Embed Size (px)
Citation preview

PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

EEG Biofeedback Case Studies Using Live Z-ScoreTraining and a Normative Database
Thomas F. Collura, PhDJoseph Guan, MM.ED, PhD
Jeffrey Tarrant, PhDJohn Bailey, PhDFred Starr, MD
ABSTRACT. This article summarizes clinical results using a neurofeedback approach that hasbeen developed over the last several years and is seeing increasing clinical use. All participantsused a form of live Z-score training (LZT) that produces sound and video feedback, based on acomputation using a normative database to produce multiple targets. The client receives simplefeedback that reflects a complex set of relationships between amplitude and connectivitymetrics. Changes in the EEG are readily seen that conform to the reinforcement parametersbeing used in relation to the live Z-scores. In addition, over multiple sessions, QEEG dataare seen to change significantly, generally on a path toward overall remediation. In thisseries of case studies LZT is seen to effectively address EEG abnormalities in a structuredfashion and to facilitate normalization of the EEG. In individual cases, specific changes areobserved, related to the initial conditions, and the brain’s ability to respond with appropriatechanges. Overall, LZT is found to be a relatively efficient form of neurofeedback that can bedemonstrated to be effective in a variety of clinical scenarios.
KEYWORDS. Biofeedback, live Z-score training, multivariate proportional training, neuro-feedback, normative database, QEEG
INTRODUCTION
This article discusses the technical back-ground, and initial clinical results obtained,in an implementation of live Z-score based
training (LZT) in an EEG biofeedbacksystem. This approach makes it possible tocompute, view, and process normative Z-scores in real time as a fundamental elementof EEG biofeedback. Although employing
Thomas F. Collura is affiliated with BrainMaster Technologies, Inc., Bedford, OH.Joseph Guan is affiliated with the Brain Enhancement Center, Singapore.Jeffrey Tarrant is affiliated with the Columbia Neurofeedback Center, Columbia, MO.John Bailey is affiliated with Allina Medical Clinic, Northfield, MN.Fred Starr is in practice in Nashville, TN.Address correspondence to: Thomas F. Collura, PhD, BrainMaster Technologies, Inc., 195 Willis Street,
Suite #3, Bedford, OH 44146 (E-mail: [email protected]).Dr. Collura has a financial interest in BrainMaster Technologies, Inc. Certain of the methods described here
are patent pending in the United States, Canada, and Europe. We acknowledge the following for their contribu-tions to the case studies in this article: Doerte Klein, PhD; Penijean Rutter, MA; Nancy Wigton, MA; HarryKerasidis, MD; Charles R. Stark, MD; and Jonathan Walker, MD.
Journal of Neurotherapy, 14:22–46, 2010Copyright # Taylor & Francis Group, LLCISSN: 1087-4208 print=1530-017X onlineDOI: 10.1080/10874200903543963
22
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010
the same type of database as conventionalQEEGpostprocessing software, LZT softwareis configured to produce results in real time,suiting it to live assessment and training,rather than solely for analysis and review.
The Z-scores described here are based ona published database and computed usingthe same software code that exists in theanalysis software, when used in ‘‘dynamicJTFA’’ (joint time-frequency analysis) mode.The database includes more than 600 people,ages 2 to 82. The system computes real-timeZ-scores using joint time-frequency analysisrather than using the Fast Fourier Trans-form, which is more commonly used forobtaining postprocessed results. As a result,Z-scores are available instantaneously, with-out windowing delays, and can be used toprovide real-time information.
Initial LZT implementations have used asingle Z-score, or a small number ofZ-scores, for example, ‘‘all coherences,’’ todevelop the feedback. In our work, we havecome to use generally all available Z-scoresin the training, providing an effective bound-ary around the EEG activity, within whichthe trainee learns to put their EEG.
All of the cases described here use a spe-cific form of Z-score training that hasevolved over several years (Collura, 2008a,2008b, 2009; Collura, Thatcher, Smith,Lambos, & Stark, 2009). Using this method,up to 248 simultaneous Z-scores are trainedat once, using a single metric that reflectsthe instantaneous state of all of the Z-scores.The method makes it possible to target parti-cular Z-scores for normalization, whileavoiding overtraining ‘‘outliers’’ and whilealso giving the brain sufficient freedom tochoose a path of self-regulation that is notlimited to ‘‘training to the norm.’’
METHODS
The concept of using Z-scores to providebiofeedback in real time was proposedby Thatcher (1998, 1999, 2004). Colluraand Thatcher (2006) discussed details andimplications of a practical design approach.The first reported implementation with clini-cal results were reported by DuRousseau
(2007), Smith (2008), Stark (2008), Wigton(2008), and Collura et al. (2009). Thesereports included six case studies with docu-mented QEEG and clinical benefits, andemployed the Lifespan Database reportedby Thatcher (1998) as a means of computingZ-scores in real time. Based on these scores,feedback variables were computed andreflected to the user in the form of soundsand graphic feedback of the type normallyused for conventional neurofeedback. Sincethese reports were published, a number ofclinicians have adopted the use of four chan-nels of what we now call LZT in their prac-tices. This article compiles a set of casestudies that were submitted upon request, asa means for disseminating clinical findings,as well as psychometric and QEEG data thatare available. All of the cases in this articleused the same approach to LZT training,which is described in more detail next. Thisarticle also discusses possible relationshipsbetween the specific training algorithms used,and the EEG changes that were observed.
Figure 1 shows the Live Z-score Text dis-play panel that is used by the practitioner.All 248 Z-scores are displayed for the four-channel montage. The display updatescontinually, and the color of the text indi-cates whether the Z-score is currently withinor outside of the standard boundaries of1.0, 1.5, and 2.0 standard deviations. Clini-cians learn to watch this screen, to quicklyidentify deviant scores, and to watch for pat-terns in time and space, as the brain adjusts tothe training parameters being presented. Thecolor coding rules for this text display are notadjustable and do not depend on the trainingcriteria. They are therefore a consistent rep-resentation of the client’s brain state; changesin this screen reflect objective changes in theEEG, and this screen can be relied upon togive a dependable ‘‘reading’’ of the client’sbrain. The screen becomes, in a sense, anavigational panel that guides the assessmentand treatment in real time. This approachcompresses the usual hours, days, or weeksrequired to get a quantitative EEG assess-ment into a fraction of a second and performsthe assessment continually. The differencebetween watching live Z-scores and readinga conventional QEEG report is similar to
Clinical Corner 23
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

the difference between watching a baseballgame or a golf match compared with readingthe statistics after the fact. They both give avaluable indication of the condition and stateof the subject, but the live representation allowsthe practitioner to understand how the num-bers got to be what they are, in terms that aredynamic and neurophysiologicallymeaningful.
While observing the LZT Text display,clinicians set up reward training by specifyingthree key parameters: the upper and lower
bounds of the Z-score ‘‘target window’’ andthe percentage of Z-scores that must bewithin these bounds to achieve a reward.The use of the percentage of Z-scores is anonobvious yet critical step and has pro-found impact on the training. Its value hasbeen found through repeated clinical treat-ment sessions and by observing the LZT Textdisplay during the training process.
Figure 2 shows two additional panels ofthe training screen. The upper area shows
FIGURE 2. Live Z-score display panels used to control feedback.
FIGURE 1. Live Z-score text display (four channels! 248 Z-scores). Note. Z-scores are colored to show whenthey are above normal range (yellow, orange, red) or below normal range (green, turquoise, blue).
24 JOURNAL OF NEUROTHERAPY
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

