-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
1/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsedTi
Offi cial reprint from UpToDatewww.uptodate.com 2016
UpToDate
AuthorsGregory YH Lip, MD, FRCPE,FESC, FACCRussell D Hull, MBBS,
MSc
Section EditorsLawrence LK Leung, MDJess Mandel, MD
Deputy EditorGeraldine Finlay, MD
Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
All topics are updated as new evidence becomes available and our
peer review process is complete.
Literature review current through: Feb 2016. | This topic last
updated: Nov 03, 2014.
INTRODUCTION Venous thromboembolism (VTE) is comprised of two
entities, deep venous thrombosis
(DVT) and pulmonary embolus (PE). VTE has significant morbidity
and mortality for both the inpatient and
outpatient population. The risk of recurrent thrombosis and
embolization is highest in the first few days and weeks
following diagnosis. Initial anticoagulation during the first 5
to 10 days is critical in the prevention of recurrence and
VTE-related death.
The agents used, timing, duration, and dosing of initial
anticoagulation for the treatment of DVT are discussed in
this topic. The indications and overview of DVT treatment, as
well as long-term (3 to 12 m onths) and extended
(indefinite) anticoagulation for patients with VTE are discussed
separately. (See "Overview of thetreatment oflower extremity deep
vein thrombosis (DVT)", section on 'Patients with contraindications
to anticoagulation' and
"Lower extremity deep venous thrombosis: Long-term
anticoagulation (10 days to three months)" and "Rationale
and indications for indefinite anticoagulation in patients with
venous thromboembolism".)
NOMENCLATURE For the purposes of discussion in this topic, the
following terms apply:
INDICATIONS Most patients with ultrasound-proven proximal DVT
(popliteal, femoral, or iliac vein DVT) and
select cases of distal DVT (below the knee and in the calf veins
peroneal, posterior, and anterior tibial DVT)
should be anticoagulated. The indication to anticoagulate is
stronger for patients with proximal DVT than with
distal DVT because the risk of complications, particularly
embolization, is higher. Although the efficacy ofanticoagulant
therapy in patients with asymptomatic DVT (ie, incidental DVT) is
unknown, we and others prefer
that this population of patients be managed or anticoagulated in
the same manner as symptomatic patients [ 2]. For
each patient, the decision to anticoagulate must weigh the risk
of morbidity and mortality without anticoagulation
against the risk of bleeding on anticoagulation. Details of the
indications for anticoagulation are discussed
separately. (See "Overview of the treatment of lower extremity
deep vein thrombosis (DVT)", section on
'Indications'.)
BLEEDING RISK In all patients, the decision to anticoagulate
should be individualized and the benefits of
venous thromboembolism (VTE) prevention carefully weighed
against the risk of bleeding (table 1). Most clinicians
agree that patients with a three-month bleeding risk less than 2
percent (low risk) should be anticoagulated and
Initial anticoagulation is administered over the first 5 to 10
days following a diagnosis of DVT. Long-term
anticoagulant therapy is typically administered for a finite
period beyond the initial period, usually three to six
months and occasionally up to 12 months. Extended
anticoagulation usually refers to therapy that is
administered indefinitely. (See "Lower extremity deep venous
thrombosis: Long-term anticoagulation (10 days
to three months)" and "Rationale and indications for indefinite
anticoagulation in patients with venous
thromboembolism".)
Factor Xa and direct thrombin inhibitors have a variety of names
including newer/novel oral anticoagulants,
non-vitamin K antagonist oral anticoagulants (NOAs, NOACs), and
target-specific oral anticoagulants
(TOACs, TSOACs) [1]. Throughout this topic we refer to these
agents by their pharmacologic class, factor
Xa and direct thrombin inhibitors. (See "Anticoagulation with
direct thrombin inhibitors and direct factor Xa
inhibitors".)
http://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=INDICATIONS&anchor=H3#H3http://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=INDICATIONS&anchor=H3#H3http://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=INDICATIONS&anchor=H3#H3http://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=INDICATIONS&anchor=H3#H3http://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=INDICATIONS&anchor=H3#H3http://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=INDICATIONS&anchor=H3#H3http://www.uptodate.com/contents/anticoagulation-with-direct-thrombin-inhibitors-and-direct-factor-xa-inhibitors?source=see_linkhttp://www.uptodate.com/contents/anticoagulation-with-direct-thrombin-inhibitors-and-direct-factor-xa-inhibitors?source=see_linkhttp://www.uptodate.com/contents/rationale-and-indications-for-indefinite-anticoagulation-in-patients-with-venous-thromboembolism?source=see_linkhttp://www.uptodate.com/contents/rationale-and-indications-for-indefinite-anticoagulation-in-patients-with-venous-thromboembolism?source=see_linkhttp://www.uptodate.com/contents/rationale-and-indications-for-indefinite-anticoagulation-in-patients-with-venous-thromboembolism?source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-long-term-anticoagulation-10-days-to-three-months?source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/rationale-and-indications-for-indefinite-anticoagulation-in-patients-with-venous-thromboembolism?source=see_linkhttp://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=Patients+with+contraindications+to+anticoagulation&anchor=H256309218#H256309218http://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=Patients+with+contraindications+to+anticoagulation&anchor=H256309218#H256309218http://www.uptodate.com/home/editorial-policyhttp://www.uptodate.com/contents/anticoagulation-with-direct-thrombin-inhibitors-and-direct-factor-xa-inhibitors?source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/1http://www.uptodate.com/contents/rationale-and-indications-for-indefinite-anticoagulation-in-patients-with-venous-thromboembolism?source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-long-term-anticoagulation-10-days-to-three-months?source=see_linkhttp://www.uptodate.com/contents/image?imageKey=PULM%2F97160&topicKey=PULM%2F95336&rank=8%7E150&source=see_linkhttp://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=INDICATIONS&anchor=H3#H3http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/2http://www.uptodate.com/contents/rationale-and-indications-for-indefinite-anticoagulation-in-patients-with-venous-thromboembolism?source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-long-term-anticoagulation-10-days-to-three-months?source=see_linkhttp://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=Patients+with+contraindications+to+anticoagulation&anchor=H256309218#H256309218http://www.uptodate.com/home/editorial-policyhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/contributorshttp://www.uptodate.com/
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
2/28
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
3/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsedTi
3
TIMING, DURATION, AND DOSING For patients with proximal DVT, the
greatest risk of embolization is
during the first three months of anticoagulant therapy and, in
particular, during the first few days following the
diagnosis. When the decision is made to anticoagulate patients
with DVT, anticoagulant therapy should be started
immediatelyas a delay may potentially increase the risk of
life-threatening embolization. Baseline coagulation
tests (prothrombin time, International Normalized Ratio [INR],
activated partial thromboplastin time [aPTT]) should
be drawn prior to the initiation of anticoagulation to guide
therapy. The timing, duration, and dose of initial
anticoagulation vary with the agent selected and are discussed
in the sections below.
