Embed Size (px)
Citation preview

ELSEVIER
Int. J. Radiation Oncology Biol. Phys., Vol. 37, No. 4, pp. 827-832, 1997 Copyright 0 1997 Elsevier Science Inc. Printed in the USA. All rights reserved
03m-3016/97 $17.00 + .I0
PII SO360-3016(96)00545-7
l Clinical Investigation
MAGNETIC RESONANCE IMAGING IN THE TREATMENT PLANNING OF RADIATION THERAPY IN CARCINOMA OF THE CERVIX TREATED WITH
THE FOUR-FIELD PELVIC TECHNIQUE
LAURENCE THOMAS, M.D.,* Bosco CHACON, M.D.,* MICHBLE KIND, M.D.,+ OLIVIER LASBAREILLES,” PIET MUYLDERMANS, M.D.,* ANTONY CHEMIN,*
ALAIN LE TREUT, M.D.,+ JAQUES PIGNEUX, M.D.* AND GUY KANTOR, M.D.* Departments of *Radiotherapy and ‘Radiology, Institut BergoniC, Comprehensive Cancer Center, Bordeaux, France
Purpose: To evaluate magnetic resonance imaging (MRI) in the planning of radiation therapy for patients with carcinoma of the cervix treated with a four-field technique. Methods and Materials: Between May 1994 and February 1995,18 patients with carcinoma of the cervix were entered in the study (1 Tl N-; 2 T2a N-; 1 T2b NO; 10 T2b N-; 2 T2b N+; 2 T3b N+). Node status was assessed by a laparoscopic pelvic lymphadenectomy. During the first step, all the patients were simulated with an isocentrlc four-field pelvic technique. In one group (11 patients) simulation was done based on clinical ex- amination, computed tomography (CT), and standard guidelines. In the second group (seven patients) simulation was based on clinical examination, CT, and with the help of diagnostic MRI, which was available at that time. During the second step, MRI in treatment position with skin markings of the isocenter of the radiation fields was then performed in every patient. During the third step, in each patient, the simulated radiation fields were correlated with the MRI defined target volume by superimposing them on midsaglttal and midcoronal MR images. The adequacy of the margins was arbitrarly defined as 1 cm around the MRI defined target volume (tumor of the cervix and its extension, and uterus). Results: In the first group (11 patients), MRI in treatment position led to a change in 7 patients: six inadequate margins in the lateral fields and one in the anterior and lateral field. In almost all the cases, the adjustments were of an increase of 10 mm, equally matched between the anterior and posterior borders of the lateral fields. In the second group (seven patients), MRI in treatment position has led to a change in lateral fields in five patients. The mean adjustment was 10 mm: four increases (two anterior border, one posterior border, one anterior and pos- terior border), and one decrease of the posterior border. In the two groups, modifications of the anterior border of the lateral fields have allowed adequate margins around the uterine fundus and modifications of the posterior border have allowed adequate coverage of the cervical tumor. Conclusion: When treating carcinoma of the cervix with a four-field radiation technique, standard portals do not exist. The design of lateral fields has to be based on individual morbid anatomy, which is given accurately by diagnostic MRI. Magnetic resonance imaglng in treatment position assesses the design of simulated lateral fields. 0 1997 Elsevier Science Inc.
Carcinoma of the cervix, Radiation treatment planning, Magnetic resonance imaging.
INTRODUCTION
Radiotherapy is curative in carcinoma of the cervix, es- pecially in nonadvanced cervical tumors. Radiotherapy is often performed using a four-field technique called box technique (anterior, posterior, and lateral fields). The ob- jective is to use portals that will include the clinical target volume (tumor and all tissues at significant risk for spread) (9) but exclude the maximum amount of normal surround- ing critical structures (16).
of tumor involvement because of its well-known soft tis- sue contrast (3, 8, 1.5), and MRI allows direct imaging in sagittal, coronal, and transverse plans without recon- struction.
Usually the treatment fields are established with stan- dard simulation techniques based on clinical (palpatory) and CT findings and with the help of anatomic and radio- graphic guidelines defined in standard radiotherapy text- books (2, 14).