the current value of the ‘‘PercentZOK’’value, which is the percentage of Z-scoresmeeting the training criteria at the currentmoment. In addition, the percentage of timethat the trainee meets the conditions, beingthe ‘‘percent reward’’ is also shown. Theupper and lower Z-score targets are thenshown. The lower area shows the progressof the training, as the PercentZOK variableis being monitored and trained. There is athreshold that it must meet, to get a reward,and there is also the percentage of time thatthis is being met, shown in a trend graph.The clinician watches all of these values clo-sely and watches the trend graph throughouttraining. This gives the clinician controlof the variables that determine how thefeedback is produced.
This method employs a Z-score ‘‘target’’that is expressed in standard deviations (e.g.,"1.5 to 2.0 SDs) and produces rewards whena specified percentage of all Z-scores meet thecriterion. It does not require all Z-scores tobe within the target window. The percentageof Z-scores achieved thus becomes a
‘‘proportional’’ feedback variable, ratherthan a simple ‘‘on=off’’ feedback signal.
One might consider widening the targetwindow to accommodate all Z-scores.However, this was observed in early studiesto provide the brain with too much freedomin which to operate. For example, usinga wide-enough window to accommodatehighly deviant amplitudes would allow otherparameters to move from a normal to anabnormal range, while the EEG continuedto meet the overall training condition. Thismotivated the approach that allows someZ-scores to remain outside the target rangeyet effectively be ignored.
Figure 3 shows the important relationshipbetween target size and percentage of Z-scores required, in various training scenarios.This concept was not obvious when workbegan, and it is not necessarily obvious toother developers of real-time Z-score systems.Naively, one might think that by allowing asubset of Z-scores to provide the feedback,it is no different than simply ignoring someset of scores, or setting an upper range where
FIGURE 3. Relationship between size of LZT targets, and the use of ‘‘Percent ZOK’’ to establish reward cri-teria. Note.Within this model, clinicians can choose which aspects of training to emphasize, and which to vary.
Clinical Corner 25
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010
Z-scores are allowed to go. But neither ofthese methods produces the same effect.When one overtly ignores Z-scores, then thepractitioner has decided what is importantand what is not. If an upper band of Z-scoresis rewarded, this would produce a ‘‘vortex,’’or attractor, that would pull certain scoresinto the abnormal range.
By specifically allowing a percentage ofany of the Z-scores to be out of the targetrange, the brain is allowed to decide how itmeets the strategy of normalization. Extremeoutliers are effectively ignored, but whichscores they are may change from momentto moment. Finally, by selecting the targetsize and position, it is possible to ‘‘comb’’through the tangle of Z-scores, and give thebrain information relating to a certainboundary of its function, and allow it tolearn from different regions of its function.
Different practitioners give differentemphasis to the use of this range of rewardstrategies. One clinician (NW) emphasizesworking at the low end of the reward range,using 25% to 40% feedback rates. Otherpractitioners work at higher levels of reward,
up to and above 90% reward. Generally, it isfound that adjusting these values during thesession is valuable, and provides importantflexibility to the training.
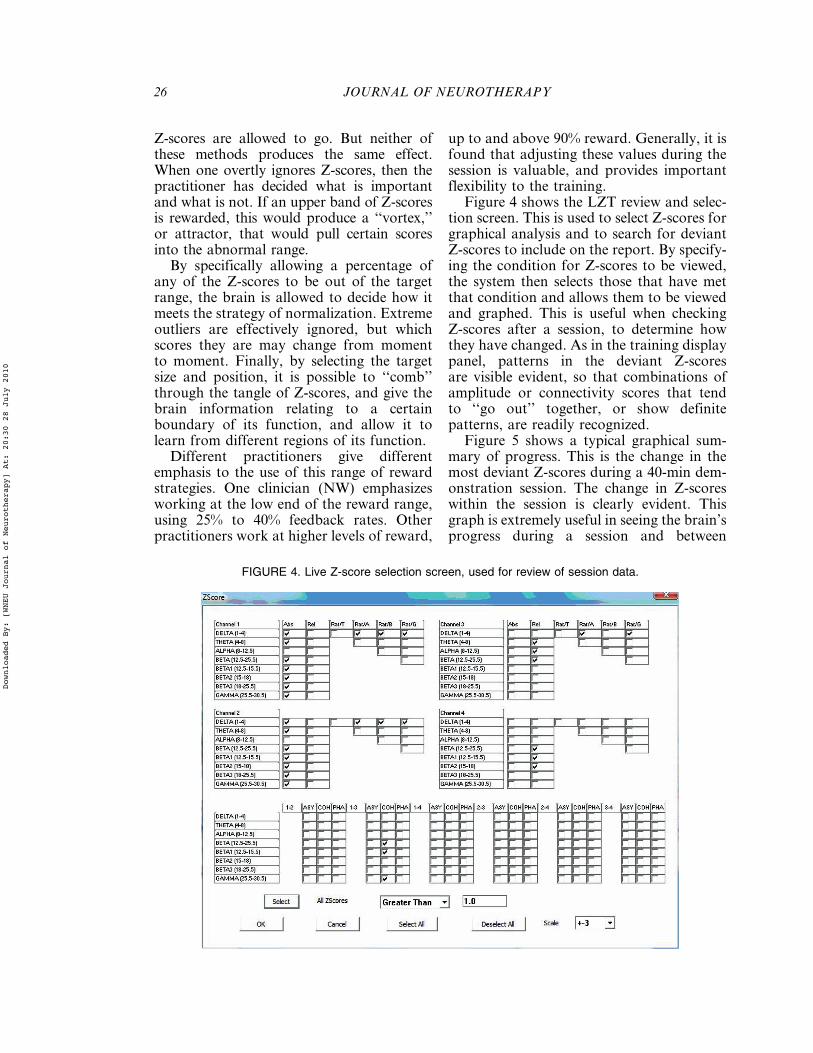
Figure 4 shows the LZT review and selec-tion screen. This is used to select Z-scores forgraphical analysis and to search for deviantZ-scores to include on the report. By specify-ing the condition for Z-scores to be viewed,the system then selects those that have metthat condition and allows them to be viewedand graphed. This is useful when checkingZ-scores after a session, to determine howthey have changed. As in the training displaypanel, patterns in the deviant Z-scoresare visible evident, so that combinations ofamplitude or connectivity scores that tendto ‘‘go out’’ together, or show definitepatterns, are readily recognized.
Figure 5 shows a typical graphical sum-mary of progress. This is the change in themost deviant Z-scores during a 40-min dem-onstration session. The change in Z-scoreswithin the session is clearly evident. Thisgraph is extremely useful in seeing the brain’sprogress during a session and between
FIGURE 4. Live Z-score selection screen, used for review of session data.
26 JOURNAL OF NEUROTHERAPY
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010
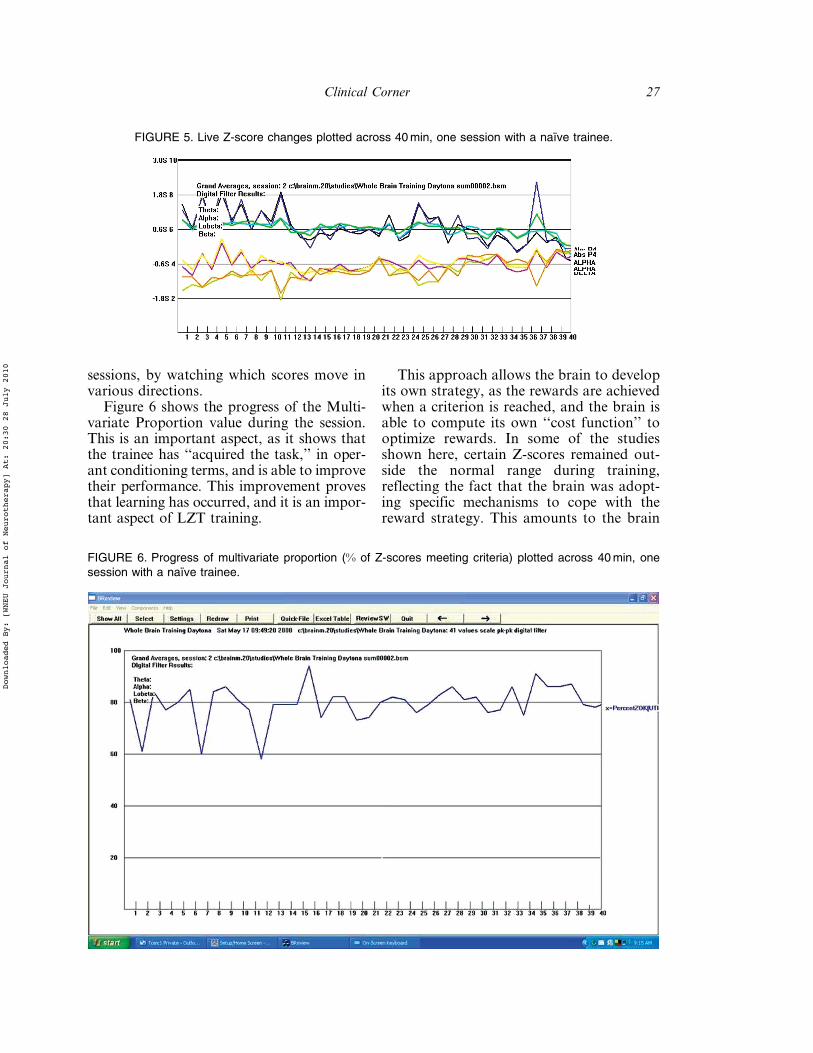
sessions, by watching which scores move invarious directions.
Figure 6 shows the progress of the Multi-variate Proportion value during the session.This is an important aspect, as it shows thatthe trainee has ‘‘acquired the task,’’ in oper-ant conditioning terms, and is able to improvetheir performance. This improvement provesthat learning has occurred, and it is an impor-tant aspect of LZT training.
This approach allows the brain to developits own strategy, as the rewards are achievedwhen a criterion is reached, and the brain isable to compute its own ‘‘cost function’’ tooptimize rewards. In some of the studiesshown here, certain Z-scores remained out-side the normal range during training,reflecting the fact that the brain was adopt-ing specific mechanisms to cope with thereward strategy. This amounts to the brain
FIGURE 5. Live Z-score changes plotted across 40min, one session with a naı̈ve trainee.
FIGURE 6. Progress of multivariate proportion (% of Z-scores meeting criteria) plotted across 40min, onesession with a naı̈ve trainee.
Clinical Corner 27
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

