Embed Size (px)
Citation preview
An Interactive Discussion of Balancing the Efficacy and Safety
of Inhaled CorticosteroidsBased on Patient Cases
Maci and Michael
Benefits Risks
David P. Skoner, MD
Director, Division of Allergy & Immunology,
Department of Pediatrics.
Professor of Pediatrics, West Virginia University
School of Medicine.

Grant/Research Support Greer Laboratories, Novartis, Genentech, Merck, GlaxoSmithKline, Sunovion, Teva, Boston Scientific
Consultant Merck, Mylan, Greer, Meda
Speaker’s Bureau Merck, Meda, Boehringer Ingelheim, Greer
Stock Shareholder Nothing to Disclose
Employee Nothing to Disclose
Other I reviewed charts and served as doctor and consultant for Maci’s family and expert witness for Michael’s family.

Learning Objectives
• Discuss the diagnosis of asthma in children.
• Review benefits and risks of ICS in children with asthma.
• Discuss the prevention and early recognition of systemic side effects of ICS.

Introducing—Michael
Lifestyle
Activities
Diagnosis
Prescription
• 16-year old male• Growing up in upper-middle class neighborhood in Pittsburgh• Intelligent parents—father is a mathematics professor and mother
is a teacher at Michael’s school
• Enjoyed playing soccer• Huge Penn State football fan• Well-liked by many friends
• Diagnosed with asthma years earlier• Experienced fall asthma symptoms yearly, always mild and persistent• Visited pediatrician annually• One visit to asthma specialist for allergy skin testing and spirometry• Never required emergency care
• Received prescriptions only for albuterol and cromolyn, both to be used as needed
• Albuterol always provided symptom relief

History of Events—Michael Fall weekend during football season in November 1999
Thursday Friday Saturday
Parents left town to celebrate their wedding anniversary
Michael's older sister (only sibling) attended school at Penn State University
Michael was left in care of his aunt, who had no knowledge of asthma
Michael developed his typical fall asthma symptoms and used albuterol
Michael awakened and struggled to catch his breath for the first time ever with no relief from albuterol
Parents called and instructed aunt to take Michael to his pediatrician, who knew him very well
Regular pediatrician was out-of-town and the office was covered by another physician not familiar with Michael
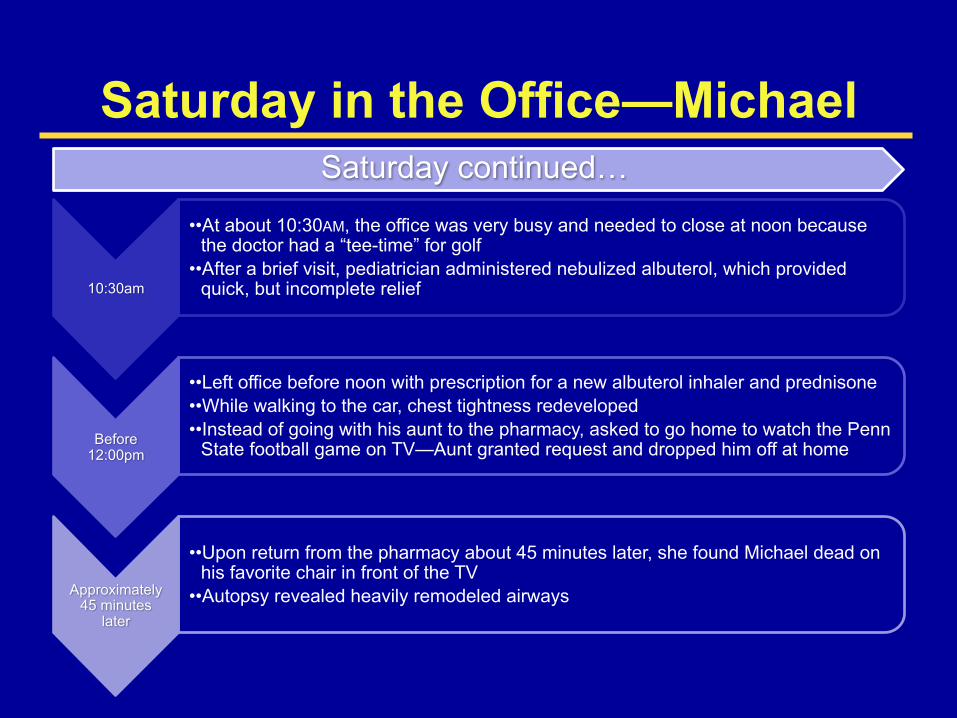
Saturday in the Office—Michael
10:30am
••At about 10:30AM, the office was very busy and needed to close at noon because the doctor had a “tee-time” for golf
••After a brief visit, pediatrician administered nebulized albuterol, which provided quick, but incomplete relief
Before12:00pm
••Left office before noon with prescription for a new albuterol inhaler and prednisone••While walking to the car, chest tightness redeveloped••Instead of going with his aunt to the pharmacy, asked to go home to watch the Penn
State football game on TV—Aunt granted request and dropped him off at home
Approximately45 minutes
later
••Upon return from the pharmacy about 45 minutes later, she found Michael dead on his favorite chair in front of the TV
••Autopsy revealed heavily remodeled airways
Saturday continued…

