Embed Size (px)
Citation preview

J. Comp. Path. 2012, Vol. -, 1e5 Available online at www.sciencedirect.com
www.elsevier.com/locate/jcpa
SPONTANEOUSLY ARISING DISEASE
Lymphocytic Hypophysitis in a Dog with DiabetesInsipidus
Cor
002
doi
Pl
(2
B. P. Meij*, G. Voorhout†, R. J. Gerritsen‡, G. C. M. Grinwisx and J. Ijzerx
*Department of Clinical Sciences of Companion Animals, †Division of Diagnostic Imaging, Faculty of Veterinary Medicine,
Utrecht University, Yalelaan 110, 3508 TD Utrecht, ‡De Kompaan e Specialistengroep Gezelschapsdieren, Van
Reeuwijkstraat 34, 7731 EH Ommen and xDepartment of Pathobiology, Faculty of Veterinary Medicine, Utrecht University,
Yalelaan 1, 3584 CL Utrecht, The Netherlands
resp
1-99
:10.1
ease
012
Summary
An 8-year-oldmale German longhaired pointer was referred for diabetes insipidus responsive to treatment withdesmopressin. The dog had polyuria and polydipsia, exercise intolerance and a dull hair coat. Plasma concen-trations of thyroid-stimulating hormone, thyroxine, growth hormone (GH) and insulin-like growth factor-1were decreased; plasma adrenocorticotropic hormone (ACTH) was slightly elevated and plasma a-melano-cyte-stimulating hormone (MSH) was within the reference range. Computed tomography revealed a heteroge-neously contrast-enhancing pituitary mass compressing the hypothalamus. Transsphenoidal hypophysectomywas performed and microscopical examination of the surgical biopsy samples revealed hypophysitis withoutevidence of pituitary adenoma. The hypophysitis was characterized by marked lymphocytic infiltration ofthe adenohypophysis that contained a mixed population of neuroendocrine cells expressing GH, ACTH ora-MSH. The lymphocytes were identified as T cells, resulting in a final diagnosis of lymphocytic hypophysitisstrongly resembling human primary lymphocytic hypophysitis.
� 2012 Elsevier Ltd. All rights reserved.
Keywords: diabetes insipidus; dog; hypophysitis; pituitary
Pituitary masses occur frequently in dogs and are al-most always pituitary adenomas (De Bruin et al.,2009; Meij et al., 2010). The most commonly encoun-tered adenoma is the pituitary corticotroph adenomathat causes excess secretion of adrenocorticotropichormone (ACTH) and results in pituitary-dependent hypercortisolism (Cushing’s-like disease)(Hanson et al., 2005). The pituitary somatotroph ad-enoma causes hypersecretion of growth hormone(GH) and results in acromegaly, but is rare in dogs(Fracassi et al., 2007). Clinically non-functional pitu-itary adenomas do not cause an endocrine syndrome,but may result in neurological signs or diabetes insip-idus due to expansion and compression of surround-ing brain structures (Th�eon and Feldman, 1998).Treatment of pituitary masses in dogs involves con-tainment of hormone excess by medical management
ondence to: B. P. Meij (e-mail: [email protected]).
75/$ - see front matter
016/j.jcpa.2012.04.006
cite this article in press as: Meij BP, et al., Lymphocytic Hypophysi
), doi:10.1016/j.jcpa.2012.04.006
or by hypophysectomy or irradiation aimed at com-pletely removing or reducing the pituitary mass.
An 8-year-old male German longhaired pointerwas referred with a history of acute onset polydipsiaand polyuria. Over a period of 1 week the dog hadstarted drinking five times the normal amount. Inthe second week the dog became depressed and devel-oped exercise intolerance. Urine examination re-vealed a specific gravity of 1.006. Kidney, liver,pancreas and muscle serum biochemistry panelswere normal. Ultrasonography of the abdomenshowed normal left and right adrenal glands. Thedog was treated with the vasopressin analogue desmo-pressin (Minrin 0.01%; Ferring B.V., Hoofddorp,The Netherlands; 8 mg q12h administered into theconjunctival sac). The dog responded immediatelywith normalization of drinking and urination.Central diabetes insipidus was suspected and com-puted tomography (CT) of the skull was performed.
