Embed Size (px)
Citation preview
LT Scott Raisor, PharmDIndian Health Service, Phoenix Area,Colorado River Service Unit
1962: Shift from distribution to clinical services
1969: Pharmacists provide direct patient care as primary care providers
1996: RADM Michael Trujillo codifies Pharmacists as Primary Care Providers (PCPs) with prescriptive authority
1997: National Clinical Pharmacy Specialist (NCPS) certification established
2011: PHS Pharmacy Report to the Surgeon General and the Surgeon General’s Support Letter
1.5 billion preventable medication related problems occur each year
The United States health care system spends over $177 billion dollars annually on medication related problems
“Advance beyond discussion of the value of expanded roles of pharmacists and move towards health system support and implementation of these roles.”
• Medication Therapy Management services are patient centered assessment and evaluation of the patient’s full medication regimen and not only individual medications
• Goals:• Optimize medication use• Improve collaboration• Enhance communication• Empower patients

MTM is separate and distinct from pharmacist managed disease state clinics
Pharmacist managed clinics require and provide a higher level of care
Medicare Part D sponsors are required to provide MTM services to their patients
42 CFR 423.153 (d)
(d)Medication therapy management program (MTMP)— (1) General rule. A Part D sponsor must have established a MTMP that—
(i) Is designed to ensure that covered Part D drugs prescribed to targeted beneficiaries described in paragraph (d)(2) of this section are appropriately used to optimize therapeutic outcomes through improved medication use; (ii) Is designed to reduce the risk of adverse events, including adverse drug interactions, for targeted beneficiaries described in paragraph (d)(2) of this section; (iii) May be furnished by a pharmacist or other qualified provider; and (iv) May distinguish between services in ambulatory and institutional settings. (v) Must enroll targeted beneficiaries using an opt-out method of enrollment only. (vi) Must target beneficiaries for enrollment in the MTMP at least quarterly during each plan year. (vii) Must offer a minimum level of medication therapy management services for each beneficiary enrolled in the MTMP that includes all of the following:
(A) Interventions for both beneficiaries and prescribers. (B) Annual comprehensive medication review with written summaries. The comprehensive medication review must include an interactive, person-to-person, or telehealth consultation performed by a pharmacist or other qualified provider unless the beneficiary is in a long-term care setting and may result in a recommended medication action plan. (C) Quarterly targeted medication reviews with follow-up interventions when necessary. (D) Standardized action plans and summaries that comply with requirements as specified by CMS for the standardized format.
Medicare criteria1. Multiple chronic
disease states2. Multiple
medications3. High drug costs
Medicaid Florida, Iowa,
Maryland, Minnesota, Missouri, Mississippi, Ohio, Virginia
Private plans Employers Self-pay
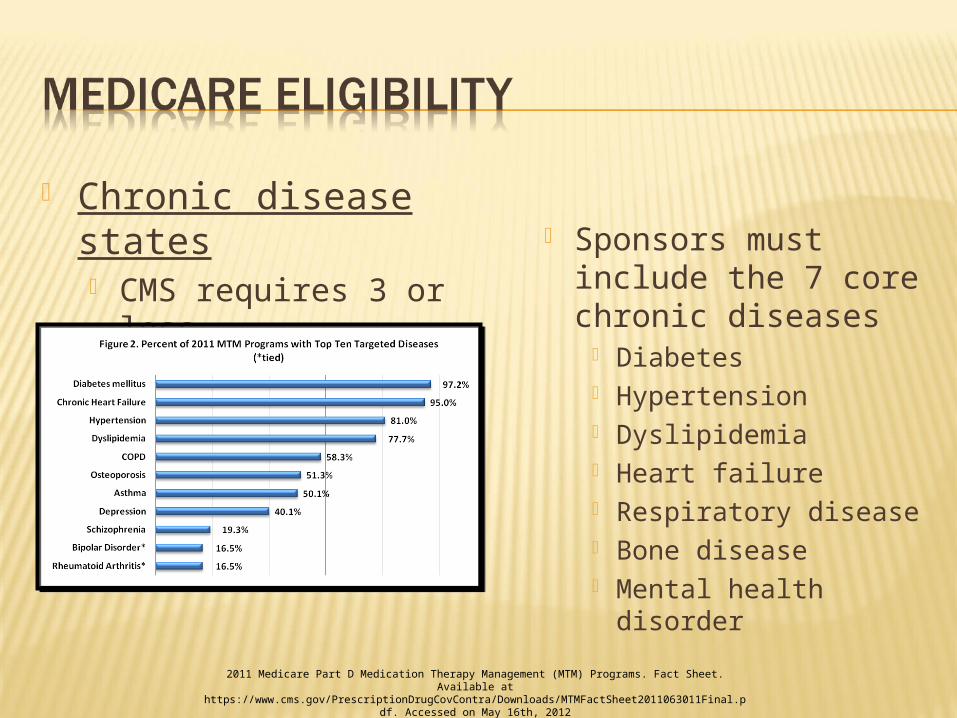
Chronic disease states CMS requires 3 or
less
Sponsors must include the 7 core chronic diseases
Diabetes Hypertension Dyslipidemia Heart failure Respiratory disease Bone disease Mental health disorder
2011 Medicare Part D Medication Therapy Management (MTM) Programs. Fact Sheet. Available at https://www.cms.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet2011063011Final.pdf.
