Embed Size (px)
Citation preview

1
Lung Cancer Update
David M. Jackman, MD
Senior Physician, Lowe Center for Thoracic Oncology,
Dana-Farber Cancer Institute
Medical Director of Clinical Pathways, Dana-Farber Cancer Institute
Assistant Professor, Harvard Medical School

2
Titles: • Senior Physician, Lowe Center for Thoracic Oncology, Dana-Farber Cancer Institute
• Medical Director of Clinical Pathways, Dana-Farber Cancer Institute
• Assistant Professor, Harvard Medical School
Education and Training:• MD: Brown Medical School
• Residency, Internal Medicine: Beth Israel Deaconess Medical Center, Boston, MA
• Fellowship, Medical Oncology: Dana-Farber/Massachusetts General Hospital, Boston, MA
Specialty: • Thoracic Oncology
• Clinical Pathways and Care Delivery
David Jackman, MD

3
• I have no financial disclosures.
Disclosures

4
• Epidemiology
• Clinical Presentation, Diagnosis, Staging
• Screening
• Overview of Lung Cancer Therapy
• Sample Questions
Agenda

5
Epidemiology

6
Practice Question 1
Which of the following statements is true about cancer?
A. Breast cancer is the most common cause of cancer death in women.
B. For former smokers, it takes ~ 10 years for the risk of lung cancer to decrease to that of a nonsmoker.
C. More than half of new lung cancers are already metastatic at the time of diagnosis.
D. Tumor grade (level of differentiation under the microscope) is a more important predictor than tumor stage (extent of disease on scans)
E. Small cell lung cancer is both more aggressive and more common than non-small cell lung cancer.
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

7
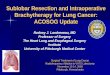
Lung Cancer is the leading cause of cancer death
PresentationScreening Lung Cancer Therapy SummaryEpidemiology
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
Death
s p
er
year
131,880
52,98048,220 44,130
LUNG
CANCER
COLON
CANCER
PANCREATIC
CANCER
BREAST
CANCERData from Cancer statistics, 2021.
Siegel et al, Ca Cancer J Clin

8
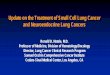
Smoking is the leading risk factor for lung cancer
Cum
ula
tive r
isk (
%)
2
4
6
8
10
12
14
5545 65 75
Continuing cigarette smokersStopped age 60Stopped age 50Stopped age 40Stopped age 30Lifelong non-smokers
Peto et al, BMJ 2000; 321 (7257): 323-9
Age
• Risk is proportional to the
amount and duration of
tobacco smoking
• Cessation lowers risk, but
it never returns to that of a
lifelong non-smoker
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

9
Non-smokers account for 10-20% of lung cancer cases in the United States
Causes of lung cancer in non-smokersAdapted from American Cancer Society Facts & Figures 2006. Special
section Environmental Pollutants.
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

10
Stage is the most important prognostic factor
Stage
Goldstraw et al, JTO 2016
Stage at
Diagnosis*
15
22
55
*Stage unknown
in 8%
SEER 2000
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

11
Impact of Lung Cancer Histology
15%
21%
34%
9%
17%
4%
Small Cell
Non-Small Cell
Squamous
Adenocarcinoma
Large
Cell
Other
NOS Small Cell Squamous Adenocarcinoma
Most Common
LocationCentral Central
Central or
Peripheral
Found in non-
smokers?Exceedingly Rare Rare Yes
Targetable
genomic
alterations
Extremely unlikely Unlikely
Possible,
especially in
nonsmokers
Classic
Paraneoplastic
Syndrome(s)
SIADH,
Cushings,
Lambert-Eaton
Hypercalcemia -
Adapted from Targeted Oncology, 11/20/17
PresentationScreening Lung Cancer Therapy SummaryEpidemiology
Non-Small Cell

12
Practice Question 1
Which of the following statements is true about cancer?
A. Breast cancer is the most common cause of cancer death in women.
B. For former smokers, it takes ~ 10 years for the risk of lung cancer to decrease to that of a nonsmoker.
C. More than half of new lung cancers are already metastatic at the time of diagnosis.
D. Tumor grade (level of differentiation under the microscope) is a more important predictor than tumor stage (extent of disease on scans)
E. Small cell lung cancer is both more aggressive and more common than non-small cell lung cancer.
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

