Embed Size (px)
Citation preview
MALABSORPTIONGROUP A
MALABSORPTION SYNDROME
Diminished intestinal absorption of one or more dietary nutrients
Not an adequate final diagnosis Most are associated with steatorrhea
Increase in stool fat excretion of >6% dietary fat intake
APPROACH TO THE PATIENTMalabsorption
HISTORY, SYMPTOMS AND INITIAL PRELIMINARY OBSERVATION
Extensive small-intestinal resection for mesenteric ischemia Short bowel syndrome
Steatorrhea with chronic alcohol intake and chronic pancreatitis Pancreatic exocrine dysfunction
ACTIVE TRANSPORT OF SITE-SPECIFIC DIETARY NUTRIENT ABSORPTION
Throughout SI (Proximal>Distal)Glucose, amino acids, lipids
Proximal SI (esp. duodenum)Calcium IronFolate
IleumCobalaminBile acids
ADAPTATION
Morphologic and functional Due to segmental resection Secondary to the presence of luminal
nutrients and hormonal stimuli Critical for survival
STEATORRHEA
Quantitative stool fat determination (72 hours)Gold standard
Qualitative Sudan III stainDoes not establish degree of fat
malabsorptionFor preliminary screening studies
Blood, breath, and isotropic testDo not directly measure fat absorptionExcellent sensitivity only with obvious
steatorrheaNot survived transition from research
laboratory to commercial application
LABORATORY TESTING Vitamin D malabsorption
Evidence of metabolic bone disease Elevated serum ALP Reduced serum calcium
Vitamin K malabsorption Elevated prothrombin time Without liver disease No intake of anti-coagulants