Magnetic resonance imaging has been found to be su- The purpose of this study was tomevaluate MFU in the perior in delineating the normal anatomy and the extent radiation treatment planning of tumors of the cervix, es-
Reprint requests to: Laurence Thomas, M.D., Department of Radiotherapy, Institut BergoniC, Regional Cancer Center, 180, rue de Saint-Gen&s, 33076 Bordeaux Cedex, France. Acknowledgements-The work with regard to the geometric ac-
curacy of MRI (1, 13) was supported by grants from Ligue Na- tionale Contre le Cancer, Con&? DCpartemental du Lot-et-Ga- ronne de la Ligue Nationale Contre le Cancer (Dr. DELAGE, President), and P81e RCgional GBM Aquitaine.
827
828 I. J. Radiation Oncology 0 Biology 0 Physics
pecially the potential benefit of sagittal and coronal im- aging for target volume delineation on lateral, anterior, and posterior fields (18). This study tries to answer the question: is diagnosic MR Imaging beneficient and suffi- cient to design lateral, and anterior posterior fields? What can bring MR Imaging in treatment position?
METHODS AND MATERIALS
Between May 1994 and February 1995,18 patients with invasive carcinoma of the cervix entered this prospective study. The eligibility criteria included: carcinoma of the cervix receiving no initial surgery on the cervix and no induction chemotherapy, with no clinical involvement of the uterosacral ligaments, and tumor of the cervix for which a four-field pelvic radiotherapy was decided (Tl, T2, small T3).
There were 13 patients with squamous cell carcinoma, 4 with adenocarcinoma, and 1 with undifferentiated car- cinoma. Clinical staging included physical examination by a gynecologic staff (surgeon, radiation oncologist, and gy- necologic oncologist), biopsy of the lesion, abdominopel- vie computed tomography (eight cases), lymphangiogra- phy (six cases), chest radiography, and routine blood cell counts.
Diagnostic MRI was added in the staging procedure and was done before simulation according to the availability of the MRI unit.
In 17 patients the node status was determined by a la- paroscopic pelvic lymphadenectomy. The extent of the disease was staged according to the TNM classification modified by the histological results of lymphadenectomy: 1 Tlb N(-); 2 T2A N(-); 10 T2b N(-); 2 T2b N(+); 1 T2b NO; 2 T3B N(+); all patients were MO.
At the simulation time, two situations occured: (a) be- cause of logistic delays, the diagnostic MRI was not done before simulation, but at the same time as the treatment planning MRI (11 patients: Group 1); (b) the diagnostic MR imaging was available at the simulation time (7 pa- tients: Group 2).
The MRI technique was different according to the type of MRI realized (diagnostic and treatment planning MRI).
For the diagnostic MRI, patients were scanned supine (curved table surface). Images were generated in trans- verse coronal and sagittal planes, using strength 1 Tesla. I T1 and Tz-weighted images were obtained with a phased array coil to improve spatial resolution and images were not magnified.
For the MRI treatment planning, patients were scanned supine in treatment position (flat table surface). The skin markings of the isocenters were placed and turbo spinecho T2 images with a body coil were generated in transverse sagittal and coronal planes.
Volume 37, Number 4, 1997
Step 1: standard radiologic simulation All patients underwent simulation films with an isocen-
tric four-field technique (anterior, posterior, and lateral fields). The patients were simulated in supine position.
