Embed Size (px)
Citation preview

96^ International Journal of Leprosy^ 1992
REFERENCES^6.
I. DtiNGAL, N. Is leprosy transmitted by arthropods?Lepr. Rev. 32 (1961) 28-35.LEWIS, D. J. The phlebotomine sanctifies of west
Pakistan. Bull. Br. Nlus. Hist. (Ent.) 19 (1967) I-57.
3. MANJA, K. S., NARAYANAN, E., KASTIJRI, G.,KIRCHHEIMER, W. F. and BALASUBRAMANYAN, M.Non-cultivable mycobacteria in some field collected
arthropods. Lepr. India 45 (1973) 231-234.4. Nlorm, G. B. and Trsii, R. 13. A simple technique
for mass rearing Luizomyia longipalpis and Phle-
botomu.s. papatasi (Diptera: Psychodidae) in the lab-
orators. J. Med. Entomol. 20 (1983) 568-569.5. NARAYANAN, E., SHANKAR MANIA, K., 13Ern. II. M.
S., RIRCHHEIMER, W. F. and BALASUBRANIANYAN,
M. Arthropods feeding experiments in leproma-
tous leprosy. Lepr. India 43 (1972) 188-193.
NARAYANAN, E., SREEVATSA, KIRCHHEIMER, W. F.and 13EDI, 13. M. S. Transfer of leprosy bacilli from
patients to mouse foot pads by . , lales aegipti. Lepr.
India 49 (1977) 181-186.NARAYANAN, E., SREEVATSA, DANIEL RAJ, A.,KIRCIIIILIMER, NV. F. and Brim, B. NI. S. Persistence
and distribution of M. leprae in Aeries ae,elpti and
Culex . fini,ecius experimentally fed on leprosy pa-tients. Lepr. India 50 (1978) 26-36.SAHA, K., JAIN, NI., NIIIKIIERJEE, M. K., CHAWLA,
and PRAKASII. N. Vi-
ability of Mycobacterium leprae within the gut ofAeries aegypt i after they feed on multibacillary lep-
romatous patients: a study by fluorescent and elec-
tron microscopes. Lepr. Rev. 56 (1985) 279-290.THEopoR, 0. Classification of the old world species
of the subfamily phlebotominae (Diptera: Psy-chodidae). Bull. Ent. Res. 39 (1948) 85-115.
7.
8.
9.
Comparison of PGL-I Level with AFB Numbers inFoot Pad Suspension
To THE EDITOR:
Since the time that phenolic glycolipid-I(PGL-I) was first isolated and characterizedas a Mycobacterium frprae-specific product( 4 ' 5 ), it has been widely used in serologicaltests for leprosy. Besides its use for purposesof detecting antibodies to the antigen, PGL-1has been found in various clinical speci-mens, such as serum ( 1-3 . '), urine (`'), andtissues (`. '), etc. However, PGL-I has neverbeen assayed in tissues of mouse foot padsinoculated with M. leprae where it couldprove to be a useful surrogate of acid-fastbacilli (AFB) numbers. Therefore, we at-tempted to measure the levels of PGL-I in
a mouse foot pad suspension using the dotenzyme-linked immunosorbent assay(ELISA) described previously ( 2 . 3 ). Briefly,foot pad suspensions (1.0-1.7 ml) were ly-ophilized, and the lipids were extracted withchloroform : methanol (2:1) solution. Afterapplication to a florisil column, the chlo-roform : methanol (19:1) elute was exam-ined for the presence of PGL-1 by dot-ELISAusing rabbit anti-M. leprae antiserum con-taining anti-PGL-I antibodies. A series ofnormal mouse foot pad suspensions con-taining different amounts of the standardPGL-I were processed using the same pro-cedures to determine the test parameters for
THE TABLE. Detection of PGL-1 in foot pad suvensions.
AFI3 numbers counted^No. assayedPGL-1-positive.'^PGL-I level (ng)
No. (%)^ Mean -±
<7.22 x 10'or <1.77 x 10 4 14 1^(7.1) 7.0
7.22 x^10'-9.4 x 10' 15 8 (53.3) 34.7 ± 39.6
1.0 x^10'-1.0 x^10" 15 15 (100) 98.0 ± 89.7
>1.0 x^10' 14 14 (100) 353.4^428.2
" Determined by dot-ELISA.Calculated based on the suspensions containing PGL-I.

