Embed Size (px)
Citation preview
MACRA in New York: CMS’s New Quality Payment
Program
National Council for Behavioral Health
Montefiore Medical Center
Northwell Health
New York State Office of Mental Health
Netsmart Technologies

Elizabeth Arend, MPH
Quality Improvement
Advisor
Nina Marshall, MSW
Senior Director, Policy
and Practice
Improvement

Change Package
Primary Drivers Secondary Drivers
Patient and Family Centered Care Design
1.1 Patient and family engagement 1.2 Team-based relationships1.3 Population management1.4 Practice as a community partner1.5 Coordinated care delivery 1.6 Organized, evidence-based care1.7 Enhanced access
Data-driven ContinuousQuality Improvement
2.1 Engaged and committed leadership2.2 QI strategy supporting a culture of quality and safety 2.3 Transparent measuring and monitoring 2.4 Optimal use of HIT
Sustainable Business Operations
3.1 Strategic use of practice revenue3.2 Staff vitality and joy in work 3.3 Capability to analyze and document value 3.4 Efficiency of operation

Outline• MACRA final rule overview
• Eligibility
• Payment Adjustments & Timeline
• Merit-based Incentive Payment System (MIPS) • Quality
• Advancing Care Information
• Cost
• Improvement Activities
• Individual vs. Group Reporting
• How to Prepare
• Q&A
Review: What is MACRA? Medicare Access and CHIP Reauthorization Act (MACRA) of 2015
• Repeals the Sustainable Growth Rate formula
• Creates a new Quality Payment Program by streamlining existing programs
• Like DSRIP, MACRA shifts payment for volume of services to payment for value
Two Paths to Payment: MACRA’s New Quality Payment ProgramClinicians can choose either:
• The Merit-Based Incentive Payment System (MIPS), which streamlines multiple quality programs
• An Advanced Alternative Payment Model (APM), which provides bonus payments for participation
An Advanced APM:
1. Requires participants to use certified EHR technology
