-
7/31/2019 Lustig 27-29 Comment Sugar 3
1/3
OBITUARYPhilip Lawl and thdiscov that DNA damagcan ca s canc
.36
LITERATUREHow Cha l sDick ns d w on sci nc , tl ft oom fo wond
.32
NEUROSCIENCETh so c of ths lf is in th ains wi ing,not individ
al n ons .31
ECOLOGYKomodo d agons andl phants co ld d c fiisk in A st alia
.30
Th toxic t th a o t s gaAdd d sw t n s pos dang s to h alth that
j stif cont olling th m lik alcohol,
a g Robert H. Lustig , Laura A. Schmidt and Claire D. Brindis
.
susceptible to non-communicable diseases;80% of deaths
attributable to them occur inthese countries.
Many people think that obesity is theroot cause of these
diseases. But 20% of obese people have normal metabolism and
Last September, the United Nationsdeclared that, for the first
time inhuman history, chronic non-commu-
nicable diseases such as heart disease, cancerand diabetes pose
a greater health burdenworldwide than do infectious
diseases,contributing to 35 million deaths annually.
This is not just a problem of the developedworld. Every country
that has adopted theWestern diet one dominated by low-cost,highly
processed food has witnessed risingrates of obesity and related
diseases. Thereare now 30% more people who are obesethan who are
undernourished. Economicdevelopment means that the populationsof
low- and middle-income countriesare living longer, and therefore
are more
will have a normal lifespan. Conversely, upto 40% of
normal-weight people manifestthe diseases that constitute the
meta-bolic syndrome: diabetes, hypertension,lipid problems, cardio
vascular disease,non-alcoholic fatty liver disease, cancer
anddementia. Obesity is not the cause; rather,it is a marker for
metabolic dysfunction,which is even more prevalent.
The UN announcement targets tobacco,alcohol and diet as the
central risk factorsin non-communicable disease. Two of thesethree
tobacco and alcohol are regulatedby governments to protect public
health,leaving one of the primary culprits behindthis worldwide
health crisis unchecked.Of course, regulating food is more
SUmmARY Sug r c nsumpti n is linked t risein n n-c mmunic ble
dise se Sug rs effects n t e b dy c n besimil r t t se f lc l Regul
ti n c uld include t x, limitings les during sc l urs, nd pl
cing
ge limits n purc sing
I l l u S t R a t I o n b y M a R k S M I t h
2 F e b r u A r y 2 0 1 2 | V O L 4 8 2 | N A T u r e | 2 7
COMMeNT
-
7/31/2019 Lustig 27-29 Comment Sugar 3
2/3
complicated food is required, whereastobacco and alcohol are
non-essential con-sumables. The key question is: what aspectsof the
Western diet should be the focus of intervention?
Denmark first chose, in October 2011,to tax foods high in
saturated fat, despitethe fact that most medical professionals
no
longer believe that fat is the primary culprit.But now, the
country is considering taxingsugar as well a more plausible and
defen-sible step. Indeed, rather than focusing on fatand salt the
current dietary bogeymen of the US Department of Agriculture
(USDA)and the European Food Safety Authority we believe that
attention should be turned toadded sugar, defined as any sweetener
con-taining the molecule fructose that is addedto food in
processing.
Over the past 50 years, consumption of sugar has tripled
worldwide. In the UnitedStates, there is fierce controversy over
the
pervasive use of one particular added sugar high-fructose corn
syrup (HFCS). It is manu-factured from corn syrup (glucose),
processedto yield a roughly equal mixture of glucoseand fructose.
Most other developed countrieseschew HFCS, relying on naturally
occurringsucrose as an added sugar, which also consistsof equal
parts glucose and fructose.
Authorities consider sugar as empty cal-ories but there is
nothing empty aboutthese calories. A growing body of
scientificevidence shows that fructose can triggerprocesses that
lead to liver toxicity and ahost of other chronic diseases 1. A
little isnot a problem, but a lot kills slowly (seeDeadly effect).
