Embed Size (px)
Citation preview

F62 Archives of Disease in Childhood 1995; 72: F62-F70
CURRENT TOPICS
Magnetic resonance imaging in perinatal asphyxia
Ernst Martin, A James Barkovich
Department ofPaediatrics, DivisionofMagnetic Resonance& DevelopmentalBrain Research,University of Zurich,SwitzerlandE Martin
Department ofRadiology, Division ofDiagnosticNeuroradiology,University ofCalifornia, SanFrancisco, USAA J Barkovich
Correspondence to:Dr Ernst Martin, UniversityChildren's HospitalMagnetic Resonance Unit,Steinwiesstrasse 75, CH-8032 Zurich, Switzerland.
IntroductionThe purpose of this review article is: (i) torecall the impact of perinatal asphyxia and itsconsequences on child development; (ii) toestablish the diagnostic benefit of magneticresonance imaging (MRI) and to compareit with other imaging modalities; (iii) tosummarise the range of imaging patternsviewed on different brain scans and to discusstheir aetiology; (iv) to describe the evolution ofcharacteristic MRI findings observed duringthe early postnatal period and during laterchildhood; and (v) to estimate the role ofMRI in predicting later neurodevelopmentaloutcome.
Acute perinatal asphyxia refers to acondition of hypoxaemia, hypercapnia andinsufficient blood perfusion of the newbornduring labour and birth. It is considered to bethe 'single most important perinatal cause ofneurological morbidity'.' Perinatal asphyxiaand its consequences have an incidence of2-9%o, in term neonates,2 which is verymuch higher in premature babies, causingnot only neurological impairment, but alsobehavioural problems and intellectualdeficits.3 Depressed fetal heart rate, meco-nium stained amniotic fluid, low Apgarscores, low scalp and cord pH, or clinicalsigns of neurological depression soon afterbirth signify the acute clinical condition ofthe newborn. The predictive value of the clin-ical features for later neurodevelopmentaloutcome is, however, rather disappointing.Affected neonates present with a characteris-tic, although non-specific, syndrome calledhypoxic-ischaemic encephalopathy (HIE).They may be initially hyperalert, or oftenlethargic, with diminished muscle tone andspontaneous movements. They demonstratepoor suck, apnoea, and other signs of brain-stem dysfunction, or in severe cases, they arecomatose, with seizures beginning withinhours of birth. The death rate in term infantswith HIE is around 11%, and as many as 60%of affected premature newborns die.Moreover, 20-30% of survivors suffer frommental retardation, cerebral palsy, andseizure disorders in later childhood.3
Despite major advances in obstetric andneonatal care, the prevalence of cerebral palsyhas not decreased over the past decade.4 About10-15% of children who later develop cerebral
palsy have intrapartum insults with symptomsof HIE during the first week of life. In anappreciable number of children with cerebralpalsy in utero hypoxia-ischaemia must there-fore have preceded the perinatal period,which caused neither maternal symptoms norrelevant HIE in the newborn.56 Sarnat hasdeveloped a grading system for HIE, based onneurological evaluation in the newborn period,which helps to differentiate babies withfavourable outcome from those with a poorprognosis for developing neurological seque-lae.7 Although it has been of great prognosticvalue for infants with mild HIE and thosewith severe encephalopathy, the prognosis ofmoderately affected infants is less certain.Moreover, many babies with HIE requireintensive care and artificial ventilation duringthe first days of life, and are not accessible toclinical evaluation.
Importance ofMRI compared with othertechniquesIn an attempt to improve diagnostic valueand prognostic power, recent efforts have beendirected towards investigatory techniquessuch as real-time ultrasound scans, Dopplerultrasound scans, computed tomographyscans, and magnetic resonance spectroscopy.
Ultrasound scanning is an easily applicablebedside tool and has been used extensively as ascreening method in preterm infants.8 9Although the signs ofHIE are often short-livedand end stage periventricular leucomalacia isinadequately assessed, ultrasound scanningstill has some predictive value, particularlywhen periventricular-intraventricular haemor-rhage is present.'1012 However, it has lowsensitivity in term babies with HIE, andcorrelation with spastic diplegia is not goodunless cystic lesions are detected, whichseverely limits its prognostic value.13-15 In sev-eral studies the assessment ofblood flow veloc-ity in the anterior cerebral artery using Dopplerultrasound scanning has shown ahigh positive predictive value, but longterm follow up has not been done.16 17 Someauthors believe that characteristic postis-chaemic cerebral lesions can be delineated oncomputed tomography only beyond the age of6 months, although the maximum extent ofacute cerebral oedema and necrosis has been
on June 20, 2020 by guest. Protected by copyright.
