Embed Size (px)
Citation preview

MAGNETIC RESONANCE ANGIOGRAPHY OF THE BRAIN ```````
Robbie Boon, RN, B.S.N., O.C.N., R.N.-B.C.
Indiana Wesleyan University

PLAGIARISM STATEMENT
I have read and understand the plagiarism policy as outlined in the syllabus and the sections in the IWU Catalog relating to the IWU Honesty/Cheating policy. By affixing this statement to this PowerPoint, I certify that I have not cheated or plagiarized in the process of completing this assignment. I also certify that the work submitted is original work specific for this course and to my program. If it is found that cheating and/ or plagiarism did take place in the writing of this paper, I understand the possible consequences of the act/s, which could include expulsion from Indiana Wesleyan University.

MAGNETIC RESONANCE ANGIOGRAPHY (MRA)
The American College of Radiology (ACR) describes MRA as using “MR pulse sequences” to determine blood flow and it may be completed by 2 dimensional (2D) of 3D technique. It also relies on time of flight (TOF) for flow images and quantitative measurements for flow velocity by phase-contrast (PC) (ACR- ASNR-SNIS-SPR practice guideline, Cervicocerbral MRA, 2010).
These methods are used with and with out the contrast medium. The contrast medium that is used is gadolinium and must be administered rapidly with a power injector. “The challenge is the roughly 10 second circulation time
within the brain”
(ACR- ASNR-SNIS-SPR practice guideline,
Cervicocerbral MRA, 2010, p. 5).
MRA image of aneurysm retrieved from http://www.plosone.org/article/fetchObject.action?uri=info:doi/10.1371/journal.pone.0054678.g003&representation=PNG_M

PATIENT SELECTION
• Patient must be able to remain still or be sedated (Pediatrics) and this must be warranted.
• Patient must be able to hold breath and follow directions to decrease distortion or overlapping structure signal.
• Contrast is needed- for proper visualization of the vasculature it is optimal which requires adequate kidney function or nephrogenic systemic fibrosis (NSF) may occur (ACR- ASNR-SNIS-SPR practice guideline, Cervicocerbral MRA, 2010).
• MRA in children is the first-line Cervicocerbral vascular examination for invasive angiographic procedure due to low risk (ACR- ASNR-SNIS-SPR practice guideline, Cervicocerbral MRA, 2010).
http://files.abstractsonline.com/CTRL/e4/c/f3b/6d1/bd8/43a/3a4/526/c11/a90/02b/db/g5784_1.pngDigital image retrieved from:

INDICATIONSPediatrics
• Arterial dissection or occlusive disease
• Dural sinus thrombosis / intracranial venous occlusive disease
• Intracranial aneurysm
• Vascular abnormalities (Sickle cell, Vasculitis and etc.)
• Blood supply to vascular neoplasm preoperatively
• Intracranial and spinal hemorrhage.
• Traumatic injury to the cervicocerebral vessels
• Congenital and acquired vascular abnormalities
• Evaluation of cerebrovasculature
-(ACR- ASNR-SNIS-SPR practice guideline, Cervicocerbral MRA, 2010).
Adults• Atherosclerotic occlusive disease and
thromboembolism
• Intracranial hemorrhage and spinal hemorrhage
• Evaluation of therapeutic measures, endovascular treatment of aneurysm and arteriovenous malformation (AVM) ablation.
• Aneurysms and vascular malformations
• Vascular supply to tumors
• Dural sinus thrombosis and intracranial venous occlusive disease.
• Congenital and acquired vascular abnormalities
• Evaluation of cerebrovasculature
-(ACR- ASNR-SNIS-SPR practice guideline, Cervicocerbral MRA, 2010).

HEADACHE
Fig 1.—"Intracranial vessels forming the circle of Willis. The circle of Willis represents the primary collateral pathway. Communication between the anterior circulation (territory supplied by the internal carotid arteries) and the posterior circulation(supplied by the basilar artery) is effective when the posterior communicating artery is patent" (Bugnicourt et al, Fig 1. p. 880, 2009).
Bugnicourt et al. (2009) found that migraineurs have Issues with perfusion related to morphologic abnormalities increasing hypoperfusion. The study did not explain every issue for migraineurs.
The next few images are called MRA-COW or MRA of the Circle of Willis. I will show some vascular abnormalities.

