Embed Size (px)
Citation preview

Annual HCAI & AMR meeting, Warsaw 2011
ValidationValidation studystudy
Maria Luisa Moro, Enrico Ricchizzi

Validity
The degree to which an assessment
measures what it is supposed to
measure

Why a validation study?
Validation of surveillance data is necessary to:
ensure its scientific credibility,
to identify methodological problems within the
surveillance programme,
to help increase compliance and participation in the
surveillance programme,
to identify data quality issues at local level.
McCoubrey J. JHI 2005

Why a validation study in HALT2?
The accuracy of infection data collection should be
measured in order to estimate the true prevalence of
infections/antimicrobial usage and to be able to
meaningfully compare countries
The gap between residents with signs/symptoms of
infection and those with infections satisfying the
modified McGeer criteria should be better understood

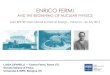
Validation studies of HAIs surveillance
Chart review by externalexperts
200100 reported NI + 100 at random
ICUsFrance
Chart review by externalexperts
148115 reported NI + 60 at random per ICU
ICUsGermany"
Chart review by externalexperts
1300All reported NI + 20% at random
ICUsBelgiumMorales I
Chart review by externalexperts, structuredinterview, capture‐recapture
39710 orthopedicoperations with, and 40 non‐SSIs
SSIFinlandHuotari, 2007
Chart review by externalexperts
8595 SSIs and the 20 most recent non‐SSIs
SSINetherlandsMannien, 2007
Chart review by externalexperts
60215 reported SSIs and 60 non‐SSIs
SSIScotlandMcCoubrey, 2005
Chart review by externalexperts
1,136All patients duringstudy period
SSIUSAEmori, 1998
Bedside inspection of allsurgical wounds
4552 consecutive prevalence studies
SSIDenmarkPoulsen, 1996
Gold standardNSamplingType ofinfectionCountryStudy, year

Validation study: how to organize it?• Bedside validation
– retrospective chart review by trained experts Advantages: higher number of patients may be reviewed; no influence on ongoing surveillance
Disadvantages: undocumented information cannot be retrieved; depending on quality of patient charts
– parallel prospective collection by trained expertsAdvantages: presence of clinical caregivers and additional information on the patient or treatment not recorded in the chart
Disadvantages: lower number of patients may be reviewed; may influence parallel data retrieval by local surveyors
• Validation by case studies
• Capture‐recapture (different data soruces)
Annual HCAI & AMR meeting, Warsaw 2011

Carley S, Emerg Med J 2005
Simple nomograms to calculate sample size in diagnostic studies

Validation study: how to organize it?
What should be validated
• quality of data collection (completeness and reliability)
• interpretation of the criteria for assessing an infection
(sensitivity and specificity)
Annual HCAI & AMR meeting, Warsaw 2011

Gold standard
• Truth (100% sensitivity and specificity)
• The best available method in applying surveillance
criteria (consistency, reliability, accuracy)


Pilot validation protocolacute care hospitals PPS
Different methods will be tested:
• Validation of HAI reported during the PPS (during the PPS or after the PPS day‐shortly or longer time after)
• Inter‐rater agreement
• Validation and accurateness of denominatordata
• Other “validation” methods: online case studies

ECDC Pilot validation study – acute care hospitals

• a validation team visited the nursing
homes in May or June 2010 and
assessed blinded, based on information
of nurses, all residents of the
participating nursing homes on having
an infection (gastro‐enteritis, influenza‐
like illness and probable pneumonia).
• Just before the visit, the local
surveyors had to fill in the register form
indicating specific infections of the
residents.
• The outcome measures are the
negative predictive value, positive
predictive value and the inter‐rater
agreement using Cohen’s kappa
coefficient.

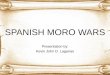
• Gastroenteritis (n=5):Sensitivity: 80%PPV: 0.67Specificity: 99.8%NPV: 1.00
• Influenza‐like illness (n=2):Sensitivity: 0%PPV: 0Specificity: 100%NPV: 1.00
• Probable pnumonia (n=5):Sensitivity: 20%PPV: 0.25Specificity: 99.8%NPV: 1.00
N = 1429 residents

Validation study in LTCFs
The variable quality of resident charts does not
allow to conduct retrospective data collection
The average size and the prevalence rate of the
LTCFs requires a large number of facilities to
reach the sample size required to assess precisely
the sensitivity and specificity

Validation study: what
Facility form: structure and
process indicators
Aggregated data:
demographic characteristics,
care load & risk factors
Infections and antimicrobial
use

Validation study: gold standard
The reference or gold standard is the HALT2
protocol and codebook, applied by a
validation team of at least one trained expert
from (and/or acting on behalf of) the
national/ regional PPS coordinating centre
(external to the validated NH), accompanied
by a LTCF staff member.
ECDC Pilot validation study – acute care hospitals

National/regional validation team
• Trained staff of the PPS coordinating centre:– At least 1 senior expert with experience in HAI surveillance
(especially case definitions) in charge of the “gold standard” data collection
– Less experienced surveillance staff can joint the VT to speed up the data collection process
• Hospital staff: the hospital staff member does not participate in the validation process/data collection as such, but he/she is crucial to:– At the start of the VT visit, introduce the VT to other hospital staff
members where needed, have a short explanatory meeting with the VT, explain how the PPS was performed in the hospital, explain the hospital information system
– Ensure that the VT is provided access to all relevant data sources, at least to the information of the patients which were selected in the validation sample
– Accompany the VT to the different wards and introduce the VT
ECDC Pilot validation study – acute care hospitals

