Embed Size (px)
Citation preview

Silvia Montoto, St Bartholomew’s Hospital, London, UKESMO Preceptorship on Lymphoma
Madrid, 25-26 November 2016
LYMPHOMA in HIV PATIENTS

Disclosures of commercial support
Roche √
Gilead √
Lymphoma in HIV patients
• AIDS-related lymphoma (ARL) is an AIDSdefining malignancy (ADM):
-DLBCL (immunoblastic)
-BL
-PCNSL
• HL is a non-AIDS defining malignancy (NADM)

WHO 2008 classification
Incidence of lymphoma in HIV patients
• Increased incidence of NHL and HL in HIV+ patients– NHL: x >100 in HIV+
– HL: x 10-20 in HIV+
• Related to:– CD4 count
– HAART
• Cause of death in HIV: 1/3 cancer (NHL mostfrequent)
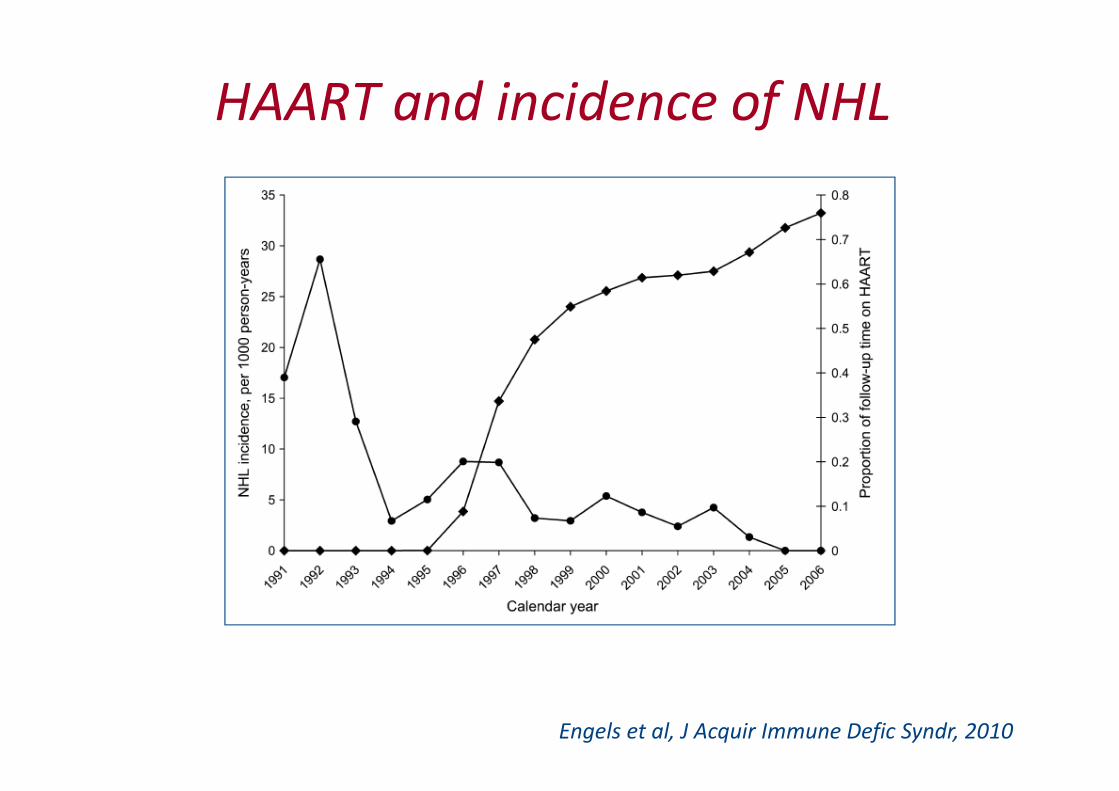
HAART and incidence of NHL
Engels et al, J Acquir Immune Defic Syndr, 2010
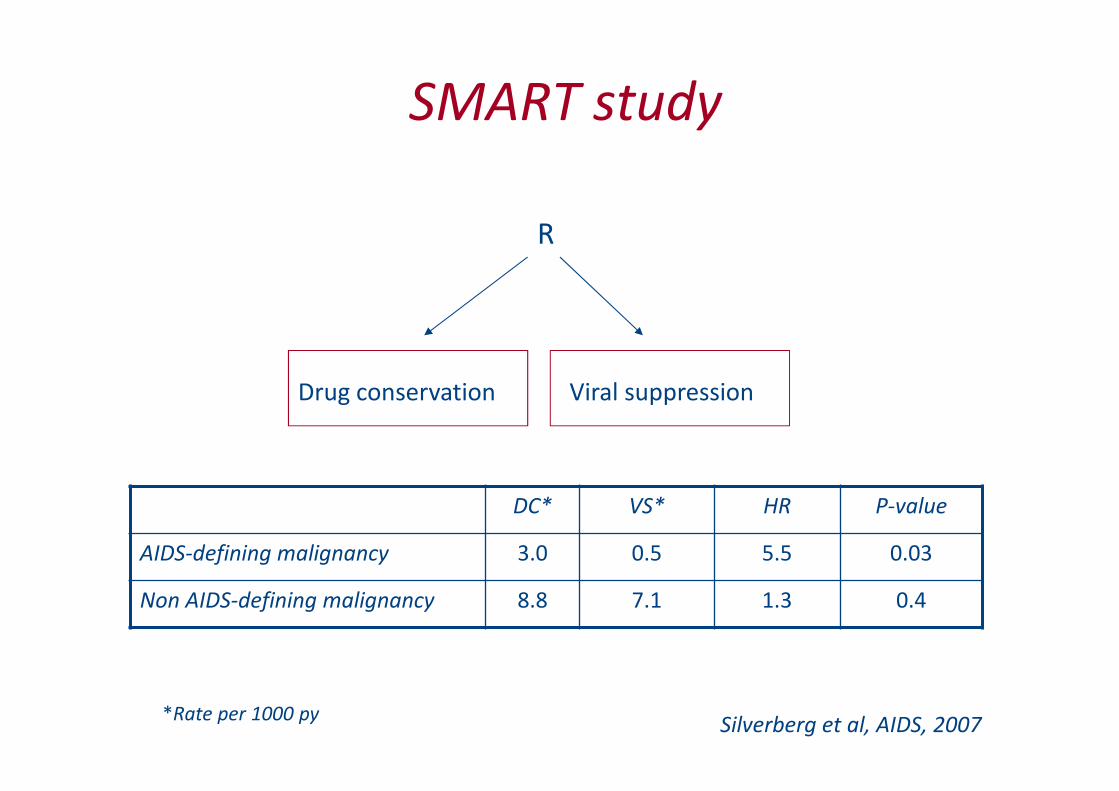
SMART study
R
Drug conservation Viral suppression
DC* VS* HR P-value
AIDS-defining malignancy 3.0 0.5 5.5 0.03
Non AIDS-defining malignancy 8.8 7.1 1.3 0.4
*Rate per 1000 pySilverberg et al, AIDS, 2007
Treatment of ‘ARL’:
controversial points
• With/without HAART
• Infusional regimens vs ‘conventional’ regimens
• With/without rituximab
• Salvage therapy
Treatment of ‘ARL’: controversial points
• With/without HAART
• Infusional regimens vs ‘conventional’ regimens
• With/without rituximab
• Salvage therapy
Controversial points: with/without HAART
• Against: ↑ toxicity
– Haematological
– NRL
• In favour: ↑ efficacy
• But...no RCT
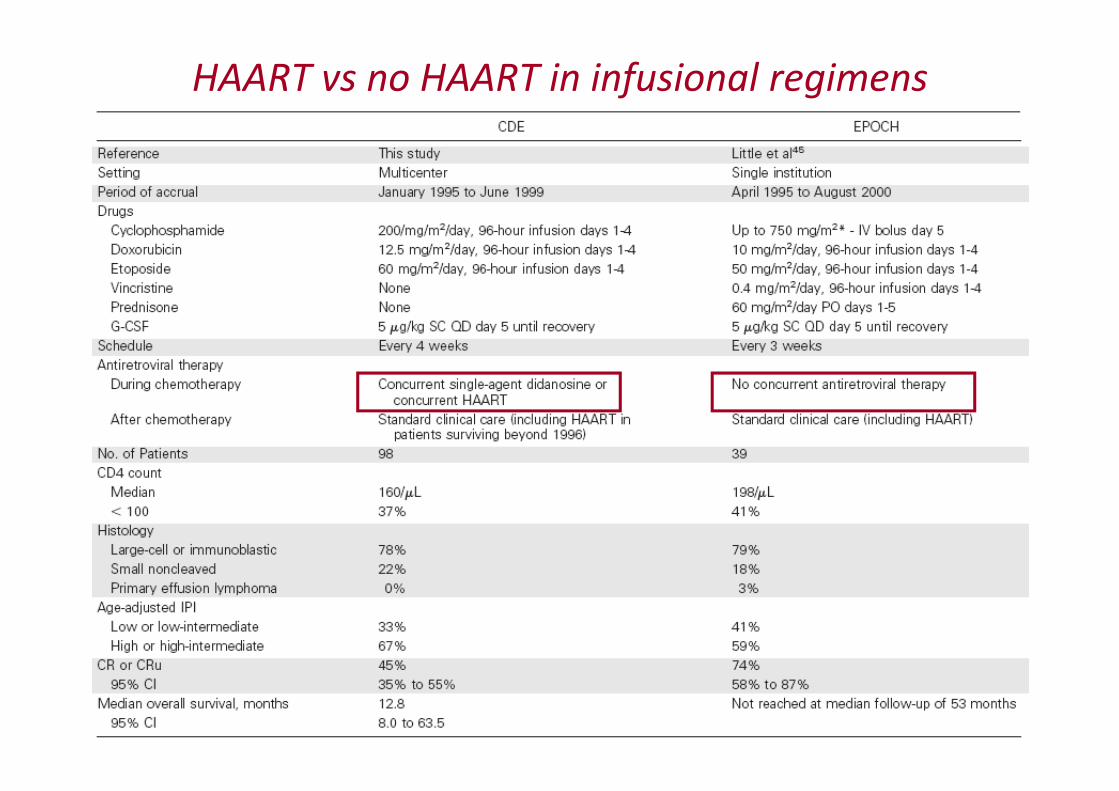
HAART vs no HAART in infusional regimens