http://fn.bmj.com
/A
rch Dis C
hild Fetal N
eonatal Ed: first published as 10.1136/fn.72.1.F
62 on 1 January 1995. Dow
nloaded from

Magnetic resonance imaging in perinatal asphyxia F63
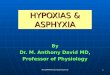
Figure I MRI scanof acute anid chronicpeniventricular zvhite nmatterinuty. Ti (A) and T2(B) weighted images of anasphyxiated 28 weeks'gestational age infantpetformed during thesecond week of life showhyperintensity andhypointensity, respectively(arrows), in theperiventricular whitematter. First echo (C) andsecond echo (D) from astudy performied at age 19mionths shows dininlishedperivenitriculattr zwhite miatterwith irregutlarly enilargedventricles anid abiionoralhvIperintrensits (arrowzus). -~~~~~~~~i
Fig IA F8ig IB
Fig JC Fig ID
demonstrated between two and four days ofthe insult, and generalised decreased tissuedensity (particularly thalamic hypodensity) inearly postnatal computed tomography clearlypredicted an unfavourable outcome in terminfants. 17-19
Because of higher sensitivity and specificityto maturational changes, such as visualisationof myelination and changes in cerebralstructures, MRI has had an enormous impacton neurological imaging.20 21 Although expen-sive and sometimes difficult to perform inacutely ill newborns, MRI overcomes many ofthe shortcomings of ultrasound scanning andcomputed tomography.22 23 It has a highersensitivity and has been extremely valuable inassessing the extent ofhypoxic-ischaemic braindamage during the early postnatal period andlater infancy.22 2426 It also is more specific,clearly differentiating fluid filled cavities,
oedema, gliosis and haemorrhage. 7 Moreover,it can provide better anatomical resolution,particularly in the basal ganglia, thalamus, andin the periphery of the cerebral cortex. MRImight be the only method to diagnose hypoxicbrain injuries in mild to moderately affectedpatients, and to detect discrete lesions ofthe cerebellum and the brain stem. Thelarge normal variability in the progress ofmyelin deposition20 21 25 sometimes makes theinterpretation of delayed myelination by earlyneonatal MRI difficult, especially on inversion-recovery images.24 However, delayed myelina-tion, as a likely consequence of neuronaldestruction, is a predictor of later longtermneurodevelopmental outcome, and thus is ofconsiderable importance.
Retrospective studies on children with cere-bral palsy, in which the magnetic resonanceexamination was carried out when the brainshowed an adult pattern of myelination - forexample, beyond 2 years of age - demonstrateabnormalities of the brain in over 900/o.21 29 30In children born prematurely a strong correla-tion was found between:(i) reduction in the amount of white matterin the centrum semiovale and in the periven-tricular area;(ii) periventricular prolongation of T2 relax-ation; and(iii) ventricular dilatation and the severity ofmotor disability. Although a close relationbetween HIE, periventricular leucomalacia,and delayed myelination in MRI with thedegree of motor impairment in prematureinfants could be demonstrated, the correlationwith cognitive outcome seems somewhatweaker.31-33 Lesions in basal ganglia andthalamus correlate strongly with athetoticcerebral palsy, most probably caused byasphyxia. Cerebral palsy in children born atterm seems to have its origin in acute perinatal
on June 20, 2020 by guest. Protected by copyright.
http://fn.bmj.com
/A
rch Dis C
hild Fetal N
eonatal Ed: first published as 10.1136/fn.72.1.F
62 on 1 January 1995. Dow
nloaded from

F64 Martin, Barkovich
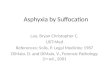
Figure 2 MRI scanofacute and chronicboundary zone injury interm (41 week) infant. (A)and (B) At age 4 days, T2weighted images showabnormal highsignal in the cortex at thevascular boundary zones(arrows). (C) and (D) Atage 3 months, the cortex isthin, the subcortical whitematter too bright, and thesubarachnoid spacesenlarged in the vascularboundary zones.
;~~~~~~~~~~~~~~~~~~~~~~~~~~~~M .:..2A.
:~~~~~~~~:1
Fig< 213
.4.
Fig 2C Fig 21)
Figure 3 MRI scan ofchronic deep grey matterand perirolandic injury.(A) T2 weighted imageat the level of the basalganglia shows highsignal (arrows) in theventrolateral thalami andposterior putamina.(B) T2 weighted imageat the high cerebral levelshows high signal (arrows)in the perirolandic region. I , ) I
_I_'/, . _,I
on June 20, 2020 by guest. Protected by copyright.
http://fn.bmj.com
/A
rch Dis C
hild Fetal N
eonatal Ed: first published as 10.1136/fn.72.1.F
62 on 1 January 1995. Dow
nloaded from

Magnetic resonance imaging in perinatal asphyxia F65
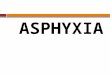
Figure 4 MRI scan ofacute deep grey matterand perirolandic injury interm infant, age 5 days.(A) Abnormal highsignal is seen in the globipallidi, putamina, andventrolateral thalami andthe normal high signal ofthe posterior limb of theinternal capsule is not seenon this Tl weighted image.(B) T2 weighted imageshows abnormnal highsignal in the lateral thalamibut is otherwise nearly nor-mal. (C) TransverseTl weighted image at theupper cerebral level showsabnormal high signal(arrows) in the deepportions of the pre-andpostcentral gyri.