For most patients, warfarin and heparin are started on the first
day, and heparin is continued for a minimum of four
to five days until the INR has been within therapeutic range for
a minimum of 24 to 48 hours. There is no benefit to
prolonged courses of systemic heparin beyond the achievement of
a therapeutic INR. (See 'Transitioning to
maintenance therapy' below.)
Low-molecular-weight heparin As described above,
low-molecular-weight (LMW) heparin is our preferred
anticoagulant for most patients with newly diagnosed DVT, in
particular for those with active cancer or pregnancy.
(See 'Selection of agent'above.)
Dosing The initial therapeutic dose of LMW heparin (eg,
enoxaparin, dalteparin, tinzaparin) varies by
product. Dosing is typically weight based and renally adjusted,
and all are administered subcutaneously (SC).
Typical starting doses are:
Dosing for obese patients and patients with renal insufficiency
is listed in the tables ( table 2 and table 3). (See
"Therapeutic use of unfractionated heparin and low molecular
weight heparin", section on 'LMW heparin'.)
Efficacy Evidence from several randomized trials and
meta-analyses have reported that, compared with
intravenous (IV) and SC unfractionated heparin (UFH), SC LMW
heparin has higher rates of thrombus regressionand lower rates of
recurrent thrombosis, major bleeding, and mortality [6-19].
However, the data are fraught with
methodologic flaws, including publication bias in favor of LMW
heparin. Thus, at minimum, LMW heparin appears
to be as safe and as effective as UFH (IV and SC).
cancer or pregnant women, their safety and efficacy is unproven,
and, as such, they should not be routinely
used in these populations.
Enoxaparin 1 mg/kg twice daily (or 1.5 mg/kg once daily)
Dalteparin 200 units/kg once daily for the first 30 days
followed by 150 units/kg for maintenance
Tinzaparin 175 units/kg once daily (not available in the United
States)
In a 2010 meta-analysis of 23 studies that compared LMW heparin
with IV or SC UFH in patients with acute
venous thromboembolism (VTE DVT and/or pulmonary embolus [PE]),
LMW heparin was associated with
the following [15]:
Fewer thrombotic complications (eg, recurrence, extension,
embolization) (3.6 versus 5.3 percent odds
ratio [OR] 0.70, 95% CI 0.57-0.85)
Improved thrombus regression (53 versus 45 percent of
participants OR 0.69, 95% CI 0.59-0.81)
Reduced rates of major hemorrhage (1 versus 2 percent OR 0.58,
95% CI 0.40-0.83)
Reduced mortality (4 versus 6 percent OR 0.77, 95% CI
0.63-0.93)
An older meta-analysis of 13 studies of patients with acute VTE
performed between 1980 and 1994 reported
that, compared with UFH, LMW heparin was associated with a lower
rate of both recurrent VTE (2.7 versus
7 percent) and major bleeding (0.9 versus 3.2 percent) [9].
A 1999 meta-analysis of 11 trials of patients with acute DVT
found a lower mortality rate at three to six
months among patients treated with LMW heparin, compared with
those receiving UFH (OR 0.71, 95% CI
http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/9http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/15http://www.uptodate.com/contents/tinzaparin-drug-information?source=see_linkhttp://www.uptodate.com/contents/dalteparin-drug-information?source=see_linkhttp://www.uptodate.com/contents/enoxaparin-drug-information?source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/6-19http://www.uptodate.com/contents/heparin-unfractionated-drug-information?source=see_linkhttp://www.uptodate.com/contents/therapeutic-use-of-unfractionated-heparin-and-low-molecular-weight-heparin?source=see_link§ionName=LMW+HEPARIN&anchor=H29#H29http://www.uptodate.com/contents/image?imageKey=HEME%2F90258&topicKey=PULM%2F95336&rank=8%7E150&source=see_linkhttp://www.uptodate.com/contents/image?imageKey=HEME%2F65464&topicKey=PULM%2F95336&rank=8%7E150&source=see_linkhttp://www.uptodate.com/contents/tinzaparin-drug-information?source=see_linkhttp://www.uptodate.com/contents/dalteparin-drug-information?source=see_linkhttp://www.uptodate.com/contents/enoxaparin-drug-information?source=see_linkhttp://www.uptodate.com/contents/warfarin-drug-information?source=see_link
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
4/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsedTi
4
Once daily regimens of LMW heparin appear to be as effective as
twice daily regimens. Meta-analyses of trials
directly comparing once versus twice daily administration found
no differences in recurrent thrombosis, major
hemorrhage, or mortality [11,12,20-25]. The largest study of 900
patients with symptomatic DVT, a third of whom
also had PE, compared the LMW heparin, enoxaparin, administered
as a standard twice daily regimen (1 mg/kg
twice daily), with a lower once daily regimen (1.5 mg/kg per
day) [11]. Although rates of recurrence (3 versus 4
percent) and hemorrhage (1 versus 2 percent) were lower with the
twice daily regimen, the difference was not
significant and may have been explained by the lower total daily
dose administered in the once daily treatment
group. Except for enoxaparin, we prefer, when once daily dosing
is being considered, that it be administered at the
same total daily dose as a twice daily schedule.