If international bodies aretruly concerned about public health,
they must consider limiting fructose and itsmain delivery vehicles,
the added sugarsHFCS and sucrose which pose dangersto individuals
and to society as a whole.
NO ORdINARY COmmOdITYIn 2003, social psychologist Thomas
Baborand his colleagues published a landmarkbook called Alcohol: No
Ordinary Commod-ity, in which they established four criteria,now
largely accepted by the public-healthcommunity, that justify the
regulation of alcohol unavoidability (or pervasivenessthroughout
society), toxicity, potential forabuse and negative impact on
society 2. Sugarmeets the same criteria, and we believe thatit
similarly warrants some form of societalintervention.
First, consider unavoidability. Evolu-tionarily, sugar as fruit
was available toour ancestors for only a few months a year(at
harvest time), or as honey, which wasguarded by bees. But in recent
years, sugarhas been added to virtually every processedfood,
limiting consumer choice 3. Naturemade sugar hard to get; man made
it easy.In many parts of the world, people are
consuming an average of more than 500 cal-ories per day from
added sugar alone (seeThe global sugar glut).
Now, lets consider toxicity. A growingbody of epidemiological
and mechanisticevidence argues that excessive sugar con-sumption
affects human health beyondsimply adding calories 4. Importantly,
sugar
induces all of the diseases associated withmetabolic syndrome
1,5. This includes: hyper-tension (fructose increases uric acid,
whichraises blood pressure); high triglyceridesand insulin
resistance through synthesis of fat in the liver; diabetes from
increased liver
glucose productioncombined with insu-lin resistance; andthe
ageing process,caused by damage tolipids, proteins andDNA through
non-enzymatic bind ing
of fructose to thesemolecules. It can alsobe argued that
fructose exerts toxic effects onthe liver similar to those of
alcohol 1. This isno surprise, because alcohol is derived fromthe
fermentation of sugar. Some early stud-ies have also linked sugar
consumption tohuman cancer and cognitive decline.
Sugar also has a clear potential for abuse.Like tobacco and
alcohol, it acts on thebrain to encourage subsequent intake.There
are now numerous studies examin-ing the dependence-producing
propertiesof sugar in humans 6. Specifically, sugardampens the
suppression of the hormoneghrelin, which signals hunger to the
brain.It also interferes with the normal transportand signalling of
the hormone leptin, whichhelps to produce the feeling of satiety.
Andit reduces dopamine signalling in the brainsreward centre,
thereby decreasing the pleas-ure derived from food and
compelling
the individual to consume more 1,6.Finally, consider the
negative effects
of sugar on society. Passive smoking anddrink-driving fatalities
provided strongarguments for tobacco and alcohol con-trol,
respectively. The long-term economic,health-care and human costs of
metabolicsyndrome place sugar overconsumption in
the same category 7
. The United States spends$65 billion in lost productivity and
$150 bil-lion on health-care resources annually forco-morbidities
associated with metabolicsyndrome. Seventy-five per cent of all
UShealth-care dollars are now spent on treat-ing these diseases and
resultant disabilities.Because 75% of military applicants are
nowrejected for obesity-related reasons, the pastthree US surgeons
general and the chairmanof the US Joint Chiefs of Staff have
declaredobesity a threat to national security.
HOw TO INTERvENE
How can we reduce sugar consumption?After all, sugar is natural.
Sugar is a nutri-ent. Sugar is pleasure. So is alcohol, but inboth
cases, too much of a good thing is toxic.It may be helpful to look
to the many genera-tions of international experience with
alcoholand tobacco to find models that work 8,9. Sofar, evidence
shows that individually focusedapproaches, such as school-based
interven-tions that teach children about diet and exer-cise,
demonstrate little efficacy. Conversely,for both alcohol and
tobacco, there is robustevidence that gentle supply side
controlstrategies which stop far short of all-out pro-hibition
taxation, distribution controls,age limits lower both consumption
of theproduct and accompanying health harms.Successful
interventions all share a commonend-point: curbing availability
2,8,9.