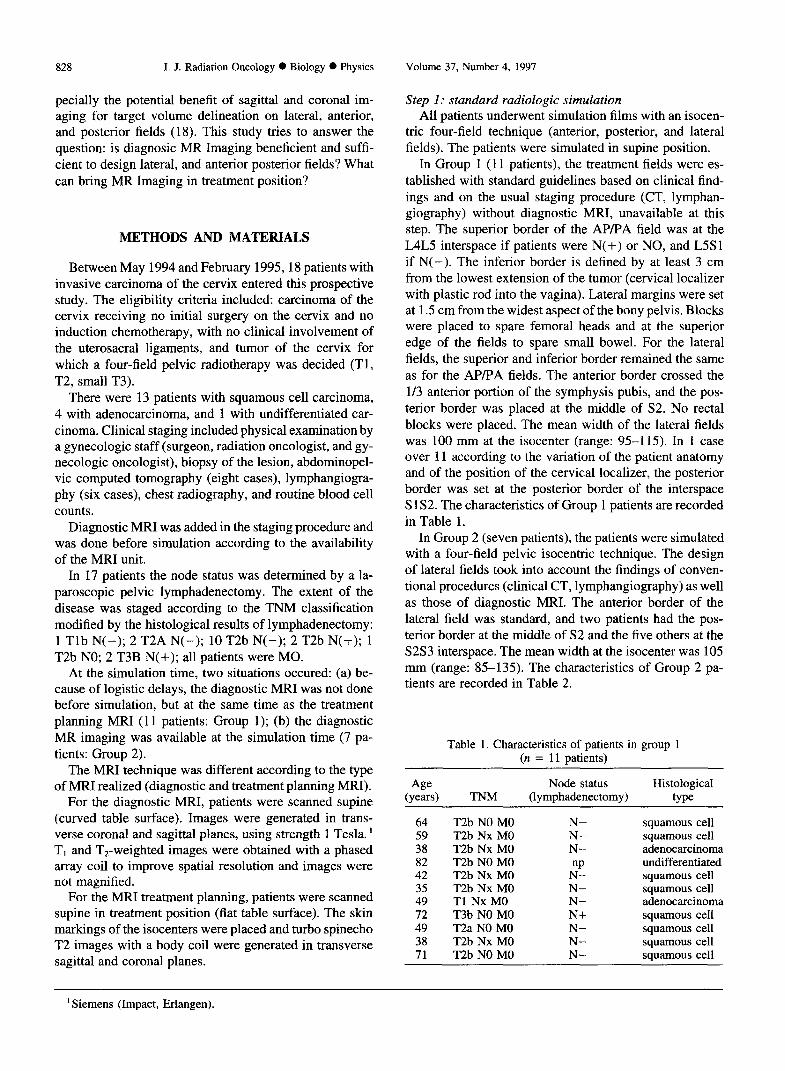
In Group 1 (11 patients), the treatment fields were es- tablished with standard guidelines based on clinical find- ings and on the usual staging procedure (CT, lymphan- giography) without diagnostic MRI, unavailable at this step. The superior border of the AP/PA field was at the L4L5 interspace if patients were N( +) or NO, and L5S 1 if N(-). The inferior border is defined by at least 3 cm from the lowest extension of the tumor (cervical localizer with plastic rod into the vagina). Lateral margins were set at 1.5 cm from the widest aspect of the bony pelvis. Blocks were placed to spare femoral heads and at the superior edge of the fields to spare small bowel. For the lateral fields, the superior and inferior border remained the same as for the APiPA fields. The anterior border crossed the l/3 anterior portion of the symphysis pubis, and the pos- terior border was placed at the middle of S2. No rectal blocks were placed. The mean width of the lateral fields was 100 mm at the isocenter (range: 95-l 15). In 1 case over 11 according to the variation of the patient anatomy and of the position of the cervical localizer, the posterior border was set at the posterior border of the interspace S 1 S2. The characteristics of Group 1 patients are recorded in Table 1.
In Group 2 (seven patients), the patients were simulated with a four-field pelvic isocentric technique. The design of lateral fields took into account the findings of conven- tional procedures (clinical CT, lymphangiography) as well as those of diagnostic MRI. The anterior border of the lateral field was standard, and two patients had the pos- terior border at the middle of S2 and the five others at the S2S3 interspace. The mean width at the isocenter was 105 mm (range: 85-135). The characteristics of Group 2 pa- tients are recorded in Table 2.
Table 1. Characteristics of patients in group 1 (n = 11 patients)
Age Node status Histological (ye=s) TNM (lymphadenectomy) We
64 T2b NO MO N- squamous cell 59 T2b Nx MO N- squamous cell 38 T2b Nx MO N- adenocarcinoma 82 T2b NO MO undifferentiated 42 T2b Nx MO ,“! squamous cell 35 T2b Nx MO N- squamous cell 49 Tl Nx MO N- adenocarcinoma 72 T3b NO MO N+ squamous cell 49 T2a NO MO N- squamous cell 38 T2b Nx MO N- squamous cell 71 T2b NO MO N- squamous cell
’ Siemens (Impact, Erlangen).
MRI in treatment planning in carcinoma of the cervix 0 L. THOMAS er al. 829
Table 2. Characteristics of patients in group 2 (n = 7 patients)
Age Node status Histological (ye=4 (lymphadenectomy) type
39 T2b Nl MO N+ adenocarcinoma 30 T2b Nx MO N- adenocarcinoma 38 T2b Nl MO N- squamous cell 44 T2b Nl MO N- squamous cell 44 T2b NO MO N+ squamous cell 52 T2a NO MO N- squamous cell 67 T3b Nl MO N-t squamous cell
Step 2: MRI treatment planning (in treatment position) In all our patients an MR imaging was done in treatment
position on a flat table surface (supine position used for their radiation treatment).