The LMW heparins have a number of advantages over unfractionated
heparin [26,27]. (See "Therapeutic use of
unfractionated heparin and low molecular weight heparin",
section on 'Advantages and limitations' .)
Disadvantages of LMW heparin compared with UFH include the
higher cost, and, although protamine is an
antidote for hemorrhage, its effect is incomplete. In addition,
efficacy is less certain in the obese population, in
patients with renal failure, and in older patients who are
underweight (
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
5/28
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
6/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsedTi
6
discussed in detail separately. (See 'Selection of agent' above
and 'Low-molecular-weight heparin'above.)
The efficacy of IV UFH depends upon achieving a critical
therapeutic level as soon as possible, preferably within
the first 24 hours of treatment, usually via a continuous IV
infusion [ 14,30,38-42]. The critical therapeutic level of
heparin, as measured by the aPTT, is a target aPTT ratio range
of 1.5 to 2.5 times the control. This corresponds to
a heparin level of 0.3 to 0.7 units/mL, when measured by an
anti-Xa assay [43,44]. Studies that support this target
range include the following:
Although there is a strong correlation between subtherapeutic
aPTT values and recurrent thromboembolism, the
relationship between supratherapeutic aPTT (ie, an aPTT ratio
2.5 or more) and bleeding is less definite [ 31].
Nonetheless, aiming for a therapeutic range with the avoidance
of periods of both subtherapeutic and
supratherapeutic levels is prudent.
The advantages of UFH compared with LMW heparin include its
lower cost and its safe use in those with renal
insufficiency. An additional advantage of the IV formulation is
its short half-life, particularly for patients in whom
there is a potential need for acute discontinuation (eg,
surgery). Disadvantages include that infusions of UFH
require hospital admission, and both SC and IV UFH are
associated with a higher potential for HIT. (See
"Therapeutic use of unfractionated heparin and low molecular
weight heparin", section on 'Other complications' .)
Direct factor Xa and thrombin inhibitors
Dosing We advocate for the use of oral factor Xa (rivaroxaban,
apixaban, edoxaban) or direct thrombin
inhibitors (dabigatran) in accordance with criteria in clinical
trials that demonstrated their efficacy. These agents
are attractive candidates as initial anticoagulants in patients
with acute DVT due to their quick onset of action
(peak efficacy one to four hours after ingestion). In trials
that evaluated dabigatran and edoxaban, all patients were
treated with five days of heparin prior to their administration
(ie, "dual therapy" initial anticoagulation) as such, we
prefer that a short course of heparin be administered before
transitioning to either dabigatran or edoxaban. In
contrast, rivaroxaban and apixaban were evaluated as
anticoagulants without prior administration of heparin (ie,
monotherapy) our clinical experience is in keeping with the data
that support their use as the sole initial
anticoagulant. Importantly, anticoagulant therapy with heparin
should not be delayed while the decision is being
made to treat with one of these newer oral agents. (See
'Selection of agent'above.)
Many of these agents are renally excreted, and patients with a
creatinine clearance of 1.5,
patients who had an aPTT ratio
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
7/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsedTi
7
Maintenance doses for long-term anticoagulation are discussed
separately. (See "Anticoagulation with direct
thrombin inhibitors and direct factor Xa inhibitors" and "Lower
extremity deep venous thrombosis: Long-term
anticoagulation (10 days to three months)", section on 'Direct
thrombin and factor Xa inhibitors'.)
In keeping with the clinical trials that demonstrated their
efficacy, in patients who are receiving heparin as the
initial anticoagulant, we prefer that oral factor Xa or direct
thrombin inhibitors be given within 6 to 12 hours
following the last dose of SC LMW heparin when administered as a
twice daily regimen, or within 12 to 24 hours
for once daily regimens. Infusions of UFH can be immediately
discontinued following the administration of these
oral agents. (See "Lower extremity deep venous thrombosis:
Long-term anticoagulation (10 days to three months)",
section on 'Transitioning to long-term therapy'.)
The efficacy and safety of factor Xa and direct thrombin
inhibitors as anticoagulants for extensive DVT (eg,
patients with phlegmasia cerulea dolens) or hemodynamically
significant pulmonary embolus are unknown, and, as
such, they should NOTbe used in these patient populations where
their use may interfere with the potential
administration of thrombolytic therapy. Similarly, because their
safety and efficacy is unproven, we prefer that
these agents NOTbe administered in patients who are pregnant or
in patients with active malignancy. (See
"Overview of the treatment of lower extremity deep vein
thrombosis (DVT)", section on 'Phlegmasia cerulea
dolens' and "Fibrinolytic (thrombolytic) therapy in acute
pulmonary embolism and lower extremity deep vein
thrombosis" and "Deep vein thrombosis and pulmonary embolism in
pregnancy: Treatment" and "Treatment of
venous thromboembolism in patients with malignancy".)
Efficacy Randomized trials of these oral agents in patients with
acute DVT examined efficacy and safety in
the context of long-term anticoagulation with the same oral
agent for three months or more. When compared with
conventional courses of LMW heparin or IV UFH followed by
long-term anticoagulation with warfarin, these agents
had similar rates of recurrent thrombosis and major hemorrhage
[45-48]. However, trials that reported efficacy for
dabigatran (direct thrombin inhibitor) and edoxaban(factor Xa
inhibitor) used a minimum of five days of
anticoagulation with LMW heparin or UFH prior to their
administration for long-term oral therapy (ie, dual therapy)
[47,48]. In contrast, trials of rivaroxaban and apixaban
reported efficacy of both agents as the sole initial
anticoagulant (monotherapy). Although short periods (
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
8/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsedTi
8
withhold when the suspicion is low, provided testing is not
delayed for >24 hours [ 3]. Empiric anticoagulation may
be considered for those in whom the suspicion is assessed as
intermediate, particularly when testing is expected
to be delayed for more than four hours. For empiric
anticoagulation, we prefer therapeutic low-molecular-weight
(LMW) or unfractionated heparin(UFH) for as short a period as is
feasible, provided there are no contraindications.
The diagnosis of DVT is discussed separately. (See "Diagnosis of
suspected deep vein thrombosis of the lower
extremity".)