� 2012 Elsevier Ltd. All rights reserved.
tis in a Dog with Diabetes Insipidus, Journal of Comparative Pathology

2 B.P. Meij et al.
Contrast-enhanced CT (Van der Vlugt-Meijeret al., 2002) revealed a heterogeneously enhancing pi-tuitary mass measuring 12.3 mm in height, 17.5 mmin width and 15.0 mm in length, consistent with a pi-tuitary tumour. The pituitary height/brain area ratio(P/B) was 0.75, indicating pituitary enlargement (ref-erence P/B <0.31; Kooistra et al., 1997). AbdominalCT scans showed normal adrenal glands.
Plasma levels of pituitary hormones and their tar-get hormones were assessed. Plasma concentrationsof thyroid-stimulating hormone (TSH) and thyroxine(Kooistra et al., 2000), and GH and insulin-likegrowth factor-1 (IGF-1) (Fracassi et al., 2007) weredecreased (Table 1), indicating hypopituitarism, sec-ondary hypothyroidism and hyposomatotropism.The pituitaryeadrenocortical system was further in-vestigated by measuring plasma concentrations ofACTH and a-melanocyte-stimulating hormone(MSH) by methods described previously (Hansonet al., 2006). The basal plasma concentration ofACTH was elevated and that of a-MSH was withinthe reference range (Table 1).
The dog continued to become more depressed andlethargic and the owner elected debulking pituitarysurgery. The dog underwent transsphenoidal hy-pophysectomy (Meij et al., 1997). The ventral surfaceof the pituitary mass was visualized through the sphe-noid slot and was dark red in colour. The dura materwas incised and the pituitary mass was extracted infour fragments (3 � 5 mm each; specimen 1). Therewas more than average diffuse haemorrhage fromthe pituitary tissue itself in comparison with pituitaryadenoma surgery. Haemostasis was accomplishedwith thrombin gel foam. After debulking, the dorsumsellae was located caudally in the sphenoid slot andthe pituitary fossa was inspected for remnant pituitarytissue, but it was difficult to assess complete removal ofthe pituitary mass since diffuse haemorrhage pre-vented an unobstructed view of the ventral hypotha-
Table 1
Plasma hormone concentrations
Hormones Values Reference values
TSH (mg/l) <0.03 <0.6*
T4 (total T4) (nmol/l) <9 13e61*
GH (mg/l) 1.7 2e5†
IGF-1 (mg/l) 71 137e425†
ACTH (pmol/l) 40.6 2.2e19.8‡
a-MSH (pmol/l) 7.8 1.5e15‡
Basal plasma concentrations of ACTH, a-MSH, GH and IGF-1 aremeans calculated from two values and the values are in SI units. Ref-
erence values:*Kooistra et al.(2000).†Fracassi et al. (2007).‡Mol and Meij (2008).
Please cite this article in press as: Meij BP, et al., Lymphocytic Hypophysi
(2012), doi:10.1016/j.jcpa.2012.04.006
lamic surface. At the end of the procedure, a smallwhite unaffected tissue fragment (8 � 5 mm) was col-lected separately from the caudal part of the pituitaryfossa (specimen 2). Both specimens were fixed in 10%neutral buffered formalin.
Recovery from surgery in the intensive care unitwas complicated. The dog remained stuporous anddid not respond to external stimuli except for deeppain stimuli. The dog’s respiration was normal andplasma sodium and potassium, central venous pres-sure and arterial blood gasses were within referenceranges. It was suspected that there was brain oedemadue to the removal of the pituitary mass and subse-quent brain shift and/or surgically inflicted hypotha-lamic damage. Repeated intravenous mannitolinfusions (0.5 g/kg) did not lead to clinical improve-ment. After 3 days of intensive care treatment theowner elected for humane destruction. Necropsy ex-amination was not permitted.
