Embed Size (px)
Citation preview
CC-1
Psychopharmacologic Drugs Advisory Committee MeetingMarch 27, 2018
LUCEMYRA (lofexidine)
Cl
O
Cl
HN
N

CC-2
Kristen Gullo
Vice President, Development & Regulatory AffairsUS WorldMeds
LUCEMYRA (lofexidine)
CC-3
AgendaTopic Speaker, Affiliation
Medical LandscapeLouis Baxter, MD, DFASAM, DABAMExecutive Medical DirectorProfessional Assistance Program of NJ, Inc.
Lofexidine DevelopmentKristen GulloVice President, Pharmaceutical Development & Regulatory AffairsUS WorldMeds
Lofexidine Trial ProgramMarc Fishman, MDMedical Director, Maryland Treatment CentersAssistant Professor, Johns Hopkins University School of Medicine
EfficacyCharles Gorodetzky, MD PhDConsultant in Pharmaceutical MedicineUS WorldMeds
SafetyMark Pirner, MD PhDSenior Medical DirectorUS WorldMeds
Clinical Perspective & Benefit-Risk
Thomas Kosten, MD Waggoner Chair and Professor of Psychiatry and PharmacologyBaylor College of Medicine
CC-4
Louis E. Baxter, Sr., MD, DFASAM, DABAMExecutive Medical DirectorProfessional Assistance Program of NJ, Inc.Assistant Clinical Professor of MedicineRutgers New Jersey Medical School Newark, NJCo-Program Director Addiction Medicine FellowshipHoward UniversityPast PresidentAmerican Society of Addiction MedicineDirector, Addiction Medicine Foundation (ABAM)
Medical Landscape
CC-5
Physical Dependence on Opioids
Prolonged exposure Chemical changes in the brainPhysical dependence developsOpioid discontinuation leads to withdrawalOpioid Withdrawal Syndrome
CC-6
Opioid Withdrawal Syndrome (OWS): Potential Symptoms
Sleep problems Muscle aches Heart racing Hypertension Runny nose Agitation Yawning Tearing Sweating
Fever Nausea Vomiting Diarrhea Stomach cramps Gooseflesh Depression Drug craving Anxiety
CC-7
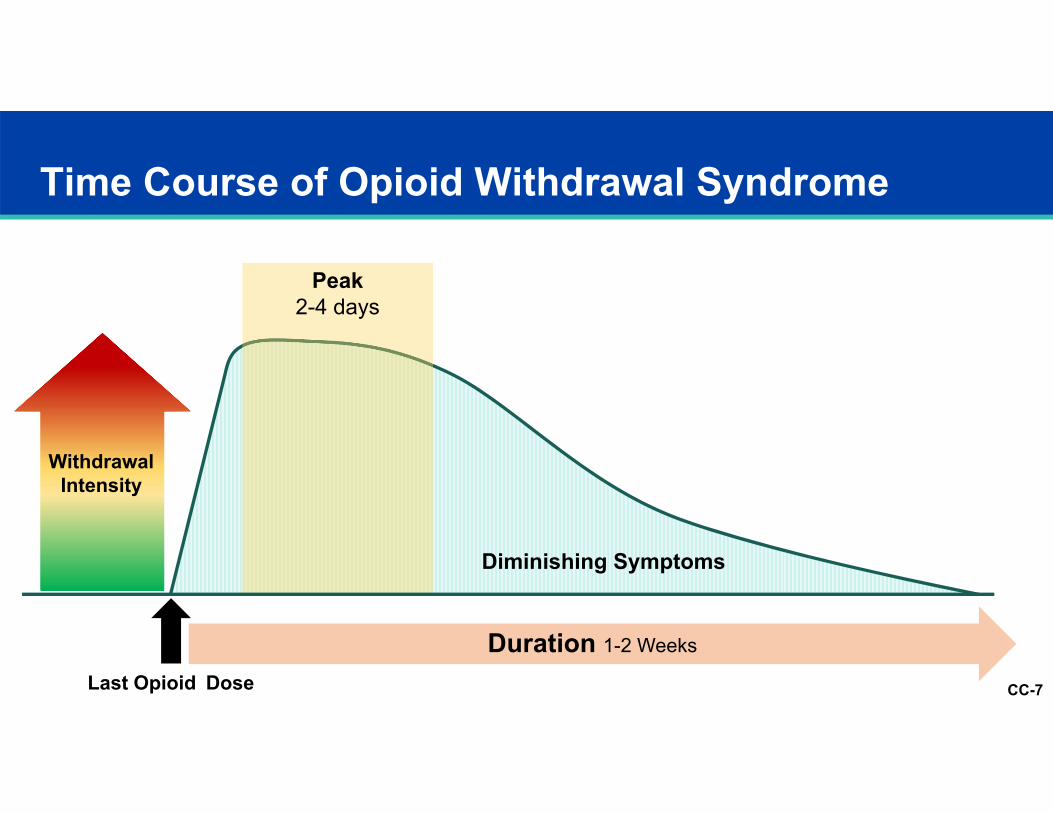
Duration 1-2 Weeks
Time Course of Opioid Withdrawal Syndrome
Last Opioid Dose
Withdrawal Intensity
Diminishing Symptoms
Peak 2-4 days
CC-8
OWS Perpetuates Opioid Use Prescription Opioid Addiction Treatment Study (POATS study)1
653 opioid dependent patients with and without chronic pain Assessed multiple factors influencing initial and current opioid use Avoiding withdrawal was the single highest rated reason for current
opioid use
1. Weiss R.D. et. al. J Subst Abuse Treat. 2014 August; 47(2):140–145.
CC-9
Withdrawal Management Overcomes Barrier of Opioid Withdrawal Syndrome
Opioid Dependence Post-Withdrawal
TreatmentOpioid Withdrawal
WithdrawalManagement
CC-10
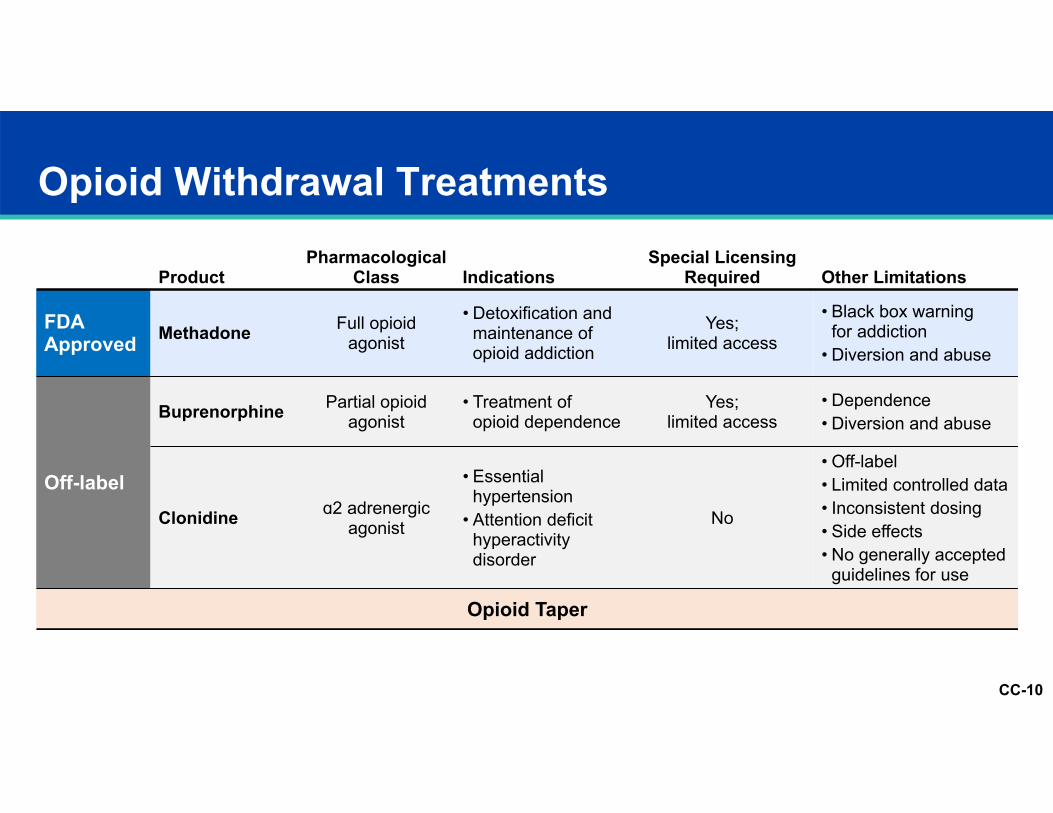
Opioid Withdrawal Treatments
ProductPharmacological
Class IndicationsSpecial Licensing
Required Other Limitations
FDA Approved Methadone Full opioid
agonist
• Detoxification and maintenance of opioid addiction
Yes; limited access
• Black box warningfor addiction
• Diversion and abuse
Off-label
Buprenorphine Partial opioid agonist
• Treatment of opioid dependence
Yes; limited access
• Dependence• Diversion and abuse
Clonidine ɑ2 adrenergic agonist
• Essential hypertension
• Attention deficit hyperactivity disorder
No
• Off-label• Limited controlled data• Inconsistent dosing• Side effects• No generally accepted
guidelines for use
Opioid Taper
CC-11
Unmet Medical Need
Non-opioid, FDA-approved treatment for management of opioid withdrawal
Evidence-based treatment guidelines for management of withdrawal
Proven and accessible treatments available to wider range of health care professionals and their patients
CC-12
Patient Selection Considerations
Motivation to discontinue opioids
Availability of caregiver support system appropriate to planned treatment setting
Appropriate expectations
Demonstrates understanding physician instructions for treatment
Planned post-withdrawal treatment, when appropriate
CC-13
Importance of Withdrawal Management
When OWS presents a barrier to discontinuing opioids, withdrawal management is required
Successful OWS management retains patients through opioid withdrawal, and into post-withdrawal care
Patients face significant risks when opioid withdrawal fails
CC-14
Kristen Gullo
Vice President, Development & Regulatory AffairsUS WorldMeds
Introduction to LUCEMYRA (lofexidine) Development
CC-15
Lofexidine (LUCEMYRA) First non-opioid medication developed for use in opioid
withdrawal management Selective α2 receptor agonistNo other clinically relevant receptor activity, including those
commonly associated with abuse potential
Proposed indicationsMitigation of symptoms associated with opioid withdrawalFacilitation of completion of opioid discontinuation treatment
Recommended dosage3.2 mg/day (4 x 0.2 mg, administered QID) for 7 daysAdditional 7 days with dosing guided by symptoms
CC-16
Lofexidine History Long history of use of α2 agonists for OWS Early lofexidine studies in OWS showed favorable results 25 years of use experience in UKSupports favorable benefit:risk of lofexidine in OWSNICE guidelines provide specific recommendation for lofexidine in OWS