60, 1^ Correspondence^ 97
the assay. The numbers of AFB inthese foot pad suspensions were obtainedmicroscopically by standard procedures ( 7 ),60 oil immersion fields being counted. Ifthere were no AFB in 60 fields, no M. lepraewere considered to have been present in thesample.
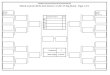
A total of 58 foot pad suspensions wereexamined. PGL-I was detectable in all sus-pensions, 29 in number, containing morethan 1.0 x 10 5 AFB (The Table). Of 15suspensions containing 7.22 x 10 3 to 9.4 x10 4 AFB, 8 specimens had detectable PGL-I. Also, PGL-I was detectable by dot-ELISAin one of 14 suspensions containing less than7.22 x 10 3 or less than 1.77 x 10 4 , whichwere considered AFB negative. When thePGL-I level was compared with the totalAFB numbers in each suspension, there wasa strong correlation (r = 0.834) (The Figure).Interestingly, PGL-I concentration in footpad suspension was much higher (about 20times) than the calculated PGL-I amountbased on the report that about 2.3% of M.leprae dry weight was PGL-I ( 4 ' 5 ). This ob-servation supports the contention that thelive bacilli actively secrete PGL-I into thesurrounding tissues, and that the antigenmay be trapped in tissues for a long time.The results also showed that the PGL-I levelin tissues corresponded approximately to theAFB numbers, especially at the critical level(10 5 AFB) when the growth of the usual 5x 10' M. leprae inoculum would have dem-onstrated unequivocal multiplication (').Therefore, it should be possible to use thePGL-I detection techniques instead ofcounting the AFB to determine bacillaryload in foot pad suspensions.
—Sang-Nae Cho, D.V.M., Ph.D.Joo-Deuk Kim, M.D., Ph.D.
Department of MicrobiologyYonsci University College of MedicineC.P.O. Box 8044Seoul 120-752, Republic of Korea
— Robert H. Gelber, M.D.Kuzell Institute for Arthritis and
Infectious DiseasesMedical Research Institute of San Francisco
at California Pacific Medical Center2200 Webster StreetSan Francisco, CA 94115-1896, U.S.A.
1000 =
1 00•^•
•^Expected•
10 =
• • •
1^i 1 Hum^1 1 1 111111^1 1 1111111^11 1111110 4^105^106^10'^105
AFB numbers/MFP suspension
THE FIGURE. Comparison of PGL-I level with AFBnumbers in the foot pad suspensions. Each dot indi-cates a suspension. The "expected line" was drawnbased on PGL-I amount calculated from the numbersof M. leprae.
—Patrick J. Brennan, Ph.D.Department of MicrobiologyColorado State UniversityFort Collins, CO 80523, U.S.A.
Acknowledgment. This work was supported by aresearch grant (1989) from the Heiser Program for Re-search in Leprosy and a contract from the G. W. LongHansen's Disease Center, Camille, Louisiana, U.S.A.We are grateful to Ms. E. 0. Shin, Lydia I'. Murray,Pat Siu. and Mabel Tsang for technical assistance.
REFERENCESI. CHANTEAU, S., CARTEL, J.-L.. PERANI, E., N'DELI,
L.. Roux, J. and GROSSET, J.-H. Relationshipsbetween PGL-I antigen in serum, tissue and via-bility of Mycobacterium leprae as determined bymouse footpad assay in multibacillary patientsduring short-term clinical trial. Lepr. Rev. 61 (1990)330-340.
2. CHO, S.-N., CELLONA, R. V., FAJARDO, T. T., JR.,
ABALOS, R. M., DELA CRUZ, E. C., WALSH, G. P.,KISI, J. D. and BRENNAN, P. J. Detection of phe-nolic glycolipid-I antigen and antibody in sera fromnew and relapsed lepromatous patients treated withvarious drug regimens. Int. J. Lepr. 59 (1991) 25-31.
3. CHO, S.-N., HUNTER, S. W., GELBER, R. H., REA,
T. H. and BRENNAN, P. J. Quantitation of thephenolic glycolipid of Mycobacterium leprae andrelevance to glycolipid antigenemia in leprosy. J.Infect. Dis. 153 (1986) 560-569.
4. HUNTER, S. W. and BRENNAN, P. J. A novel phe-nolic glycolipid from Mycobacterium leprae pos-
_J0a-

98^ International Journal of Leprosy^ 1992
sibly involved in immunogenicity and pathoge-nicity. J. Bacteriol. 147 (1981) 728-735.