Infusional regimens: toxicity
DA-EPOCH
No HAART
CDE
Pre-HAART HAART
(43) (55)
Febrile neutropenia 13% 10%* 6%*
Dose reductions NS 48% 36%
OI 8% 19% 8%
Deaths 5 in remission (of 39
pts)
9% TRM 0
*grade 4 infection
Sparano et al, JCO, 2004
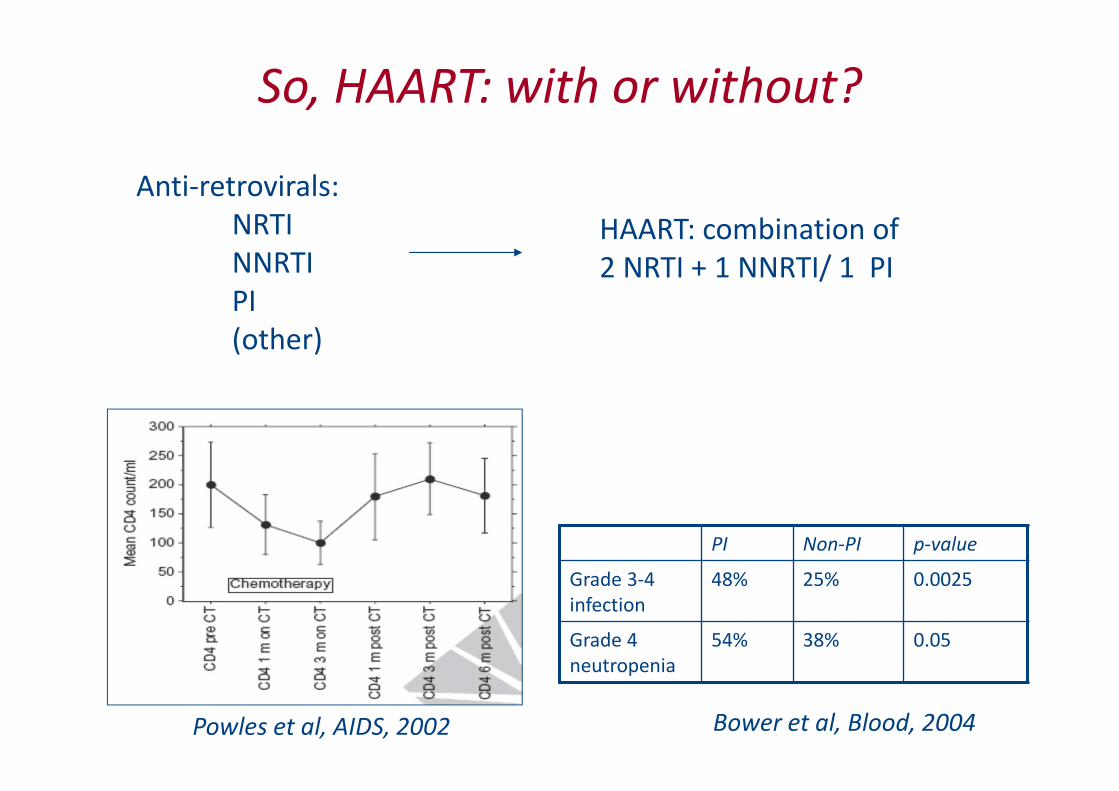
So, HAART: with or without?
Powles et al, AIDS, 2002 Bower et al, Blood, 2004
PI Non-PI p-value
Grade 3-4
infection
48% 25% 0.0025
Grade 4
neutropenia
54% 38% 0.05
Anti-retrovirals:
NRTI
NNRTI
PI
(other)
HAART: combination of
2 NRTI + 1 NNRTI/ 1 PI

Outcome of HIV+ve on HAART vs no HAART
DLBCL: CHOP vs CHOP-HAART HL: Chemo vs chemo-HAART
Vaccher et al, Cancer, 2001 Hentrich et al, Ann Oncol, 2006