discovering dynamics that allow it to reducethe overall index of abnormality whileallowing certain features to remain outsidenormal, and to function as coping or com-pensatory mechanisms. This is significant,as it avoids the pitfall of ‘‘training to an out-lier’’ that may result when all Z-scores arerequired to meet the training targets.
RESULTS
Practitioners who adopted the LZTapproach and had been instructed on itsuse were invited to submit case studies thatillustrated their experience with the tech-nique. Not all cases were submitted, so thisarticle presents selected successful cases thatwere submitted. The details for each case,as well as clinical, behavioral, psychometric,and QEEG changes, when available, aresummarized in Table 2.
Application of Training Protocol
All of the reported cases used a form ofwhat we refer to as ‘‘multivariate compositetargeting,’’ in which a number of Z-score tar-gets are continually assessed in a particularway, and used to produce the feedback. Allof the reported cases used this capability inthe form of the ‘‘Percent ZOK’’ algorithm inLZT. In all cases, there were individual differ-ences in the precise strategy and control meth-odology used. The protocol provides sufficient
freedom for the clinician to determine the nat-ure and extent of information presented to thebrain, relative to the current state of the mul-tiple Z-scores. This is to be distinguished tomore simple ‘‘training to the mean’’ that maybe assumed to be used, if one is not knowledge-able of the relevant details.
Various practitioners differ in their preciseuse of the controls and options within theLZT paradigm. Although all practitionersmake use of target size and percentageof Z-scores as control variables, the exactprocess used varies. Some practitionersemphasize adjusting target size and allowingthe brain to learn the various levels of taskdifficulty, whereas others focus on the per-centage of Z-scores as the key variable. How-ever, as the values are interrelated, there isalways a dynamic interplay in changing one,the other, or both. The LZT approach allowsthe practitioner to emphasize different aspectsof the Z-score training, based on the observedclinical and electrophysiological changes.
Summary of Cases
Details for all cases are presented in thesecond table. This section summarizes specificresults including Z-score statistics, QEEGmaps, and relevant psychometric results,which illustrate the clinical and electrophysio-logical changes which were observed.
Three cases (‘‘S,’’ ‘‘C,’’ and ‘‘Z’’) were pre-sented by one clinician (JG), who uniformly
FIGURE 7. Percentage of amplitude Z-scores outside #1.0 SDs for 3 participants ‘‘S,’’ ‘‘Z,’’ and ‘‘C,’’ 10sessions each.
28 JOURNAL OF NEUROTHERAPY
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

used 10 sessions of four-channel LZTtraining on each of three patients. Figure 7summarizes the percentage of amplitudeZ-scores (absolute power, relative power,power ratios) that were outside the nominalrange of #1.0 SDs. This illustrates therepeatable reduction in deviant Z-scoreswhile revealing some difference betweenparticipants. It is interesting that the parti-cipants who presented with the most deviantZ-scores on the outset showed the leastnumber of deviant scores after training.
Figure 8 shows the percentage of connec-tivity Z-scores (coherence, phase, asymmetry)outside the range #1.0 SDs for the samethree participants. Although uniformreduction is seen in two participants, anactual increase is seen in one. It is shownlater that this reflects a compensatory mech-anism, in which the brain evidently allowssome scores to become deviant, to achievegreater overall normalization. Note that thisphenomenon likely depends on the abilityof the training software to allow some scores
FIGURE 8. Percentage of connectivity Z-scores (asymmetry, coherence, and phase) outside #1.0 SDs, 3participants, 10 sessions each.
FIGURE 9. Number of amplitude Z-scores outside target range as a function of target size, participant ‘‘S.’’Note. The number of Z-scores outside the narrow range 1.0 actually rises, whereas the overall distributionpulls strongly within the 1.5 and 2.0 ranges.
Clinical Corner 29
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

FIGURE 10. Number of connectivity Z-scores outside target range as a function of target size, participant ‘‘S.’’Note. Although many scores begin outside the 2.0 and 2.5 SD ranges, all Z-scores fall within the range 1.5 SDafter 10 sessions.
FIGURE 11. Pre- and posttreatment QEEG maps for participant DQ.
30 JOURNAL OF NEUROTHERAPY
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

to remain outside normal bounds whilecontinuing to reward for training.
Figure 9 shows the number of amplitudeZ-scores outside specified target ranges, forone participant.Note that, at the outset, a greatmany scores are outside even the larger targetsof 2.5, 3.0, and larger targets.After training, thenumber of scores outside of the larger rangeshas reduced dramatically. At the same time,the number of scores outside the range #1.0has increased, as a result of ‘‘packing’’ of thescores into the narrower ranges. This reflectsthe ability of the brain to achieve overall nor-malization while having room to move at thelower limits of the training targets.
Figure 10 shows the number of connectiv-ity (coherence, phase, asymmetry) Z-scoresoutside of specified target sizes. Thereduction of scores outside the range #1.5is essentially complete, as no Z-scores arefound outside this range after the training.This demonstrates the brain’s ability to pro-cess dozens of Z-scores in a single trainingparadigm, and effectively normalize all ofthem, while performing a simple training.
Figure 11 shows pre- and post-QEEGmaps for participant ‘‘DQ’’ presented byclinician JT. Improvements are visible inboth the power and the coherence maps,after 39 sessions.
FIGURE 12. Pre- and posttreatment maps (26 sessions) for participant TB. Note. Top pair: Absolute powermaps, Bottom pair: Coherence maps.
Clinical Corner 31
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

Figure 12 shows pre- and post-QEEGmaps from participant ‘‘TB’’ (clinician JT).The normalization of power as well ascoherence maps is visibly evident after 26sessions. It is interesting to note examplesof ‘‘overshoot’’ in which one value movesout of normal range, whereas others normal-ize. For example, a slight excess of right deltaand theta appears, whereas the excess of highbeta and alpha normalizes. Also, there is aslight alpha hypocoherence that appears,along with the significant normalization ofother coherences.
Figure 13 shows pre- and post-QEEGmaps, and Figure 14 shows post-QEEG
maps after 20 sessions, for participant‘‘Norb’’ (clinician F8) using a Laplacianderivation. All evident power and asym-metry abnormalities are seen to effectivelynormalize. Although the pre maps show sig-nificant delta and theta excess, and a deficitof high frequencies, the post maps are essen-tially normal, with only a very slight betaexcess on the left, which may be musclerelated.
Figure 14 shows IVA$Plus StandardScales Analysis for ‘‘Norb.’’ The Full ScaleResponse Control Quotient rises from 94 to101, whereas the Full Scale AttentionQuotient rises from 62 to 95.
FIGURE 13. Pre- (left) and posttreatment (right) QEEG maps after 20 sessions, patient Norb.
FIGURE 14. Pre- and posttreatment IVA$Plus, patient Norb, 20 sessions.
32 JOURNAL OF NEUROTHERAPY
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

Figure 15 shows pre- and post-QEEGmaps for participant ‘‘44YOM’’ (clinicianNW), after 25 sessions. Visible trendsinclude a reduction in coherence and phaseabnormalities, and some improvement inrelative power.
Figure 16 shows IVA$Plus results fromparticipant ‘‘44YOM.’’ Full-Scale ResponseControl Quotient rises from 29 to 94,whereas Full Scale Attention Quotient risesfrom 0 to 96.
Figure 17 shows the progression ofparticipant ‘‘12YOM,’’ clinician PR, with eyesopen, after 20 and after 40 sessions. This pro-gression shows definite compensatorymechanisms at work, as the post-20 sessionmaps show interesting adaptations to thetraining. In absolute power, areas that weredeficient in delta are normalized in 20sessions, whereas surrounding areas exhibit adelta excess. This suggests a global reregula-tion mechanism wherein surrounding areasadjust their function, as a compensation forthe normalization of other areas. Similarly,whereas hypocoherence across frequency
bands is seen to remediate, there is a signifi-cant hypercoherence in high beta thatemerges, again likely as a compensating mech-anism. The final condition characterized byoverall normalization in the presence of hyper-coherent beta, suggests amechanism involvingcortico-cortical binding, as a strategy towardproducing the requisite overall normalization.
Figure 18 shows the progression ofeyes-closed QEEG maps for the same clientas Figure 17. A rather different pattern ofnormalization is evident, suggesting that thebrain adopts a different strategy to keepingitself normalized, depending on whether theeyes are open or closed. In this case, the finalQEEG shows essential normalization, alongwith a phase deficit (phase-locking) in alphaacross the head. This suggests a stronger-than-normal thalamocortical binding, inwhich thalamic activity is controlling corticalrhythms with excessively tight timing. Inother words, rather than having several some-what independent alpha generating processes(e.g., occipital, frontal, temporal), the brain isdominated by a single alpha pacemaker.
FIGURE 15. Pre- (left) and posttreatment (right) QEEG maps, 25 sessions, patient 44YOM.
Clinical Corner 33
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