2. Provides payment for covered professional services based on CMS quality measures
3. Is a Medical Home Model expanded under CMS Innovation Center authority, OR
4. Requires participants to bear more than nominal financial risk
CMS will announce final list of Advanced APMs no later than January 1, 2017
Merit-based Incentive Payment System (MIPS)
• Combines and modifies three existing programs: oPhysician Quality Reporting System (PQRS)oElectronic Health Records Incentive Program (“Meaningful
Use”)oValue-based Payment Modifier (VM)
• Adds “Improvement Activities” category
In 2017, MIPS applies to:
Clinicians who bill Medicare Part B using the physician fee schedule, including:
• Physicians (including psychiatrists)
• Physician assistants
• Nurse practitioners
• Clinical nurse specialists
• Certified registered nurse anesthetists
MIPS participation is voluntary for other health care providers in 2017, but they will not receive a payment adjustment
In 2017, MIPS does NOT apply to:
• Providers billing Medicaid
• Clinicians who are newly enrolled in Medicare
• Clinicians who are significantly participating in an advanced APM
• Hospital-based and facility-based payment programs
• Clinicians and groups who are NOT paid under the Physician Fee Schedule (i.e. FQHCs and partial hospitalization programs)
In 2017, MIPS does NOT apply to:
• Individual clinicians and groups that fall beneath the “low volume threshold” who serve 100 or fewer Medicare recipients OR bill Medicare $30,000 or less per year• Low-volume threshold will be applied to individual clinicians if they decide to
report to MIPS as individuals
• Low-volume threshold will be applied to groups for clinicians who choose to report to MIPS as part of a group
• Clinician/group volume will be determined during the 2017 performance year
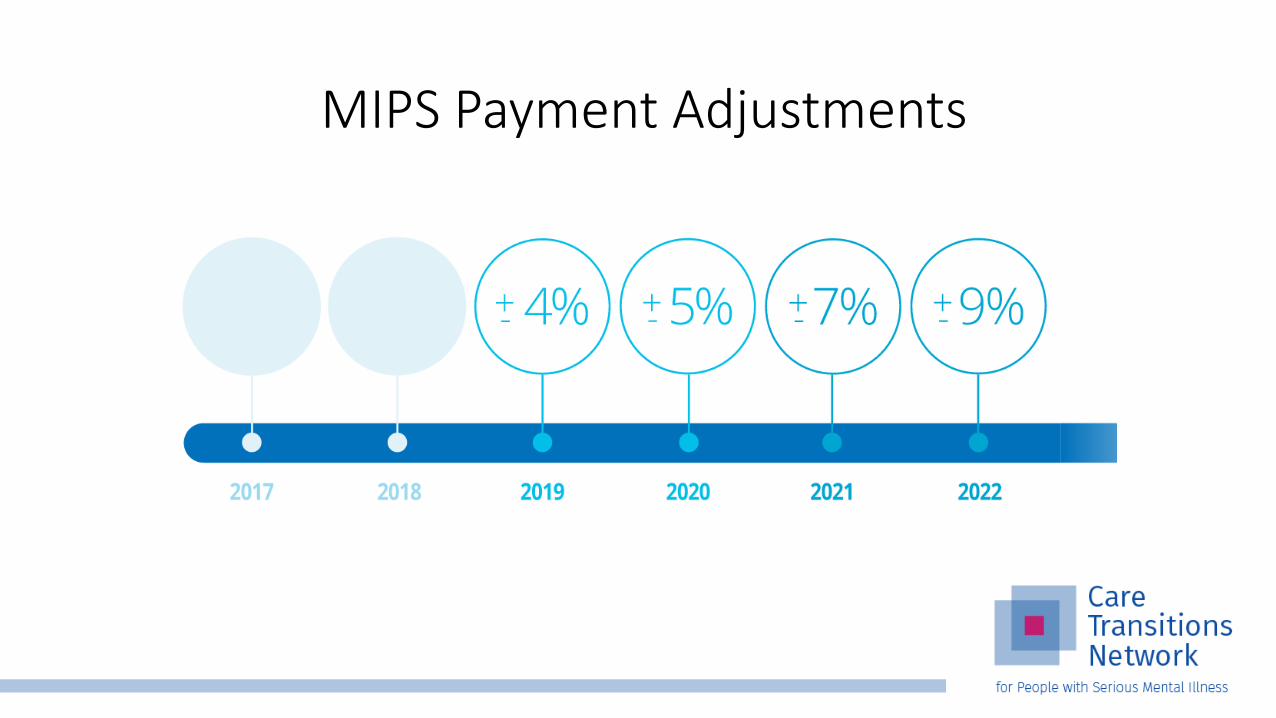
MIPS Payment Adjustments
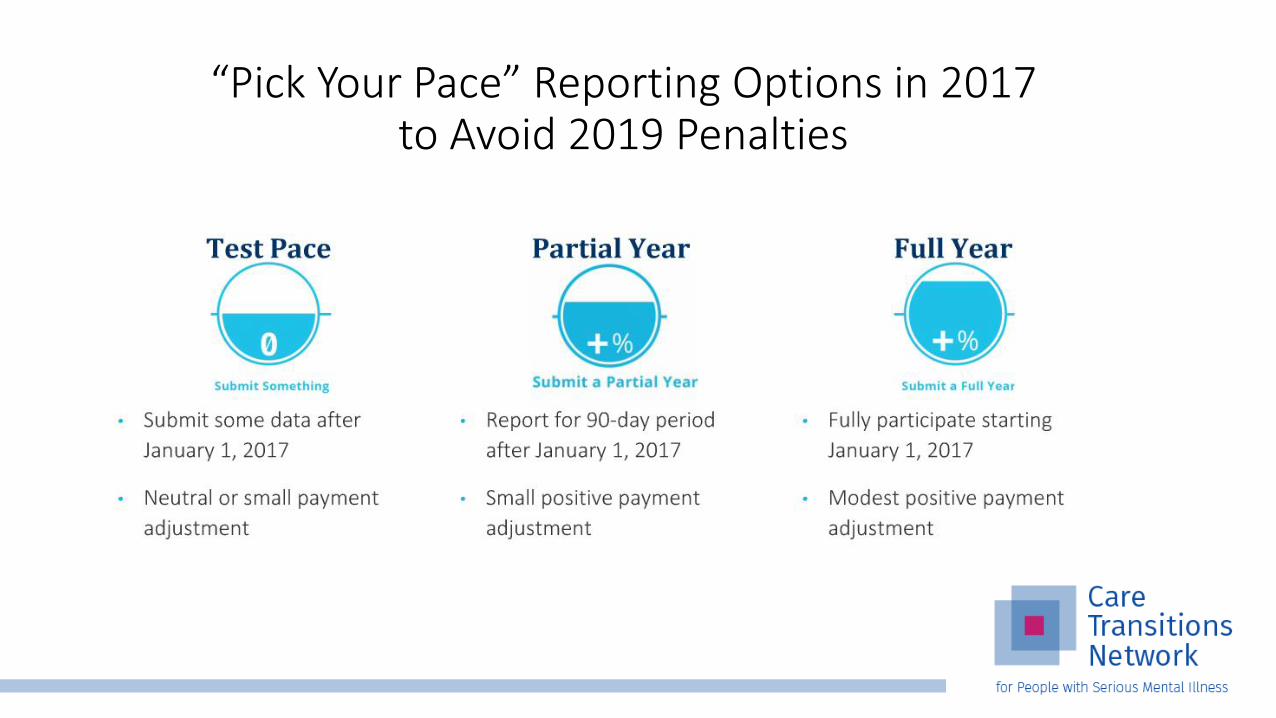
“Pick Your Pace” Reporting Options in 2017 to Avoid 2019 Penalties