Fig 4A
Fig 4AFig 4B
Fig 4C
asphyxia in only 15 to 25%. Moreover, theMRI scan shows a more heterogeneous pat-tern, ranging from cortical dysplasia to focalinfarcts and atrophy, or basal ganglia lesions,depending on the timing of the asphyctic eventduring gestation.
Hypoxic-ischaemic brain lesionsAs neurons are particularly vulnerable to oxygenand glucose deficiency, cerebral lesions areeither a direct consequence of hypoxia-ischaemia or gradually develop during recovery,when excitatory amino acids, mainly glutamate,and calcium ions have an important destructiverole.34 35 Several distinct neuropathological pat-terns of ischaemic brain injury have beenobserved, depending on the gestational age ofthe child and the severity of the insult:(i) selective neuronal necrosis of the cortex,
predominantly the hippocampus, and also ofdeep grey matter nuclei;(ii) leucomalacia of periventricular and sub-cortical white matter; and(iii) focal or more generalised infarction.There is a dynamic evolution of any hypoxic-ischaemic injury, and the MRI pattern devel-ops gradually until the final stage is achieved.The clinician urgently needs early informationabout the severity of HIE because importantdecisions on continuation of intensive caremeasures and potential therapeutic inter-ventions are being considered at that time.Therefore, the issue of optimal timing for MRIbecomes crucial.
Patterns of injury and their aetiologyThe pattern of injury that results from HIE inthe neonate, as determined by MRI, seemsto depend primarily on two factors: (i) thegestational age - the maturity of the brain, atthe time of the injury; and (ii) the duration andseverity of the hypoxic-ischaemic insult.
PARTIAL ASPHYXIAWhen injury is caused primarily by mild ormoderate hypoxia or hypotension, injuryseems to occur in regions that have themost tenuous perfusion.24 The periventricularwhite matter is most severely affected in infantsof less than about 34 weeks' postconceptionalage (fig 1).24 3A0 By 40 weeks, the matureintervascular boundary zones (the mostperipheral zones of the areas perfused bythe anterior, middle, and posterior cerebralarteries) are affected. Included in thesezones are the periventricular white matter,subcortical white matter, and cerebral cortex inthe boundary regions (fig 2).24 3741 42 Thedeep grey matter structures of the cerebrumare typically spared in these patients.The patterns observed on MRI scans
suggest that the injury is caused by simple
on June 20, 2020 by guest. Protected by copyright.
http://fn.bmj.com
/A
rch Dis C
hild Fetal N
eonatal Ed: first published as 10.1136/fn.72.1.F
62 on 1 January 1995. Dow
nloaded from

F66 Martin, Barkovich
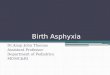
Figure 5 MRI scan ofsubacute or chronic deepgrey matter injury at age 8weeks. Tl (A) and T2(B) weighted images showloss ofperiventnicular braintissue. The basal nucleiare shrunken and showabnormal patchy highsignal on Tl weightedimage and abnormalpatchy low signal on T2weighted image (arrows).
S~~~~~~~~~~~~~~~~~: "
s.1EFij|~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. _ 1 1 .! ,^~~~~~~~~~~~~~~~~~~~ ipI~~~~~~~~~~~~~~~~~~~~~~~~~~~~B....:i-__l~~~~~~~~~~
,I u, i -I-I.'_
--.-W
:'L------W
!Fo - '''rr
B.
-M-..
-S|--:- ----
,
It , *.\. ]]
hypoperfusion, perhaps as a result of impairedautoregulation. Some authors have suggestedthat the change in pattern of injury from ex-clusively periventricular (with cortical sparing)to largely cortical or subcortical is the result ofmaturation of the cerebral vasculature.36 39 40These postulated changes in the cerebral vascu-lar supply during the last trimester have beendisputed.4445 Others have suggested that theperiventricular injury in premature neonates isthe result of oligodendrocyte development inthe germinal zone during the first half of the lasttrimester, consequent increased metabolicdemands in the periventricular zone, and, per-haps, vulnerability of oligodendrocytes to theexcitatory amino acids produced byischaemia.4648 This controversy has a greaterimpact on the proposed mechanism of injurythan on the observation that the region of injuryvaries with brain maturity.