SPECIAL POPULATIONS When choosing an initial anticoagulant,
patients with malignancy, pregnant women,
outpatients, and those with a history of heparin-induced
thrombocytopenia (HIT) deserve special consideration.
Malignancy For most patients with malignancy and DVT who have a
reasonable life expectancy and adequate
renal function (creatinine clearance 30 mL/min),
low-molecular-weight (LMW) heparin is the preferred agent for
initial anticoagulation, rather than other agents. There is
insufficient evidence to support the use of factor Xa and
direct thrombin inhibitors in patients with malignancy at this
time. This is discussed in more detail separately. (See
"Treatment of venous thromboembolism in patients with
malignancy".)
Pregnancy For pregnant women with acute DVT, adjusted-dose
subcutaneous (SC) LMW heparin is the
preferred agent for initial anticoagulation because it has a
more favorable safety profile, especially when compared
with warfarin. Warfarin freely crosses the placental barrier and
can produce an embryopathy when given between
the sixth and ninth weeks of pregnancy. Intravenous (IV) and SC
forms of unfractionated heparin (UFH) are
alternatives to LMW heparin. Factor Xa and direct thrombin
inhibitors have not been adequately tested in pregnantwomen with
acute DVT and should not be administered. (See "Deep vein
thrombosis and pulmonary embolism in
pregnancy: Treatment" and "Use of anticoagulants during
pregnancy and postpartum".)
Outpatients Not all patients who have acute DVT need to be
admitted to the hospital for initial anticoagulation.
Several randomized trials and meta-analyses that have compared
outpatient therapy with SC LMW heparin with
inpatient therapy with IV UFH suggest that, in select
populations, treatment at home with LMW heparin is safe
and effective. Most clinicians agree that outpatient therapy
with LMW heparin can be considered in
hemodynamically stable patients with a low bleeding risk, who
have a practical system in place for the
administration and surveillance of anticoagulant therapy, who
are also without renal insufficiency, massive DVT,
concurrent pulmonary embolism, or other comorbid conditions that
require inpatient care (table 7). The decision to
anticoagulate as an outpatient should be made in the context of
the patients understanding of the risk-benefit ratio,preferences,
and clinical condition. The outpatient treatment of DVT and
pulmonary embolism are discussed
separately. (See "Overview of the treatment of lower extremity
deep vein thrombosis (DVT)", section on
'Outpatient therapy' and "Overview of the treatment, prognosis,
and follow-up of acute pulmonary embolism in
adults", section on 'Outpatient anticoagulation'.)
Heparin-induced thrombocytopenia For patients with a DVT and a
prior diagnosis of HIT, any form of heparin
is contraindicated. This includes systemic UFH, LMW heparin,
heparin flushes, heparin-bonded catheters, and
heparin-containing medications. Immediate anticoagulation with a
non-heparin anticoagulant (eg, argatroban,
danaparoid, fondaparinux, bivalirudin) is indicated (table 8).
The diagnosis and management of patients with HIT
are discussed in detail separately. (See "Clinical presentation
and diagnosis of heparin-induced thrombocytopenia"
and "Management of heparin-induced thrombocytopenia".)
TRANSITIONING TO MAINTENANCE THERAPY Therapeutic anticoagulation
should be ensured during the
transition from initial to long-term (maintenance) therapy. The
optimal transition strategy varies with the long-term
anticoagulant chosen.
When warfarin is chosen as the agent for long-term
anticoagulation, it is typically started on the same day with
low-molecular-weight (LMW) heparin, unfractionated heparin(UFH),
or fondaparinuxand dose adjusted until the
International Normalized Ratio (INR) is within the therapeutic
range (2 to 3 target 2.5) for a minimum of 24 to 48
hours [50]. Typical starting doses of warfarin are 5 mg/day for
two days (range 2 mg to 10 mg/day) (table 9). Initial
doses at the lower range (2 to 5 mg/day) may be considered in
those assessed at high bleeding risk (eg, older
adults), and doses in the higher range (5 to 10 mg/day) may be
selected in healthy individuals who are without
http://www.uptodate.com/contents/image?imageKey=HEME%2F71791&topicKey=PULM%2F95336&rank=8%7E150&source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/50http://www.uptodate.com/contents/fondaparinux-drug-information?source=see_linkhttp://www.uptodate.com/contents/heparin-unfractionated-drug-information?source=see_linkhttp://www.uptodate.com/contents/warfarin-drug-information?source=see_linkhttp://www.uptodate.com/contents/management-of-heparin-induced-thrombocytopenia?source=see_linkhttp://www.uptodate.com/contents/clinical-presentation-and-diagnosis-of-heparin-induced-thrombocytopenia?source=see_linkhttp://www.uptodate.com/contents/image?imageKey=HEME%2F73727&topicKey=PULM%2F95336&rank=8%7E150&source=see_linkhttp://www.uptodate.com/contents/bivalirudin-drug-information?source=see_linkhttp://www.uptodate.com/contents/fondaparinux-drug-information?source=see_linkhttp://www.uptodate.com/contents/danaparoid-drug-information?source=see_linkhttp://www.uptodate.com/contents/argatroban-drug-information?source=see_linkhttp://www.uptodate.com/contents/overview-of-the-treatment-prognosis-and-follow-up-of-acute-pulmonary-embolism-in-adults?source=see_link§ionName=Outpatient+anticoagulation&anchor=H286668969#H286668969http://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=Outpatient+therapy&anchor=H726449277#H726449277http://www.uptodate.com/contents/image?imageKey=HEME%2F70140&topicKey=PULM%2F95336&rank=8%7E150&source=see_linkhttp://www.uptodate.com/contents/use-of-anticoagulants-during-pregnancy-and-postpartum?source=see_linkhttp://www.uptodate.com/contents/deep-vein-thrombosis-and-pulmonary-embolism-in-pregnancy-treatment?source=see_linkhttp://www.uptodate.com/contents/heparin-unfractionated-drug-information?source=see_linkhttp://www.uptodate.com/contents/warfarin-drug-information?source=see_linkhttp://www.uptodate.com/contents/treatment-of-venous-thromboembolism-in-patients-with-malignancy?source=see_linkhttp://www.uptodate.com/contents/diagnosis-of-suspected-deep-vein-thrombosis-of-the-lower-extremity?source=see_linkhttp://www.uptodate.com/contents/heparin-unfractionated-drug-information?source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/3
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
9/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsedTi
9
obvious risk for bleeding. Subsequent dose adjustments are made
to target an INR of 2 to 3. Initial dosing and
maintenance therapy for warfarin are discussed separately. (See
"Therapeutic use of warfarin and other vitamin K
antagonists", section on 'Warfarin administration' and "Lower
extremity deep venous thrombosis: Long-term
anticoagulation (10 days to three months)", section on
'Warfarin' .)