Taxing alcohol and tobacco products inthe form of special excise
duties, value addedtaxes and sales taxes are the most popular
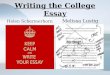
dEAdLY EffECTExcessive c nsumpti n f fruct se c n c use m ny f t
e s me e lt pr blems s lc l.
Chronic ethanol exposure Chronic fructose exposure
hem t l gic dis rders
Electr lyte bn rm lities
hypertensi n hypertensi n (uric cid)
C rdi c dil t ti n
C rdi my p t y My c rdi l inf rcti n (dyslipidemi ,
insulinresist nce)
Dyslipidemi Dyslipidemi (de n v lip genesis)
P ncre titis P ncre titis ( ypertriglyceridemi )
obesity (insulin resist nce) obesity (insulin resist nce)
M lnutriti n M lnutriti n ( besity)
hep tic dysfuncti n ( lc lic ste t ep titis) hep tic dysfuncti n
(n n- lc lic ste t ep titis)
Fet l lc l syndr me
addicti n h bitu ti n, if n t ddicti n
S urce: ref. 1
Sugar is cheap, sugar tastes good,and sugar sells,so companies
have little incentive to
change.
2 8 | N A T u r e | V O L 4 8 2 | 2 F e b r u A r y 2 0 1 2
COMMENT
-
7/31/2019 Lustig 27-29 Comment Sugar 3
3/3
and effective ways to reduce smoking and
drinking, and in turn, substance abuse andrelated harms 2.
Consequently, we proposeadding taxes to processed foods that
containany form of added sugars, such as HFCS andsucrose. This
would include sweetened fizzy drinks (soda) and other
sugar-sweetenedbeverages (for example, juice, sports drinksand
chocolate milk), and also sugared cereal.Already, Canada and some
European coun-tries impose small additional taxes on somesweetened
foods. The United States is cur-rently considering a
penny-per-ounce sodatax (about 34 cents per litre), which
wouldraise the price of a can of soda by 1012cents. Currently, each
US citizen consumesan average of 216 litres of soda per year, of
which 58% contains sugar; taxing at a penny an ounce could provide
annual revenues inexcess of $45 per capita (roughly $14 billionper
year); however, this would be unlikely to reduce total consumption.
Statisticalmodelling suggests that the price wouldhave to double to
significantly reduce sodaconsumption so a $1 can of soda shouldcost
$2 (ref. 10).
Other successful tobacco- and alcohol-control strategies limit
availability, such asreducing the hours that retailers are
open,controlling the location and density of retailmarkets and
limiting who can legally pur-chase the products 2,9. A reasonable
parallelfor sugar would tighten licensing require-ments on vending
machines and snack barsthat sell sugary products in schools
andworkplaces. Many schools have removedsoda and candy from vending
machines, butoften replaced them with juice and sportsdrinks, which
also contain added sugar.States could apply zoning ordinances
tocontrol the number of fast-food outlets andconvenience stores in
low-income commu-nities, and especially around schools,
whileproviding incentives for the establishment of grocery stores
and farmers markets.
Another option would be to limit sales
during school operation, or to designatean age limit (such as
17) for the purchase of drinks with added sugar, particularly
soda.Indeed, parents in South Philadelphia, Penn-sylvania, recently
took this upon themselvesby lining up outside convenience stores
andblocking children from entering them afterschool. Why couldnt a
public-health direc-tive do the same?
THE pOSSIBLE dREAmGovernment-imposed regulations onthe marketing
of alcohol to young peoplehave been quite effective, but there is
no suchapproach to sugar-laden products. Even so,the city of San
Francisco, California, recently instituted a ban on including toys
withunhealthy meals such as some types of fastfood. A limit or,
ideally, ban on televi-sion commercials for products with
addedsugars could further protect childrens health.