Outcome depending on response to HAART
Patients with HL treated with ABVD + HAART
OS EFS
Xicoy et al, Haematologica, 2007
Treatment of ARL: controversial points
• With/without HAART
• Infusional regimens vs ‘conventional’regimens
• With/without rituximab
• Salvage therapy

Infusional regimens in HIV-ve patients with
DLBCL
To be presented at ASH 2016
• 524 patients
• Median follow-up: 5 yrs
• No diffs EFS or OS

Infusional regimens in HIV-lymphoma
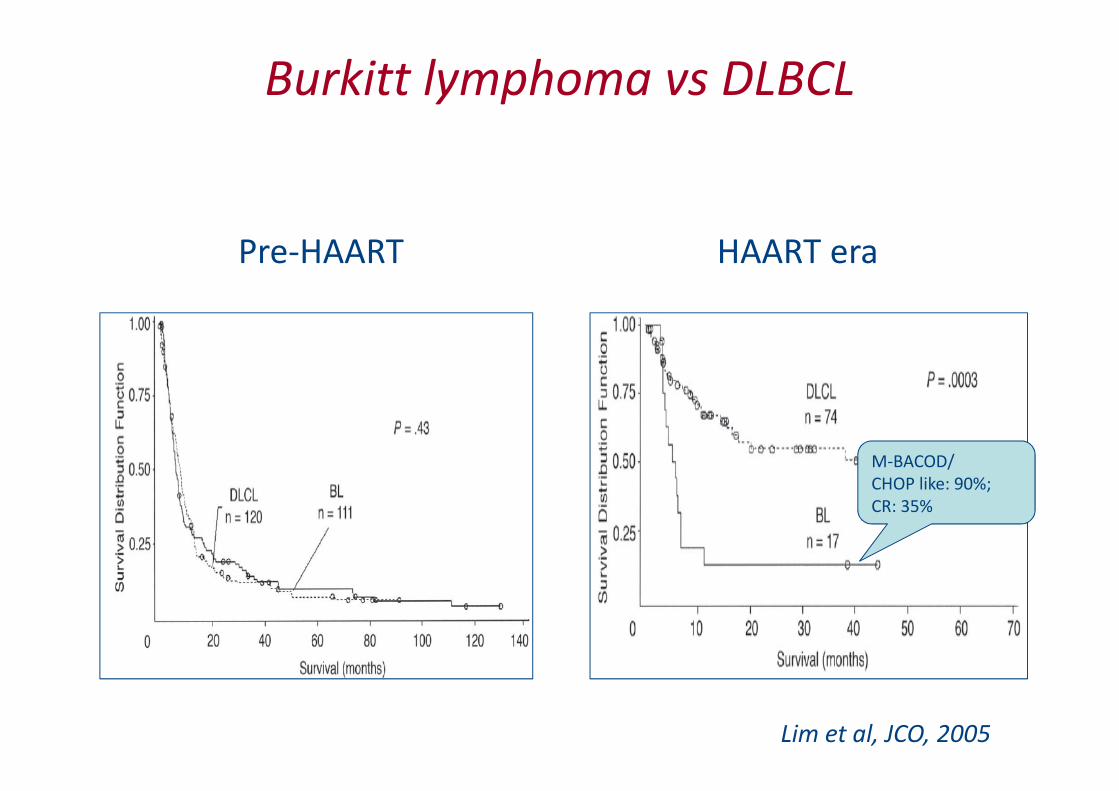
Burkitt lymphoma vs DLBCL
Lim et al, JCO, 2005
Pre-HAART HAART era
M-BACOD/
CHOP like: 90%;
CR: 35%
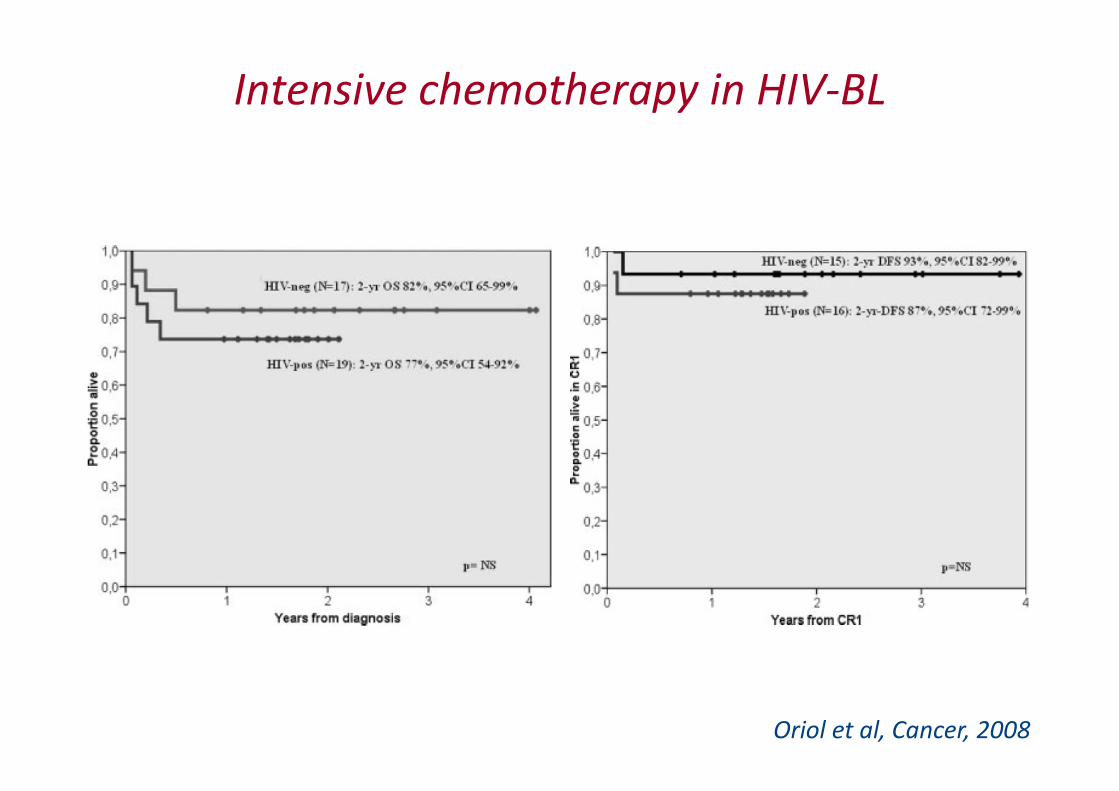
Intensive chemotherapy in HIV-BL
Oriol et al, Cancer, 2008
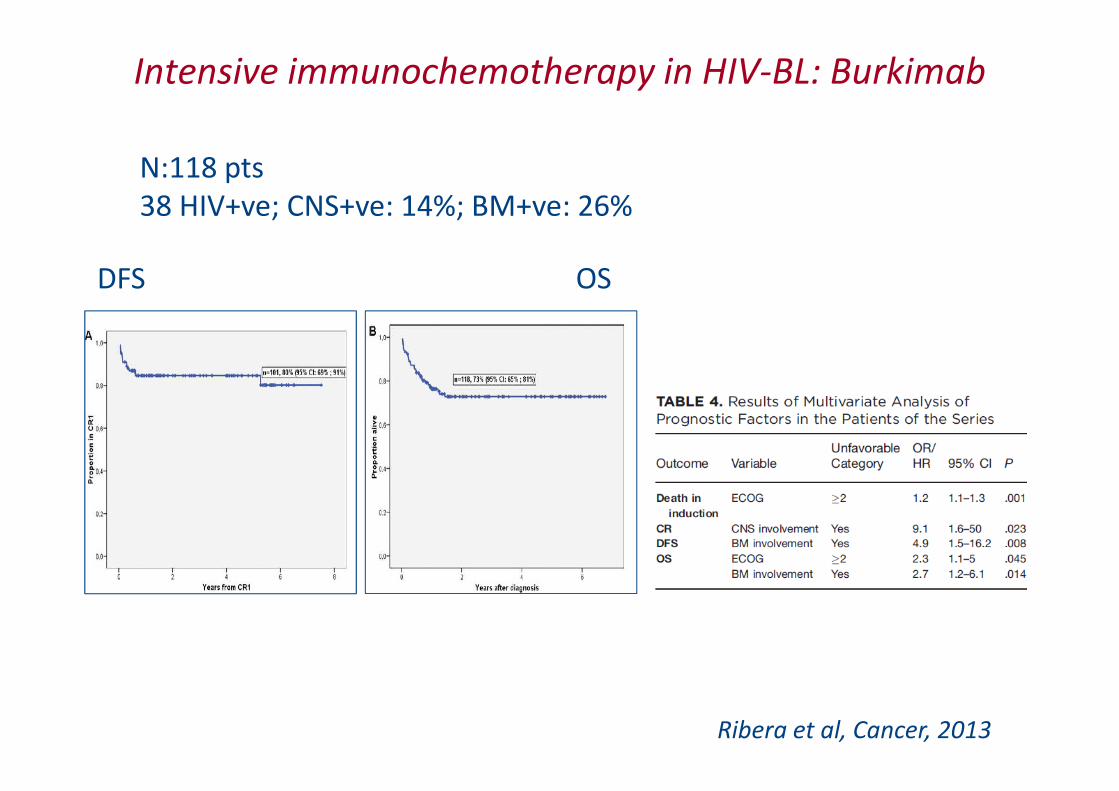
Intensive immunochemotherapy in HIV-BL: Burkimab
N:118 pts
38 HIV+ve; CNS+ve: 14%; BM+ve: 26%
Ribera et al, Cancer, 2013
DFS OS
Treatment of ARL: controversial points
• With/without HAART
• Infusional regimens vs ‘conventional’ regimens
• With/without rituximab
• Salvage therapy
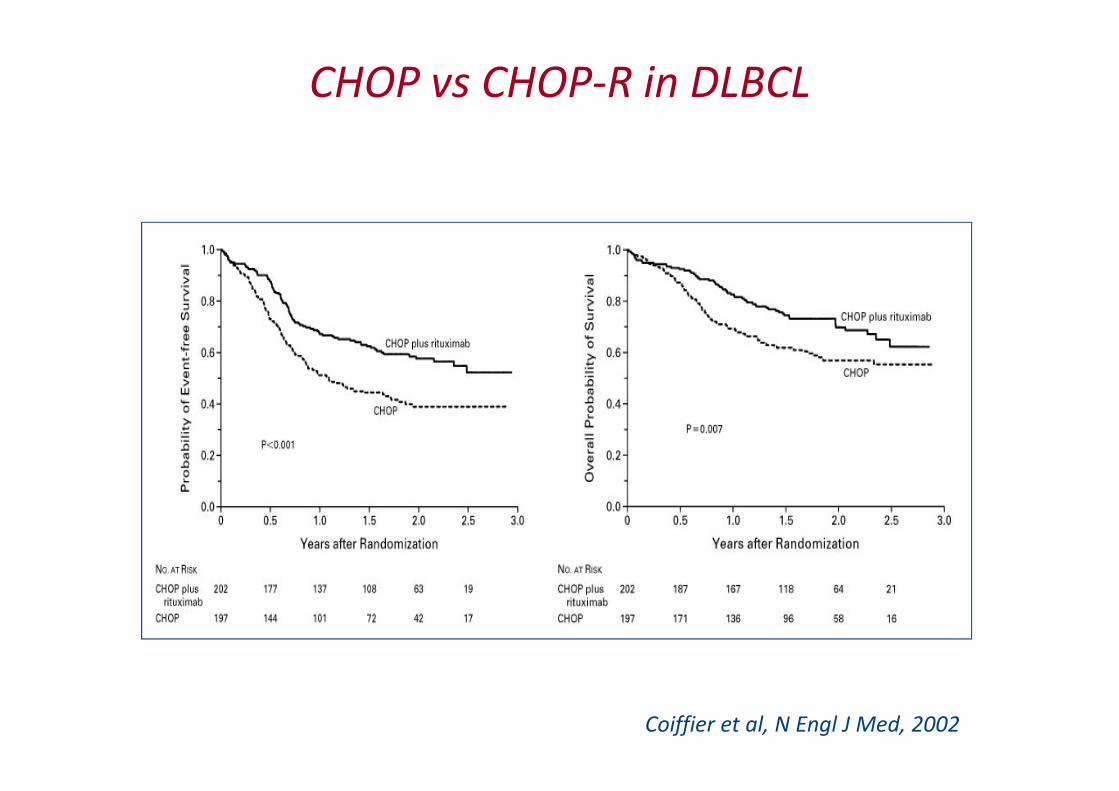
CHOP vs CHOP-R in DLBCL
Coiffier et al, N Engl J Med, 2002