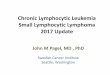
Specimens 1 and 2 were processed routinely andembedded in paraffin wax. Sections (3 mm) werestained with haematoxylin and eosin (HE). Micro-scopical examination of specimen 1 revealed severalgroups of chromophobic, acidophilic and basophilicneuroendocrine cells in a well-vascularized oedema-tous stroma with multifocal haemorrhage and a mod-erate multifocal lymphocytic infiltrate (Fig. 1).Additionally, some plasma cells and scattered indi-vidual macrophages were present. In specimen 1 noneoplastic tissue was detected and specimen 2 con-sisted of cerebral white matter.
Immunohistochemistry (IHC)was performed on se-rial sections of specimen 1 with antibodies specific for
Fig. 1. Surgical biopsy sample removed during transsphenoidalhypophysectomy. The vascularized tissue is infiltrated bysmall cells (arrowheads) with scant cytoplasm and a darknucleus, consistent with lymphocytes. There is local infil-tration with plasma cells and there are few pre-existing ac-idophilic neuroendocrine cells (arrow). HE. Bar, 100 mm.
tis in a Dog with Diabetes Insipidus, Journal of Comparative Pathology

Table 2
Antibodies used for IHC
Antibody Type Dilution Code Source Reference
Anti-synthetic
ACTH1-24
Monoclonal mouse 1 in 100 e UU Diaz Espi~neira et al. (2008)
Anti-synthetic
human a-MSH
Polyclonal rabbit 1 in 600 PU060-UP Biogenex Laboratories,
San Ramon, California, USA
Meij et al. (1997)
Anti-porcine GH Polyclonal porcine 1 in 5000 4750e3959 Biogenesis Ltd., Poole, Dorset, UK Diaz Espi~neira et al. (2008)
Anti-CD3 Polyclonal rabbit 1 in 300 A0452 Dako Cytomation, Glostrup,Denmark
Mekonnen et al. (2007)
Anti-CD79 Monoclonal mouse 1 in 50 M7051 Dako Cytomation Mahapokai et al. (2001)
UU: Utrecht University, Faculty of Veterinary Medicine, Department of Infectious Diseases and Immunology.
Lymphocytic Hypophysitis in a Dog 3
ACTH1-24, a-MSH, GH, the T-cell marker CD3 andthe B-cell marker CD79 (Table 2). Normal canine pi-tuitary tissue served as control tissue for ACTH,a-MSH and GH, while for CD3 and CD79 sectionsof a normal canine lymph node were used. For all an-tibodies, the negative control consisted of omission ofthe primary antibody. a-MSH labelling was negative,while individual cells expressed GH (Fig. 2) andACTH (Fig. 3) with a GH:ACTH ratio of 5:1. Thepopulation of lymphocytes in specimen 1 expressedCD3 (Fig. 4), but not CD79. Based on these findings,specimen 1 was identified as pre-existent adenohy-pophyseal tissue with a moderate to severe infiltrationof T lymphocytes. The microscopical lesions were con-sistent with lymphocytic hypophysitis. No neoplasticchanges were encountered in either specimen.
Lymphocytic hypophysitis in man is a neuroendo-crine disorder characterized by autoimmune inflam-mation of the pituitary gland with various degrees ofpituitary dysfunction (Rivera, 2006). It occurs mainlyinwomen during pregnancy or the postpartum period,although there are also reported cases in men(Couldwell and Weiss, 1999). The disorder is an
Fig. 2. Intracytoplasmic expression of GH (brown) in dispersedneuroendocrine cells. IHC. Bar, 100 mm.
Please cite this article in press as: Meij BP, et al., Lymphocytic Hypophysi
(2012), doi:10.1016/j.jcpa.2012.04.006
important differential diagnosis when space-occupying lesions of the sellar region are encountered.Lymphocytic hypophysitis may present as endocrinedysfunction and a diffuse mass, which can mimica non-functional pituitary tumour. The adenohypoph-ysis is heavily infiltrated by T lymphocytes and plasmacells (Saeger, 2001). During the acute inflammatoryphase, the pituitary gland may be markedly enlargedwith suprasellar extension. During the chronic phase,the pituitary becomes atrophic due to replacement ofadenohypophyseal tissue with connective tissue(Thapar and Kovacs, 1998; Stefaneanu et al., 2000).Microscopically, three main morphological subtypesof primary hypophysitis can be discerned, lympho-cytic, granulomatous and xanthomatous, but it is un-clear whether these are truly distinct entities orrepresent different stages of the same disease.