13
Lung Cancer Screening

14
According to current USPSTF Guidelines, low-dose CT screening for lung cancer is currently recommended for which of the following asymptomatic patients?
A. A 42 year-old nonsmoking former naval midshipmen with a history of asbestos
exposure
B. A 56 year-old non-smoker whose father had died of lung cancer at age 64.
C. A 76 year-old who had smoked 1 pack per day for 30 years (from age 16-46).
D. A 70 year-old who had smoked 1 pack per day for 30 years (from age 35-65).
E. A frail 84 year-old with Class III CHF who has continued to smoke 2 packs per day
since age 14.
Practice Question 2
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

15
ABCs of Lung Cancer Screening
PresentationScreening Lung Cancer Therapy SummaryEpidemiology
BenefitAudience Calendar
• Asymptomatic adults, and
• Aged 55 to 80 years, and
• Heavy and recent
smoking history:
• > 20 pack-years, and
• Currently smoke or
quit smoking within
the past 15 years.
• Annual Low-Dose Chest
CT
• Screening should be
discontinued once a person
has not smoked for 15
years or develops a health
problem that substantially
limits life expectancy or the
ability or willingness to have
curative lung surgery.
NLST (NEJM 2011. 365: 395-409):
• 20% decrease in lung cancer
mortality
• 6.7% decrease in all cause
mortality
NELSON (de Koning et al, WCLC
2018):
• 26% decrease in lung cancer
mortality
USPSTF: Grade B

16
Follow-up of Radiographic Findings
Setting Guidelines
Screening of an asymptomatic patient LUNG-RADS1
Incidental finding on a scan performed for another
reason
Fleishner Guidelines2
Radiographic study performed as part of evaluation
of a symptomatic patient
Aggressive follow-up
1. LUNG-RADS: American College of Radiology. https://www.acr.org/-/media/ACR/Files/RADS/Lung-
RADS/LungRADSAssessmentCategoriesv1-1.pdf
2. Fleishner Guidelines: MacMahon et al, Radiology 2017.
https://pubs.rsna.org/doi/10.1148/radiol.2017161659
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

17
Screening Follow-up: LUNG-RADS
Category Definition
Risk of
Malignancy
Estimated
Population
Prevalence Recommended Follow-Up
Category 0 (incomplete)
• prior CT studies were performed, but are not available for comparison
• Part or all of lungs cannot be evaluated
N/A 1%
Comparison with prior studies
before assignment of Lung-
RADS classification
Category 1: Negative
• no lung nodules
• lung nodule(s) with specific findings favoring benign nodule(s): complete, central,
and/or popcorn calcification; calcification in concentric rings; fat-containing nodules
<1%
90%
Continue annual screening with
LDCT
Category 2: Benign appearance or behavior
• solid nodule(s)
• <6 mm at baseline
• new nodule <4 mm
• subsolid nodule(s)
• <6 mm on baseline screening
• ground glass nodule(s)
• <30 mm (Version 1.1 change previously 20 mm)
• ≥30 mm and unchanged or slowly growing (Version 1.1 change previously 20
mm)
• category 3 or 4 nodules that are unchanged for ≥3 months
< 1%
Continue annual screening with
LDCT
From 2019 LUNG-RADS from ACR
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

18
Category DefinitionRisk of
Malignancy
Estimated
Population
Prevalance
Recommended
Follow-Up
Category 3: Probably Benign
• Solid nodule(s)
• ≥6 mm to <8 mm at baseline, OR
• new nodule 4 mm to <6 mm
• Part solid nodule(s)
• ≥6 mm total diameter with solid component <6 mm, OR
• new <6 mm total diameter
• Non-solid nodule(s)
• (GGN) ≥30 mm on baseline CT or new
1-2% 5%
6-month follow-up
with LDCT
Category 4A: Suspicious
• Solid nodule(s)
• ≥8 mm to <15 mm at baseline, OR
• growing nodule(s) <8 mm, OR
• new nodule 6 mm to <8 mm
• Part solid nodule(s)
• ≥6 mm total diameter with solid component ≥6 mm to <8 mm, OR
• With a new or growing <4 mm solid component
• Endobronchial nodule
5-15% 2%
• 3-month follow-up
with LDCT
• PET/CT may be
used if there is a
≥8 mm solid
component
Screening Follow-up: LUNG-RADS From 2019 LUNG-RADS from ACR
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

