Embed Size (px)
DESCRIPTION
LUNG TRANSPLANTATION CURRENT STATUS. Iskander Al-Githmi, MD, FRCSC-GS , FRCSC -Ts , FRCSC-CDs, FACS, FCCP. Division of Cardiothoracic Surgery. King Abdulaziz University Hospital. NUMBER OF LUNG TRANSPLANTS REPORTED BY YEAR AND PROCEDURE TYPE. - PowerPoint PPT Presentation
Citation preview

LUNG TRANSPLANTATION CURRENT STATUS
Iskander Al-Githmi, MD, FRCSC-GS, FRCSC -Ts , FRCSC-CDs, FACS, FCCP Division of Cardiothoracic SurgeryKing Abdulaziz University Hospital


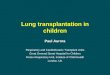
NUMBER OF LUNG TRANSPLANTS REPORTED BY YEAR AND PROCEDURE TYPE
5 7 36 78190
419
704
922
10871223
13581338145014601491
16281690
187919302071
23862448
2708
0
250
500
750
1000
1250
1500
1750
2000
2250
2500
2750
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
Nu
mb
er
of
Tra
ns
pla
nts
Bilateral/Double LungSingle Lung
ISHLTNOTE: This figure includes only the lung transplants that are reported to the ISHLT Transplant Registry. As such, this should not be construed as representing changes in the number of lung transplants performed worldwide.
2009

AVERAGE CENTER VOLUMELung Transplants: January 1, 2000 - June 30, 2008
46
2533
22 17730
10
20
30
40
50
60
1-4 5-9 10-19 20-29 30-39 40-49 50+
Average number of lung transplants per year
Nu
mb
er
of
ce
nte
rs
0
5
10
15
20
25
30
Number of centers Percentage of transplants
Per
cen
tag
e o
f tr
ansp
lan
ts
ISHLT
2009

Lung Transplantation in KSA
• 4 transplants at KFH – Jeddah 1991 - 1994
• 1996 ,first single lung transplant at KFSH & RC (Riyadh )
• First bilateral lung transplant at KFSH & RC (Riyadh ) 1998• 2001 , the lung transplant unit was established at KFSH & RC
( Jeddah)• Dec. 23,2001, the first successful bilateral lung transplant in
the Middle East was performed at KFSH & RC (Jeddah)

KFSH&RC – Jeddah Lung Transplantation Program
• Patients with end-stage lung diseases, N=13
• Indications: • Pulmonary fibrosis (n=8) • Bronchiectasis (n=2)• Pulmonary HTN (n=1)• COPD (n=1)• LAM (n=1)

Types of transplantation:• Single lung (n=10)• Bilateral lung (n=3)
Results:10/13 survivedMortality 3/13 (n=1 liver failure, n=1 stroke, n=1 T.B.)1 year survival 95 %

Lung transplantation in KSA
• KFSH & RC ( Jeddah ) is the only active hospital performing lung transplantation in the Middle East
• IPF is the commonest indication followed by Broncheictasis• 95% 1 year survival

AGE DISTRIBUTION OF LUNG TRANSPLANT RECIPIENTS (1/1985-6/2008)
0
5
10
15
20
25
30
35
0-11 12-17 18-29 30-39 40-49 50-59 60-65 66+
Recipient Age
% o
f tr
an
sp
lan
ts
ISHLT
2009

DONOR AGE DISTRIBUTION FOR LUNG TRANSPLANTS (1/1985-6/2008)
0
5
10
15
20
25
30
35
0-11 12-17 18-29 30-39 40-49 50-59 60-65 66+
Donor Age
% o
f tr
an
sp
lan
ts
ISHLT
2009

LUNG TRANSPLANTS: Transplant Recipient Age by Year of Transplant
Transplants: January 1, 1987 – June 30, 2008
0%
20%
40%
60%
80%
100%
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
0
10
20
30
40
50
60
0-11 12-17 18-34 35-49 50-59 60-65 66+ Mean Age
Mea
n r
ecip
ien
t ag
e (y
ears
)
% o
f T
ran
sp
lan
tsrs
Year of Transplant
ISHLT
2009

Lung transplantation evaluation process
• Cardiothoracic Transplant Surgeon• Transplant Pulmonologist• Transplant Coordinator• Transplant Anesthiologist• Infectious Disease• Nutritionist• Social services• Psychologist• Physiotherapist

Recipient Selective Criteria:• End-stage pulmonary disease with life expectancy < 2 yrs.• Absence of severe extra pulmonary diseases.• Strong motivation towards the idea of lung transplantation.• Severe functional limitation, but potential for rehabilitation.• Excellent psychosocial support.• No current smoking or substances abuse

Indications:• Obstructive air way disease (29%)
- COPD- Alpha 1 antitrypsin deficiency
• Idiopathic pulmonary fibrosis (19%)• Septic pulmonary disease (16%)
- Bronchiectasis- cystic fibrosis
• Primary pulmonary hypertension (11%)