Accessed on May 16th, 2012
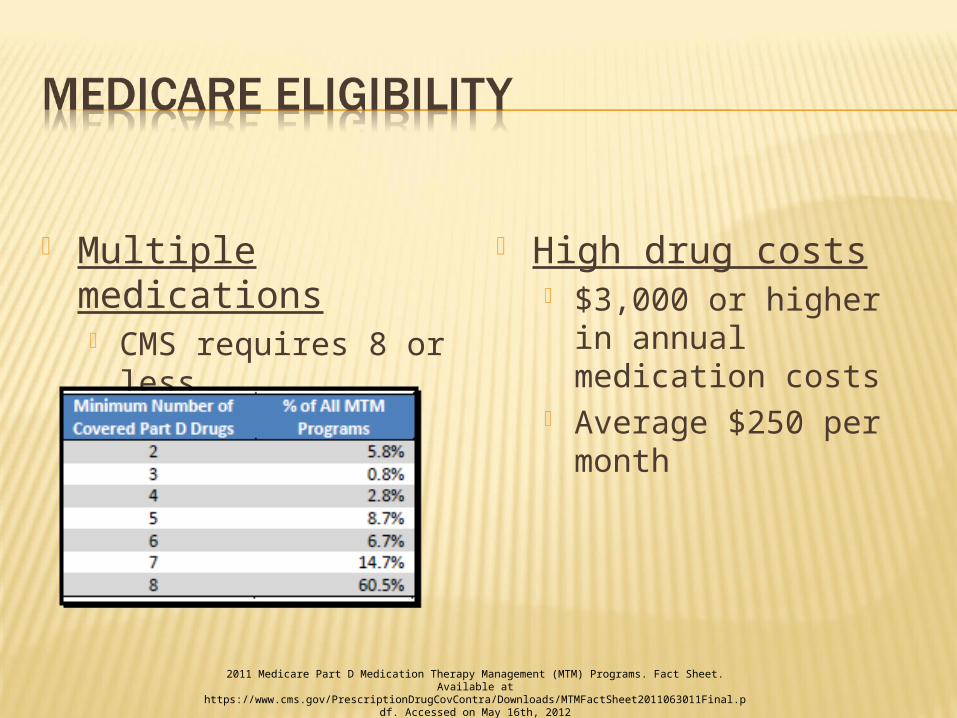
Multiple medications CMS requires 8 or
less
High drug costs $3,000 or higher in
annual medication costs
Average $250 per month
2011 Medicare Part D Medication Therapy Management (MTM) Programs. Fact Sheet. Available at https://www.cms.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet2011063011Final.pdf.
