Embed Size (px)
Citation preview
Images in Gynecologic Surgery
Lymphatic Spread of Endometriosis to Para-Aortic Nodes
Pedro F. Escobar, MD*From the Division of Gynecologic Oncology, Women’s Health Institute, Cleveland Clinic, Cleveland, Ohio, and HIMA Health, Caguas, Puerto Rico.
DISCUSS
Fig. 1
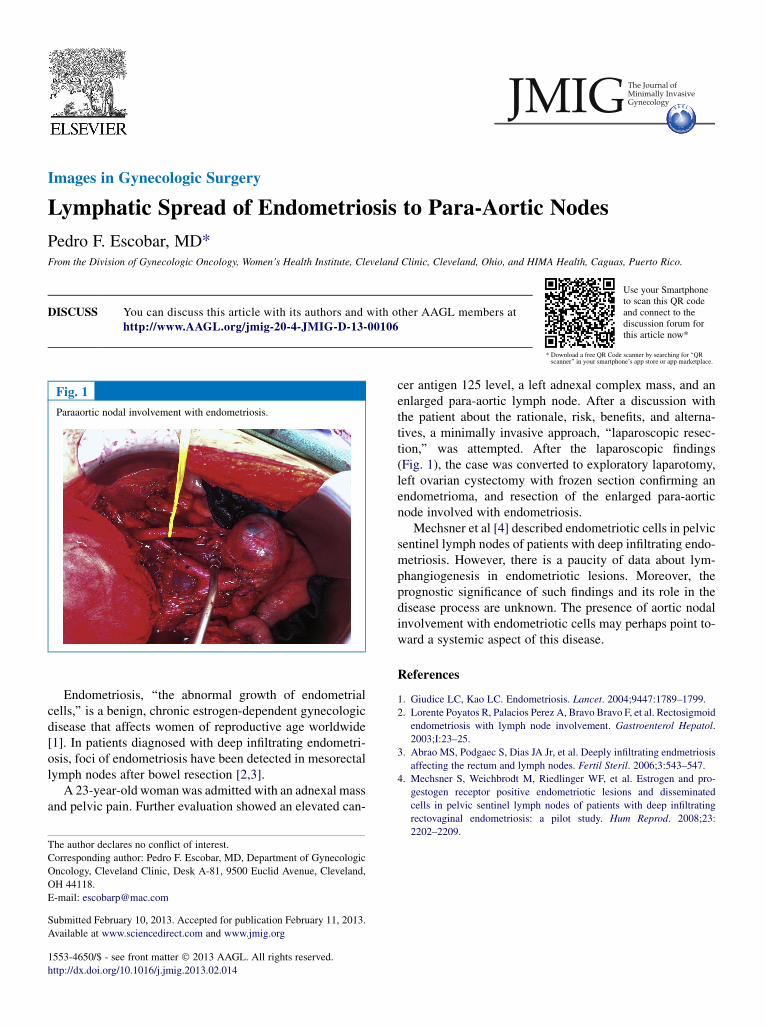
Paraaortic noda
The author decla
Corresponding au
Oncology, Clevel
OH 44118.
E-mail: escobarp
Submitted Februa
Available at www
1553-4650/$ - se
http://dx.doi.org/1
You can discuss this article with its authors and with other AAGL members athttp://www.AAGL.org/jmig-20-4-JMIG-D-13-00106
l involvement with endometriosis.
res no conflict of interest.
thor: Pedro F. Escobar, MD, Department of Gynecologic
and Clinic, Desk A-81, 9500 Euclid Avenue, Cleveland,
@mac.com
ry 10, 2013. Accepted for publication February 11, 2013.
.sciencedirect.com and www.jmig.org
e front matter � 2013 AAGL. All rights reserved.
0.1016/j.jmig.2013.02.014
Utoadth
se your Smartphonescan this QR code
nd connect to theiscussion forum foris article now*
* Download a free QR Code scanner by searching for ‘‘QRscanner’’ in your smartphone’s app store or app marketplace.
Endometriosis, ‘‘the abnormal growth of endometrialcells,’’ is a benign, chronic estrogen-dependent gynecologicdisease that affects women of reproductive age worldwide[1]. In patients diagnosed with deep infiltrating endometri-osis, foci of endometriosis have been detected in mesorectallymph nodes after bowel resection [2,3].
A 23-year-old woman was admitted with an adnexal massand pelvic pain. Further evaluation showed an elevated can-
cer antigen 125 level, a left adnexal complex mass, and anenlarged para-aortic lymph node. After a discussion withthe patient about the rationale, risk, benefits, and alterna-tives, a minimally invasive approach, ‘‘laparoscopic resec-tion,’’ was attempted. After the laparoscopic findings(Fig. 1), the case was converted to exploratory laparotomy,left ovarian cystectomy with frozen section confirming anendometrioma, and resection of the enlarged para-aorticnode involved with endometriosis.
Mechsner et al [4] described endometriotic cells in pelvicsentinel lymph nodes of patients with deep infiltrating endo-metriosis. However, there is a paucity of data about lym-phangiogenesis in endometriotic lesions. Moreover, theprognostic significance of such findings and its role in thedisease process are unknown. The presence of aortic nodalinvolvement with endometriotic cells may perhaps point to-ward a systemic aspect of this disease.
References
1. Giudice LC, Kao LC. Endometriosis. Lancet. 2004;9447:1789–1799.
2. Lorente Poyatos R, Palacios Perez A, Bravo Bravo F, et al. Rectosigmoid
endometriosis with lymph node involvement. Gastroenterol Hepatol.
2003;I:23–25.
3. Abrao MS, Podgaec S, Dias JA Jr, et al. Deeply infiltrating endmetriosis
affecting the rectum and lymph nodes. Fertil Steril. 2006;3:543–547.
4. Mechsner S, Weichbrodt M, Riedlinger WF, et al. Estrogen and pro-
gestogen receptor positive endometriotic lesions and disseminated
cells in pelvic sentinel lymph nodes of patients with deep infiltrating
rectovaginal endometriosis: a pilot study. Hum Reprod. 2008;23:
2202–2209.