LABORATORY TESTING Cobalamin/Folate malabsorption
Macrocytic anemia Iron malabsorption
Iron deficiency anemia No occult bleeding from GIT Non-menstruating female Exclusion of celiac sprue
Iron is absorbed in the proximal SI
DIAGNOSTIC PROCEDURESMalabsorption
DIAGNOSIS OF MALABSORPTION
Effect of prolonged (>24h) fasting on stool output Osmotic diarrhea
Decrease in stool output: Presumptive evidence that diarrhea is related to malabsorption
Secretory diarrhea Persistence of stool output: Not due to nutrient
deficiency
STOOL OSMOTIC GAP
Normal: 290-300 mosmol/kg H20 Significant osmotic gap
Suggests the presence of anions other than Na and K are present in the stool, presumably the cause of diarrhea
Diff >50: osmotic gap present, dietary nutrient is not absorbed
Diff <25: dietary nutrient is not responsible for the diarrhea
Useful in differentiating secretory from osmotic diarrhea
2 x (stool [Na+] + [stool K+]) ≤ stool osmolality
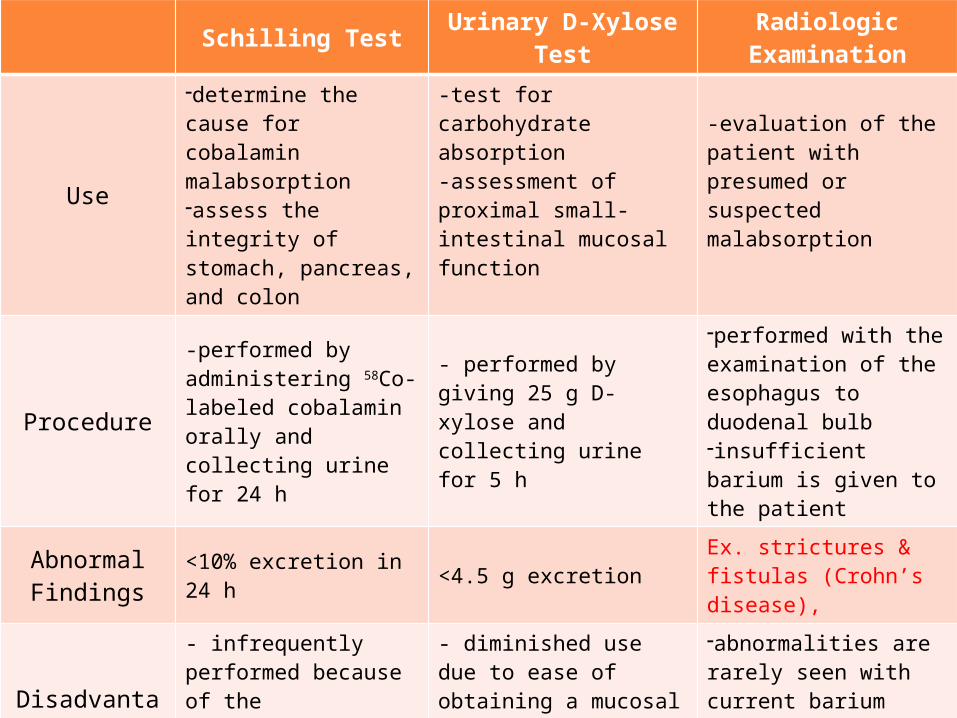
Schilling Test Urinary D-Xylose Test
Radiologic Examination
Use
-determine the cause for cobalamin malabsorption-assess the integrity of stomach, pancreas, and colon
-test for carbohydrate absorption-assessment of proximal small-intestinal mucosal function
-evaluation of the patient with presumed or suspected malabsorption
Procedure
-performed by administering 58Co-labeled cobalamin orally and collecting urine for 24 h
