Embed Size (px)
Citation preview

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 4 , N O . 7 , 2 0 1 1
© 2 0 1 1 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . D O I : 1 0 . 1 0 1 6 / j . j c m g . 2 0 1 1 . 0 3 . 0 1 7
LV Thrombus Detection byRoutine EchocardiographyInsights Into Performance Characteristics Using Delayed Enhancement CMR
Jonathan W. Weinsaft, MD,*� Han W. Kim, MD,*§ Anna Lisa Crowley, MD,*†§Igor Klem, MD,*§ Chetan Shenoy, MD,*§ Lowie Van Assche, MD,* Rhoda Brosnan, MD,*§Dipan J. Shah, MD,¶ Eric J. Velazquez, MD,†‡§ Michele Parker, RN, MS,*§Robert M. Judd, PHD,*§ Raymond J. Kim, MD*§
Durham, North Carolina; and New York, New York
O B J E C T I V E S This study sought to evaluate performance characteristics of routine echo for leftventricular thrombus (LVT).
B A C K G R O U N D Although the utility of dedicated echocardiography (echo) for LVT is established, echo
is widely used as a general test for which LVT is rarely the primary indication. We used delayed-enhancement
cardiac magnetic resonance (DE-CMR) as a reference to evaluate LVT detection by routine echo.
M E T H O D S Dedicated LVT assessment using DE-CMR was prospectively performed in patients withleft ventricular systolic dysfunction. Echoes were done as part of routine clinical care. Echo and CMR wereindependently read for LVT and related indexes of LVT size, shape, and image quality/diagnosticconfidence. Follow-up was done for embolic events and pathology validation of LVT.
R E S U L T S In this study, 243 patients had routine clinical echo and dedicated CMR within 1 week withoutintervening events. Follow-up supported DE-CMR as a reference standard, with �5-fold difference in endpointsbetween patients with versus without LVT by DE-CMR (p � 0.02). LVT prevalence was 10% by DE-CMR. Echocontrast was used in 4% of patients. Echo sensitivity and specificity were 33% and 91%, with positive and negativepredictive values of 29% and 93%. Among patients with possible LVT as the clinical indication for echo, sensitivityand positive predictive value were markedly higher (60%, 75%). Regarding sensitivity, echo performance relatedto LVT morphology and mirrored cine-CMR, with protuberant thrombus typically missed when small (p � 0.02).Therewas also a strong trend tomissmural thrombus irrespective of size (p� 0.06). Concerningpositive predictivevalue, echoperformance related to imagequality, with lower diagnostic confidence scores for echoes readpositivefor LVT in discordance with DE-CMR compared with echoes concordant with DE-CMR (p � 0.02).
C O N C L U S I O N S Routine echo with rare contrast use can yield misleading results concerning LVT. Echoperformance is improved when large protuberant thrombus is present and when the clinical indication isspecifically for LVT assessment. (J Am Coll Cardiol Img 2011;4:702–12) © 2011 by the American College ofCardiology Foundation
From the *Duke Cardiovascular Magnetic Resonance Center, Duke University Medical Center, Durham, North Carolina;†Duke Cardiac Diagnostic Unit, Duke University Medical Center, Durham, North Carolina; ‡Duke Clinical ResearchInstitute, Duke University Medical Center, Durham, North Carolina; §Department of Medicine, Duke University MedicalCenter, Durham, North Carolina; �Department of Medicine, Greenberg Division of Cardiology, Weill Cornell MedicalCollege, New York, New York; and ¶The Methodist DeBakey Heart Center, Houston, Texas. This work was supported byGrant Nos. R01-HL64726 (to Dr. Kim) and R01-HL63268 (to Dr. Judd), a Doris Duke Clinical Scientist DevelopmentAward (to Dr. Weinsaft), and K23 HL102249-01 (to Dr. Weinsaft). Dr. Weinsaft is a recipient of a research grant fromLantheus Medical Imaging on left ventricular thrombus (echo contrast manufacturer). Drs. Judd and Kim are inventors of aU.S. patent on delayed enhancement magnetic resonance imaging, which is owned by Northwestern University. All otherauthors have reported that they have no relationships to disclose.
Manuscript received December 20, 2010; revised manuscript received February 16, 2011, accepted March 10, 2011.

IaDssttbpcddcmc
wuEcTateatHCpwpii
tetfpfFwotwpe
transient ischemic attack
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
703
n clinical practice, echocardiography (echo) iswidely accepted as the primary screening test forleft ventricular thrombus (LVT) (1,2). This ap-proach is supported by multiple studies showing
that echo performs well as a test for LVT whenimaging is tailored for this purpose (3–5). Morerecently, sonographic contrast has been shown tofurther improve diagnosis of LVT (6,7). Indeed,prior research by our group and others has demon-strated that a routine strategy of echo contrast use inat-risk patients can markedly improve LVT assess-ment, reducing both false positives and false nega-tives (8,9).
See page 713
While the utility of dedicated echo for LVT isestablished, echo is widely performed as a generalscreening test of cardiac structure and function forwhich thrombus is rarely the primary indication(10). Echo contrast use also remains low (11),possibly attributable to recent U.S. Food and DrugAdministration–mandated product safety labelwarnings (12) and resultant controversy surround-ing widespread use (11,13,14). Thus, for manypatients at risk for LVT, such as those with systolicdysfunction, both the primary indication and theuse of echo contrast for LVT is rare. As echo is themost common imaging test in the United States(15), better understanding of its performance char-acteristics in a real-life clinical setting is of substan-tial importance.
Delayed enhancement (DE) cardiac magneticresonance (CMR) can establish LVT based onavascular tissue characteristics, an approach that hasbeen shown to be highly accurate in multiplevalidation studies (8,16–18). As DE-CMR is non-invasive, it holds the added utility of studying LVTin broad at-risk populations for whom an invasivestandard such as surgical pathology would be im-practical. To date, DE-CMR has not been used tostudy factors that influence performance of routineclinical echo for detection of LVT.