Reduced fructose consumption couldalso be fostered through
changes in sub-sidization. Promotion of healthy foods inUS
low-income programmes, such as theSpecial Supplemental Nutrition
Programfor Women, Infants and Children and theSupplemental
Nutrition Assistance Pro-gram (also known as the
food-stampsprogramme) is an obvious place to start.Unfortunately,
the petition by New York City to remove soft drinks from the
food-stampprogramme was denied by the USDA.
Ultimately, food producers and dis-tributors must reduce the
amount of sugaradded to foods. But sugar is cheap, sugartastes
good, and sugar sells, so companieshave little incentive to change.
Althoughone institution alone cant turn this jug-gernaut around,
the US Food and DrugAdministration could set the table forchange8.
To start, it should consider remov-ing fructose from the Generally
Regardedas Safe (GRAS) list, which allows food
manufacturers to add unlimited amounts toany food. Opponents
will argue that othernutrients on the GRAS list, such as iron and
vitamins A and D, can also be toxic whenover-consumed. However,
unlike sugar,these substances have no abuse potential.Removal from
the GRAS list would send apowerful signal to the European Food
Safety
Authority and the rest of the world.Regulating sugar will not be
easy particularly in the emerging markets of developing countries
where soft drinksare often cheaper than potable water ormilk. We
recognize that societal interven-tion to reduce the supply and
demand forsugar faces an uphill political battle againsta powerful
sugar lobby, and will requireactive engagement from all
stakeholders.Still, the food industry knows that it hasa problem
even vigorous lobbying by fast-food companies couldnt defeat thetoy
ban in San Francisco. With enough
clamour for change, tectonic shifts inpolicy become possible.
Take, for instance,bans on smoking in public places and theuse of
designated drivers, not to mentionairbags in cars and condom
dispensers inpublic bathrooms. These simple measures which have all
been on the battlegroundof American politics are now taken
forgranted as essential tools for our publichealth and wellbeing.
Its time to turn ourattention to sugar.
Robert H. Lustig is in the Department of Pediatrics and the
Center for Obesity Assessment, Study and Treatment at theUniversity
of California, San Francisco,California 94143, USA.Laura A. Schmidt
and Claire D. Brindis are at the Clinical and Translational Science
Institute and the Philip R. Lee Institute for Health PolicyStudies,
University of California, SanFrancisco, California 94118,
USA.e-mail: [email protected]
1. l s ig, R. h. J. Am. Diet. Assoc. 110, 13071321(2010).
2. b r, t. e . Alcohol: No Ordinary Commodity:Research and
Public Polic y (oxf rd u iv. Press,2003).
3. Vi , F. & u y, R. i Food Policy for Developing
Countries: Case Studies (eds Pi s r p-a derse ,P. & C e g,
F.) n . 9-5 (2007); v i e p://g . re.c m/prjs 4
4. J i Who/Fao Exper C s i .Diet,Nutrition and the Prevention of
Chronic Diseases Who tec ic Rep r Series 916 (Who; 2003).
5. t ppy, l., l, k. a., tr , C, & P q , n. Nutrition 26,
10441049 (2010).
6. G r er, a. k. & l s ig, R. h. Curr. Drug Abuse Rev.4,
146162 (2011).
7. Fi e s ei , E. a., Fie e r , I. C. & W g, G.Health Aff.
W3 (s pp .), 219226 (2003).
8. E ge rd, C. l., G rs , a. Jr & D r , S.Reducing Obesity:
Policy Strategies from theTobacco Wars (ur I s i e, 2009); v i
e
p://g . re.c m/w4 59. R m, R., Sc mid , l. a., Re m, J. & M
e P. Br.
Med. J. 337, 2364 (2008).10. S rm, R., P we l. M., C riq i, J.
F. & C p ,
F. J. Health Aff. 29, 10521058 (2010).
THE GLOBAL SUGAR GLUTGlobal sugar supply (in the form of sugar
and sugar crops, excluding fruit
and wine) expressed as calories per person per day, for the year
2007.
>600
Calories perperson per day
500600400500300400200300100200