The skin markings of the isocenter of the radiation fields (anterior and lateral) were outlined with plastic tubes filled with lipiodol. The plastic tubes were included in a Plexi- glas block so they were more easily demonstrated on the MR images. Patients were scanned according to the tech- nique described above.
Evaluation of the geometric accuracy of MRI has been previously studied and described (1, 13). Within the size of the field of view (Fov) used (1400 mm), the risk of distortion is comparable with the size of a pixel. The op- timal sequences have been studied related to pelvic tumors and skin landmarkings.
Step 3: MRI assisted target dejnition The adequacy of the simulated variation ports was then
evaluated by correlating them with MRI defined tumor volume and its potential extension. A margin of at least 1 cm around the tumor of the cervix and its extension and around the uterus was considered as adequate. For each patient, the simulated lateral radiation field was superim- posed on the midsagittal plane MR image and the simu- lated anterior radiation field on the coronal MR image, which crossed by the isocenters of the lateral fields.
The adequacy was evaluated by two radiation oncologists.
RESULTS
The results are presented according to each group of patients based on the availability of diagnostic MRI at the simulation time.
Group 1 (II patients) Ten of 11 patients were simulated according to standard
guidelines. Inadequate margin of tumor volume was ar- bitrarily defined as less than 1 cm of normal tissue around the tumor of the cervix and its extension, and the uterus. Magnetic resonance imaging in treatment position led to a change in seven patients (63%): six inadequate margins of lateral fields and one of the anterior and lateral fields.
Fig. 1. Lateral simulated film (patient Group 1). Adenocarcinoma of the cervix T2b N-.
When an increase of the lateral fields was necessary and led to a relative sparing of a very small part of the rectum, the advantage of using lateral fields was questionable and we preferred to change the technique from four-field to two-field anterior posterior in four out of seven patients. The adjustments of the portals were minimal with an in-
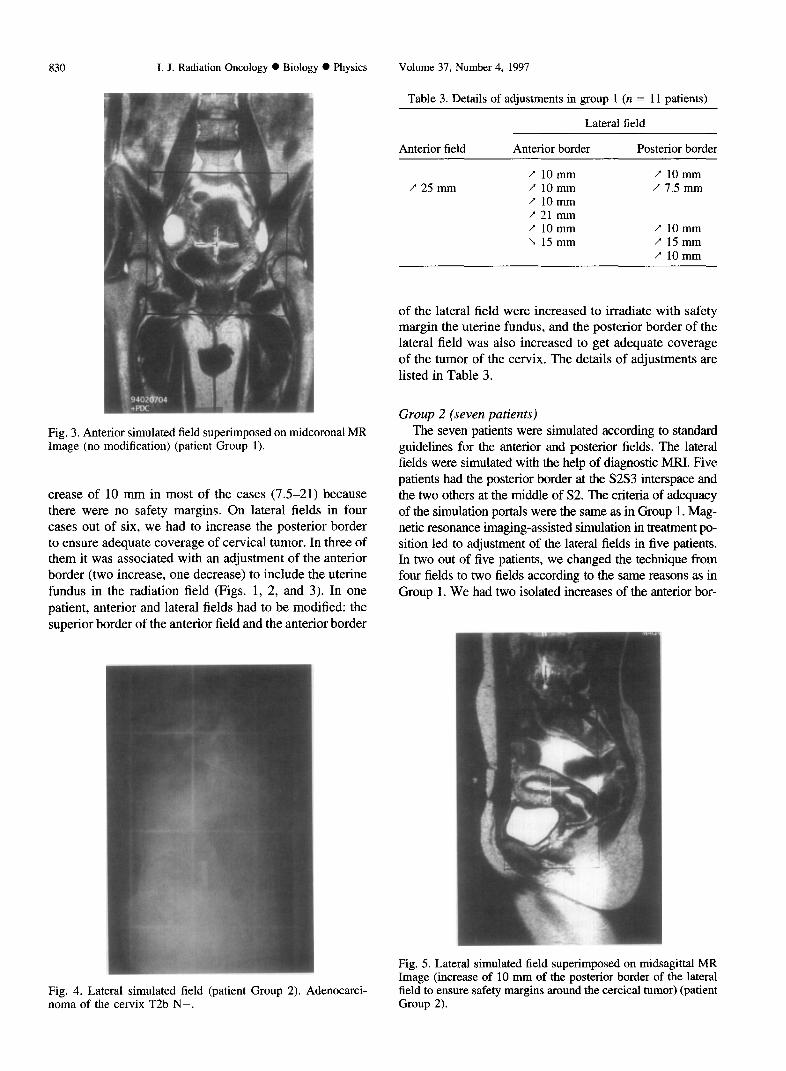
Fig. 2. Lateral field superimposed on midsagittal Magnetic Res- onance (MR) Image (increase of 10 mm of the anterior and posterior border to give adequate margin around the uterine fun- dus and around the posterior border of the cervical tumor) (pa- tient group 1).