Figure 19 summarizes the progress ofparticipant ‘‘12YOM.’’ In our analysis anddiscussions with clinicians, observed changes
in Z-scores may indicate compensatingmechanisms in which areas surrounding theoriginal delta excess change their state, as a
FIGURE 16. Pre- (left) and posttreatment (right) IVA Standard Scales Analysis, 25 sessions, subject 44YOM.
FIGURE 17. Overview of client 12YOM progress in Eyes Open condition, after 20 and 40 sessions.
34 JOURNAL OF NEUROTHERAPY
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

way of containing the abnormal areas. Whenthere is a worsening of an EEG deviation, wehypothesize that it may represent a com-pensatory mechanism. For example, whenthere is an area with a deficit of deltaactivity, surrounding areas may exhibitexcess delta during the normalization pro-cess, even as the previously abnormal areasnow become normal. Temporarily, thesechanges look like a cap or a wrapper aroundthe areas which in fact are normalized in the20-session maps. So the brain has adopted astrategy to lower its mean scores, by allowing
the surrounding areas to provide acontaining medium for the abnormalactivity, as the brain globally produceshigher delta amplitudes. The global natureof the delta is indicated by the newlyemerged hypercoherence after 20 sessions.
After 40 sessions, when most all amplitudeand connectivity measures are normalized, weare still left with very specific EEG abnor-malities that again seem to be coping or com-pensating mechanisms. As an example, thisclient had extreme phase synchrony in alphawith eyes closed and extreme beta coherence
FIGURE 18. Overview of client 12YOM progress in Eyes Closed condition, after 20 and 40 sessions.
FIGURE 19. Summary of changes EC and EO.
Clinical Corner 35
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010
with eyes open. We believe that thebrain may be setting up its own bindingmechanisms, again, to maximize the globalnormality. In this case, where the remainedphase synchrony and coherence abnormali-ties, it was nonetheless noted that the clientexperienced significant clinical benefits uni-formly from treatment. To quote the clin-ician,
Changes in delta absolute power andcoherence over the course of the train-ing indicate some interesting possibili-ties for future research. There may bea mid-training phase that prioritizesallocation of cortical resources for thepurpose of reorganizing neural connec-tivity. Hypercoherence could be a mani-festation of increased thalamocorticalactivity which necessitates a temporarydiversion of energetic resources toimprove the efficiency of the interactivepathways between the thalamus and thecortex. (Rutter, 2009)
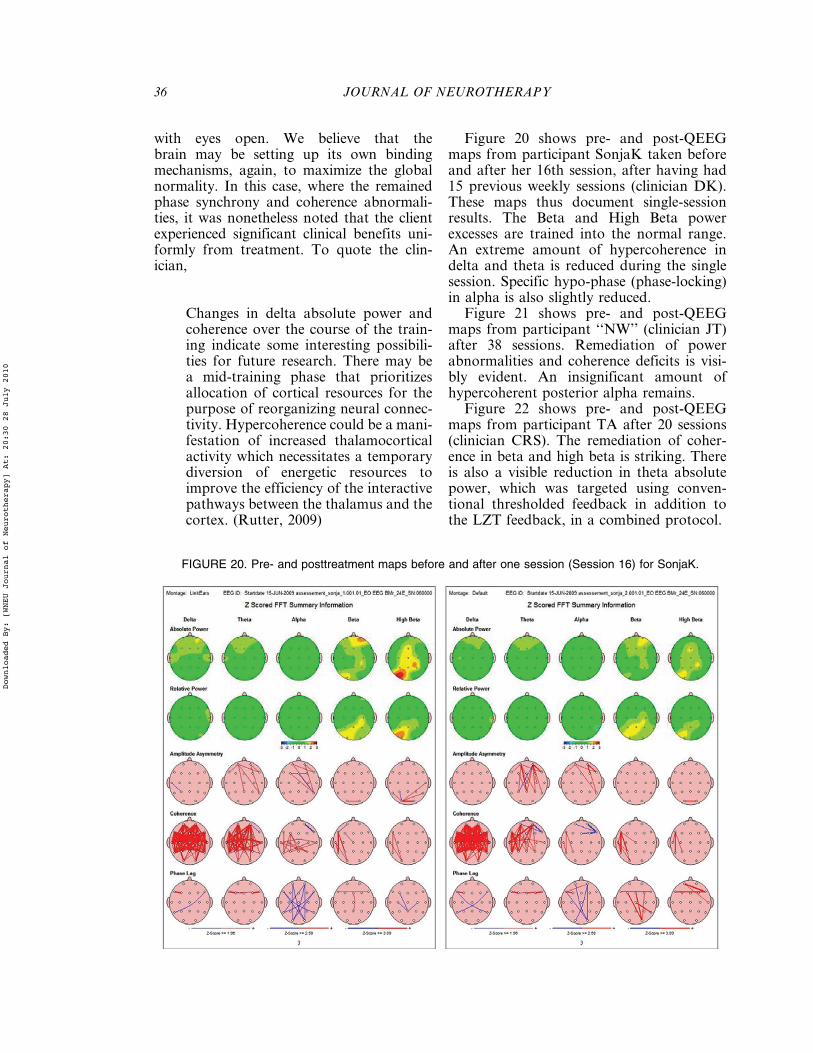
Figure 20 shows pre- and post-QEEGmaps from participant SonjaK taken beforeand after her 16th session, after having had15 previous weekly sessions (clinician DK).These maps thus document single-sessionresults. The Beta and High Beta powerexcesses are trained into the normal range.An extreme amount of hypercoherence indelta and theta is reduced during the singlesession. Specific hypo-phase (phase-locking)in alpha is also slightly reduced.
Figure 21 shows pre- and post-QEEGmaps from participant ‘‘NW’’ (clinician JT)after 38 sessions. Remediation of powerabnormalities and coherence deficits is visi-bly evident. An insignificant amount ofhypercoherent posterior alpha remains.
Figure 22 shows pre- and post-QEEGmaps from participant TA after 20 sessions(clinician CRS). The remediation of coher-ence in beta and high beta is striking. Thereis also a visible reduction in theta absolutepower, which was targeted using conven-tional thresholded feedback in addition tothe LZT feedback, in a combined protocol.
FIGURE 20. Pre- and posttreatment maps before and after one session (Session 16) for SonjaK.
36 JOURNAL OF NEUROTHERAPY
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

Commonalities in Clinical Results
The overall numbers of studies with out-come reporting, and the numbers showingimprovement, are summarized in Table 1.Detailed specific observations are summar-ized in Table 2.
Of the 19 cases reporting presentingsymptoms, they were 7 Cognitive and Affect-ive Problems, 5 ADD=ADHD, 3 AutisticDisorder or ASD, 2 Behavioral Problems, 1Cerebral Palsy, and 1 TraumaticHead Injury.
All respondents reporting clinical out-come identified clinical improvement duringthe treatment sessions, as noted in Table 2.
QEEG Results
When QEEG data are available, allrespondents show visible improvement in
QEEG maps relative to the normative data-base used for analysis. In most cases, theNeuroGuide ANI (‘‘Lifespan’’) databasewas included in the analysis. In some cases,the QEEG normalization is dramatic, result-ing in essentially normal QEEG maps afterthe training. In other cases, we see eitherremaining abnormalities or newly emergentdeviations that may reflect compensatingmechanisms. The availability of pre- andpost-QEEG maps is found to be of consider-able value in monitoring and assessing theprogress of LZT training. Whereas LZTtraining can be viewed as an automatic guid-ance mechanism for feedback, EEG andQEEG analyses provide important infor-mation guiding the placement of sensors,choice of protocols, and management ofanticipated and observed clinical and beha-vioral changes. In some of the cases, indicessuch as the NeuroGuide Traumatic Brain
FIGURE 21. Pre- and posttreatment QEEG maps for participant NW, 38 sessions. Note. Top pair: AbsolutePower maps, Bottom pair: Coherence Maps.
Clinical Corner 37
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

Index or Predicted IQ are reported, andshow improvements.
Abreactions/Negative Side Effects
In this clinical series, no abreactions to theLZT training were noted. In earlier clinicalwork, one initial mechanism identified forabreaction occurred when the target windowrequired for Z-scores was excessively wide(e.g., #.3.0 SDs). In one case (not reported
here), an individual presenting with excessiveEEG absolute power was trained with a widewindow. The result included an ‘‘overshoot,’’in which excessively high power Z-scores werefound to become excessively low, in effectfinding another limit at which to function. Itbecame necessary, through the software, toprovide separate upper and lower limitvalues, so that the Z-scores could be trainedwith an upper limit of 3.0 standard deviationsbut a lower limit of "1.0 standard deviations.Training with this modification eliminated
FIGURE 22. Pre- (left) and post- (right) QEEG maps, 20 sessions, participant TA.
TABLE 1. Overall studies with outcome reporting and the numbers showing improvement.
No. Reported Visible Improvement
Total cases reported 24Reporting presenting symptoms 22 22Reporting clinical=behavioraloutcome
23 23
Pre- and posttreatment LZT data 10 10Pre- and posttreatmentQEEG data
12 12
Pre- and posttreatment IVA data 5 4
Note. LZT! live Z-score training; IVA! Integrated Visual and Auditory Performance Test.
38 JOURNAL OF NEUROTHERAPY
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

