Embed Size (px)
Citation preview

Citation: Bourcier J-E, Babinet M and Garnier D. Lung Ultrasound Leading to a Diagnosis of Bronchial Foreign Body. Austin J Pulm Respir Med 2016; 3(2): 1044.
Austin J Pulm Respir Med - Volume 3 Issue 2 - 2016ISSN : 2381-9022 | www.austinpublishinggroup.com Bourcier et al. © All rights are reserved
Austin Journal of Pulmonary & Respiratory Medicine
Open Access
Abstract
A 78 years old lady presented to the Emergency Room (ER) due to a three-month persistent cough despite symptomatic treatment and a short corticosteroid therapy. Clinical examination and lung ultrasound revealed an atelectasis of the left lower lobe. The etiologic assessment concluded to a bronchial foreign body.
bronchopneumonia on aspiration of foreign body.
After further questioning, the patient reported the loss of a dental bridge during a meal, four months ago. She did not pay much attention at that time, as she thought she had swallowed it. She showed no penetration syndrome. The patient was therefore transferred to a pulmonology department and a probabilistic antibiotic combination was initiated (amoxicillin + clavulanic acid: 1 g three times a day).
Bronchoscopy revealed abundant purulent secretions at the left bronchial tree, associated with an aspect of granuloma. Bacterial samples were completed. The tooth was not found during the endoscopy: the patient hat spit the tooth in the morning before the examination. The outcome was favourable under simple antibiotic treatment.
DiscussionAspiration of foreign body is widely under diagnosed in adults,
as a consequence of a poor or subtle presentation. Regarding the children, there is a peak incidence during the second year, this phenomenon being between the sixth and seventh decade in adults [1].
Case PresentationA 78 years old lady presented to the emergency room with a
three-month history of dry cough. She came in the afternoon of a day off, her general practitioner being absent, despite her appointment with her chest physician on the following day. She consulted the ER because the cough became debilitating.
Her past medical history was significant for a hypothyroidism and a well-controlled post-infective cylindrical bronchiectasis. Her last pulmonary function test did not show any sign of obstructive airway defect: Forced Vital Capacity (FVC) 2,37L; Forced Expiratory Volume in 1 second (FEV1) 1,84 L; FEV1/FVC ratio 77,6%; Residual Volume (RV) 1,27 L, Total Lung Capacity (TLC) 3,77L; Diffusing Capacity (DLCO) 18 ml/min/mmHg. The patient showed no active or passive smoking history, and no known allergy was to be reported. She described a dry cough which appeared gradually over several weeks, predominantly during the night and went crescendo for the last ten days. The patient consulted her general practitioner the previous week and was treated by antitussive syrup and systemic corticosteroids for three days. On this lap of time, she did not feel any improvement despite the subscribed treatment.
On admission, the patient had a dry cough and exhibited no sign of respiratory distress: her respiratory rate was normal, she was not cyanotic, and her oxygen saturation was 95% without oxygen supplementation. Pulmonary auscultation noted a silence in the left lung base. Pulse, blood pressure and temperature were normal.
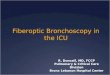
Lung ultrasonography performed by the Emergency Physician (EP) highlighted a pulmonary atelectasis associated with a left basal pneumonia (Figure 1).
Chest x-ray, confirmed the pulmonary condensation and an aspect of air bronchogram, as well as a one centimeter unidentified radiopaque image, located at the left lower lobar bronchus (Figure 2).
The biological assessment found an inflammatory syndrome with a leucocytosis at 22 900/mm3 (19,300 neutrophils granulocytes), a CRP at 257 mg/L. Haemoglobin, platelets and biochemistry were within normal range.
These examinations led to the diagnosis of a left basal
Case Report
Lung Ultrasound Leading to a Diagnosis of Bronchial Foreign BodyJean-Eudes Bourcier*, Marion Babinet and Didier GarnierEmergency, Anesthesiology and Critical Care Department, Lourdes Hospital, France
*Corresponding author: Jean-Eudes Bourcier, Emergency, Anesthesiology and Critical Care Department, Lourdes Hospital, 2 Avenue Alexandre Marqui 65100 Lourdes, France
Received: June 20, 2016; Accepted: June 25, 2016; Published: June 28, 2016
Figure 1: Ultrasound of the left lower lobe.

Austin J Pulm Respir Med 3(2): id1044 (2016) - Page - 02
Jean-Eudes Bourcier Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.com
The recorded contributing factors are: alcohol intoxication, sedation, poor dentition, senility, mental retardation, Parkinson’s disease, head trauma with loss of consciousness, epilepsy and general anaesthesia. These factors impair the cough reflex, resulting in an alteration of airway protection mechanisms during swallowing. Chronic cough is the most common symptom [2].