CHOP-R vs CHOP
• Randomised• N: 150• 80% DLBCL• CHOP-R x 6 + rituximab x 3• HAART, G-CSF
• CR/CRu rate: 58 vs 47%• Disease progression: 8 vs 22%
Kaplan et al, Blood, 2005
NS when CD4< 50
excl
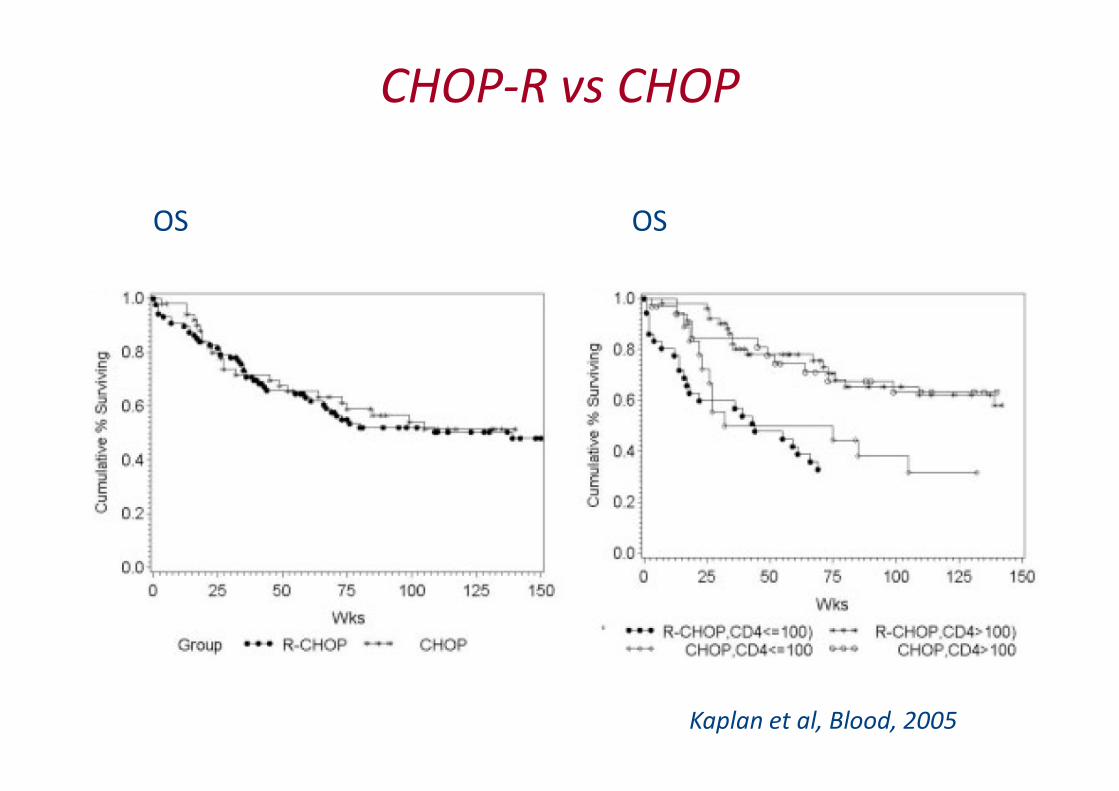
CHOP-R vs CHOP
Kaplan et al, Blood, 2005
OS OS