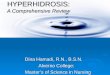
Fig 3.—"Magnetic resonance angiograms illustrating the classification of the morphology of the circle of Willis (CW): (a) complete CW: presence of both posterior communicating arteries; (b) incomplete CW: presence of only one (left) posterior communicating artery; (c) incomplete CW: absence of both posterior communicating arteries; (d) both fetal-type posterior cerebral arteries:posterior communicating arteries supplied only by the internal carotid artery – in this case, the CW is graded incomplete."(Bugnicourt et al, Fig 3. p. 882, 2009)
In these diagrams you can see how hypoperfusionCan occur with these CW inconsistencies. The past Studies of ischemia and migraine are well correlatedAnd the diagnostic evidence is reveals more “Incomplete CW posteriorly in 37 patients (29.8%) or6.5; 95% CI 2.6-16.2; P<.001” this occurrence was more Frequent in migraineurs with aura but did not accountFor all incomplete CW anomalies, the study results didnot result in levels of significance (Bugnicourt et al.,2009)

.plosone.org/article/info:doi/10.1371/journal.pone.0054678
Renfrew (2011) mentions the use of MRA specifically to various headachesIncluding cluster headache(HA) stating the preference for this HA is related the need to exclude aneurysm, meningioma and pituitary tumor with and without contrast.
The vascular malformations that make up the Bugnicourt et al. 2009 scenarios are only visible by MRA. HA may be caused by a subdural hematoma, tumor, vascular and avascular scenarios which require further evaluation by MRA.
Picture retrieved from

Differential Diagnosis in Scenario
Lucy is a 40 year old Caucasian female presents with HA and cranial nerve (CN) palsy stating that she has a history of migraines. Lucy states “I do not have the pain so much, but I do not feel right.” Lucy admits to N/V and states “that is better now.” The CN III with some transient nerve palsy on exam. Ptosis and difficulty with facial movement and expression being CN VII involvement. Temperature is 97.8 ℉, pulse of 68, respirations of 18, and B/P at 150/78. No nuchal rigidity is noted, but slight visual
Deciding to evaluate the situation and the residual effects: A MRI/ MRA is ordered when deciding she is a candidate for evaluation.My differentials are:
• Vascular Headache; Migraine headache & Cluster primary headache• Increased intracranial pressure; non-traumatic subarachnoid hemorrhage,
tumor, abscess, hydrocephalus, cerebral edema• Decreased intracranial pressure; cerebrospinal leak• Meningeal inflammation; meningitis, leukemia, SAH or subdural
hemorrhage• CVA, vascular malformation (Ferri, 2014).
The MRA showed no vascular malformations, but some morphologic abnormalities at CW indicating migraine.

SUBARACHNOID HEMORRHAGE (SAH)/ CEREBRAL ANEURYSM
MRA image of aneurysm retrieved from http://www.plosone.org/article/fetchObject.action?uri=info:doi/10.1371/journal.pone.0054678.g003&representation=PNG_M
MRA following a transient ischemic attach is very important. It may be a simple HA in presentation that can be detected and enhanced by ultrasound to reveal stenosis, ulceration, dissection, hematoma, and aneurysms (Renfrew, 2011).
Rajajee et al, (2008) revealed by clinical study 39% of patients with large vessel arthroboembolism, cardioembolism, small vessel stroke, or undetermined etiology stroke or more than one etiology (TOAST criteria)MRA did not reveal lesions. When time matters for stroke MRA may not be the best option.

ANEURYSMSaleem & Loch Macdonald (2013) present the cased of aneurysm rupture after HA, cranial nerve palsies, and seizures. The aneurysm was only visible by examination of the MRA. It was a posterior communication artery aneurysm that manifests from meningitis.
Digital image retrieved from Huang T-C, Chang C-K, Liao C-H, Ho Y-J (2013) Quantification of Blood Flow in Internal Cerebral Artery by Optical Flow Method on Digital Subtraction Angiography in Comparison with Time-Of-Flight Magnetic Resonance Angiography. PLoS ONE 8(1): e54678. doi:10.1371/journal.pone.0054678

