39:33–37
52. Felden A, Vagner J, Hinz A, Fischer H, Pfleiderer SO, et al. 2002. ROBITOM-robot for biopsy and therapy of the mamma. Biomed. Tech. 47:2–5
53. Tsekos NV, Ozcan A, Christoforou E. 2005. A prototype manipulator for MR-guided interventions inside standard cylindrical MRI scanners. J. Biomech. Eng.127:972–80
54. Kim SG, Ugurbil K. 1997. Functional magnetic resonance imaging of the hu-man brain. J. Neurosci. Methods 74:229–43
55. Yue GH, Liu JZ, Siemionow V, Ranganathan VK, Ng TC, Sahgal V. 2000.Brain activation during human finger extension and flexion movements. BrainRes. 856:291–300
56. Calautti C, Baron JC. 2003. Functional neuroimaging studies of motor recoveryafter stroke in adults: a review. Stroke 34:1553–66
57. Kim YH, Park JW, Ko MH, Jang SH, Lee PK. 2004. Plastic changes of motornetwork after constraint-induced movement therapy. Yonsei. Med. J. 45:241–46
58. Cramer SC, Benson RR, Himes DM, Burra VC, Janowsky JS, et al. 2005. Useof functional MRI to guide decisions in a clinical stroke trial. Stroke 36:e50–52
59. Lindberg P, Schmitz C, Forssberg H, Engardt M, Borg J. 2004. Effects ofpassive-active movement training on upper limb motor function and corticalactivation in chronic patients with stroke: a pilot study. J. Rehabil. Med. 36:117–23
60. Pariente J, Loubinoux I, Carel C, Albucher JF, Leger A, et al. 2001. Fluoxetinemodulates motor performance and cerebral activation of patients recoveringfrom stroke. Ann. Neurol. 50:718–29
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 383
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
61. Luft AR, McCombe-Waller S, Whitall J, Forrester LW, Macko R, et al. 2004.Repetitive bilateral arm training and motor cortex activation in chronic stroke:a randomized controlled trial. JAMA 292:1853–61
62. Carey JR, Kimberley TJ, Lewis SM, Auerbach EJ, Dorsey L, et al. 2002. Analysisof fMRI and finger tracking training in subjects with chronic stroke. Brain125:773–88
63. Kimberley TJ, Lewis SM, Auerbach EJ, Dorsey LL, Lojovich JM, CareyJR. 2004. Electrical stimulation driving functional improvements and corticalchanges in subjects with stroke. Exp. Brain Res. 154:450–60
64. Riener R, Villgrattner T, Kleiser R, Nef T, Kollias S. 2005. fMRI-compatibleelectromagnetic haptic interface. Proc. IEEE Eng. Med. Biol. Soc., 27th, Annu.Int. Conf., pp. 7024, Shanghai, China
65. Diedrichsen J, Hashambhoy Y, Rane T, Shadmehr R. 2005. Neural correlatesof reach errors. J. Neurosci. 25:9919–31
66. Gassert R, Dovat L, Lambercy O, Ruffieux Y, Chapuis D, et al. 2006. A 2-DOF fMRI compatible haptic interface to investigate the neural control of armmovements. Proc. IEEE Int. Conf. Robotics Automation, pp. 3825, Orlando, FL
67. Izawa J, Shimizu T, Gomi H, Toyama S, Ito K. 2006. MR compatible manip-ulandum with ultrasonic motor for fMRI studies. Proc. IEEE Int. Conf. RoboticsAutomation, pp. 3850. Orlando, FL: IEEE
68. Cramer SC, Weisskoff RM, Schaechter JD, Nelles G, Foley M, et al. 2002.Motor cortex activation is related to force of squeezing. Hum. Brain Mapp.16:197–205
69. Hidler J, Mbwana J, Zeffiro T. 2005. MRI compatible force sensing system forreal-time monitoring of wrist moments during fMRI testing. Proc. IEEE Int.Conf. Rehabilitation Robotics, 9th, pp. 212, Chicago, IL
70. Liu JZ, Dai TH, Elster TH, Sahgal V, Brown RW, Yue GH. 2000. Simultaneousmeasurement of human joint force, surface electromyograms, and functionalMRI-measured brain activation. J. Neurosci. Methods 101:49–57
71. Schaechter JD, Stokes C, Connell BD, Perdue K, Bonmassar G. 2006. Fingermotion sensors for fMRI motor studies. Neuroimage 31:1549–59
72. Graham SJ, Staines WR, Nelson A, Plewes DB, McIlroy WE. 2001. New de-vices to deliver somatosensory stimuli during functional MRI. Magn. Reson.Med. 46:436–42
73. Harrington GS, Wright CT, Downs JH. 2000. A new vibrotactile stimulatorfor functional MRI. Hum. Brain Mapp. 10:140–45