R-chemo vs chemo followed by R
Sparano et al, Blood, 2010
R-EPOCH vs EPOCH + 6 weekly doses of R

R-CHOP for DLBCL according to HIV status
Coutinho et al, AIDS, 2010
Treatment of ARL: controversial points
• With/without HAART
• Infusional regimens vs ‘conventional’ regimens
• With/without rituximab
• Salvage therapy
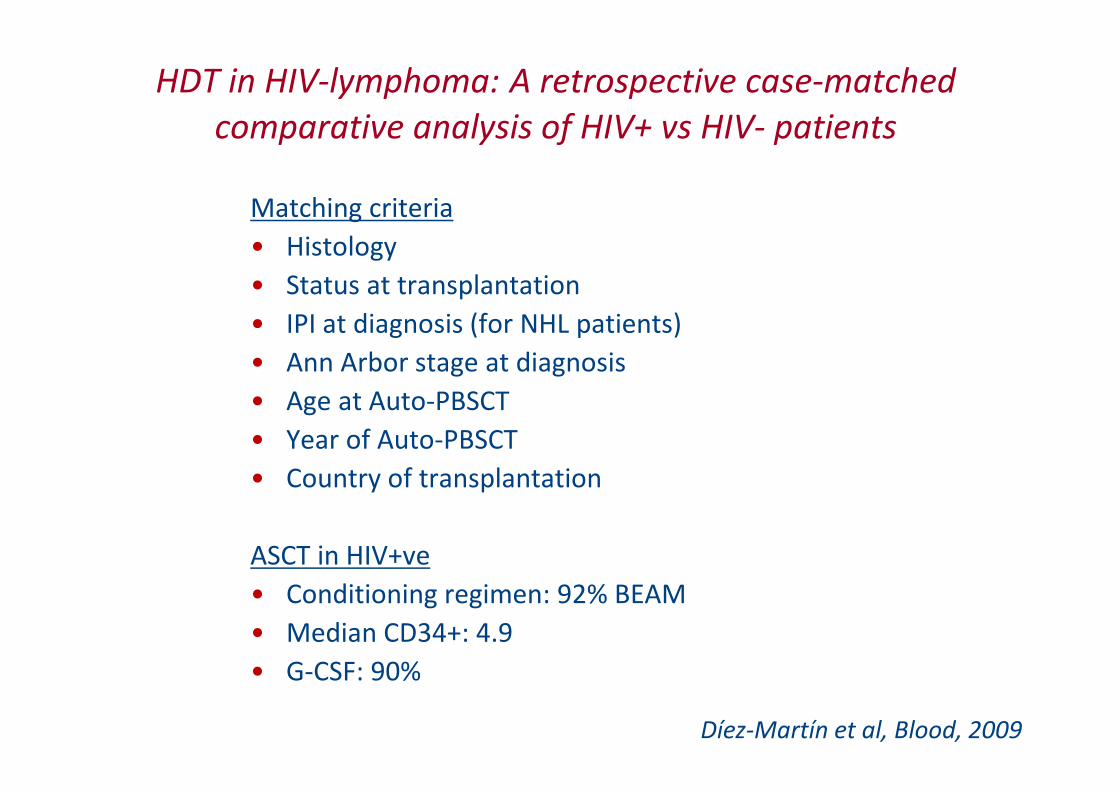
HDT in HIV-lymphoma: A retrospective case-matched
comparative analysis of HIV+ vs HIV- patients
Matching criteria
• Histology
• Status at transplantation
• IPI at diagnosis (for NHL patients)
• Ann Arbor stage at diagnosis
• Age at Auto-PBSCT
• Year of Auto-PBSCT
• Country of transplantation
ASCT in HIV+ve
• Conditioning regimen: 92% BEAM
• Median CD34+: 4.9
• G-CSF: 90%
Díez-Martín et al, Blood, 2009

HDT in HIV-lymphoma: EBMT study
Díez-Martín et al, Blood, 2009

ConclusionTreat HIV-lymphoma as lymphoma in HIV-ve
BUT….
Remember:
• Work with HIV team
• Patients must be on HAART
– Avoid PI if possible
• Prophylactic antibiotics:
– Septrin (or pentamidine)
– Fluconazole
– Azythromycine
– Acyclovir