Accessed on May 16th, 2012
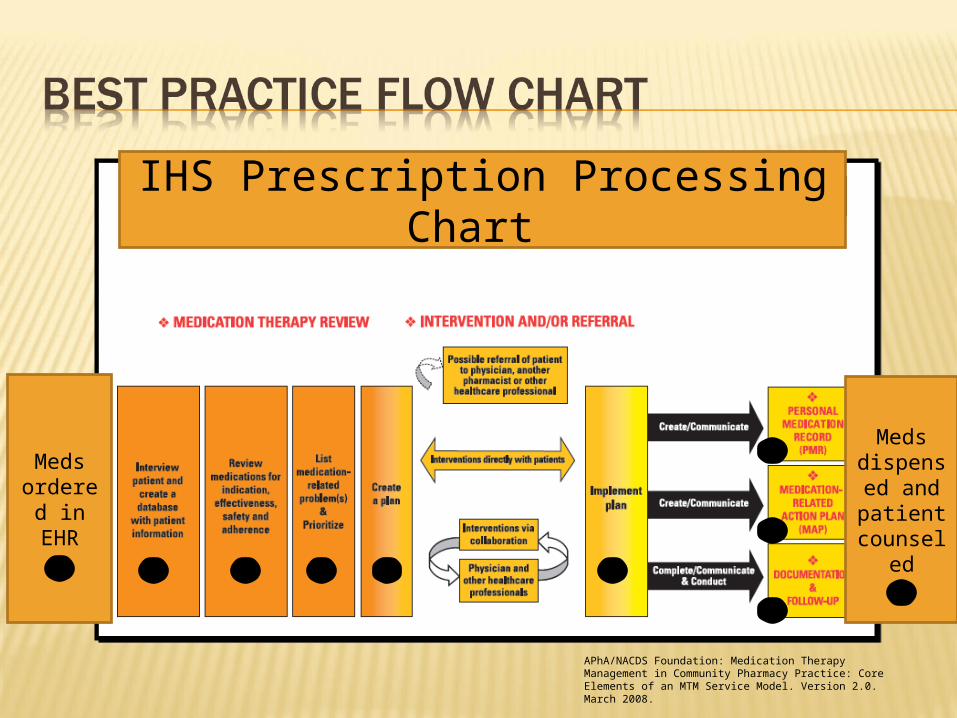
APhA/NACDS Foundation: Medication Therapy Management in Community Pharmacy Practice: Core Elements of an MTM Service Model. Version 2.0. March 2008.
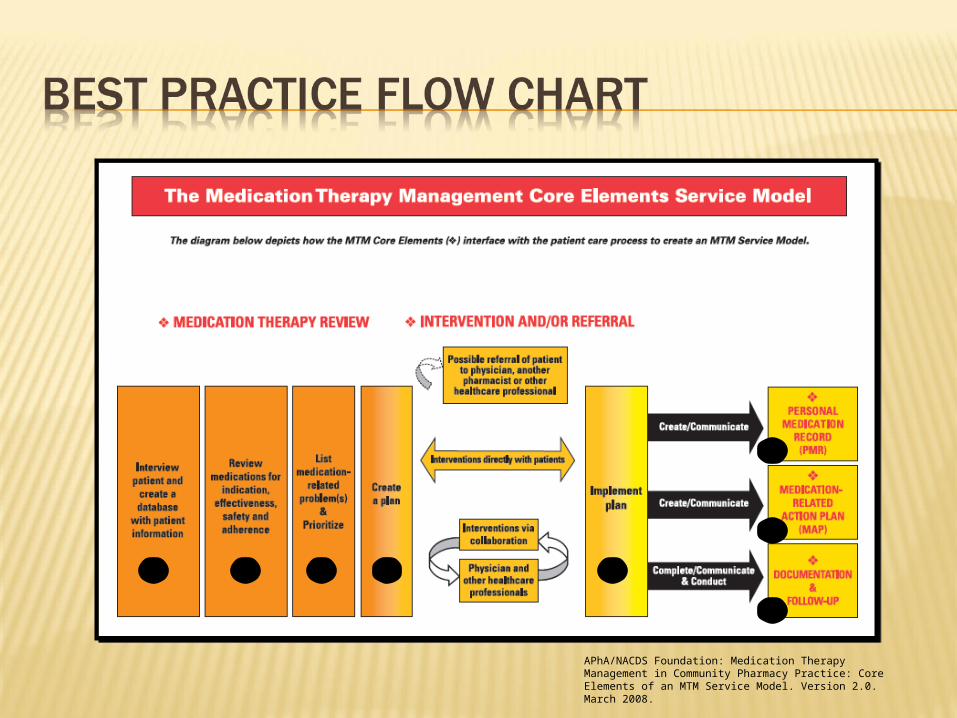
CMS regulations established a general framework that allows for best practices
10 pharmacy organizations collaborated to develop the core elements of an MTM visit
Medication Therapy Review (MTR)
“is a systematic process of collecting patient-specific information, assessing medication therapies to identify medication-related problems, developing a prioritized list of medication-related problems, and creating a plan to resolve them”
Personal Medication Record (PMR)
“is a comprehensive record of the patient’s medications”
Medication-Related Action Plan (MAP)
“is a patient-centric document containing a list of actions for the patient to use in tracking progress for self-management”
Interventions or Referrals “The pharmacist provides
consultative services and intervenes to address medication-related problems; when necessary, the pharmacist refers the patient to a physician or other healthcare professional”
Documentation and Follow Up “MTM services are
documented in a consistent manner, and a follow-up MTM visit is scheduled based on the patient’s medication-related needs, or the patient is transitioned from one care setting to another”
APhA/NACDS Foundation: Medication Therapy Management in Community Pharmacy Practice: Core Elements of an MTM Service Model. Version 2.0. March 2008.