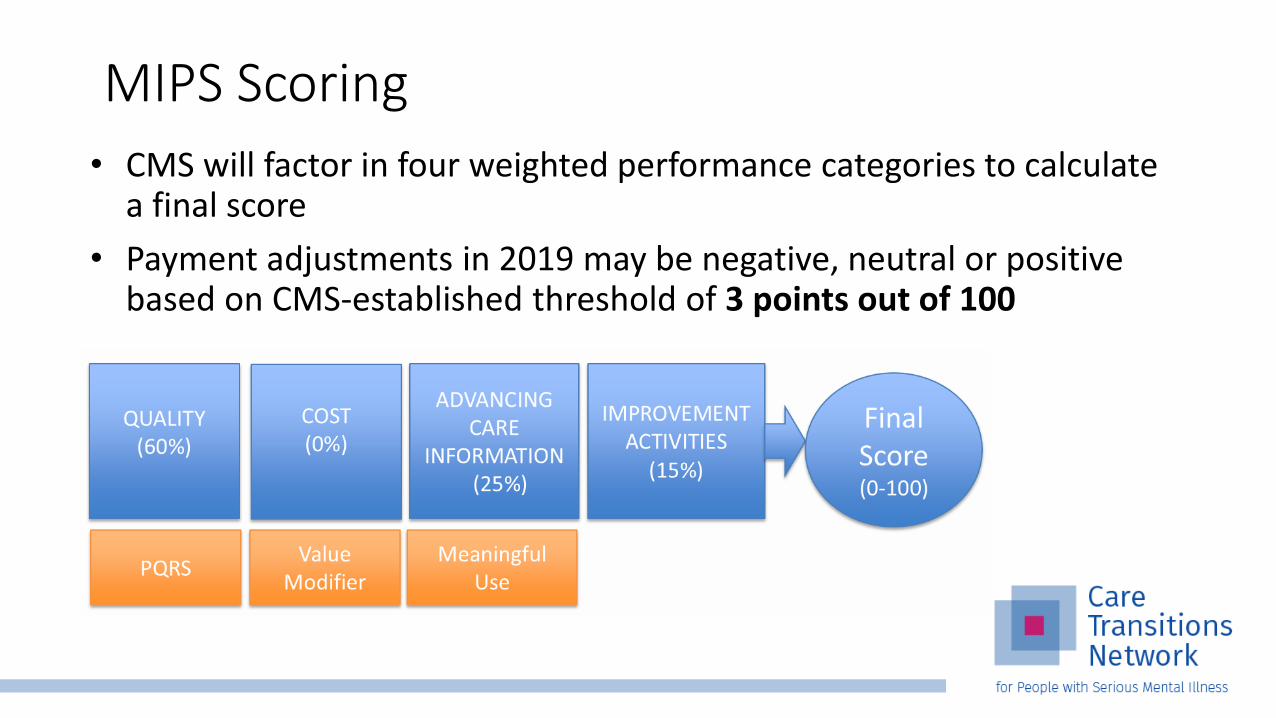
• CMS will factor in four weighted performance categories to calculate a final score
• Payment adjustments in 2019 may be negative, neutral or positive based on CMS-established threshold of 3 points out of 100
MIPS Scoring

• If you cannot report on ACI, weight will shift to Quality category Applications should be submitted annually (similar to EHR incentive program
“hardship exemption”)
• If you cannot report on quality measures, CMS will redistribute weight to other categories
• Clinicians need to report on at least two performance categories to get a positive payment adjustment in 2019
• A final score of 70+ will be eligible for the exceptional performance adjustment, funded from a pool of $500 million
Final Score Calculation

2017 MIPS Performance Categories
Quality (60%)• Requires providers to report six quality measures for a minimum of 90
consecutive days
• One measure must be an outcome measure. If an outcome measure is not available, report on one “high priority” measure: • Appropriate use
• Care coordination
• Patient experience
• Patient safety
• Clinicians may choose six of the 25 quality measures in the behavioral/mental health specialty measure set
What if there aren’t enough quality measures? • For the 2017 transition year, clinicians who submit one out of at least
six quality measures will meet the MIPS performance threshold of 3
• Clinicians who do not have enough measures to meet the reporting requirement should choose and report on all of the measures that apply to them
• Clinicians can choose to report on six of the 25 measures in the Behavioral/Mental Health Specialty Measure Set
• CMS will conduct a data validation process to determine if the clinician has reported all applicable measures

MIPS Quality Measures: Overlap with CTN and DSRIPMeasure Definition High
Priority?
Adherence to Antipsychotic Medications For Individuals with Schizophrenia