830 I. J. Radiation Oncology 0 Biology 0 Physics Volume 37, Number 4, 1997
Fig. 3. Anterior simulated field superimposed on midcoronal MR Image (no modification) (patient Group 1).
crease of 10 mm in most of the cases (7.5-21) because there were no safety margins. On lateral fields in four cases out of six, we had to increase the posterior border to ensure adequate coverage of cervical tumor. In three of them it was associated with an adjustment of the anterior border (two increase, one decrease) to include the uterine fundus in the radiation field (Figs. 1, 2, and 3). In one patient, anterior and lateral fields had to be modified: the superior border of the anterior field and the anterior border
Table 3. Details of adjustments in group 1 (n = 11 patients)
Lateral field
Anterior field Anterior border Posterior border
/” 1omm 7 10mm / 25 mm / 10mm / 7.5 mm
/ 1omm 7 21 mm / 10mm F 10mm L 15mm / 15mm
/ 10mm
of the lateral field were increased to irradiate with safety margin the uterine fundus, and the posterior border of the lateral field was also increased to get adequate coverage of the tumor of the cervix. The details of adjustments are listed in Table 3.
Group 2 (seven patients) The seven patients were simulated according to standard
guidelines for the anterior and posterior fields. The lateral fields were simulated with the help of diagnostic MRI. Five patients had the posterior border at the S2S3 interspace and the two others at the middle of S2. The criteria of adequacy of the simulation portals were the same as in Group 1. Mag- netic resonance imaging-assisted simulation in treatment po- sition led to adjustment of the lateral fields in five patients. In two out of five patients, we changed the technique from four fields to two fields according to the same reasons as in Group 1. We had two isolated increases of the anterior bor-
Fig. 4. Lateral simulated field (patient Group 2). Adenocarci- noma of the cervix T2b N-.
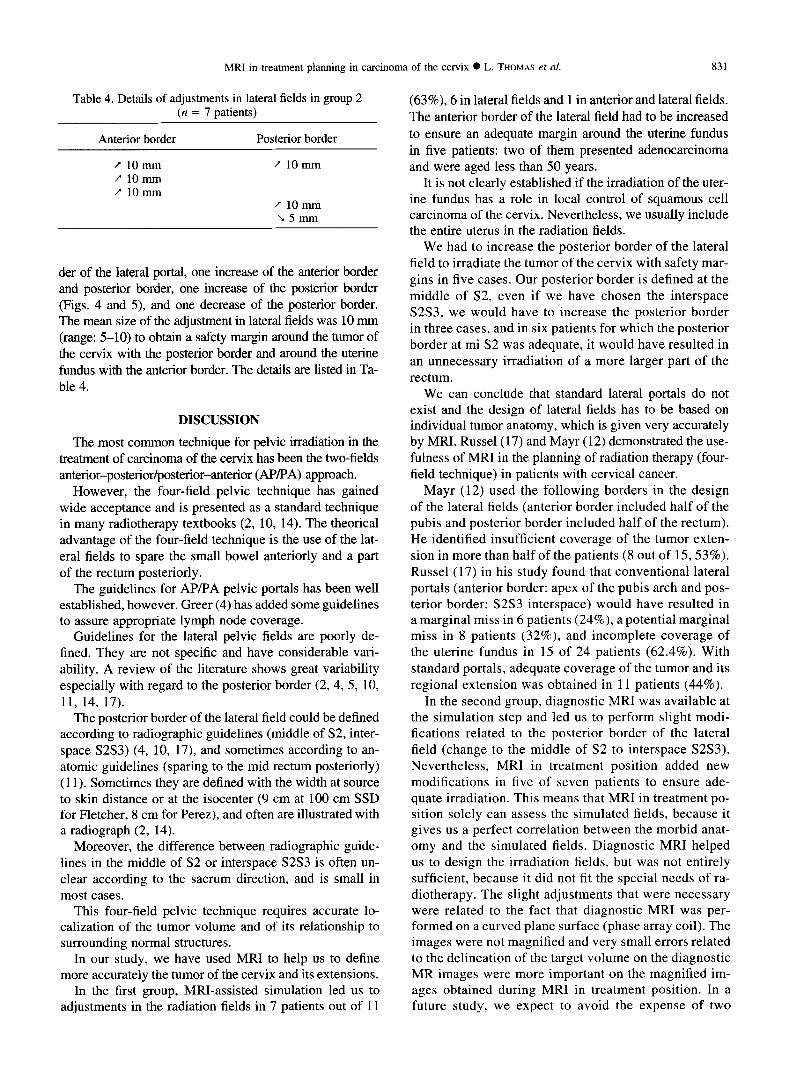
Fig. 5. Lateral simulated field superimposed on midsagittal MR Image (increase of 10 mm of the posterior border of the lateral field to ensure safety margins around the cercical tumor) (patient Group 2).
MRI in treatment planning in carcinoma of the cervix 0 L. THOMAS et al. 831
Table 4. Details of adjustments in lateral fields in group 2 (n = 7 patients)
Anterior border
/ 1onnn Y 1omm / 10mm
Posterior border
f 1omm
/” 1omm Mmtn