PROFOUND ASPHYXIAA different, more complex, pattern of injuryis produced when injury is the result of amore severe event, such as cardiocirculatoryarrest or profound hypotension. The MRIimaging findings in these patients correlatewell with reported pathological studies.22 49 50The pattern of injury in this group ofneonates varies with postconceptional age(brain maturity) of the affected child, as itdoes in infants who have partial asphyxia.However, the regions of brain affected arequite different. The volume of damaged brainalso seems to vary with the duration of theinjury in profoundly asphyxiated neonates.An arrest of long duration (25 minutes orgreater) damages nearly the entire brain; nouseful patterns can be detected by imaging.Arrests of shorter duration, however, showspecific patterns that vary with the state ofbrain maturity. Profound injuries to infantsof about 26 to 32 weeks' postconceptionalage result in injury primarily to the lateral
thalami. By 34 to 36 weeks, the lentiformnucleus and hippocampus are injured and,in some patients, the perirolandic cortex.By 40 weeks, the corticospinal tracts areaffected from the internal capsule to theperirolandic cortex (fig 3). More severe ormore prolonged events result in injury to theoptic radiations.The regions of brain injured in profound
asphyxia correlate temporally and topographi-cally with the progression of myelination andof metabolic activity within the brain at thetime of the injury. The ventral lateral thalamicnuclei and pallidothalamic fibres begin tomyelinate by about 25 weeks' gestational age.51The lentiform nuclei and the pre- and post-central gyri stain for myelin at 35 weeks andthe optic radiations at 37 weeks. The posteriorlimb of the internal capsule and the subcorticalwhite matter of the postcentral gyrus showevidence of myelination at 40 weeks.5' Itwould be expected that metabolic activitywould increase as myelination proceeds.Although no studies have described localisedcerebral metabolic activity in preterm infants,localised glucose metabolism has beenreported in term infants using positronemission tomography (PET) measurements of2-deoxy-2[18F]fluoro-D-glucose.52 In thisstudy term neonates showed highest metabolicactivity in the thalami, basal ganglia, and theprimary sensorimotor areas of the cerebralcortex (the pre- and postcentral gyri). Therelation between the location of myelinationand the location of brain injury in the asphyxi-ated neonate can be explained by anothermechanism. Axons in the immature nervoussystem can substantially regenerate afterinjury.53 However, some myelin componentsseem to inhibit axonal growth.54 It is thereforepossible that the brain is diffusely injured byprofound asphyctic events and that only those
on June 20, 2020 by guest. Protected by copyright.
http://fn.bmj.com
/A
rch Dis C
hild Fetal N
eonatal Ed: first published as 10.1136/fn.72.1.F
62 on 1 January 1995. Dow
nloaded from

Magnetic resonance imaging in perinatal asphyxia F67
Figure 6 MRI scan ofnormal newborn. (A) Tiweighted image through thelevel of the basal gangliashows that the high signal(arrows) of the posteriorlimb of the internal capsuleis the brightest on theimage. This high signalmerges imperceptibly withthe ventrolateral thalamicand posterior putaminalhigh signal. (B) T2weighted image at thelevel of the basal gangliashows low signal, indicatingmyelination, in theventrolateral thalami (largeopen arrows), dorsalputamina (large closedarrows), and posterior limbof the internal capsules(small arrows). (C) T2weighted image at the uppercerebral level shows morepronounced low signal inthe pre- and postcentralgyrti, indicating the presenceof myelination in thosestructures.
Fig 6A Fig 6B
Fig 6C
regions that are myelinated are unable toregenerate.
Evolution ofMRI observationsThere are few published reports about thechanges that occur in the MRI signal intensityof the cerebral parenchyma after hypoxic-ischaemic injury of the newborn infant.Reports of findings in term infants in allstages after asphyctic injury can be found,2225but reports of MRI findings in asphyxiatedpremature infants almost exclusively focuson subacute and chronic changes.24 55 56Therefore, this discussion will focus primarilyon the evolution of MRI findings in asphyxi-
ated term infants. MRI scans performed withinthe first two to three days after injury show lowsignal on Ti weighted images and high signalon T2 weighted images in the affected regions.In term infants with profound asphyxia signalchanges are seen in the lentiform nuclei andalong the corticospinal tracts; in term infantswith partial asphyxia the changes are secn inthe vascular boundary zones (fig 2). By four tofive days, Ti shortening becomes evident inthe affected regions (fig 4). This becomes quitepronounced by about seven days after theinjury. It remains present for a variable time,almost always for at least four weeks andsometimes for as much as eight or 10 weeksafter the injury (fig 5). T2 shortening (lowsignal on T2 weighted images) slowly developsduring the first month and lasts for two to threemonths (fig 5). Notably, the location of thelentiform nuclei signal abnormalities in infantswith profound neonatal asphyxia is subtlydifferent at the age of 2 to 3 months than in thefirst few weeks after the injury. They arelocated in the lateral thalami and posteriorputamina (fig 5). As the Ti and T2 shorteninggradually disappear, the injured areas of brainshow tissue loss with low signal intensity onTi weighted images and high signal on T2weighted images (fig 3).The MRI signal abnormalities associated
with asphyctic brain injury can be subtle anddifficult to detect in the first few days of life. Inpatients with profound asphyxia injury tends tooccur in those areas that are myelinating ormyelinated. Unfortunately, identification ofinjured regions ofbrain is hampered by the factthat the signal characteristics of myelin, withrespect to the unmyelinated brain, are similarto those of the damaged tissue. Two imagingfeatures are helpful in distinguishing the nor-mal from the damaged brain in these patients.The first is the appearance of the internalcapsule. In the normal newborn the posterior
on June 20, 2020 by guest. Protected by copyright.