19
Category DefinitionRisk of
Malignancy
Estimated
Population
Prevalence
Recommended Follow-Up
Category 4B, Very Suspicious
• Solid nodule(s)
• ≥ 15 mm at baseline, OR
• new or growing, and ≥8 mm
• subsolid nodule(s)
• solid component ≥8 mm, OR
• new or growing ≥4 mm solid component
>15% 2%
For 4B and 4X:
• Chest CT with or without
contrast, as appropriate
• PET-CT and/or tissue
sampling depending on
the probability of
malignancy and
comorbidities (PET-CT if
solid component ≥8 mm)
• For new large nodules that
develop on an annual
repeat screening CT, a 1
month LDCT may be
recommended to address
potentially infectious or
inflammatory conditions.
Category 4X, Very Suspicious
• category 3 or 4 nodules with additional features or imaging findings that increase
the suspicion of malignancy
• includes:
• spiculation
• ground glass nodule(s) that double in size in 1 year
• enlarged regional lymph nodes
>15% 2%
Category S: Other - Modifier may add on to category 0‐4 coding
• Clinically Significant or Potentially Clinically Significant Findings (non lung cancer)N/A 10%
• As appropriate to the
specific finding
Screening Follow-up: LUNG-RADSFrom 2019 LUNG-RADS from ACR
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

20
According to current USPSTF Guidelines, low-dose CT screening for lung cancer is currently recommended for which of the following asymptomatic patients?
A. A 42 year-old nonsmoking former naval midshipmen with a history of asbestos
exposure
B. A 56 year-old non-smoker whose father had died of lung cancer at age 64.
C. A 76 year-old who had smoked 1 pack per day for 30 years (from age 16-46).
D. A 70 year-old who had smoked 1 pack per day for 30 years (from age 35-65).
E. A frail 84 year-old with Class III CHF who has continued to smoke 2 packs per day
since age 14.
Practice Question 2
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

21
Clinical Presentation,
Diagnosis,
and Staging

22
A 68 year-old man with ongoing tobacco use (1ppd x 50 years) presents with worsening shortness of breath over 2 months time, along with hoarseness. CT angiogram is negative for pulmonary embolus, but it does show a large left hilar mass, along with subcarinal and left supraclavicular adenopathy and concerns for lesions in the liver and left adrenal. Serum chemistries are notable for a sodium of 124.
What is the most likely cause of hyponatremia?
Practice Question 3
A. DehydrationB. Psychogenic polydipsiaC. Syndrome of inappropriate andidiuretic hormone (SIADH)D. Laboratory error
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

23
Clinical Presentation of Lung Cancer:
PresentationScreening Lung Cancer Therapy SummaryEpidemiology
Lungs
Brain
Liver
Adrenals
Bones
Lymph Nodes
Generalized Symptoms
Symptoms related to local destruction, obstruction, or replacement
Paraneoplastic Syndromes
• Fatigue
• Weight loss
• Night sweats
• Cough
• Shortness of breath
• Hemoptysis
• SVC Syndrome
• Focal bone pain
• Fracture
• Cord Compression
• Focal CNS symptoms
• Seizure
• Altered Mental Status
• SIADH
• Paraneoplastic Cushings
• Hypercalcemia

24
CT chest with IV contrast
Lung Cancer Staging:
Mediastinal Nodes
• Mediastinal staging:
• For potentially resectable
patients
• For patients with locally
advanced disease
• How:
• Mediastinoscopy
• Bronchoscopy/EBUS
• Lymph node dissection at
the time of surgery
Lungs
Lymph Nodes
Brain MRI with gad (preferred), or
CT head with IV contrast
PET/CT (preferred), or
Bone scanBones
Liver
Adrenals
Brain
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

25
Lung Cancer Diagnosis:
ENDS
❑ Safe, timely, accurate diagnosis
❑ Obtain sufficient tissue for subsequent
biomarker studies, clinical trial eligibility
❑ Confirm spread (when applicable)
MEANS
❑ CT-guided biopsy
❑ Bronchoscopy/EBUS
❑ Mediastinoscopy
❑ Thoracentesis, other drainage
❑ Surgical procedure
❑ Other
Additional Information:
❑ Bone biopsies are usually inadequate for biomarker studies, trial eligibility. The
decalcification process that bone biopsies undergo denatures DNA.
❑ If there appears to be only a single site of spread, it should be biopsied to confirm or rule
out metastasis.
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