der of the lateral portal, one increase of the anterior border and posterior border, one increase of the posterior border (Figs. 4 and 5), and one decrease of the posterior border. The mean size of the adjustment in lateral fields was 10 mm (range: 5-10) to obtain a safety margin around the tumor of the cervix with the posterior border and around the uterine fundus with the anterior border. The details are listed in Ta- ble 4.
DISCUSSION
The most common technique for pelvic irradiation in the treatment of carcinoma of the cervix has been the two-fields anterior-posterior/posterior-anterior @P/PA) approach.
However, the four-field pelvic technique has gained wide acceptance and is presented as a standard technique in many radiotherapy textbooks (2, 10, 14). The theorical advantage of the four-field technique is the use of the lat- eral fields to spare the small bowel anteriorly and a part of the rectum posteriorly.
The guidelines for AP/PA pelvic portals has been well established, however. Greer (4) has added some guidelines to assure appropriate lymph node coverage.
Guidelines for the lateral pelvic fields are poorly de- fined. They are not specific and have considerable vari- ability. A review of the literature shows great variability especially with regard to the posterior border (2,4, 5, 10, 11, 14, 17).
The posterior border of the lateral field could be defined according to radiographic guidelines (middle of S2, inter- space S2S3) (4, 10, 17), and sometimes according to an- atomic guidelines (sparing to the mid rectum posteriorly) (11). Sometimes they are defined with the width at source to skin distance or at the isocenter (9 cm at 100 cm SSD for Fletcher, 8 cm for Perez), and often are illustrated with a radiograph (2, 14).
Moreover, the difference between radiographic guide- lines in the middle of S2 or interspace S2S3 is often un- clear according to the sacrum direction, and is small in most cases.
This four-field pelvic technique requires accurate lo- calization of the tumor volume and of its relationship to surrounding normal structures.
In our study, we have used MRI to help us to define more accurately the tumor of the cervix and its extensions.
In the first group, MRI-assisted simulation led us to adjustments in the radiation fields in 7 patients out of 11
(63%), 6 in lateral fields and 1 in anterior and lateral fields. The anterior border of the lateral field had to be increased to ensure an adequate margin around the uterine fundus in five patients: two of them presented adenocarcinoma and were aged less than 50 years.
It is not clearly established if the irradiation of the uter- ine fundus has a role in local control of squamous cell carcinoma of the cervix. Nevertheless, we usually include the entire uterus in the radiation fields.