TABLE2.Summarize
dca
sedetails,includingclinical,behavioral,psy
chometric,andQEEG
changes.
Study#
CLIN
IDPrese
ntin
gPreviousTreatm
ent
Preassessment
#LZTSessionsandSite
sResu
ltEEG
Change
1JG
Z17YO
male
seve
rely
autistic
w=little
speech
,frequenttantrums,
short
attentio
nsp
an,doesnot
listento
instructions
LZT:highamplitude
generally,co
herence
deficits
10se
ssionsF7F8T5T6
more
clarity
insp
eech
and
longerse
ntence
s,talksmore
appropriately,less
andless
tantrumsandmuch
calm
er,
more
willingto
carryout
instructionsandtriesall
dishesthatthemaid
cooks
Reductionin
aberrant
Z-Sco
res:
1st
session:36
Z-sco
res>1.0
SD
during
session.10th
session:13
Z-sco
res>1.0
SD.
Reductionin
both
amplitudeand
connectivity
Z-Sco
res
2JG
C7YO
female
cerebral
palsy,
speaks
twoto
threewords,
limite
dgross
andfin
emotor
skills(can’twalk
yet’’,
shortattentio
nsp
an,
dreamy
Othmerwideinhibitsite
specific
6mo.Slow
but
steadyprogress
LZT:highamplitude
generally,co
herence
deficits
10se
ssionsF7F8T5T6
more
resp
onsive
tothe
environment,sp
eakingmore
with
longerse
ntence
s,reciproca
tetwo-w
ay
communicatio
n,interacts
more
with
otherch
ildrenin
school,demonstratesmore
strength
inhermove
ments
Reductionin
aberrant
Z-Sco
res:
1st
session:35
Z-sco
res>1.0
SD
during
session.10th
session:27
Z-sco
res>1.0
SD.
Reductionprimarily
inamplitudeZ-Sco
res
3JG
Shaan
52YO
female
with
occasionalmemory
lapse
s,difficulty
inrememberingnew
learning
LZT:highamplitude
generally,co
herence
deficits
10se
ssionsF7F8T5T6
able
toremembermost
ofthe
stepsoftheChinese
classicaldancingandis
able
toabso
rbmore
ofhear
learningoftheKorean
language.Now
whensh
etake
sco
ffeesh
edoesnot
have
aheadach
eanym
ore
Reductionin
aberrant
Z-Sco
res:
1st
session:60
Z-sco
res>1.0
SD
during
session.10th
session:31
Z-sco
res>1.0
SD.
Reductionin
both
amplitudeand
connectivity
4JT
DQ
9YO
male,behavioral
problemsatschooland
home,incidents
of
verbalandphysical
aggression,inability
toco
ntroltemper,
stuttering
place
don1=2
day
attendance
,individual
behavioralplan,
vestibularand
proprioce
ptivetraining
QEEG
map:significa
nt
lack
ofalphaactivity,
significa
ntexcess
of
delta
activity
frontally,
mixedhyp
er-
and
hyp
o-coherence
39se
ssionsF3F4P3P4,
FzPzC3C4,F3F4Cz
PzT3T4FzCzF3F4
P3P4alphaenhance
addedwith
emphasison
parietalviathresh
olds
speech
improve
dsignifica
ntly
after15se
ssions,
much
less
stutteringataroundse
ssion
17,less
argumentativeand
stoppedtempertantrums
afterse
ssion22,hadstopped
takingmedicatio
nsatse
ssion
26,se
emedhappierand
friendlieratse
ssion27.
improve
denergyandaffect,
more
cognitive
flexibility,able
tohandle
transitio
nsin
sessionandin
office,no
longerstutteredafter39
sessions.
planto
return
tofull
dayattendance
BASCbehaviorassessment
system
resu
ltssh
ow
improve
ment14of28
scoresim
prove
d2or
more
standard
deviatio
ns,
pre-andpost-Z-Sco
res
show
changes
significa
ntly
inhighbeta
frontally,andin
reductionsin
hyp
ercoherence
s
5JT
TB
11
YO
male,
refusa
lto
complete
schoolwork,
easily
distracted,
unorganizedwork
area,
IVA
shows
diagnosis
of
ADHD,CombinedTyp
e.
QEEG
map:significa
nt
excess
ofhighbeta
activity
focu
sedin
parietalregions,
26se
ssionsT3P3Fp2P4
thenFp1Fp2FzCz
manydeviatio
nsvisibly
cleared
upmidwayse
ssionsasearly
asse
ssion2.After7th
session,‘‘hasbeenve
ry
individualizedbehavior
questionnaireprovidedto
motherandch
ecklists
scoredandave
ragedas
(Con
tinu
ed)
39
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010
TABLE2
(contin
ued)
Study#
CLIN
IDPrese
ntin
gPreviousTreatm
ent
Preassessment
#LZTSessionsandSite
sResu
ltEEG
Change
flataffect,‘‘head
twitching’’,
avo
idance
of
physicalactivities,
physicalawkw
ardness
=clumsiness,andso
cial
immaturity
significa
nt
hyp
ercoherence
inall
bands,
esp
ecially
beta
andhighbeta
cooperativein
schoolthis
week’’,‘‘tryingnew
thingsat
swim
lessons’’,‘‘only
notice
ticsoccasionally,after
session13,‘‘finally
rodea
bike!"
pre-andpost-treatm
ent
scores.
IVA
perform
ance
testsim
prove
d,3of6
scoresim
prove
dmore
than2standard
deviatio
ns
6FS
Norb
21YO
female,cu
rrently
on
aca
demic
leave
from
college‘‘requiredto
get
mentalhealth
treatm
ent
togoback
toschool’’
difficulty
makingfriends,
socializing,moderate
sxofdepression.
Engrossedin
inner
‘‘fantasy
life"
diagnose
dwith
ADHD,
place
donstim
ulant.Not
currently
taking
prescribedmedicatio
n(adderall).Currently
takingce
lexa
20mg.
Previouslytookproza
k20mg
QEEG
map:excess
delta
andtheta
left
centrotemporal,
anorexia,bingepurging
type,remission.ADD
by
report.MDE:moderate,
partialremission,mTBI
byreport.SocialPhobia
from
mother:Idose
eim
prove
mentin
B.Seemsto
befollowingthroughbetter
andco
mpletin
gtasks.
Has
discu
ssedwith
methe
reco
mmendatio
nsaboutpast
rigity.Agreethatsh
eneeds
tolearn
toalte
rherplansand
stillaccomplishtasks.
She
hasco
mealongwayandI
seeagreatdealof
improve
ment.organizatio
nis
betterandco
nfid
ence
isup.
QEEG
mapsh
ows
significa
ntnorm
alizatio
n,
amplitudesnow
norm
al.
TBIdiscrim
inantreduce
dfrom
porobability
of97.5%
to70.0%.IVAplusscores
pre-andpost
show
improve
mentin
attentio
nsu
bscales
7FS
bers1
54YO
CF
(anesthesiologist),
diagnose
dwith
ADD,
inattentivetype,
GeneralizedAnxiety
Disorder,Recu
rrent
MajorDepression.
Complaints
relatedto
inattentio
n,fatig
ue,
worry,
and‘‘feelingblue"
Methylphenidate
96mg
daily,Lexa
pro
20mg
daily.Disco
ntin
uedand
wash
edoutpriorto
QEEG.
IVA$PlusQ
Sco
res;
QEEG
EC
andEO
showeddecrease
dpowerat1Hz,
frontal
low
powerF3andF4.
low
power9–10Hzin
all
leads.
Increase
dpower
ove
rT4,T6from
13–15Hzand24–30Hz,
maximaldeviatio
nat
28Hz.
20
sessions
conve
ntio
nal
training,monopolarto
reduce
fruntaltheta,10
sessionsalpha
asymmetrytraining.20
LZTse
ssionsEO
Fz=
T3=T
4=P
zusingDVD
playe
r
IVA$Plus
QSco
res
show
improve
mentof10%
to20%
inGlobalResp
onse
Control,
GlobalAttentio
n,and
Audito
ryResp
onse
Control
andAttentio
nSubscales.
Hyp
eractivity
indexincrease
dfrom
95to
109.Im
prove
ment
inove
rallattentio
n,
occupatio
nalfunctioning,
increase
dproductivity,better
organizatio
n,greaterjob
satisfaction.decrease
inBeck
Depressionfrom
25at
base
lineto
14atpost
LZT.
Changespersistedat3mo.
follow-up.Lowered
Methylphenidate
to70mg,
disco
ntin
uedLexa
pro
QEEG
showsgeneraltrend
toward
norm
alizatio
n,
changesof1.0–2.0
SD
notedove
ralltraining
sites.
Low
Powerat
9–10Hzco
mpletely
norm
alized.
8FS
math1
IVA$PlusQ
Sco
res
IVA$Plus
QSco
res
show
improve
mentof10%
to30%
inGlobalResp
onse
Control,
andAudito
ryResp
onse
Controla
ndVisualP
rudence
.
40
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