• Other Varieties (11%)e.g. - sarcoidosis
- lymphangioliomyomatosis (LAM)
- eosinophilic granuloma

Contra-indications:• Age > 65 years• Active smoking• Poor compliance with the treatment• Severe active infections (HIV, Hepatitis B & C)

Con’t.• Active malignancy within the past two years.• Drugs or alcohol abuse.• Dysfunction of major other organs
- renal dysfunction- untreatable CAD or LV dysfunction- liver dysfunction
• Ventilator dependence - high mortality
• BMI < 16 and BMI > 30• Severe osteoporosis

Donor Selection Criteria (Standard):• Age < 55 years• ABO blood group compatibility• No significant lung diseases• Absence of chest trauma• Smoking Hx < 20 pack years• Clear CXR• PaO2 > 300mm Hg on F102 1.0 and PEEP 5 cm for 5 min.
• Bronchoscopy – clear• Sputum gram stain- Absence of organisms

Donor-Recipient Matching Issues
ABO blood group is the most antigen system Panel reactive antibodies Size matching
Undesized: persistent pneumothorax and increase work of breathing.
Oversized: atelectasis and distortion of anatomy

Donor Supply
Increasing gap between demand and supply Newer strategiesA. Marginal donors
Do not fill these criteria:-1- Age < 55 yrs2- Clear Chest X-ray3- No smoking history
` 4- Sputum gram stain negative5- Normal gas exchange

Donor Supply
B. Living lobar transplantation Harvesting left lower lobe from one healthy donor &
right lower lobe from another ( 25% of TLC for each) Pioneered by University of southern California (Vaughn
Starns). Impressive result in both children & adults Associated with Significant morbidity but no fatalities
reported

Donor Supply
C. Non -heart beating donor (NHBD) A donor whose death is defined by irreversible cessation of
circulatory and respiratory functions (UDDA) Period of time between a systole and retrieval is
controversial , recommendation is 2-5min NHBD contributes < 1% of the numbers of transplants in USA In Holland 50% of cadaveric transplants are from NHBD

Non-heart beating donor

Donor Supply
D. XenotransplantationInitial enthusiasm – unlimited donor supply
Hardening factors1. Severe immune response2. Apparent incompatibilities between the
coagulation systems of the two species
European resp.journal 2003;supp

Donor Supply
Reconditioning Lung Donor

Toronto Xvivo Lung Perfusion System

Shaf Keshavjee, MD,FRCSCDirector of Lung Transplant ProgramUniversity of Toronto

Lung transplantation
Single or double lung Wait time
-Blood Type-Size
Severity of illness-Life expectancy while on the waiting list-Outcome post transplant
Surgical time (6-8 hours) Hospital stay (14-21 days) Follow up ( life long, frequent office visits)

ADULT LUNG TRANSPLANTATION: Indications for Single Lung Transplants (Transplants: January 1995 - June 2008)
ISHLT
*Other includes:
Sarcoidosis: 2.1%
Bronchiectasis: 0.4%
Congenital Heart Disease: 0.2%
LAM: 0.8%
OB (non-ReTx): 0.5%
Miscellaneous: 6.3%
49%
29%
3%1%
2%
6%
10%
Alpha-1 COPD CF IPF IPAH Re-Tx Other*
2009

ADULT LUNG TRANSPLANTATION: Indications for Bilateral/Double Lung Transplants (Transplants: January 1995 - June 2008)
26%
14%2%5%
26%
8%
19%
Alpha-1 COPD CF IPF IPAH Re-Tx Other*
ISHLT
*Other includes:
Sarcoidosis: 2.9%
Bronchiectasis: 4.5%
Congenital Heart Disease: 1.1%
LAM: 1.2%
OB (non-ReTx): 1.1%
Miscellaneous: 7.7%
2009

ADULT LUNG TRANSPLANTATIONKaplan-Meier Survival (Transplants: January 1994 - June 2007)
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10
Years
Su
rviv
al
(%)
.
Bilateral/Double Lung (N=12,246)
Single Lung (N=10,081)
All Lungs (N=22,328)
Double lung: 1/2-life = 6.6 Years; Conditional 1/2-life = 9.0 YearsSingle lung: 1/2-life = 4.6 Years; Conditional 1/2-life = 6.4 YearsAll lungs: 1/2-life = 5.4 Years; Conditional 1/2-life = 7.4 Years
P < 0.0001
ISHLT
2009

