Embed Size (px)
Citation preview
LYMPHANGIOMA OF THE TONGUE
By FRANK ROBINSON, B.Sc., M.B., F.R.C.S.
From Christie Hospital and Holt Radium Institute, Manchester
SIMPLE tumours of the tongue are comparatively rare, but diffuse lymphangioma is the most common cause of macroglossia and localised growths also occur. Both types of congenital origin are met with chiefly in childhood. Treatment is either by surgery or by radiation and variable results have been reported.
In this paper the pathology, clinical features, and treatment of lymphangioma as it occurs in the tongue are reviewed, an attempt being made to assess the relative place of surgery and radiation. One case of lymphangiomatous macroglossia is described in detail. It was treated by partial resection on two occasions, between which a course of radiation was given. The records of the four other patients treated in this hospital by radiation in the years i94o-51 were examined and these cases are reported briefly.
PATHOLOGY
Virchow (I854) showed that lymphangiomata arise from dilatation of lymphatic spaces. Ewing (I942) has further remarked that, being composed of lymph vessels, they consist of endothelial cells and supporting connective tissue, both of which take part in the neoplastic process. They arise in congenital lymphatic rests, which may not be entirely separate from normal lymph channels and in many cases there is evidence of true new formation of lymph vessels by endothelial proliferation, followed by canalisation. Secondary dilatation of the newly formed vessels later occurs and this process may be accelerated by the recurrent attacks of inflammation to which these turnouts are subject.
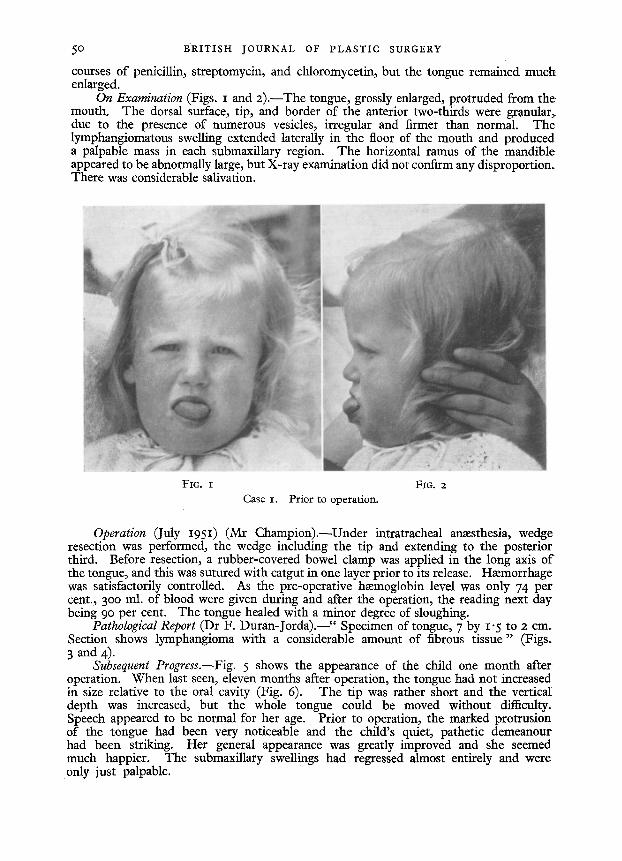
In the tongue they are usually cavernous in type, consisting of many com- municating spaces in a connective tissue stroma. Capillary tufts lie between these and may project into them. They are lined by one layer of endothelial cells. The stroma is variable in amount, partly depending upon the inflammatory changes which have occurred. There is also an infiltration with small round cells. The lymphatic spaces lie mainly in the subepithelial layer, but in the diffuse form may replace much of the muscle of the tongue. They may be found in the epithelium itself (Fig. 3) and when present in the papilla~ produce superficial vesicles on the surface of the tongue.
Their contents vary. Some contain coagulated lymph, some lymphocytes, and yet others red and white blood cells. These are thought to be the result of erosion of small blood-vessels which then rupture into the spaces rather than to be newly formed blood channels (Rigg and Waldapf~l, i94o).