We had to increase the posterior border of the lateral field to irradiate the tumor of the cervix with safety mar- gins in five cases. Our posterior border is defined at the middle of S2, even if we have chosen the interspace S2S3, we would have to increase the posterior border in three cases, and in six patients for which the posterior border at mi S2 was adequate, it would have resulted in an unnecessary irradiation of a more larger part of the rectum.
We can conclude that standard lateral portals do not exist and the design of lateral fields has to be based on individual tumor anatomy, which is given very accurately by MRI. Russel(17) and Mayr (12) demonstrated the use- fulness of MRI in the planning of radiation therapy (four- field technique) in patients with cervical cancer.
Mayr (12) used the following borders in the design of the lateral fields (anterior border included half of the pubis and posterior border included half of the rectum). He identified insufficient coverage of the tumor exten- sion in more than half of the patients (8 out of 15,53%). Russel (17) in his study found that conventional lateral portals (anterior border: apex of the pubis arch and pos- terior border: S2S3 interspace) would have resulted in a marginal miss in 6 patients (24%), a potential marginal miss in 8 patients (32%) and incomplete coverage of the uterine fundus in 15 of 24 patients (62.4%). With standard portals, adequate coverage of the tumor and its regional extension was obtained in 11 patients (44%).
In the second group, diagnostic MRI was available at the simulation step and led us to perform slight modi- fications related to the posterior border of the lateral field (change to the middle of S2 to interspace S2S3). Nevertheless, MRI in treatment position added new modifications in five of seven patients to ensure ade- quate irradiation. This means that MRI in treatment po- sition solely can assess the simulated fields, because it gives us a perfect correlation between the morbid anat- omy and the simulated fields. Diagnostic MRI helped us to design the irradiation fields, but was not entirely sufficient, because it did not fit the special needs of ra- diotherapy. The slight adjustments that were necessary were related to the fact that diagnostic MRI was per- formed on a curved plane surface (phase array coil). The images were not magnified and very small errors related to the delineation of the target volume on the diagnostic MR images were more important on the magnified im- ages obtained during MRI in treatment position. In a future study, we expect to avoid the expense of two

832 I. J. Radiation Oncology 0 Biology 0 Physics
MRIs with a diagnostic MRI in two parts, which will answer to specific needs of imaging and radiotherapy.
Computed tomography treatment planning is recom- mended by Kim (6) to prevent inadequate margins in the design of lateral fields in cancer of the cervix, and he has reported an increase of pelvic control in patients with CT treatment planning (7). Despite the higher availability of CT machines compared to MR units; in our study, we do not use CT reconstruction to design the irradiation fields, because the multiplanar capacities from MRI with direct imaging in different planes is superior to the CT-based reconstruction and the target volume is delineated more
Volume 37, Number 4, 1997
accurately with MRI than CT, because of superior contrast resolution (3, 8, 15).
CONCLUSION
Magnetic resonance imaging provides us with direct and accurate images of the tumors of the cervix with their extension a real knowledge of the morbid anatomy. The availability of this imaging technology allows an individ- ualized custom treatment taking into account the real spa- tial relationship between tumor and normal anatomy within each patient. The new possibilities offered by this new imaging technology are promising.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
Chomy, F.; Muyldermans, P.; Chemin, A.; Kind, M.; Tho- mas, L.; Le Treut, A.; Kantor, G. IRM et radiotherapie. Re- p&es externes, selection des plans et mesures de la distor- sion. Bull. Cancer/Radiother. 81:241-246; 1994. Fletcher, G. H.; Hamberger, A. D. Female pelvis: Squamous cell carcinoma of the uterine cervix. In: Fletcher, G. J., ed. Textbook of radiotherapy, 3rd ed. Philadelphia, PA: Lea and Febiger; 1980:720-773. Greco, A.; Mason, P.; Leung, A. W. L.; et al. Staging of carcinoma of the uterine cervix: MRI surgical correlation. Clin. Radiol. 40:401405; 1989. Greer, B. E.; Koh, W. J.; Figge, D. C.; Russel, A. H.; Cain, J. M.; Tamini, H. K. Gynecologic radiotherapy fields defined by intraoperative measurements. Gynecol. Oncol. 38:421- 424; 1990. Greer, B. E.; Koh, W. J.; Stelzer, K. J.; Goff, B. A.; Comsia, N.; Tran, A. Expanded pelvic radiotherapy fields for treat- ment of local-regionally advanced carcinoma of the cervix: Outcome and complications. Am. J. Obstet. Gynecol. 174:1141-l 150; 1996. Kim, R. Y.; McGinnis, L. S.; Spencer, S. A.; Meredith, R. F.; Jennelle, R. L. S.; Salter, M. M. Conventional four- field pelvic radiotherapy technique without CT treatment planning in cancer of the cervix: Potential geographic miss. Radiother. Oncol. 30: 140-145; 1994. Kim, R. Y.; McGinnis, L. S.; Spencer, S. A.; Meredith, R. F.; Richard, M. D.; Jennelle, R. L. S.; Salter, M. M. Con- ventional four field pelvic radiotherapy technique without computed tomography-treatment planning in cancer of the cervix: Potential geographic miss and its impact on pelvic control. Int. J. Radiat. Oncol. Biol. Phys. 31:109-112; 1995. Kim, S. H.; Chi, B. I.; Lee, H. P.; et al. Uterine cervical carcinoma: Comparison of CT and MR findings. Radiology 175:45-51; 1990. Landberg, T.; Wambersie, A.; Chavaudra, J.; Dobbs, J.; Hanks, G.; Johanssen, K. A.; Moller, T.; Purdy, J.; Aka-
10.