- performed by giving 25 g D-xylose and collecting urine for 5 h
-performed with the examination of the esophagus to duodenal bulb-insufficient barium is given to the patient
AbnormalFindings
<10% excretion in 24 h <4.5 g excretion
Ex. strictures & fistulas (Crohn’s disease),
Disadvantage
- infrequently performed because of the unavailability of human intrinsic factor
- diminished use due to ease of obtaining a mucosal biopsy by endoscopy and false-negative rate
-abnormalities are rarely seen with current barium suspensions, skilled personnel required
COBALAMIN ABSORPTION
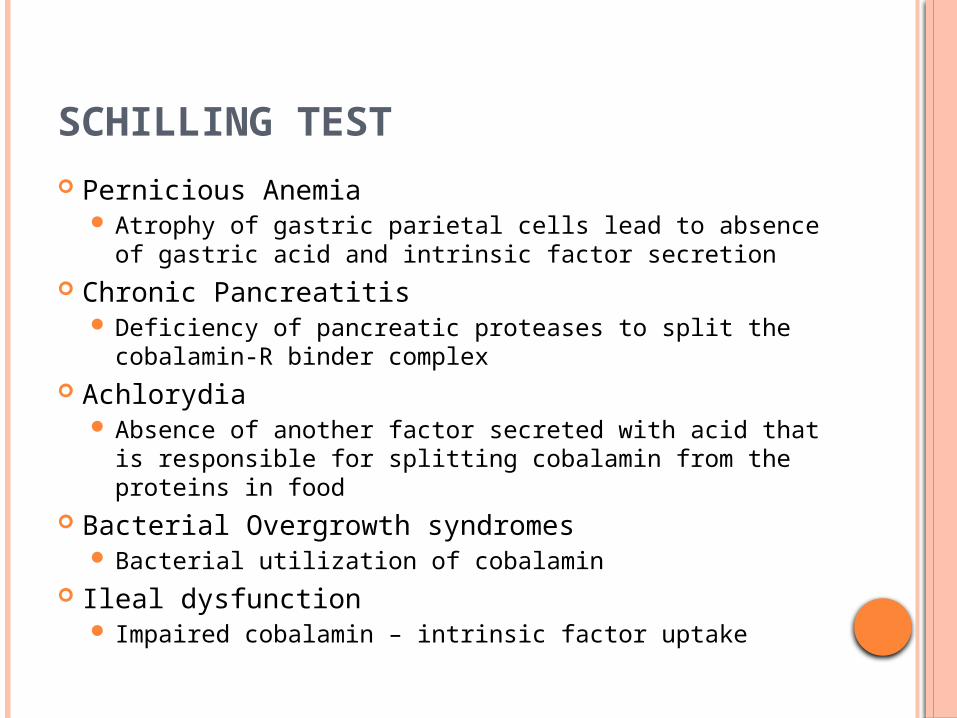
SCHILLING TEST
Pernicious Anemia Atrophy of gastric parietal cells lead to absence of
gastric acid and intrinsic factor secretion Chronic Pancreatitis
Deficiency of pancreatic proteases to split the cobalamin-R binder complex
Achlorydia Absence of another factor secreted with acid that is
responsible for splitting cobalamin from the proteins in food
Bacterial Overgrowth syndromes Bacterial utilization of cobalamin
Ileal dysfunction Impaired cobalamin – intrinsic factor uptake
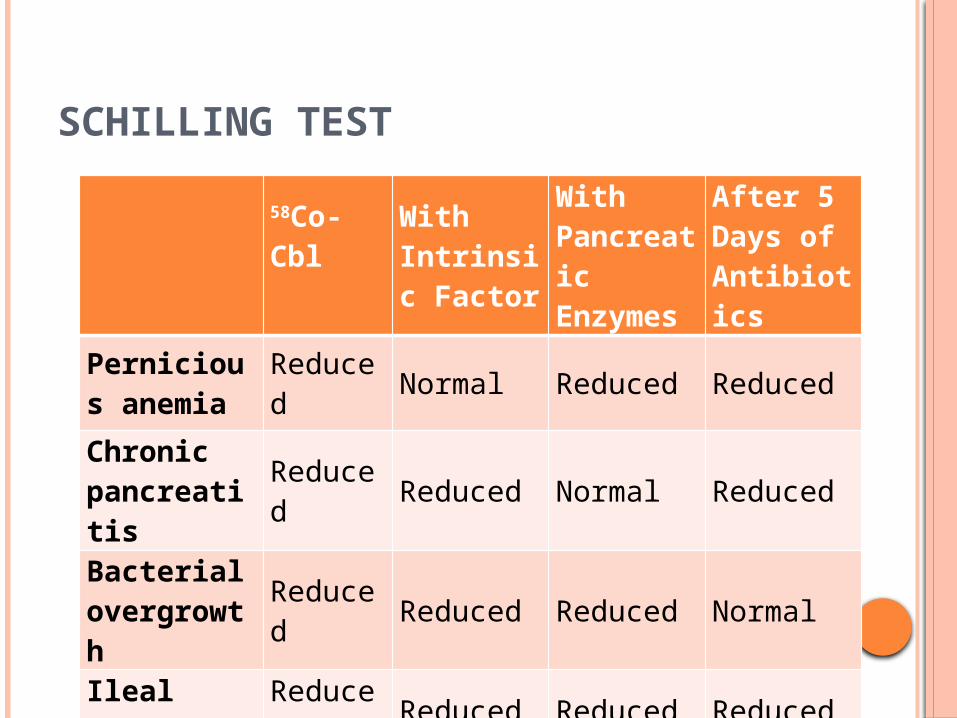
SCHILLING TEST
58Co-Cbl
With Intrinsic Factor
With Pancreatic Enzymes
After 5 Days of Antibiotics
Pernicious anemia Reduced Normal Reduced Reduced
Chronic pancreatitis Reduced Reduced Normal Reduced
Bacterialovergrowth Reduced Reduced Reduced Normal
Ileal disease Reduced Reduced Reduced Reduced