48
LYMPHANGIOMA OF THE TONGUE 49
CLINICAL FEATURES
Lymphangiomata are usually present at birth or are noticed in the first few months of life. Further evidence of their congenital origin is their constant situation in the anterior two-thirds of the tongue, the part derived from the lateral tongue swellings and the tuberculum impar of the mandibular arches, and the frequent co-existence of other congenital abnormalities, e.g., h~emangioma, spina bifida, and cystic hygroma of the neck. This last condition was present in all three cases reported by Lierle (I944).
The tumour grows slowly or may remain quiescent for a considerable time, but after the deciduous teeth have appeared, or after puberty, it becomes subject to attacks of inflammation with considerable swelling, followed by remissions. Ulceration of the more superficial vesicles may occur, possibly with ha~morrhage. Each attack is followed by fibrosis with consequent enlargement, this inflammatory formation of connective tissue adding to its slow, regular formation as described by Ewing. Two types have been described: (I) the localised lymphatic n~evus or nodular lymphangioma ; (z) diffuse lymphangioma--lymphangiomatous macroglossia.
Both are found in the anterior portion of the tongue. The localised growth forms a nodular turnout usually elevated above the general surface. Its surface is irregular and granular, due to the presence of vesicles of varying size. Many are visible to the naked eye and may be as large as small peas. Their centres appear translucent, but as the vesicles are thick-walled these may be surrounded by an opaque ring. Characteristically, bright red spots are seen between and sometimes through the vesicles ; these are capillary tufts.
Diffuse lymphangioma may be unilateral, limited sharply by the median raphe, or more usually bilateral. In the very young child the affected part of the tongue is soft, but when it has become large enough to protrude from the mouth, particularly if inflammation has occurred, it becomes much firmer to the touch. The protruding portion becomes dried and may be fissured. The surface is granular with enlargement of the papillm. These may end in a club-shaped manner and contain a lymphatic space in the free end (Fitzwilliams, i927).