74. Zappe AC, Maucher T, Meier K, Scheiber C. 2004. Evaluation of a pneumati-cally driven tactile stimulator device for vision substitution during fMRI studies.Magn. Reson. Med. 51:828–34
75. Ugurbil K, Adriany G, Andersen P, Chen W, Garwood M, et al. 2003. Ultra-high field magnetic resonance imaging and spectroscopy. Magn. Reson. Imaging21:1263–81
76. Schenck JF. 1998. MR safety at high magnetic fields. Magn. Reson. Imaging Clin.N. Am. 6:715–30
77. Schenck JF. 2000. Safety of strong, static magnetic fields. J. Magn. Reson. Imaging12:2–19
384 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
78. Shellock FG, Crues JV. 2004. MR procedures: biologic effects, safety, and pa-tient care. Radiology 232:635–52
79. Moscatel MA, Shellock FG, Morisoli SM. 1995. Biopsy needles and devices:assessment of ferromagnetism and artifacts during exposure to a 1.5-T MRsystem. J. Magn. Reson. Imaging 5:369–72
80. Shellock FG, Shellock VJ. 1998. Cardiovascular catheters and accessories: exvivo testing of ferromagnetism, heating, and artifacts associated with MRI. J.Magn. Reson. Imaging 8:1338–42
81. Shellock FG. 2000. Radiofrequency energy-induced heating during MR pro-cedures: a review. J. Magn. Reson. Imaging 12:30–36
82. Keeler EK, Casey FX, Engels H, Lauder E, Pirto CA, et al. 1998. Accessoryequipment considerations with respect to MRI compatibility. J. Magn. Reson.Imaging 8:12–18
83. FDA, Group CMRW. 1997. A primer on medical device interactions withmagnetic resonance imaging systems. http://www.fda.gov/cdrh/ode/primerf6.html.
84. Jolesz FA, Morrison PR, Koran SJ, Kelley RJ, Hushek SG, et al. 1998. Com-patible instrumentation for intraoperative MRI: expanding resources. J. Magn.Reson. Imaging 8:8–11
85. Schueler BA, Parrish TB, Lin JC, Hammer BE, Pangrle BJ, et al. 1999. MRIcompatibility and visibility assessment of implantable medical devices. J. Magn.Reson. Imaging 9:596–603
86. Chinzei K, Kikinis R, Jolesz FA. 1999. MR compatibility of mechatronic devices:design criteria. Proc. Med. Image Comput. Comput.-Assisted Intervention, pp. 1020–31. Cambridge, UK: Springer
87. Dempsey MF, Condon B, Hadley DM. 2001. Investigation of the factors re-sponsible for burns during MRI. J. Magn. Reson. Imaging 13:627–31
88. Schenck JF. 1996. The role of magnetic susceptibility in magnetic resonanceimaging: MRI magnetic compatibility of the first and second kinds. Med. Phys.23:815–50
89. Kim D, Kobayashi E, Dohi T, Sakuma I. 2002. A new, compact MR-compatiblesurgical manipulator for minimally invasive liver surgery. Proc. Med. Image Com-put. Comput.-Assisted Intervention, pp. 164–69, Tokyo, Jpn
90. Moser R, Gassert R, Burdet E, Sache L, Woodtli HR, et al. 2003. An MRcompatible robot technology. Proc. IEEE Int. Conf. Robotics Automation, pp. 670–75, Taipei, Taiwan
91. Stoianovici D, Patriciu A, Mazilu D, Petrisor D, Kavoussi LR. 2007. Pneumaticstep motor. IEEE/ASME Transac. Mechatron. In press
92. Muntener M, Patriciu A, Petrisor D, Mazilu D, Kavoussi L, et al. 2007. MRIguided robotic system for fully automated brachytherapy seed placement. Urol-ogy. In press
93. Vogan J, Wingert A, Plante JS, Dubowsky S, Hafez M, et al. 2004. Manipulationin MRI devices using electrostrictive polymer actuators: with an application toreconfigurable imaging coils. Proc. IEEE Int. Conf. Robotics Automation, pp. 2498–504, New Orleans, LA
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 385
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
94. Yamamoto A, Ichiyanagi K, Higuchi T, Imamizu H, Gassert R, et al. 2005.Evaluation of MR-compatibility of electrostatic linear motor. Proc. IEEE Int.Conf. Robotics Automation, pp. 3669–74, Barcelona, Spain
95. Khanicheh A, Muto A, Triantafyllou C, Weinberg L, Astrakas L, et al. 2005.MR compatible ERF driven hand rehabilitation device. In Proc. IEEE Int. Conf.Rehabilitation Robotics, 9th, pp. 7–12. Chicago, IL. Piscataway, NJ: Inst. ElectricsElectron. Eng. Comput. Soc.