We have previously reported the results of aprospective registry in which patients with leftventricular (LV) dysfunction underwent dedicatedCMR thrombus imaging and were thereafter fol-lowed for prognostic assessment (18). In this priorstudy, only cine- and DE-CMR were comparedand echo was not part of the research protocol. Forthe current study, we evaluated registry patients inwhom echo was performed as part of clinical care.
The goal was to employ DE-CMR as a means to Linvestigate real-life practice patterns and perfor-mance characteristics of routine echo for LVT.
M E T H O D S
Population. The study population was accrued fromn ongoing CMR registry of consecutive patients atuke University with LV systolic dysfunction. The
ole criterion for registry participation was impairedystolic function, defined as a left ventricular ejec-ion fraction (LVEF) below 50% measured quanti-atively on cine-CMR. No patients were excludedased on clinical characteristics or other criteria. Asreviously reported (18), the CMR imaging proto-ol entailed tailored (cine and DE) imaging foredicated LVT assessment. Comprehensive clinicalata was collected at the time of CMR, includingoronary risk factors, revascularization history, andedication regimen. Echocardiography was not a
omponent of the registry protocol.For the current study, clinical records
ere queried for all registry patients whonderwent echo within 1 week of CMR.cho was performed as part of routine
are at the discretion of treating clinicians.o standardize interpretation of thrombus
nd assess imaging factors that could po-entially influence echo performance,choes were retrieved from image archivesnd interpreted for the express purpose ofhis study by experienced (American
eart Association/American College ofardiology level III) readers blinded toatient identifiers or CMR results. Echoesere also reviewed for factors that couldotentially influence performance characteristics,ncluding sonographic contrast use and clinicalndication for echo.
In accordance with the established registry pro-ocol (18), prospective follow-up was performed forndpoints consistent with presence or absence ofhrombus by imaging. For the current investigation,ollow-up was examined in the subcohort of registryatients that underwent CMR and echo. Theollow-up protocol consisted of two components:irst, all records were carefully reviewed in patientsho had direct inspection and pathology evaluationf the LV (i.e., patients who underwent heartransplantation, LV aneurysmectomy, or necropsy)ithin 6 months of imaging. Second, follow-up waserformed for identification of clinical embolicvents that were highly suggestive of the presence of
A B B
A N D
CMR �
reson
CVA �
DE �
echo
LV �
ventri
LVEF
fractio
LVT �
TI � i
TIA �
VT. These events consisted of a docum
R E V I A T I O N S
A C R O N YM S
cardiac magnetic
ance
cerebrovascular accident
delayed enhancement
� echocardiography
left ventricle/left
cular
� left ventricular ejection
n
left ventricular thrombus
nversion time
ented

attcrwaec
ta
rwpwts
mtcwhtcbttmaeac
epowawac
ca(a[mfidIuat3
wrwapoCdd
Lc(sthEtm
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
704
cerebrovascular accident (CVA) or transient isch-emic attack (TIA) that occurred within 6 months ofimaging. Concordant with established criteria(19,20), CVA was defined as an acute neurologicdeficit of presumed vascular origin lasting �24 h,nd TIA a deficit lasting �24 h. Clinical informa-ion was obtained via: 1) telephone interview withhe patient, or, if deceased, with family members; 2)ontact with the patient’s physician; and 3) hospitalecords. All reported clinical events (CVA, TIA)ere confirmed based on medical documentation bytreating physician. Death was not considered
vidence of LVT unless attributed to a cerebrovas-ular embolic event.
This study was performed with the approval ofhe Institutional Review Board at Duke University;ll patients provided written informed consent.Image acquisition. CARDIAC MAGNETIC RESONANCE.
CMR was performed using 1.5-T scanners (Sie-mens Sonata or Avanto, Siemens, Malvern, Penn-sylvania). The pre-specified CMR protocol con-sisted of two components: cine-CMR foranatomical/functional assessment and DE-CMRfor tissue characterization. Cine-CMR used asteady-state free-precession sequence (typical repe-tition time: 3.0 ms; echo time: 1.5 ms; in-planespatial resolution: 1.7 � 1.4 mm; temporal resolu-tion: 35 to 40 ms). DE-CMR, performed 10 to 30min after gadolinium (0.15 mmol/kg) administra-tion, used a segmented inversion-recovery sequence(in-plane spatial resolution: 1.8 � 1.3 mm, tempo-al resolution: 160 to 200 ms). Cine and DE-CMRere obtained in matching short- and long-axislanes (slice thickness: 6 mm). Short-axis imagesere acquired every 1 cm (gap: 4 mm) throughout
he entire LV. Long-axis images were obtained intandard 2-, 3-, and 4-chamber orientations.
On standard DE-CMR (tailored to null viableyocardium; inversion time [TI]: 250 to 350 ms),
hrombus typically had an etched appearance (grayentrally, black border) whereas viable myocardiumas black and infarcted myocardium white. As weave previously reported (18), the diagnosis ofhrombus by standard DE-CMR can sometimes behallenging as both viable myocardium and throm-us appear relatively dark and are difficult to dis-inguish from one another. Although contrast up-ake is low in viable compared with infarctedyocardium, it is not zero as is the case with
vascular tissue such as thrombus, and the differ-nce in contrast uptake between viable myocardiumnd thrombus can be used to improve the conspi-
uity of thrombus. Thus, a tailored DE-CMR asequence was designed in which TI was increasedfrom that needed to null the viable myocardium(250 to 350 ms) to a fixed time (600 ms) needed toselectively null the avascular tissue such as thrombus(21). With this long TI sequence, regions withcontrast uptake (i.e., LV cavity and myocardium)appear bright, thrombus appears homogeneouslyblack, and there is improved thrombus delineation(18).