(Con
tinu
ed)
Hyp
eractivity
indexincrease
dfrom
69to
86
9FS
pase
1IVA$PlusQ
Sco
res
IVA$PlusQ
Sco
ressh
ow
improve
mentof10%
to20%
inGlobalResp
onse
Control,
GlobalAttentio
n,and
Audito
ryResp
onse
Control
andAttentio
nSubscales.
Hyp
eractivity
index
decrease
dfrom
95to
50
10FS
skeg1
56YO
CF,guidance
counse
lor,difficulties
with
comprehension,
earlymorningwaking
ove
rse
veralye
ars.
Complaints
relatedto
hyp
eractivity,audito
ryproce
ssing,audito
rymemory.
long-actingstim
ulant,
SSRI,and
non-benzo
diaze
ine
sleepaid.Disco
ntin
ued
andwash
edoutpriorto
QEEG.
IVA$PlusQ
Sco
res
consistentwith
proce
ssingprudence
andaudito
ryco
mprehension
problems.
Global
abnorm
alitiesove
rF3,
F4,T3,T4,C3,C4,P3,
P4,O1,O2.Slow
wave
spredominate
ove
rT3
andO2between1–3Hz,
fast
activity
ove
rO2in
15–20Hzrange.Loreta
identifiesBrodman
areas10,30and
anteriorcingulate
abnorm
alities.
9LZTse
ssionseye
sopen,
30–40minutes,
P3=P
4=
O1=O
2usingDVD
and
complextonereward.
$1SDin
delta
atF3,F4,
C3,C4,T3,T4.Also$1
SD
inbeta
andgamma
atT3andT4.Move
toF3=F
4=P
3=P
4andF3=
F4=T
3=T
4to
target
proce
ssingand
attentio
n.
20
LZT
sessions
completed.
IVA$PlusQ
Sco
resmostly
steady,
show
improve
mentof
10%
to20%
inAudito
ryPrudence
,Audito
ryComprehension.
Hyp
eractivity
indexminim
al
changefrom
109to
111.
Subjectivereport
improve
mentin
audito
ryproce
ssing,audito
rymemory,
ove
rallattentio
n.Noted
improve
ments
inoccupatio
nalfunctioning,
increase
dproductivity,better
organizatio
n,greaterjob
satisaction.Sleepim
prove
dmost
ove
rall,
nolonger
requiringsleepmedicatio
n.
Generaltrendtoward
norm
alizatio
nvisible
inQEEG,most
evidentin
low
frequency
range
(1–3Hz)
inleftfrontal,left
temporal,andoccipita
lleadsin
mid
tohigh
frequencies(16–22Hz).
Decrease
inco
herence
notedbetweenP3O1and
P4O2.
11JB
11YOF
11YO
female,depression
andanxiety,irritability,
low
moticatio
n,high
forgetfulness
&disco
ganizedattentio
n,
poorschool
perform
ance
nse
ssions
F3=F
z=P3=P
zF3=F
p1=P
3=P
zF3=F
4=
C3=C
4
could
only
tolerate
DVD
feedback
ofstop=g
o,but
wantedto
train
for40
minutes.
Did
notwantto
stop
NFtraining
able
toreduce
LZT
target
size
from
$="
2.0
SD
to$1.5="
1.2
SD
12JB
10YOM
10YO
male,pervasive
deve
lopmentaldelay
(6weeks
premature,3
weeks
inneonatalunit),
ADHD
symptoms,
inattentio
n,
hyp
eractivity,ca
n’t
handle
transitio
ns;
lack
ofco
operativeness,
problemsin
school;
difficulty
with
sleep
19se
ssionssitesbase
donQEEG,parental
reportofsymptoms&
subjectiveresp
onse
totraining
Improve
mentco
nsistently
noticedin
2days
post
training
andbytheendlastedforthe
fullweekwith
very
noticeable
improve
mentin
postivie
moodandleve
lof
cooperativeness
&noreports
ofproblemsatschoolforth
elast
twomonthsoftraining
parents
tracked
improve
mentonscales
for2–4-6
days
post
training.
(Con
tinu
ed)
41
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

TABLE
2(contin
ued)
Study#
CLIN
IDPrese
ntin
gPreviousTreatm
ent
Preassessment
#LZTSessionsandSite
sResu
ltEEG
Change
13JB
12YOM
12YO
male,depression&
ADHD
with
hairpulling
onleftsideatC3;
complete
shutdownsat
schoolwith
oppositio
nal
refusa
lto
dowork;not
doinganyhomework
medicatio
nhadbeen
ineffective&
wasatrisk
ofbeingse
ntto
aresidentia
lprogram
QEEG
showsfrontal
slowingatF3
1se
ssion
F3=F
4=C
3=C
3;
addedlow
alpha
coherence
reward
sound=v
isualF3F4&
C3=C
4,thenaddedlow
beta
coherence
reward
sound=v
isualforF3=C
3
single
sessionpositive
resp
onse
notedafterse
ssion
haslasted-parents
and
teach
ers
rate
itat75%
improve
ment=noneedfor
residentia
l.
norm
alizedF3
beta1=g
ammabyfirst
norm
alizingthelow
coherence
s;
14JB
14YOM
14YO
male,wantedto
be
offmedicatio
n,wanted
totrain
his
brain,poor
schoolperform
ance
,not
doingch
ores,
rather
irritable
and
argumentative
5se
ssions
F3=F
4=P
3=P
4with
addedreward
for
norm
alizingbeta
coherence
F3=F
4
reports50%
improve
mentin
sleeppattern,in
homework
completio
nandin
doing
choreswith
outparental
promptin
g.Hereports75%
improve
mentin
sports
perform
ance
and75%
improve
mentin
beingless
irritable,andproneto
anger
oroppositio
nalin
resp
onse
sto
parents.
15JB
17YOM
17YO
male,Asp
ergers
with
seve
redepression=
Anxiety.
6se
ssionstraditional
neurofeedback
(1–6),10
sessionsOthmer(14–
23)
23se
ssionstotal,LZT
for
sessions7–13
complete
symptom
reliefwith
both
depressionandanxiety
low
andmuch
improve
dschoolperform
ance
and
socialrelatio
ns.
16JB
10YOM2
10YO
male,ADHD;IQ
inthe70s,
distractible,
doesn
’tfin
ishtasks,
poor
memory,im
pulsive,
emotio
naloutbursts,
easily
frustrated,misse
sso
cialcu
es,
problems
with
reading&
comprehension
use
sAVE
andCaptains
Logathome
QEEG:
dim
inished
beta
activity,loca
lizedin
left
parietal&occipita
lareas;
more
pronounce
dEEG
abnorm
alities
undertask
17
sessions
C3=C
4=P
3=
P4C3=F
3=F
z=C4C3=
C4=T
5=F
z$C4SMR
Fp1=F
p2=F
3=F
4C3=
C4=T
5=F
z$bipolar
T3=F
p1&T4=P
4
Reductionin
aberrant
Z-Sco
res
17NW
44YOM
44YO
male,ADHD,
bipolar,occasional
anxiety
symptoms,
rarely
hasmanic
episodes,
multiple
blows
tothehead,rece
ntly
stoppedworking
variouspsych
otropic
medicatio
nssince
2001,
lack
ofadequate
symptom
reso
lutio
nfrom
medicatio
ns
QEEG
maps:
significa
nt
amplitudeand
connectivity
deviatio
ns
IVA:50$behavioral
symptoms=
functioning
issu
es
25se
ssionsF3=C
3=P
z=F4
F3=F
4=P
z=C4P3=P
4=
Cz=PzF3=F
4=C
z=Pz
beginningofsymptom
reso
lutio
natse
ssion5.able
tofunctionadequately
after
medicatio
ntitratio
n.After2
monthsand25se
ssions
clientsu
ccessfully
titratedoff
ofallmedicatio
nsandnew
QEEG
take
n.Reportsbeing
able
toove
rallfunctionbetter
thanbefore
NF,eve
nwith
out
medicatio
n.betterable
tofocu
sandfunctionin
QEEG:EO
mapssh
ow
significa
ntnorm
alizatio
n,
reductionin
amplitude
excesses,
andin
hyp
ercoherence
s;so
me
hyp
oco
herence
remains.
EC
mapssh
ow
significa
nt
norm
alizatio
n,so
me
residualhyp
ercoherence
.After9more
sessions,
clientreturnedto
work
andfelthis
improve
ment
42
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