When subcutaneous LMW heparin and fondaparinux are chosen for
long-term anticoagulation and they have not
been chosen as the initial anticoagulant, they can be
administered subcutaneously (SC) and intravenous (IV) UFH
immediately discontinued. Oral factor Xa or direct thrombin
inhibitors are generally given within 6 to 12 hours
following the last dose of a twice daily regimen of SC LMW
heparin, within 12 to 24 hours for once daily regimens,
and upon the discontinuation of the IV UFH infusion.
Transitioning from initial to maintenance therapy and
switching anticoagulants during therapy are discussed in detail
separately. (See "Lower extremity deep venous
thrombosis: Long-term anticoagulation (10 days to three
months)", section on 'Transitioning to long-term therapy'
and "Lower extremity deep venous thrombosis: Long-term
anticoagulation (10 days to three months)", section on
'Transitioning during therapy'.)
INFORMATION FOR PATIENTS UpToDate offers two types of patient
education materials, The Basics and
Beyond the Basics. The Basics patient education pieces are
written in plain language, at the 5th to 6th grade
reading level, and they answer the four or five key questions a
patient might have about a given condition. These
articles are best for patients who want a general overview and
who prefer short, easy-to-read materials. Beyond
the Basics patient education pieces are longer, more
sophisticated, and more detailed. These articles are written
at the 10th to 12th grade reading level and are best for
patients who want in-depth information and are comfortable
with some medical jargon.
Here are the patient education articles that are relevant to
this topic. We encourage you to print or e-mail these
topics to your patients. (You can also locate patient education
articles on a variety of subjects by searching on
patient info and the keyword(s) of interest.)
SUMMARY AND RECOMMENDATIONS
Basics topics (See "Patient information: Deep vein thrombosis
(DVT) (Beyond the Basics)".)
Beyond the Basics topics (see "Patient information: Deep vein
thrombosis (DVT) (Beyond the Basics)" and
"Patient information: Warfarin (Coumadin) (Beyond the
Basics)")
Initial anticoagulation refers to systemic anticoagulation
administered for the first 5 to 10 days following a
diagnosis of deep venous thrombosis (DVT). Anticoagulation
should be started immediately as a delay
increases the risk of embolization and death. The choice of
initial anticoagulation is the same for patients
with proximal, distal, symptomatic, and asymptomatic DVT. (See
'Nomenclature'above.)
Every patient with acute DVT should be assessed for the risk of
bleeding prior to anticoagulation. Most
clinicians agree that anticoagulation should be administered to
patients with a low risk of bleeding and
avoided in those at high risk. For patients with a moderate risk
of bleeding, the decision to anticoagulate
must be individualized according to the values and preferences
of the patient as well as the risk-benefit ratio
as assessed by the clinician. (See 'Bleeding risk' above and
"Overview of the treatment of lower extremity
deep vein thrombosis (DVT)", section on 'Assessing bleeding
risk' and "Management of warfarin-associated
bleeding or supratherapeutic INR", section on 'Bleeding
risk'.)
For patients with acute DVT, treatment options for initial
anticoagulation include the following: low-molecular-
weight (LMW) heparin, fondaparinux, unfractionated heparin(UFH),
and oral factor Xa and direct thrombin
inhibitors. In general:
For most patients, we suggest LMW heparin rather than other
agents (fondaparinux, intravenous [IV]
UFH, factor Xa or direct thrombin inhibitors) (Grade 2B).
Fondaparinux is an acceptable alternative for
nonpregnant patients. A decision between LMW heparin and
fondaparinux is usually made based on
clinician experience and availability. Dosing is individualized
for each product. (See 'Selection of agent'
http://www.uptodate.com/contents/grade/5?title=Grade%202B&topicKey=PULM/95336http://www.uptodate.com/contents/fondaparinux-drug-information?source=see_linkhttp://www.uptodate.com/contents/heparin-unfractionated-drug-information?source=see_linkhttp://www.uptodate.com/contents/fondaparinux-drug-information?source=see_linkhttp://www.uptodate.com/contents/management-of-warfarin-associated-bleeding-or-supratherapeutic-inr?source=see_link§ionName=BLEEDING+RISK&anchor=H624013#H624013http://www.uptodate.com/contents/overview-of-the-treatment-of-lower-extremity-deep-vein-thrombosis-dvt?source=see_link§ionName=ASSESSING+BLEEDING+RISK&anchor=H102101510#H102101510http://www.uptodate.com/contents/warfarin-coumadin-beyond-the-basics?source=see_linkhttp://www.uptodate.com/contents/deep-vein-thrombosis-dvt-beyond-the-basics?source=see_linkhttp://www.uptodate.com/contents/deep-vein-thrombosis-dvt-beyond-the-basics?source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-long-term-anticoagulation-10-days-to-three-months?source=see_link§ionName=TRANSITIONING+DURING+THERAPY&anchor=H105730846#H105730846http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-long-term-anticoagulation-10-days-to-three-months?source=see_link§ionName=TRANSITIONING+TO+LONG-TERM+THERAPY&anchor=H28215420#H28215420http://www.uptodate.com/contents/fondaparinux-drug-information?source=see_linkhttp://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-long-term-anticoagulation-10-days-to-three-months?source=see_link§ionName=Warfarin&anchor=H105731110#H105731110http://www.uptodate.com/contents/therapeutic-use-of-warfarin-and-other-vitamin-k-antagonists?source=see_link§ionName=WARFARIN+ADMINISTRATION&anchor=H21#H21
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
10/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
10
Use of UpToDate is subject to the Subscription and License
Agreement.