7
The child remained symptomatic and had diminished lung function despite high-dose oral steroid use for years
Grossly thickened basement membrane and edema within the lamina propria
Endobronchial Biopsy of a 16-year-old Male with Steroid-dependent Asthma
Reprinted with permission from Jenkins HA, et al. Chest. 2003;124:32-41.
In severe childhood asthma, significant airway remodeling can occur as early as 6 years of age, with little or no airway inflammation, and in spite of aggressive, long-term treatment with systemic and inhaled corticosteroids à need to look beyond inflammation in the treatment of severe asthma.
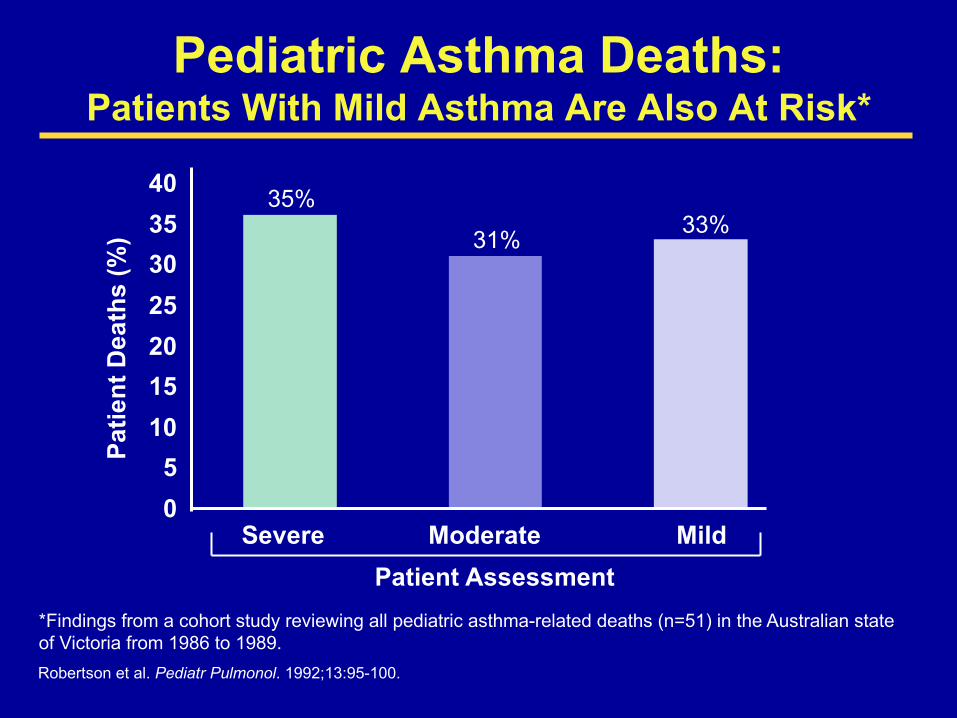
Pediatric Asthma Deaths:Patients With Mild Asthma Are Also At Risk*
05
10152025303540
Severe Moderate MildPatient Assessment
Patie
nt D
eath
s (%
)
Robertson et al. Pediatr Pulmonol. 1992;13:95-100.
*Findings from a cohort study reviewing all pediatric asthma-related deaths (n=51) in the Australian state of Victoria from 1986 to 1989.
35%
31% 33%

Benefits of Low-dose ICS
The index date for case patients and matched controls was the date of each case patient’s death from asthma. The rate ratio is adjusted for the age and sex of the patient; the number of prescriptions for theophylline, nebulized and oral β-adrenergic agonists, and oral corticosteroids in the year before the index date; the number of canisters of inhaled β-adrenergic agonists, dispensed in the year before the index date; and the number of hospitalizations for asthma during the two years before the index date.
Suissa S, et al. N Engl J Med. 2000;343(5):332-336.
0
0.5
1
1.5
2
2.5
0 1 2 3 4 5 6 7 8 9 10 11Number of Canisters of ICSs per Year
Rat
e R
atio
for D
eath
Fro
m A
sthm
a
12
The regular use of low-dose ICS is associated with a decreased risk of death
from asthma (powerful benefit at low-doses portends side effects)