26
Paraneoplastic SyndromesDisease Paraneoplastic Syndrome Mechanism
Squamous NSCLC Hypercalcemia PTHrP
Small cell lung cancer Syndrome of inappropriate antidiuretic
hormone (SIADH)
Anti-diuretic hormone
(aka arginine vasopressin)
Cushing syndrome Ectopic ACTH
Lambert-Eaton Ab against voltage-gated calcium
channels
Thymoma Myasthenia gravis Ab against nicotinic acetylcholine
receptors
Pure red cell aplasia Suspect IgG against erythroblasts,
epo
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

27
A 68 year-old man with ongoing tobacco use (1ppd x 50 years) presents with worsening shortness of breath over 2 months time, along with hoarseness. CT angiogram is negative for pulmonary embolus, but it does show a large left hilar mass, along with subcarinal and left supraclavicular adenopathy and concerns for lesions in the liver and left adrenal. Serum chemistries are notable for a sodium of 124.
What is the most likely cause of hyponatremia?
Practice Question 3
A. DehydrationB. Psychogenic polydipsiaC. Syndrome of inappropriate andidiuretic hormone (SIADH)D. Laboratory error
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

28
Overview of Therapy
For Lung Cancer

29
A 66 year-old woman currently on therapy for her stage IV non-small cell lung cancer presents to her local ED with several days of worsening shortness of breath, dry cough, and low-grade fevers. CT chest is concerning for pneumonitis. Which of the following could be an explanation for these findings?
Practice Question 4
A. Alectinib (ALK inhibitor)-related pneumonitisB. Docetaxel-related pneumonitisC. Pembrolizumab (immunotherapy)-related pneumonitisD. SARS CoV2 infectionE. All of the above
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

30
Overview of Therapy for Lung Cancer
NSCLC
SCLC
Stage I
Stage II
Stage III
Stage IV
Limited
Extensive
Stage Stage Description Therapy
Limited to one lung +/- regional nodes,
in a feasible radiation portChemoradiotherapy
Anything beyond limited stage Palliative systemic therapy
Contralateral/distant spread and/or
malignant effusionPalliative systemic therapy
Even larger lung mass, and/or
mediastinum or supraclavicular nodesMultidisciplinary Therapy
Larger lung mass, and/or local/hilar
nodes
Resection +/- adjuvant
systemic therapy
Small lung mass, no spread Resection
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

31
Overview of Therapy for Lung Cancer
NSCLC
SCLC
Stage I
Stage II
Stage III
Stage IV
Limited
Extensive
Stage Stage Description Therapy
Limited to one lung +/- regional nodes,
in a feasible radiation portChemoradiotherapy
Anything beyond limited stage Palliative systemic therapy
Contralateral/distant spread and/or
malignant effusionPalliative systemic therapy
Even larger lung mass, and/or
mediastinum or supraclavicular nodesMultidisciplinary Therapy
Larger lung mass, and/or local/hilar
nodes
Resection +/- adjuvant
systemic therapy
Small lung mass, no spread Resection
PresentationScreening Lung Cancer Therapy SummaryEpidemiology
Genomically
Targeted Therapy
Chemotherapy +
Immunotherapy
Immunotherapy +
Immunotherapy
Chemotherapy

32
Role of Radiation in Lung Cancer
PresentationScreening Lung Cancer Therapy SummaryEpidemiology
The Role of Radiation in Lung CancerCurative
• Early-stage: alternative to
surgery in poor operative
candidates
• Locally advanced: with
chemotherapy as a
neoadjuvant (pre-operative)
or definitive strategy
Palliative
• To address an urgent
symptom. e.g.: cord
compression, SVC
syndrome, airway or
esophageal obstruction
• To palliate: e.g., bone
metastasis
• Brain metastases
Other
• Prophylactic cranial
irradiation (small cell)
• Consolidative chest radiation
(small cell)
• Oligo-progressive disease,
particularly for patients on
targeted tx or immunotherapy

33
FDA Approvals for Lung Cancer
PresentationScreening Lung Cancer Therapy SummaryEpidemiology
Landmark Approvals:
• 2004: The first targeted agents (gefitinib, erlotinib) are
approved for non-small cell lung cancer
• 2015: The first immunotherapy agent (nivolumab,
pembrolizumab) approved in non-small cell lung cancer