REFERENCES
1. Husted S, de Caterina R, Andreotti F, et al. Non-vitamin K
antagonist oral anticoagulants (NOACs): No
above and 'Low-molecular-weight heparin'above and
'Fondaparinux'above.)
For patients with severe renal failure (eg, creatinine
clearance
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
11/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
1
longer new or novel. Thromb Haemost 2014 111:781.
2. Hull RD, Raskob GE, Rosenbloom D, et al. Heparin for 5 days
as compared with 10 days in the initialtreatment of proximal venous
thrombosis. N Engl J Med 1990 322:1260.
3. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy
for VTE disease: Antithrombotic Therapy andPrevention of
Thrombosis, 9th ed: American College of Chest Physicians
Evidence-Based Clinical PracticeGuidelines. Chest 2012
141:e419S.
4. den Exter PL, van Es J, Erkens PM, et al. Impact of delay in
clinical presentation on the diagnosticmanagement and prognosis of
patients with suspected pulmonary embolism. Am J Respir Crit Care
Med2013 187:1369.
5. Smith SB, Geske JB, Maguire JM, et al. Early anticoagulation
is associated with reduced mortality for acutepulmonary embolism.
Chest 2010 137:1382.
6. Segal JB, Streiff MB, Hofmann LV, et al. Management of venous
thromboembolism: a systematic review fora practice guideline. Ann
Intern Med 2007 146:211.
7. Kakkar VV, Hoppenstead DA, Fareed J, et al. Randomized trial
of different regimens of heparins and in vivothrombin generation in
acute deep vein thrombosis. Blood 2002 99:1965.
8. Lensing AW, Prins MH, Davidson BL, Hirsh J. Treatment of deep
venous thrombosis with low-molecular-weight heparins. A
meta-analysis. Arch Intern Med 1995 155:601.
9. Siragusa S, Cosmi B, Piovella F, et al. Low-molecular-weight
heparins and unfractionated heparin in thetreatment of patients
with acute venous thromboembolism: results of a meta-analysis. Am J
Med 1996
100:269.10. Dolovich LR, Ginsberg JS, Douketis JD, et al. A
meta-analysis comparing low-molecular-weight heparins
with unfractionated heparin in the treatment of venous
thromboembolism: examining some unansweredquestions regarding
location of treatment, product type, and dosing frequency. Arch
Intern Med 2000160:181.
11. Merli G, Spiro TE, Olsson CG, et al. Subcutaneous enoxaparin
once or twice daily compared withintravenous unfractionated heparin
for treatment of venous thromboembolic disease. Ann Intern Med
2001134:191.
12. Breddin HK, Hach-Wunderle V, Nakov R, et al. Effects of a
low-molecular-weight heparin on thrombusregression and recurrent
thromboembolism in patients with deep-vein thrombosis. N Engl J Med
2001344:626.
13. Gould MK, Dembitzer AD, Doyle RL, et al.
Low-molecular-weight heparins compared with unfractionatedheparin
for treatment of acute deep venous thrombosis. A meta-analysis of
randomized, controlled trials.Ann Intern Med 1999 130:800.
14. Prandoni P, Carnovali M, Marchiori A, Galilei Investigators.
Subcutaneous adjusted-dose unfractionatedheparin vs fixed-dose
low-molecular-weight heparin in the initial treatment of venous
thromboembolism. ArchIntern Med 2004 164:1077.
15. Erkens PM, Prins MH. Fixed dose subcutaneous low molecular
weight heparins versus adjusted doseunfractionated heparin for
venous thromboembolism. Cochrane Database Syst Rev 2010
:CD001100.
16. Faivre R, Neuhart Y, Kieffer Y, et al. [A new treatment of
deep venous thrombosis: low molecular weightheparin fractions.
Randomized study]. Presse Med 1988 17:197.
17. Lopaciuk S, Meissner AJ, Filipecki S, et al. Subcutaneous
low molecular weight heparin versussubcutaneous unfractionated
heparin in the treatment of deep vein thrombosis: a Polish
multicenter trial.Thromb Haemost 1992 68:14.
18. Kearon C, Ginsberg JS, Julian JA, et al. Comparison of
fixed-dose weight-adjusted unfractionated heparinand
low-molecular-weight heparin for acute treatment of venous
thromboembolism. JAMA 2006 296:935.
19. Castellucci LA, Cameron C, Le Gal G, et al. Clinical and
safety outcomes associated with treatment ofacute venous
thromboembolism: a systematic review and meta-analysis. JAMA 2014
312:1122.
20. Couturaud F, Julian JA, Kearon C. Low molecular weight
heparin administered once versus twice daily inpatients with venous
thromboembolism: a meta-analysis. Thromb Haemost 2001 86:980.
21. Bhutia S, Wong PF. Once versus twice daily low molecular
weight heparin for the initial treatment of venousthromboembolism.
Cochrane Database Syst Rev 2013 7:CD003074.
22. van Dongen CJ, MacGillavry MR, Prins MH. Once versus twice
daily LMWH for the initial treatment of
http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/22http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/21http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/20http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/19http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/18http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/17http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/16http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/15http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/14http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/13http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/12http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/11http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/10http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/9http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/8http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/7http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/6http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/5http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/4http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/3http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/2http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/1
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
12/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
12
venous thromboembolism. Cochrane Database Syst Rev 2005
:CD003074.
23. Charbonnier BA, Fiessinger JN, Banga JD, et al. Comparison
of a once daily with a twice dailysubcutaneous low molecular weight
heparin regimen in the treatment of deep vein thrombosis.
FRAXODIgroup. Thromb Haemost 1998 79:897.
24. Holmostrm M, Berglund MC, Granquist S, et al. Fragmin once
or twice daily subcutaneously in thetreatment of deep venous
thrombosis of the leg. Thromb Res 1992 67:49.