BIOPSY OF SMALL-INTESTINAL MUCOSA
Essential in the evaluation of a patient with documented steatorrhea or chronic diarrhea
Preferred method to obtain histologic material of proximal small-intestinal mucosa
Indications: Evaluation of a patient either with documented
or suspected steatorrhea or with chronic diarrhea
Diffuse or focal abnormalities of the small intestine defined on a small-intestinal series
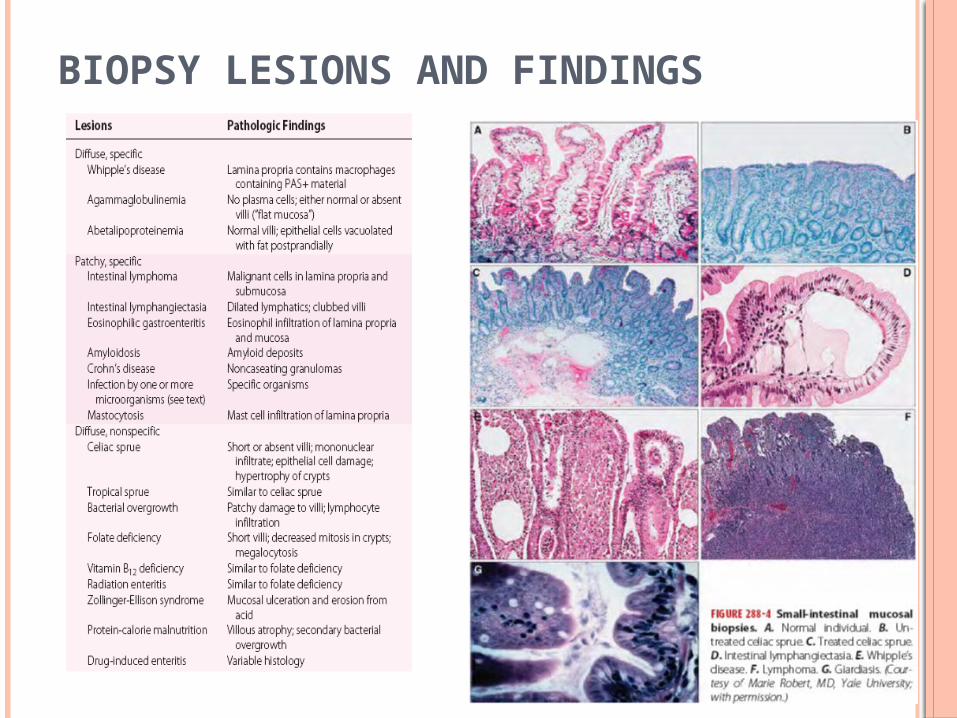
BIOPSY LESIONS AND FINDINGS
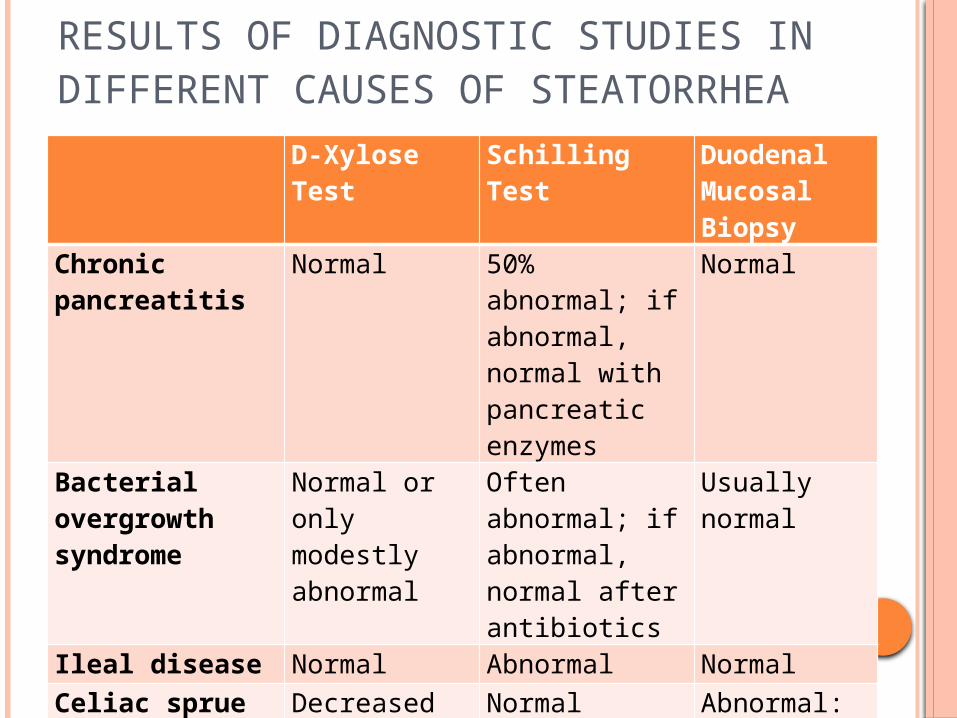
RESULTS OF DIAGNOSTIC STUDIES IN DIFFERENT CAUSES OF STEATORRHEA
D-Xylose Test Schilling Test Duodenal Mucosal Biopsy
Chronic pancreatitis Normal 50% abnormal; if abnormal, normal with pancreatic enzymes
Normal
Bacterial overgrowth syndrome
Normal or only modestly abnormal
Often abnormal; if abnormal, normal after antibiotics
Usually normal
Ileal disease Normal Abnormal NormalCeliac sprue Decreased Normal Abnormal:
probably "flat"Intestinal lymphangiectasia
Normal Normal Abnormal: "dilated lymphatics"
DIFFERENTIAL DIAGNOSIS FOR CHRONIC DIARRHEA: APPROACH TO A PATIENT WITH MALABSORPTION
DISEASE ENTITIES CAUSING MALABSORPTION
CELIAC SPRUE Other names:
Nontropical sprue, Celiac disease, gluten-sensitive enteropathy
Etiology is not known Environmental – gliadin-associated Immunologic – IgA antigliadin, IgA antiendomysial, IgA
anti-tTg antibodies Genetic – HLA-DQ2 allele