34
FDA Approvals for Lung Cancer
PresentationScreening Lung Cancer Therapy SummaryEpidemiology
Genomic alterations in lung cancer associated with an
FDA-approved targeted therapy
Mutations EGFR
BRAF V600E
KRAS G12C
MET exon 14
Fusions/Rearrangements ALK
ROS1
NTRK
RET

35
Toxicities with Targeted Therapies
PresentationScreening Lung Cancer Therapy Other Thoracic TumorsEpidemiology
Gene Agent CYP3A4?1 Selected Common Side Effects2 Selected Serious Side Effects2
EGFR 1st gen:
• erlotinib
• gefitinib
2nd gen:
• afatinib
• dacomitinib
3rd gen:
• osimertinib
Y
Y
N
Y
Y
Rash, skin dryness, diarrhea Pneumonitis/Interstitial lung disease,
hepatotoxicity, nephrotoxicity, severe
rash/mucositis, severe diarrhea.
Osimertinib: Cardiotoxicity
ALK 1st gen:
• crizotinib
2nd gen
• alectinib
• brigatinib
• ceritinib
3rd gen:
• lorlatinib
Y
Y
Y
Y
Y
Fatigue, diarrhea, nausea, visual
changes.
Crizotinib: hypogonadism
Pneumonitis, hepatotoxicity
Lorlatinib: CNS / cognitive changes
ROS1 crizotinib Y Fatigue, diarrhea, nausea, visual
changes. Hypogonadism
Pneumonitis, hepatotoxicity
BRAF Dabrafenib+trametinib Y Fever, nausea. Hepatotoxicity, cardiotoxicity. Basal cell CA
NTRK entrectonib
larotrectinib
Y
Y
Hepatotoxicity, fatigue, nausea -
MET capmatinib Y Edema, nausea, nephrotoxicity Interstitial lung disease, hepatotoxicity
RET selpercatinib Y Dry mouth, diarrhea, hepatotoxicity Hepatotoxicity, hypertension
1. Collated from www.drugs.com. 2. This is not a comprehensive list of toxicities. For more information, see prescribing info for each agent.

36
• Side effects can occur at any point in treatment course
• Can get immune-mediated toxicity of essentially any system
• Some severe but rare side effects include: pneumonitis,
hepatotoxicity, CNS toxicity, cardiotoxicity, SJS
• For severe toxicity: consult, hospitalization, steroids,
immunomodulators
Considerations with immunotherapy
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

37
A 66 year-old woman currently on therapy for her stage IV non-small cell lung cancer presents to her local ED with several days of worsening shortness of breath, dry cough, and low-grade fevers. CT chest is concerning for pneumonitis. Which of the following could be an explanation for these findings?
Practice Question 4
A. Alectinib (ALK inhibitor)-related pneumonitisB. Docetaxel-related pneumonitisC. Pembrolizumab (immunotherapy)-related pneumonitisD. SARS CoV2 infectionE. All of the above
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

38
Cancer statistics, 2020.
Siegel et al, Ca Cancer
J Clin

39
• Stage is the most important predictor of outcome
• Small cell lung cancer is the most likely to be associated
with smoking and with paraneoplastic syndromes (esp
SIADH)
• Lung cancer screening: in smokers heavy (> 20 pk-yrs)
and recent (quit within the last 15 years)
• Staging: Chest CT w/ contrast, PET/CT, Brain MRI
Take Home Points, Test Prep version
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

40
• Staging: Brain imaging needs IV contrast
• The importance of adequate tissue for diagnosis and
testing (core > FNA, non-bone > bone)
• Many targeted therapies – metabolized via CYP3A4 –
drug interactions
• Lung Cancer Screening
Take Home Points, Clinical Practice Version
PresentationScreening Lung Cancer Therapy SummaryEpidemiology

41
• Cancer statistics, 2020. Siegel et al, Ca Cancer J Clin
• www.drugs.com
• LUNG-RADS: American College of Radiology.
https://www.acr.org/-/media/ACR/Files/RADS/Lung-
RADS/LungRADSAssessmentCategoriesv1-1.pdf
• Fleishner Guidelines: MacMahon et al, Radiology 2017.
https://pubs.rsna.org/doi/10.1148/radiol.2017161659
References