ECHOCARDIOGRAPHY. Transthoracic 2-dimensionalchocardiograms were obtained by experienced sonogra-hers on commercially available equipment (Sonos-5500r 7500, Philips Healthcare, Andover, Massachusetts)ith phased and sector array transducers. Echoes were
cquired in standard parasternal short- and long-axis asell as apical 2-, 3-, and 4-chamber imaging planes in
ccordance with American Society of Echocardiographyonsensus guidelines (22).
All echoes were performed as part of routinelinical practice; sonographer protocols were notltered for the current study. Echo contrast agentsperflutren lipid [Definity, Lantheus Medical Im-ging, North Billerica, Massachusetts] or proteinOptison, GE Healthcare, Waukesha, Wisconsin]icrospheres) were selectively used for cavity opaci-cation and endocardial border delineation ifeemed clinically necessary at the time of imaging.mages were digitally stored, viewed, and analyzedsing Xcelera workstations (Philips Healthcare). Inccordance with echo lab standards at our institu-ion, images were displayed at a typical frame rate of0 frames/s.
Data analysis. THROMBUS ASSESSMENT. Imagesere interpreted by consensus of two experienced
eaders (Level III trained in CMR and echo) whoere blinded to subject identifiers, clinical history,
nd all prior imaging tests (CMR and echo). Are-designated third reader was consulted in casesf interpretive discordance (cine-CMR: 1%, DE-MR: 4%, echo: 11%). Studies were read in ran-om order. Each modality was interpreted indepen-ently of the others.For DE-CMR, thrombus was identified as an
V mass with post-contrast inversion-recoveryharacteristics consistent with avascular tissue17,18). Thrombus appeared as a low-signal inten-ity mass surrounded by high-signal intensity struc-ures such as intracavitary blood and/or hyperen-anced myocardial infarction on DE-CMR.stablished criteria (21,23) were used to distinguish
hrombus from acute myocardial infarction withicrovascular obstruction, which may also appear as
filling defect. Differentiating features included:
mtmpvmmtgwwa�
ptpeeff
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
705
1) surrounding structures (no-reflow zones shouldbe completely encompassed by hyperenhancedmyocardium or LV cavity); 2) appearance (no-reflow occurs within the myocardium and thrombusin the LV cavity); and 3) stability of size onconsecutive DE-CMR acquisitions (no-reflow sizeshrinks from contrast fill-in at the periphery,thrombus size is stable). When thrombus was iden-tified, morphology was classified as protuberant (ifborders were distinct from endocardial contourswith protrusion into LV cavity) or mural (borderswere contiguous with adjacent endocardial con-tours) (24), with exams independently reinterpretedto assess intrareader and inter-reader reproducibil-ity. Thrombus volume was measured quantitativelyvia planimetry. Thrombus location was scoredbased on the nearest myocardial tissue using astandard 17-segment LV model.
For echo and cine-CMR, thrombus was diag-nosed using established anatomic criteria (25).Thrombus was defined as a mass within the LVcavity with margins distinct from ventricular endo-cardium and distinguishable from papillary muscles,chordae, trabeculations, or technical artifact.Thrombus was diagnosed based on review of para-sternal short- and long-axis images, and apical 2-,3-, and 4-chamber images. Echoes interpreted aspositive for thrombus were scored for diagnosticconfidence on a 3-point scale (low, medium, highconfidence) based on clarity of thrombus definition(distinct borders, independent mobility pattern)and overall image quality (endocardial border defi-nition, LV cavity artifacts).
LEFT VENTRICULAR QUANTIFICATION. LVEF andLV volumes were quantified based on end-diastolicand end-systolic endocardial contours from thestack of short-axis cine-CMR images. Regionalwall motion and scarring were assessed on a stan-dard 17-segment model using previously describedmethods (26). Regional function on cine-CMR wasgraded on a 5-point scale as follows: 0 � normalcontraction; 1 � mild-to-moderate hypokinesia;2 � severe hypokinesia; 3 � akinesia; 4 � dyski-nesia. Regional scarring based on area of hyperen-hanced (bright) myocardium on DE-CMR wasgraded on a 5-point scale as follows: 0 � nohyperenhancement; 1 � 1% to 25%; 2 � 26% to50%; 3 � 51% to 75%; 4 � 76% to 100%. Globalscar size as a percentage of LV myocardium wascalculated by summing the segmental scores (eachweighted by the midpoint of the range of hyperen-hancement) and dividing by the total number of
regions (27). tStatistical methods. Continuous data (expressed asean � SD) were compared using 2-sampled t
ests. Non-normally distributed data (expressed asedian and 25th to 75th percentiles) were com-
ared using the Wilcoxon rank sum test. Thrombusolumes were compared after logarithmic transfor-ation; results are expressed as the antilog of theean and 95% confidence intervals. Chi-square
ests were used to compare discrete data betweenroups; in those cases where the expected cell countas �5, Fisher exact test was used. McNemar testas used for paired comparisons of discrete vari-
bles. All statistical tests were 2-tailed; p values0.05 were regarded as significant.
R E S U L T S
Population characteristics. The study populationconsisted of 243 patients who underwent routineclinical echo and dedicated registry CMR within a1 week (1.5 � 2.7 days) interval. The most commonclinical indications for echo were to assess LV(92%) and/or valve (29%) function. Assessmentfollowing CVA/TIA/systemic embolism was un-common (2.5%; n � 6), as was evaluation forpossible LVT (5%; n � 13; known LV aneurysm/apical dysfunction, n � 5; prior documented LVT,n � 4; recent CVA, n � 3; anterior myocardialinfarction, n � 1).
Table 1 details patient characteristics, with com-parison between the current study population andregistry patients. Patients with echo were relativelysimilar to those without echo based on age, priorthromboembolic events, and rates of warfarin use.However, they were more often female and wereless likely to have prior coronary revascularizationand ischemic cardiomyopathy. Additionally, echopatients were more likely to have advanced systolicdysfunction as measured by LVEF or regional wallmotion score (both p � 0.0001). Consistent withthis, prevalence of thrombus by DE-CMR wasslightly greater among the echo study populationversus registry patients who did not undergo echo-cardiography (10% vs. 6%, p � 0.04).Follow-up validation. Follow-up was performed asart of the registry protocol for endpoints supportinghe imaging diagnosis of thrombus (CVA, TIA,athology verification). Of the 243 patients withcho, 216 (89%) had complete follow-up for thentire 6 months after imaging. Patients withollow-up were similar to those withoutollow-up (n � 27) based on prevalence of
hrombus by DE-CMR or echo, LVEF, or clin-
diac
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
706
ical indexes such as age, diabetes, or hypertension(all p � NS).