Percentage of individuals at least 18 years of age as of the beginning of the measurement period with schizophrenia or schizoaffective disorder who had at least two prescriptions filled for any antipsychotic medication and who had a Proportion of Days Covered (PDC) of at least 0.8 for antipsychotic medications during the measurement period (12 consecutive months)
Yes
Follow-Up After Hospitalization for Mental Illness (FUH)
1. The percentage of discharges for which the patient received follow-up within 30 days of discharge.2. The percentage of discharges for which the patient received follow-up within 7 days of discharge
Yes
Screening for Clinical Depression and Follow-Up Plan
Percentage of patients aged 12 years and older screened for depression on the date of the encounter using an age appropriate standardized depression screening tool AND if positive, a follow-up plan is documented on the date of the positive screen
No
Quality Benchmark Comparisons• Quality measure data will be compared to benchmarks in order to
determine your Quality score
• Not all quality measures will have a benchmark. If there is no benchmark for a measure, clinicians / groups will receive three points
• CMS will publish benchmarks prior to the start of each performance year
Future Quality Measures • CMS plans to increase the number of required outcome measures
through future rulemaking, as more outcome measures become available
• CMS also plans to increase reporting requirements for measures related to: • Appropriate use• Patient experience• Safety• Care coordination
• CMS will update/add quality measures annually based on clinician input
Quality Bonus Points
The final rule includes an option to earn bonus points in the quality category by:
• Reporting on patient experience through CAHPS (group practices only)
• Gathering and reporting quality measure data via the QCDR, qualified registry, CMS Web Interface, or CEHRT submission mechanisms.