USWM led US development in collaboration with National Institute on Drug Abuse (NIDA)US WorldMeds sponsored IND since 2003Key NIDA support milestones in 2006, 2010 and 2012 Full NCE development package: CMC, nonclinical and clinical programs
CMC=Chemistry, Manufacturing and Controls; NCE=New Chemical Entity; NICE=National Institute for Health and Care Excellence
CC-17
Clinical Development Overview 24 total clinical studies 16 clinical pharmacology studies Phase 3 programStudy 1 (supporting efficacy)Study 2 (pivotal)Study 3-1 (pivotal)Study 3-2 (open-label safety)
Safety database1276 patients received lofexidine1104 opioid-dependent patients
CC-18
Neurobiology of Withdrawal Opioid withdrawal characterized by symptomatology driven by
increased levels of norepinephrine Driven by complex changes in brain associated with opioid
dependence, wherein brain has achieved equilibrium in presence of opioids
When opioids no longer present in dependent patient, predictable and rapid disruption of brain equilibrium occurs
Causes extreme physical and emotional distress, encouraging return to opioid use
CC-19
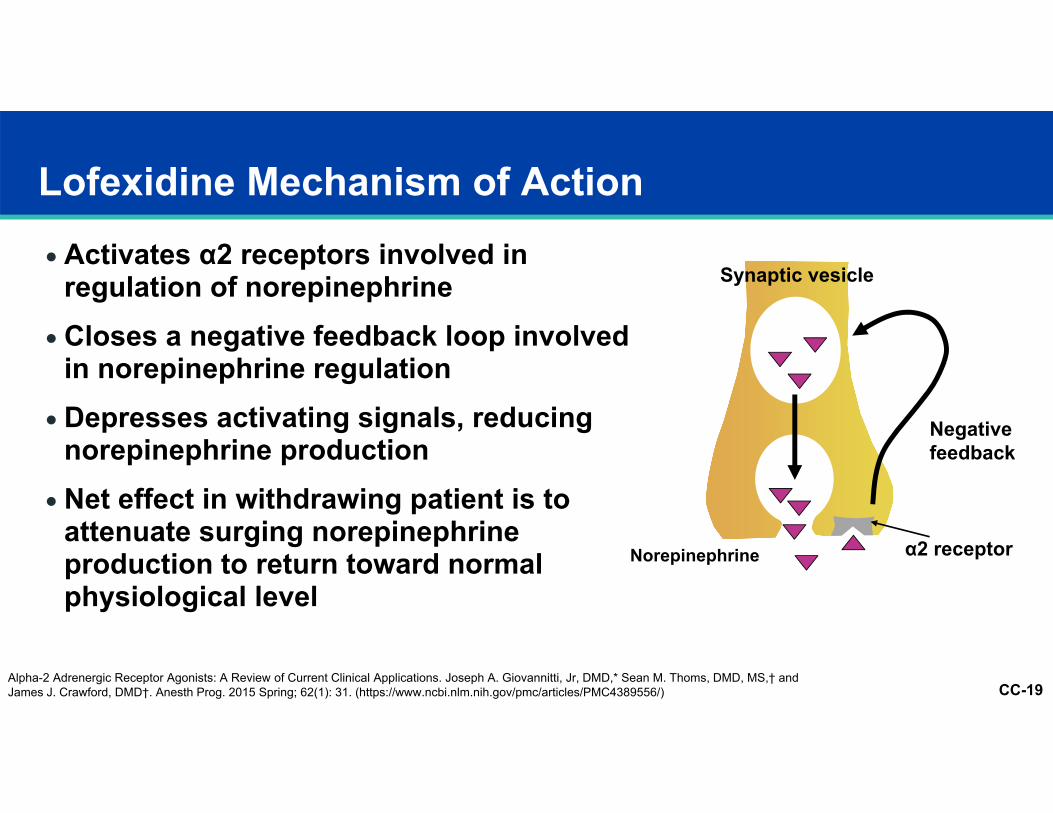
Lofexidine Mechanism of Action Activates α2 receptors involved in
regulation of norepinephrine Closes a negative feedback loop involved
in norepinephrine regulation Depresses activating signals, reducing
norepinephrine production Net effect in withdrawing patient is to
attenuate surging norepinephrine production to return toward normal physiological level
Synaptic vesicle
Norepinephrine
Negative feedback
α2 receptor
Alpha-2 Adrenergic Receptor Agonists: A Review of Current Clinical Applications. Joseph A. Giovannitti, Jr, DMD,* Sean M. Thoms, DMD, MS,† and James J. Crawford, DMD†. Anesth Prog. 2015 Spring; 62(1): 31. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4389556/)
CC-20
Marc Fishman, MD
Medical Director, Maryland Treatment CentersAssistant Professor, Johns Hopkins University School of Medicine
Lofexidine Trial Program
CC-21
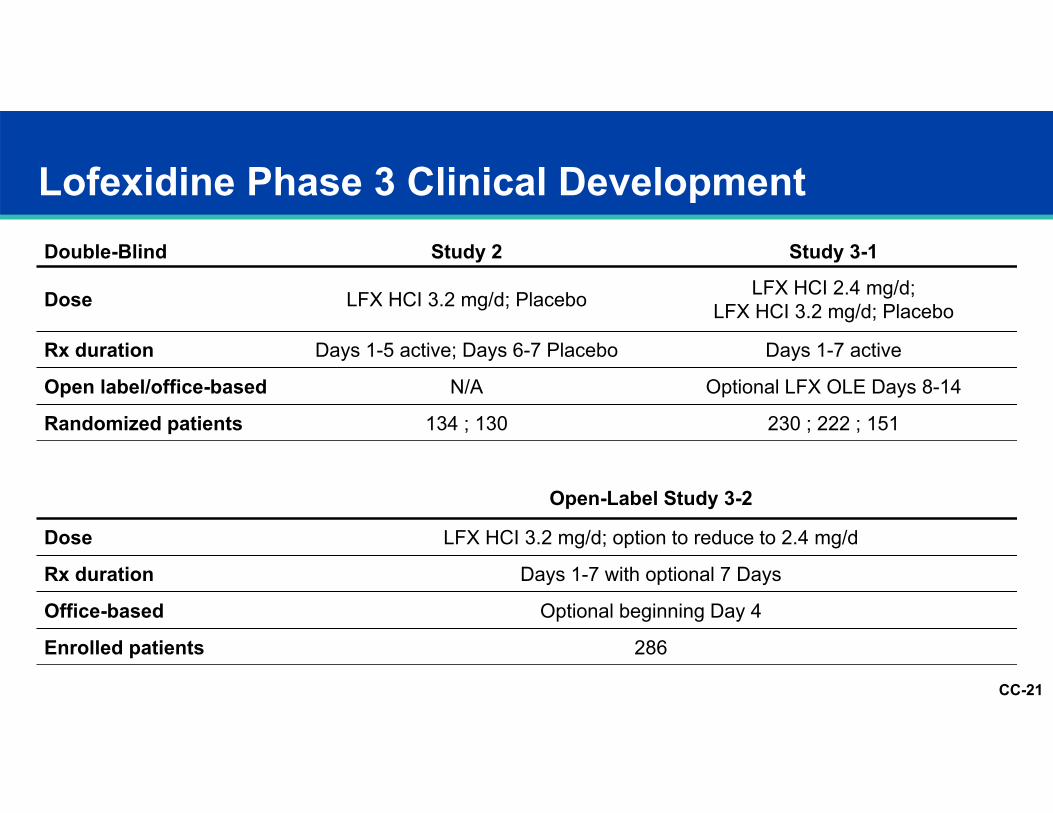
Double-Blind Study 2 Study 3-1
Dose LFX HCI 3.2 mg/d; Placebo LFX HCI 2.4 mg/d; LFX HCI 3.2 mg/d; Placebo
Rx duration Days 1-5 active; Days 6-7 Placebo Days 1-7 active
Open label/office-based N/A Optional LFX OLE Days 8-14
Randomized patients 134 ; 130 230 ; 222 ; 151
Lofexidine Phase 3 Clinical Development
Open-Label Study 3-2
Dose LFX HCI 3.2 mg/d; option to reduce to 2.4 mg/d
Rx duration Days 1-7 with optional 7 Days
Office-based Optional beginning Day 4
Enrolled patients 286
CC-22
Bed-based care settings because of demands of research protocol Heterogeneity of sitesAcademic research unitsCommunity treatment programsPrivate clinical research centers
Site Characteristics
CC-23
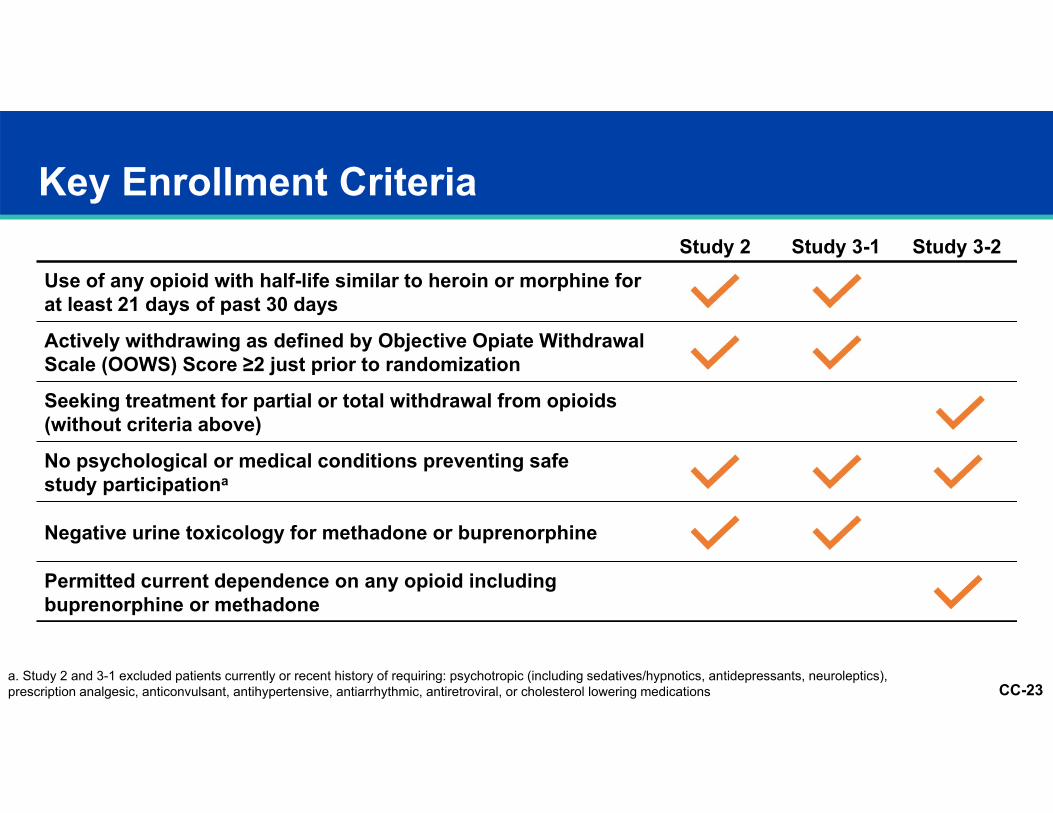
Study 2 Study 3-1 Study 3-2Use of any opioid with half-life similar to heroin or morphine for at least 21 days of past 30 days
Actively withdrawing as defined by Objective Opiate Withdrawal Scale (OOWS) Score ≥2 just prior to randomization
Seeking treatment for partial or total withdrawal from opioids(without criteria above)
No psychological or medical conditions preventing safe study participationa
Negative urine toxicology for methadone or buprenorphine
Permitted current dependence on any opioid including buprenorphine or methadone
Key Enrollment Criteria
a. Study 2 and 3-1 excluded patients currently or recent history of requiring: psychotropic (including sedatives/hypnotics, antidepressants, neuroleptics), prescription analgesic, anticonvulsant, antihypertensive, antiarrhythmic, antiretroviral, or cholesterol lowering medications
CC-24
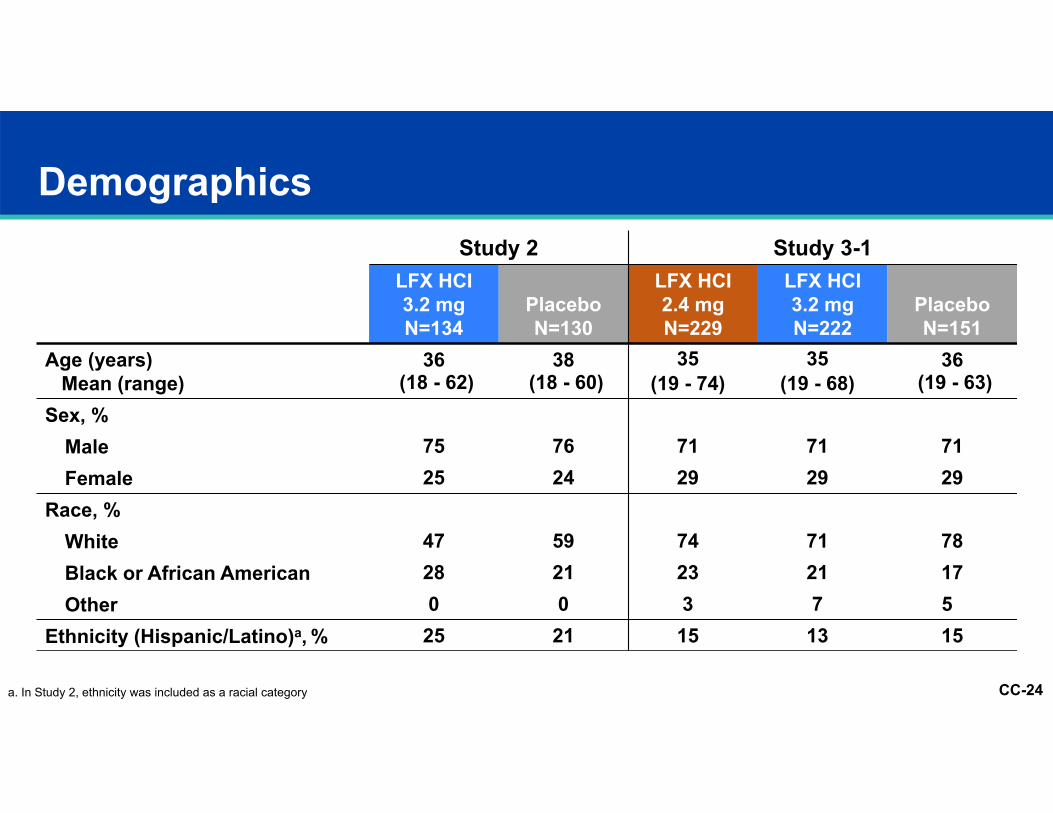
Study 2 Study 3-1LFX HCI3.2 mgN=134
PlaceboN=130
LFX HCI2.4 mgN=229
LFX HCI3.2 mgN=222
PlaceboN=151
Age (years)Mean (range)
36(18 - 62)
38(18 - 60)
35 (19 - 74)
35(19 - 68)
36(19 - 63)
Sex, %Male 75 76 71 71 71Female 25 24 29 29 29
Race, %White 47 59 74 71 78Black or African American 28 21 23 21 17Other 0 0 3 7 5
Ethnicity (Hispanic/Latino)a, % 25 21 15 13 15
Demographics
a. In Study 2, ethnicity was included as a racial category
CC-25
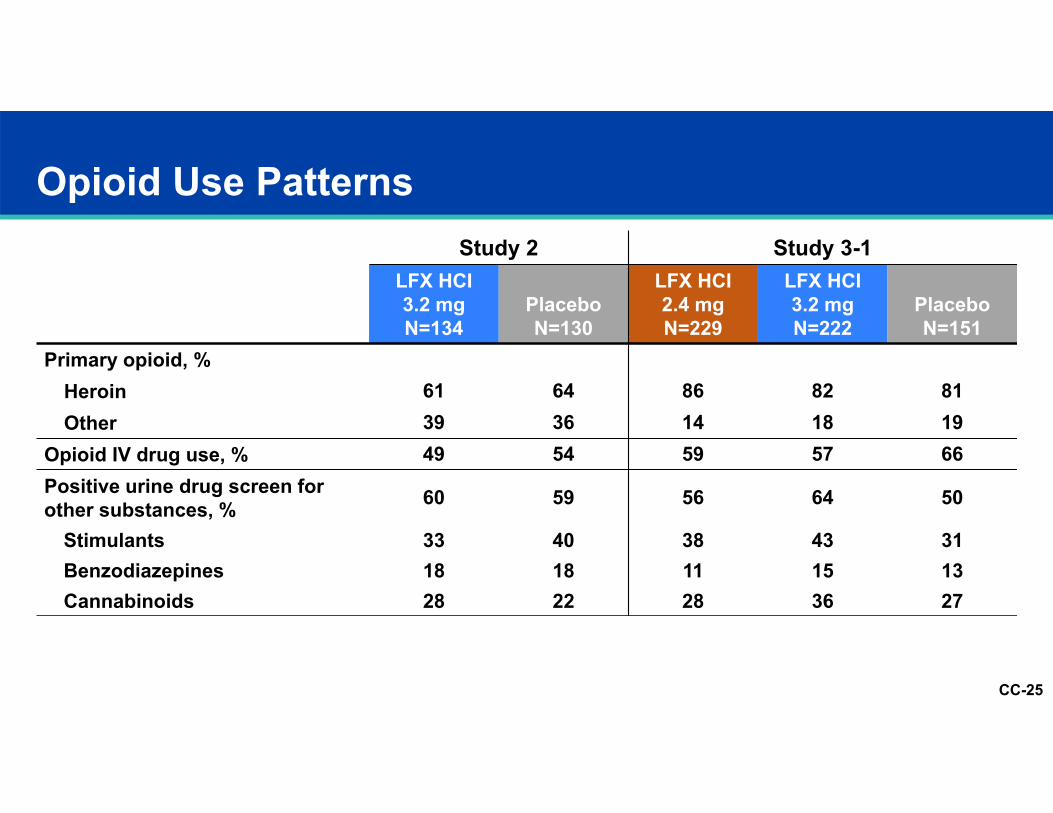
Opioid Use PatternsStudy 2 Study 3-1
LFX HCI3.2 mgN=134
PlaceboN=130
LFX HCI2.4 mgN=229
LFX HCI3.2 mgN=222
PlaceboN=151
Primary opioid, %Heroin 61 64 86 82 81Other 39 36 14 18 19
Opioid IV drug use, % 49 54 59 57 66Positive urine drug screen for other substances, % 60 59 56 64 50
Stimulants 33 40 38 43 31Benzodiazepines 18 18 11 15 13Cannabinoids 28 22 28 36 27
CC-26
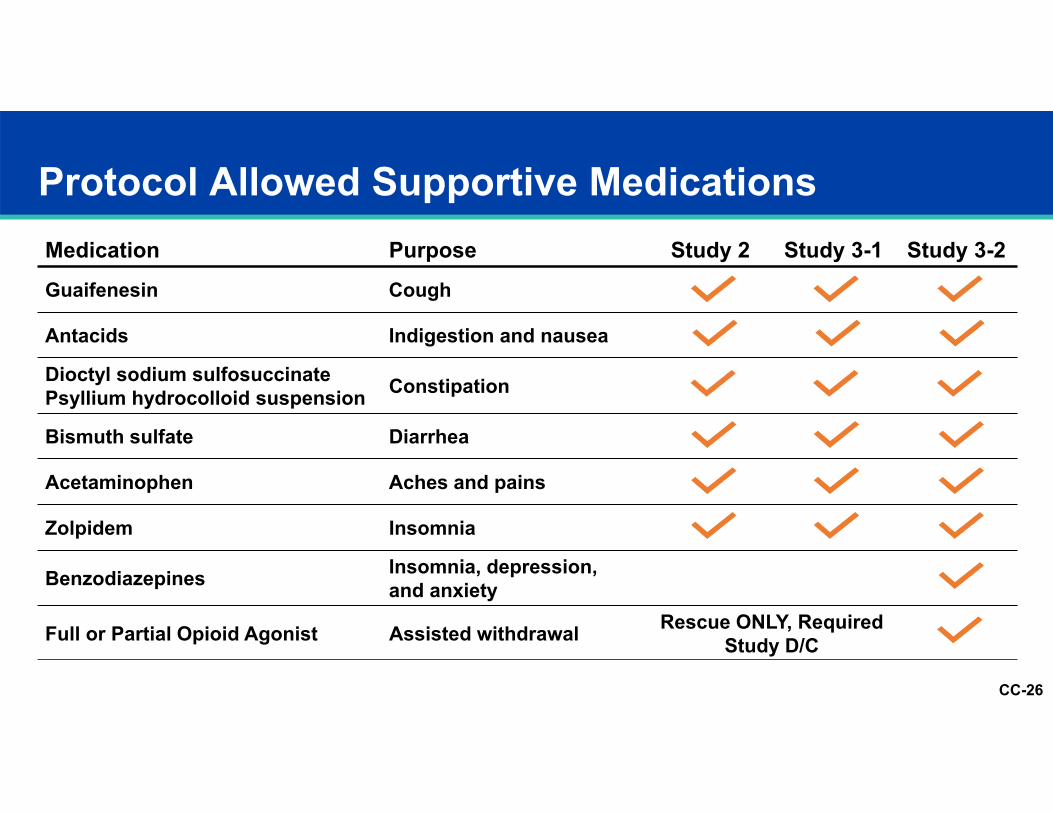
Protocol Allowed Supportive MedicationsMedication Purpose Study 2 Study 3-1 Study 3-2Guaifenesin Cough
Antacids Indigestion and nausea
Dioctyl sodium sulfosuccinatePsyllium hydrocolloid suspension Constipation
Bismuth sulfate Diarrhea
Acetaminophen Aches and pains
Zolpidem Insomnia
Benzodiazepines Insomnia, depression,and anxiety