APhA/NACDS Foundation: Medication Therapy Management in Community Pharmacy Practice: Core Elements of an MTM Service Model. Version 2.0. March 2008.
Medicare sponsors must provide a minimum level of MTM services1. Comprehensive Medication Review (CMR)
Annually
2. Targeted Medication Review (TMR) Quarterly
Comprehensive annual review of all medications
Interactive person to person Phone call Pharmacy visit
Affordable Care Act standardizes the content and format of the CMR starting January 1, 2013 Components
Cover Letter Medication Action Plan Personal Medication List
TMR must be provided at least quarterly
TMR is meant to address specific or potential medication-related problems
Does not have to be face-to-face
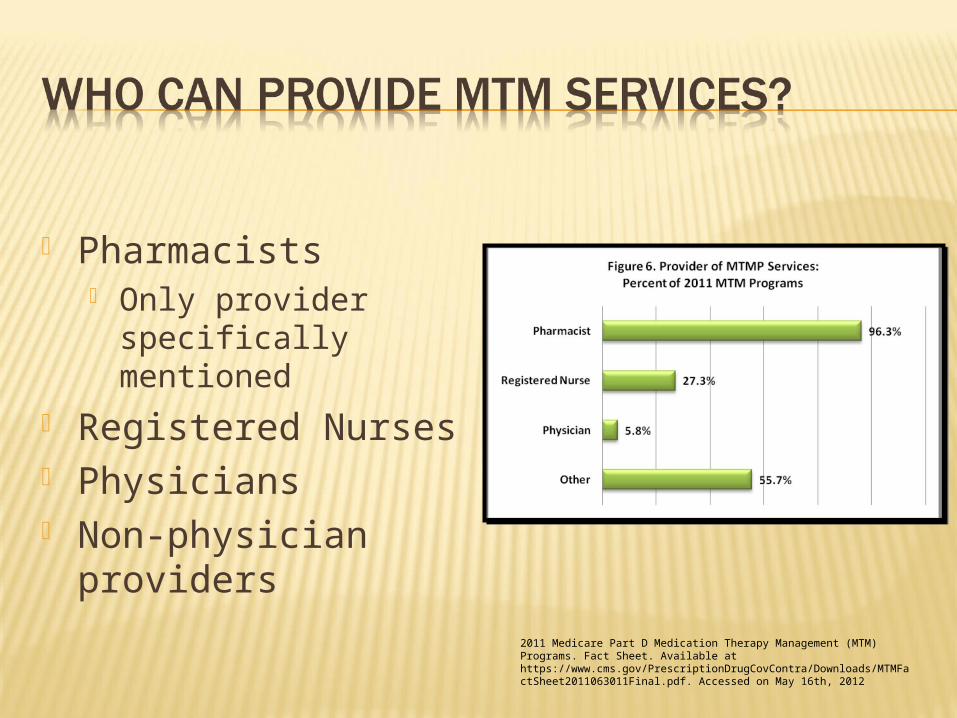
Pharmacists Only provider
specifically mentioned
Registered Nurses Physicians Non-physician
providers
2011 Medicare Part D Medication Therapy Management (MTM) Programs. Fact Sheet. Available at https://www.cms.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet2011063011Final.pdf. Accessed on May 16th, 2012
Electronic Health Record (EHR) Allows for comprehensive reviews
Physician notes, lab work, and medication lists IHS mode of counseling
New Three prime questions
Refill Show and tell
Open dialogue about disease not just medicine
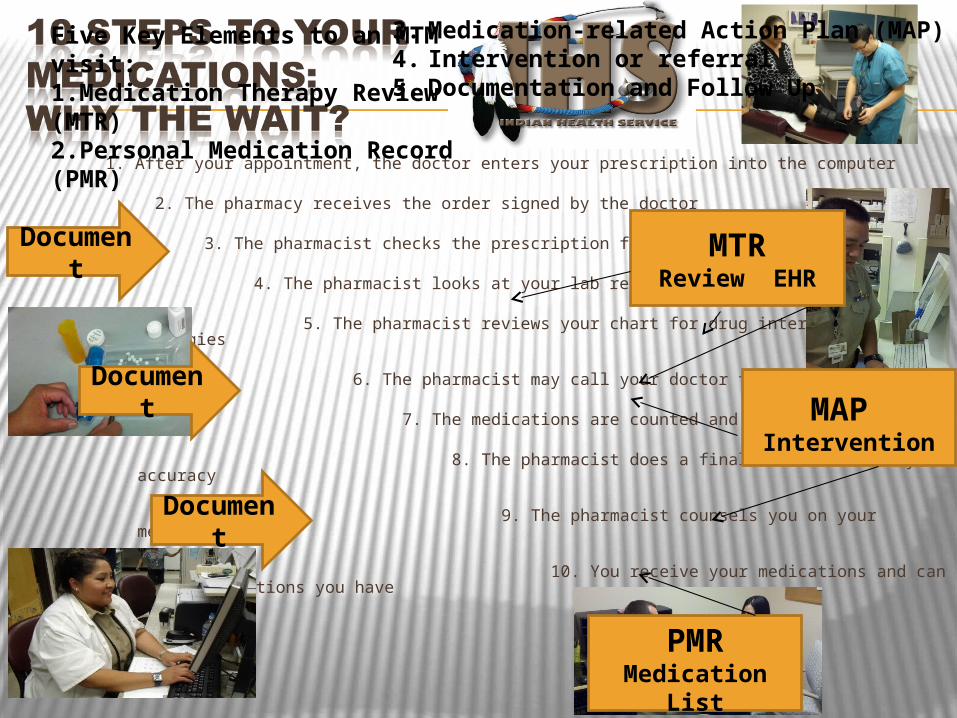
1. After your appointment, the doctor enters your prescription into the computer
2. The pharmacy receives the order signed by the doctor
3. The pharmacist checks the prescription for errors
4. The pharmacist looks at your lab results
5. The pharmacist reviews your chart for drug interactions and allergies
6. The pharmacist may call your doctor for questions
7. The medications are counted and packaged
8. The pharmacist does a final check for safety and accuracy
9. The pharmacist counsels you on your medications
10. You receive your medications and can ask any questions you have
Five Key Elements to an MTM visit:1.Medication Therapy Review (MTR)2.Personal Medication Record (PMR)
Document
Document
Document