With great increase in size there is profuse salivation, and mastication may be affected. The horizontal ramus of the mandible is elongated and forms a more .obtuse angle than usual with the ascending ramus. The incisor and canine teeth project more horizontally than normal and are separated anteriorly when the molars are in contact. At this stage, hardly likely to be encountered at the present time, speech is affected.
CASE REPORTS
Case i .--Lymphangiomatous Maeroglossia.--P. B., a female child, was I9 months old when seen in May I95 r. She was born with a large tongue, and when 9 months old wedge resection had been performed with considerable reduction in its size.' It increased in size again with growth and began to protrude from the mouth. At x5 months of age radon seeds were implanted to a total dose of 3,ooo r. The tongue became very swollen indeed, and for the next few weeks there was intermittent pyrexia. It ~ 'was considered that a hmmatoma following the implant had become infected. There was bilateral submaxillary adenitis. The swelling eventually receded following
I D
5o B R I T I S H JOURNAL OF PLASTIC SURGERY
courses of penicillin, streptomycin, and chloromycetin, but the tongue remained muck enlarged.
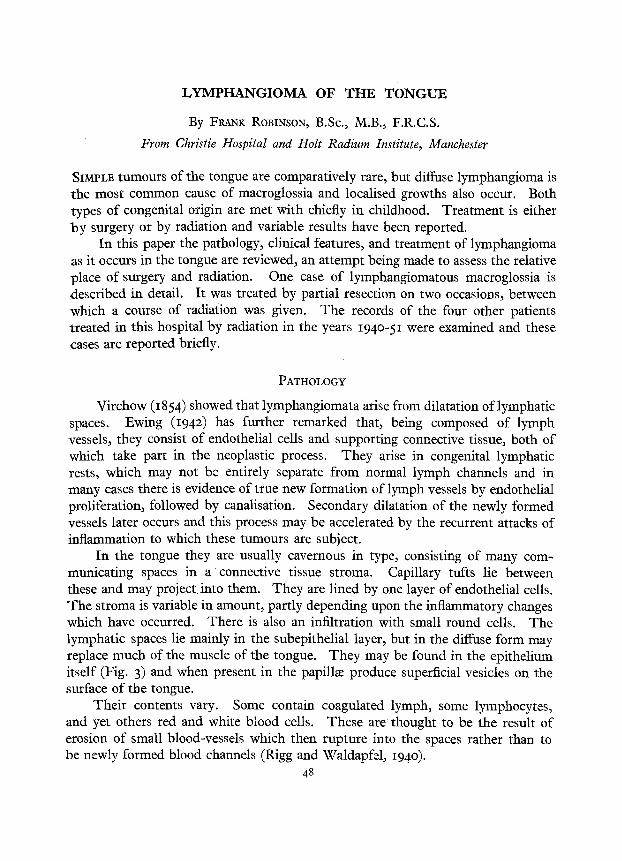
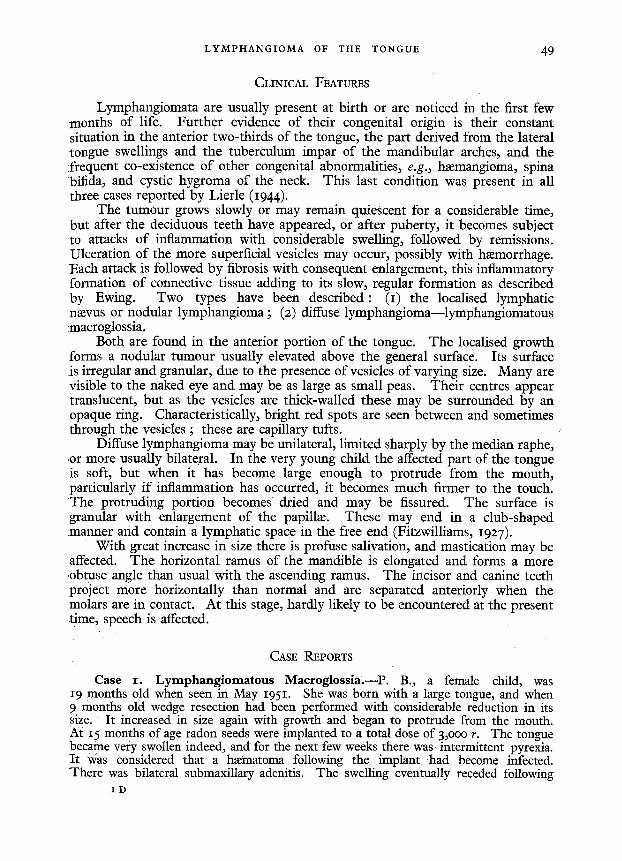
On Examination (Figs. I and 2).--The tongue, grossly enlarged, protruded from the. mouth. The dorsal surface, tip, and border of the anterior two-thirds were granular, due to the presence of numerous vesicles, irregular and firmer than normal. The lymphangiomatous swelling extended laterally in the floor of the mouth and produced a palpable mass in each submaxillary region. The horizontal ramus of the mandible appeared to be abnormally large, but X-ray examination did not confirm any disproportion~ There was considerable salivation.
FIG. I FIG. 2
Case I. Prior to operation.
Operation (July I95I) (Mr Champion).--Under intratracheal anmsthesia, wedge resection was performed, the wedge including the tip and extending to the posterior third. Before resection, a rubber-covered bowel clamp was applied in the long axis of the tongue, and this was sutured with catgut in one layer prior to its release. Hmmorrhage was satisfactorily controlled. As the pre-operative hmmoglobin level was only 74 per cent., 300 ml. of blood were given during and after the operation, the reading next day being 90 per cent. The tongue healed with a minor degree of sloughing.