Figure 1 shows the rate of study endpoints forgroups stratified by the presence or absence ofthrombus as determined by imaging. Previouslyreported results of the overall registry are shown for
Table 1. Patient Characteristics
ParameterStudy Po
(n �
Clinical
Age, yrs 60 �
Male 63% (
Atherosclerosis risk factors
Diabetes mellitus 35% (
Hypertension 61% (
Tobacco use 24% (
Hypercholesterolemia 39% (
Prior myocardial infarction 44% (
Coronary revascularization 28% (
Percutaneous intervention 16% (
Coronary artery bypass grafting 17% (
Ischemic cardiomyopathy 63% (
Atrial fibrillation 19% (
Lifetime history of prior cerebrovascular event
Cerebrovascular accident 9% (
Transient ischemic attack 7% (
Therapeutic regimen
Aspirin 58% (
Warfarin 14% (
Thienopyridines 6% (
Beta-blocker 51% (
ACE inhibitor 46% (
Angiotensin receptor blocker 6% (
Loop diuretic 31% (
Spironolactone 11% (
Digoxin 16% (
Nitroglycerin 28% (
Cardiac magnetic resonance
LV thrombus (DE-CMR) 10% (
LV function and morphology
Ejection fraction, % 28 �
Wall motion score 1.7 �
% LV with akinesis or dyskinesis 24% (
End-diastolic volume, ml 210 �
End-systolic volume, ml 156 �
Aneurysm present 16% (
LV infarction
Myocardial Infarction (presence) 71% (
Infarct size (% LV) 10% (
% LV with �50% transmural infarction 0% (
Values are mean � SD, % (n), or median (25th to 75th percentile). Numbers inACE � angiotensin-converting enzyme; DE-CMR � delayed enhancement car
comparison. For DE-CMR, patients with throm-
bus had over a 5-fold higher rate of endpoints thanthose without thrombus (16.7% vs. 3.1%, p �0.02), a proportion similar to the �7-fold differencein the overall registry (18). There was a 1.8-folddifference in endpoints when patents were stratifiedby presence or absence of thrombus by echo (7.7%
ation)
Registry Patients Without Echo(n � 541) p Value
61 � 14 0.86
74% (398) 0.004
26% (142) 0.009
59% (320) 0.57
29% (156) 0.15
57% (306) <0.0001
50% (269) 0.17
40% (268) <0.0001
31% (169) <0.0001
27% (147) 0.003
74% (401) 0.002
14% (74) 0.08
7% (37) 0.28
4% (22) 0.13
69% (371) 0.003
19% (101) 0.14
18% (98) <0.0001
71% (386) <0.0001
63% (343) <0.0001
13% (70) 0.005
45% (244) 0.0003
18% (96) 0.02
28% (150) 0.0004
18% (44) 0.004
6% (31) 0.04
33 � 10 <0.0001
1.5 � 0.7 <0.0001
) 24% (6–35) 0.054
206 � 85 0.50
142 � 79 0.03
12% (63) 0.12
75% (404) 0.25
) 16% (0–29) 0.03
) 12% (0–29) 0.002
dface indicate p values �0.05.magnetic resonance; LV � left ventricular.
pul243
15
154)
86)
149)
58)
94)
108)
67)
39)
42)
154)
45)
22)
16)
140)
35)
16)
125)
111)
15)
76)
26)
39)
150)
24)
11
0.7
6–41
89
83
38)
172)
0–25
0–24
bol
vs. 4.2%, p � 0.34). Rate of endpoints was lower

o0dhDpaw
irCt
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
707
among patients with thrombus by echo comparedwith DE-CMR, despite the fact that patients withthrombus by echo tended to be less likely to beanticoagulated than were patients with thrombus byDE-CMR (36% vs. 63%, p � 0.054).Prevalence of LVT. DE-CMR identified LVT in10% (n � 24) of patients, whereas echo was readas positive in 12% (n � 28). Despite similar
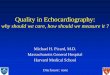
verall prevalence by echo and DE-CMR (p �.5), there was substantial discordance between mo-alities, as evidenced by the fact that only 8 patientsad thrombus concordantly detected by echo andE-CMR. Figure 2 provides a representative exam-
le of discordance between techniques, with echo reads negative and DE-CMR read as positive in a patientith thrombus verified by pathology.
Echo contrast use. Echo contrast was administeredn 4% (n � 10) of patients. Of the 10 patients whoeceived echo contrast, 2 had thrombus by DE-MR and 8 were negative. Echo was negative for
hrombus in all 10 of these cases (accuracy 80%).Diagnostic performance. Table 2 reports diagnosticperformance of echo and cine-CMR using thereference of DE-CMR. Echo yielded a sensitivityof 33% and specificity of 91%, and positive andnegative predictive values of 29% and 93%, respec-
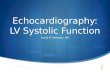
Figure 1. Follow-Up Endpoints in Relation to Imaging Findings
Stratification of patients with follow-up according to presence or abmagnetic resonance (DE-CMR) yielded over a 5-fold difference in stpathology-verified thrombus) between groups, whereas stratificatioyielded a 1.8-fold difference (pink � thrombus �, green � thromb
tively. Although overall sensitivity and positive
predictive value were limited, echo performancevaried based on clinical indication, with sensitivityincreased more than 2-fold (60% vs. 26%) andpositive predictive value more than 3-fold (75% vs.21%) for echoes performed for the clinical indica-tion of LVT assessment compared with those per-formed for nonthrombus indications.