3. Medication-related Action Plan (MAP)4. Intervention or referral5. Documentation and Follow Up
MTRReview EHR
PMRMedication
List
MAP Intervention
APhA/NACDS Foundation: Medication Therapy Management in Community Pharmacy Practice: Core Elements of an MTM Service Model. Version 2.0. March 2008.
IHS Prescription Processing Chart
Meds ordered in EHR
Meds dispensed and patient counsel
ed
Our legacy of innovation has allowed PHS pharmacists to lead the profession Providing clinical services since 1962 We are already providing MTM for our
patients
Potential reimbursement opportunities?
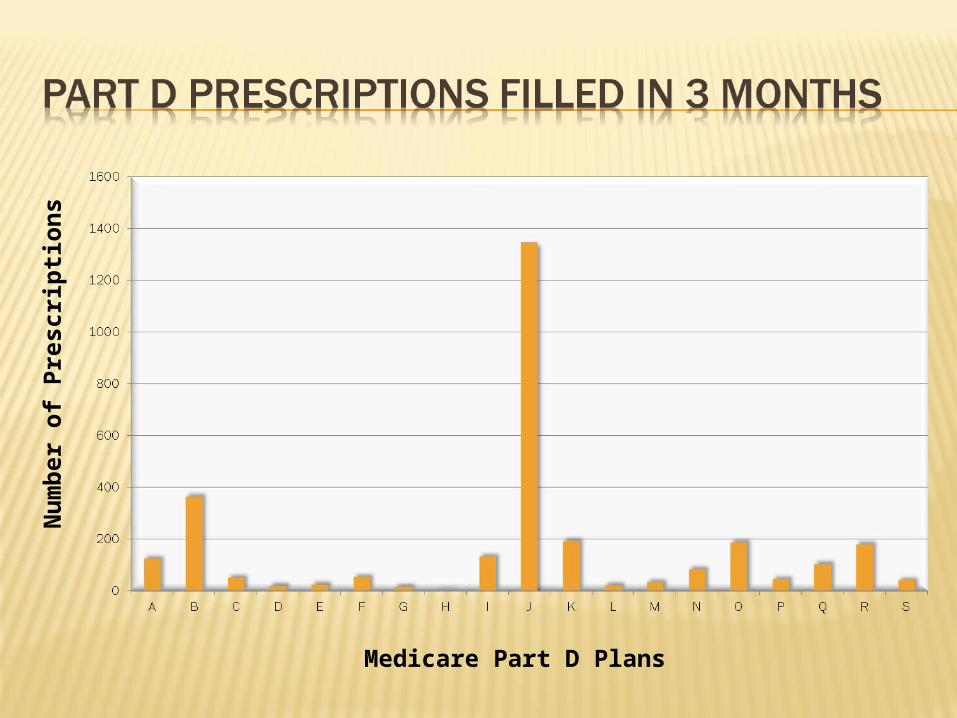
Medicare Part D Plans
Nu
mb
er
of
Pre
scri
pti
on
s
The largest Part D provider does not allow for reimbursement to community pharmacists for MTM services
The second largest provider only has four patients who qualify for MTM reimbursable services
Part D sponsors determine payments for MTM services Considered
administrative costs 80% allow external
personnel 31% use vendors 25% use community
pharmacists Plans require
contracts with pharmacies Separate from
medication dispensing
There is not much published on reimbursement Limited to vendor’s
published numbers
MirixaPro®®
Mirixa.com No cost for
participation
MirixaEdge®®
Pay Provides
documentation to submit to non-contracted part D plans or for out of pocket billing
Outcomes®®
Getoutcomes.com No cost for
participation
Others: PharmMD®®
Pharmmd.com Employ pharmacists Can make
$2,000/month
MirixaPro®®
Comprehensive medication review $60 Welcome review $40 Medication adherence
15 minute initial $30 10 minute follow up (2) $20
Cardiovascular risk 45 minute initial $90 Follow up $30
www.mirixa.com
Outcomes®®
+Comprehensive Medication Review $50 to $75
+Prescriber Consultation× Cost Efficacy Management $20× Drug Therapy Problem $20
+Patient Compliance Consultation $20+Patient Education/Monitoring $10+Prescriber Refusal $2+Patient Refusal $2
www.getoutcomes.com
Providing MTM services improves outcomes