Full or Partial Opioid Agonist Assisted withdrawal Rescue ONLY, Required Study D/C
CC-27
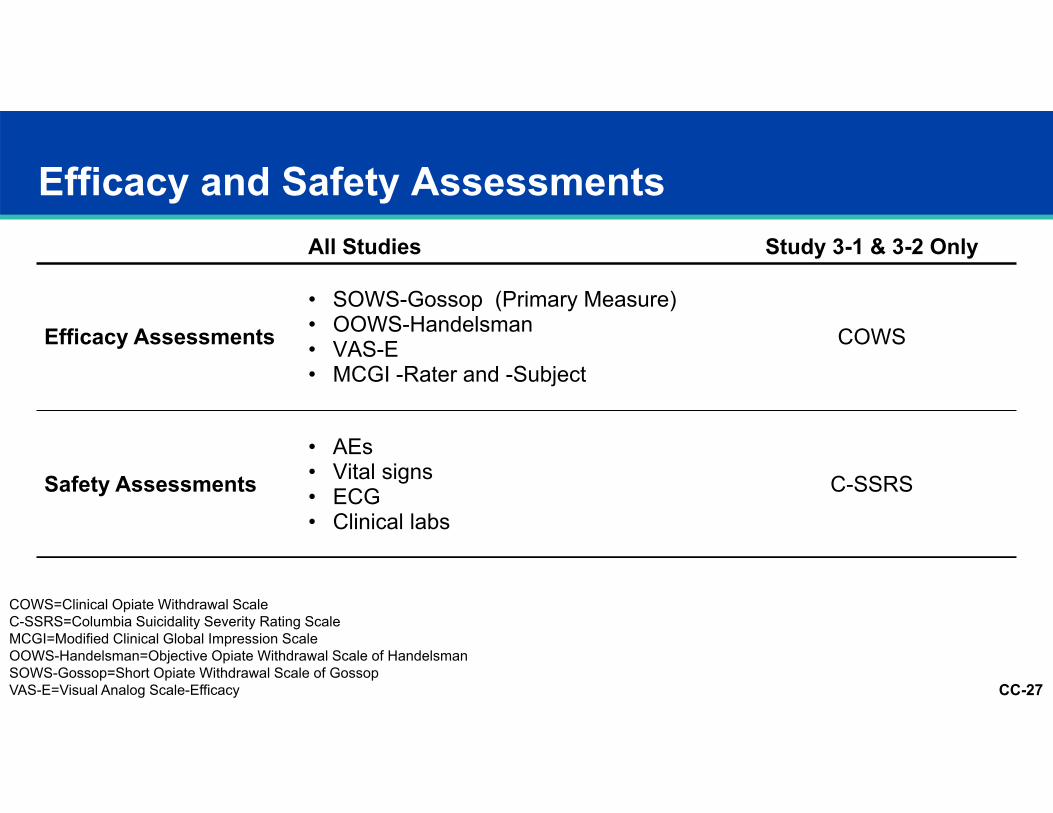
All Studies Study 3-1 & 3-2 Only
Efficacy Assessments• SOWS-Gossop (Primary Measure)• OOWS-Handelsman• VAS-E• MCGI -Rater and -Subject
COWS
Safety Assessments• AEs• Vital signs• ECG• Clinical labs
C-SSRS
Efficacy and Safety Assessments
COWS=Clinical Opiate Withdrawal ScaleC-SSRS=Columbia Suicidality Severity Rating ScaleMCGI=Modified Clinical Global Impression ScaleOOWS-Handelsman=Objective Opiate Withdrawal Scale of HandelsmanSOWS-Gossop=Short Opiate Withdrawal Scale of GossopVAS-E=Visual Analog Scale-Efficacy
CC-28
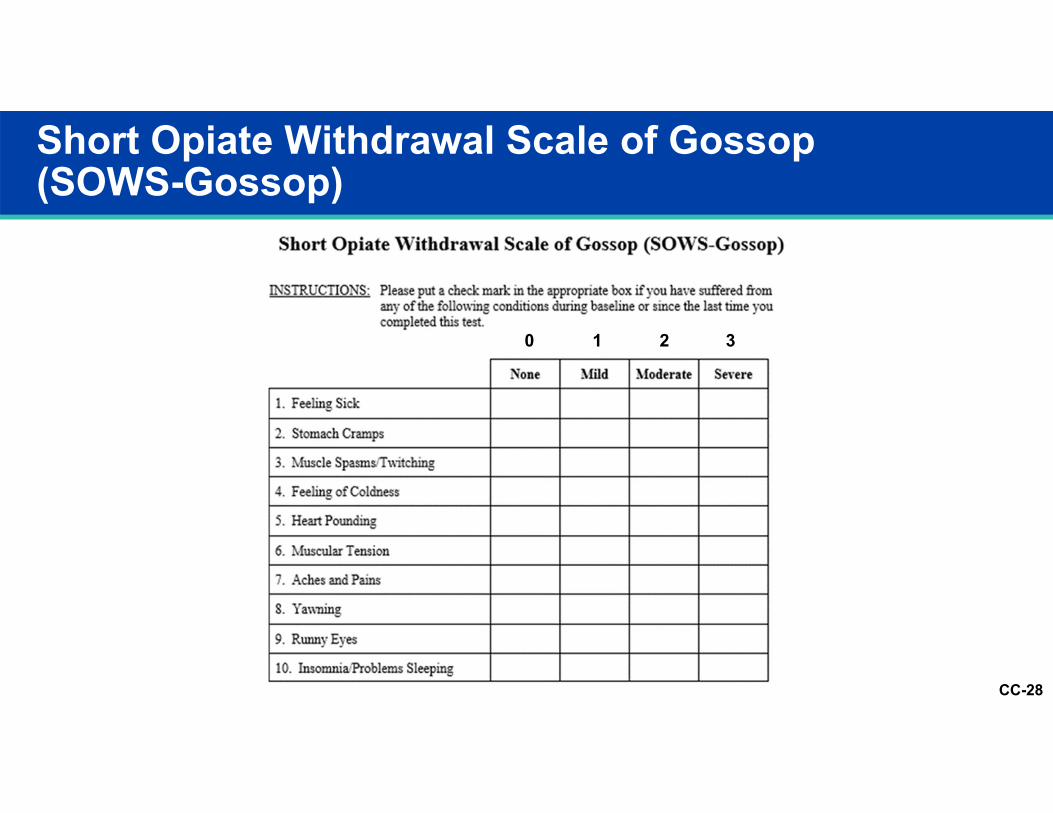
Short Opiate Withdrawal Scale of Gossop (SOWS-Gossop)
0 1 2 3
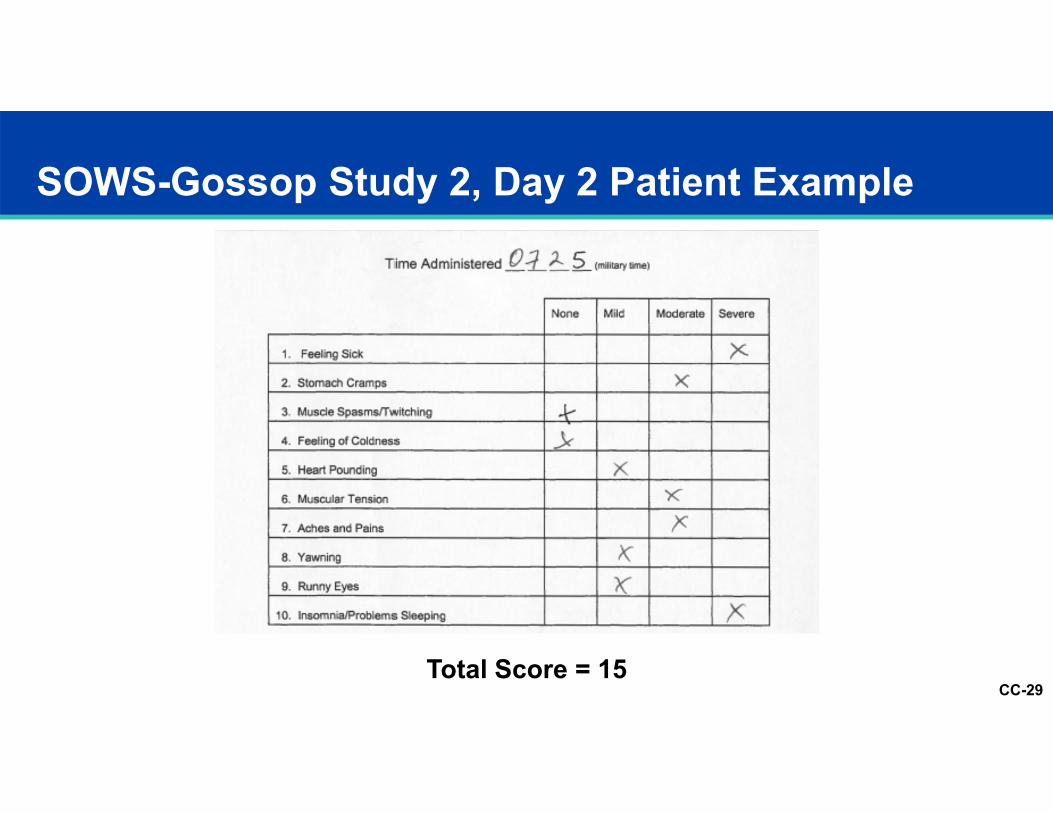
CC-29
SOWS-Gossop Study 2, Day 2 Patient Example
Total Score = 15
CC-30
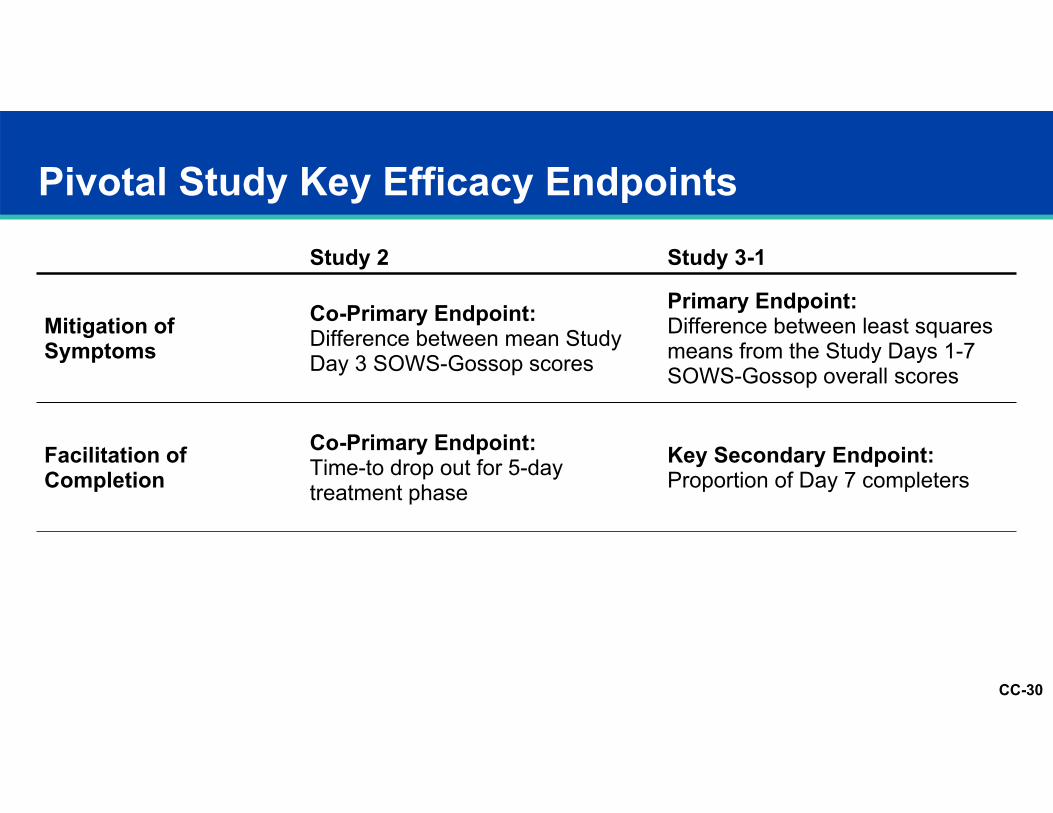
Pivotal Study Key Efficacy EndpointsStudy 2 Study 3-1
Mitigation of Symptoms
Co-Primary Endpoint: Difference between mean Study Day 3 SOWS-Gossop scores
Primary Endpoint: Difference between least squares means from the Study Days 1-7 SOWS-Gossop overall scores
Facilitation of Completion
Co-Primary Endpoint: Time-to drop out for 5-day treatment phase
Key Secondary Endpoint: Proportion of Day 7 completers
CC-31
Charles W. Gorodetzky, MD, PhD
Principal Investigator, Lofexidine Clinical TrialsConsultant, Pharmaceutical Medicine
Efficacy Results
CC-32
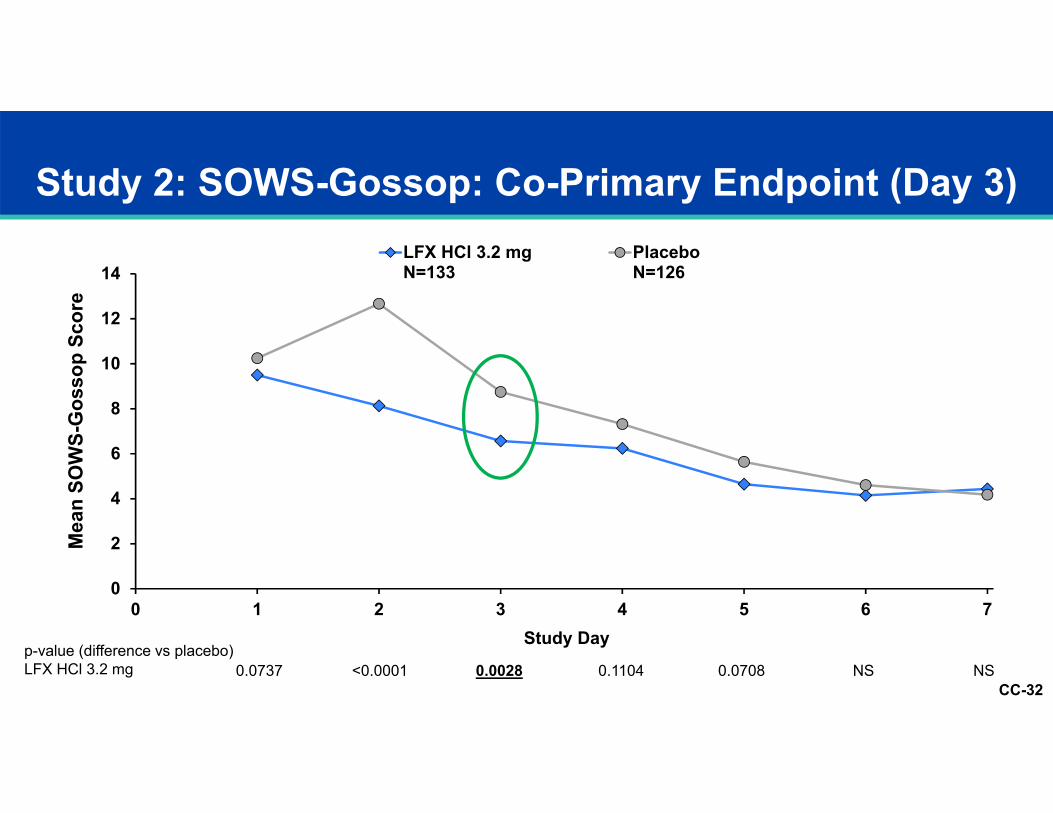
Study 2: SOWS-Gossop: Co-Primary Endpoint (Day 3)
0
2
4
6
8
10
12
14
0 1 2 3 4 5 6 7
Mea
n SO
WS-
Gos
sop
Scor
e
Study Day
LFX HCl 3.2 mgN=133
PlaceboN=126
0.0737 <0.0001 0.0028 0.1104 0.0708 NS NSp-value (difference vs placebo)LFX HCl 3.2 mg
CC-33
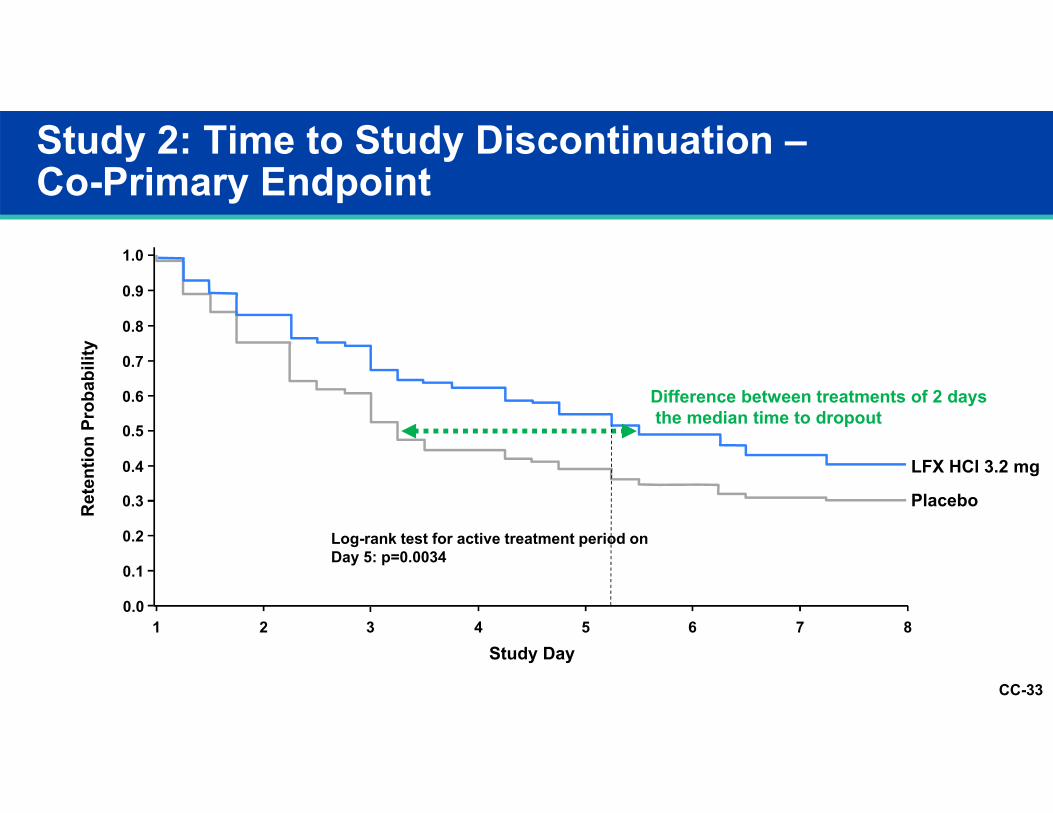
Log-rank test for active treatment period on Day 5: p=0.0034
LFX HCl 3.2 mg
Placebo
Difference between treatments of 2 days the median time to dropout
Study 2: Time to Study Discontinuation –Co-Primary Endpoint
1
1.0
0.9
0.8
0.7
0.6
Ret
entio
n Pr
obab
ility
0.4
0.3
0.5
0.2
0.1
0.02 3 4 5 6 7
Study Day8
CC-34
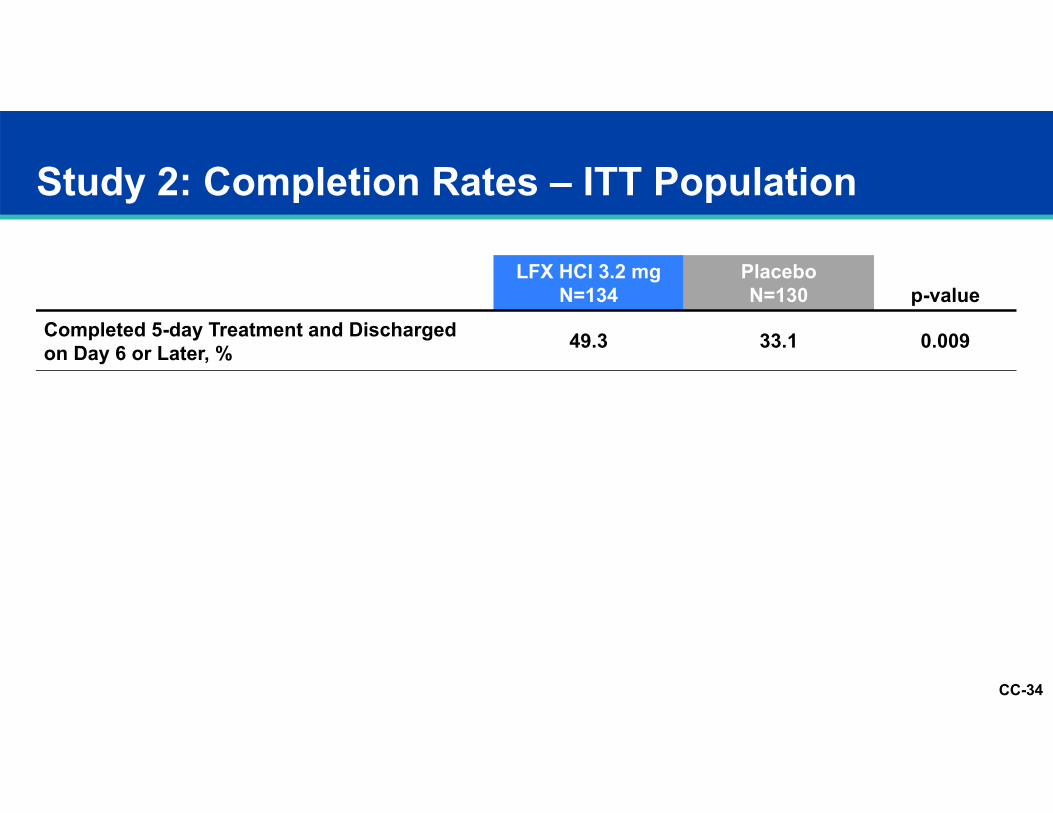
Study 2: Completion Rates – ITT Population
LFX HCl 3.2 mgN=134
PlaceboN=130 p-value
Completed 5-day Treatment and Discharged on Day 6 or Later, % 49.3 33.1 0.009
CC-35
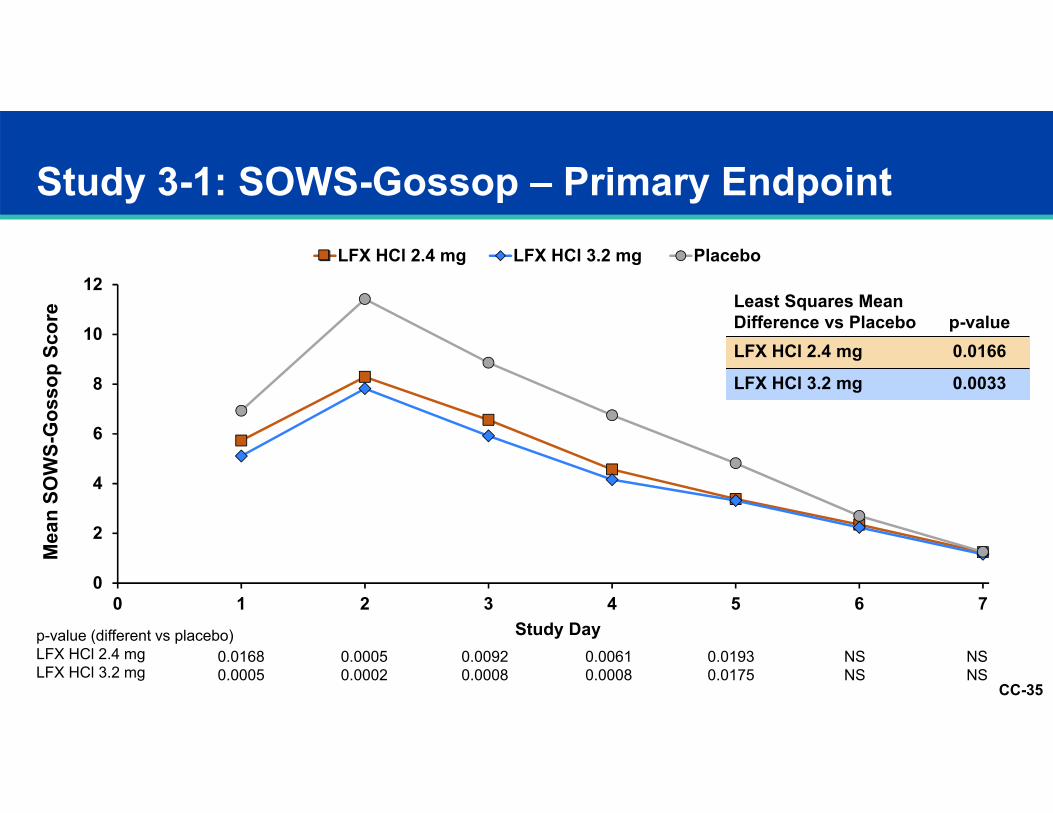
p-value (different vs placebo)LFX HCl 2.4 mgLFX HCl 3.2 mg
0.01680.0005
0.00050.0002
0.00920.0008
0.00610.0008
0.01930.0175
NSNS
NSNS
Study 3-1: SOWS-Gossop – Primary Endpoint
0
2
4
6
8
10
12
0 1 2 3 4 5 6 7
Mea
n SO
WS-
Gos
sop
Scor
e
Study Day
LFX HCl 2.4 mg LFX HCl 3.2 mg Placebo
Least Squares MeanDifference vs Placebo p-valueLFX HCl 2.4 mg 0.0166
LFX HCl 3.2 mg 0.0033
CC-36
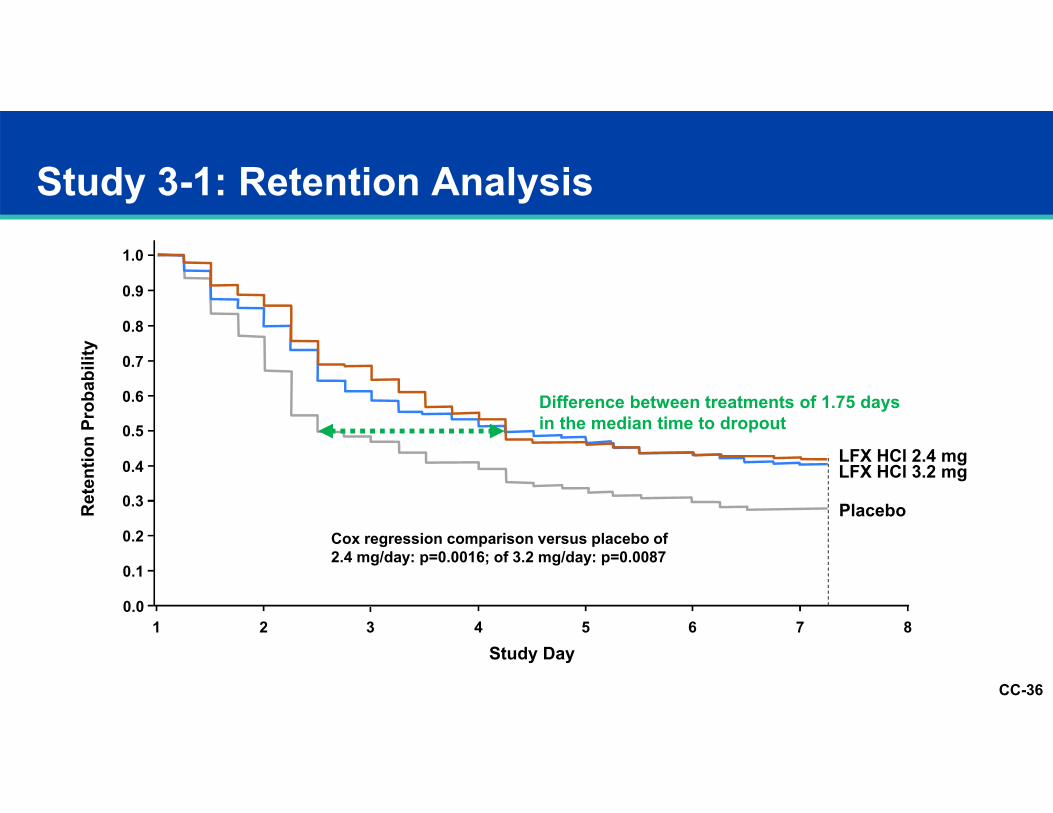
Study 3-1: Retention Analysis
1 2 3 4 5 6 7Study Day
1.0
0.9
0.8
0.7
0.6
Ret
entio
n Pr
obab
ility
0.4
0.3
0.5
0.2
0.1
0.0
LFX HCl 3.2 mg
Placebo
LFX HCl 2.4 mg
Difference between treatments of 1.75 days in the median time to dropout
8
Cox regression comparison versus placebo of 2.4 mg/day: p=0.0016; of 3.2 mg/day: p=0.0087
CC-37
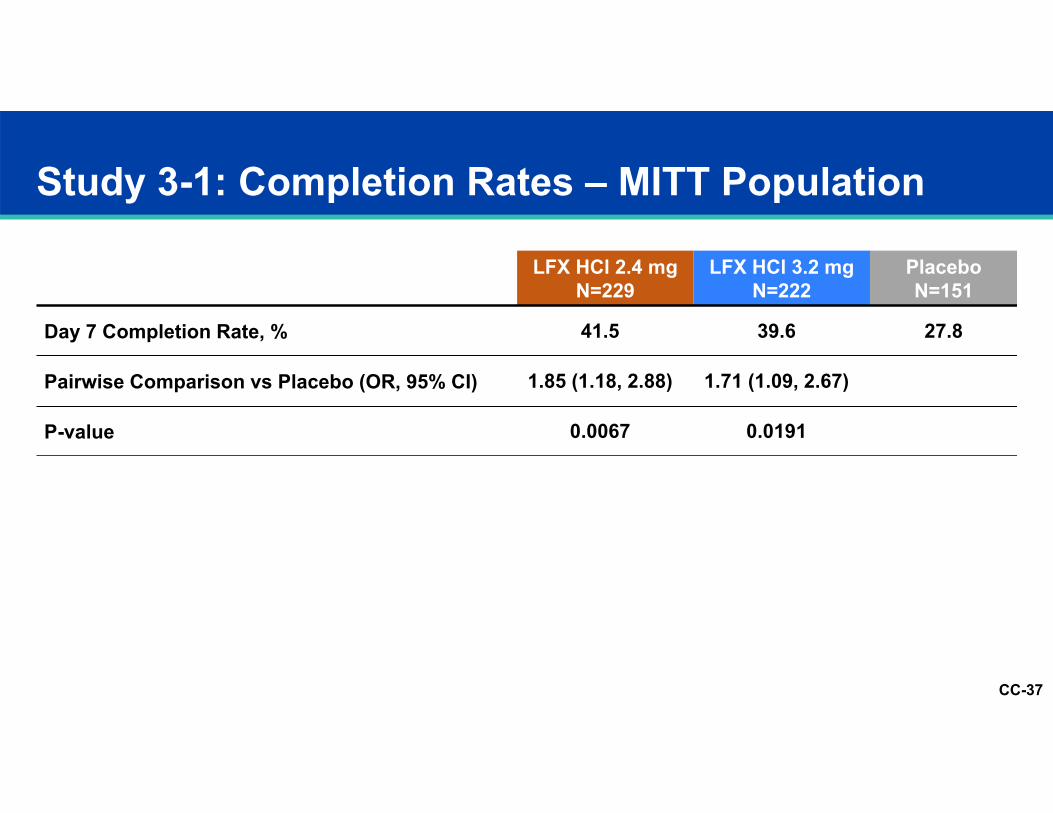
Study 3-1: Completion Rates – MITT Population
LFX HCl 2.4 mgN=229
LFX HCl 3.2 mgN=222
PlaceboN=151
Day 7 Completion Rate, % 41.5 39.6 27.8
Pairwise Comparison vs Placebo (OR, 95% CI) 1.85 (1.18, 2.88) 1.71 (1.09, 2.67)
P-value 0.0067 0.0191
CC-38
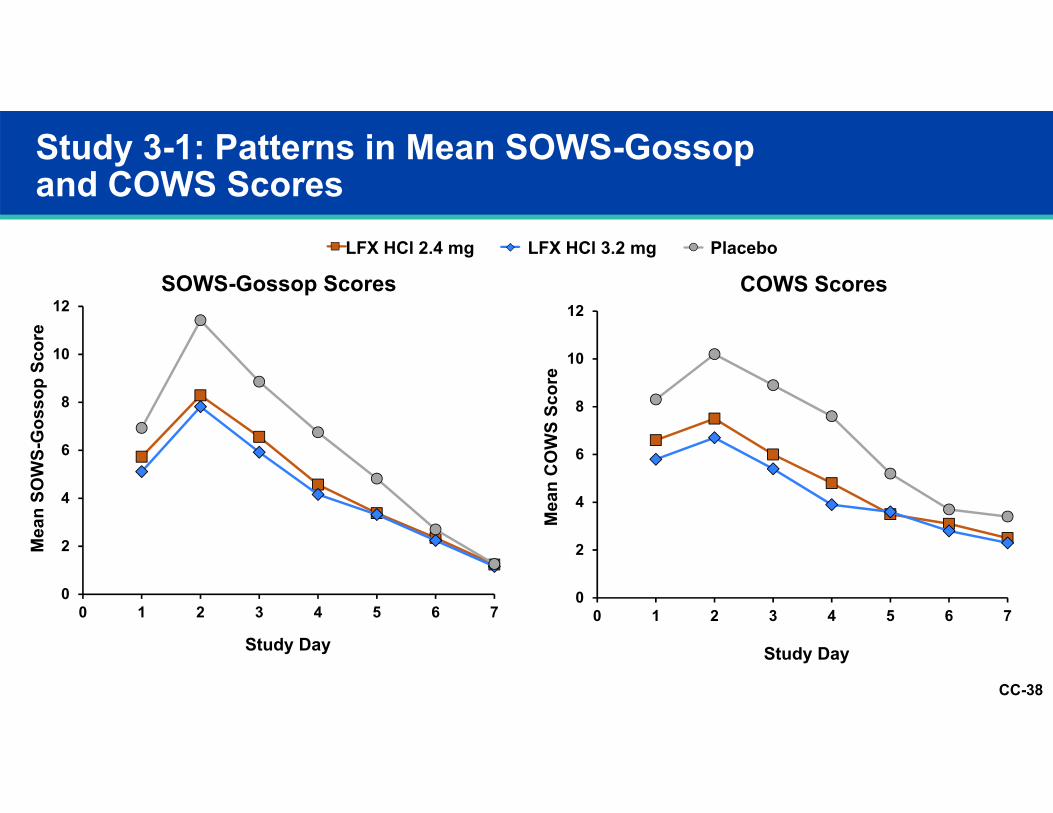
Study 3-1: Patterns in Mean SOWS-Gossop and COWS Scores
0
2
4
6
8
10
12
0 1 2 3 4 5 6 7
Mea
n SO
WS-
Gos
sop
Scor
e
Study Day
LFX HCl 2.4 mg LFX HCl 3.2 mg Placebo
SOWS-Gossop Scores COWS Scores
0
2
4
6
8
10
12
0 1 2 3 4 5 6 7
Mea
n C
OW
S Sc
ore
Study Day
CC-39
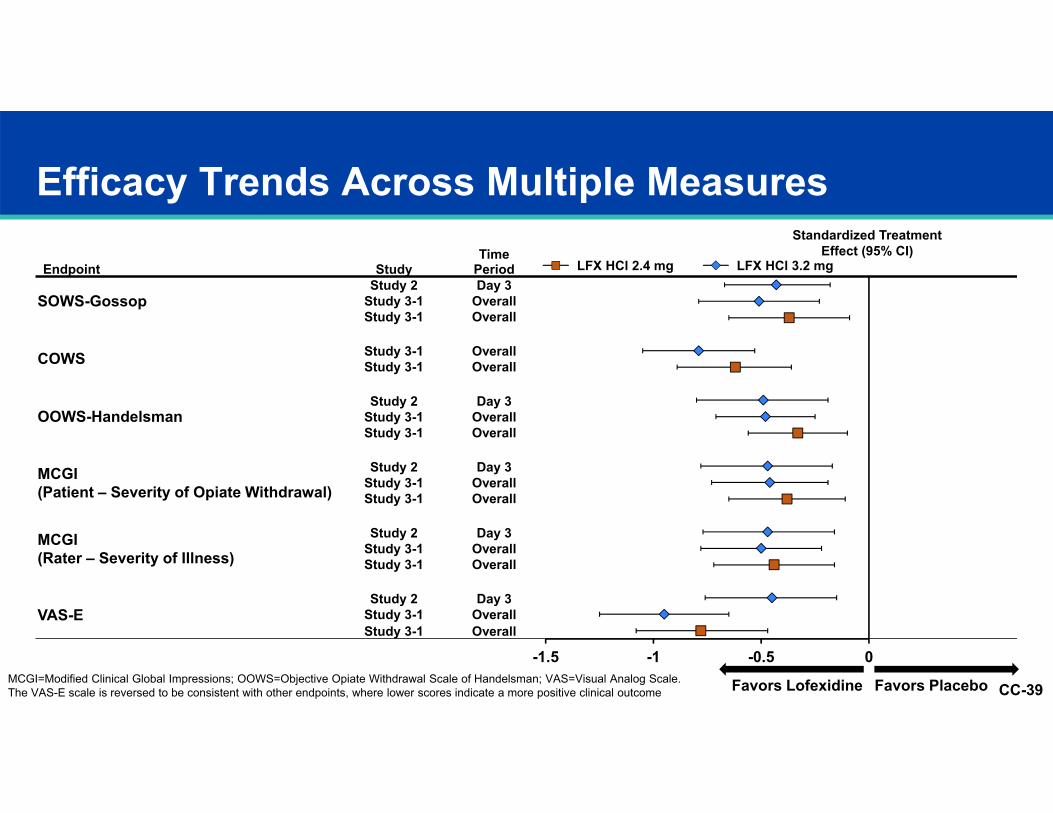
Efficacy Trends Across Multiple Measures
Endpoint StudyTime
Period
Standardized Treatment Effect (95% CI)
SOWS-GossopStudy 2 Day 3 -0.43 (-0.67, -0.18)
Study 3-1 Overall -0.51 (-0.79, -0.23)Study 3-1 Overall -0.37 (-0.65, -0.09)
COWS Study 3-1 Overall -0.79 (-1.05, -0.53)Study 3-1 Overall -0.62 (-0.89, -0.36)
OOWS-HandelsmanStudy 2 Day 3 -0.49 (-0.80, -0.19)
Study 3-1 Overall -0.48 (-0.71, -0.25)Study 3-1 Overall -0.33 (-0.56, -0.10)
MCGI (Patient – Severity of Opiate Withdrawal)
Study 2 Day 3 -0.47 (-0.78, -0.17)Study 3-1 Overall -0.46 (-0.73, -0.19)Study 3-1 Overall -0.38 (-0.65, -0.11)
MCGI (Rater – Severity of Illness)
Study 2 Day 3 -0.47 (-0.77, -0.16)Study 3-1 Overall -0.50 (-0.78, -0.22)Study 3-1 Overall -0.44 (-0.72, -0.16)
VAS-EStudy 2 Day 3 -0.45 (-0.76, -0.15)
Study 3-1 Overall -0.95 (-1.25, -0.65)Study 3-1 Overall -0.78 (-1.08, -0.47)
Favors Lofexidine Favors Placebo
LFX HCl 2.4 mg LFX HCl 3.2 mg
-1.5 -1 -0.5 0MCGI=Modified Clinical Global Impressions; OOWS=Objective Opiate Withdrawal Scale of Handelsman; VAS=Visual Analog Scale.The VAS-E scale is reversed to be consistent with other endpoints, where lower scores indicate a more positive clinical outcome