As foreign bodies can go unnoticed among adults, a specific examination in search of an aspiration episode (or a history of choking) is required, since the patient usually has no recollection [3]. A large number of foreign bodies are indeed found incidentally on a radiograph performed for another indication (asthma, persistent pneumonia) [3,4]. In this case lung ultrasound led to the diagnosis of left pneumonia and atelectasis. We should have performed a CT scan rather than chest X ray to clarify the lesions, and the tooth should appeared. Shall the diagnosis not be established, residual foreign body can lead to persistent pneumonia, lung abscess and bronchiectasis. In addition, the formation of inflammatory granuloma around the foreign body can mimic lung carcinoma imaging [1].
Pulmonary atelectasis is the most encountered radiographic sign in adults [1]. The foreign body is usually found at the right main stem bronchus for anatomical reasons (more vertical and larger in diameter than the left main stem bronchus) [1]. Dental foreign body is more often encountered in adults than in children [5]. The literature data highlights the fact that pulmonary ultrasound has a higher specificity and sensitivity than chest X-ray in the diagnosis of alveolar syndrome [6-8]. As a matter of fact, it showed within our current case a heterogeneous picture combining air bronchogram and a left base pseudo-tissue appearance, compatible with pulmonary condensation [9], whereas chest X-ray can only highlight a limited percentage of radiopaque foreign bodies. One can furthermore observe indirect signs such as atelectasis, entrapment of air (on an exhalation cliché), pneumomediastinum, and mediastinal deviation [10]. Radiolucent objects such as wood or plastic won’t be seen with X-ray or CT scan. The tendency for this disorder to simulate other disease processes creates traps for the clinician, which is even harder to avoid if there is a prolonged asymptomatic period between the
time of aspiration and the patient’s appearance in the physician’s office. This interval may be so long that patients frequently neglect to volunteer information about the previous aspiration, not suspecting that it bears any relationship to their existing symptoms [11]. In case of high clinical suspicion, with a picture of acute respiratory distress following a syndrome of penetration, flexible bronchoscopy remains the gold standard examination for diagnostic purposes [12].
In this context of chronic cough, a chest CT scan should have been performed as a first line, allowing a more accurate morphological assessment, regardless of the nature of the foreign body.
Since its first introduction in 1897, the treatment is based on the removal of the foreign body by rigid bronchoscopy [13]. Subsequently, bronchial pneumonia on foreign body should be considered as conventional aspiration pneumonia. An active antibiotic therapy on anaerobic germs and on Gram-negative bacilli should therefore be established [14].
References1. Baharloo F, Veyckemans F, Francis C, Biettlot MP, Rodenstein DO.
Tracheobronchial foreign bodies: presentation and management in children and adults. Chest. 1999; 115: 1357-1362.
2. Rafanan AL, Mehta AC. Adult airway foreign body removal. What’s new? Clin Chest Med. 2001; 22: 319-330.
3. Yilmaz A, Akkaya E, Damadoglu E, Gungor S. Occult bronchial foreign body aspiration in adults: analysis of four cases. Respirology. 2004; 9: 561-563.
4. Boyd M, Chatterjee A, Chiles C, Chin R Jr. Tracheobronchial foreign body aspiration in adults. South Med J. 2009; 102: 171-174.
5. Tamura N, Nakajima T, Matsumoto S, Ohyama T, Ohashi Y. Foreign bodies of dental origin in the air and food passages. Int J Oral Maxillofac Surg. 1986; 15: 739-751.
6. Cortellaro F, Colombo S, Coen D, Duca PG. Lung ultrasound is an accurate diagnostic tool for the diagnosis of pneumonia in the emergency department. Emerg Med J EMJ. 2012; 29: 19-23.
7. Bourcier JE, Paquet J, Seinger M, Gallard E, Redonnet JP, Cheddadi F, et al. Performance comparison of lung ultrasound and chest x-ray for the diagnosis of pneumonia in the ED. Am J Emerg Med. 2014; 32: 115-118.
8. Ye X, Xiao H, Chen B, Zhang S. Accuracy of Lung Ultrasonography versus Chest Radiography for the Diagnosis of Adult Community-Acquired Pneumonia: Review of the Literature and Meta-Analysis. PloS One. 2015; 10: e0130066.
9. Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012; 38: 577-591.
10. Swanson KL. Airway foreign bodies: what’s new? Semin Respir Crit Care Med. 2004; 25: 405-411.
11. Aronovitch M, Szabo AJ. Prolonged Retention of a Radiolucent Bronchial Foreign Body. Can Med Assoc J. 1962; 87: 1071-1073.
12. Dixit S, Agarwal R, Kumar N, Verma RK, Krishna V, Sahni JL. Management of tracheobronchial foreign bodies-experience of cardiothoracic department of cardiology institute. Indian J Thorac Cardiovasc Surg. 2010; 27: 33-35.
13. Mahmoud M, Imam S, Patel H, King M. Foreign Body Aspiration of a Dental Bridge in the Left Main Stem Bronchus. Case Rep Med. 2012.
14. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis Off Publ Infect Dis Soc Am. 2007; 44 Suppl 2: S27-72.
Figure 2: Chest X ray.