Advancing Care Information (ACI) (25%) • Requires MIPS eligible clinicians to use
certified EHR technology (CEHRT)
• Emphasis on interoperability, information exchange and security
• Two measure sets in 2017 for reporting based on EHR edition:
1. ACI Objectives and Measures
2. ACI Transition Objectives and Measures (2017)

ACI Reporting Options
EHR Certified to 2015 Edition:
Option 1: ACI Objectives and
Measures
Option 2: Combination of the two
measure sets
EHR Certified to 2014 Edition:
Option 1: 2017 ACI Transition
Objectives and Measures
Option 2: Combination of the two
measure sets
ACI Scoring: 100 points
• Base score = 50% (no partial credit)
• Performance score = up to 90% if you report on all performance score measures
• Bonus Points: • 5% bonus for reporting to additional Public Health or Clinical Data Registry
Reporting measures
• 10% bonus for using CEHRT to complete certain Improvement Activities
Total Score = 100 points
ACI Base Score (50%)
Clinicians must submit a numerator/ denominator OR yes/no combination for each of the following measures:
Protect patient health information
Electronic prescribing
Patient electronic access
Health Information Exchange: Send summary of care
Health Information Exchange: Request/accept summary of care
ACI Performance Score (up to 90%)
• Based on a MIPS eligible clinician’s performance rate for each measure reported
• Nine measures= possibility to earn up to 90 percentage points • Patient Electronic Access
• Coordination of Care through Patient Engagement
• Health Information Exchange

Cost (0% in 2017)
Clinicians do NOT select cost measures• CMS will apply measures to clinicians and determine score based
on Medicare Part B claims analysis
• No independent reporting required
Cost score based on: • Total per capita cost for all attributed beneficiaries
• Medicare spending per beneficiary (MSPB)
• 10 episode of care measures (not yet finalized)
Cost Performance Scoring