CC-40
Lofexidine Efficacy Summary
Achieved primary efficacy endpointsEffective on multiple efficacy measuresBoth doses effectiveAlleviated withdrawal symptomsHigher completion rate
CC-41
Mark Pirner, MD, PhD
Senior Medical DirectorUS WorldMeds
Lofexidine Safety
CC-42
Safety Presentation Outline
Exposure
CC-43
Safety Presentation Outline
ExposureOverall treatment emergent adverse events (AEs)
CC-44
Safety Presentation Outline
ExposureOverall treatment emergent adverse events (AEs)Drug class AEs and vital sign analyses
CC-45
Safety Presentation Outline
ExposureOverall treatment emergent adverse events (AEs)Drug class AEs and vital sign analysesSerious adverse events and AEs leading to discontinuation
CC-46
Safety Presentation Outline
ExposureOverall treatment emergent adverse events (AEs)Drug class AEs and vital sign analysesSerious adverse events and AEs leading to discontinuationTopics of special interest (QTc, renal/hepatic dose adjustment)
CC-47
Safety Presentation Outline
ExposureOverall treatment emergent adverse events (AEs)Drug class AEs and vital sign analysesSerious adverse events and AEs leading to discontinuationTopics of special interest (QTc, renal/hepatic dose adjustment)UK Safety Experience
CC-48
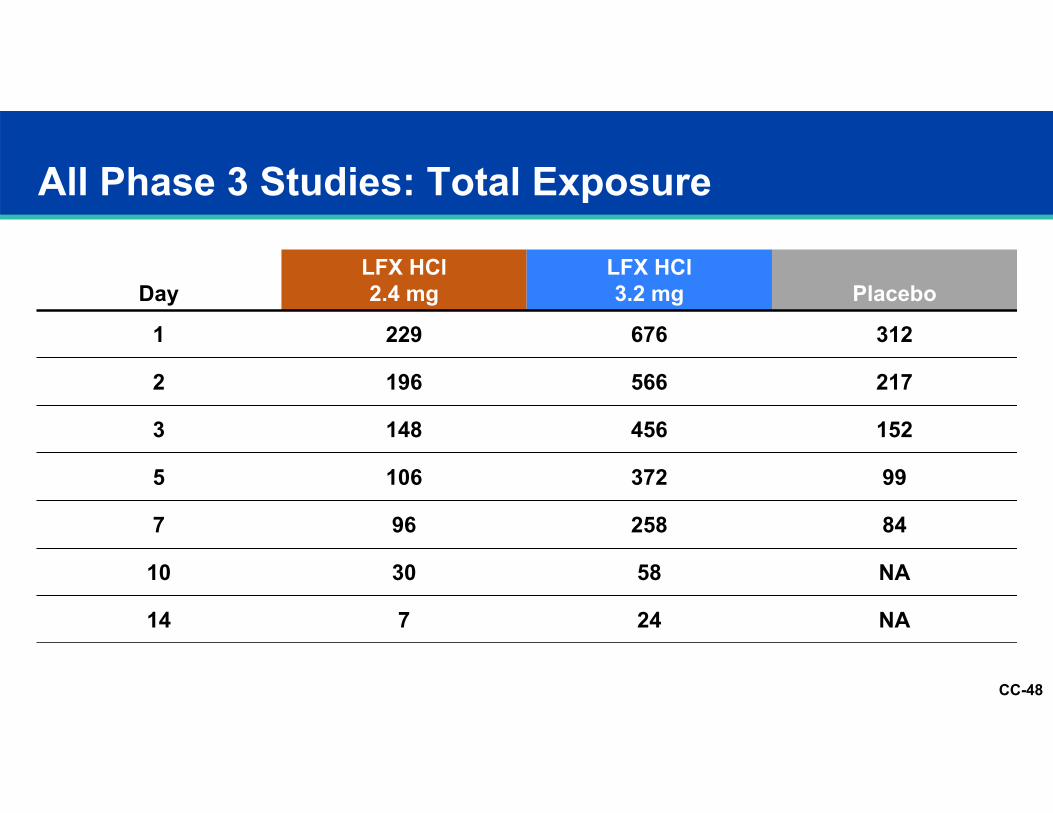
All Phase 3 Studies: Total Exposure
DayLFX HCl 2.4 mg
LFX HCl 3.2 mg Placebo
1 229 676 312
2 196 566 217
3 148 456 152
5 106 372 99
7 96 258 84
10 30 58 NA
14 7 24 NA
CC-49
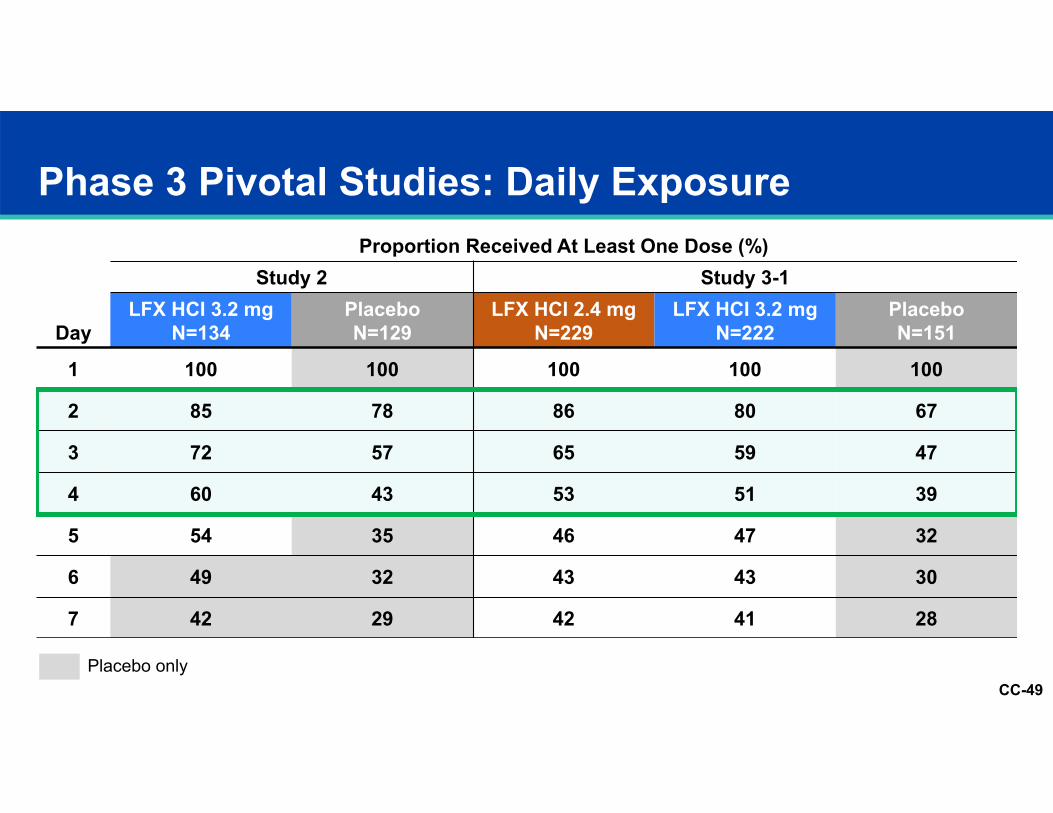
Phase 3 Pivotal Studies: Daily Exposure
Placebo only
Day
Proportion Received At Least One Dose (%)Study 2 Study 3-1
LFX HCI 3.2 mgN=134
PlaceboN=129
LFX HCI 2.4 mgN=229
LFX HCI 3.2 mgN=222
PlaceboN=151
1 100 100 100 100 100
2 85 78 86 80 67
3 72 57 65 59 47
4 60 43 53 51 39
5 54 35 46 47 32
6 49 32 43 43 30
7 42 29 42 41 28
CC-50
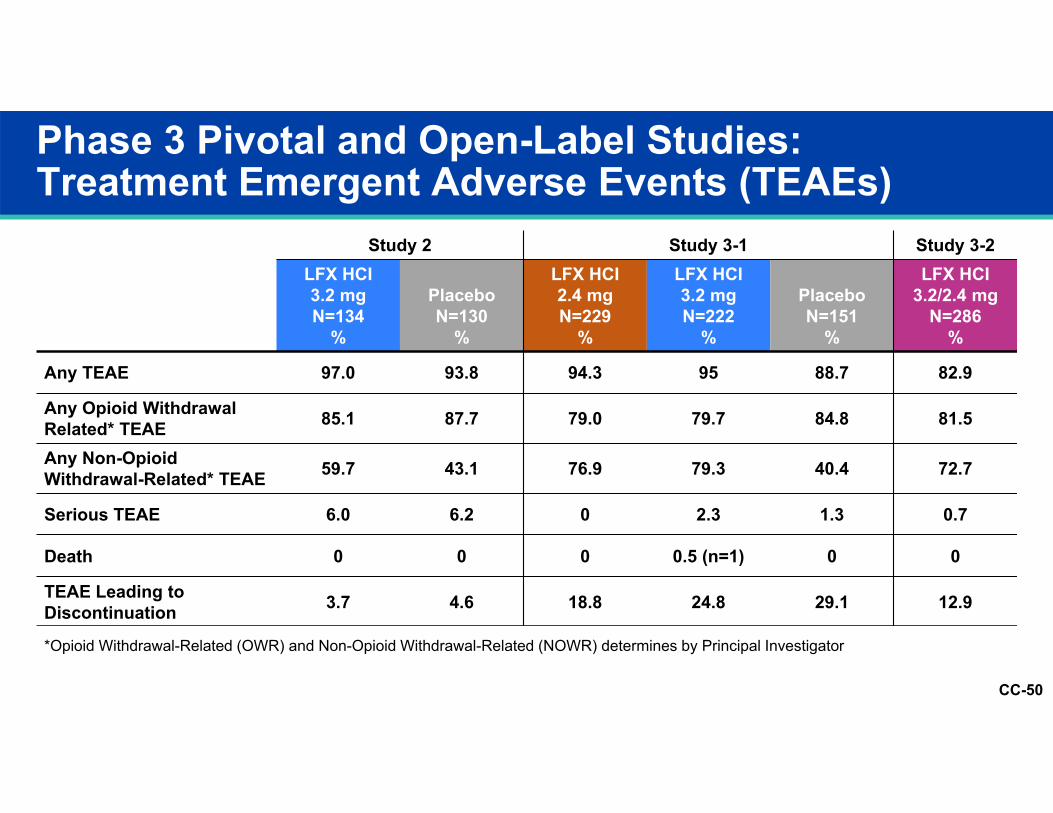
Phase 3 Pivotal and Open-Label Studies: Treatment Emergent Adverse Events (TEAEs)
TEAEs
Study 2 Study 3-1 Study 3-2LFX HCI3.2 mgN=134
%
PlaceboN=130
%
LFX HCI2.4 mgN=229
%
LFX HCI3.2 mgN=222
%
PlaceboN=151
%
LFX HCI3.2/2.4 mg
N=286%
Any TEAE 97.0 93.8 94.3 95 88.7 82.9
Any Opioid Withdrawal Related* TEAE 85.1 87.7 79.0 79.7 84.8 81.5
Any Non-Opioid Withdrawal-Related* TEAE 59.7 43.1 76.9 79.3 40.4 72.7
Serious TEAE 6.0 6.2 0 2.3 1.3 0.7
Death 0 0 0 0.5 (n=1) 0 0
TEAE Leading to Discontinuation 3.7 4.6 18.8 24.8 29.1 12.9
*Opioid Withdrawal-Related (OWR) and Non-Opioid Withdrawal-Related (NOWR) determines by Principal Investigator
CC-51
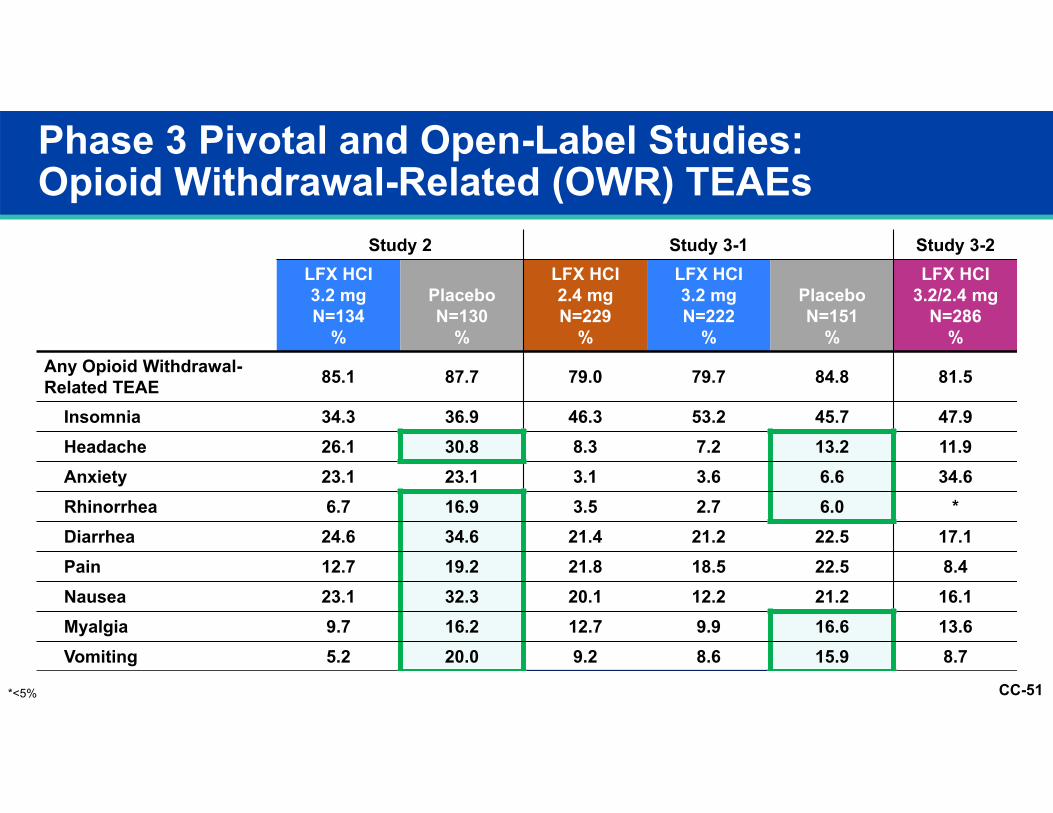
Phase 3 Pivotal and Open-Label Studies: Opioid Withdrawal-Related (OWR) TEAEs
TEAEs
Study 2 Study 3-1 Study 3-2LFX HCI3.2 mgN=134
%
PlaceboN=130
%
LFX HCI2.4 mgN=229
%
LFX HCI3.2 mgN=222
%
PlaceboN=151
%
LFX HCI3.2/2.4 mg
N=286%
Any Opioid Withdrawal-Related TEAE 85.1 87.7 79.0 79.7 84.8 81.5
Insomnia 34.3 36.9 46.3 53.2 45.7 47.9Headache 26.1 30.8 8.3 7.2 13.2 11.9Anxiety 23.1 23.1 3.1 3.6 6.6 34.6Rhinorrhea 6.7 16.9 3.5 2.7 6.0 *Diarrhea 24.6 34.6 21.4 21.2 22.5 17.1Pain 12.7 19.2 21.8 18.5 22.5 8.4Nausea 23.1 32.3 20.1 12.2 21.2 16.1Myalgia 9.7 16.2 12.7 9.9 16.6 13.6Vomiting 5.2 20.0 9.2 8.6 15.9 8.7
*<5%
CC-52
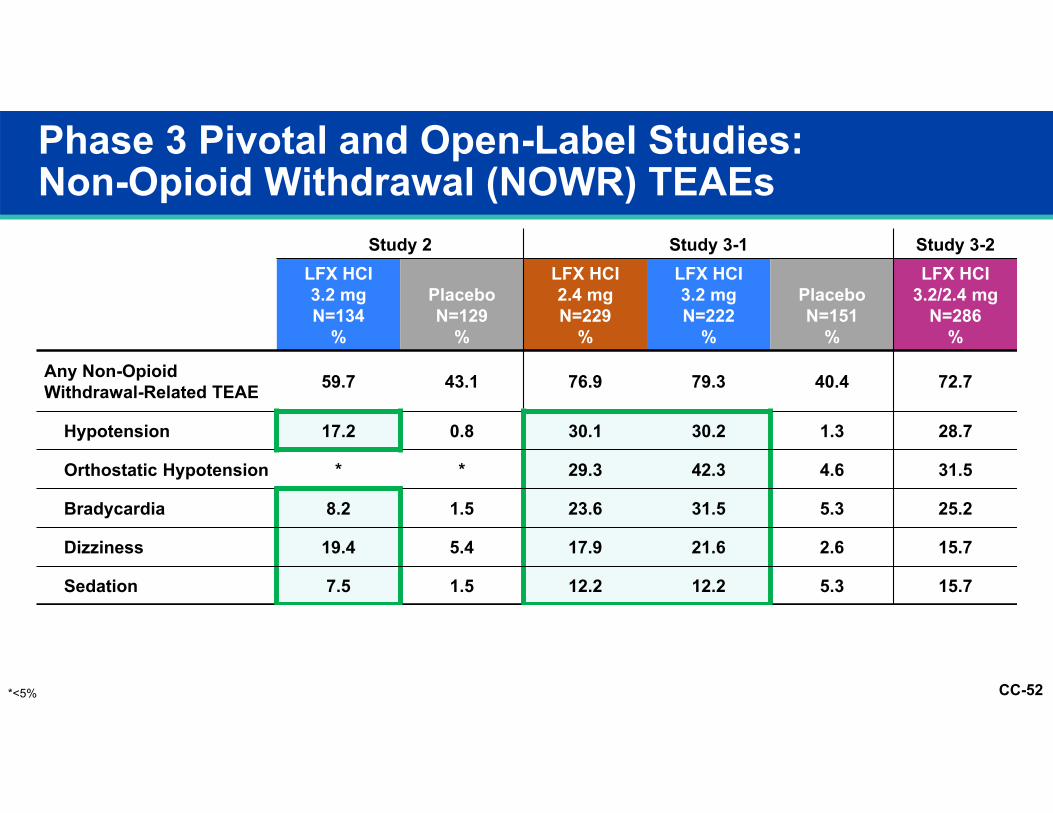
Phase 3 Pivotal and Open-Label Studies:Non-Opioid Withdrawal (NOWR) TEAEs
TEAEs
Study 2 Study 3-1 Study 3-2LFX HCI3.2 mgN=134
%
PlaceboN=129
%
LFX HCI2.4 mgN=229
%
LFX HCI3.2 mgN=222
%
PlaceboN=151
%
LFX HCI 3.2/2.4 mg
N=286%
Any Non-Opioid Withdrawal-Related TEAE 59.7 43.1 76.9 79.3 40.4 72.7
Hypotension 17.2 0.8 30.1 30.2 1.3 28.7
Orthostatic Hypotension * * 29.3 42.3 4.6 31.5
Bradycardia 8.2 1.5 23.6 31.5 5.3 25.2
Dizziness 19.4 5.4 17.9 21.6 2.6 15.7
Sedation 7.5 1.5 12.2 12.2 5.3 15.7
*<5%
CC-53
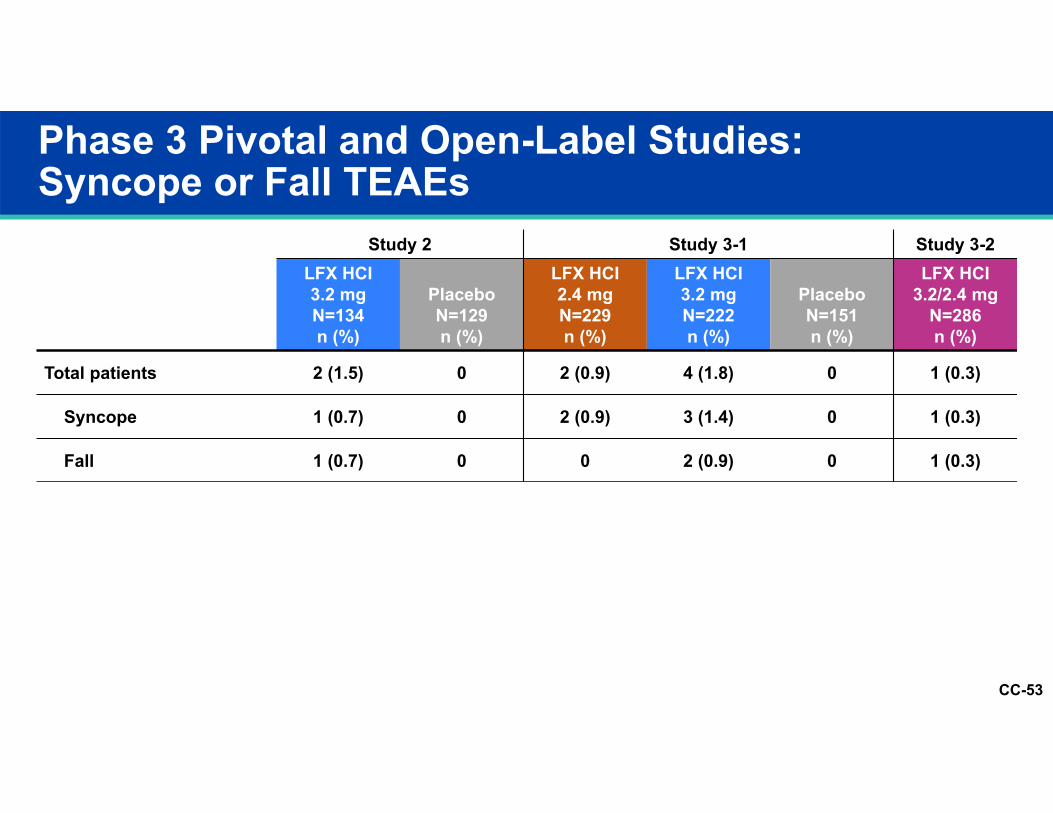
Phase 3 Pivotal and Open-Label Studies:Syncope or Fall TEAEs
TEAEs
Study 2 Study 3-1 Study 3-2LFX HCI3.2 mgN=134n (%)
PlaceboN=129n (%)
LFX HCI2.4 mgN=229n (%)
LFX HCI3.2 mgN=222n (%)
PlaceboN=151n (%)
LFX HCI 3.2/2.4 mg
N=286n (%)
Total patients 2 (1.5) 0 2 (0.9) 4 (1.8) 0 1 (0.3)
Syncope 1 (0.7) 0 2 (0.9) 3 (1.4) 0 1 (0.3)
Fall 1 (0.7) 0 0 2 (0.9) 0 1 (0.3)
CC-54-5
0
5
10
15
20
0 1 2 3 4 5 6 7
BPM
Study Day
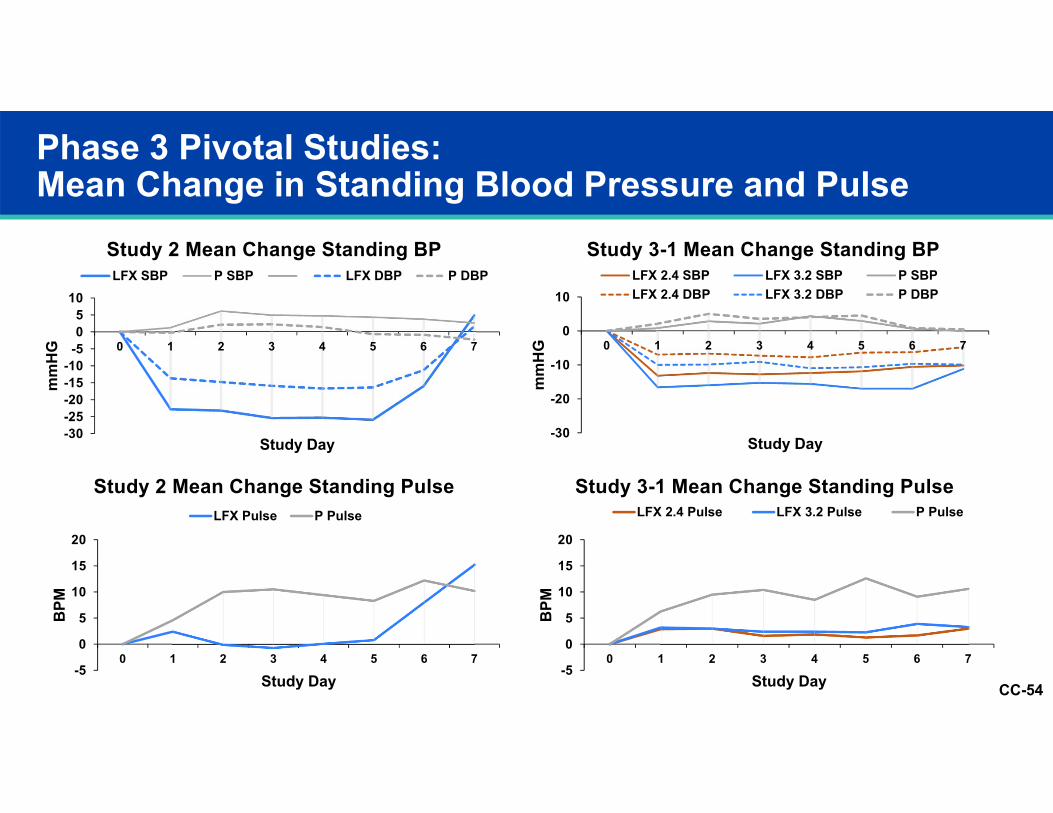
Study 3-1 Mean Change Standing PulseLFX 2.4 Pulse LFX 3.2 Pulse P Pulse
Phase 3 Pivotal Studies: Mean Change in Standing Blood Pressure and Pulse
-30-25-20-15-10
-505
10
0 1 2 3 4 5 6 7
mm
HG
Study Day
Study 2 Mean Change Standing BPLFX SBP P SBP LFX DBP P DBP
-5
0
5
10
15
20
0 1 2 3 4 5 6 7
BPM
Study Day
Study 2 Mean Change Standing PulseLFX Pulse P Pulse
-30
-20
-10
0
10
0 1 2 3 4 5 6 7
mm
HG
Study Day
Study 3-1 Mean Change Standing BPLFX 2.4 SBP LFX 3.2 SBP P SBPLFX 2.4 DBP LFX 3.2 DBP P DBP
CC-55
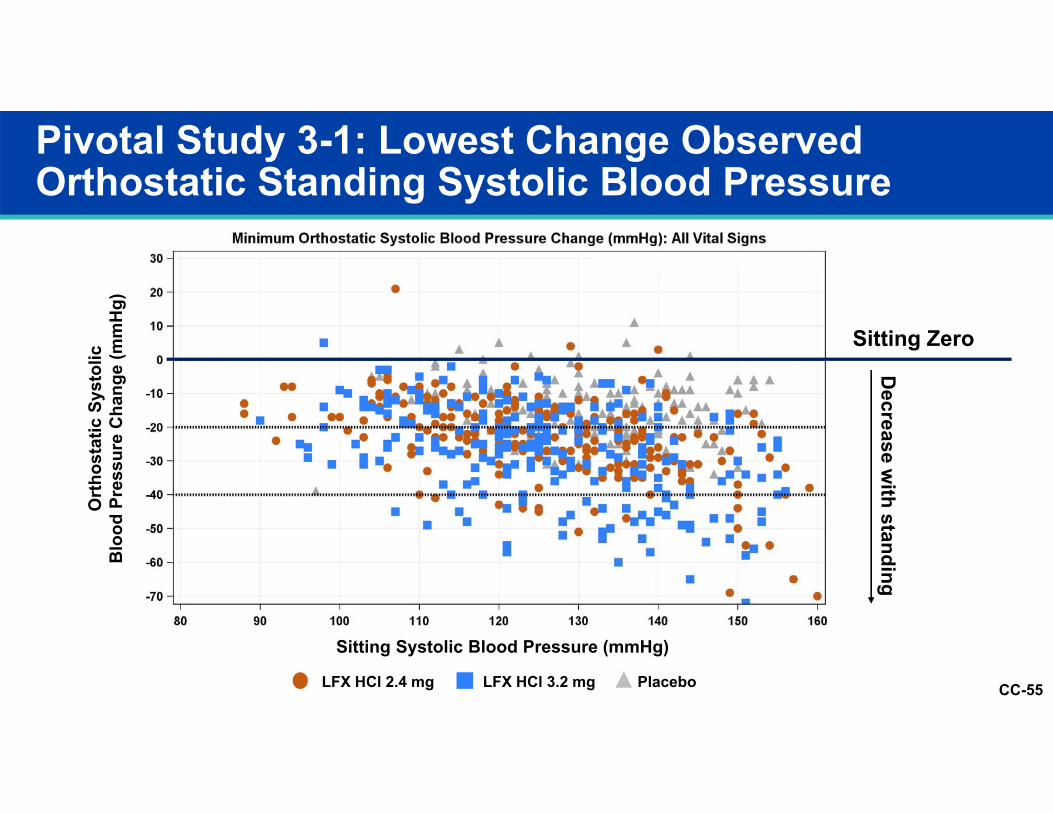
Pivotal Study 3-1: Lowest Change Observed Orthostatic Standing Systolic Blood Pressure
LFX HCl 2.4 mg PlaceboLFX HCl 3.2 mg