http://fn.bmj.com
/A
rch Dis C
hild Fetal N
eonatal Ed: first published as 10.1136/fn.72.1.F
62 on 1 January 1995. Dow
nloaded from

F68 Martin, Barkovich
-~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~fY: W05 C::f
Figure 7 Chronic boundary zone injury. First echo (A) and second echo (B) T2 weightedimages show cortical thinning and high signal of the white matter in the vascular boundaryzones (white arrows) and ventricular enlargement (black arrows). Asymmetric injury isseen more commonly than symmetric injury.
limb of the internal capsule is bright on Tiweighted images; it cannot be distinguishedfrom the myelinated ventrolateral thalamicnucleus medially, or the myelinating posteriorputamen laterally (fig 6). In the asphyxiatednewborn the posterior limb of the internal cap-sule is hypointense relative to the high signal inthe thalamus and putamen (fig 4). Moreover,the globus pallidus is sometimes bright in theasphyxiated newborn. The second helpful fea-ture involves the differentiation of the normalshort Ti and T2 seen in the neonatal pre- andpostcentral gyri from the short Ti and T2 ofdamaged gyri. In the normal newborn thealtered signal (bright on Ti weighted imagesand dark on T2 weighted images) is seenalong the length of the gyrus. In the asphyxi-ated newborn, the altered signal is greaterin the deepest portion of the affected gyrus(fig 4), an area known to be more severelyaffected in asphyxia injury.57The MRI findings are also subtle in term
neonates with partial asphyxia. The majorfinding on MRI in these neonates is oedemawithin the affected cortex. Because oedema-tous cortex has a higher water content thannormal cortex, it has longer Ti and T2 relax-ation times (darker on Ti weighted imagesand brighter on T2 weighted images). Thedamaged cortex, therefore, becomes iso-intense with the subjacent unmyelinatedwhite matter. The appearance is one ofapparently discontinuous cortex (fig 2).Unless the entire cerebral cortex is scrutinisedfor these areas of discontinuity, the damagedregions may be missed.
Although it is accepted that the Ti and T2prolongation in acutely damaged tissue isthe result of oedema, the cause or causes of theTi and T2 shortening in the subacute phaseis not firmly established.22 Some attribute itto haemorrhage,23 but it would be unusualfor parenchymal haemorrhage to remainunchanged in size and signal intensity over aperiod of one to two months, as is seen on MRI
scans of asphyxiated newborns. Possible causesof short TI and T2 other than haemorrhageinclude the presence of lipids from myelinbreakdown, TI shortening secondary tomyelin clumping (status marmoratus), anddystrophic calcification. Lipid is an unlikelysource in view of the small amount of lipidpresent in the newborn brain and the lack ofchemical shift artefact (which should, theo-retically, be present when lipid protons aresituated next to water protons) on those MRIstudies that have been analysed. Myelinclumping, known to occur in the basal gangliaafter profound asphyxia,58 could cause accen-tuated TI shortening of water protons in theregion. Another possibility is that petechialhaemorrhage, present in the early phasesafter injury, slowly undergoes dystrophiccalcification as the blood products areresorbed. This process would explain the slightchange in the location of abnormal signalwithout substantial change in the signalcharacteristics. Future studies may help toelucidate better the cause of the signal changes.As the patient ages and the brain myelinates
damaged areas become more difficult toidentify by changes in signal intensity on TIweighted images. Instead, regions of focalatrophy must be detected. Damaged areas aredifficult to detect on T2 weighted imagesbefore adequate myelination has occurred. Inparticular, signal abnormalities are difficult todetect on T2 weighted images before the age of8 to 10 months.41 As myelination progressesand the brain becomes more hypointense onT2 weighted images, areas of damage becomemore conspicuous, appearing as regions of T2prolongation (figs 3 and 7). The damaged fociremain hyperintense on T2 weighted imagesfor decades afterward.22 24
Prognostic value of early MRISeveral prospective studies have tried to com-pare acute hypoxic-ischaemic cerebral lesionsevaluated with MRI shortly after birth withlater MRI patterns, stages of myelination,and neurodevelopmental outcome of thechild.23 25 26 59 Although there is much debateabout the usefulness of early MRI in aclinically unstable asphyxiated neonate, westrongly believe that MRI can provideexcellent morphological information aboutthe cerebral injury. This information allowsoutcome to be anticipated in most cases,based on location, extent, and severity of theprincipal ischaemic damage and the occur-rence of secondary lesions like oedema,haemorrhage, or thrombosis, even in the acuteneonatal period.56 59 In our experience a nor-mal MRI obtained in the first 24-72 hoursalways predicts a favourable outcome even in aseverely asphyxiated baby. On the other hand,extensive brain oedema with effacement of thecortical ribbon or lesions in the ventro-lateralthalamic nuclei and the dorsal striatum have apoor outcome, irrespective of birth variables,such as Apgar score or cord pH. In somepatients the prognostic value can be improvedby repeating the study after several weeks
on June 20, 2020 by guest. Protected by copyright.