Cine-CMR, which was acquired using a tailoredthrombus protocol and analyzed for thrombus usingthe same criteria as echo, was used to provideinsight into echo performance by testing the degreeto which optimized anatomic imaging might influ-ence diagnosis of LVT. As shown in Figure 3A,echo sensitivity was 50% among cases in whichcine-CMR detected thrombus, whereas sensitivitywas only 10% in which cine-CMR missed throm-bus (p � 0.08). Regarding positive predictive value,Figure 3B stratifies the diagnosis of thrombus firstby echo and then by cine-CMR. Among caseswhere cine-CMR diagnosed thrombus, positivepredictive value of echo was 88%. When cine-CMRwas negative for thrombus, positive predictive valueof echo was 5% (p � 0.0001).
Echo results also demonstrated that positivepredictive value was related to image quality/diagnostic confidence. Echoes read for thrombus in
ce of left ventricular thrombus by delayed enhancement cardiacendpoints (transient ischemic attack, cerebrovascular accident, orcording to left ventricular thrombus by echocardiography (echo)).
senudyn acus �
discordance with DE-CMR had lower diagnostic

2
smToc
ar th
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
708
confidence scores (assigned at the time of blindedinterpretation) than echoes with concordant throm-bus assessment to DE-CMR (1.95 � 0.69 vs..63 � 0.51, p � 0.02).
Thrombus morphology. Among the 24 cases of DE-CMR evidenced thrombus, 17 were classified asprotuberant and 7 as mural. Reproducibility washigh for both inter-reader (23 of 24) and intrareader(23 of 24) classification of thrombus morphology(kappa � 0.90, 95% confidence interval: 0.69 to1.0). Table 3 reports echo performance according tothrombus morphology and size. As shown, echowas far less likely to identify mural thrombus, withnearly all protuberant thrombi detected (7 of 8; p �0.06). Improved detection of protuberant thrombusoccurred despite the fact that protuberant andmural thrombi were, on average, virtually identicalin size (2.9 cm3). Further stratification demon-
Table 2. Thrombus Diagnosis by Routine Echo and Cine-CMR
Sensitivity Specificity
Echo (overall) 33% (8/24) 91% (199/219)
Clinical Indication
LVT 60% (3/5) 88% (7/8)
Other* 26% (5/19) 91% (192/211)
Cine-CMR (overall) 58% (14/24) 99% (218/219)
Values are % (n/N). *Excluding patients with echo done for stated indication o
Figure 2. Typical Example of LVT Assessment by Routine Echo a
(A) Routine echo demonstrates absence of thrombus but prominensuboptimal image quality. (B) DE-CMR demonstrates a large muralabsence of apical thrombus. Note that thrombus on DE-CMR appeaing. DE-CMR findings were confirmed by direct surgical inspectionstain, high power) of surgically resected material, which demonstrafibrin content) adjacent to the LV anterior wall. LVT � left ventricul
CMR � cardiac magnetic resonance; echo � echocardiography; LVT � left ventricular
trated that, for protuberant thrombus, size was aajor determinant of echo detection. As shown inable 3, protuberant thrombi detected by echo werever 4-fold larger than those missed (6.6 vs. 1.3m3, p � 0.02). Echo performance paralleled that
of cine-CMR, for which detected protuberantthrombi were over 6-fold larger than those missed(4.9 vs. 0.8 cm3, p � 0.01).
D I S C U S S I O N
Echocardiography is the most common cardiacimaging test in the United States (15), with over 21million exams performed annually (28). While theutility of echo for the dedicated purpose of diag-nosing LVT is established (3–5), echo is commonlyused as a general screening test and rarely per-formed for the specific indication of LVT (10). We
ccuracyPositive Predictive
ValueNegative Predictive
Value
(207/243) 29% (8/28) 93% (199/215)
(10/13) 75% (3/4) 78% (7/9)
(197/230) 21% (5/24) 93% (192/206)
(232/243) 93% (14/15) 96% (218/228)
sible LVT assessment (n � 13).
Dedicated DE-CMR
ar-field artifact within the left ventricular (LV) apex resulting inmbus adherent to the LV anterior wall (asterisk) as well aslack on long inversion time (TI) and etched on standard TI imag-e LV and histopathology examination (C) (hematoxylin and eosina thrombus with organizing features (prominent collagen andrombus; other abbreviations as in Figure 1.
A
85%
77%
86%
95%
f pos
nd
t nethrors bof thted
thrombus.

odmwcetftav
T
E-C
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
709
believe the current study is the first to assessperformance characteristics of routine echo for de-tection of LVT. Major new findings include: 1)how routine echo performs as a test for LVT incontext of everyday clinical practice; 2) factors thatinfluence LVT assessment, including fixed (i.e.,thrombus morphology) and potentially modifiable(i.e., image quality) indexes; and 3) magnitude ofimprovement to be expected if echo protocols wereoptimized for detection of LVT based on anatom-ical appearance.
It is important to recognize that this study shouldnot be construed as an equivalent comparison betweendiagnostic tests—echo versus DE-CMR. This wouldrequire sonographic contrast use in all patients, astrategy previously tested in our prior research (8). Forur current study, DE-CMR was performed in aedicated manner using tailored LVT imaging toake sure that our reference standard was optimized,hereas echo was performed according to routine
linical practice. With this approach, we sought toxamine current clinical practice patterns for echo ando determine factors that influence echo performanceor assessment of LVT. One of the primary findings ishat echo performance varied by indication for testing,s evidenced by over a 2-fold higher sensitivity (60%
Figure 3. Imaging Results Concerning LVT
Echo results concerning the diagnosis of thrombus stratified by cinBoth echo sensitivity (A) and positive predictive value (B) were highversus those in which cine-CMR was negative. Whereas cine-CMR apecho, both tests were negative in 9 of 24 patients with thrombus by D
s. 26%) and 3-fold higher positive predictive value
(75% vs. 21%) among exams performed for the spe-cific clinical indication of LVT.