SENSITIVITY AND SPECIFICITYPositive Predictive Values
• MRA sensitivity in aneurysms was reported as having a specificity of 85 to 93% in detecting aneurysms smaller than 3mm and sensitivity of 93 to 97% in detecting aneurysms > 3mm (Kapsalaki, Rountas, & Fountas, 2012).
• Kapsalaki et al. (2012) reports the systematic review by White et al, 2000; MRA has an accuracy of 90% and sensitivity of 87%, a specificity of 95% per aneurysm.
• The positive predictive value is 97% reported by White in Kapsalaki et al, 2012.
Negative Predictive Values
• The negative predictive value is 77% reported by White in Kapsalaki et al, 2012 per aneurysm.
http://files.abstractsonline.com/CTRL/e4/c/f3b/6d1/bd8/43a/3a4/526/c11/a90/02b/db/g5784_1.png

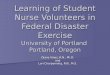
Figure 2. Results of a two-way sensitivity analysis comparing sensitivity of CT to specificity of LP. CT = computed tomography; CTA = CT angiography; LP = lumbar puncture; MRA = magnetic resonance angiogram.
Chart retrieved from Ward, M., Bonomo, J., Adeoye, O., Raja, A., & Pines, J. (2012). Figure 2, p. 1141

COST EFFECTIVENESS
Ward, Bonomo, Adeoye, Raja, & Pines (2012) revealed several key features on a study of cost analysis and quality adjusted life years (QALYs) to a study on evaluation of subarachnoid hemorrhage.
• The study revealed that computer tomography (CT alone) costs according to the 2009 Medicare diagnosis related groups about $10,300 and effectiveness of 20.25 QALYs.
• CT and lumbar puncture (LP) costs approximately $15,120 and effective for 20.36 QALYs.
• CT/MRA costs $16,200 with 20.27 QALYS.• CT/CTA costs $ 12,840 with 20.24 QALYS.
http://files.abstractsonline.com/CTRL/e4/c/f3b/6d1/bd8/43a/3a4/526/c11/a90/02b/db/g5784_1.png

REFERENCESACR-ASNR-SNIS-SPR practice guideline for the performance of pediatric and adult cervicocerebral magnetic
resonance angiography (MRA).(2010). Cervicocerbral MRA. Retrieved from
http://www.acr.org/~/media/ACR/Documents/PGTS/guideslines/Cervicocerbral_MRA.pdf
Bunicort, J., Garcia, P., Peltier, J., Bonnaire, B., Picard, C., & Godefroy, O. (2009). Incomplete posterior Circle
of Willis: A risk factor for Migraine?. Headache: The Journal of Head and Face Pain, 49(6), 879-886.
Ferri, F. F. (2014). Ferri’s Clinical Advisor: 5 Books in 1. Philadelphia, PA: Mosby Elsevier.
Kapsalaki, E., Rountas, C., & Fountas, K.N. (2012). The role of 3 Tesla MRA in the detection of intracranial
aneurysms. International Journal of Vascular Medicine. Article ID 792834, 9 pages, Retrieved from
http://dx.doi.org/10.1155/2012/792834

REFERENCES
Rajajee, V., Kidwell, C., Starkman, S., Ovbiagele, B., Alger, J., Villablanca, P., & Saver, J. (2008). Diagnosis of
lacunar infarcts within 6 hours of onset by clinical CT criteria versus MRI. Journal of Neuroimaging:
Official Journal of The American Society of Neuroimaging, 18(1),66-72. doi:10.1111/j.1552- 6569.2007.00150.x
Renfrew, D. L. (2011). Symptom based radiology. Sturgeon Bay, WI: Symptom Based Radiology Publishing.
Saleem, M., & Loch Macdonald, R. R. (2013). Cerebral aneurysm presenting with aseptic meningitis: A case report.
Journal of Medical Case Reports, 7(1), 2-11. doi: 10.1186/1752-1947-7-244
Ward, M. Bonomo, J., Adeoye, O., Raja, A., & Pines, J. (2012). Cost-effectiveness of diagnostic strategies for
evaluation of suspected subarachnoid hemorrhage in the emergency department. Academic Emergency
Medicine: Official Journal Of The Society For Academic Emergency Medicine, 19(10) ,1134- 1144.
doi:10.1111/j.1553-2712.2012.01455.x