• CMS will provide feedback based on 2017 performance, and will starting counting cost toward final score in 2018 performance year
• Cost performance category contribution to the final score will gradually increase from 0 to 30 percent by 2019 performance year / 2021 payment year
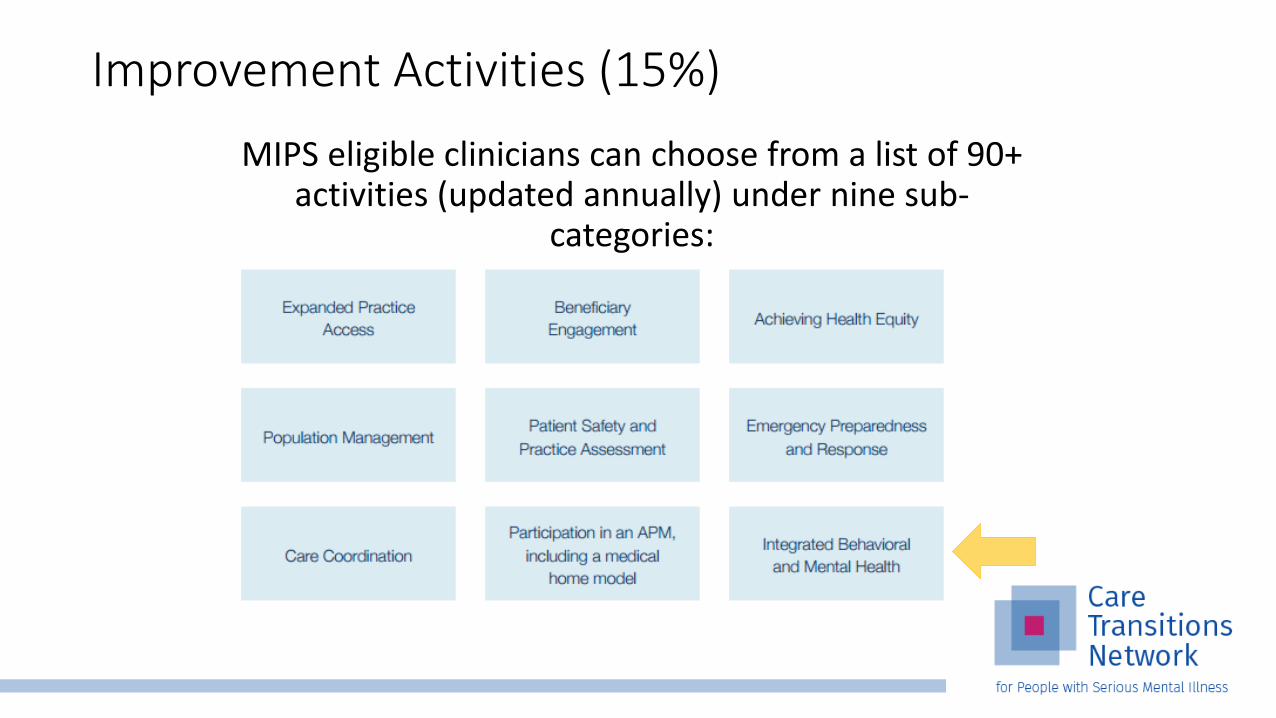
MIPS eligible clinicians can choose from a list of 90+ activities (updated annually) under nine sub-
categories:
Improvement Activities (15%)

Improvement Activities Scoring
• Must perform selected activities for at least 90 consecutive days
• Must attest each activity performed by selecting “yes” during reporting through: • Qualified registry
• EHR
• Qualified Clinical Data Registry
• CMS Web Interface (groups of 25+ only)
Improvement Activities Scoring (40 points) • Activity weight: Complete up to four activities for at least 90 days
o High = 20 points
o Medium = 10 points
• Activity weights for small/rural/HPSA practices: Complete up to two activities for at least 90 days
o High = 40 points
o Medium = 20 points
• Full credit for clinicians in a patient-centered medical home, Medical Home Model or similar specialty practice
• Zero score for non-participation
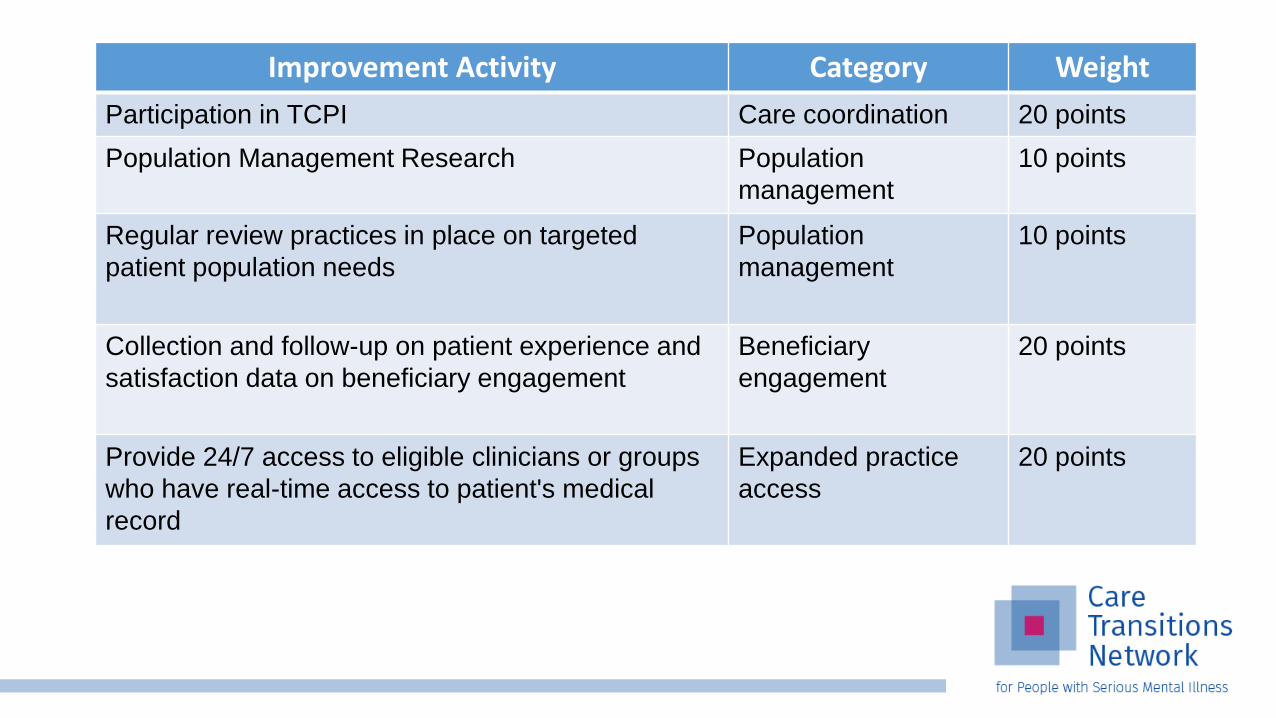
Improvement Activity Category Weight
Participation in TCPI Care coordination 20 points
Population Management Research Population
management
10 points
Regular review practices in place on targeted
patient population needs
Population
management
10 points
Collection and follow-up on patient experience and
satisfaction data on beneficiary engagement
Beneficiary
engagement
20 points
Provide 24/7 access to eligible clinicians or groups
who have real-time access to patient's medical
record
Expanded practice
access
20 points
MIPS Individual vs. Group Reporting
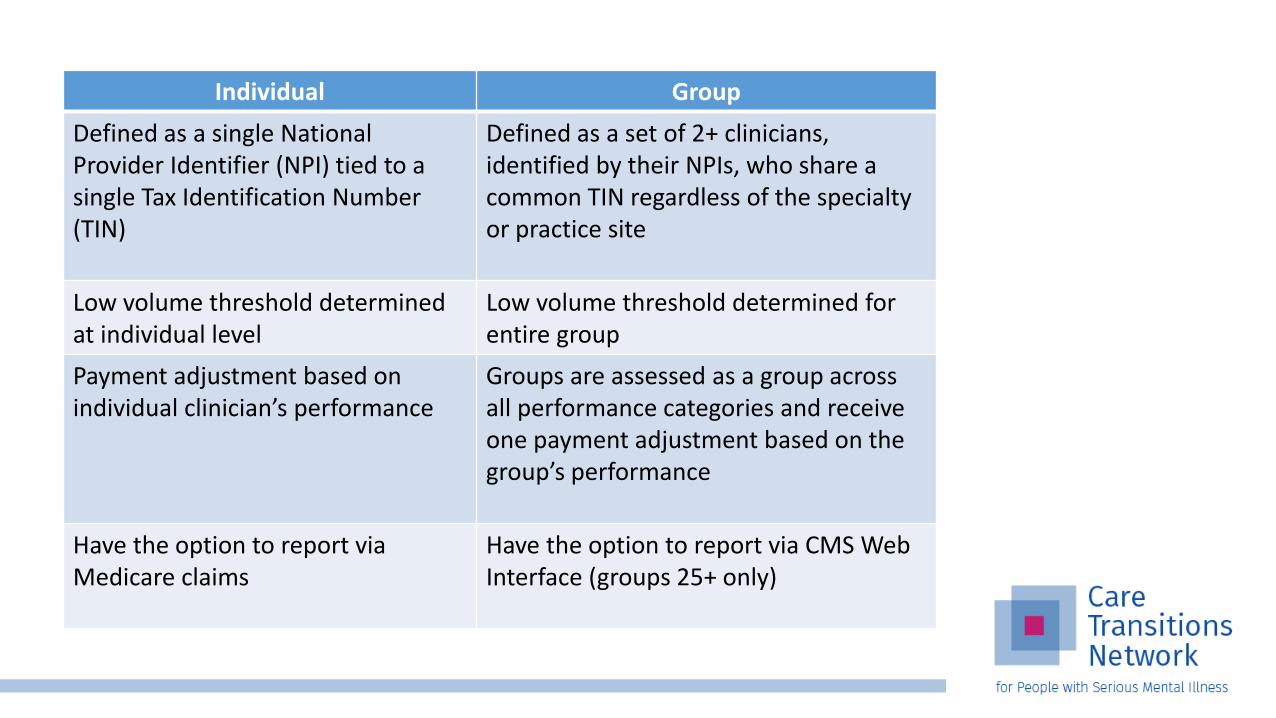
Individual Group
Defined as a single National Provider Identifier (NPI) tied to a single Tax Identification Number (TIN)