ADULT LUNG TRANSPLANTATIONKaplan-Meier Survival by Procedure Type and Era
(Transplants: January 1990 – June 2007) Diagnosis: Idiopathic Pulmonary Fibrosis, Single Lung
0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10
Years
Su
rviv
al
(%)
IPF/Single lung/1990-1994 (N=456)
IPF/Single lung/1995-1999 (N=823)
IPF/Single lung/2000-6/2007 (N=1,775)
Survival comparisons1990-1994 vs. 1995-1999: p = 0.51591990-1994 vs. 2000-6/2007: p = 0.00281995-1999 vs. 2000-6/2007: p = 0.0066
N=14
N=62
N=52
ISHLT
2009

ADULT LUNG TRANSPLANTATIONKaplan-Meier Survival by Procedure Type and Era
(Transplants: January 1990 – June 2007) Diagnosis: Idiopathic Pulmonary Fibrosis, Double Lung
0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10
Years
Su
rviv
al
(%)
IPF/Double lung/1990-1994 (N=67)
IPF/Double lung/1995-1999 (N=263)
IPF/Double lung/2000-6/2007 (N=1,310)
Survival comparisons1990-1994 vs. 1995-1999: p = 0.55111990-1994 vs. 2000-6/2007: p =0.02871995-1999 vs. 2000-6/2007: p < 0.0001
N=11
N=33
N=10
ISHLT
2009

ADULT LUNG TRANSPLANTATIONKaplan-Meier Survival By Diagnosis (Transplants: January 1990 – June 2007)
0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10 11 12Years
Su
rviv
al
(%)
Alpha-1 (N=2,085) CF (N=3,746) COPD (N=8,812)
IPF (N=4,695) IPAH (N=1,065) Sarcoidosis (N=597)
HALF-LIFE Alpha-1: 6.1 Years; CF: 7.0 Years; COPD: 5.1 Years; IPF: 4.3 Years; IPAH: 5.6 Years; Sarcoidosis: 5.3 Years
ISHLT
Survival comparisonsAlpha-1 vs. CF: p < 0.0001Alpha-1 vs. COPD: p < 0.0001 Alpha-1 vs. IPF: p < 0.0001Alpha-1 vs. Sarcoidosis: p = 0.0380CF vs. COPD: p < 0.0001CF vs. IPF: p < 0.0001CF vs. IPAH: p < 0.0001CF vs. Sarcoidosis: p < 0.0001IPAH vs. IPF: p = 0.0046COPD vs. IPF: p < 0.0001
2009

ADULT LUNG TRANSPLANTATION Kaplan-Meier Survival by Gender (Transplants: January 1990 – June 2007)
0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10
Years
Su
rviv
al
(%)
Male (N=13,251)
Female (N=11,981)
HALF-LIFE Male: 5.0 years; Female: 5.4 Years
p = 0.0006
N at risk at 5 years=3,456
N at risk = 783N at risk at 5 years=3,311
N at risk = 762
ISHLT
2009

ADULT LUNG TRANSPLANTATION Kaplan-Meier Survival by Age Group (Transplants: January 1990 – June 2007)
0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10
Years
Su
rviv
al
(%)
.
18-34 (N = 4,420)35-49 (N = 6,629)50-59 (N = 9,229)60-65 (N = 4,262)66+ (N = 694)
Survival comparisonsAll p-values significant at p < 0.0001 except 18-34 vs. 35-49: p = 0.7127; 60-65 vs. 66+: p = 0.0007
HALF-LIFE 18-34: 5.9 Years; 35-49: 6.3 Years; 50-59: 5.1 Years; 60-65: 4.2 Years; 66+: 3.2 Years
ISHLT
2009












Eur J Cardiothorac Surg 2006;30:846-851



Novalung

Novalung Technical Data
ataGas exchange by diffusion across a plasma tight membrane
Heparin coated surface (ACT 120 – 140s)
Low shear stress (blood trauma)
Low resistance (6mmHg at 1.5 l/min)
Blood flow 0.5 – 4.5 L/min
Filling volume = 250 ml saline

Novalung as a bridge to lung transplantation
J Thorac Cardiovasc Surg 2006;131:719

Initianal experience with novalung as a bridge to lung transplant- Hannover Medical School
• N=12 patients • Patients with refractory respiratory failure• Hypercapnea and acidosis despite maximal conventional
ventilation• Placed on Novalung as a bridge to lung transplantation

Initianal experience with novalung as a bridge to lung transplant- Hannover Medical School
J Thorac Cardiovasc Surg 2006;131:719

Initianal experience with novalung as a bridge to lung transplant- Hannover Medical Schoo
• 10/12 patients successfully bridged to transplantation• 8/10 survived lung transplant• Cause of death : multi-organ failure• 2 prior, 2 after lung transplant

Conclusions
Lung transplantation is life saving procedure for end-stage lung diseases
Mortality on the waiting list remains a major problem Reduce the gap between demands and supply i.e increase
donor supply will decrease mortality on the waiting list Novalung is a safe and valuable option to bridge patients to
lung transplantation.

Thank you