NAEPP Guidelines—Benefits of ICSs• ICSs are preferred in the treatment of mild persistent
asthma in children, while cromolyn is recommended as an alternative
• ICS:– anti-inflammatory;– most effective long-term therapy for mild,
moderate, or severe persistent asthma;– well tolerated and safe at “recommended” doses.
• ICS DO NOT modify natural history.
NAEPP. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. August 28, 2007. Available online at http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf. Accessed March 30, 2016.
ICS = inhaled corticosteroid

Lessons From Michael’s Case• Children with “mild” asthma can die during their first
asthma attack and can have unexpectedly heavily remodeled airways.
• Children with asthma flare-ups should never be left alone.
• Patients with acute asthma must be monitored for rebound bronchoconstriction after albuterol treatment.
• Inhaled corticosteroids reduce risk of asthma death.
Balancing Efficacy and Safety
EfficacyMichael
SafetyMaci

Introducing—Maci
History
• 6.5 years of age• Presented to Pediatric Allergist on
11/23/09• 3-years of runny nose, nasal congestion,
posterior nasal drainage • Cough during colds and occasionally with
exercise• No recent shortness of breath or wheezing• Recurrent infections (sinusitis, otitis media,
RSV, others)• Mother had allergy and asthma

Introducing—Maci
Current Medications(can’t tell if they helped)
Physical Examination
Allergy Skin Testing/Other
• Cetirizine l0 mg qd• Montelukast 5 mg qd• Fluticasone furoate – 2 sprays qd, started January, 2009• Albuterol inhaler prn• Multivitamin daily
• Height 43.5 in (5th %ile), Weight 41lbs (10th %ile) • Well-developed and well-nourished • Allergic shiners, pale, edematous nasal turbinates, watery
nasal discharge, and lymphoid hyperplasia of the posterior pharyngeal wall
• Remainder of exam normal
• Puncture skin tests – positive to tree and grass pollen, mold and house dust mite
• Chest radiograph – not done

Spirometry

Spirometry

Introducing—Maci
Diagnosis by the Allergist
Recommendations and Dosages
• Allergic rhinitis• Asthma (cough-variant)• Cough• Recurrent sinusitis
• Mometasone INCS - 2 sprays in each nostril qd(FDA-unapproved dose)
• Fluticasone MDI - 110 mcg 2 puffs bid with AeroChamber®
(FDA-unapproved dose, NIH asthma guideline “high-dose”)• Cetirizine and Montelukast and Albuterol• Asthma action plan using symptoms• Follow-up visit in 6 weeks

Follow-up—Maci1/14/10
(6 years, 9 months old)8/3/10
(7 years, 4 months old)2/21/11
(7 years, 10 months)
• No interval asthma symptoms• No albuterol or prednisone use• Medication compliance good (>90%)
• Physical examination unchanged• Poor spirometry technique• FEV1 63%-75%, ACT Score 23-25
• Continue medications • Return visit 6 months
• Continue medications• Return visit 6 months
• Slight cough today• Mother worried about weight
gain and easy bruising of skin• Height 3rd percentile• Weight slightly >25th
percentile

Height/weight Plot Changes Not Viewed as Significant
fff

Follow-up—Maci2/21/11 continued…
(7 years, 10 months)
• Considering Mom’s concerns and Maci’s improvement, “it was time to wean the Fluticasone MDI anyway”
• Continue medications, except decrease Fluticasone MDI 110 mcg to 2 puffs qhs after the cough resolves
• Rinsing, gargling, spitting and brushing after use appeared for the first time in the asthma action plan
• Return visit 6 months
BUT, SHE NEVER MADE IT TO THAT FOLLOW-UP VISIT!INSTEAD, SHE EXPERIENCED A “GAME-CHANGING” EVENT.