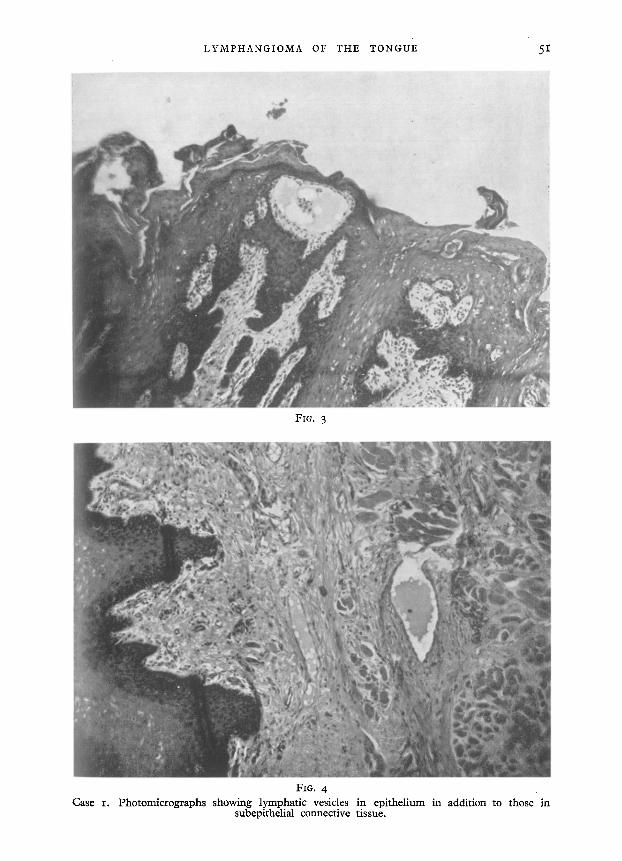
Pathological Report (Dr F. Duran-Jorda).--" Specimen of tongue, 7 by I "5 to 2 cm. Section shows lymphangioma with a considerable amount of fibrous t issue" (Figs. 3 and 4)-
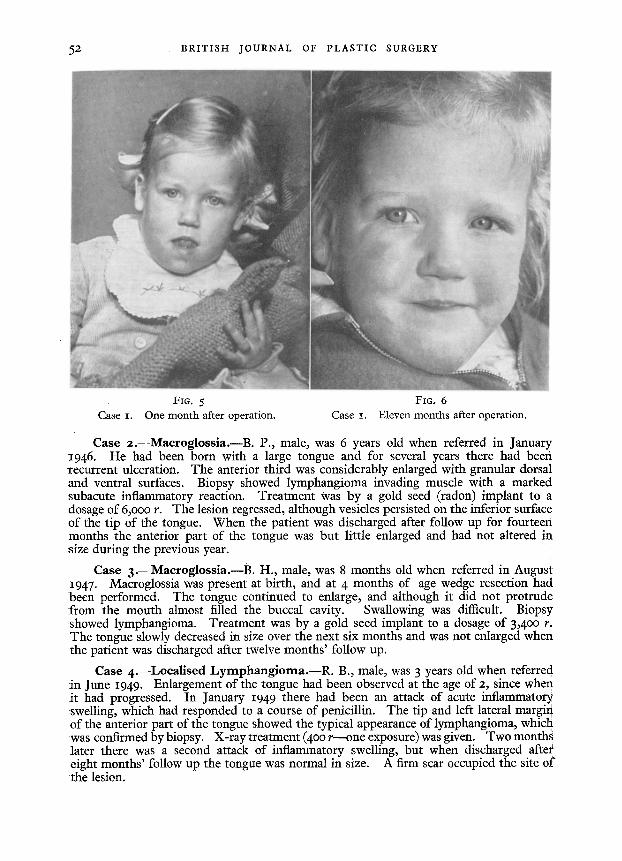
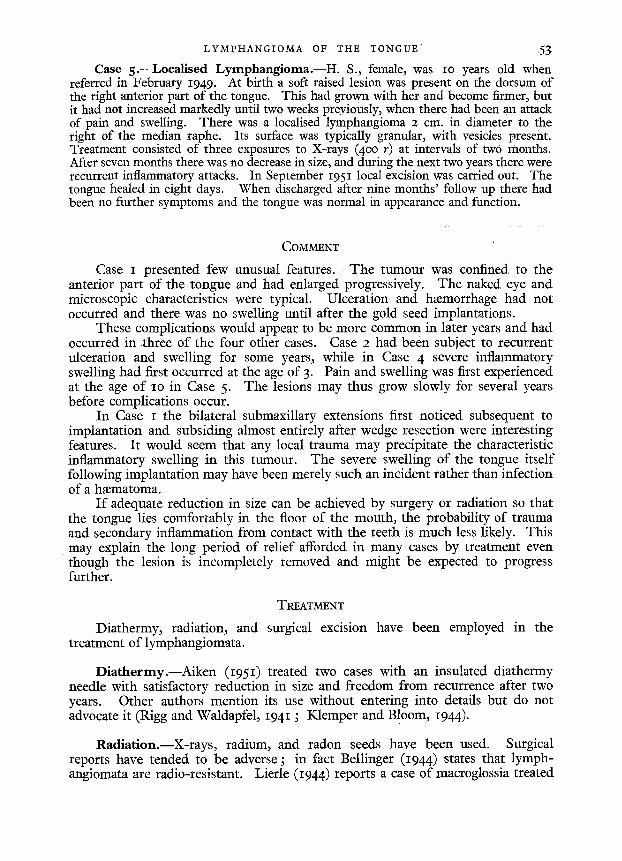
Subsequent Progress.--Fig. 5 shows the appearance of the child one month after operation. When last seen, eleven months after operation, the tongue had not increased in size relative to the oral cavity (Fig. 6). The tip was rather short and the verticaI depth was increased, but the whole tongue could be moved without difficulty. Speech appeared to be normal for her age. Prior to operation, the marked protrusion of the tongue had been very noticeable and the child's quiet, pathetic demeanour had been striking. Her general appearance was greatly improved and she seemed much happier. The submaxillary swellings had regressed almost entirely and were only just palpable.