(Con
tinu
ed)
business.nolongersu
pport
workingdiagnosisofADHD
wasdirectly
dueto
NF
trainingandthatheno
longerneededto
contin
ue
with
NF
18PR
12YOM
12YO
male,autistic
disorder,delayin
deve
lopmentofve
rbal
andnon-verbal
communicatio
n,lack
of
socialoremotio
nal
reciprocity,stereotyped
andrepetitivemotor
manners,im
pairedfin
emotor,Tourettes-like
physicalsp
asm
s,and
high-pitched
voca
lizatio
ns,
failure
todeve
loppeer
relatio
nsh
ips
QEEG
maps:
EC:bilateral
excess
ofhighbeta,
alphadeficitce
ntrally,
delta
excess
rt.Frontal,
delta
deicitce
ntrally,
broadfrontoce
ntral
hyp
oco
herence
s.
20
sessions
F3=F
4=C
3=
C4
verbalizatio
nsch
angedfrom
primarily
promptedand
time-delaye
dto
spontaneous
andreal-tim
e.Spontaneous
displays
ofaffection.
Decrease
inrepetitive
behaviors
andve
rbalizatio
ns.
Increase
dmotoricandve
rbal
self-regulatio
n.Increase
dvo
luntary
interactionwith
peers
inso
cialandschool
environments,im
prove
dsleeppatters,anddecrease
dnocturnalenuresis
QEEG
mapssh
owed
compensa
tion
mech
anismsatlow
and
highfrequency
after20
sessions,
‘‘containing’’
deficitareaswith
neighboring
compensa
tory
amplitude
excesses,
and
connectivity
‘‘ove
rshoot’’.
Furthernorm
alizatio
nse
enafter40se
ssions.
Evidence
ofsp
ecific
thalamic
andco
rtical
adaptivemech
anisms
dueto
operant
conditioning
19WLSam
7YO
male
rapid
learner,
easily
excite
dand
aggressivewith
other
children.Canbe
classifiedasAD=H
D
QEEG
maps:
EO:Delta
andtheta
excess
frontally,highbeta
excess
ove
rPz,
global
hyp
ercoherence
inall
bands,
particularlydelta
andhighbeta
21se
ssionsF3F4P3P4
visible
improve
mentin
behavior,notable
changein
interactionwith
NFstaff,
more
positiveand
cooperative,schoolreports
improve
dbehaviorand
reductionin
aggression
QEEG
mapssh
ow
significa
ntnorm
alizatio
n.
Phase
andrelated
measu
resremain
outside
norm
s
20DK
SonjaK
13
YO
female,diagnose
dICD
10earlych
ildhood,
F94.0
electivemutism,
now
F93.2
emotio
nal
disorderwith
anxiety,
F83.2
disca
lculia.
Emotio
naldiagnostics:
emothionalstress,total
blockingwith
‘‘open’’
tasks.
Markedso
ciala
nd
emotio
naltendency
towith
draw
successfulergotherapy,
waldorf-sch
ool7
thgrade
poormath,no
medicatio
n.HAWIK
3markedly
below
ave
rage,assumeddue
toanxiety
disorder
QEEG
maps:
significa
nt
excess
ofdelta
and
theta
diffuse
ly,andhigh
beta
occipita
l
15weeklyse
ssionsT3T4
C3C4Fp1Fp2O1O2F3
F4T5T6C3T3T5P3
Fp1F4T4P4(address
mirrorneurons;
empathy)
high
compliance
dim
inished
feelings
of
being
dominated,betterability
tostandupto
classmates,
beginssh
opping,meetin
gwith
friends.
Reports
increase
dalertness,
awake
ness
aftereach
session.Thinks
ofNFdisplay
‘‘dolphins’’duringschool
tests,
increase
dreaso
ning.
Improve
dse
lf-assurance
,math,so
cialskills,
open-m
indedness,ve
rbal
communicatio
n
QEEG
mapssh
ow
norm
alizatio
nduring1
session(session16),both
amplitudeand
connectivity.T3-C
4hyp
ercoherence
reduce
d,
Theta
T3,C4,T4,
hyp
ercoherence
fast
wave
snorm
alized,T5-P3,
prefrontalDelta
,ove
rall
frontalslowing
norm
alized.IVA,TOVA,
CPTforthco
ming
21JT
NW
9YO
female
moodsw
ings,
impulseco
ntrol
problems,
conce
ntratio
ndifficulties.
18mgConce
rtaplus
GABA
QEEG
maps:
excess
amplitudes,
hyp
oco
herence
theta
andalphaposterior
temporal
38se
ssions4-channel26
sessionsC3C4P3P4
11se
ssionsF3F4CzPz
atse
ssion27teach
erreported
significa
ntim
prove
ments
inse
lfco
ntrol.Atse
ssion33,
parents
indicatedthat
remainingproblemswere
due
BASCbehaviorassessment
system
resu
ltssh
ow
improve
ment,pre-and
post-Z-Sco
ressh
ow
changes.
24z-scores
(Con
tinu
ed)
43
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

TABLE
2(contin
ued)
Study#
CLIN
IDPrese
ntin
gPreviousTreatm
ent
Preassessment
#LZTSessionsandSite
sResu
ltEEG
Change
tofamily
dyn
amicsandold
behavioralhabits
-family
soughttherapy
show>1SD
change.
QEEG
mapssh
ow
essentia
lnorm
alizatio
n22DSTA
14YO
male,
preadolescentLD,
conce
ntratio
nproblems,
impulsivebehavior
Seve
ralADD
medicatio
ns
previouslyw=lim
ited
benefits,
unacceptable
sideeffects.
10mg
Abilify
for2.5
yrw=no
sideeffects,
some
increase
dco
nce
ntratio
n
20se
ssionsLZT
w=a
mplitudetrainingto
lower3–8Hz,
raise
16–19,andlower
22–30Hz.
self-reportedclinical
improve
mentin
allsymptoms
QEEG
mapssh
ow
light
reductionin
theta
z-scoresaswellas
20–30Hzz-scores.
16–19Hzrangerise
sto
%"1.6
SD.Essentia
llyco
mplete
coherence
norm
alizatio
nand
moderate
theta
abso
lute
powerim
prove
ments
visibly
evident
23HKHAR9
23YO
female
traumatic
headinjury
(atage13)
with
chronic
residual
cognitive
deficits
and
sleepdisturbance
.Short
term
memory
andword
retrieva
lproblems,
impulsivity,difficulty
conce
ntratin
g
Partialrighttemporal
lobectomyand
ventriculostomy.
AdderallXR
20mgand
Provigil200mgdaily,
helpedlittle
with
hyp
ersomnolence
.Paxil
20mgsince
age16.
Imipramine50mgthen
20mgdaily
Glasg
ow
Comascale
3on
admissionto
ER,in
comafor6.5
weeks.
Base
lineQEEG
shows
excess
Beta
andHigh
beta,mostly
leftfrontal.
Loreta
confirmsleft
frontalandtemporal
invo
lvementat9–25Hz
20
sessions
F3=C
3=T
4=
C430minutesonce
=weekso
metim
estwice=
week.
Counse
ling,
Vita
min
B2added
after7se
ssions,
significa
nt
improve
mentreportedby
patie
ntandmotherin
memory
andenvironmental
awareness.After20
sessions,
reportedsignifica
nt
improve
mentin
sleep
patterns,
able
tofallasleep
faster,andreturn
tosleepif
shewoke
upin
middle
of
night.increase
dawareness
ofco
gnitive
deficitand‘‘lost
time’’.
INcrease
dawareness
offuture,andability
toplan
foreduca
tionalactivities.
StartedB2,headach
es
decrease
d.
Post-treatm
ent
QEEG
forthco
ming.Contin
uing
weeklyse
ssions,
reports
steadyim
prove
mentof
memory
andco
gnition
24JW
NK
6YO
F,ch
ronic
anxiety,
difficulty
with
anger
control,reading
difficulty;left-handed
noprevioustreatm
ent
QEEG
showsexcess
slow
1–10HzatT5,O2,T3,
T6,T4,F8,Fp1,Fp2.
Excess
21–30HzatF3,
C3,P3,O1,Pz,
P4.
Coherence
deficitdelta
5L,1R,theta
3L,1R,
andalpha1R.
53se
ssions3x=
week,
variousplace
ments
No
longeranxious.
No
further
angeroutbursts.Readingat
gradeleve
l.Im
prove
dsh
ort-term
memory.
Improve
dfocu
singability.
AllQEEG
abnorm
alities
norm
alized.
Note.QEEG
Maps:
19-channelEEG
reco
rdingsanalyze
dusingNeuroGuide(AppliedNeurosc
ience
).Othmerrefers
tothelow-frequency
bipolartrainingperOthmer(2008).
LZT!LiveZ-Sco
retext
displays
onlivesc
reenoronstatisticalsummaries;
QEEG!quantitativeEEG;IVA!IntegratedVisuala
ndAudito
ryPerform
ance
Test;SSRI!
serotonin
re-uptake
inhibito
rs;NF!neurofeedback
;TOVA!Test
ofVariablesofAttentio
n.
44
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