Sitting Zero
Decrease w
ith standing
Ort
host
atic
Sys
tolic
Blo
od P
ress
ure
Cha
nge
(mm
Hg)
Sitting Systolic Blood Pressure (mmHg)
CC-56
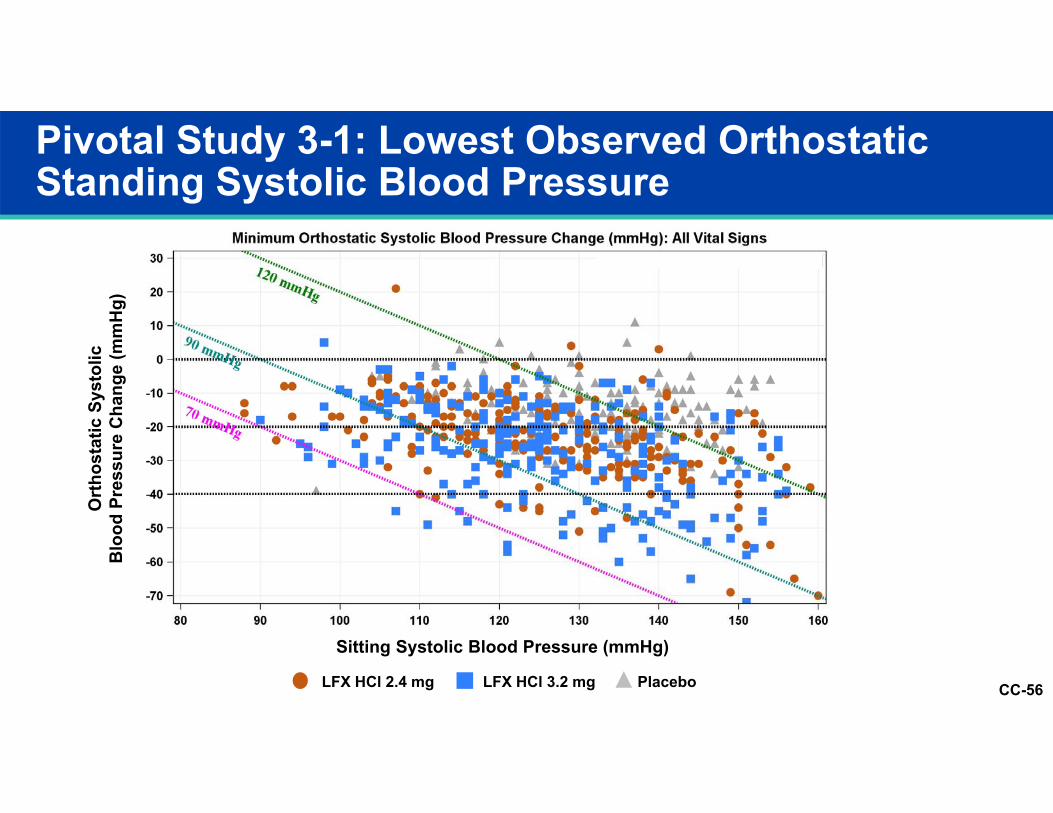
Pivotal Study 3-1: Lowest Observed Orthostatic Standing Systolic Blood Pressure
Sitting Systolic Blood Pressure (mmHg)
Ort
host
atic
Sys
tolic
Blo
od P
ress
ure
Cha
nge
(mm
Hg)
LFX HCl 2.4 mg PlaceboLFX HCl 3.2 mg
CC-57
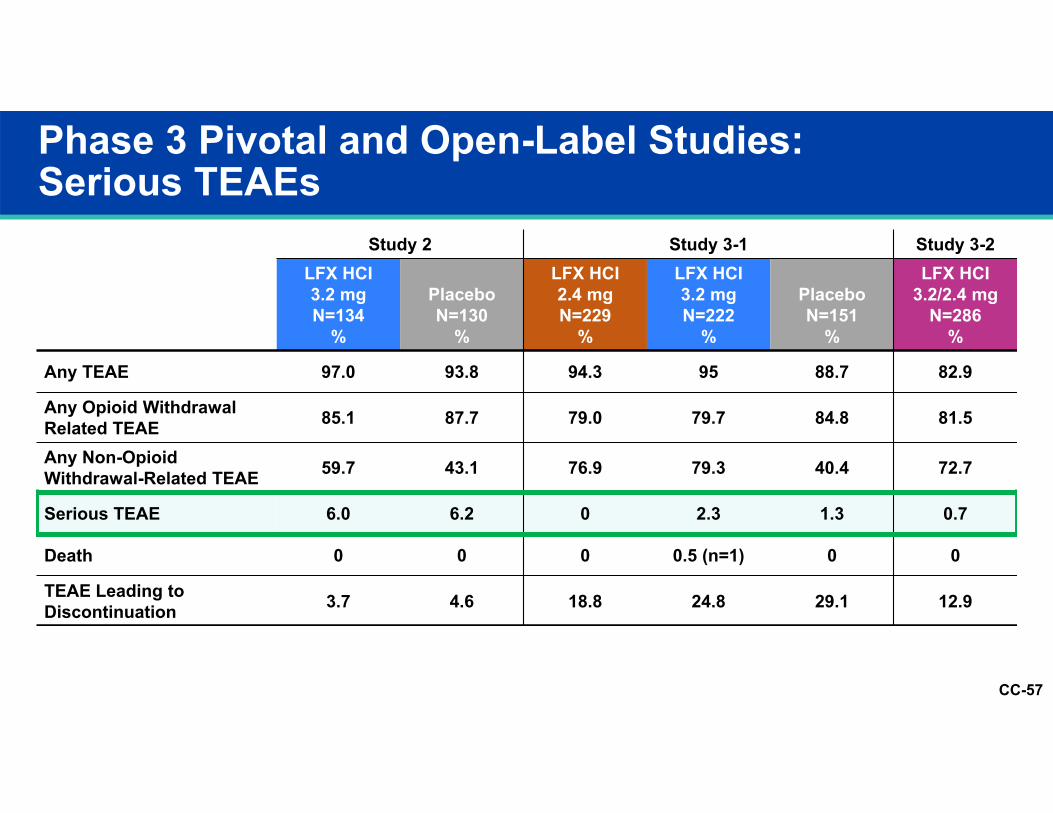
Phase 3 Pivotal and Open-Label Studies: Serious TEAEs
TEAEs
Study 2 Study 3-1 Study 3-2LFX HCI3.2 mgN=134
%
PlaceboN=130
%
LFX HCI2.4 mgN=229
%
LFX HCI3.2 mgN=222
%
PlaceboN=151
%
LFX HCI3.2/2.4 mg
N=286%
Any TEAE 97.0 93.8 94.3 95 88.7 82.9
Any Opioid Withdrawal Related TEAE 85.1 87.7 79.0 79.7 84.8 81.5
Any Non-Opioid Withdrawal-Related TEAE 59.7 43.1 76.9 79.3 40.4 72.7
Serious TEAE 6.0 6.2 0 2.3 1.3 0.7
Death 0 0 0 0.5 (n=1) 0 0
TEAE Leading to Discontinuation 3.7 4.6 18.8 24.8 29.1 12.9
CC-58
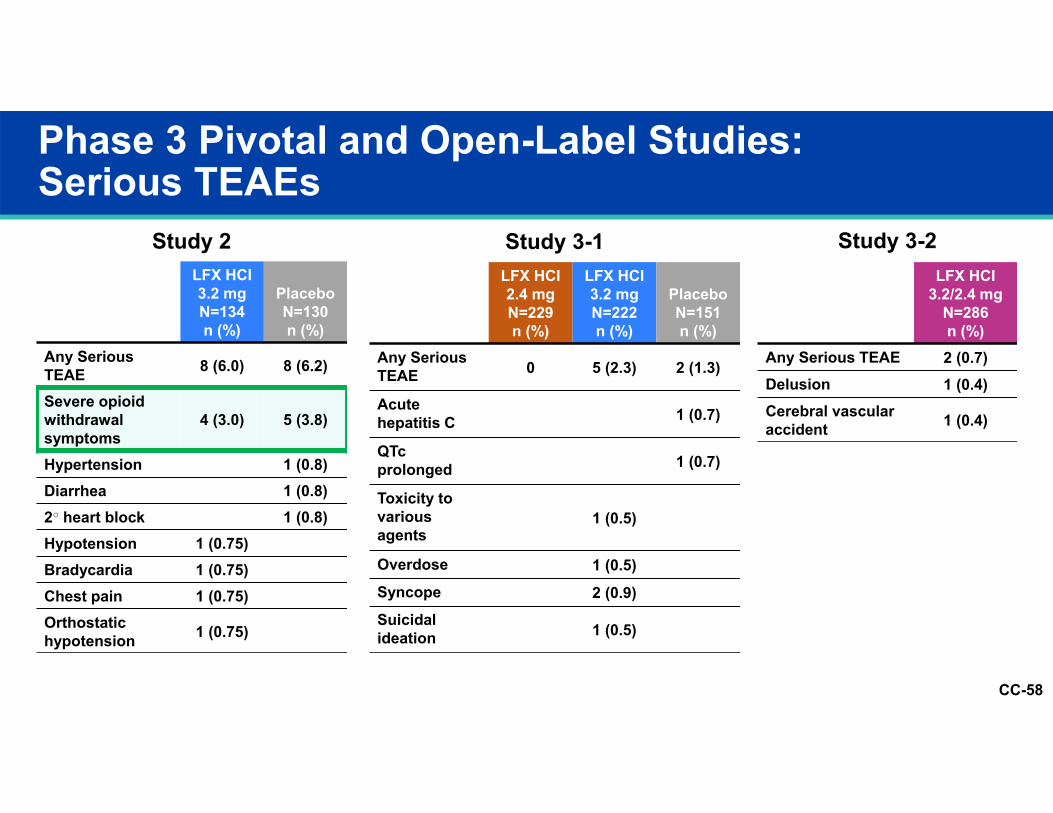
Phase 3 Pivotal and Open-Label Studies:Serious TEAEs
LFX HCI 3.2 mgN=134n (%)
PlaceboN=130n (%)
Any Serious TEAE 8 (6.0) 8 (6.2)
Severe opioid withdrawal symptoms
4 (3.0) 5 (3.8)
Hypertension 1 (0.8)Diarrhea 1 (0.8)2○ heart block 1 (0.8)Hypotension 1 (0.75)Bradycardia 1 (0.75)Chest pain 1 (0.75)Orthostatic hypotension 1 (0.75)
LFX HCI 2.4 mgN=229n (%)
LFX HCI 3.2 mgN=222n (%)
PlaceboN=151n (%)
Any Serious TEAE 0 5 (2.3) 2 (1.3)
Acute hepatitis C 1 (0.7)
QTc prolonged 1 (0.7)
Toxicity to various agents
1 (0.5)
Overdose 1 (0.5)Syncope 2 (0.9)Suicidal ideation 1 (0.5)
LFX HCI3.2/2.4 mg
N=286n (%)
Any Serious TEAE 2 (0.7)Delusion 1 (0.4)Cerebral vascular accident 1 (0.4)
Study 2 Study 3-1 Study 3-2
CC-59
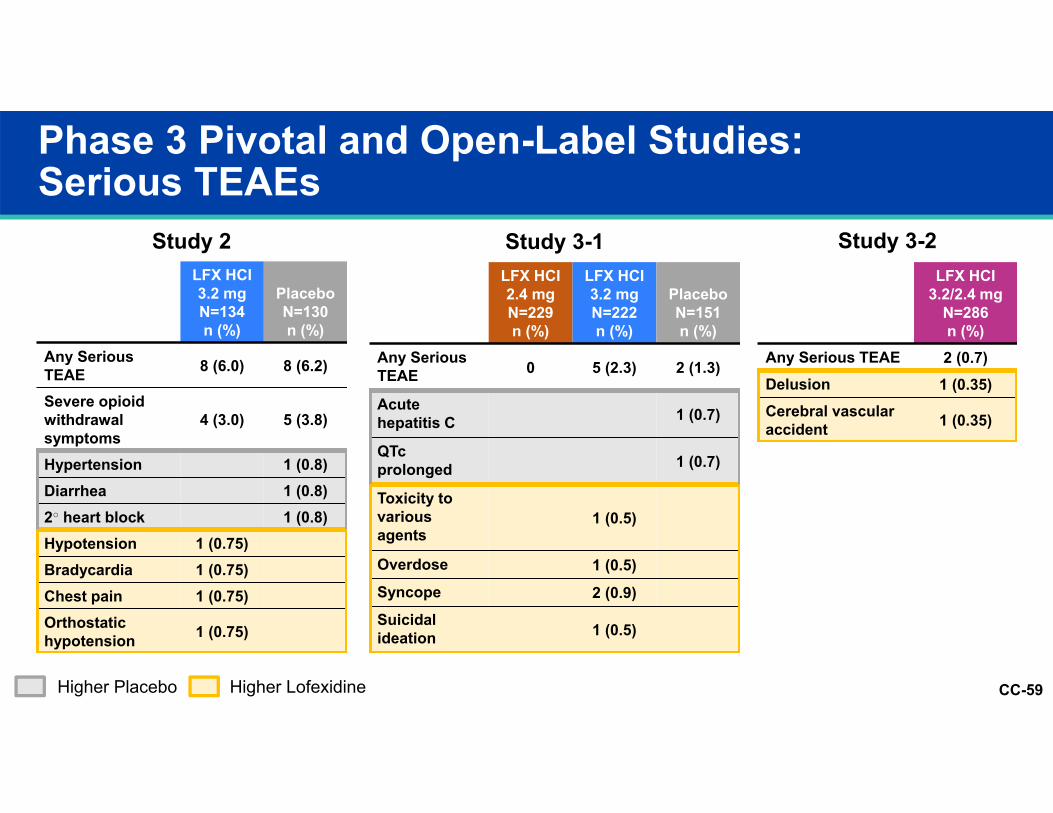
Phase 3 Pivotal and Open-Label Studies:Serious TEAEs
LFX HCI 3.2 mgN=134n (%)
PlaceboN=130n (%)
Any Serious TEAE 8 (6.0) 8 (6.2)
Severe opioid withdrawal symptoms
4 (3.0) 5 (3.8)
Hypertension 1 (0.8)Diarrhea 1 (0.8)2○ heart block 1 (0.8)Hypotension 1 (0.75)Bradycardia 1 (0.75)Chest pain 1 (0.75)Orthostatic hypotension 1 (0.75)
LFX HCI 2.4 mgN=229n (%)
LFX HCI 3.2 mgN=222n (%)
PlaceboN=151n (%)
Any Serious TEAE 0 5 (2.3) 2 (1.3)
Acute hepatitis C 1 (0.7)
QTc prolonged 1 (0.7)
Toxicity to various agents
1 (0.5)
Overdose 1 (0.5)Syncope 2 (0.9)Suicidal ideation 1 (0.5)
LFX HCI3.2/2.4 mg
N=286n (%)
Any Serious TEAE 2 (0.7)Delusion 1 (0.35)Cerebral vascular accident 1 (0.35)
Study 2 Study 3-1 Study 3-2
Higher Placebo Higher Lofexidine
CC-60
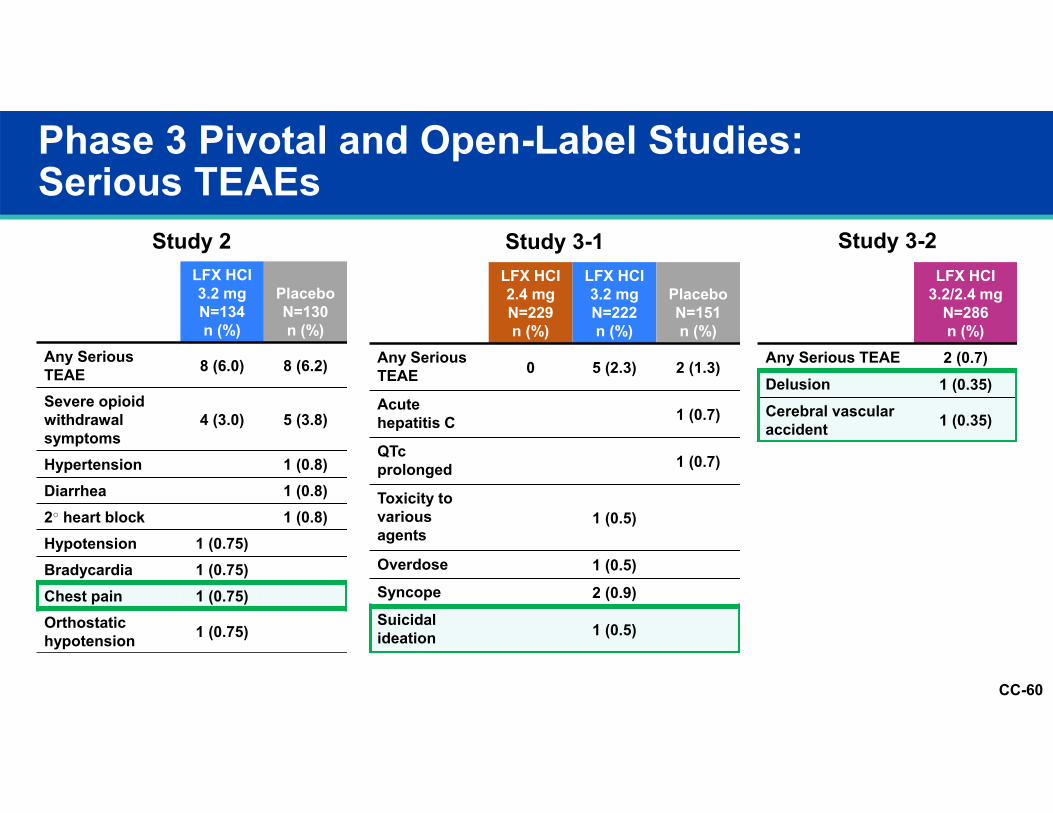
Phase 3 Pivotal and Open-Label Studies:Serious TEAEs
LFX HCI 3.2 mgN=134n (%)
PlaceboN=130n (%)
Any Serious TEAE 8 (6.0) 8 (6.2)
Severe opioid withdrawal symptoms
4 (3.0) 5 (3.8)
Hypertension 1 (0.8)Diarrhea 1 (0.8)2○ heart block 1 (0.8)Hypotension 1 (0.75)Bradycardia 1 (0.75)Chest pain 1 (0.75)Orthostatic hypotension 1 (0.75)
LFX HCI 2.4 mgN=229n (%)
LFX HCI 3.2 mgN=222n (%)
PlaceboN=151n (%)
Any Serious TEAE 0 5 (2.3) 2 (1.3)
Acute hepatitis C 1 (0.7)
QTc prolonged 1 (0.7)
Toxicity to various agents
1 (0.5)
Overdose 1 (0.5)Syncope 2 (0.9)Suicidal ideation 1 (0.5)
LFX HCI3.2/2.4 mg
N=286n (%)
Any Serious TEAE 2 (0.7)Delusion 1 (0.35)Cerebral vascular accident 1 (0.35)
Study 2 Study 3-1 Study 3-2
CC-61
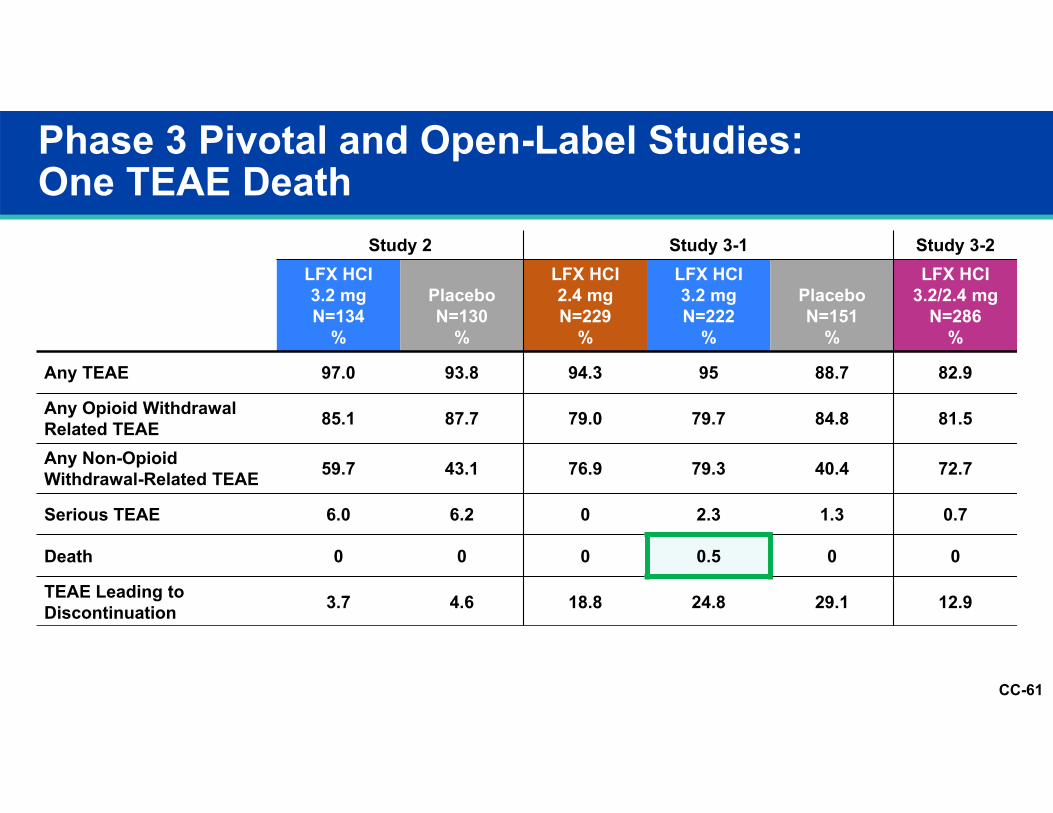
Phase 3 Pivotal and Open-Label Studies:One TEAE Death
TEAEs
Study 2 Study 3-1 Study 3-2LFX HCI3.2 mgN=134
%
PlaceboN=130
%
LFX HCI2.4 mgN=229
%
LFX HCI3.2 mgN=222
%
PlaceboN=151
%
LFX HCI3.2/2.4 mg
N=286%
Any TEAE 97.0 93.8 94.3 95 88.7 82.9
Any Opioid Withdrawal Related TEAE 85.1 87.7 79.0 79.7 84.8 81.5
Any Non-Opioid Withdrawal-Related TEAE 59.7 43.1 76.9 79.3 40.4 72.7
Serious TEAE 6.0 6.2 0 2.3 1.3 0.7
Death 0 0 0 0.5 0 0
TEAE Leading to Discontinuation 3.7 4.6 18.8 24.8 29.1 12.9
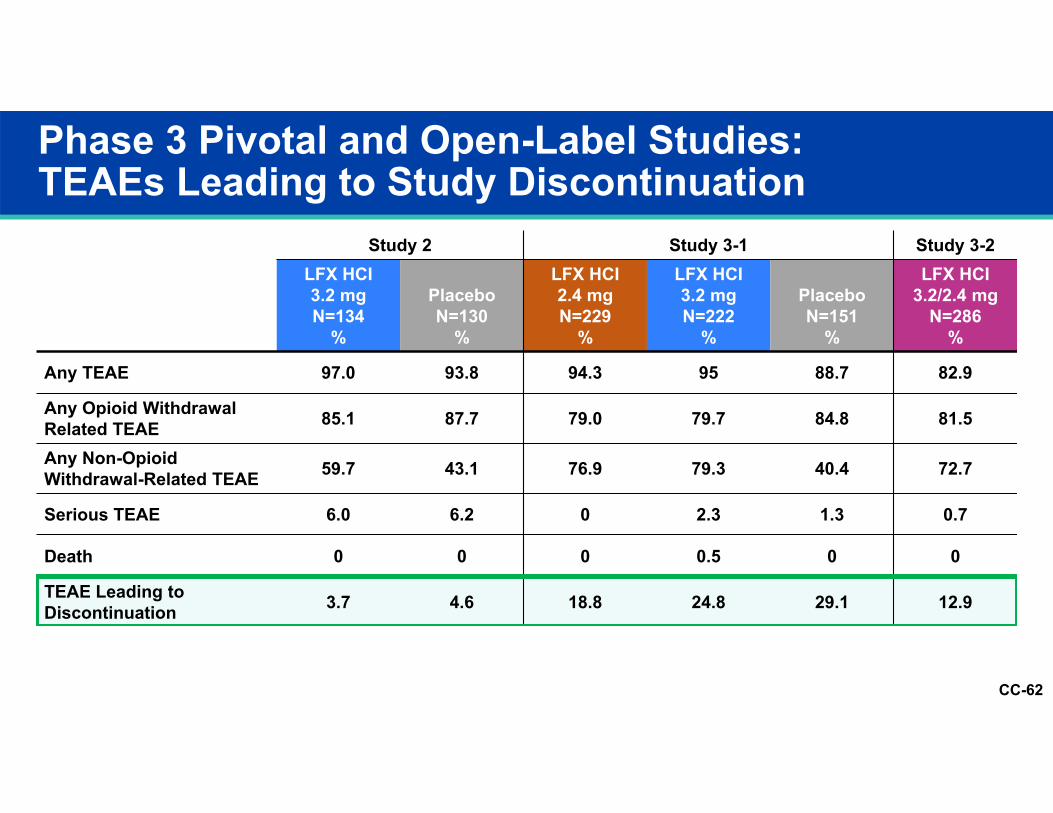
CC-62
Phase 3 Pivotal and Open-Label Studies:TEAEs Leading to Study Discontinuation
TEAEs
Study 2 Study 3-1 Study 3-2LFX HCI3.2 mgN=134
%
PlaceboN=130
%
LFX HCI2.4 mgN=229
%
LFX HCI3.2 mgN=222
%
PlaceboN=151
%
LFX HCI3.2/2.4 mg
N=286%
Any TEAE 97.0 93.8 94.3 95 88.7 82.9
Any Opioid Withdrawal Related TEAE 85.1 87.7 79.0 79.7 84.8 81.5
Any Non-Opioid Withdrawal-Related TEAE 59.7 43.1 76.9 79.3 40.4 72.7
Serious TEAE 6.0 6.2 0 2.3 1.3 0.7
Death 0 0 0 0.5 0 0
TEAE Leading to Discontinuation 3.7 4.6 18.8 24.8 29.1 12.9
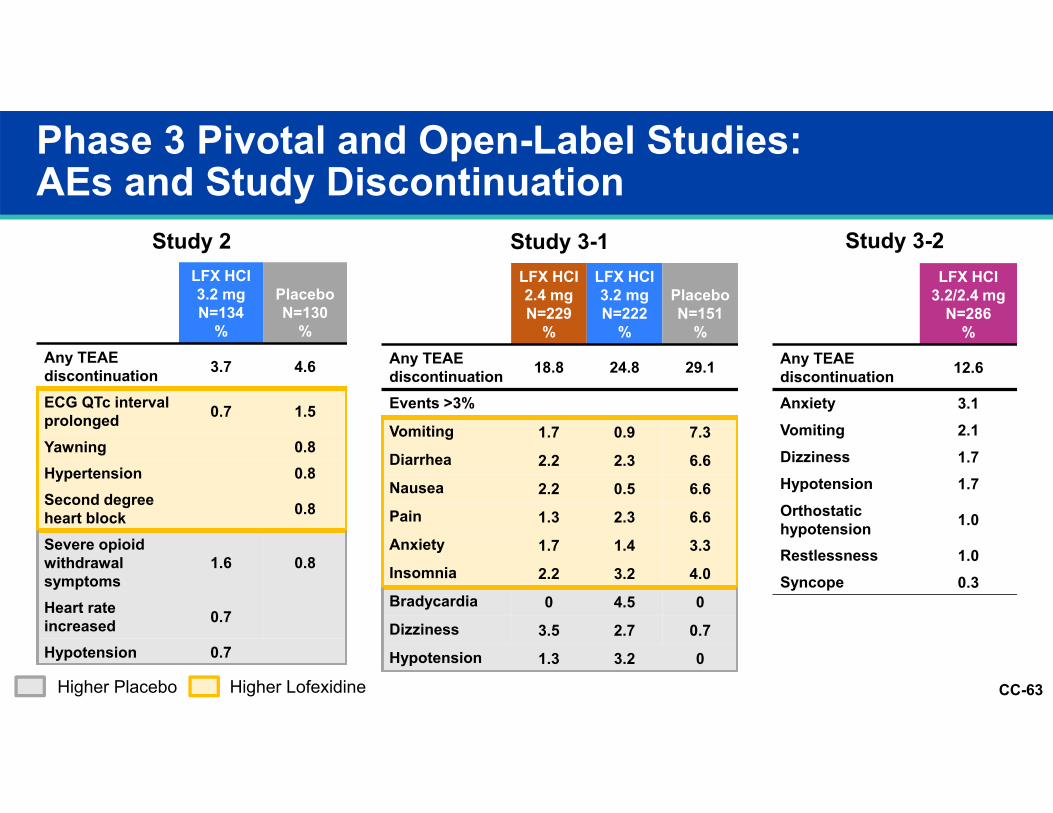
CC-63
Phase 3 Pivotal and Open-Label Studies:AEs and Study Discontinuation
LFX HCI3.2 mgN=134
%
PlaceboN=130
%Any TEAE discontinuation 3.7 4.6
ECG QTc interval prolonged 0.7 1.5
Yawning 0.8Hypertension 0.8Second degree heart block 0.8
Severe opioid withdrawal symptoms
1.6 0.8
Heart rate increased 0.7
Hypotension 0.7
LFX HCI2.4 mgN=229
%
LFX HCI3.2 mgN=222
%
PlaceboN=151
%Any TEAE discontinuation 18.8 24.8 29.1
Events >3%
Vomiting 1.7 0.9 7.3Diarrhea 2.2 2.3 6.6Nausea 2.2 0.5 6.6Pain 1.3 2.3 6.6Anxiety 1.7 1.4 3.3Insomnia 2.2 3.2 4.0Bradycardia 0 4.5 0Dizziness 3.5 2.7 0.7Hypotension 1.3 3.2 0