LYMPHANGIOMA OF THE TONGUE 51
Fro. 3
FIG. 4 Case I. Photomicrographs showing lymphatic vesicles in epithelium in addition to those in
subepithelial connective tissue.
52 BRITISH JOURNAL OF PLASTIC SURGERY
Fla. 5 FIG. 6 Case I. One month after operation. Case i. Eleven months after operation.
Case 2. - -Maeroglossia . - -B. P., male, was 6 years old when referred in January 1946. He had been born with a large tongue and for several years there had been recurrent ulceration. The anterior third was considerably enlarged with granular dorsal and ventral surfaces. Biopsy showed lymphangioma invading muscle with a marked subacute inflammatory reaction. Treatment was by a gold seed (radon) implant to a dosage of 6,00o r. The lesion regressed, although vesicles persisted on the inferior surface of the tip of the tongue. When the patient was discharged after follow up for fourteen months the anterior part of the tongue was but little enlarged and had not altered in :size during the previous year.
Case 3. - -Maeroglossia . - -B. H., male, was 8 months old when referred in August 1947. Macroglossia was present at birth, and at 4 months of age wedge resection had been performed. The tongue continued to enlarge, and although it did not protrude from the mouth almost filled the buccal cavity. Swallowing was difficult. Biopsy showed lymphangioma. Treatment was by a gold seed implant to a dosage of 3,4oo r. The tongue slowly decreased in size over the next six months and was not enlarged when the patient was discharged after twelve months' follow up.
Case 4.---Localised L y m p h a n g i o m a . - - R . B., male, was 3 years old when referre d :in June 1949. Enlargement of the tongue had been observed at the age of 2, since when i t had progressed. In January 1949 there had been an attack of acute inflammatory swelling, which had responded to a course of penicillin. The tip and left lateral margiri o f the anterior part of the tongue showed the typical appearance of lymphangioma, whicli was confirmed by biopsy. X-ray treatment (400 r - -one exposure) was given. Two month~ later there was a second attack of inflammatory swelling, but when discharged aftet eight months' follow up the tongue was normal in size. A firm scar occupied the site of the lesion.
LYMPHANGIOMA OF THE TONGUE 53
Case 5.--Loeallsed Lymphang ioma . - -H . S., female, was IO years old when referred in February 1949. At birth a soft raised lesion was present on the dorsum of the right anterior part of the tongue. This had grown with her and become firmer, but it had not increased markedly until two weeks previously, when there had been an attack of pain and swelling. There was a localised lymphangioma 2 cm, in diameter to the right of the median raphe. Its surface was typically granular, with vesicles present. Treatment consisted of three exposures to X-rays (400 r) at intervals of two months. After seven months there was no decrease in size, and during the next two years there were recurrent inflammatory attacks. In September x951 local excision was carried out. The tongue healed in eight days. When discharged after nine months' follow up there had been no further symptoms and the tongue was normal in appearance and function.
COMMENT
Case I presented few unusual features. The tumour was confined to the anterior part of the tongue and had enlarged progressively. The naked eye and microscopic characteristics were typical. Ulceration and h~emorrhage had not occurred and there was no swelling until after the gold seed implantations.