Thank you!
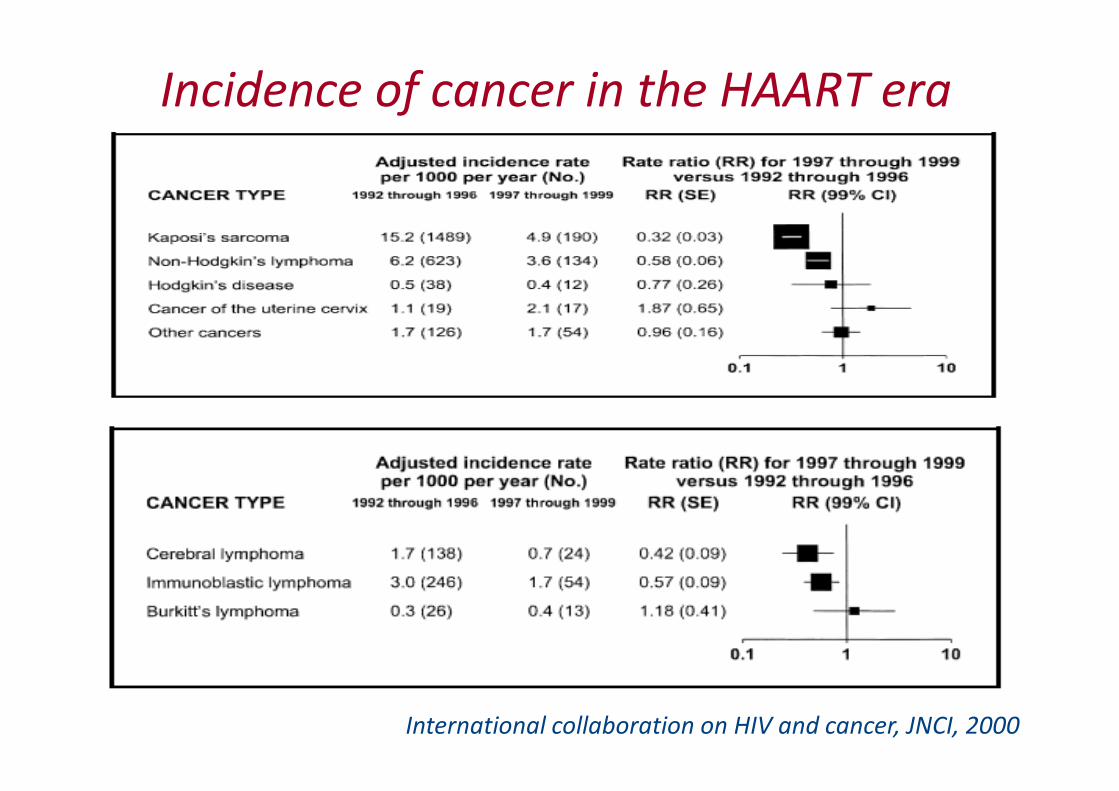
Incidence of cancer in the HAART era
International collaboration on HIV and cancer, JNCI, 2000
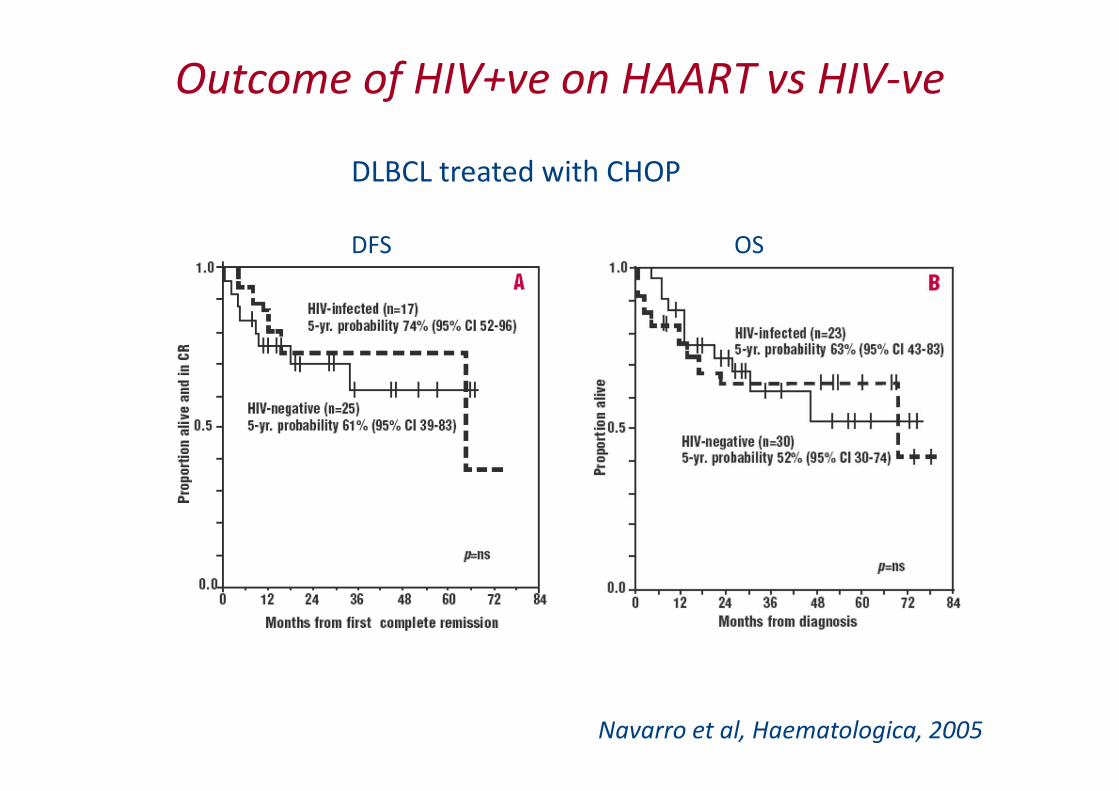
Outcome of HIV+ve on HAART vs HIV-ve
DLBCL treated with CHOP
DFS OS
Navarro et al, Haematologica, 2005