5. HUNTER, S. W., FUJIWARA, T. and BRENNAN, P. J.Structure and antigenicity of the major specificglycolipid antigen of ilfycobacterium leprae. J. Biol.Chem. 257 (1982) 15072-15078.
6. KALDANY, R. R. J. and NURLIGN, A. Develop-ment of a dot-ELISA for detection of leprosy an-tigenuria under field conditions. Lepr. Rev. 57Suppl. 2 (1986) 95-100.
7. SHEPARD, C. C. and McRAE, D. FL A method forcounting acid-fast bacteria. Int. J. Lepr. 36 (1986)78-82.
8. VEMURI, N., KHANDKE, L., MAHADEVAN, P. R.,HUNTER, S. W. and BRENNAN, P. J. Isolation ofphenolic glycolipid I from human lepromatousnodules. Int. J. Lepr. 53 (1985) 487-489.
9. VENKATESAN, K., MINNIKIN, D. E., SINGH, H.,RAMU, G. and BlIARADWAJ, V. P. Detection ofrnycobacterial lipids in skin biopsies from leprosypatients. FEMS Microbiol. Lett. 44 (1987) 167-172.
10. YOUNG, D. B., HARNISCH, J. P., KNIGHT, J. andBUCHANAN, T. M. Detection of phenolic glyco-lipid I in sera from patients with lepromatous lep-rosy. J. Infect. Dis. 152 (1985) 1078-1081.
Long-Term Follow up of Lepromatous Leprosy PatientsReceiving Intralesional Recombinant Gamma-Interferon
To THE EDITOR:The primary defect in lepromatous lep-
rosy is probably the lack of generation ofsensitized T cells (') which results in defi-ciency of gamma-interferon (IFN--y) in thelesion ( 5). Macrophages in the tissue as wellas in the circulation of lepromatous patientsremain functionally normal because they re-lease oxygen intermediates when activatedby IFN-y and other antigens ( 3). Kaplan, etal. in their study on the effect of intralesionalrecombinant IFN-y (rIFN-y) have dem-onstrated the accumulation of lymphocytesand monocytes, marked thickening of theepidermis, and increased expression of Iaand y-IP-10 at the site of injection. Withrepeated injections of rIFN-y there was areduction in OKT-6 cells in the dermis anda distinct fall in the tissue bacterial index(BI) (5,000-10,000-fold) at the site of in-jection. This was often associated with theformation of an epithelioid granuloma withmultinucleated giant cells (24 ). The localchanges prompted us to follow these casesto see whether intralesional rIFN-y also in-fluences tissue response at distant sites.
Twenty-two lepromatous leprosy pa-tients (15 LLp, 7 LLs) were included in thisstudy. There were 18 males and four fe-males whose ages ranged from 23-58 years.Out of these 22 patients, six cases were un-treated and 15 cases were on treatment forless than 1 year. Only one patient was onantileprosy drugs for more than 5 years. Ly-
ophilized rl FN--y (Boehringer, Ingelheim amRhein, Germany) specific activity 2 X 10 7
U/mg protein was diluted and 10 pg IFN-yin 100 pi of excipient was injected at thelesional site. The number of such injectionsin an individual patient varied from 1 to 3or more. If a patient received more than oneinjection, it was on consecutive days andinto the same lesion.
Patients were subjected to clinical chart-ing, slit-skin smear, skin biopsy, and lep-romin testing initially and then at an inter-val of 3-6 months for 18 months. Allpatients were on conventional multidrugtherapy (MDT) throughout the study.
The clinical response in all 22 patientswas similar to what we observe with con-ventional MDT in our clinic. None showedevidence of clinical or histological upgrad-ing or lepromin conversion. Severe erythe-ma nodosum leprosum (ENL) was observedin four patients and mild-to-moderate ENLwas seen in seven patients. In two patientsneural pain was aggravated.
The average fall in the BI was of 1.0 (Rid-ley's scale) after 18 months of follow up.Histological examination revealed that thereduction in the size of the granuloma was1.16 and the fall in the granuloma BI was1.01 after 18 months of follow up (The Ta-ble).
The nature of the infiltrate was predom-inantly of the macrophage type, and the in-flux of lymphocytes was insignificant up to