These complications would appear to be more common in later years and had occurred in ,three of the four other cases. Case 2 had been subject to recurrent ulceration and swelling for some years, while in Case 4 severe inflammatory swelling had first occurred at the age of 3. Pain and swelling was first experienced at the age of ~o in Case 5. The lesions may thus grow slowly for several years before complications occur.
In Case I the bilateral submaxillary extensions first noticed subsequent to implantation and subsiding almost entirely after wedge resection were interesting features. It would seem that any local trauma may precipitate the characteristic inflammatory swelling in this tumour. The severe swelling of the tongue itself following implantation may have been merely such an incident rather than infection of a ha:matoma.
I f adequate reduction in size can be achieved by surgery or radiation so that the tongue lies comfortably in the floor of the mouth, the probability of trauma and secondary inflammation from contact with the teeth is much less likely. This may explain the long period of relief afforded in many cases by treatment even though the lesion is incompletely removed and might be expected to progress further.
TREATMENT
Diathermy, radiation, and surgical excision have been employed in the treatment of lymphangiomata.
Diathermy.--Aiken (1951) treated two cases with an insulated diathermy needle with satisfactory reduction in size and freedom from recurrence after two years. Other authors mention its use without entering into details but do not advocate it (Rigg and Waldapfel, 1941 ; Klemper and Bloom, 1944).
Radiation.--X-rays, radium, and radon seeds have been used. Surgical reports have tended to be adverse ; in fact Bellinger (1944) states that lymph- angiomata are radio-resistant. Lierle (1944) reports a case of macroglossia treated
54 B R I T I S H JOURNAL OF P L A S T I C SURGERY
by X-rays to a dosage of 3,ooo r. There was an initial decrease in size, but the tongue again enlarged and finally wedge resection was necessary. Klemper and Bloom (1944) comment on the increased fibrosis after radiation.
On the other hand Spencer and Cade (1931) describe three unilateral cases, two treated by radium plaque and one by seeds. All three diminished progressively and after seven months the third was said to be normal in appearance.
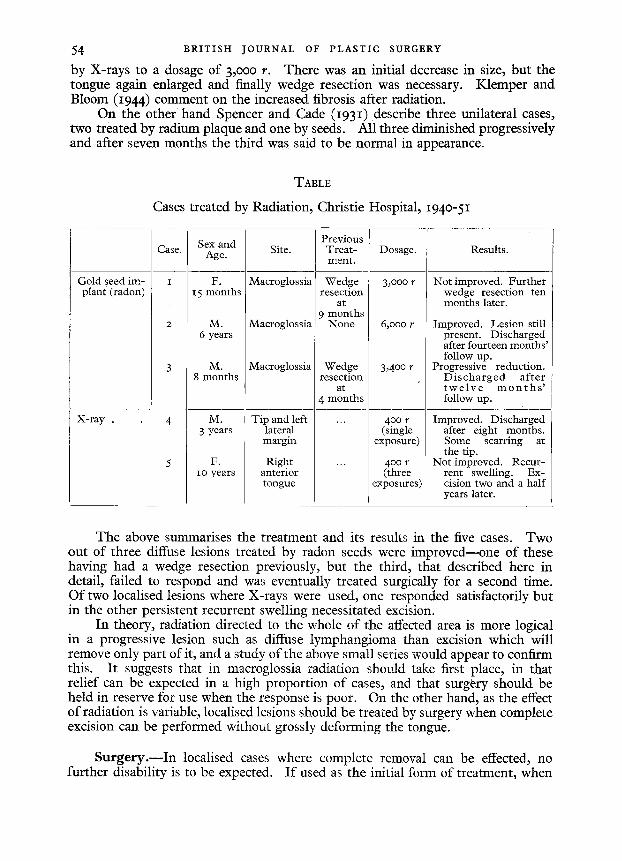
TABLE
Cases treated by Radiation, Christie Hospital, 194o-51
Gold seed im- plant (radon)
X-ray .
Case.
I
Sex and Site. Age.
F. Macroglossia 15 months
M. Macroglossia 6 years
M. Macroglossia 8 months
M. Tip and left 3 years lateral
margin
F. Right io years anterior
tongue
Previous Treat- m.ent.