Non-randomised R-CHOP vs R-EPOCH
Barta et al, Cancer, 2011
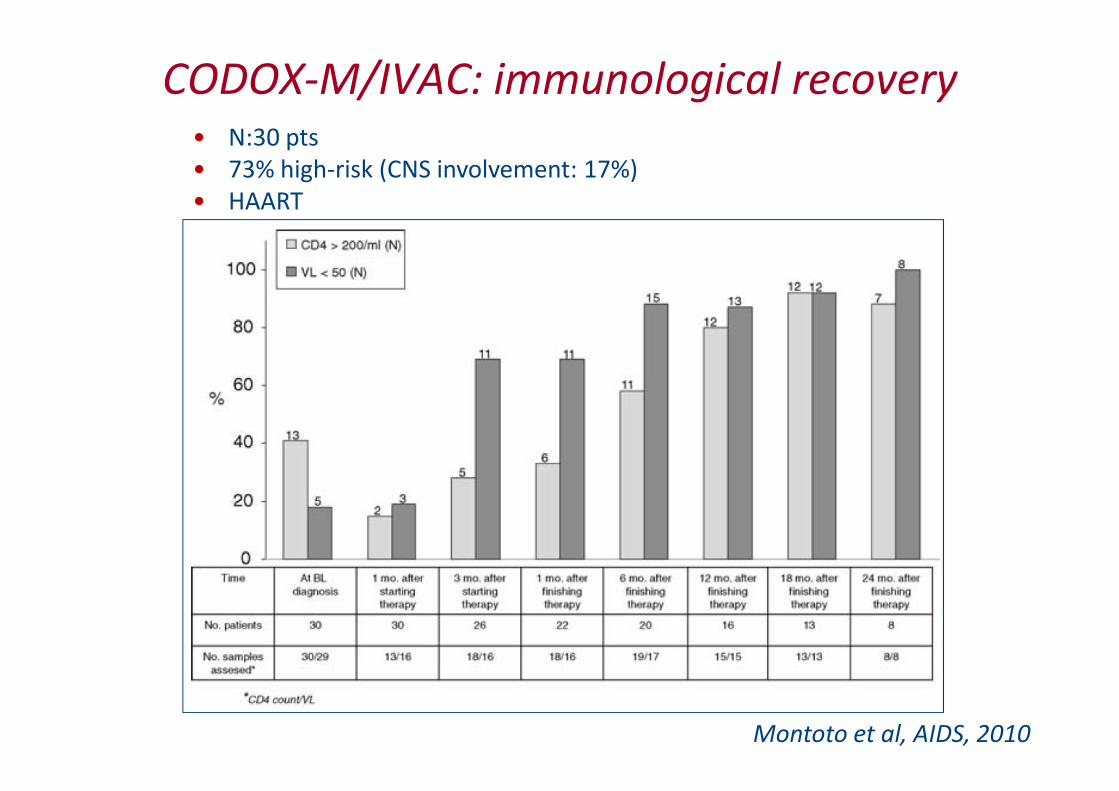
CODOX-M/IVAC: immunological recovery
Montoto et al, AIDS, 2010
• N:30 pts
• 73% high-risk (CNS involvement: 17%)
• HAART
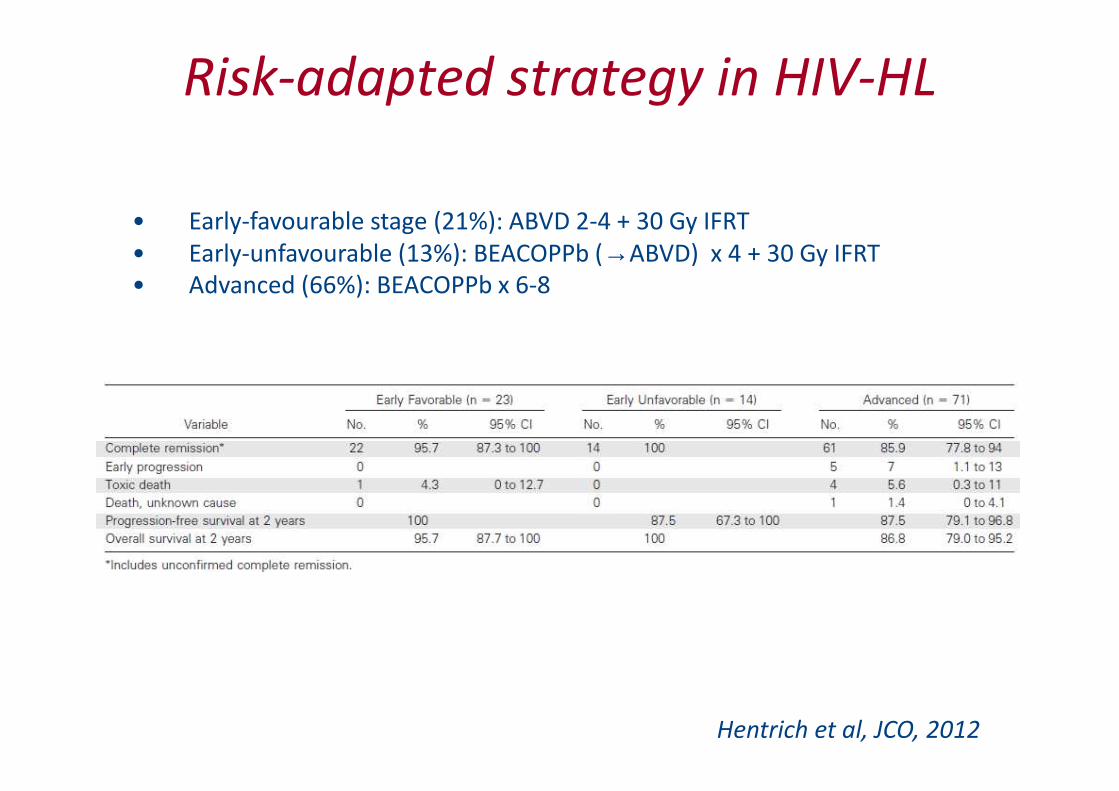
Risk-adapted strategy in HIV-HL
• Early-favourable stage (21%): ABVD 2-4 + 30 Gy IFRT
• Early-unfavourable (13%): BEACOPPb (→ABVD) x 4 + 30 Gy IFRT
• Advanced (66%): BEACOPPb x 6-8
Hentrich et al, JCO, 2012

Risk-adapted strategy in HIV-HL
Stage (N) ‘Under-treated’ ‘Over-treated’
Early-favourable (23) 7 4
Early-unfavourable (14) 6 2
Advanced (71) 6 0
Hentrich et al, JCO, 2012

Infusional chemotherapy in HIV-BL: SC-EPOCH-R
Dunleavy et al, N Engl J Med, 2013
N=11
BM+ve: 9%
CNS+ve: 0
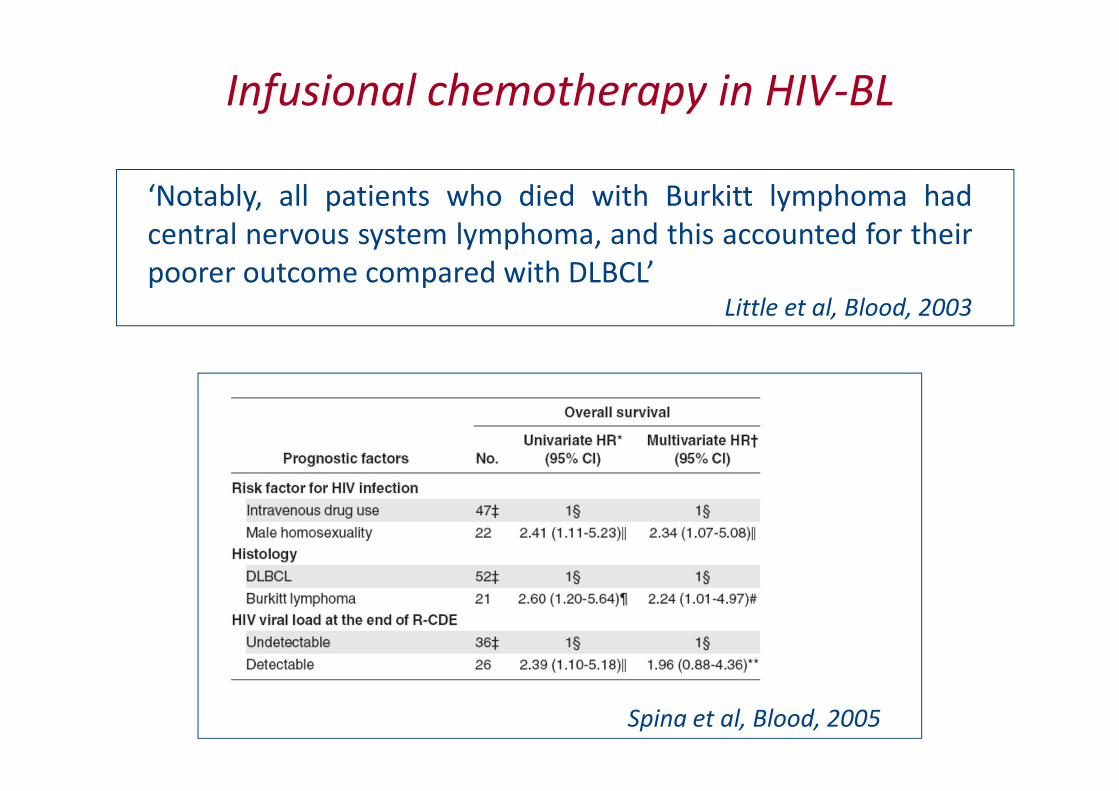
Infusional chemotherapy in HIV-BL
‘Notably, all patients who died with Burkitt lymphoma had
central nervous system lymphoma, and this accounted for their
poorer outcome compared with DLBCL’Little et al, Blood, 2003
Spina et al, Blood, 2005
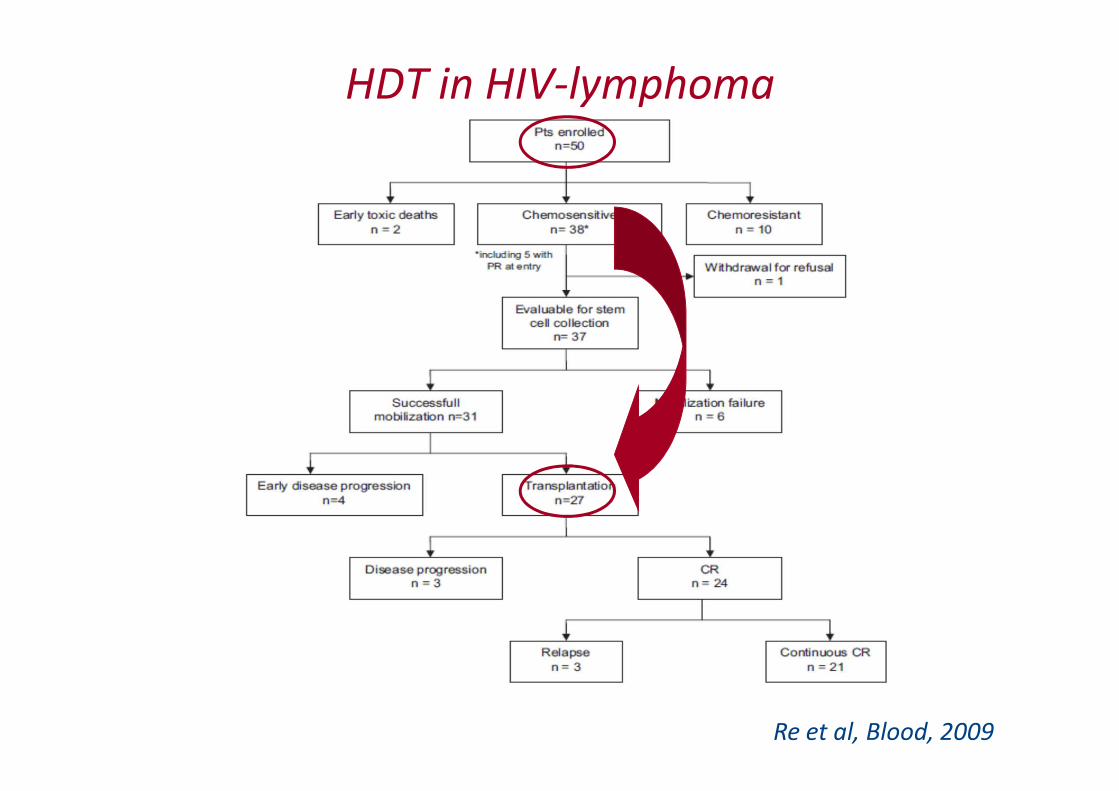
HDT in HIV-lymphoma
Re et al, Blood, 2009