In this real-life clinical cohort, echo contrast wasrarely used (4%). It is highly likely that echo perfor-mance in this study would have substantially improvedwere sonographic contrast used more frequently (6).
his low rate of echo contrast use is reflective of
d DE-CMR findings (pink � thrombus �, green � thrombus �).mong cases in which thrombus was also evidenced by cine-CMRriately detected thrombus in an additional 7 patients with negativeMR tissue characterization. Abbreviations as in Figures 1 and 2.
Table 3. Thrombus Morphology in Relation to Echo Detection
LVT by DE-CMR (n � 24)
Echo � (n � 8) Echo – (n
Type
Protuberant 7 10
Mural 1 6*
Thrombus Size (cm3)
Thrombus Detected Thrombus
Echo
Overall 6.6 (2.0–21.4) 2.0 (1.2–
Protuberant thrombus 6.6 (2.0–21.4) 1.3 (0.8–
Cine-CMR
Overall 4.9 (2.6–9.3) 1.4 (0.6–
Protuberant thrombus 4.9 (2.2–11.0) 0.8 (0.5–
Indexes reported as antilog of mean (95% confidence intervals) of log transfboldface indicate p values �0.05. *In 1 case, DE-CMR detected mural thrombuswall and excluded apical thrombus; echo was negative for anterior wall thrombthrombus p value based on thrombus detection by correct location.
e- aner aprop
p Value� 16)
0.06
Missed
3.5) 0.054
2.3) 0.02
3.0) 0.02
1.1) <0.01
ormed data. Numbers inadherent to mid anteriorus but positive for apical
Abbreviations as in Tables 1 and 2.

J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
710
national practice patterns. In a recent multicenterstudy encompassing over 4.3 million patients, echocontrast was used in only 1.4% of exams (11). How-ever, this study was a survey of a general populationand may not apply to our cohort of patients withsystolic dysfunction, in whom echo contrast may beparticularly useful for semi-quantitative evaluation ofLV systolic performance as well as LVT.
The importance of echo contrast is well estab-lished. In prior research by our group amongpatients at risk for thrombus (8), an obligate strat-egy of echo contrast yielded nearly a 2-fold increasein echo sensitivity (33% vs. 61%) for thrombus asestablished by the reference standard of DE-CMR.This concept was also demonstrated by Kurt et al.(9), who studied patients with technically difficultecho and reported that use of contrast excludedthrombus in 34 of 35 patients in whom noncontrastecho was positive while detecting thrombus in 5additional patients in whom noncontrast echo wasnegative. Whereas consensus guidelines recom-mend that echo contrast be used in cases of subop-timal image quality (22–29), low echo contrastutilization rates persist despite the fact that 15% ofechoes without contrast have been reported to betechnically difficult (9) and up to 46% are inconclu-sive for LVT (6). Our results demonstrate the im-portance of diagnostic uncertainty concerning LVT.Echoes that read positive for thrombus in discordancewith DE-CMR were assigned lower diagnostic con-fidence scores than those that read in concordancewith DE-CMR (p � 0.02). Taken together, thesefindings demonstrate the importance of optimizedimaging protocols, including the frequent use of con-trast, when echo is to be used to diagnose LVT.
To better elucidate the magnitude of improve-ment in echo performance that could be expected ifimaging protocols were optimized, our analysisincluded comparison of echo to cine-CMR—a testthat provides excellent endocardial border defini-tion (30) while identifying thrombus using the sameanatomical criteria as echo. Echo results generallytracked cine-CMR, with both echo sensitivity (p �0.08) and positive predictive value (p � 0.0001)improved when limited to patients in whom cine-CMR also detected thrombus. Cine-CMR dididentify thrombus in an additional 7 patients inwhom routine echo was negative, and it is likelythat echo would have also detected these if imagingwere tailored for optimized thrombus assessment.On the other hand, even cine-CMR missed nearlyone-half (42%) of thrombi detected by DE-CMR,
suggesting that echo limitations are not modality-specific but are partially attributable to detection ofthrombus based on anatomic rather than tissue-characteristic–based criteria. Regarding this point, it isimportant to recognize that perfusion echo can be alsoused for tissue characterization, and this approach hasbeen shown to be useful for assessment of thrombus(31). Though promising, perfusion echo is not per-formed as part of routine clinical practice at our centerand thus was not incorporated in the current study.
Stratification of thrombus detection based onmorphology and size demonstrated parallels be-tween echo and cine-CMR. For both echo andcine-CMR, protuberant thrombus was more likelyto be detected when large (p � 0.02). Muralthrombus was less likely to be detected by echoirrespective of size (p � 0.06), and this findingparalleled results for the overall registry (18), inwhich cine-CMR was shown to miss over half(58%) of all mural thrombi detected by DE-CMR.
Our current findings extend results of priorstudies comparing echo to DE-CMR. Srichai et al.(17), who studied patients with aneurysms under-going LV reconstruction surgery, reported thatsensitivity of transthoracic echo for thrombus was23% compared with 88% for CMR. All patients inthis study had pathology validation of the imagingdiagnosis of thrombus. However, in contradistinc-tion to our study, all patients were at high pre-testprobability for LVT, imaging reports were retro-spectively reviewed instead of primary interpreta-tion of images, and neither cine-CMR nor DE-CMR were analyzed as independent tests. Mollet etal. (23) reported that the sensitivity of echo was42% versus the reference of DE-CMR. However,this study evaluated a small cohort of 57 patientswith CAD and no independent standard for throm-bus was applied. In a separate study by our group(8), conducted primarily among patients with acutemyocardial infarction, sensitivity of contrast echowas 61%. However, these echoes were performed aspart of a research protocol that required obligatesonographic contrast use in all patients.