http://fn.bmj.com
/A
rch Dis C
hild Fetal N
eonatal Ed: first published as 10.1136/fn.72.1.F
62 on 1 January 1995. Dow
nloaded from

Magnetic resonance imaging in perinatal asphyxia F69
to months, when delayed myelination andstructural damage can be appreciated moreeasily.6061 As myelin is produced by oligo-dendrocytes which are dependent on oxygenand nutrient supply, early detection of delayedmyelination is possible, and important forpredicting neurodevelopmental outcome, suchas cerebral palsy. Yet it has to be borne in mindthat MRI by itself remains a morphologicalmethod, and that either degenerative or ongo-ing destructive processes, or reparative brainplasticity, can only be estimated.
This work was supported by the Swiss National Foundation,grant No 32-37811.93.
1 Volpe JJ. Neurology of the newborn. 2nd edn. Philadelphia:WB Saunders, 1987.
2 Hill A. Current concepts of hypoxic-ischemic injury in theterm newborn. Pediatr Neurol 1991; 7: 317-25.
3 Volpe JJ. Intra-ventricular haemorrhage and brain injury inthe premature infant. Clin Perinatol 1989; 16: 361-86.
4 Pharoah POD, Cooke T, Rosenbloom I, Cooke RW.Trends in birth prevalence of cerebral palsy. Arch DisChild 1987; 62: 379-84.
5 Scher MS, Belfar H, Martin J, Painter MJ. Destructive brainlesions of presumed fetal onset: antepartum causes ofcerebral palsy. Pediatrics 1991; 88: 898-906.
6 Nelson KB, Ellenberg JH. Antecedents of cerebral palsy.Multivariate analysis of risk. N Engl J Med 1986; 315:81-6.
7 Sarnat HB, Sarnat MS. Neonatal encephalopathy followingfetal distress. Arch Neurol 1976; 33: 696-704.
8 Costello AM de L, Hamilton PA, Baudin J, Townsend J,Bradford BC, Stewart AL, Reynolds EOR. Prediction ofneurodevelopmental impairment at four years from brainultrasound appearance of very preterm infants. Dev MedChild Neurol 1988; 30: 711-22.
9 Fawer CL, Diebold P, Calame A. Periventricular leukoma-lacia and neurodevelopmental outcome in preterminfants. Arch Dis Child 1987; 62: 30-6.
10 Levene MI. Cerebral ultrasound and neurological impair-ment: telling the future. Arch Dis Child 1990; 65: 469-7 1.
11 De Vries IS, Eken P, Pierrat V, Daniels H, Casaer P.Prediction of neurodevelopmental outcome in thepreterm infant: short latency cortical somatosensoryevoked potentials compared with cranial ultrasound. ArchDis Child 1992; 67: 1177-81.
12 Van de Bor M, Ensdokkum M, Schreuder AM, Veen S,Brand R, Verloovevanhorick SP. Outcome of periventric-ular-intraventricular haemorrhage at five years of age. DevMed Child Neurol 1993; 35: 33-41.
13 Siegel M, Shackelford G, Perlman J, Fulling K. Hypoxic-ischaemic encephalopathy in term infants: diagnosis andprognosis evaluated by ultrasound. Radiology 1984; 152:395-9.
14 De Vries LS, Dubowitz LMS, Dubowitz V, Kaiser A,Lary S, Silverman M, et al. Predictive value of cranialultrasound: a reappraisal. Lancet 1985; ii: 137-40.
15 De Vries LS, Pierrat V, Eken P, Minami T, Daniels H,Casaer P. Prognostic value of somatosensory evokedpotentials for adverse outcome in full-term infants withbirth asphyxia. Brain Dev 1991; 13: 320-5.
16 Levene MI, Fenton AC, Evans DH, Archer LNJ, ShortlandDB, Gibson A. Severe birth asphyxia and abnormal cere-bral blood-flow velocity. Dev Med Child Neurol 1989; 31:427-34.
