Embed Size (px)
Citation preview

Magnetic Resonance Imaging in Subacute Necrotizing Encephalomyelopathi (Leigh‘s Disease) Thomas K. Koch, MD,”t Melvin H. C. Yee, MD,” Harrol T. Hutchinson, MD,*t and Bruce 0. Berg, MDYt
Magnetic resonance imaging (MRI) offers a sensitive alternative to computed tomography (CT) for lesion localization. Patients with subacute necrotizing en- cephalomyelopathy (SNE) may be diagnosed by tinding focal lesions on CT that correspond to sites of anatomi- cal involvement. We report serial CT and MRI scanning findings in a patient with clinical, radiographic, and laboratory evidence of SNE. MRI was more sensitive in detecting lesions involving the basal ganglia, brain- stem, and cortex. We believe MRI is a valuable and sen- sitive means to establish an antemortem diagnosis of SNE.
Koch TK, Yee MHC, Hutchinson HT, Berg BO: Magnetic resonance imaging (MRI) in subacute
necrotizing encephalomyelopathy (Leigh’s disease). Ann Neurol 19605-607, 1986
Subacute necrotizing encephalomyelopathy (SNE; Leigh’s disease) is a rare autosomal recessive neuro- degenerative disorder primarily affecting infants and children [4]. Clinical presentation may vary but psy- chomotor retardation, feeding and respiratory diffi- culties, cranial nerve palsies, nystagmus, and disorders of muscle tone, movement, and blindness are all com- mon 151. Although a disorder of brain pyruvic acid metabolism has been proposed 12, 51, no specific biochemical marker has been identified. A definitive antemortem diagnosis is often difficult to establish. Computed tomography (CT) may demonstrate bilat- eral symmetrical radiolucencies involving the basal ganglia, thalamus, brainstem, and cerebellum {7 ] . Al- though these CT findings may establish the antemor- tem diagnosis, we have recently reported radiographic variability on serial patient scanning 131.
Magnetic resonance imaging (MRI) offers a sensitive alternative to CT scanning. It has proved to be of great
From the Departments of ‘Neurology and tPediauics, University of California, San Francisco, San Francisco, CA 94143. Received July 31, 1985, and in revised form Oct 16. Accepted for publication Oct 28, 1985. Address reprint requests to Dr Koch, Child Neurology, M-650, University of California, San Francisco, CA 94143.
value in the identification of degenerative disorders of children 181. We report enhanced detection of lesions involving the basal ganglia, brainstem, and cortex in a patient with clinical, laboratory, and radiographic findings consistent with SNE.
Case Report A boy, 11 years, 7 months of age, had been born at full term. He weighed 6 Ib, 9 oz at birth, and the pregnancy, labor, and delivery had been uncomplicated. Early developmental mile- stones were normal.
He first came to medical attention at 4 years of age with poor visual acuity and optic atrophy. A CT brain scan was normal. At 5 years of age, he was noted to be slightly clumsy but without any other neurological findings. At 7 years of age, he developed a prolonged episode of unexplained vomiting. Physical examination at 8 years disclosed poor fine motor movements, brisk reflexes, and optic atrophy. A sec- ond CT scan was normal. At 10 years of age he began having generalized seizures. An electroencephalogram was n o d but &nation revealed a mild spastic diparesis and optic atrophy. He began taking phenobarbital, with good seizure control.
The patient’s condition continued to worsen, and by 10% years, he was unable to use his right arm and required assis- tance to walk. Examination then revealed dystonic posturing on the right, spastic diparesis, truncal ataxia, hyperreflexia, and bilateral plantar extensor responses. A CT scan showed symmetrical bilateral radiolucent lesions involving the puta- men; there was also a lucency in the left caudate nucleus. Soon after, he lost the ability to walk. His speech became slurred and he began having difficulty controlling his se- cretions. He developed palatal myoclonus, yawning, and hic- cuping. At 10 years, 11 months of age, he was admitted to the hospital for gastrostomy because of inability to handle secretions. On neurological examination, he was awake and responsive, but his mentation was impaired. Speech was labored and slow with a pseudobulbar quality. Both optic disks were pale. Microsaccadic eye movements were present with tracking. There was facial diparesis. Muscle bulk was diminished throughout. There was severe spastic quadri- paresis. The patient was unable to sit or stand without assis- tance. There was no evidence of cerebellar or sensory dys- function. Deep tendon reflexes were brisk with bilateral ankle clonus. Plantar responses were extensor bilaterally.
Laboratory studies revealed a mildly depressed serum bi- carbonate level (20 mEq/L; normal, 24 to 32) and a mildly elevated serum lactate level (25 mg/dl; normal, 5 to 18). The remainder of the serum, urine, and cerebrospinal fluid stud- ies were normal.
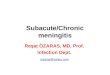
Prior to discharge, the patient became aphemic. He was unable to recognize his parents. Both CT and axial MRI scans of the brain were performed (Figs 1, 2). CT scanning (Fig 1) revealed similar findings to those observed 5 months previously. Both TI- and Tz-weighted spin-echo techniques were used for MRI. The T2-weighted images demonstrated numerous bilateral focal high-intensity abnormalities of the gray matter, most prominent in the putamen, caudate nu- cleus, and midbrain, and scattered throughout the cerebral cortex (Fig 2). Involvement of the brainstem and right cau-
6 0 5

