Embed Size (px)
Citation preview

BRIEF REPORTM-BCR Rearrangement in a Case of T-Cell Childhood Acute
Lymphoblastic Leukemia
Maria Luiza Macedo Silva, MSc,1,2* Teresa de Souza Fernandez, MSc,1,2
Maria Helena Ornellas de Souza, MD, PhD,2 Rose Mary Pereira Soares, BS,2
Lilian Ayres Sa, ChB,1 Jane Dobbin, MD,2 Claudete Klumb, MD,2
Daniel Tabak, MD,2 Raul Correa Ribeiro, MD,3 and Eliana Abdelhay, PhD1
Key words: blast crisis; childhood cancer
We report clinical and molecular data of a case ofT-cell childhood acute lymphoblastic leukemia (ALL)with a Ph chromosome (Ph) that showed rearrangementinvolving the M-BCR region. He was 16-year-old boywho was admitted with a 1-week history of enlargementof cervical lymph nodes. He initially described general-ized bone pain with increased intensity over the leftflank.He then developed frontal headache, recurrent vomiting,and fever, and noticed a submandibular lymphnode. At ex-amination he was slightly disoriented. Diplopia and bilat-eral nistagmus were present. The neck was stiff; multiplecervical and inguinal lymph nodes were palpable. Liver andspleen were palpaple 3 cm below the costal margin.
Initial laboratory studies revealed a white blood cellcount of 700 × 109/L and a platelet count of 49 × 109/L.Peripheral blood cells were 100% lymphoblasts. Blastmorphology was compatible with ALL-L2, according tothe French-American-British (FAB) criteria. Cytochem-ical studies demonstrated Sudan Black negative cells and100% acid phosphatase focal staining positive. The chestX-ray examination showed mediastinal enlargement. De-spite emergency leucopheresis, his neurologic status pro-gressed and respiratory failure developed. He became co-matose and died 1 day after admission due to a cerebralhemorrhage.
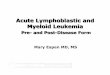
Immunophenotype of leukemic blast cells showed theprofile of T-cell leukemia in intermediate stage of dif-ferentiation. Surface CD3 was negative but cytoplasmicCD3 was 50% positive. The immunophenotypes wereCD7+, CD2+, CD4+, and CD8+, but cells were negativefor B-antigen (CD19) and myeloid-associated markers.Peripheral blood cells karyotype after GTG banding [1]showed 10 normal cells (31%) and 22 (69%) with46,XY,t(9;22)(q34;q11) according to the InternationalSystem of Human Cytogenetic Nomenclature (ISCN) [2].This rearrangement was present as a sole abnormality.Thebreakpoint analysis by Southern blotting using the exon 1M-BCR probe from ATCC (Fig. 1) and by Western blotting
using monoclonal antibody to c-abl [c-abl(Ab-2)] showed aM-BCR rearrangement producing the p210 protein (Fig. 2).
DISCUSSION
The clinical distinction between blast crisis of CMLand de novo Ph in acute leukemia is not always clear. Thefeatures that are used to distinguish Ph ALL from CML inblast crisis include the presence of chromosomally normalcells accompanying the Ph clone at diagnosis or later in thedisease; and the achievement of true hematological and, insome cases, cytogenetic remission [3].
Recently, studies of lineages determination to distin-guish de novo Ph in acute leukemia and blast crisis ofCML showed that multilineage was associated with theM-BCR/ABL fusion, and lymphoblast-restricted diseasewas seen in cases with m-BCR/ABL [4]. However, it wasdemonstrated by Tachibana et al. [5] in a case with m-BCR/ABL rearrangement that there was multilineage in-volvement and by Secker-Walker and Craig [3] that theM-BCR/ABL rearrangement occurred in a case of lym-phoblastic lineage, showing that the rearrangement at mo-lecular level do not distinguish the two types of Ph blasts.
Due to the fact that blast crisis of T-type is very rare,our results showing the presence of normal cells at thesame time with Ph cells, the lack of myeloid antigens,and the presence of mediastinal mass suggest the features
1Universidade Federal do Rio de Janeiro, Instituto de Biofı´sica CarlosChagas Filho, Laborato´rio de Biologia Molecular Maury Miranda, Riode Janeiro, Brasil2Instituto Nacional de Caˆncer, Rio de Janeiro, Brasil3Departments of Hematology, Oncology and Pediatrics, St. Jude Chil-dren’s Research Hospital, University of Tennessee College of Medi-cine, Memphis, Tennessee*Correspondence to: Maria Luiza Macedo Silva, Instituto Nactional deCancer, Prac¸a Cruz Vermelha, 23, 7 andar, Centro, Rio de Janeiro, RJ,CEP 20230-130, Brasil.
Received 8 June 1998; Accepted 10 November 1998
Medical and Pediatric Oncology 32:455–456 (1999)
© 1999 Wiley-Liss, Inc.

of a de novo Ph in T-cell acute leukemia. So this casecould be the first de novo T-cell childhood ALL showingthe expression of p210 protein associated with a veryaggressive clinical evolution.
REFERENCES
1. Seabright M. A rapid banding technique for human chromosomes.Lancet 1971;2:971–972.
2. ISCN. An International System for Human Cytogenetic Nomen-clature. Mitelman F, editor. Basel: S. Karger; 1995.
3. Secker-Walker LM, Craig JM. Prognostic implications of break-point and lineage heterogeneity in Philadelphia positive acutelymphoblastic leukemia: a review. Leukemia 1993;7:147–151.
4. Anastasi J, Feng J, Dickstein JI, et al. Lineage involvement byBCR-ABL in Ph+ lymphoblastic leukemias: chronic myelogenousleukemia presenting in lymphoid blast phase vs. Ph+ acute lym-phoblastic leukemia. Leukemia 1996;10:795–802.
5. Tachibana N, Raimondi SC, Lauer SJ, et al. Evidence for a mul-tipotential stem cell disease in some childhood Philadelphia chro-mosome positive acute lymphoblastic leukemia. Blood 1987;70:1458–1461.
Fig. 2. Western blot analysis using a mouse monoclonal antibody toABL [c-abl(Ab-2), Oncogene Science], showing the presence of p210and p145 proteins in the extract of ALL patient cells and absence of thep210 protein in normal bone marrow cells.
Fig. 1. DNA Southern blot analysis after restriction withEcoR1,BglII, and HindIII. The BCR gene fragment containing exon 1 ofM-BCR region was labeled by random priming procedure usingaP32
dATP and used as probe. Lane 1: control DNA; lane 2: CML patientDNA; lane 3: ALL patient DNA.EcoR1 fragments: wild-type 17 kb,CML rearrangement 23 kb, ALL rearrangement 4.2 kb.BglII frag-ments: wild-type 7.0 kb, CML rearrangements 8.9 kb, ALL rearrange-ments 8.9 kb and 2.2 kb.HindIII fragments: wild-type 8.9 kb, CMLrearrangements 1.8 kb, ALL rearrangements 1.8 kb.
456 Silva et al.