96. Khanicheh A, Muto A, Trlantafyllou C, Weinberg B, Astrakas L, et al. 2005.MR compatible ERF driven hand device for rehabilitation after stroke. ASMEInt. Conf. Robot Dyn. Contr., pp. IMECE2005-82283, Orlando, FL. New York:Am. Soc. Mech. Eng.
97. Khanicheh A, Muto A, Triantafyllou C, Weinberg B, Astrakas L, et al. 2006.fMRI-compatible rehabilitation hand device. J. Neuroeng. Rehabil. 3:24
98. Christoforou E, Tsekos NV. 2006. Robotic manipulators with remotely-actuated joints: implementation using drive shafts and u-joints. Proc. IEEE Int.Conf. Robotics Automation, pp. 2886–71, Orlando, FL
99. Koseki Y, Kikinis R, Jolesz F, Chinzei K. 2004. Precise evaluation of position-ing repeatability of MR-compatible manipulator inside MRI. Proc. Med. ImageComput. Comput.-Assisted Intervention, pp. 192–99. Rennes, France: Springer
100. Takahashi N, Tada M, Ueda J, Matsumoto Y, Ogasawara T. 2003. An optical6-axis force sensor for brain function analysis using fMRI. Proc. IEEE Int. Conf.Sensors, pp. 253–58, Toronto, Canada
101. Gassert R, Moser R, Burdet E, Bleuler H. 2006. MRI/fMRI-compatible roboticsystem with force feedback for interaction with human motion. IEEE/ASMETransact. Mechatron. 11:216
102. Tada M, Kanade T. 2004. Development of an MR-compatible optical forcesensor. Proc. Int. Conf. IEEE EMBS, pp. 2022–2, San Francisco, CA
103. Hidler J, Hodics T, Xu B, Dobkin B, Cohen LG. 2006. MR compatible forcesensing system for real-time monitoring of wrist moments during fMRI testing.J. Neurosci. Methods 155:300–7
104. Bock M, Melzer A, Bardenheuer H, Ghaderi H, Gutmann B, et al. 2005. MR-Guided percutaneous interventions using a robotic assistance system: initialexperiences in a pig model. Proc. Int. Soc. Mag. Reson. Med. p. 2662
105. Dumoulin CL, Souza SP, Darrow RD. 1993. Real-time position monitoring ofinvasive devices using magnetic resonance. Magn. Reson. Med. 29:411–15
106. Gui D, Tsekos NV. 2006. Fast magnetization-driven preparation for imaging ofcontrast-enhanced coronary arteries during intra-arterial injection of contrastagent. J. Magn. Reson. Imaging 24:1151–58
107. Chinzei K, Yoshinaka K, Washio T. 2006. Numerical simulations and lab testsfor design of MR-compatible robots. Proc. IEEE Int. Conf. Robotics Automation,pp. 3819–24, Orlando, FL
108. Deibert E, Kraut M, Kremen S, Hart JJ. 1999. Neural pathways in tactile objectrecognition. Neurology 52:1413–17
109. Valenza N, Ptak R, Zimine I, Badan M, Lazeyras F, Schnider A. 2001. Disso-ciated active and passive tactile shape recognition: a case study of pure tactileapraxia. Brain 124:2287–98
386 Tsekos et al.
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

ANRV317-BE09-12 ARI 7 June 2007 18:44
110. Golaszewski SM, Siedentopf CM, Baldauf E, Koppelstaetter F, Eisner W, et al.2002. Functional magnetic resonance imaging of the human sensorimotor cor-tex using a novel vibrotactile stimulator. Neuroimage 17:421–30
111. Golaszewski SM, Zschiegner F, Siedentopf CM, Unterrainer J, Sweeney RA,et al. 2002. A new pneumatic vibrator for functional magnetic resonance imagingof the human sensorimotor cortex. Neurosci. Lett. 324:125–28
112. Briggs RW, Dy-Liacco I, Malcolm MP, Lee H, Peck KK, et al. 2004. A pneu-matic vibrotactile stimulation device for fMRI. Magn. Reson. Med. 51:640–43
113. Chapuis D, Gassert R, Sache L, Burdet E, Bleuler H. 2004. Design of a simpleMRI/fMRI compatible force/torque sensor. Proc. IEEE/RSJ Int. Conf. IntelligentRobots Systems, pp. 2593–99, Sendal, Jpn
114. Ku J, Mraz R, Baker N, Zakzanis KK, Lee JH, et al. 2003. A data glove withtactile feedback for FMRI of virtual reality experiments. Cyberpsychol. Behav.6:497–508
115. Mraz R, Hong J, Quintin G, Staines WR, McIlroy WE, et al. 2003. A platformfor combining virtual reality experiments with functional magnetic resonanceimaging. Cyberpsychol. Behav. 6:359–68
116. Cheng CP, Schwandt DF, Topp EL, Anderson JH, Herfkens RJ, Taylor CA.2003. Dynamic exercise imaging with an MR-compatible stationary cycle withinthe general electric open magnet. Magn. Reson. Med. 49:581–85
117. Chitwood WRJ, Nifong LW. 2000. Minimally invasive videoscopic mitral valvesurgery: the current role of surgical robotics. J. Card. Surg. 15:61–75
118. Hockstein NG, Weinstein GS, O’Malley BW Jr. 2005. Maintenance ofhemostasis in transoral robotic surgery. J. Otorhinolaryngol. Relat. Spec. 67:220–24