A central aspect of our study concerns our use ofprospective follow-up to validate the imaging detec-tion of LVT. Whereas dedicated DE-CMR yieldedover a 5-fold difference in endpoints between patientswith and without LVT (p � 0.02), routine echoyielded a 1.8-fold difference (p � 0.34). Prior echostudies have yielded conflicting results regarding theclinical risks of LVT, with some reporting that throm-bus does (32,33) and others that thrombus does not(34,35) increase embolic event risk. Our results may
potentially explain the conflicting prior data, demon-
KD
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
711
strating that although LVT is inherently associatedwith increased thromboembolic event risk, this asso-ciation may be missed if imaging is suboptimal. Asthrombus can be effectively treated with anticoagula-tion, our findings regarding the clinical risks of throm-bus and the importance of optimized imaging forLVT assessment bear important clinical and thera-peutic implications.Study limitations. A limitation of our data concernsthe fact that although anticoagulation status wasobtained after imaging, long-term status was notserially assessed throughout follow-up. It is possiblethat the timing and intensity of warfarin treatmentmay have been suboptimal in some patients withLVT, and this may have influenced the risk forthromboembolic events.
C O N C L U S I O N S
In summary, our study provides new data concern-ing routine clinical echo as a screening test forLVT. Among this diverse cohort of patients withsystolic dysfunction, routine echo with rare use ofcontrast often yielded misleading results concerningpresence or absence of thrombus. Echo performanceimproved when imaging was performed for the spe-cific indication of LVT. Diagnostic performance of
validation. Chest 1983;83:228–32. sue characterization
ity and positive predictive value among patients inwhich cine-CMR was positive for thrombus. Likecine-CMR, echo was less likely to detect protuberantthrombus when small, although mural thrombus wasfrequently missed independent of size.
The results of this study add to a growing body ofliterature that has demonstrated the utility of DE-CMR for LVT assessment in high-risk popula-tions, such as individuals with advanced LV systolicdysfunction, aneurysms, and/or large myocardialinfarctions. A dedicated DE-CMR protocol, in-cluding use of long-TI imaging, could be used toconfirm the diagnosis of LVT by routine echo incases when diagnostic confidence is low or sono-graphic contrast use is not used. However, thesefindings should be confirmed by other groups be-fore recommending broad changes in practice pat-terns regarding imaging for LVT. Future research isalso necessary to compare the relative utility ofdedicated thrombus imaging by tailored echo andDE-CMR for prognostic assessment and therapeu-tic management of patients at risk for LVT.
Reprint requests and correspondence: Dr. Raymond J.im, Duke Cardiovascular Magnetic Resonance Center,uke University Medical Center, Box 3439, Durham,
echo paralleled cine-CMR, with higher echo sensitiv- North Carolina 27710. E-mail: [email protected].
R E F E R E N C E S
1. Cheitlin MD, Armstrong WF, Au-rigemma GP, et al. ACC/AHA/ASE2003 guideline update for the clinicalapplication of echocardiography—summary article: a report of theAmerican College of Cardiology/American Heart Association TaskForce on Practice Guidelines (ACC/AHA/ASE Committee to Update the1997 Guidelines for the Clinical Ap-plication of Echocardiography). J AmColl Cardiol 2003;42:954–70.
2. Cheitlin MD, Alpert JS, ArmstrongWF, et al. ACC/AHA guidelines forthe clinical application of echocardiog-raphy. A report of the American Col-lege of Cardiology/American HeartAssociation Task Force on practiceguidelines (Committee on ClinicalApplication of Echocardiography).J Am Coll Cardiol 1997;29:862–79.
3. Visser CA, Kan G, David GK, LieKI, Durrer D. Two dimensional echo-cardiography in the diagnosis of leftventricular thrombus. A prospectivestudy of 67 patients with anatomic
4. Ezekowitz MD, Wilson DA, SmithEO, et al. Comparison of indium-111platelet scintigraphy and two-dimensionalechocardiography in the diagnosis ofleft ventricular thrombi. N EnglJ Med 1982;306:1509–13.
5. Stratton JR, Lighty GW Jr., PearlmanAS, Ritchie JL. Detection of left ven-tricular thrombus by two-dimensionalechocardiography: sensitivity, speci-ficity, and causes of uncertainty. Cir-culation 1982;66:156–66.
6. Thanigaraj S, Schechtman KB, PerezJE. Improved echocardiographic delin-eation of left ventricular thrombuswith the use of intravenous second-generation contrast image enhance-ment. J Am Soc Echocardiogr 1999;12:1022–6.
7. Mansencal N, Nasr IA, Pilliere R, etal. Usefulness of contrast echocardiog-raphy for assessment of left ventricularthrombus after acute myocardial in-farction. Am J Cardiol 2007;99:1667–70.
8. Weinsaft JW, Kim RJ, Ross M, et al.Contrast-enhanced anatomic imagingas compared to contrast-enhanced tis-
for detection of
left ventricular thrombus. J Am CollCardiol Img 2009;2:969–79.
9. Kurt M, Shaikh KA, Peterson L, et al.Impact of contrast echocardiographyon evaluation of ventricular functionand clinical management in a largeprospective cohort. J Am Coll Cardiol2009;53:802–10.
10. Okrah K, Vaughan-Sarrazin M, CramP. Trends in echocardiography utili-zation in the Veterans AdministrationHealthcare System. Am Heart J 2010;159:477–83.
11. Main ML, Ryan AC, Davis TE, Al-bano MP, Kusnetzky LL, Hibberd M.Acute mortality in hospitalized pa-tients undergoing echocardiographywith and without an ultrasound con-trast agent (multicenter registry resultsin 4,300,966 consecutive patients).Am J Cardiol 2008;102:1742–6.
12. U.S. Food and Drug Administration.New U.S. Food and Drug Adminis-tration prescribing information forDefinity approved October 10, 2007.Available at: http://www.fda.gov/cder/foi/label/2007/021064s007lbl.
pdf. Accessed October 20, 2007.
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 4 , N O . 7 , 2 0 1 1
J U L Y 2 0 1 1 : 7 0 2 – 1 2
Weinsaft et al.