25. Siegbahn A, Y-Hassan S, Boberg J, et al. Subcutaneous
treatment of deep venous thrombosis with lowmolecular weight
heparin. A dose finding study with LMWH-Novo. Thromb Res 1989
55:767.
26. Linkins LA, Dans AL, Moores LK, et al. Treatment and
prevention of heparin-induced thrombocytopenia:Antithrombotic
Therapy and Prevention of Thrombosis, 9th ed: American College of
Chest PhysiciansEvidence-Based Clinical Practice Guidelines. Chest
2012 141:e495S.
27. Weitz JI. Low-molecular-weight heparins. N Engl J Med 1997
337:688.
28. Bller HR, Davidson BL, Decousus H, et al. Fondaparinux or
enoxaparin for the initial treatment ofsymptomatic deep venous
thrombosis: a randomized trial. Ann Intern Med 2004 140:867.
29. Leroyer C, Bressollette L, Oger E, et al. Early versus
delayed introduction of oral vitamin K antagonists incombination
with low-molecular-weight heparin in the treatment of deep vein
thrombosis. a randomizedclinical trial. The ANTENOX Study Group.
Haemostasis 1998 28:70.
30. Raschke RA, Reilly BM, Guidry JR, et al. The weight-based
heparin dosing nomogram compared with a"standard care" nomogram. A
randomized controlled trial. Ann Intern Med 1993 119:874.
31. Hull RD, Raskob GE, Rosenbloom D, et al. Optimal therapeutic
level of heparin therapy in patients withvenous thrombosis. Arch
Intern Med 1992 152:1589.
32. Fennerty AG, Thomas P, Backhouse G, et al. Audit of control
of heparin treatment. Br Med J (Clin Res Ed)1985 290:27.
33. Wheeler AP, Jaquiss RD, Newman JH. Physician practices in
the treatment of pulmonary embolism anddeep venous thrombosis. Arch
Intern Med 1988 148:1321.
34. Cruickshank MK, Levine MN, Hirsh J, et al. A standard
heparin nomogram for the management of heparintherapy. Arch Intern
Med 1991 151:333.
35. Hylek EM, Regan S, Henault LE, et al. Challenges to the
effective use of unfractionated heparin in thehospitalized
management of acute thrombosis. Arch Intern Med 2003 163:621.
36. Vardi M, Zittan E, Bitterman H. Subcutaneous unfractionated
heparin for the initial treatment of venousthromboembolism.
Cochrane Database Syst Rev 2009 :CD006771.
37. Holbrook A, Schulman S, Witt DM, et al. Evidence-based
management of anticoagulant therapy:Antithrombotic Therapy and
Prevention of Thrombosis, 9th ed: American College of Chest
PhysiciansEvidence-Based Clinical Practice Guidelines. Chest 2012
141:e152S.
38. Basu D, Gallus A, Hirsh J, Cade J. A prospective study of
the value of monitoring heparin treatment withthe activated partial
thromboplastin time. N Engl J Med 1972 287:324.
39. Hull RD, Raskob GE, Hirsh J, et al. Continuous intravenous
heparin compared with intermittentsubcutaneous heparin in the
initial treatment of proximal-vein thrombosis. N Engl J Med 1986
315:1109.
40. Brandjes DP, Heijboer H, Bller HR, et al. Acenocoumarol and
heparin compared with acenocoumarol alonein the initial treatment
of proximal-vein thrombosis. N Engl J Med 1992 327:1485.
41. Hull RD, Raskob GE, Brant RF, et al. The importance of
initial heparin treatment on long-term clinicaloutcomes of
antithrombotic therapy. The emerging theme of delayed recurrence.
Arch Intern Med 1997157:2317.
42. Hull RD, Raskob GE, Brant RF, et al. Relation between the
time to achieve the lower limit of the APTTtherapeutic range and
recurrent venous thromboembolism during heparin treatment for deep
vein thrombosis.
Arch Intern Med 1997 157:2562.
43. Hirsh J, Raschke R. Heparin and low-molecular-weight
heparin: the Seventh ACCP Conference onAntithrombotic and
Thrombolytic Therapy. Chest 2004 126:188S.
44. Garcia DA, Baglin TP, Weitz JI, et al. Parenteral
anticoagulants: Antithrombotic Therapy and Prevention ofThrombosis,
9th ed: American College of Chest Physicians Evidence-Based
Clinical Practice Guidelines.Chest 2012 141:e24S.
http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/44http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/43http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/42http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/41http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/40http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/39http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/38http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/37http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/36http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/35http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/34http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/33http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/32http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/31http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/30http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/29http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/28http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/27http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/26http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/25http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/24http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/23http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/22
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
13/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
13
45. EINSTEIN Investigators, Bauersachs R, Berkowitz SD, et al.
Oral rivaroxaban for symptomatic venousthromboembolism. N Engl J
Med 2010 363:2499.
46.Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the
treatment of acute venous thromboembolism. NEngl J Med 2013
369:799.
47. Hokusai-VTE Investigators, Bller HR, Dcousus H, et al.
Edoxaban versus warfarin for the treatment ofsymptomatic venous
thromboembolism. N Engl J Med 2013 369:1406.
48. Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus
warfarin in the treatment of acute venousthromboembolism. N Engl J
Med 2009 361:2342.
49. Gallus A, Jackaman J, Tillett J, et al. Safety and efficacy
of warfarin started early after submassive venousthrombosis or
pulmonary embolism. Lancet 1986 2:1293.
50.Ansell J, Hirsh J, Hylek E, et al. Pharmacology and
management of the vitamin K antagonists: AmericanCollege of Chest
Physicians Evidence-Based Clinical Practice Guidelines (8th
Edition). Chest 2008133:160S.