LFX HCI3.2/2.4 mg
N=286%
Any TEAE discontinuation 12.6
Anxiety 3.1Vomiting 2.1Dizziness 1.7Hypotension 1.7Orthostatic hypotension 1.0
Restlessness 1.0Syncope 0.3
Study 2 Study 3-1 Study 3-2
Higher Placebo Higher Lofexidine
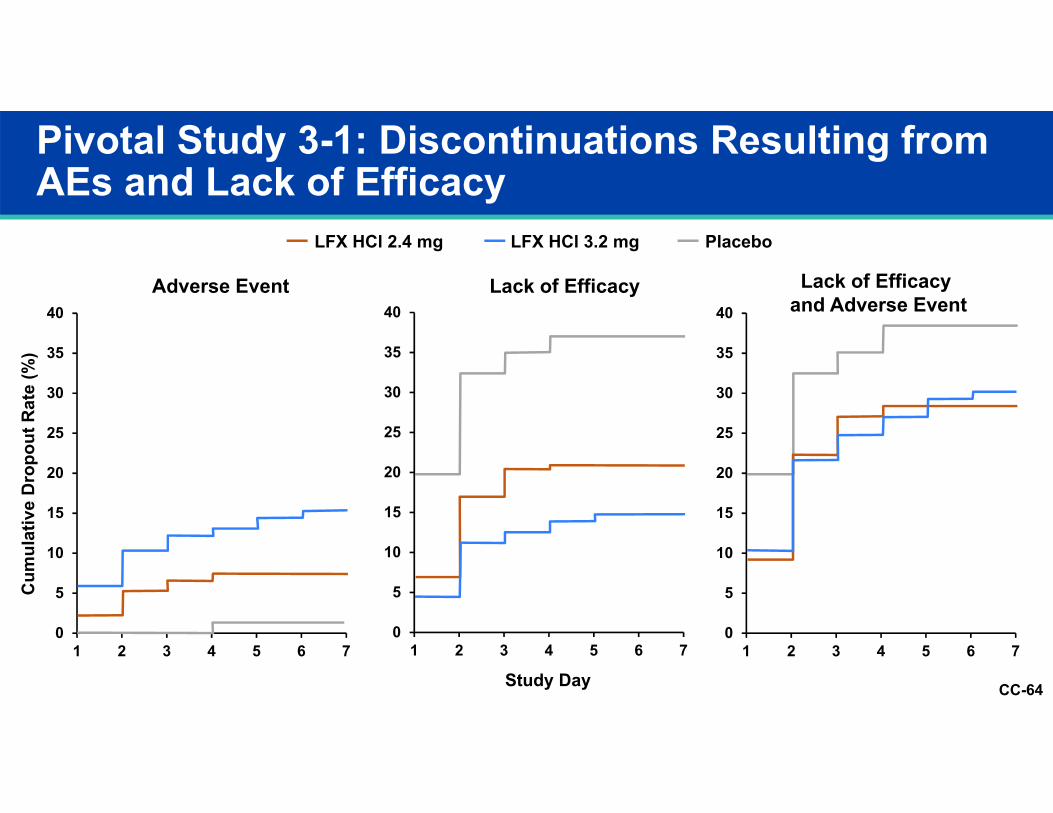
CC-64
Pivotal Study 3-1: Discontinuations Resulting from AEs and Lack of Efficacy
0
5
10
15
20
25
30
35
40
1 2 3 4 5 6 70
5
10
15
20
25
30
35
40
1 2 3 4 5 6 70
5
10
15
20
25
30
35
40
1 2 3 4 5 6 7
Study Day
Cum
ulat
ive
Dro
pout
Rat
e (%
)
LFX HCl 2.4 mg LFX HCl 3.2 mg Placebo
Adverse Event Lack of Efficacy Lack of Efficacy and Adverse Event

CC-65
Topics of Special Interest: QTc, Renal/Hepatic Dose Adjustment
CC-66
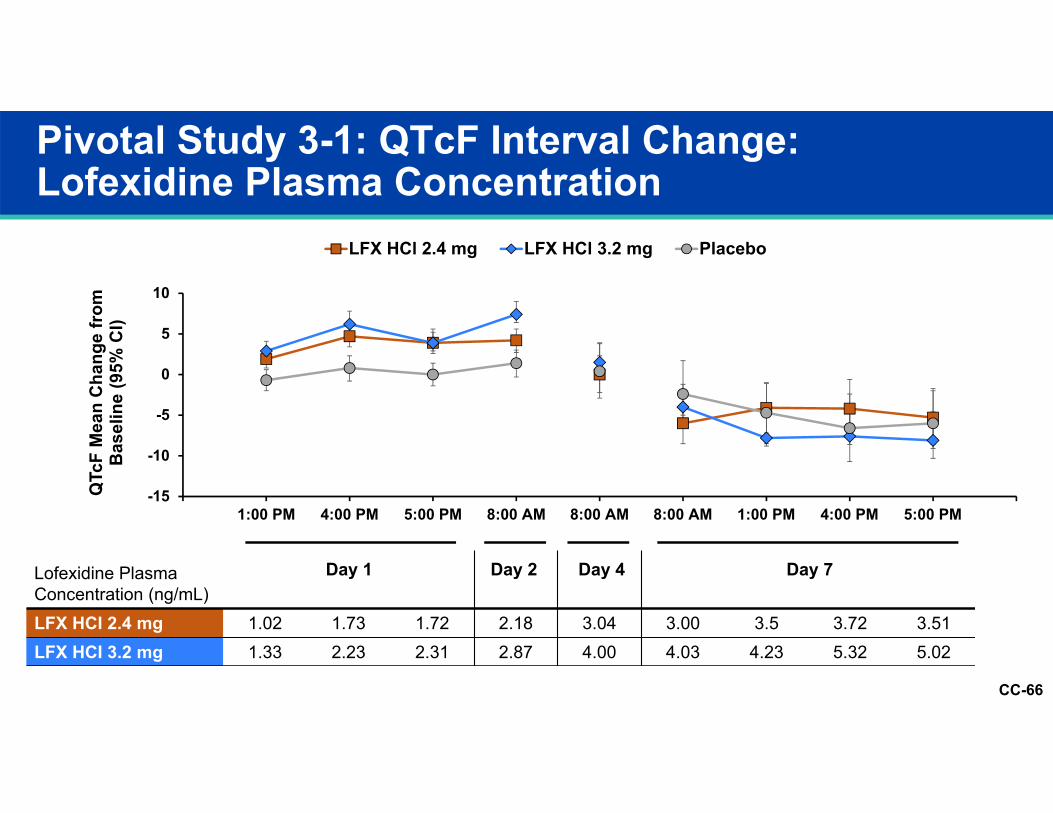
Pivotal Study 3-1: QTcF Interval Change: Lofexidine Plasma Concentration
Lofexidine Plasma Concentration (ng/mL)LFX HCI 2.4 mg 1.02 1.73 1.72 2.18 3.04 3.00 3.5 3.72 3.51LFX HCI 3.2 mg 1.33 2.23 2.31 2.87 4.00 4.03 4.23 5.32 5.02
-15
-10
-5
0
5
10
1:00 PM 4:00 PM 5:00 PM 8:00 AM 8:00 AM 8:00 AM 1:00 PM 4:00 PM 5:00 PM
QTc
F M
ean
Cha
nge
from
B
asel
ine
(95%
CI)
LFX HCl 2.4 mg LFX HCl 3.2 mg Placebo
Day 1 Day 7Day 4Day 2
CC-67
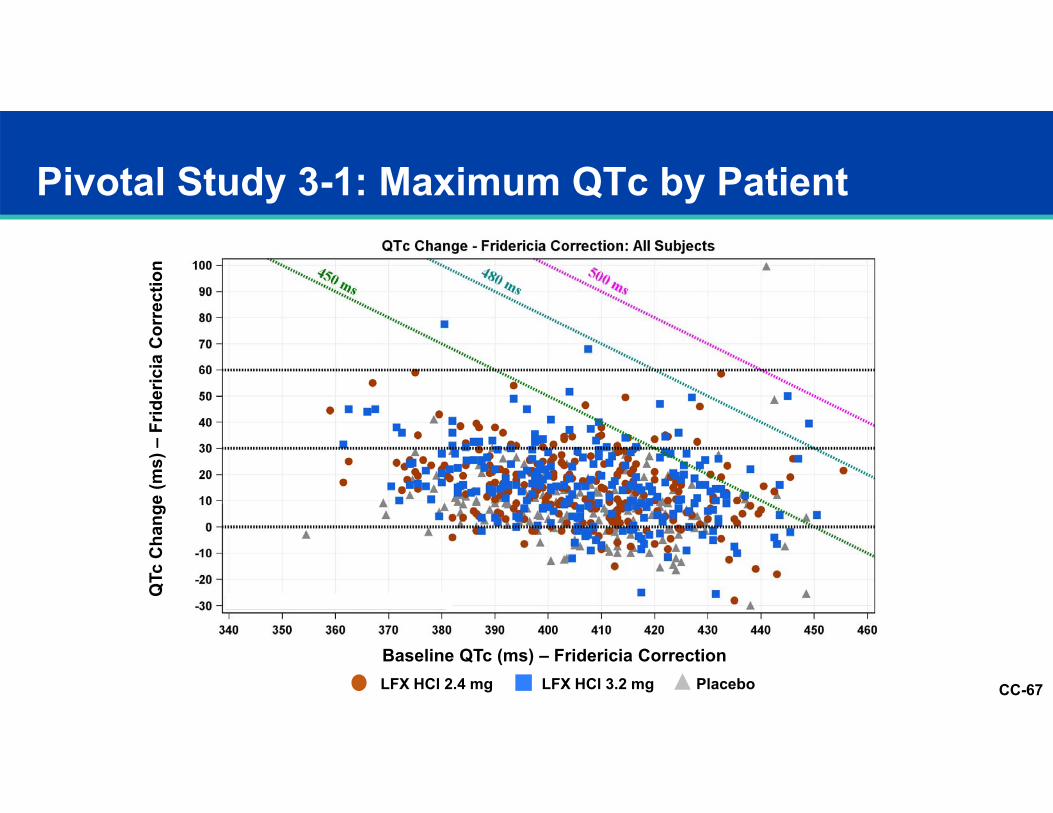
Pivotal Study 3-1: Maximum QTc by Patient
LFX HCl 2.4 mg PlaceboLFX HCl 3.2 mg
QTc
Cha
nge
(ms)
–Fr
ider
icia
Cor
rect
ion
Baseline QTc (ms) – Fridericia Correction
CC-68
Dose Adjustment Renal or Hepatic Insufficiency
Renal impairment‒ Reduce dose by 25% - 62.5% depending on degree of renal impairment
Hepatic impairment‒ Reduce dose by 25% - 62.5% depending on degree of hepatic impairment
CC-69
UK Safety
CC-70
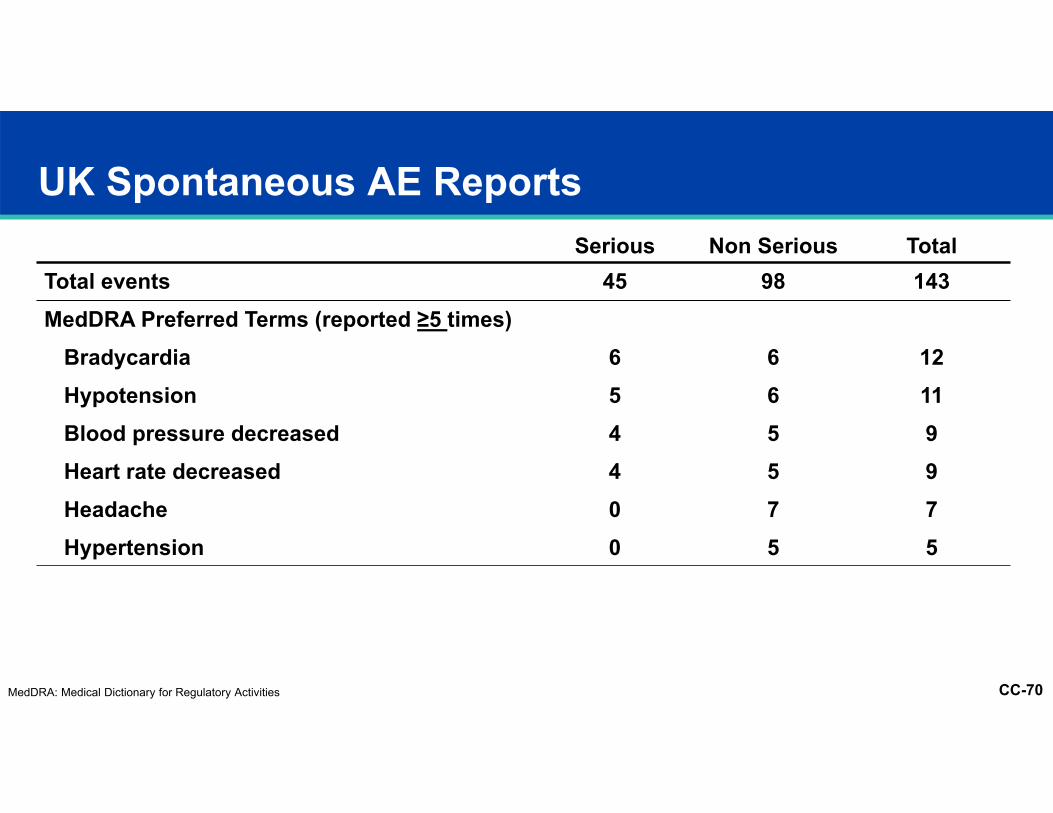
UK Spontaneous AE ReportsSerious Non Serious Total
Total events 45 98 143MedDRA Preferred Terms (reported ≥5 times)
Bradycardia 6 6 12Hypotension 5 6 11Blood pressure decreased 4 5 9Heart rate decreased 4 5 9Headache 0 7 7Hypertension 0 5 5
MedDRA: Medical Dictionary for Regulatory Activities
CC-71
UK Safety Assessment of Marketed Medicines (SAMM) Survey 19991
1074 opiate detoxifications 62.5% community setting Mean dose lofexidine 2.2 mg/day; mean duration 10 days Most frequent AEsDizziness (9%)Sedation (7%)Dry mouth (5%)
60% successful detoxificationNo difference community vs. inpatient
1. Akhurst, JS. The Use of Lofexidine by Drug Dependency Units in the United Kingdom. Eur Add. 1999;Res 5:43–9
CC-72
Summary Lofexidine Safety Exposure adequate Confirm placebo lack of efficacy Expected and manageable drug class effects at both doses Well-tolerated Precautions:Hypotension and bradycardia in at risk patientsRebound hypertensionQTc prolongation in high risk patientsRenal or hepatic insufficiencyCNS sedation
CC-73
Sponsor Education Materials Patient selectionAppropriate withdrawal management settingConcomitant psychiatric and medical conditionsConcomitant medicationsAppropriate and available support
Patient counselingDosing instructions and precautions (e.g. hydration, reduced activity)Appropriate expectationsWhat to look for and when to call
Clinical managementDose hold/reductionPrecautions and warnings
CC-74
Thomas R. Kosten, MDWaggoner Chair and Professor of Psychiatry and Pharmacology,Baylor College of MedicineDirector, Division of AddictionsPast President, American Academy of Addiction PsychiatryPast President, College on Problems of Drug DependenceDirector, Department of Defense National Substance Use Disorders ConsortiumPast Director, VA National Substance Abuse Quality Evaluation ResearchInitiative QUERI
Clinical Perspective
CC-75
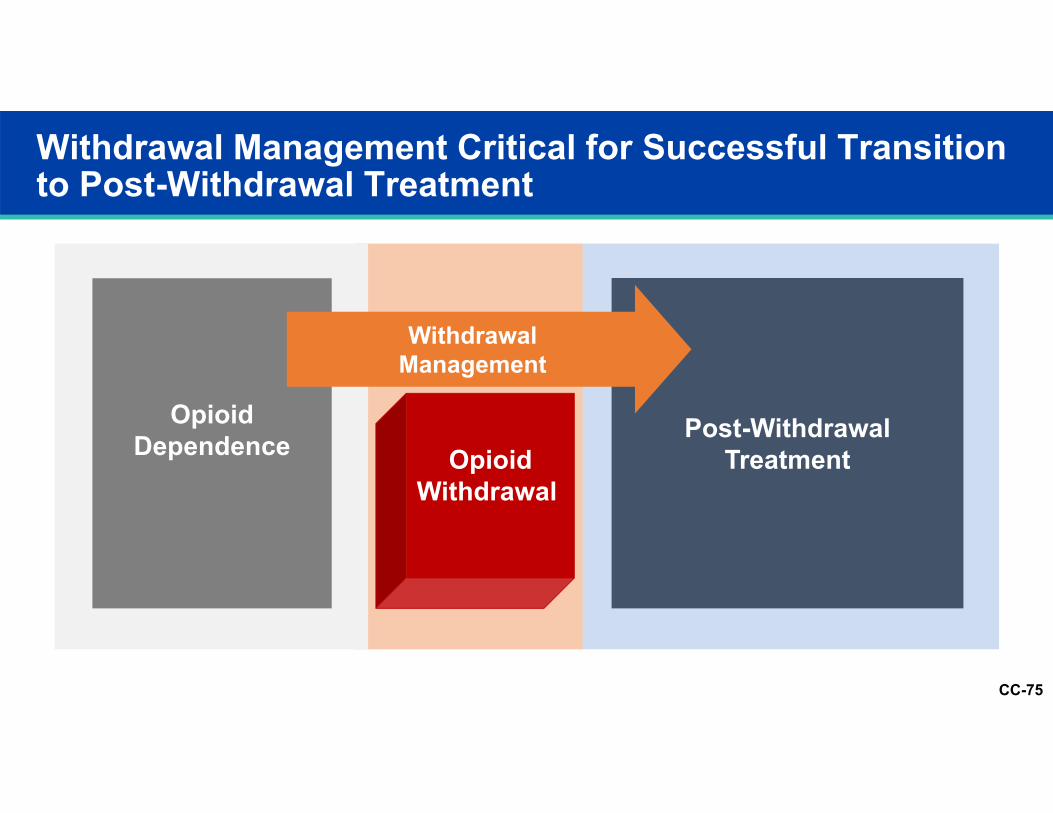
Withdrawal Management Critical for Successful Transition to Post-Withdrawal Treatment
Opioid Dependence Post-Withdrawal
TreatmentOpioid Withdrawal
WithdrawalManagement
CC-76
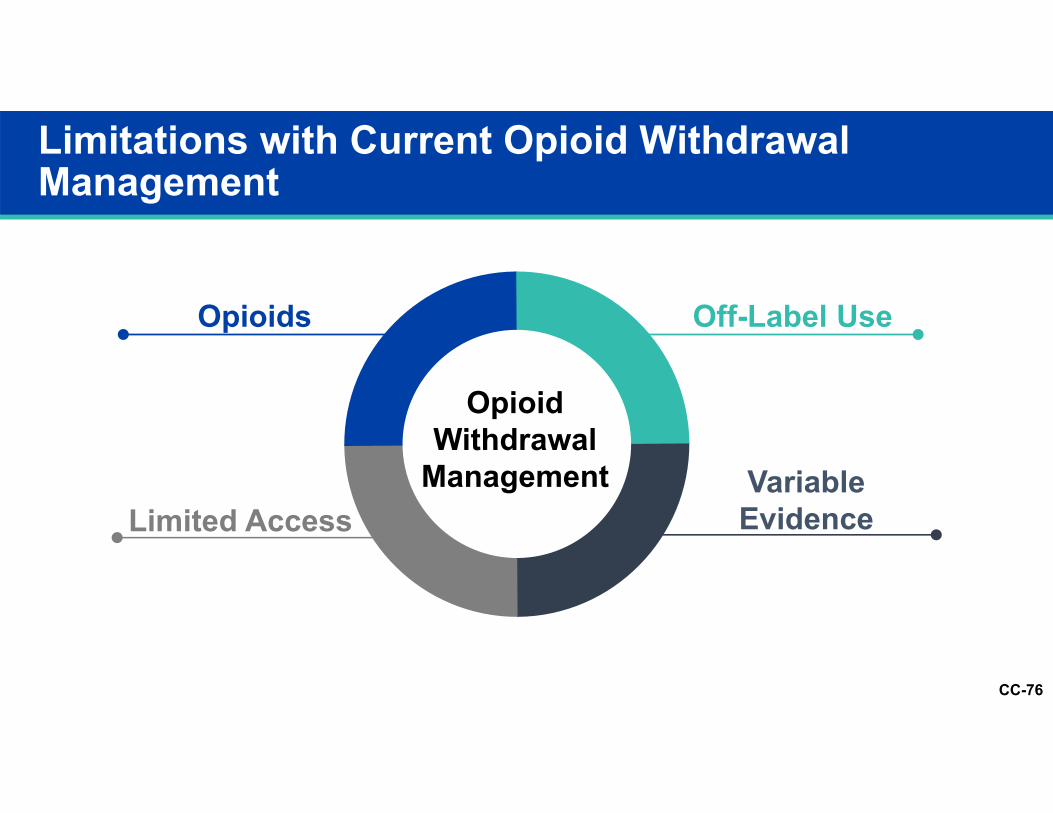
Limitations with Current Opioid Withdrawal Management
OpioidWithdrawal
Management
Opioids
Limited AccessVariable Evidence
Off-Label Use
CC-77
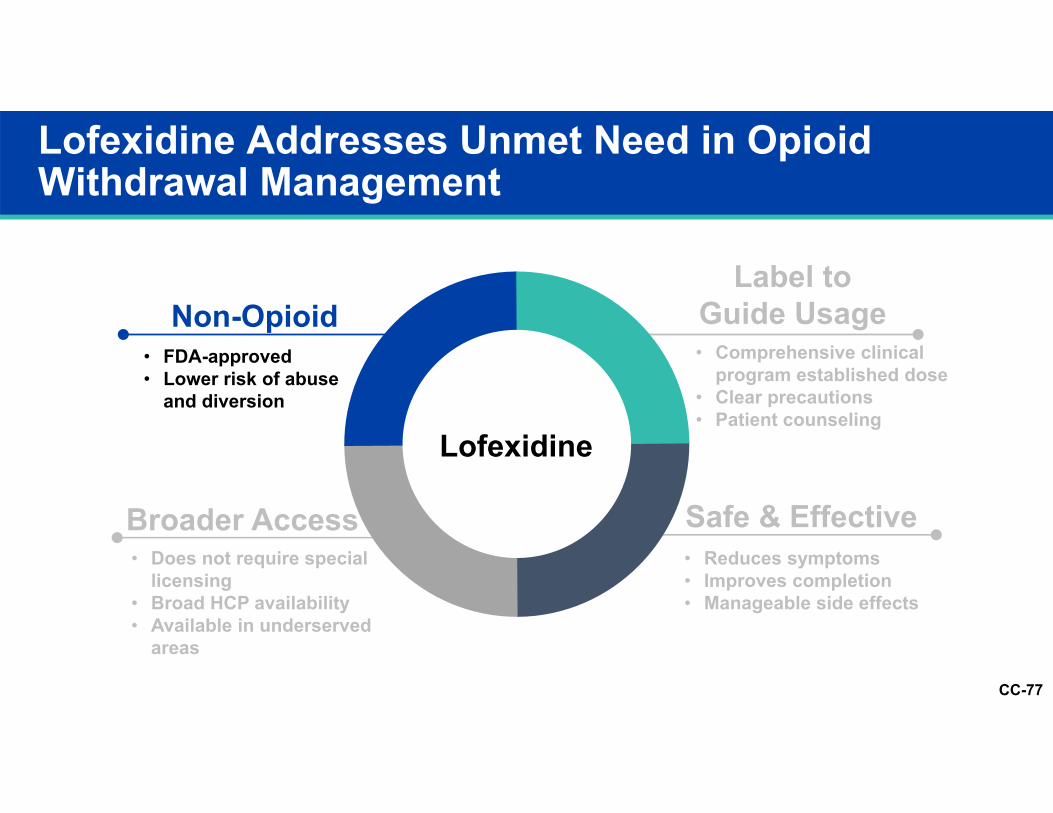
Lofexidine Addresses Unmet Need in Opioid Withdrawal Management
Lofexidine
Non-Opioid
Broader Access Safe & Effective
Label to Guide Usage• Comprehensive clinical
program established dose• Clear precautions• Patient counseling
• Does not require special licensing
• Broad HCP availability • Available in underserved
areas
• Reduces symptoms• Improves completion• Manageable side effects
• FDA-approved• Lower risk of abuse
and diversion
CC-78
Lofexidine Addresses Unmet Need in Opioid Withdrawal Management
Lofexidine
Non-Opioid
Broader Access Safe & Effective
Label to Guide Usage• Comprehensive clinical
program established dose• Clear precautions• Patient counseling
• Does not require special licensing
• Broad HCP availability • Available in underserved
areas
• Reduces symptoms• Improves completion• Manageable side effects
• FDA-approved• Lower risk of abuse