119. Krieger A, Susil RC, Fichtinger G, Atalar E, Whitcomb LL. 2004. Design ofa novel MRI compatible manipulator for image guided prostate intervention.Proc. IEEE Int. Conf. Robotics Automation, pp. 377–82, New Orleans, LA
www.annualreviews.org • MR-Compatible Robotic and Mechatronics Systems 387
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

AR317-FM ARI 7 June 2007 19:9
Annual Reviewof BiomedicalEngineering
Volume 9, 2007Contents
Cell Mechanics: Integrating Cell Responses to Mechanical StimuliPaul A. Janmey and Christopher A. McCulloch � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 1
Engineering Approaches to BiomanipulationJaydev P. Desai, Anand Pillarisetti, and Ari D. Brooks � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 35
Forensic Injury BiomechanicsWilson C. Hayes, Mark S. Erickson, and Erik D. Power � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 55
Genetic Engineering for Skeletal Regenerative MedicineCharles A. Gersbach, Jennifer E. Phillips, and Andrés J. García � � � � � � � � � � � � � � � � � � � � � � 87
The Structure and Function of the Endothelial Glycocalyx LayerSheldon Weinbaum, John M. Tarbell, and Edward R. Damiano � � � � � � � � � � � � � � � � � � � � � �121
Fluid-Structure Interaction Analyses of Stented Abdominal AorticAneurysmsC. Kleinstreuer, Z. Li, and M.A. Farber � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �169
Analysis of Time-Series Gene Expression Data: Methods, Challenges,and OpportunitiesI.P. Androulakis, E. Yang, and R.R. Almon � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �205
Interstitial Flow and Its Effects in Soft TissuesMelody A. Swartz and Mark E. Fleury � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �229
Nanotechnology Applications in CancerShuming Nie, Yun Xing, Gloria J. Kim, and Jonathan W. Simons � � � � � � � � � � � � � � � � � �257
SNP Genotyping: Technologies and Biomedical ApplicationsSobin Kim and Ashish Misra � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �289
Current State of Imaging Protein-Protein Interactions In Vivo withGenetically Encoded ReportersVictor Villalobos, Snehal Naik, and David Piwnica-Worms � � � � � � � � � � � � � � � � � � � � � � � � � � �321
Magnetic Resonance–Compatible Robotic and Mechatronics Systemsfor Image-Guided Interventions and Rehabilitation: A Review StudyNikolaos V. Tsekos, Azadeh Khanicheh, Eftychios Christoforou,and Constantinos Mavroidis � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �351
v
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.

AR317-FM ARI 7 June 2007 19:9
SQUID-Detected Magnetic Resonance Imaging in Microtesla FieldsJohn Clarke, Michael Hatridge, and Michael Moßle � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �389
Ultrasound Microbubble Contrast Agents: Fundamentals andApplication to Gene and Drug DeliveryKatherine Ferrara, Rachel Pollard, and Mark Borden � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �415
Acoustic Detection of Coronary Artery DiseaseJohn Semmlow and Ketaki Rahalkar � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �449
Computational Anthropomorphic Models of the Human Anatomy:The Path to Realistic Monte Carlo Modeling in Radiological SciencesHabib Zaidi and Xie George Xu � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �471
Breast CTStephen J. Glick � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �501
Noninvasive Human Brain StimulationTimothy Wagner, Antoni Valero-Cabre, and Alvaro Pascual-Leone � � � � � � � � � � � � � � � � � � �527
Design of Health Care Technologies for the Developing WorldRobert A. Malkin � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �567
Indexes
Cumulative Index of Contributing Authors, Volumes 1–9 � � � � � � � � � � � � � � � � � � � � � � � � � � �589
Cumulative Index of Chapter Titles, Volumes 1–9 � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �593
Errata
An online log of corrections to Annual Review of Biomedical Engineering chapters(if any, 1977 to the present) may be found at http://bioeng.annualreviews.org/
vi Contents
Ann
u. R
ev. B
iom
ed. E
ng. 2
007.
9:35
1-38
7. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by U
nive
rsity
of
Lim
eric
k (U
L)
on 0
5/22
/13.
For
per
sona
l use
onl
y.