Protean manifestations most of which are secondary to nutrient malabsorption
Onset of symptoms occur at ages ranging from first year of life to eighth decade
Clinical manifestations: Appear with the introduction of cereals in an infants
diet ranges from significant malabsorption to multiple
nutrients, diarrhea, steatorrhea, weight loss, consequences of nutrient depletion to absence of any GI symptoms but with evidence of a single nutrient depletion
Hallmark: malabsorption and histologic changes
Mechanism of diarrhea: Steatorrhea Secondary lactase deficiency Bile acid malabsorption Endogenous fluid secretion
Associated diseases: Dermatitis herpetiformis (DH) DM type 1 IgA deficiency
Complications: GI and non GI neoplasms Intestinal ulceration Refractory sprue Collagenous sprue
TROPICAL SPRUE
Affects 5-10% of population in some tropical area
Etiology and pathogenesis is uncertain Clinical manifestations:
Chronic diarrhea Steatorrhea Weight loss Folate and cobalamin deficiencies
SHORT BOWEL SYNDROME General term for
digestive problems that occur after a resection
Depends on Segment resected Length of segment Presence of ileocecal
valve Extent of colon removal Residual disease
Generally, need to lose 2/3 of intestine
Usually acquired Can be congenital in
children Congenital short bowel
After resection, intestine undergoes adaptation.
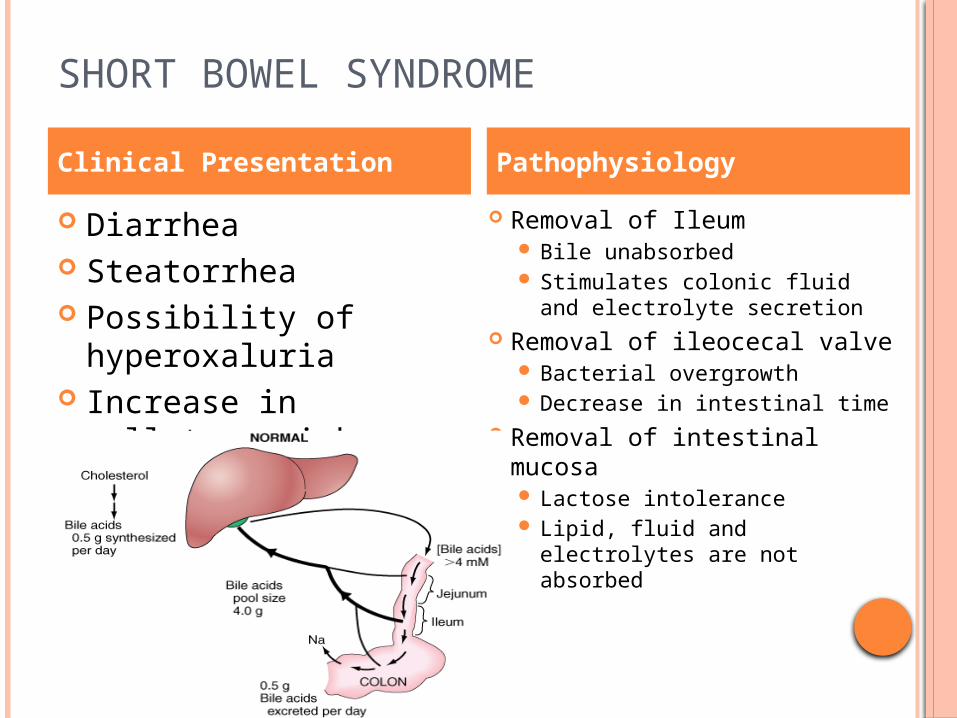
SHORT BOWEL SYNDROME
Diarrhea Steatorrhea Possibility of