HDT in HIV-ve + DLBCL: CORAL study
Gisselbrecht et al, JCO, 2010

Other lymphomas in patients
with HIV: HL

HL in HIV+
• B-symptoms
• Stage IV
• BM+ve
• MC/LD
• EBV+
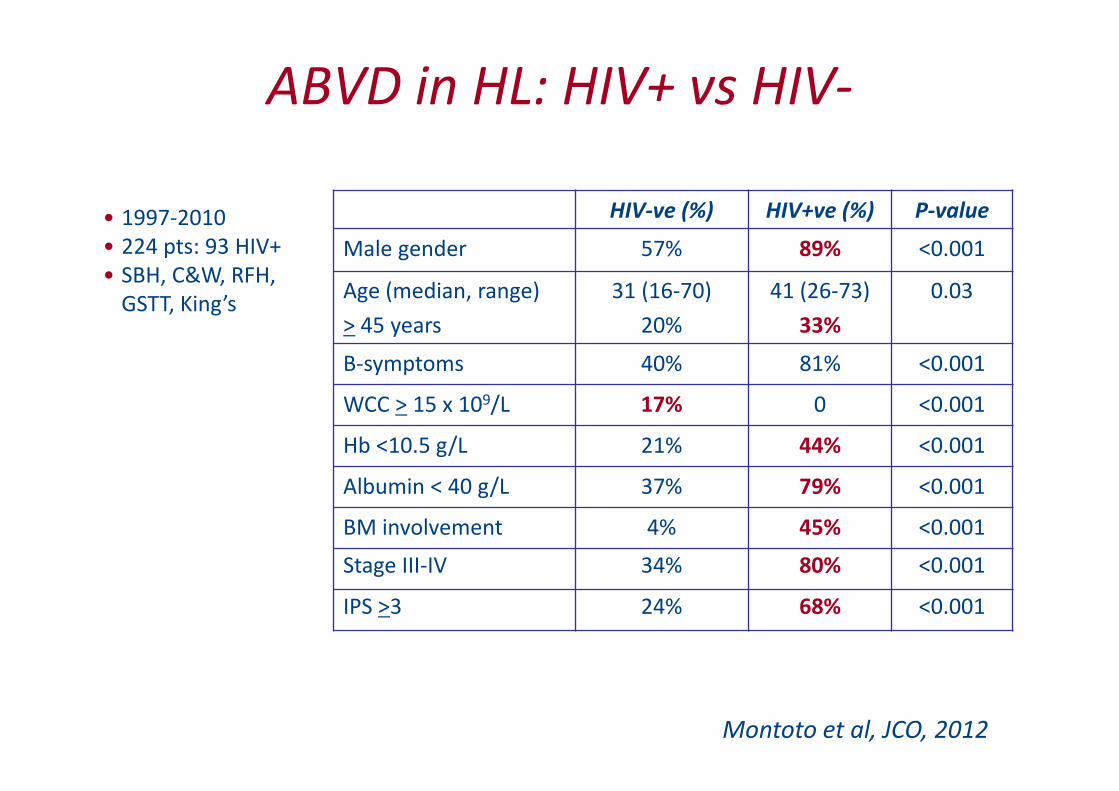
ABVD in HL: HIV+ vs HIV-
HIV-ve (%) HIV+ve (%) P-value
Male gender 57% 89% <0.001
Age (median, range)
> 45 years
31 (16-70)
20%
41 (26-73)
33%
0.03
B-symptoms 40% 81% <0.001
WCC > 15 x 109/L 17% 0 <0.001
Hb <10.5 g/L 21% 44% <0.001
Albumin < 40 g/L 37% 79% <0.001
BM involvement 4% 45% <0.001
Stage III-IV 34% 80% <0.001
IPS >3 24% 68% <0.001
Montoto et al, JCO, 2012
• 1997-2010
• 224 pts: 93 HIV+
• SBH, C&W, RFH,
GSTT, King’s

ABVD in HL: HIV+ vs HIV-
Montoto et al, JCO, 2012
EFS OS
Multivariate analysis DFS EFS OS
IPS
0-2 vs 3-7 0.9 0.15 0.09
HIV status
-ve vs +ve 0.5 0.9 0.6





