17 Gray PH, Tudehope DI, Masel JP, Burns YR, Mohay HA,O'Callaghan J, et al. Perinatal hypoxic-ischaemic braininjury: prediction of outcome. Dev Med Child Neurol1993; 35: 965-73.
18 Lipp-Zwahlen AE, Deonna T, Micheli JL Calame A.Prognostic value of neonatal CT in asphyxiated termbabies: Low density score compared with neonatal neuro-logical signs. Neuropediatrics 1985; 16: 209-17.
19 Flodmark 0, Roland EH, Hill A, Whitfiled MF.Periventricular leukomalacia: Radiologic diagnosis.Radiology 1987; 162: 119-24.
20 Barkovich AJ, Kjos BO, Jackson DE, Norman D. Normalmaturation of the neonatal and infant brain: MR imagingat 1-5 TI. Radiology 1988; 166: 173-80.
21 Martin E, Boesch C, Zuerrer M, Kikinis R, Molinari L,Kaelin P, et al. MR imaging of brain maturation in normaland developmentally handicapped children. Jf ComputAssist Tomogr 1990; 14: 685-92.
22 Barkovich AJ. MR and CT evaluation of profound neonataland infantile asphyxia. Am J Neuroradiol 1992; 13:959-72.
23 Keeney 5, Adcock EW, McArdle CB. Prospective observa-tions of 100 high-risk neonates by high field (1-5 Tesla)
magnetic resonance imaging of the central nervous sys-tem: II. Lesions associated with hypoxic-ischemicencephalopathy. Pediatrics 1991; 87: 431-8.
24 Barkovich AJ, Truwit CL. Brain damage from perinatalasphyxia: correlation ofMRI findings with gestational age.AmJ Neuroradiol 1990; 11: 1087-96.
25 Stinlin M, Dirr R, Martin E, Boesch C, Largo RH, FanconiS, Boltshauser E. MRI following severe perinatalasphyxia: preliminary experience. Pediatr Neurol 1991; 7:164-70.
26 Byrne P, Welch R, Johnson MA, Darrah J, Piper M. Serialmagnetic resonance imaging in neonatal hypoxic-ischemicencephalopathy. J Pediatr 1990; 117: 694-700.
27 Schouman-Claeys E, Henry-Feugeas MC, Roset F,Larroche JC, Rassine D, Sadik JC, et al. Periventricularleukomalacia: Correlation between MR imaging andautopsy findings during the first 2 months of life.Radiology 1993; 189: 59-64.
28 Brody BA, Kinney HC, Kloman AS, Gilles FH.Myelination in human infancy, 1. An autopsy studyof myelination. J Neuropathol Exp Neurol 1987; 46:283-301.
29 Truwit CL, Barkovich AJ, Koch TK, Ferriero DM.Cerebral palsy; MR findings in 40 patients. Am JNeuroradiol 1992; 13: 67-78.
30 Yokochi K, Aiba K, Horie M, Inukai K, Fujimoto S,Kodama M, et al. Magnetic resonance imaging in childrenwith spastic diplegia: Correlation with the severity of theirmotor and mental abnormality. Dev Med Child Neurol1991; 33: 18-25.
31 DeVries LS, Connell JA, Dubowitz LMS, Cozeer RC,Dubowitz V. Neurological, electrophysiological and MRIabnormalities in infants with extensive cystic leukomala-cia. Neuropediatrics 1987; 18: 61-6.
32 Konishi Y, Kuiryama M, Hayakawa K, Konishi K,Yasujima M, Fujii H, et al. Periventricular hyperintensitydetected by MRI in infancy. Pediatr Neurol 1990; 6:229-32.
33 Feldman HM, Scher MS, Kemp SS. Neurodevelopmentaloutcome of children with evidence of periventricularleukomalacia on late MRI. Pediatr Neurol 1990; 6:296-302.
34 Clark GD. Role of excitatory amino acids in brain injurycaused by hypoxia-ischemia. Clin Perinatol 1989; 16:459-74.
35 Volpe JJ. Current concepts of brain injury in the prematureinfant. Am 7Radiol 1989; 153: 243-5 1.
36 Banker BQ, Larroche JC. Periventricular leukomalacia ofinfancy: a form of neonatal anoxic encephalopathy. ArchNeurol 1962; 7: 386-410.
37 Koeda T, Suganuma I, Kohno Y, Takamatsu T, TakeshitaK. MR imaging of spastic diplegia: comparative studybetween preterm and term infants. Neuroradiology 1990;32: 187-90.
38 Wigglesworth JS, Pape KE. An integrated model for hemor-rhage and ischemic lesions in the newborn brain. EarlyHum Dev 1978; 2: 179-89.
39 deReuck J. The human periventricular arterial blood supplyand the anatomy of cerebral infractions. Eur Neurol 1971;5: 321-34.