Defined as a set of 2+ clinicians, identified by their NPIs, who share a common TIN regardless of the specialty or practice site
Low volume threshold determined at individual level
Low volume threshold determined for entire group
Payment adjustment based on individual clinician’s performance
Groups are assessed as a group across all performance categories and receive one payment adjustment based on the group’s performance
Have the option to report via Medicare claims
Have the option to report via CMS Web Interface (groups 25+ only)
How to Prepare

How to Prepare Determine QPP eligibility
Educate your team
Review CMS PQRS performance feedback / QRUR
Review applicable quality measures and improvement activities
Make sure your EHR is certified by the Office of the National Coordinator for Health Information Technology
Consider using a qualified clinical data registry or a registry to extract and submit your quality data.
Check out our complete MIPS Resource Guide and Preparation Checklist
CMS Funded Technical Assistance
• Transforming Clinical Practice Initiative Practice Transformation Networks (PTNs) will assist 140,000+ clinicians to achieve large-scale health transformation over four years
• CMS is investing $100 million in technical assistance over five years to assist clinicians in rural areas, medically underserved areas, and practices with low MIPS final scores or those in transition to APM participation
Additional CMS Resources
Quality Payment Program Service Center• 1-866-288-8912
• TTY: 1-877-715-6222
• Open Monday-Friday, 8am-8pm ET
• Quality Innovation Networks (QINs) & Quality Improvement Organizations (QIOs)
• Self-service QPP Online Portal


Questions
Thank you!www.CareTransitionsNetwork.org
The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U.S. Department of Health & Human Services, Centers for Medicare & Medicaid Services.
Disclaimer: The contents provided are solely the responsibility of the authors and do not necessarily represent the official views of HHS or any of its agencies.