and diversion
CC-79
Lofexidine Addresses Unmet Need in Opioid Withdrawal Management
Lofexidine
Non-Opioid
Broader Access Safe & Effective
Label to Guide Usage• Comprehensive clinical
program established dose• Clear precautions• Patient counseling
• Does not require special licensing
• Broad HCP availability • Available in underserved
areas
• Reduces symptoms• Improves completion• Manageable side effects
• FDA-approved• Lower risk of abuse
and diversion
CC-80
Lofexidine Addresses Unmet Need in Opioid Withdrawal Management
Lofexidine
Non-Opioid
Broader Access Safe & Effective
Label to Guide Usage
• FDA-approved• Lower risk of abuse
and diversion
• Comprehensive clinical program established dose
• Clear precautions• Patient counseling
• Does not require special licensing
• Broad HCP availability • Available in underserved
areas
• Reduces symptoms• Improves completion• Manageable side effects
CC-81
Patient Risk1 - 2 Week Treatment Duration
PATIENT RISKS
Symptomatic orthostasis• Low rates of dizziness• Rare reports of syncope fall
Low rates of sedationTransient QTc changes
CC-82
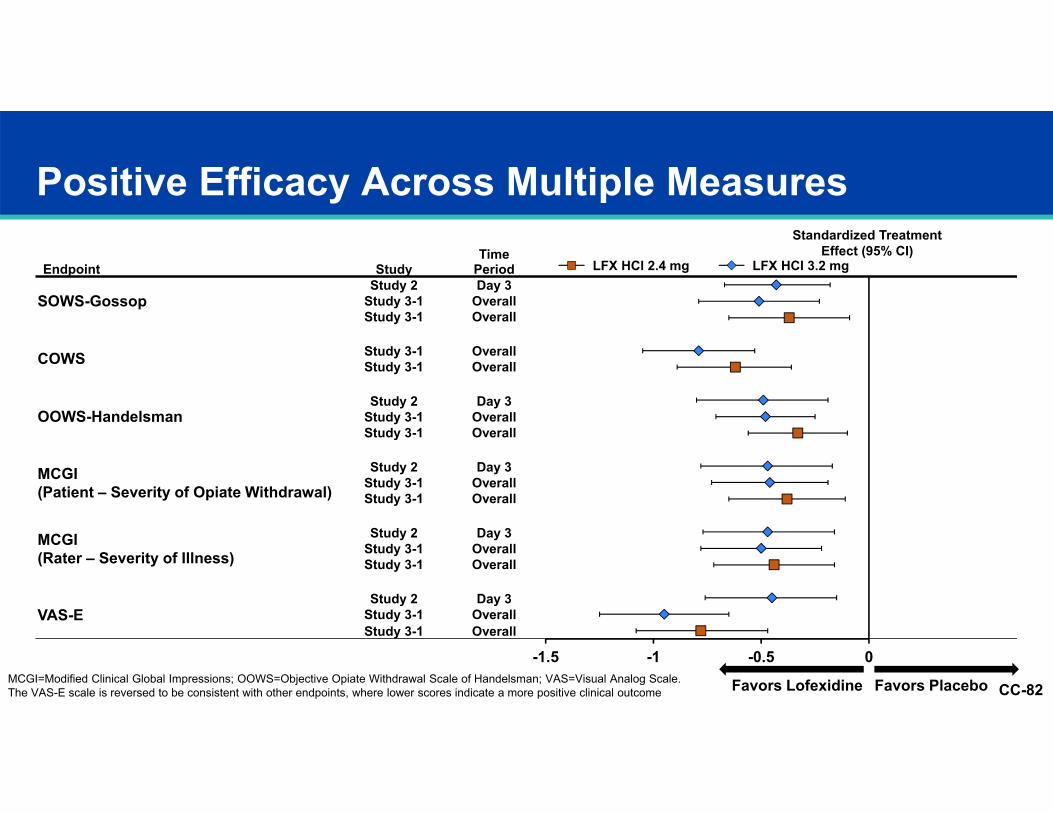
Positive Efficacy Across Multiple Measures
Endpoint StudyTime
Period
Standardized Treatment Effect (95% CI)
SOWS-GossopStudy 2 Day 3 -0.43 (-0.67, -0.18)
Study 3-1 Overall -0.51 (-0.79, -0.23)Study 3-1 Overall -0.37 (-0.65, -0.09)
COWS Study 3-1 Overall -0.79 (-1.05, -0.53)Study 3-1 Overall -0.62 (-0.89, -0.36)
OOWS-HandelsmanStudy 2 Day 3 -0.49 (-0.80, -0.19)
Study 3-1 Overall -0.48 (-0.71, -0.25)Study 3-1 Overall -0.33 (-0.56, -0.10)
MCGI (Patient – Severity of Opiate Withdrawal)
Study 2 Day 3 -0.47 (-0.78, -0.17)Study 3-1 Overall -0.46 (-0.73, -0.19)Study 3-1 Overall -0.38 (-0.65, -0.11)
MCGI (Rater – Severity of Illness)
Study 2 Day 3 -0.47 (-0.77, -0.16)Study 3-1 Overall -0.50 (-0.78, -0.22)Study 3-1 Overall -0.44 (-0.72, -0.16)
VAS-EStudy 2 Day 3 -0.45 (-0.76, -0.15)
Study 3-1 Overall -0.95 (-1.25, -0.65)Study 3-1 Overall -0.78 (-1.08, -0.47)
Favors Lofexidine Favors Placebo
LFX HCl 2.4 mg LFX HCl 3.2 mg
-1.5 -1 -0.5 0MCGI=Modified Clinical Global Impressions; OOWS=Objective Opiate Withdrawal Scale of Handelsman; VAS=Visual Analog Scale.The VAS-E scale is reversed to be consistent with other endpoints, where lower scores indicate a more positive clinical outcome
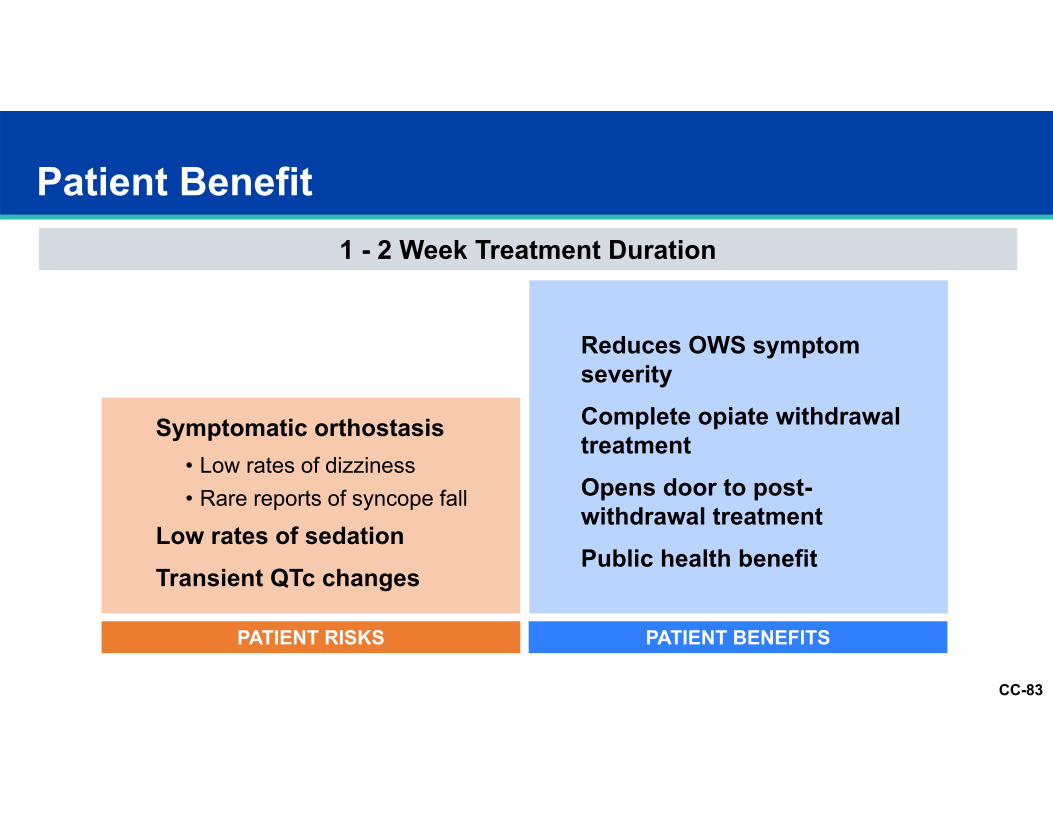
CC-83
Patient Benefit1 - 2 Week Treatment Duration
PATIENT BENEFITSPATIENT RISKS
Reduces OWS symptom severityComplete opiate withdrawal treatmentOpens door to post-withdrawal treatmentPublic health benefit
Symptomatic orthostasis• Low rates of dizziness• Rare reports of syncope fall
Low rates of sedationTransient QTc changes
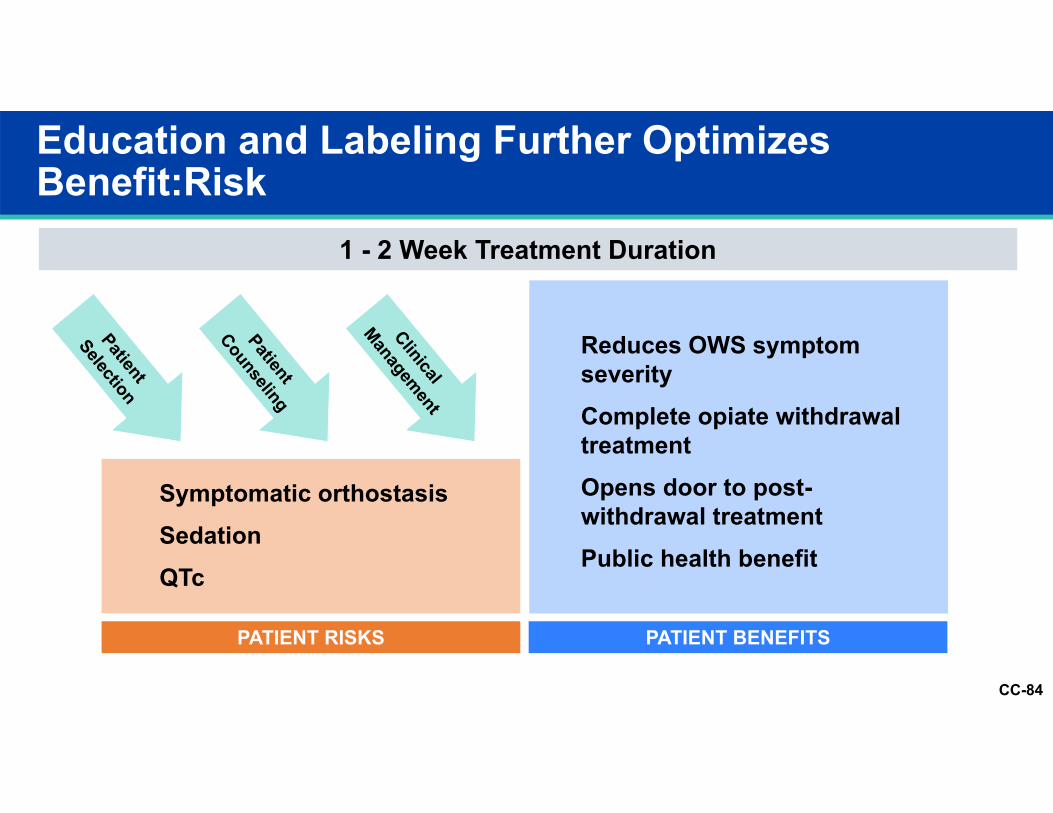
CC-84
PATIENT RISKS
Education and Labeling Further Optimizes Benefit:Risk
1 - 2 Week Treatment Duration
Symptomatic orthostasisSedationQTc
PATIENT BENEFITS
Reduces OWS symptom severityComplete opiate withdrawal treatmentOpens door to post-withdrawal treatmentPublic health benefit
CC-85
Opioid use disorder consequences demand attention
Current withdrawal management options leave unmet need
Lofexidine benefits for opioid withdrawal significant and its risks manageable
Both lofexidine doses safe and effective; 3.2 mg dose has best risk/benefit profile
Labeling and education plans can optimize appropriate product use
Holistic treatment approaches essential in opioid dependent patients, including withdrawal management
Lofexidine has positive benefit risk profile and provides valuable therapeutic option for managing opioid withdrawal.
Comprehensive Risk:Benefit Analysis
CC-86
Psychopharmacologic Drugs Advisory Committee MeetingMarch, 2018
LUCEMYRA (lofexidine)
Cl
O
Cl
HN
N
CC-87
Pediatric ProgramsPK Study in Adolescents to Determine Dose (12-17)Pediatric Iatrogenic Opioid Withdrawal (2-17)Neonatal Opioid Withdrawal Syndrome (0 to few weeks)
Opioid Taper ScenarioFocus on analgesic taper scenario, higher unmet need and consistent with
recommended treatment Characterize benefits in enhancing taper efficiency and comfort
Future Research Directions
CC-88
Supporting LUCEMYRA Patients
Patient and HCP websites
Encouragement phone application
Patient and caregiver handouts
“What to expect” for patients and caregivers
Collaborations with medical associations and societies
Connections to local resources
Support education for HCPs
CC-89
Additional Responders
Richard Bittman, PhD Statistician PresidentBittman Biostat, Inc.
Joseph Pergolizzi, MD Pain Specialist COONEMA Research Inc
Peter Kowey, MD, FACC, FHRS, FAHA Cardiologist
William Wikoff Smith Chair in Cardiovascular Research; Professor of Medicine and Clinical Pharmacology Jefferson Medical College
James Longstreth, PhD Pharmacokineticist Founder, PresidentLongstreth & Associates, Inc.
Kerri Schoedel, PhD Abuse/Dependence Pharmacologist
Director, Co-FounderAltreos Research Partners, Inc.