Wedge resection
at 9 months
None
Wedge resection
at 4 months
Dosage.
3,000 r
6~000 r
3,4o0 r
40o r (single
exposure)
400 r (three
exposures)
Results.
Not improved. Further wedge resection ten months later.
Improved. Lesion still present. Discharged after fourteen months' follow up.
Progressive reduction. D i s c h a r g e d af ter t w e l v e m o n t h s ' follow up.
Improved. Discharged after eight months. Some scarring at the tip.
Not improved. Recur- rent swelling. Ex- cision two and a half years later.
The above summarises the treatment and its results in the five cases. Two out of three diffuse lesions treated by radon seeds were improved--one of these having had a wedge resection previously, but the third, that described here in detail, failed to respond and was eventually treated surgically for a second time. Of two localised lesions where X-rays were used, one responded satisfactorily but in the other persistent recurrent swelling necessitated excision.
In theory, radiation directed to the whole of the affected area is more logical in a progressive lesion such as diffuse lymphangioma than excision which will remove only part of it, and a study of the above small series would appear to confirm this. It suggests that in macroglossia radiation should take first place, in that relief can be expected in a high proportion of cases, and that surgery should be held in reserve for use when the response is poor. On the other hand, as the effect of radiation is variable, localised lesions should be treated by surgery when complete excision can be performed without grossly deforming the tongue.
Surgery . - - In localised cases where complete removal can be effected, no further disability is to be expected. I f used as the initial form of treatment, when
LYMPHANGIOMA OF THE TONGUE 55
the lesion is diffuse, the prognosis should be guarded, in that the course is progressive and the complications already described may be delayed for some years and necessitate re-operation. Very few cases have been followed up for long periods, but Lierle's case mentioned above was free from recurrence after four years. In the present series, initial treatment by surgery was disappoint- ing in that both cases continued to enlarge and further measures were required after four months and six months respectively.
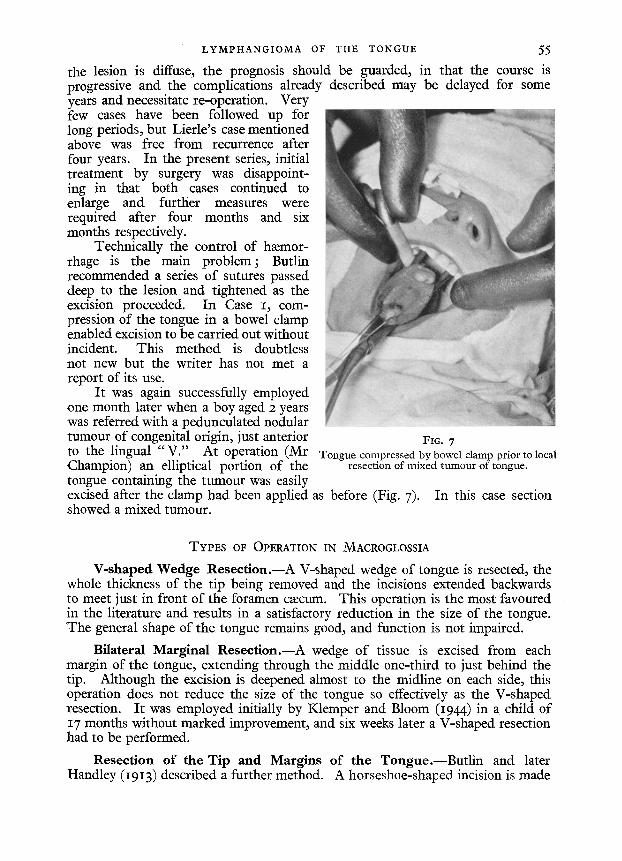
Technically the control of hmmor- rhage is the main problem; Butlin recommended a series of sutures passed deep to the lesion and tightened as the excision proceeded. In Case I, com- pression of the tongue in a bowel clamp enabled excision to be carried out without incident. This method is doubtless not new but the writer has not met a report of its use.
It was again successfully employed one month later when a boy aged 2 years was referred with a pedunculated nodular tumour of congenital origin, just anterior to the lingual "V ." At operation (Mr Champion) an elliptical portion of the tongue containing the turnout was easily excised after the clamp had been applied as before (Fig. 7). In this case section showed a mixed tumour.