the overshoot phenomenon and allowed thefeedback to be more effectively targeted.
Once the use of separate upper andlower Z-score limits became the practice,abreactions or negative side effects havenot been reported from the field, where thegeneral clinical population is involved.Results from our early clinical reports andtrials thus far suggest that well-targetedEEG normalization does not appear to havesignificant downside risk, when the pretreat-ment EEG is initially clearly abnormal. Mildabreactions have been observed by oneauthor (TFC) during training demonstra-tions on some individuals, in which theprominent EEG deviations appeared topotentially represent coping or compensa-tory mechanisms, and the Z-score traininghas the effect of reducing the deviations.Such deviations may be in amplitude or inconnectivity, or in both. For example,chronic pain sufferers may present with glo-bally decreased alpha power. We hypothe-size that this may reflect a state of tensionand abnormal activation of the cortex repre-senting some kind of coping mechanism, andthus, when alpha activity is uptrained, it mayresult in an increased experience of pain asthe coping mechanism is reduced. Whetheror not this is an abreaction is a matter of ter-minology, as restoration of sensory aware-ness, including pain, might be used as apath toward self-regulation and recovery.
As another example, clients with chronicanxiety may exhibit excess alpha, whichmay be a coping mechanism, or may simplyreflect their individual state of activation,particularly where emotional control andregulatory centers are involved. Again,downtraining the alpha, which is an acti-vation procedure, may result in increasedperception of anxiety, even as the EEGnormalizes. Another example arises whennormal, functional, achieving adults presentwith what the Z-score software interprets as‘‘excess SMR.’’ This excess is not necessarilyabnormal, may simply reflect an above-average ability to sit still and remain motion-less, or may reflect the normal onset ofdrowsiness. This variant is in fact commonlyseen in clinical professionals, for whom still-ness and attentiveness are traits that are
cultivated and nurtured, and in trainingworkshops, in which drowsiness may appearunder normal circumstances. In some indivi-duals in these circumstances, downtrainingthe SMR has been seen to result in a feelingof irritation and uneasiness, secondary to theactivation of the trained areas.
DISCUSSION AND CONCLUSIONS
It has been seen that the LZT trainingused here is capable of inducing brainchanges that are specific and profound,particularly with regard to whole-brainactivation and connectivity. Using this tech-nique in conjunction with QEEG and beha-vioral data, it is possible to demonstrateclinical effects that are well correlated withobjective measures, and support the claimthat this approach is an important additionto clinical practice.
It has been found that four-channel LZTtraining is sufficient to resolve globalconnectivity issues and that it can effectivelytarget abnormalities visible on the LOR-ETA, and to resolve them. This is likelybecause the brain has limited degrees of free-dom, and in order to bring a predominanceof parameters into the normal range, otherparameters must also normalize. That is,when sufficiently constrained, the brain can-not conspire to ‘‘circumvent’’ the training,and produce untoward effects.
Nonetheless, when using the MVPapproach, it is found that the brain is pro-vided with information that is particularlyvaluable. By ignoring ‘‘outliers,’’ the braincan concentrate on fundamental mechan-isms, without being distracted by details thatmay confound the training. If only somefraction of Z-scores are required to fallwithin a target for rewards, then the trainee’sEEG is given a large dynamic range withinwhich to function. By using smaller targets,and allowing some Z-scores to remain out-side the defined range, the brain is providedwith options, that it appears to be preparedto use to best advantage.
With LZT training, the brain is exploringits dynamic range, and this is key to theeffectiveness. It is broadening its functional
Clinical Corner 45
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

repertoire, and is finding a trajectory andpath toward normalization that is not astraight line through state space. It is a cir-cuitous path, but it is a path that the brainseems to be equipped to navigate. Everyperson may respond differently, but LZTtrainees receive concise information withwhich to develop and implement a strategytoward self-regulation.
Again, because the technique using MVPallows the extreme deviations to beuntouched, you are allowing the brain to cre-ate its own strategy toward normalization. Itis significant that clients may have clinicalbenefits uniformly through the treatment. Itis also important to vary the target size andthe percentage of Z-scores required, so thatthe brain has full information to explorethese boundaries, without requiring fullnormalization from the start.
We have found that four channels is actu-ally very effective at localizing and trainingthe entire brain, and some of our publishedresults show the whole-head EEG beingessentially normalized, as a result ofjudicious choice of the four channels. Mostoften, montages such as F3=F4=P3=P4 orF3=F3=C3=C4 are used. There is also a‘‘big box’’ that can be used, which is F7=F8=T5=T6. When four channels are well cho-sen, the brain does not have a lot of room tomove around. We do not generally see pro-blems due to the fact that the four channelshave missed anything. It is possible to ident-ify certain montages that appear to isolatefunctional hubs and subsystems. Theseprovide additional focus and meaning forplacements for four-channel training. Forexample, posterior integration issues associa-ted with stress or aging are well addressed byusing C3=C4=P3=P4.
We believe that assessing the client’sclinical signs and ‘‘complaints’’ is essentialto planning and carrying out the LZT train-ing. It is possible to more flexibly addressvarious brain areas quickly when the chan-nels can be quickly changed, as with aMINI-Q, or when using a full 19-channelcap with LZT training. However, the econ-omy and convenience of applying fourmonopolar leads provides benefits of sim-plicity. It is fair to say that four-channel
LZT training is being proven and that it isa robust and effective method.
REFERENCES
Collura, T. F. (2008a, April). Whole-head normaliza-tion using live Z-scores for connectivity training(Part 1). NeuroConnections, 12–18.
Collura, T. F. (2008b, July). Whole-head normaliza-tion using live Z-scores for connectivity training(Part 2). NeuroConnections, 9–12.
Collura, T. F. (2009). Neuronal dynamics in relation tonormative electroencephalography assessment andtraining. Biofeedback, 36, 134–139.
Collura, T. F., & Thatcher, R. W. (2006, April 29).Real-time EEG Z-score training, realities and pro-spects. Bedford, OH: BrainMaster Technologies,Inc, and Applied Neurosciences, Inc.
Collura, T. F., Thatcher, R. W., Smith, M. L.,Lambos, W. A., & Stark, C. A. (2009). EEG bio-feedback training using live Z-scores and a norma-tive database. In T. Budzynski, H. Budzynski, J.Evans, & A. Abarbanal (Eds.), Introduction toquantitative EEG and neurofeedback (2nd ed., pp.103–141). Amsterdam: Elsevier.
DuRousseau, D. (2007, September). Simultaneoustraining of slow cortical potentials & coherence inchildren with AD=HD using realtime Z-score neuro-feedback: A preliminary study. Paper presented atthe annual meeting of the International Societyfor Neurofeedback and Research.
Rutter, P. (2009, April). Reconnecting our lost childrento the world – Z-score training and autistic disorder.Paper presented at the 40th annual meeting of theAssociation for Applied Psychophysiology and Bio-feedback, Albuquerque, NM.
Smith, M. L. (2008, April). A father finds a solution:Z-score training. NeuroConnections, 22–25.
Stark, C. (2008, April). Consistent dynamic Z-scorepatterns observed during Z-score training sessions.NeuroConnections, 37–38.
Thatcher, R. W. (1998). EEG normative databases andEEGbiofeedback. Journal ofNeurotherapy, 2(4), 8–39.
Thatcher, R. W. (1999) EEG database guided neu-rotherapy. In J. R. Evans & A. Abarbanal (Eds.),Introduction to quantitative EEG and neurofeedback(pp. 72–93). San Diego, CA: Academic.
Thatcher, R. W. (2004) Z-score EEG biofeedback—Technical foundations. St. Petersburg, FL: AppliedNeurosciences, Inc.
Wigton, N. (2008, August–September). Does Z-scoreNF work better than non Z-score NF? Paperpresented at the 16th Annual International Societyfor Neurofeedback and Research Conference, SanAntonio, TX.
46 JOURNAL OF NEUROTHERAPY
Downloaded By: [WNEU Journal of Neurotherapy] At: 20:30 28 July 2010

![WHS AGA Presentation Version - IGA+roh ,q 7rwdo 3du 6 , 6fruh 6xqq\vlgh *roi &oxe %urq]h 7hhv &rxuvh 5dwlqj 6orsh 5dwlqj 1dph ri 3od\hu -dqhw 6plwk &rxuvh +dqglfds 1hw grxeoh erjh\](https://img.pdfslide.us/doc/110x75/5f85003bd6d0aa294f330747/whs-aga-presentation-version-iga-roh-q-7rwdo-3du-6-6fruh-6xqqvlgh-roi-oxe.jpg)