40 Volpe JJ, Herscovitch P, Perlman JM, Raichle ME. Positronemission tomography in the newborn: extensive impair-ment of regional blood flow with intraventricular hemor-rhage and hemorrhagic intracerebral involvement.Pediatrics 1983; 72: 589-95.
41 Volpe JJ, Herscovitch P, Perlman JM, Kreusser KL, RaichleME. Positron emission tomography ;-n the asphyxiatedterm newborn: parasagittal impairment of cerebral bloodflow. Ann Neurol 1985; 17: 287-96.
42 Takashima S, Tanaka K. Development of the cerebrovascu-lar architecture and its relationship to periventricularleukomalacia. Arch Neurol 1978; 35: 11-16c.
43 Rorke LB. Anatomical features of the developing brainimplicated in pathogenesis of hypoxic-ischemic injury.Brain Pathol 1992; 2: 211-21.
44 Kuban KCK, Gilles FH. Human telencephalic angiogene-sis. Ann Neurol 1985; 17: 539-48.
45 Nelson MD Jr, Gonzalez-Gomez I, Gilles FH. The searchfor human telencephalic ventriculofugal arteries. Am JNeuroradiol 1991; 12: 215-22.
46 Volpe JJ. Brain injury in the premature infant - Currentconcepts of pathogenesis and prevention. Biol Neonate1992; 62: 231-42.
47 Oka A, Belliveau MJ, Rosenberg PA, Volpe JI. Vulnerabilityof oligodendroglia to glutamate: pharmacology, mecha-nisms, and prevention. J Neurosci 1993; 13: 1441-53.
48 Rivkin MJ, Volpe JJ. Hypoxic-ischemic brain injury in thenewborn. Semin Neurol 1993; 13: 30-9.
49 Hayashi M, Satoh J, Sakamoto K, Morimatsu Y. Clinicaland neuropathological findings in severe athetoid cerebralpalsy: a comparative study of globo-luysian and thalamo-putaminal groups. Brain Dev 1991; 13: 47-51.
50 Schneider H, Ballowitz L, Schachinger H, Hanefeld F,Droszus JU. Anoxic encephalopathy with predominantinvolvement of basal banglia, brain stem, and spinal cordin the perinatal period. Acta Neuropathol 1975; 32:287-98.
51 Hasegawa M, Houdou 5, Mito T, Takashimna 5, Asanuma
on June 20, 2020 by guest. Protected by copyright.
http://fn.bmj.com
/A
rch Dis C
hild Fetal N
eonatal Ed: first published as 10.1136/fn.72.1.F
62 on 1 January 1995. Dow
nloaded from

F70 Martin, Barkovich
K, Ohno T. Development of myelination in the humanfetal and infant cerebrum: a myelin basic proteinimmunohistochemical study. Brain Dev 1992; 14: 1-6.
52 Chugani HT, Phelps ME, Mazziotta JC. Positron emissiontomography study of human brain functional develop-ment. Ann Neurol 1987; 22: 487-97.
53 Saunders NR, Balkwill P, Knott G, et al. Growth of axonsthrough a lesion in the intact CNS of fetal rat maintainedin long-term culture. Proc Roy Soc Lond 1992; 250:171-80.
54 Caroni P, Schwab ME. Two membrane protein fractionsfrom rat central myelin. Biology 1988; 106: 1281-8.
55 McArdle CB, Richardson CJ, Hayden CK, et al.Abnormalities of the neonatal brain: MR imaging, part II.Hypoxic-ischemic brain injury. Radiology 1987; 163:395-403.
56 Baenziger 0, Martin E, Steinlin M, et al. Early pattern
recognition in severe perinatal asphyxia: a prospectiveMRI study. Neuroradiology 1993; 35: 437-42.
57 Takashima S, Tanaka K. Subcortical leukomalacia, relation-ship to development of the cerebral sulcus, and its vascularsupply. Arch Neurol 1978; 35: 470-6.
58 Friede RL. Developmental neuropathology. 2nd edn. Berlin:Springer-Verlag, 1989.
59 Kuenzle CH, Baenziger 0, Martin E, Thun-Hohenstein L,Steinlin M, Wood M, et al. Prognostic value of early MRimaging in term infants with severe perinatal asphyxia.Necropediatrics 1994; 25: 191-200.
60 Fujii Y, Konishi Y, Kuriyama M, Maeda M, Saito M, IshiiY, et al. MRI assessment of myelination patterns inhigh-risk infants. Pediatr Neurol 1993; 9: 194-7.
61 Van de Bor M, Guit GL, Schreuder AM, Wondergem J,Vielvoye GJ. Early detection of delayed meylination inpreterm infants. Pediatrics 1989; 84: 407-11.
on June 20, 2020 by guest. Protected by copyright.
http://fn.bmj.com
/A
rch Dis C
hild Fetal N
eonatal Ed: first published as 10.1136/fn.72.1.F
62 on 1 January 1995. Dow
nloaded from