hyperoxaluria Increase in gallstone
risk Increase in gastrin
levels
Removal of Ileum Bile unabsorbed Stimulates colonic fluid and
electrolyte secretion Removal of ileocecal valve
Bacterial overgrowth Decrease in intestinal time
Removal of intestinal mucosa Lactose intolerance Lipid, fluid and electrolytes
are not absorbed
Clinical Presentation Pathophysiology
SHORT BOWEL SYNDROME KEY POINTS
Follows resection of intestines Generally inadequacy in absorbing food and
fluids because of lack of surface area
BACTERIAL OVERGROWTH SYNDROME Proliferation of colonic type bacteria within
small intestine Clinical Manifestation
DiarrheaSteatorrheaMacrocytic anemia
BACTERIAL OVERGROWTH SYNDROME
Pathogenesis Etiology
BACTERIAL OVERGROWTH SYNDROME KEY POINTS
Macrocytic anemia Because of lack of B12
Stasis = allows bacteria to multiply
WHIPPLE’S DISEASE Insidious in presentation Chronic multisystem disease Usually causesClinical Manifestation
DiarrheaSteatorrheaWeight lossAbdominal painArthralgiaCNS/ cardiac problems
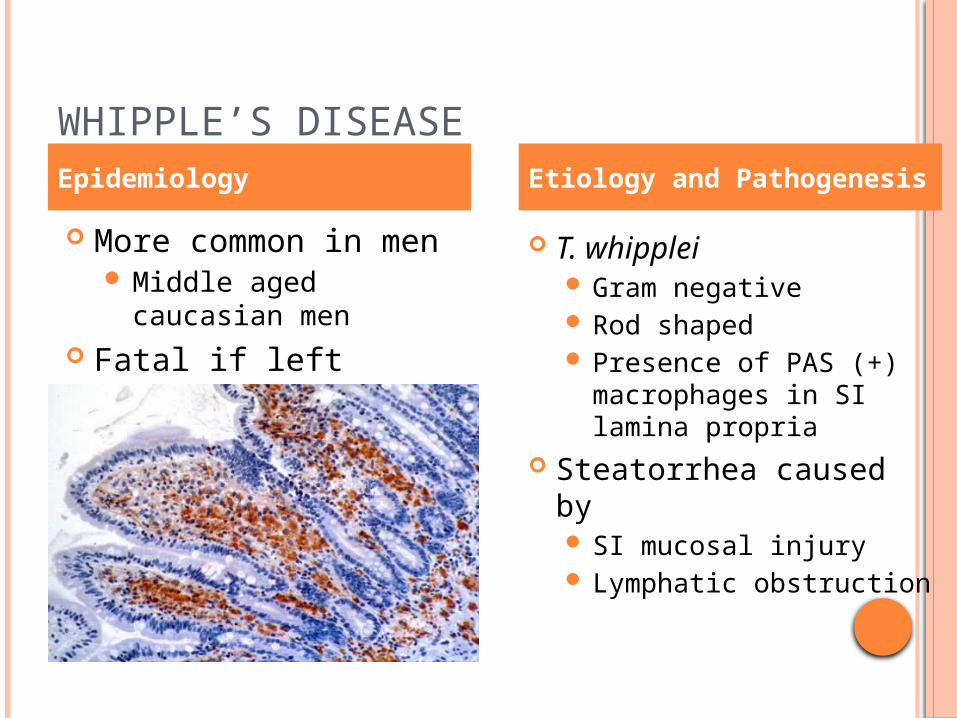
WHIPPLE’S DISEASE
More common in men Middle aged caucasian
men Fatal if left untreated
T. whipplei Gram negative Rod shaped Presence of PAS (+)
macrophages in SI lamina propria
Steatorrhea caused by SI mucosal injury Lymphatic obstruction
Epidemiology Etiology and Pathogenesis
WHIPPLE’S DISEASE KEY POINTS
Rare, SYSTEMIC disease Insidious CNS and cardiac symptoms