11.
12.
13.
14.
15.
16.
17.
18.
numa, A.; Gerard, J. P.; Horiot, J. C.; Suntharaling, A. M. Prescribing recording and reporting photon beam therapy. ICRUSO report. International Commission on Radiation Units and Measurements. Bethesda, MO: ICRU publications; 1994. Le Bourgeois, J. P.; Chavaudra, J.; Eschwege, F. Cancers gynecologiques. In: Radiotherapie oncologique. Paris: Her- mann Editeurs des Sciences et des Arts; 1992:253-267. Mar&l, V. A. The cervix. In: Moss, W. T.; Cox, J. D., eds. Radiation oncology: Rationale, technique, results, 6th ed. St Louis, MO: C. V. Mosby Co.; 1989:512-558. Mayr, N. A.; Tali, E. T.; Yuh, W. T. C.; Brown, B. P.; Wen, B. C.; Buller, R. E.; Anderson, B.; Hussey, D. H. Cervical cancer: Application of MR Imaging in radiation therapy. Ra- diology 189:601-608; 1993. Muyldermans, P.; Chemin, A.; Chomy, F.; Richaud, P.; Le Treut, A.; Kantor, G. MRI and radiotherapy planning: Geo- metrical verifications. 13th Annual ESTRO Meeting. Ra- diother. Oncol. 32(Suppl. l):S147; 1994. Perez, C. A. Carcinoma of the uterine cervix. In: Brady, L. W.; Perez, C. A., eds. Principles and practice of radiation oncology. Philadelphia: Lippincott Co; 1992: 1143-1202. Rubens, D.; Thornbury, J. R.; Angel, C.; et al. Stage IB cervical carcinoma: Comparison of clinical, MR, and path- ologic staging. AJR 150:135-138; 1988. Russel, A. H. Contempory radiation treatment planning for patients with cancer of the uterine cervix. Semin. Oncol. 21:30-41; 1994. Russell, A. H.; Walter, J. P.; Anderson, M. W.; Zukowski, C. L. Sagittal magnetic resonance imaging in the design of lateral radiation treatment portals for patients with locally advanced squamous cancer of the cervix. Int. J. Radiat. On- col. Biol. Phys. 23449455; 1992. Thomas, L.; Chacon, B.; Kind, M.; Lasbareilles, 0.; Muyl- dermans, P.; Pigneux, J.; Le Treut, A.; Kantor, G. MRI in the treatment planning of radiation therapy in cervical car- cinomas. ECCO 8, Paris, 29 Octobre-2 Novembre 1995. Eur. J. Cancer 31A (suppl5):S43, 191; 1995.







![Unusual Metastasis from Carcinoma Cervix · Carcinoma cervix is the most prevalent malignancy in Indian women with incidence of about 19–44 per 100,000 women [3]. The standard treatment](https://img.pdfslide.us/doc/110x75/5f704683f3e5dc1d486aa6c3/unusual-metastasis-from-carcinoma-cervix-carcinoma-cervix-is-the-most-prevalent.jpg)