The type, phase and degree of lymphocytic infiltra-tion determine the clinical symptoms in human pa-tients. Marked lymphocytic infiltration disrupts thearchitecture of the adenohypophysis leading to pitui-tary insufficiency. Most frequently, diabetes insipidus,hypopituitarism, headache and visual defects are re-ported (Rivera, 2006). In the case of inflammation ofthe anterior part of the pituitary only, the lesion istermed lymphocytic adenohypophysitis, when the pos-terior lobe and the infundibulum are affected it iscalled lymphocytic infundibuloneurohypophysitis,and if there is a global infiltration of the pituitary glandit is called lymphocytic panhypophysitis. Lymphocyticinfundibuloneurohypophysitis typically presents asacute onset diabetes insipidus with intracranial mass-effect symptoms (Abe, 2008) and resembles the courseof the disease in the present case. Radiological differen-tiation from neoplasia is impossible (Schubiger, 1996).Pituitary magnetic resonance imaging in people withlymphocytic hypophysitis presenting with diabetes in-sipidus shows loss of the ‘bright spot’ of the posteriorlobe, thickening of the pituitary stalk and pituitarygland enlargement with suprasellar extension(Shimono et al., 1999; Akahori and Sugimoto, 2010).
tis in a Dog with Diabetes Insipidus, Journal of Comparative Pathology

Fig. 3. Intracytoplasmic expression of ACTH (brown) in an indi-vidual neuroendocrine cell (arrow) surrounded by lym-phocytes (arrowheads). IHC. Bar, 100 mm.
4 B.P. Meij et al.
After treatment with glucocorticoids, the pituitary re-duces in size (Akahori and Sugimoto, 2010). Pituitaryinsufficiency may affect all pituitary hormones, butnormal and elevated plasma levels have also been re-ported, probably representing different stages of thedisease (Shimono et al., 1999). Indeed, in the presentcase there was reduced TSH and GH, but normal toelevated a-MSH and ACTH concentrations. The im-portance of recognizing lymphocytic hypophysitis isthat it may be self-limiting and respond to medicalanti-inflammatory treatment with glucocorticoids.
In the present case, lymphocytic hypophysitis wasdiagnosed by histopathological examination of surgi-cal biopsies. The uniform cellular appearance of thelymphocytes and the simultaneous presence of fewother inflammatory cells (plasma cells and macro-phages) were consistent with an inflammatory reac-tion rather than lymphoma. No other evidence of
Fig. 4. Immunohistochemical labelling for theT-cellmarkerCD3.Bar, 100 mm.
Please cite this article in press as: Meij BP, et al., Lymphocytic Hypophysi
(2012), doi:10.1016/j.jcpa.2012.04.006
lymphoma was found in this dog and primary pitui-tary lymphoma has not been reported in the litera-ture. The suprasellar expansion of pituitaryadenomas in dogs primarily affects the hypothalamus,which contains the supraoptic and paraventricularnuclei where vasopressin is synthesized. In pituitarymasses with suprasellar expansion, these nuclei maybecome compromised, possibly leading to diabetes in-sipidus. This may also occur after hypophysectomy(Hanson et al., 2005, 2007). Plasma ACTH concen-tration was moderately elevated in the present case,which may be a reflection of the acute systemic in-flammatory phase of the disease before destructionof the adenohypophysis leads to complete pituitary in-sufficiency. In a recent case report in a 4.5-year-oldgreat Pyrenees dog with hypothyroidism and hypoa-drenocorticism, lymphocytic adenohypophysitis andadrenalitis were found. B lymphocytes and plasmacells dominated the adenohypophysitis, but T cellsdominated the adrenalitis (Adissu et al., 2010). Inthat dog the pituitary gland was slightly enlargedand the adrenal and thyroid glands were bilaterallyatrophic. This combination of primary hypothyroid-ism and hypoadrenocorticism resembled type II auto-immune polyendocrine syndrome or Schmidtsyndrome in man (Adissu et al., 2010). In the presentcase the adrenal glands were of normal size on ultra-sonography, the pituitary gland was markedly en-larged and the thyroid gland, although less active,still showed some hormonal activity. Moreover, thedominant T-cell infiltration of the pituitary gland ofthe present case represents a distinct difference com-pared with the inflammation of the pituitary glandof the great Pyrenees dog and suggests that inflamma-tion in the present case had an underlying diseasemechanism more comparable with human lympho-cytic hypophysitis. Lymphocytic adenohypophysitisin the dog may therefore reveal different histopatho-logical patterns and lead to variants in clinical presen-tation.