Reimbursement for pharmacist-delivered patient care is a step forward, BUT: Part D pays the pharmacy not the pharmacist Pharmacists are not the only providers Right now, MTM does not look to prevention
Eligible patients are already a burden on health system
“Pharmacist-delivered patient care services fit most definitions of “primary care” services (with the exception of diagnosis) as defined by major medical and health organizations”
“Compensation … should reflect the level of care provided”
Giberson S, Yoder S, Lee MP. Improving Patient and Health System Outcomes through Advanced Pharmacy Practice. A Report to the U.S. Surgeon General. Office of the Chief Pharmacist. U.S.
Public Health Service. Dec 2011.
Potential reimbursement for actions that PHS pharmacists engage in currently Create time to make appointments, proper
documentation, and provide opportunities for reimbursement and reporting
Work with Tribes Provide presentations on correct medication habits
MTM should not prevent PHS pharmacists from continually leading with new and innovative patient care practices
APhA/NACDS Foundation: Medication Therapy Management in Community Pharmacy Practice: Core Elements of an MTM Service Model. Version 2.0. March 2008.
Lee MP, Giberson S. Implementation of the Indian Health Service National Clinical Pharmacy Specialists (NCPS) Program. Available at www.usphs.gov/corpslinks/pharmacy/clinpharm/doc/ncps.ppt. Accesses May 16th, 2012.
2011 Medicare Part D Medication Therapy Management (MTM) Programs. Fact Sheet. Available at https://www.cms.gov/PrescriptionDrugCovContra/Downloads/MTMFactSheet2011063011Final.pdf. Accessed on May 16th, 2012.
Giberson S, Yoder S, Lee MP. Improving Patient and Health System Outcomes through Advanced Pharmacy Practice. A Report to the U.S. Surgeon General. Office of the Chief Pharmacist. U.S. Public Health Service. Dec 2011.
Schupbach R. Insights from the bizarre perspective and mind of Ryan Schupbach. Presented at the Oklahoma Area IHS Pharmacy Chief’s Meeting, February 17th, 2012.
LT Scott [email protected] River Service Unit12033 Agency Road Parker, AZ 85344928.669.3330