CC-90
Backup Slides Shown
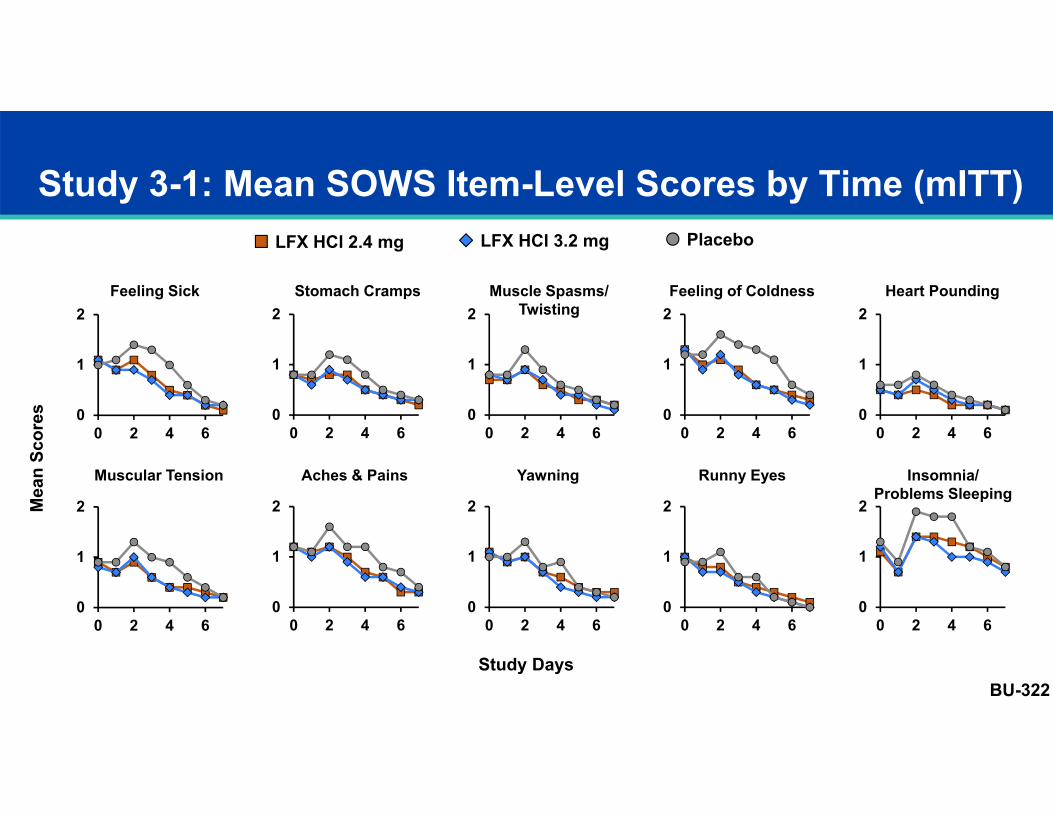
Study 3-1: Mean SOWS Item-Level Scores by Time (mITT)
Mea
n Sc
ores 0
1
2
0 2 4 6
Feeling Sick Stomach Cramps Muscle Spasms/Twisting
Feeling of Coldness Heart Pounding
Muscular Tension Aches & Pains Yawning Runny Eyes Insomnia/Problems Sleeping
Study Days
LFX HCl 2.4 mg LFX HCl 3.2 mg Placebo
BU-322
0
1
2
0 2 4 60
1
2
0 2 4 60
1
2
0 2 4 60
1
2
0 2 4 6
0
1
2
0 2 4 60
1
2
0 2 4 60
1
2
0 2 4 60
1
2
0 2 4 60
1
2
0 2 4 6
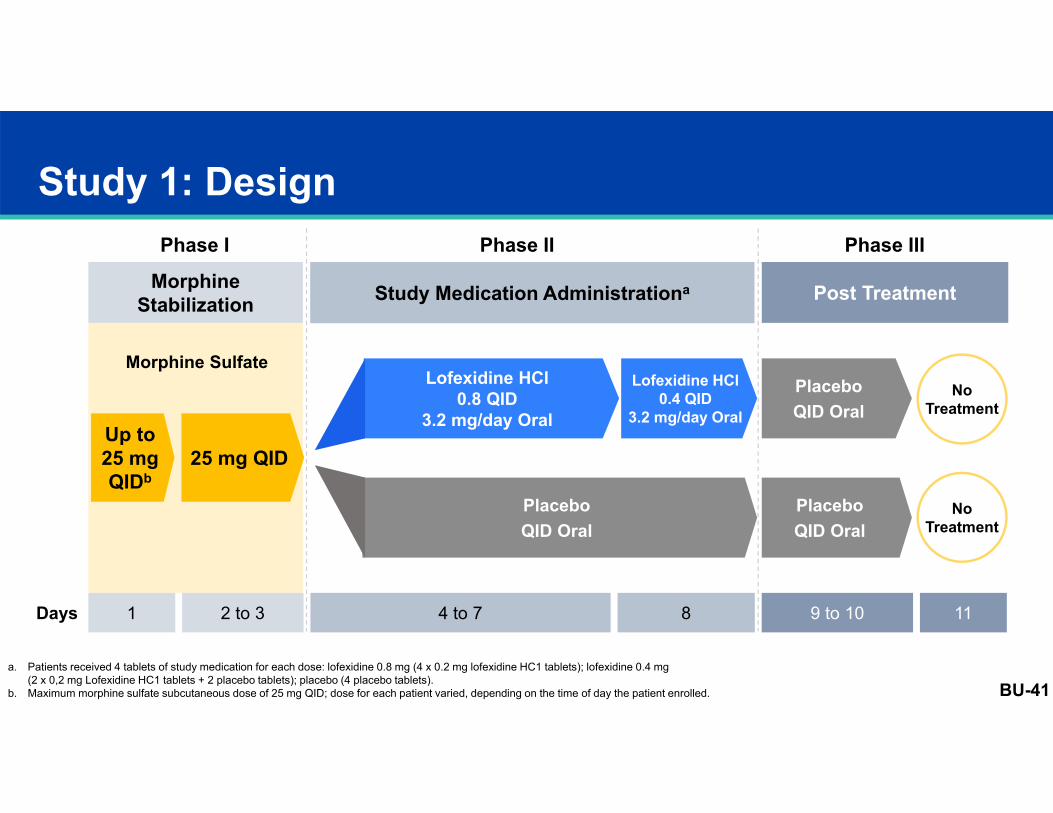
Study 1: Design
Morphine Stabilization Study Medication Administrationa Post Treatment
8 9 to 10
PlaceboQID Oral
PlaceboQID Oral
NoTreatment
NoTreatment
4 to 71Days
Lofexidine HCl0.8 QID
3.2 mg/day Oral
PlaceboQID Oral
a. Patients received 4 tablets of study medication for each dose: lofexidine 0.8 mg (4 x 0.2 mg lofexidine HC1 tablets); lofexidine 0.4 mg (2 x 0,2 mg Lofexidine HC1 tablets + 2 placebo tablets); placebo (4 placebo tablets).
b. Maximum morphine sulfate subcutaneous dose of 25 mg QID; dose for each patient varied, depending on the time of day the patient enrolled.
2 to 3 11
Phase I Phase II Phase III
Morphine SulfateLofexidine HCl
0.4 QID3.2 mg/day Oral
Up to 25 mg QIDb
25 mg QID
BU-41
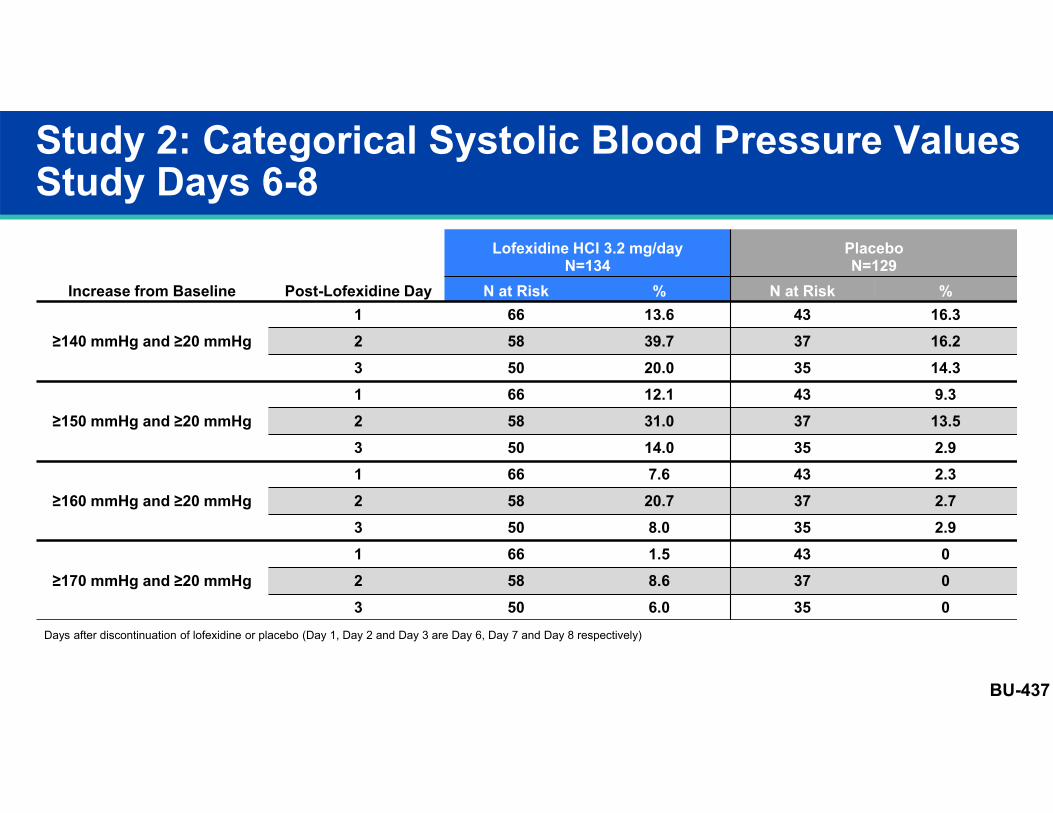
Study 2: Categorical Systolic Blood Pressure Values Study Days 6-8
Increase from Baseline Post-Lofexidine Day
Lofexidine HCl 3.2 mg/dayN=134
PlaceboN=129
N at Risk % N at Risk %
≥140 mmHg and ≥20 mmHg1 66 13.6 43 16.32 58 39.7 37 16.23 50 20.0 35 14.3
≥150 mmHg and ≥20 mmHg1 66 12.1 43 9.32 58 31.0 37 13.53 50 14.0 35 2.9
≥160 mmHg and ≥20 mmHg1 66 7.6 43 2.32 58 20.7 37 2.73 50 8.0 35 2.9
≥170 mmHg and ≥20 mmHg1 66 1.5 43 02 58 8.6 37 03 50 6.0 35 0
Days after discontinuation of lofexidine or placebo (Day 1, Day 2 and Day 3 are Day 6, Day 7 and Day 8 respectively)
BU-437
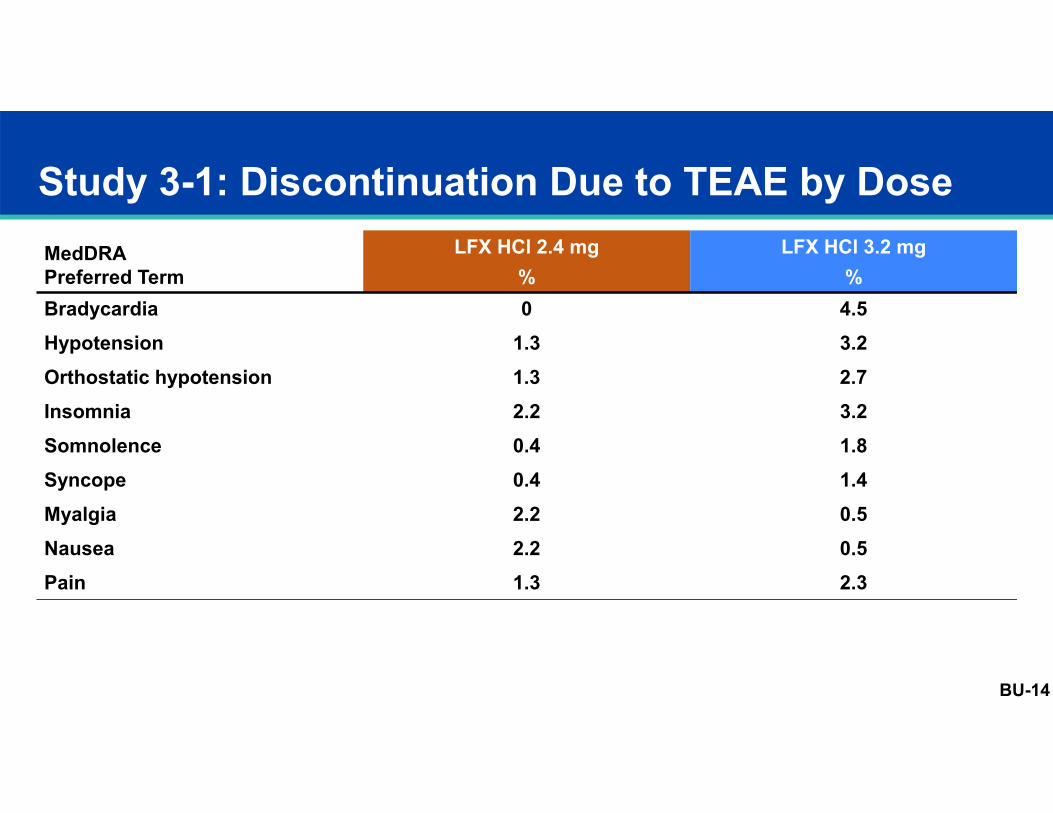
Study 3-1: Discontinuation Due to TEAE by Dose MedDRAPreferred Term
LFX HCl 2.4 mg%
LFX HCl 3.2 mg%
Bradycardia 0 4.5Hypotension 1.3 3.2Orthostatic hypotension 1.3 2.7Insomnia 2.2 3.2Somnolence 0.4 1.8Syncope 0.4 1.4Myalgia 2.2 0.5Nausea 2.2 0.5Pain 1.3 2.3
BU-14
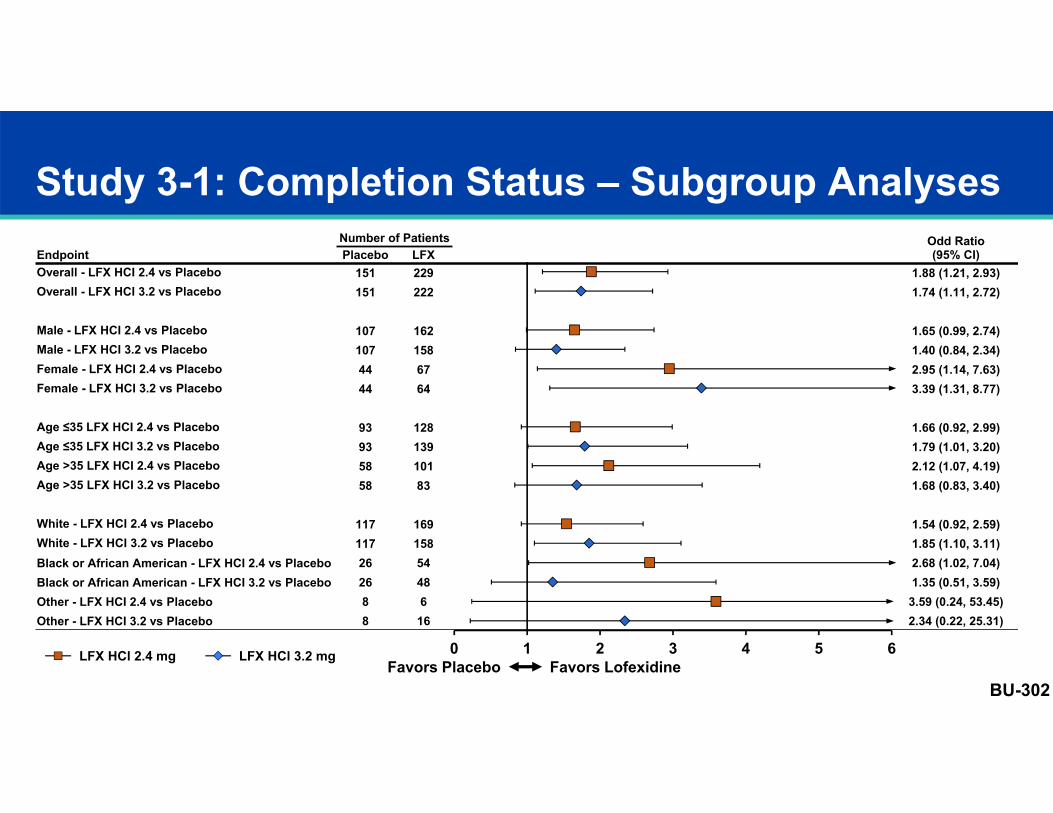
Study 3-1: Completion Status – Subgroup AnalysesEndpoint
Number of Patients Odd Ratio(95% CI)Placebo LFX
Overall - LFX HCI 2.4 vs Placebo 151 229 1.88 (1.21, 2.93)Overall - LFX HCI 3.2 vs Placebo 151 222 1.74 (1.11, 2.72)
Male - LFX HCI 2.4 vs Placebo 107 162 1.65 (0.99, 2.74)Male - LFX HCI 3.2 vs Placebo 107 158 1.40 (0.84, 2.34)Female - LFX HCI 2.4 vs Placebo 44 67 2.95 (1.14, 7.63)Female - LFX HCI 3.2 vs Placebo 44 64 3.39 (1.31, 8.77)
Age ≤35 LFX HCI 2.4 vs Placebo 93 128 1.66 (0.92, 2.99)Age ≤35 LFX HCI 3.2 vs Placebo 93 139 1.79 (1.01, 3.20)Age >35 LFX HCI 2.4 vs Placebo 58 101 2.12 (1.07, 4.19)Age >35 LFX HCI 3.2 vs Placebo 58 83 1.68 (0.83, 3.40)
White - LFX HCI 2.4 vs Placebo 117 169 1.54 (0.92, 2.59)White - LFX HCI 3.2 vs Placebo 117 158 1.85 (1.10, 3.11)Black or African American - LFX HCI 2.4 vs Placebo 26 54 2.68 (1.02, 7.04)Black or African American - LFX HCI 3.2 vs Placebo 26 48 1.35 (0.51, 3.59)Other - LFX HCI 2.4 vs Placebo 8 6 3.59 (0.24, 53.45)Other - LFX HCI 3.2 vs Placebo 8 16 2.34 (0.22, 25.31)
Favors Placebo Favors LofexidineLFX HCl 2.4 mg LFX HCl 3.2 mg 0 1 2 3 4 5 6
BU-302
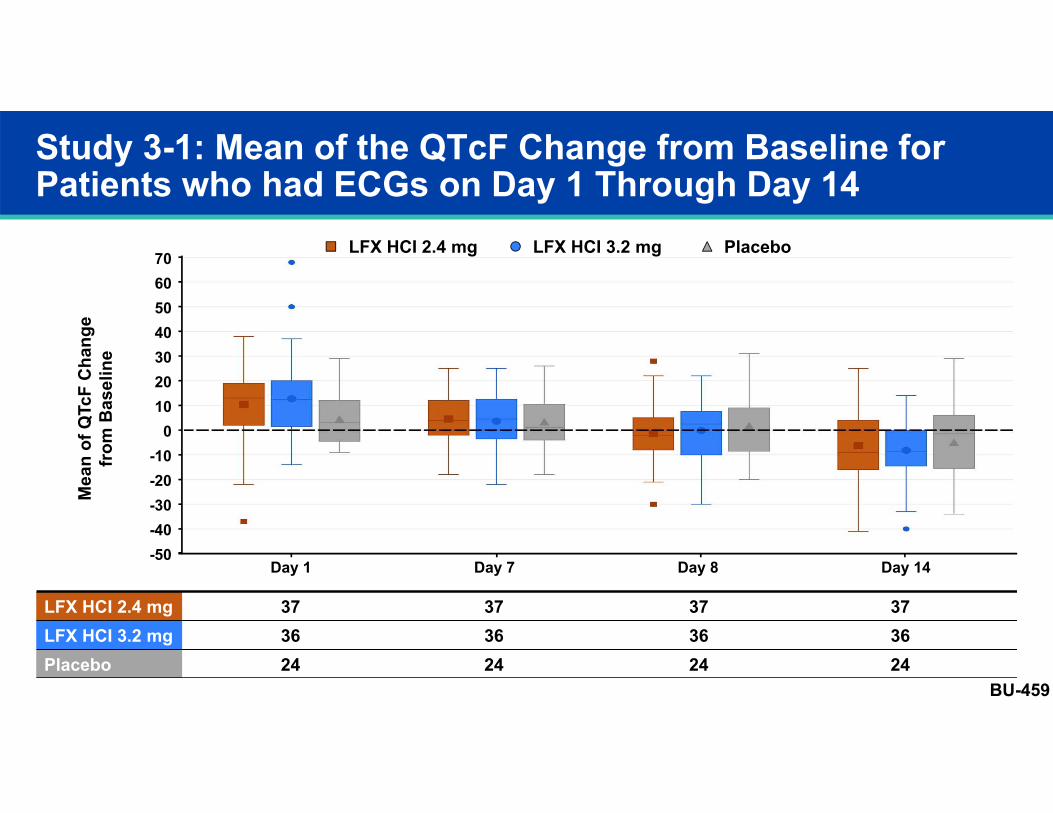
Study 3-1: Mean of the QTcF Change from Baseline for Patients who had ECGs on Day 1 Through Day 14
LFX HCI 2.4 mg 37 37 37 37LFX HCI 3.2 mg 36 36 36 36Placebo 24 24 24 24
70605040
-20-30-40-50
20100
-10
30
Day 1 Day 7 Day 8 Day 14
Mea
n of
QTc
FC
hang
efr
om B
asel
ine
LFX HCI 2.4 mg LFX HCI 3.2 mg Placebo
BU-459
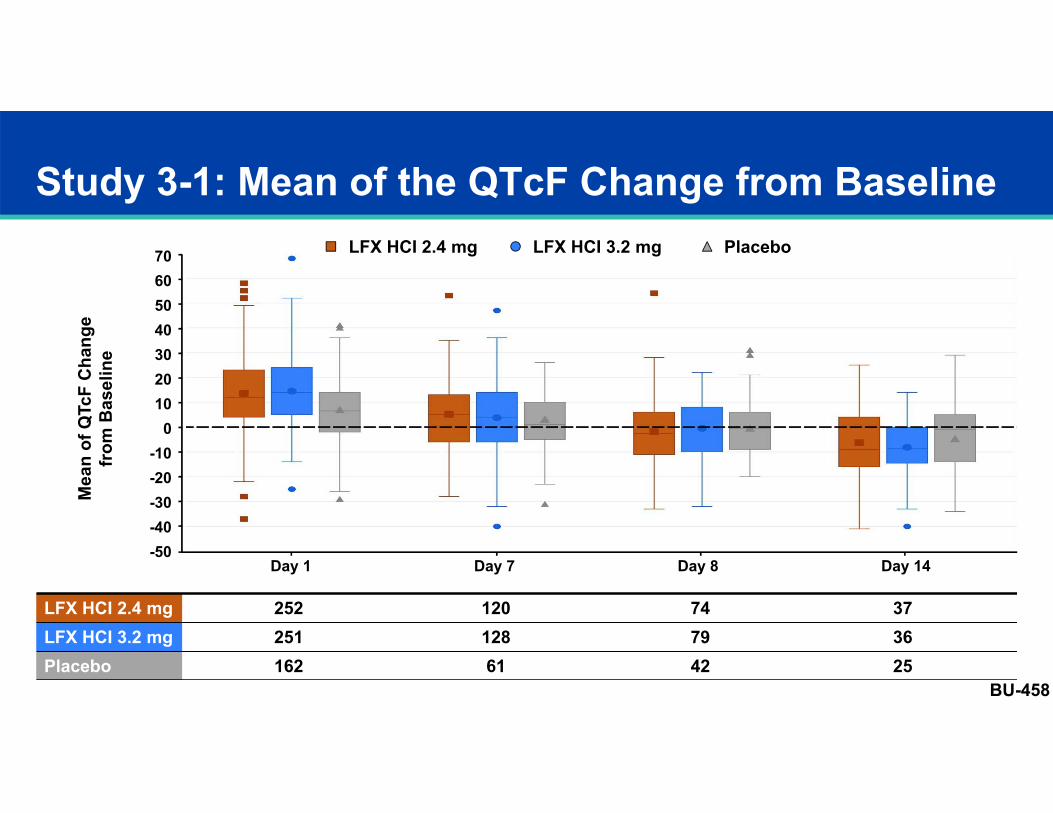
LFX HCI 2.4 mg 252 120 74 37LFX HCI 3.2 mg 251 128 79 36Placebo 162 61 42 25
Study 3-1: Mean of the QTcF Change from Baseline70605040
-20-30-40-50
20100
-10
30
Day 1 Day 7 Day 8 Day 14
Mea
n of
QTc
FC
hang
efr
om B
asel
ine
LFX HCI 2.4 mg LFX HCI 3.2 mg Placebo
BU-458
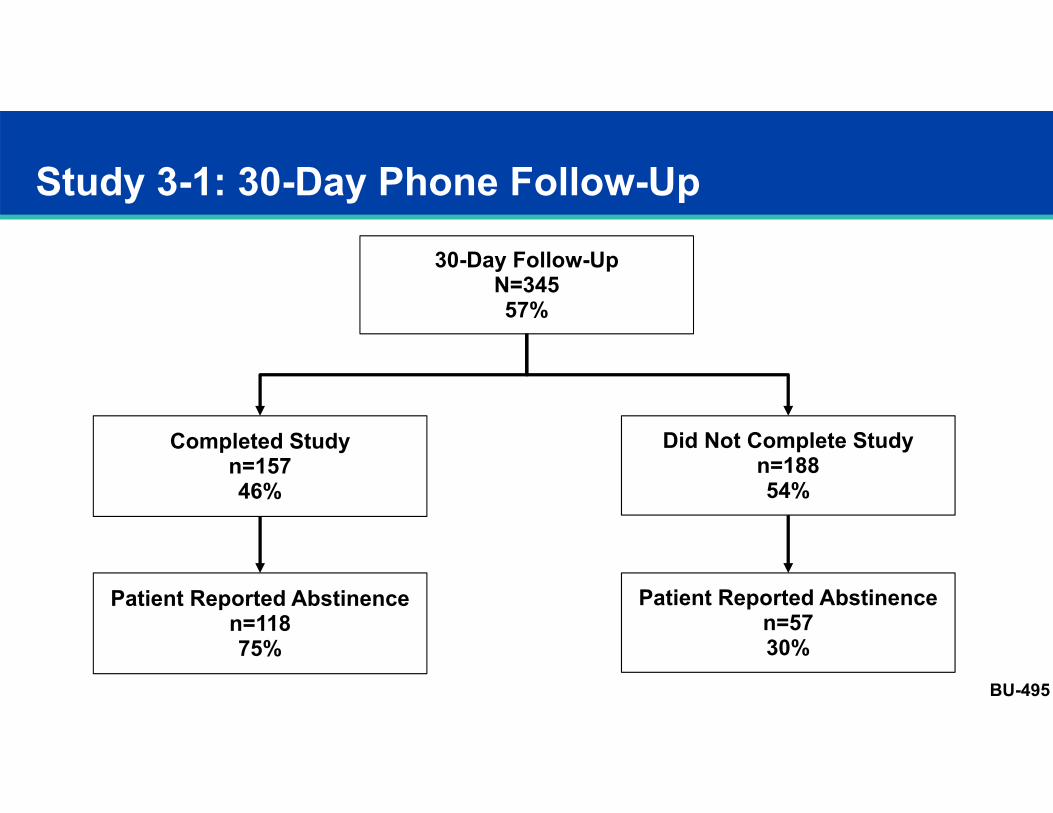
Study 3-1: 30-Day Phone Follow-Up
30-Day Follow-UpN=34557%
Completed Studyn=15746%
Did Not Complete Studyn=18854%
Patient Reported Abstinence n=11875%
Patient Reported Abstinence n=5730%
BU-495