Routine Echo for LV Thrombus
712
13. Main ML, Goldman JH, GrayburnPA. Thinking outside the “box”—theultrasound contrast controversy. J AmColl Cardiol 2007;50:2434–7.
4. Kusnetzky LL, Khalid A, KhumriTM, Moe TG, Jones PG, Main ML.Acute mortality in hospitalized pa-tients undergoing echocardiographywith and without an ultrasound con-trast agent: results in 18,671 consecu-tive studies. J Am Coll Cardiol 2008;51:1704–6.
5. Pearlman AS, Ryan T, Picard MH,Douglas PS. Evolving trends in theuse of echocardiography: a study ofMedicare beneficiaries. J Am CollCardiol 2007;49:2283–91.
6. Barkhausen J, Hunold P, EggebrechtH, et al. Detection and characteriza-tion of intracardiac thrombi on MRimaging. AJR Am J Roentgenol 2002;179:1539–44.
7. Srichai MB, Junor C, Rodriguez LL,et al. Clinical, imaging, and patho-logic characteristics of left ventricularthrombus: a comparison of contrastenhanced magnetic resonance imag-ing, transthoracic echocardiographyand transesophageal echocardiographywith surgical or pathological valida-tion. Am Heart J 2006;152:75–84.
8. Weinsaft J, Kim H, Shah DJ, et al.Detection of left ventricular thrombusby delayed-enhancement CMR: prev-alence and markers in patients withsystolic dysfunction. J Am Coll Car-diol 2008;52:148–57.
9. Karas MG, Francescone S, Segal AZ,et al. Relation between mitral annularcalcium and complex aortic atheroma inpatients with cerebral ischemia referredfor transesophageal echocardiography.Am J Cardiol 2007;99:1306–11.
0. Sacco RL, Adams R, Albers G, et al.Guidelines for prevention of stroke inpatients with ischemic stroke or tran-sient ischemic attack: a statementfor healthcare professionals fromthe American Heart Association/American Stroke Association Councilon Stroke: co-sponsored by the Coun-
cil on Cardiovascular Radiology andIntervention: the American Academyof Neurology affirms the value of thisguideline. Stroke 2006;37:577–617.
1. Shah DJ, Judd RM, Kim RJ. Myocar-dial viability. In: Edelman RR HJR,Zlatkin MB, Crues JV, editors. ClinicalMagnetic Resonance Imaging. 3rd edi-tion. New York, NY: Elsevier, 2006.
2. Lang RM, Biereg M, Devereux RM, etal. Recommendations for chamber quan-tification: a report from the AmericanSociety of Echocardiography’s Guide-lines and Standards Committee and theChamber Quantification WritingGroup. J Am Soc Echocardiogr 2005;18:1440–63.
3. Mollet NR, Dymarkowski S, VoldersW, et al. Visualization of ventricularthrombi with contrast-enhanced mag-netic resonance imaging in patientswith ischemic heart disease. Circula-tion 2002;106:2873–6.
4. Domenicucci S, Chiarella F, Bellotti P,Bellone P, Lupi G, Vecchio C. Long-term prospective assessment of left ven-tricular thrombus in anterior wall acutemyocardial infarction and implicationsfor a rational approach to embolic risk.Am J Cardiol 1999;83:519–24.
5. Asinger RW, Mikell FL, Elsperger J,Hodges M. Incidence of left-ventricular thrombosis after acutetransmural myocardial infarction. Se-rial evaluation by two-dimensionalechocardiography. N Engl J Med1981;305:297–302.
6. Wagner A, Mahrholdt H, Holly TA,et al. Contrast-enhanced MRI androutine single photon emission com-puted tomography (SPECT) perfusionimaging for detection of subendocardialmyocardial infarctions: an imagingstudy. Lancet 2003;361:374–9.
7. Sievers B, Elliott MD, Hurwitz LM, etal. Rapid detection of myocardial infarc-tion by subsecond, free-breathing de-layed contrast-enhancement cardiovas-cular magnetic resonance. Circulation2007;115:236–44.
8. U.S. Government Accountability Of-fice. Report to Congressional Com-mittees: Medicare Ultrasound Proce-dures—Consideration of Payment
Reforms and Technician QualificationRequirements. Washington, DC: tGovernment Accountability Office,June 2007.
9. Quinones MA, Douglas PS, Foster E,et al. ACC/AHA clinical competencestatement on echocardiography: a re-port of the American College of Car-diology/American Heart Association/American College of Physicians—American Society of Internal MedicineTask Force on Clinical Competence.J Am Coll Cardiol 2003;41:687–708.
0. Thiele H, Nagel E, Paetsch I, et al.Functional cardiac MR imaging withsteady-state free precession (SSFP)significantly improves endocardialborder delineation without contrastagents. J Magn Reson Imaging 2001;14:362–7.
1. Kirkpatrick JN, Wong T, Bednarz JE,et al. Differential diagnosis of cardiacmasses using contrast echocardio-graphic perfusion imaging. J Am CollCardiol 2004;43:1412–9.
2. Stratton JR, Resnick AD. Increasedembolic risk in patients with left ven-tricular thrombi. Circulation 1987;75:1004–11.
3. Crawford TC, Smith WT, VelazquezEJ, Taylor SM, Jollis JG, Kisslo J.Prognostic usefulness of left ventric-ular thrombus by echocardiographyin dilated cardiomyopathy in pre-dicting stroke, transient ischemic at-tack, and death. Am J Cardiol 2004;93:500 –3.
4. Nihoyannopoulos P, Smith GC, Ma-seri A, Foale RA. The natural historyof left ventricular thrombus in myo-cardial infarction: a rationale in sup-port of masterly inactivity. J Am CollCardiol 1989;14:903–11.
5. Ciaccheri M, Castelli G, Cecchi F, etal. Lack of correlation between intra-cavitary thrombosis detected by crosssectional echocardiography and sys-temic emboli in patients with dilatedcardiomyopathy. Br Heart J 1989;62:26–9.
Key Words: cardiac magneticresonance y echocardiography y
hrombus.