Endocrinologist—Maci
Evaluation by Endocrinologist
on 4/5/11(8 years, 0 months)
• Mother requested endocrine referral from pediatrician for short stature and fast weight gain
• Still on Fluticasone MDI 110 mcg 2 puffs bid and MometasoneINCS
• Physical examination: Round faces and cheek fullness, a fat pad on the back of the neck, and centripetal deposit of adiposity
• Serum cortisol <2 mcg/dL (normal 2.5-22.9), ACTH <5 pg/mL (normal 5-46)
• Urinary free cortisol <1 mcg/L (low) • Normal bone age

Endocrinologist—Maci
Diagnosis by Endocrinologist
• (Iatrogenic) Cushing’s Syndrome• But, there was still reluctance to attribute this to
the inhaled steroids because no one had ever seen it before. So, her mother didn’t know if the adrenal gland would recover function or not, and was concerned that her daughter would die (Dr. Skoner’s involvement)

What the Parents Were Told About the Cause* of Maci’s New Symptoms and Signs after Starting the Medications
Symptom/Sign FluticasoneMDI/Mometasone INCS
Maci’s Diet/Activity Level/Genetics/Idiopathic
Short Stature
Fast Weight Gain
Easy Skin BruisingBMI Increase
Loss of Adrenal Gland Function
XXXX
X
* = not the cause; = the cause. X
Tumor (Pituitary)

Three questions the family needed Dr. Skoner to answer
Question ResponseHave you seen cases like Maci’s before? Yes
Can the ICS cause adrenal suppression? Yes
Will Maci’s adrenal gland recover after withdrawal of ICS?
Yes
Endocrinologist—Maci
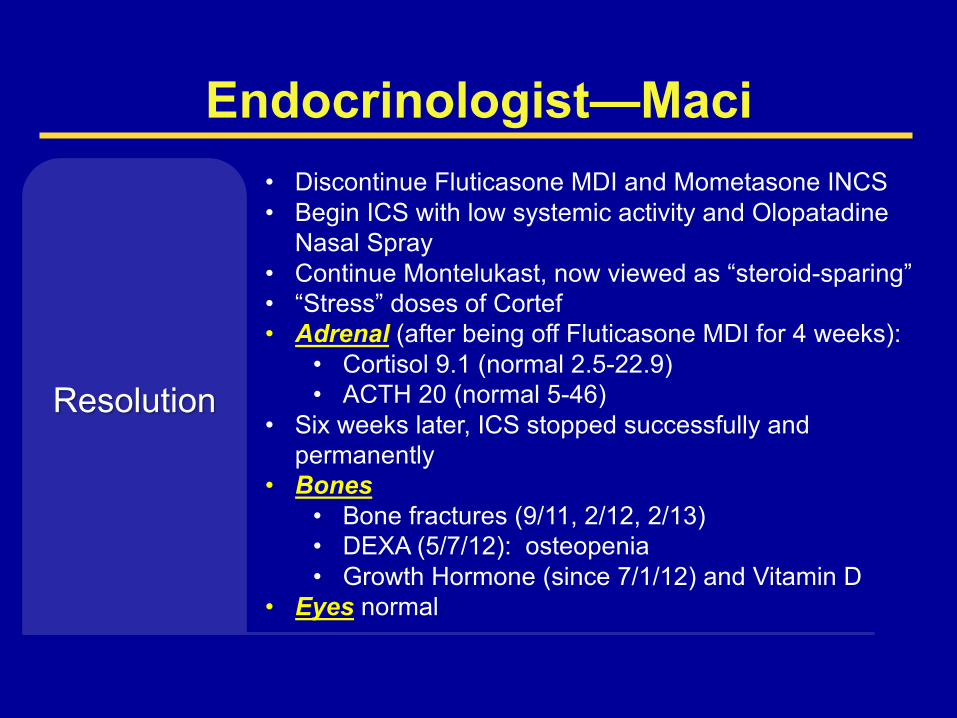
Resolution
• Discontinue Fluticasone MDI and Mometasone INCS• Begin ICS with low systemic activity and Olopatadine
Nasal Spray• Continue Montelukast, now viewed as “steroid-sparing” • “Stress” doses of Cortef• Adrenal (after being off Fluticasone MDI for 4 weeks):
• Cortisol 9.1 (normal 2.5-22.9)• ACTH 20 (normal 5-46)
• Six weeks later, ICS stopped successfully and permanently
• Bones• Bone fractures (9/11, 2/12, 2/13)• DEXA (5/7/12): osteopenia • Growth Hormone (since 7/1/12) and Vitamin D
• Eyes normal
Lessons From Maci’s CasevAsthma is difficult to diagnose in small children.vSome ICS have sufficient systemic activity to produce
Maci’s outcome (i.e. Cushing’s Syndrome, which was NOT caused by prednisone!).
vSystemic side effects begin to develop during the first 3 months of ICS therapy (good time for follow-up visit).
vChildren are unique: 1) NOT just little adults; 2) treatment risks; and 3) “at risk” when there is insufficient attention to ICS safety.
Skoner DP. Allergy Asthma Proc. 2016;37:1-12. Skoner DP. Ann Allergy Asthma Immunol. 2016;117:595-600.
Why Did This Happen to Maci? What Can We Do About This?
Raise awareness and learn how to more carefully balance safety and efficacy!