In dogs with pituitary masses that are not associ-ated with an endocrine syndrome (Cushing’s-like dis-ease or acromegaly), a histological biopsy of thepituitary mass is necessary to differentiate betweennon-functional pituitary adenoma and lymphocytichypophysitis. In non-functional adenoma, treatmentis aimed at cytoreduction with pituitary surgery or ra-diotherapy, while in lymphocytic hypophysitis thetreatment of choice is medical intervention with glu-cocorticoids.
References
Abe T (2008) Lymphocytic infundibuloneurohypophysitisand infundibulopanhypophysitis regarded as
tis in a Dog with Diabetes Insipidus, Journal of Comparative Pathology

Lymphocytic Hypophysitis in a Dog 5
lymphocytic hypophysitis variant. Brain Tumour Pathol-
ogy, 25, 59e66.AdissuHA,Hamel-JoletteA,FosterRA (2010)Lymphocytic
adenohypophysitis and adrenalitis in a dog with adrenaland thyroid atrophy. Veterinary Pathology, 47, 1082e1085.
Akahori H, Sugimoto T (2010) Lymphocytic hypophysitiswith a long latent period from onset of central diabetesinsipidus to development of pituitary enlargement. Inter-nal Medicine, 49, 1565e1571.
Couldwell WT, Weiss MH (1999) Nonadenomatous le-sions of the pituitary. In: Pituitary Disorders. Comprehen-
sive Management, AF Krisht, GT Tindall, Eds.,Lippincott, Williams and Wilkins, Baltimore, pp.327e336.
De Bruin C, Meij BP, Kooistra HS, Hanson JM,Lamberts SW et al. (2009) Cushing’s disease in dogsand humans. Hormone Research, 71(Suppl. 1), 140e143.
Diaz Espi~neira MM, Mol JA, van den Ingh TSGAM, vander Vlugt-Meijer RH, Rijnberk A et al. (2008) Func-tional and morphological changes in the adenohypoph-ysis of dogs with induced primary hypothyroidism: lossof TSH hypersecretion, hypersomatotropism, hypopro-lactinemia, and pituitary enlargement with transdiffer-entiation. Domestic Animal Endocrinology, 35, 98e111.
Fracassi F, Gandini G, Diana A, Preziosi R, van denIngh TSGAM et al. (2007) Acromegaly due to a somato-troph adenoma in a dog. Domestic Animal Endocrinology,32, 43e54.
Hanson JM, Kooistra HS, Mol JA, Teske E, Meij BP(2006) Plasma profiles of adrenocorticotropic hormone,cortisol, alpha-melanocyte-stimulating hormone, andgrowth hormone in dogs with pituitary-dependent hy-peradrenocorticism before and after hypophysectomy.Journal of Endocrinology, 190, 601e609.
Hanson JM, Teske E, Voorhout G, Galac S, Kooistra HSet al. (2007) Prognostic factors for outcome aftertranssphenoidal hypophysectomy in dogs withpituitary-dependent hyperadrenocorticism. Journal of
Neurosurgery, 107, 830e840.Hanson JM, van ’t Hoofd MM, Voorhout G, Teske E,
Kooistra HS et al. (2005) Efficacy of transsphenoidal hy-pophysectomy in treatment of dogs with pituitary-dependent hyperadrenocorticism. Journal of Veterinary
Internal Medicine, 19, 687e694.Kooistra HS, Diaz-Espineira MM, Mol JA, van den
Brom WE, Rijnberk A (2000) Secretion pattern ofthyroid-stimulating hormone in dogs during euthyroid-ism and hypothyroidism. Domestic Animal Endocrinology,18, 19e29.