Dementia = POOR prognosis Caused by damage to mucosa and lymphatic
obstruction
PROTEIN LOSING ENTEROPATHY Group of diseases with Hypoproteinemia and
edema WITHOUT Proteinuria/ kidney problems Protein synthesis defects/ liver problems
Clinical Manifestation Peripheral edema Diarrhea Steatorrhea
PROTEIN LOSING ENTEROPATHY
Excess protein loss in the GI tract Exceeds the normal
10% protein catabolism
Pathogenesis Etiology
PROTEIN LOSING ENTEROPATHY KEY POINTS
Peripheral edema, hypoproteinemia More than >10% total protein breakdown Proteins lost through exudates, altered
permeability, lymphatic obstruction
TREATMENT
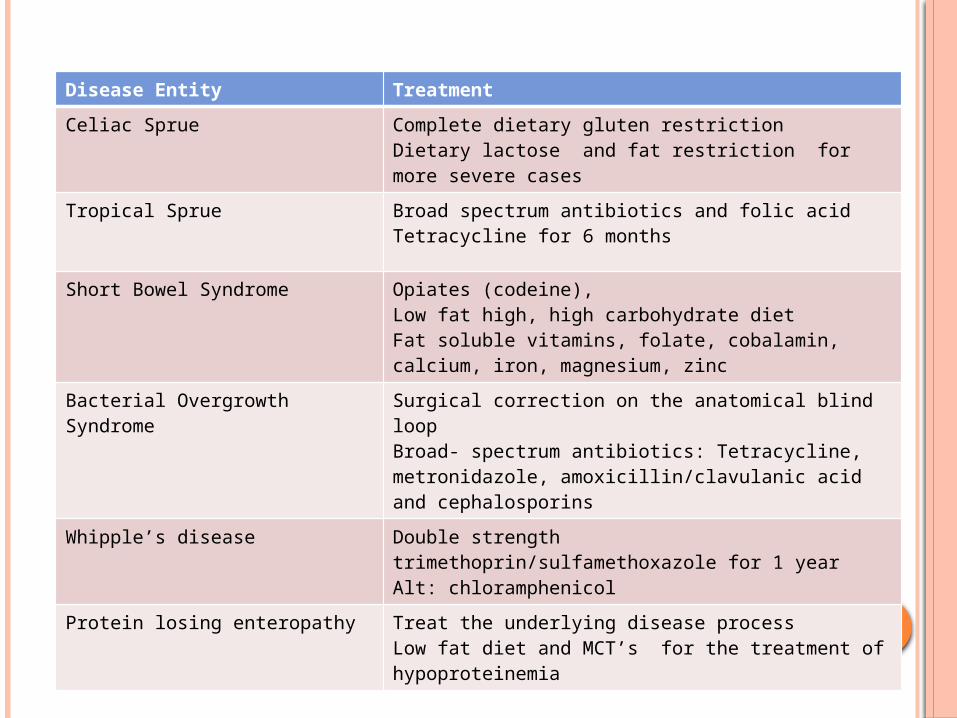
Disease Entity Treatment
Celiac Sprue Complete dietary gluten restrictionDietary lactose and fat restriction for more severe cases
Tropical Sprue Broad spectrum antibiotics and folic acidTetracycline for 6 months
Short Bowel Syndrome Opiates (codeine), Low fat high, high carbohydrate dietFat soluble vitamins, folate, cobalamin, calcium, iron, magnesium, zinc
Bacterial Overgrowth Syndrome Surgical correction on the anatomical blind loopBroad- spectrum antibiotics: Tetracycline, metronidazole, amoxicillin/clavulanic acid and cephalosporins
Whipple’s disease Double strength trimethoprin/sulfamethoxazole for 1 yearAlt: chloramphenicol
Protein losing enteropathy Treat the underlying disease processLow fat diet and MCT’s for the treatment of hypoproteinemia





