FIG. 7 Tongue compressed by bowel clamp prior to local
resection of mixed tumour of tongue.
TYPES OF OPERATION IN MACROGLOSSIA
V-shaped Wedge Reseet ion.--A V-shaped wedge of tongue is resected, the whole thickness of the tip being removed and the incisions extended backwards to meet just in front of the foramen cmcum. This operation is the most favoured in the literature and results in a satisfactory reduction in the size of the tongue. The general shape of the tongue remains good, and function is not impaired.
Bilateral Marginal Reseet ion.--A wedge of tissue is excised from each margin of the tongue, extending through the middle one-third to just behind the tip. Although the excision is deepened almost to the midline on each side, this operation does not reduce the size of the tongue so effectively as the V-shaped resection. It was employed initially by Klemper and Bloom (1944) in a child of 17 months without marked improvement, and six weeks later a V-shaped resection had to be performed.
Resection of the Tip and Margins of the Tongue.--Butl in and later Handley (1913) described a further method. A horseshoe-shaped incision is made
5 6 BRITISH JOURNAL OF PLASTIC SURGERY
posterior to the tip and the free edge of the tongue is sutured. The incision is, then prolonged backwards on each side, finally tailing off to the margins of the tongue, further sutures being inserted as excision proceeds. This plan of operation should be equally efficacious in macroglossia, but in most cases wedge resection has been preferred.
SUMMARY
Lymphangioma of congenital origin occurs in the anterior two-thirds of the tongue either as a localised growth or as a diffuse infiltration. Diffuse lymph- angioma is the commonest cause of macroglossia.
The course is slowly progressive with characteristic attacks of inflammatory swelling followed by remissions. Lymphangiomatous macroglossia may become severe enough to interfere with mastication, deglutition, and speech.
Radiation or surgical resection have been employed in the treatment of most reported cases, although diathermy also has been used. Surgical resection is usually recommended in preference to radiation.
By contrast a study of five cases led to the conclusion that, while localised lesions should be excised where complete removal can be effected without grossly deforming the tongue, radiation should take first place in the treatment of lymph- angiomatous macroglossia. The majority of cases will respond and surgical resection may be held in reserve for those where failure occurs. The types of surgical resection available are discussed.
M y thanks are due to Mr .4. H. R. Champion for encouraging me to report Case I, and to Dr F. Duran-7orda who provided the pathological report and photomicrographs.
Dr Ralston Paterson kindly gave me permission to review the records of the other cases treated at the Christie Hospital and Holt Radium Institute.
The photographs were taken by Mr G. Ward.
REFERENCES
AMEN, D. (1951). Brit. me&ft., 2, 1123. BELLINCER, D. H. (1944)- J. oral Surg., 2, 141. EWlNG, J. (1942). "Neoplast ic Diseases." Four th Edition. Philadelphia and L o n d o n :
W. B. Saunders Co. FITZWILLIAMS, D. C. L. (1927). " The Tongue and its Diseases." London : Oxford Universi ty
Press. HANDLEY, S. (1913). Brit. ft. Surg., I , 42. HOWELL, B. W. (1918). Proc. R. Soc. Med., x2, 78. KLEMPER, J. W., and BLOOM, M. J. (I944). Amer. ft. Orthodont. (Oral Surgery Section), 3 o, 718. LIERLE, D. M. (1944). Ann. Otol., etc., St Louis, 53, 574. McDONALD, S. (1933). ft. Path. Bact., 36, 18 3. PETIT, G. (1923). Brit. ft. Derm., 35, 157. RING, J. P., and WALDAPFEL, R. (194o). Arch. Otolaryng., Chicago, 3 x, 966. - - (I94I). Amer. J. Orthodont. (Oral Surgery Section), 27, 128. SPENCER, W. G., and CADE, S. (I93I). " Diseases of the Tongue." Thi rd Edition. London :
H. K. Lewis. STONES, H. M. (I95I). " Oral and Dental Diseases." Edinburgh : E. & S. Livingstone. VmCHOW, J. (1854). Virchows Arch., 7, 127. Quoted by Spencer and Cade (I931).





