Kooistra HS, Voorhout G, Mol JA, Rijnberk A (1997) Cor-relation between impairment of glucocorticoid feedbackand the size of the pituitary gland in dogs withpituitary-dependent hyperadrenocorticism.Journal of En-docrinology, 152, 387e394.
Mahapokai W, van den Ingh TSGAM, van Mil F, vanGarderen E, Schalken JA et al. (2001) Immune response
Please cite this article in press as: Meij BP, et al., Lymphocytic Hypophysi
(2012), doi:10.1016/j.jcpa.2012.04.006
in hormonally-induced prostatic hyperplasia in the dog.Veterinary Immunology and Immunopathology, 78, 297e303.
Meij BP, Kooistra HS, Rijnberk A (2010) Hypothalamus-pituitary system. In: Clinical Endocrinology of Dogs and
Cats, 2nd Edit., A Rijnberk, HS Kooistra, Eds.,Schl€utersche, Hannover, pp. 13e54.
Meij BP, Voorhout G, Van den Ingh TS, Hazewinkel HA,Van’t Verlaat JW (1997) Transsphenoidal hypophysec-tomy in beagle dogs: evaluation of a microsurgical tech-nique. Veterinary Surgery, 26, 295e309.
Mekonnen GA, Ijzer J, Nederbragt H (2007) Tenascin-Cin chronic canine hepatitis: immunohistochemical local-ization and correlation with necro-inflammatory activ-ity, fibrotic stage, and expression of alpha-smoothmuscle actin, cytokeratin 7, and CD3+ cells. VeterinaryPathology, 44, 803e813.
Mol JA, Meij BP (2008) Pituitary function. In: Clinical Bio-chemistry of Domestic Animals, 6th Edit., JJ Kaneko,JW Harvey, ML Bruss, Eds., Academic Press, Amster-dam, pp. 561e604.
Rivera JA (2006) Lymphocytic hypophysitis: disease spec-trum and approach to diagnosis and therapy. Pituitary,9, 35e45.
Saeger W (2001) Tumor-like lesions of the sellar region. In:Diagnosis and Management of Pituitary Tumors, K Thapar,K Kovacs, BW Scheithauer, RV Lloyd, Eds., HumanaPress, Totowa, pp. 449e460.
Schubiger O (1996) Radiology of pituitary adenomas.In: Pituitary Adenomas, AM Landolt, ML Vance,PL Reilly, Eds., Churchill Livingstone, New York,pp. 177e219.
Shimono T, Yamaoka T, Nishimura K, Koshiyama H,Sakamoto M et al. (1999) Lymphocytic hypophysitispresenting with diabetes insipidus: MR findings. Euro-pean Radiology, 9, 1397e1400.
Stefaneanu L, Kovacs K, Horvath E, Scheithauer BW(2000) The adenohypophysis. In: Molecular and Cellular
Endocrine Pathology, L Stefaneanu, H Sasano,K Kovacs, Eds., Arnold, London, pp. 75e117.
ThaparK, Kovacs K (1998) Neoplasms of the sellar region.In: Russell and Rubinstein’s Pathology of Tumors of the Ner-
vous System, 6th Edit., DD Bigner, RE McLendon,JM Bruner, Eds., Arnold, London, pp. 561e677.
Th�eon AP, Feldman EC (1998)Megavoltage irradiation ofpituitary macrotumors in dogs with neurologic signs.Journal of the American Veterinary Medical Association,213, 225e231.
Van der Vlugt-Meijer RH, Voorhout G, Meij BP (2002)Imaging of the pituitary gland in dogs with pituitary-dependent hyperadrenocorticism. Molecular and Cellular
Endocrinology, 197, 81e87.
tis in a Dog with
½ R
A
D
eceived, February 23rd, 2012
ccepted, April 28th, 2012
iabetes Insipidus, Journal of Com
�
parative Pathology