Fig 1. Unenhanced computed tomographic scan at 10 years, I I months of age. Symmetrical lucency of the putamen bilaterally (large arrows) and lucency of the ldt caudzte nucleus (small arrow) are evident.
date nucleus as well as many of the cortical lesions was not seen on CT.
The patient remained vegetative for approximately 6 months and then slowly his condition began to improve. When re-evaluated at 11 years, 7 months of age, he was awake and alert. Although unable to speak, he could answer “yes” and “no” by using a buzzer. There were impaired up- gaze and mild nystagmus on lateral gaze. Occasional palatal myoclonus and yawning were noted. Motor examination re- vealed a severe spastic quadriparesis with minimal volitional movement. Reflexes were hyperactive, with right ankle clonus and brisk bilateral plantar extensor responses.
Repeat CT scanning revealed ventriculomegaly, cortical atrophy, and gray matter lucencies involving the putamen bilaterally as well as some superficial cortical areas (Fig 3). The distribution of the lesions changed slightly from those noted 8 months earlier. The previous lesion in the left cau- date nucleus had disappeared and the number of superficial cortical lucencies (not seen in Fig 3) had decreased. Similarly, MRI scans disclosed a change in the pattern of involvement of the basal ganglia, but in contrast to CT, numerous superficial cortical lesions were seen (Fig 4).
Discussion In the absence of a specific biochemical marker, SNE may be diagnosed definitively only at autopsy. Patho-
Fig 2. Axial T2-weighted spin-echo magnetic resonance imaging Jcan at 10 years, 11 months of age. High-intensity signah in- volving the putamen (large arrows) and caudate nucleus (small arrows) bilaterally are shown.
logically, SNE resembles Wernicke’s encephalopathy with symmetrical foci of variable necrosis, vascular proliferation, and spongiform loosening of the neu- ropil. The major pathological difference in SNE is sparing of the mamillary bodies. The disclosure by CT of radiolucent lesions involving the basal ganglia, brainstem, and cerebellum has been useful in establish- ing the antemortem diagnosis [7), although these typi- cal findings are dynamic and may vary considerably with time [3]. We have recently postulated that this variability may be due to the detection of active lesions with vascular proliferation, which do not necessarily all progress to gross necrosis and cavitation 131.
MR1 is a sensitive technique to detect changes in brain water content and it provides excellent lesion delineation [ 1, b}. In cerebral infarction, MRI is some- times superior to x-ray CT [l]. It is therefore likely that active foci of disease in SNE may easily be de- tected by MRI.
Our patient had a progressive encephalomyelopathy characterized by cognitive, extrapyramidal, pyramidid, and brainstem involvement. Laboratory studies re- vealed a mild lactic acidosis and CT scanning demon- strated radiolucent lesions involving the basal ganglia
606 Annals of Neurology Vol 19 No 6 June 1986

Fig 3. Unenhanced computed tomographic scan at 1 1 years, 7 months of age. Cortical atrophy, enlarged ventricles, and lucency of the putamen bilaterally are present (arrows). The previous lucency of the lejit caudate nucleus is not apparent.
and superficial cortex. Serial scanning disclosed vari- ability in the radiographic involvement. MRI in this patient demonstrated all the lesions seen by CT, in- cluding the disappearance of the lesion involving the left caudate nucleus. MRI additionally revealed lesions involving the brainstem and right caudate nucleus, and extensive involvement of the cortex. The increased sensitivity of MRI may allow earlier detection of char- acteristic basal ganglia and brainstem involvement and provide a valuable means for establishing the antemor- tem diagnosis of SNE.
R.eferences 1. Buonanno FS, De Win LD, Pyken IL, et al: Proton ('H)NMR
imaging in stroke syndromes. Neurol Clin 11243-262, 1983 2. DeVivo DC, Haymond MW, Obert KA, et al: Defective activa-
Fig 4. Axial T2-weighted spin-echo mgnetic resonance imaging scan. High-intensity signals involving the putamen bilaterally (large arrows) and scattered cortical lesions (small arrows) are shown. The previous lucency of the left caudate nucleus is not present.
tion of the pyruvate dehydrogenase complex in subacute nec- rotizing encephalomyelopathy (Leigh disease). Ann Neurol
Koch TK, Lo WD, Berg BO: Variability of serial CT scans in subacute necrotizing encephalomyelopathy (Leigh disease). Pediatr Neurol 1:48-51, 1985 Leigh D: Subacute necrotizing encephalomyelopathy in an infant. J Neurol Neurosurg Psychiatry 14:216-221, 1951 Pincus JH: Subacute necrotizing encephalomyelopathy (Leigh's disease): a consideration of clinical features and etiology. Dev Med Child Neurol 1487-101, 1972 Schmidley JW, Brito A, Chan PH, et al: Using nuclear magnetic resonance imaging to study changes in brain water. Neurology 33(suppl 2):151, 1983 Schwartz WJ, Hutchison HT, Berg BO: Computerized tomog- raphy in subacute necrotizing encephalornyelopathy (Leigh dis- ease). Ann Neurol 10:268-271, 1981 Young RSK, Osbakken MD, Alger PM, et al: Magnetic reso- nance imaging in Ieukodystrophies of childhood. Pediatr Neurol 1:15-19, 1985
6483-494, 1979
Brief Communication: Koch et d. Magnetic Resonance Imaging in Leigh's Disease 607