0%
10%
20%
30%
40%
50%
LOWDOSE(176UG/DAY)
HIGHDOSE(>880UG/DAY)
17%
43%
The Reason for Maci’s Adrenal Failure and FDA’s Lack of Approval of Fluticasone 110µg & 220µg for Children
“HPA Axis Suppression”
% with MorningSerum Cortisol<5.5 µg/dl
62 children with moderate to severe asthma followed for two years.Eid N et al. Pediatrics 2002; 109: 217-221.
Guideline: High Dose is >352 µg/dayMaci received 440 µg/day (110µg)

Duration of Side Effect
The Reason for Maci’s Growth Suppression and Long-Term Growth Hormone Treatment
“Systemic Activity”
Kelly HW et al. N Engl J Med. 2012;367(10):904-912.
Effect of Low-Dose Budesonide (Turbuhaler 200 µg bid) on Adult Height*Height Difference, Budesonide vs Placebo
Mean Age (yr) 9 11 13 25No. of ParticipantsBudesonidePlacebo
311418
296396
281383
281377
Treatment period(400 µg/day)
3 –
2 –
1 –
0 –
-1 –
-2 –
-3 –0 2 4 6 8 10 12 14 16
Years Since Randomization
Bud
eson
ide
vs P
lace
bo
Hei
ght D
iffer
ence
(cm
)
* Adherence steadily declined and was only about 50% at end of treatment period. J Allergy Clin Immunol 2012;129:112-8.
Duration of Benefit

*
RAISE AWARENESS AND EDUCATE
T = TeachingE = EveryoneA = AboutM = MedicationS = Safetywww.macisteams.org(site under construction)
CME coming soon.Patient Education.
More to come!Thankfully, able to
be selected by::

Two Cases Illustrate the Importance of Balancing Efficacy and Safety of ICS in Children
(Keys to Using ICS and INCS Wisely and Safely)
Efficacy1,2
§ Unquestioned, unparalleled.
Safety3,4
§ Make sure diagnosis is correct,§ Consider non-steroid alternatives, § Pick the safest steroid, § Use the lowest effective dose, § Optimize steroid sparing strategies,§ Treat comorbidities such as allergies, § Monitor growth, appearance, and behavior,§ Proactively discuss safety.1. NAEPP. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. August 28, 2007. Available online at http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf. Accessed March 30, 2016. 2. Suissa S et al. N Engl J Med. 2000;343(5):332-336. 3. Skoner DP. Pediatrics 2002: 109(2):381-392. 4. Skoner DP. Allergy Asthma Proc. 2016;37:1-12.

The Swinging Pendulum of ICS Safety
1990’sFearUnderuseMichael
2000’sNo fear
OveruseMaci
Stop Here
Stop Here

The Safety Landscape Has ChangedRead about how to pick the safest INS/INCS!
Skoner DP. Allergy Asthma Proc. 2016;37:1-12.

Michael’s and Maci’s Case(Perfect Storms and Opposing Forces)
Maci Michael
Age 6 years 16 years
High Level of Family Education and Resources?
Yes Yes
Allergic? Yes Yes
Asthma (Severity)? Not confirmed (Mild) Yes (Mild)
Failure of Doctors to Follow Guidelines?
Yes Yes
Role of ICS? Yes, too much* Yes, too little!
Life Threatening Event? Yes (Adrenal) Yes (Asthma)
Fatal Outcome? No Yes
*Use of high, FDA-unapproved doses of both inhaled and intranasal corticosteroids with systemic activity, with high adherence, lack of step-down over 18 months, and failure to acknowledge that evolving cushingoid features were drug-related.
Most likely, both would have had better outcomes on low-dose ICS!

1
SavetheDate12th AnnualNemacolinInternationalAsthmaConference
“LikebeingcourtsideatanNBAbasketballgame”
November 9–11, 2017
www.ahn.org/nemacolin-asthmaConference Directors
Deborah Gentile, MDTemple University
Paul O'Byrne MB, FRCP(C), FRSCMcMaster University
Giovanni Piedimonte, MD Cleveland Clinic Pediatric Institute
David P. Skoner, MDTemple University and West Virginia University
Sally E. Wenzel, MDUniversity of Pittsburgh