Validation study: how
Parallel data collection
• an external trained expert will visit a random
sample of LTCFs the PPS day
• the data collection will be blinded from the
local surveyors
Pilot validation study – Long Term Care Facilities

Validation study: how
Timing of data collection
• Simultaneous validation: same day in same
ward, after the primary data collection, good
approximation of the availability of results at
the time of the survey
Pilot validation study – Long Term Care Facilities

Validation study: howBlinded collection
• Results of PPS data collectors are not disclosed during or immediately after the validation of a patient, but only at the end of the complete validation data collection in the ward
Pilot validation study – Long Term Care Facilities
Advantage:
• Better guarantee for independent data collection
• Random sampling of patients
• Can be done at the same time as the primary data collection
Disadvantage:
• No indication of which data were found by the primary data collectors and that should be verified by the VT – therefore the quality of the validation may be less good than in the semi‐blinded method
• No differential sampling possible (eg all positives) to improve precision of specificity estimation
• Possibly more time consuming

Validation study: what
Facility form: structure and
process indicators
Aggregated data:
demographic characteristics,
care load & risk factors
Infections and antimicrobial
use

Validation study: what
Facility form: structure and
process indicators
The external surveyor will assess presence of item that can be documented by NH staff (e.g.. presence of written protocol, both written that electronic, etc.)

Validation study:Institutional questionnaire
Structure and process indicators
D – INFECTION CONTROL PRACTICE IN THE FACILITY
4. Which of the following tasks are in operation in the facility?
□ Registration of residents colonized/infected with multi‐resistant microorganisms
□ Feedback on surveillance results to the nursing/medical staff of the facility
8. In the facility, is a written protocol available for:
□ the management of MRSA carriers?
□ hand hygiene?
□ the management of urinary catheters?
□ the management of venous catheters/lines?
□ the management of enteral feeding?

Validation study:Institutional questionnaire
Structure and process indicators
E – ANTIBIOTIC POLICY
4. Which of following elements are present/available in the facility?□ written guidelines for appropriate AB use (good practice) in the facility□microbiological samples taken for guidance of best AB choice□ permission from a designated person(s) for prescribing of restricted Abs, not included in local formulary □ therapeutic formulary, comprising a list of antibiotics□ feedback to the GPs on AB consumption in the facility
5. If written therapeutic guidelines are present in the facility, are they on:□ Respiratory tract infections?□ Urinary tract infections?□Wound and soft tissue infections?

Validation study: what
Facility form: structure and
process indicators
Aggregated data:
demographic characteristics,
care load & risk factors
Infections and antimicrobial
use

Validation study:Institutional questionnaire
Care load & Risk factors
• Representative random sample of eligible population
• Which data will be collected using medical and nursing documentation & staff interviews:
• care load factors
• risk factors
• Data will be collected using the Resident questionnaire
This allows to simultaneously assess both the reliability of aggregated data and the presence of false negative cases

Validation study: what
Facility form: structure and
process indicators
Aggregated data:
demographic characteristics,
care load & risk factors
Infections and antimicrobial
use

Validation study:Resident questionnaire
Antibiotics and Infections
• All cases identified within the residents random sample (care load & risk factors) with signs & symptoms of infection or atb treatment + All cases detected by the internal surveyor
• Blinded data collection
• Data collection from clinical records and NH staff (not performing survey)

Validation study:Resident questionnaire
Antibiotics and Infections • Data collection of resident data:resident case mix must match the case mix recorded in the ward list!

Validation study:Resident questionnaire
• Data on therapeutic use of ATB:if the antibiotics use is reported infections signs and symptoms should be recorded!

Validation study:Resident questionnaire
• McGeer criteria for definition of infection:use of modified McGeer checklist to report signs and symptoms of infection and confirm HAI.

Validation study:Resident questionnaire
Antibiotics and Infections
• Infections: the external surveyor will decide for each infection if it satisfies Modified McGeer criteria, or not, or if it is impossible to judge from the available information
• Additional information on the quality of clinical records:
All the information used for the definition of infections were present in the clinical record
Some or all the information were collected from staff

Validation study:
pilot study
• LTCFs
• December 2011 ‐ February 2012
• 18 Italian NH, ranging from 20 to 190 beds
• Total population of 1200 residents
• No experience in PPS and Infection surveillance
One day course on surveillance and HALT protocol
No previous experience on HALT survey

Validation study:pilot study
•External surveyor: Geriatric specialist trainee
•Experience in infections and antibiotics survey
•Trained on the HALT protocol and definitions
•Data collection:
•Representative random sample of LTCF eligible population
•Aid of LTCF contact point

Discussion
Annual HCAI & AMR meeting, Warsaw 2011
• Sustainability at the European level of a parallel
validation study with an external reviewer?
• Feasable sample size (low prevalence + small
facilities + few facilities enrolled in each country)?
• Other possible validation approaches (eg case
studies)?