Topic 95336 Version 7.0
http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/50http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/49http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/48http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/47http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/46http://www.uptodate.com/contents/lower-extremity-deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days/abstract/45
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
14/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
14
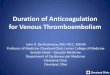
GRAPHICS
Risk factors for bleeding with anticoagulant therapy and
estimated
risk of major bleeding in low, moderate, and high risk
categories
Risk factors*
Age >65 years
Age >75 years
Previous bleeding
Cancer
Metastatic cancer
Renal failure
Liver failure
Thrombocytopenia
Previous stroke
Diabetes
Anemia
Antiplatelet therapy
Poor anticoagulant control
Comorbidity and reduced functional capacity
Recent surgery
Frequent falls
Alcohol abuse
Estimated absolute risk of major bleeding (%)
Categorization of
risk of bleeding
Low risk (0 risk
factors)
Moderate risk (1
risk factor)
High risk (2 risk
factors)
Anticoagulation 0 to 3 months
Baseline risk
(%)
0.6 1.2 4.8
Increased risk
(%)
1 2 8
Total risk (%) 1.6 3.2 12.8
Anticoagulation after first 3 months
Baseline risk
(%/years)
0.3 0.6 2.5
Increased risk
(%/years)
0.5 1 4
Total risk
(%/years)
0.8** 1.6** 6.5
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
15/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
15
* The increase in bleeding associated with a risk factor will
vary with (1) severity of the risk factor (eg,
location and extent of metastatic disease, platelet count), (2)
temporal relationships (eg, interval from
surgery or a previous bleeding episode), and (3) how effectively
a previous cause of bleeding was
corrected (eg, upper-GI bleeding).
Important for parenteral anticoagulation (eg, first 10 days),
but less important for long-term or
extended anticoagulation.
Although there is evidence that risk of bleeding increases with
the prevalence of risk factors, this
categorization scheme has not been validated. Furthermore, a
single risk factor, when severe, will resultin a high risk of
bleeding (eg, major surgery within the past two days, severe
thrombocytopenia).
Compared with low risk patients, moderate risk patients are
assumed to have a twofold risk and high
risk patients an eightfold risk of major bleeding.
The 1.6% corresponds to the average of major bleeding with
initial UFH or LMWH therapy followed by
VKA therapy. We estimated baseline risk by assuming a 2.6
relative risk of major bleeding with
anticoagulation (refer to footnote ).
Consistent with frequency of major bleeding observed by Hull et
al in high risk patients .
We estimate that anticoagulation is associated with a 2.6-fold
increase in major bleeding based on
comparison of extended anticoagulation with no extended
anticoagulation. The relative risk of major
bleeding during the first three months of therapy may be greater
than during extended VKA therapy
because (1) the intensity of anticoagulation with initial
parenteral therapy may be greater than with VKA
therapy (2) anticoagulant control will be less stable during the
first three months and (3)
predispositions to anticoagulant-induced bleeding may be
uncovered during the first three months of
therapy. However, studies of patients with acute coronary
syndromes do not suggest a 2.6 relative risk
of major bleeding with parenteral anticoagulation (eg, UFH or
LMWH) compared with control.
Our estimated baseline risk of major bleeding for low risk
patients (and adjusted up for moderate and
high risk groups as per footnote ).
** Consistent with frequency of major bleeding during
prospective studies of extended anticoagulation
for VTE.
Reference:
1. Hull RD, Raskob GE, Rosenbloom D, et al. Heparin for 5 days
as compared with 10 days in the
initial treatment of proximal venous thrombosis. N Engl J Med
1990 322:1260.
Reproduced from: Kearon C, Akl EA, Comerota AJ, et al.
Antithrombotic therapy for VTE disease:
Antithrombotic Therapy and Prevention of Thrombosis, 9th ed:
American College of Chest Physicians
Evidence-Based Clinical Practice Guidelines. Chest 2012
141:e419S. Table used with the permission of
Elsevier Inc. All rights reserved.
Graphic 97160 Version 2.0
[1]
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
16/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
16
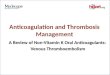
Suggested doses of low molecular weight heparins in obese
patients
VTE
treatment
Acute
coronary
syndromes
VTE
prophylaxis
Official
prescribing
information
on use in
obesepatients
Enoxaparin* Use standard
treatment dosing
(ie, 1 mg/kg every
12 hours based on
ABW).
In patients with a
BMI 40 kg/m , a
lower dose (ie,
0.74 mg/kg every
12 hours, based
on ABW), was
suggested in a
small case series
based on peak
anti-factor Xa
levels, but has not
been clinically
evaluated.
Once daily dosingregimens of
enoxaparin are
not
recommended.
Unstable angina
or non-STEMI:
Use standard
treatment dosing
(ie, 1 mg/kg every
12 hours based on
ABW) as
alternative to UFH
for patients not
undergoing an
early invasive
approach.
STEMI (for
patients not
managed with
PCI):
Age 50
kg/m : 60 mg
every 12 hours.
Marginal increase
observed in mean
anti-factor Xa
activity using
actual body weight
[ABW] and once
daily dosing in
healthy obese
persons (BMI 30to 48 kg/m )
compared with
non-obese
persons.
Dalteparin Approved by the Unstable angina BMI 30 to 39 Use
ABW-based
2
[1]
[2,3]
[2,3]
2
2
2
[4,5]
2
[5]
2
[3]
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
17/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
17
US FDA only for
extended
treatment of
cancer-associated
VTE. Use standard
treatment dosing
(ie, 200 units/kg
once daily based
on ABW for thefirst month,
followed by 150
units/kg once daily
for subsequent
months).
Consider using
100 units/kg
every 12 hours
based on ABW for
patients weighing
>100 kg.
or non-STEMI:
Use standard
treatment dosing
(ie, 120 units/kg
every 12 hours
based on ABW).
kg/m : Use
standard
prophylaxis dosing
(ie, 2500 or 5000
units once daily).
BMI 40
kg/m :
Empirically
increase standard
prophylaxis dose
by 30 percent (ie,
increase to 3250
or 6500 units
once daily).
dosing for patients
weighing up to 90
kg (acute coronary
syndromes) or 99
kg (cancer-
associated VTE).
Use a maximum
dose of 10,000
units per dose forpatients weighing
>90 kg (acute
coronary
syndromes) or
18,000 units per
day for patients
weighing >99 kg
(cancer-associated
VTE).
Tinzaparin
(not
available in
the United
States)
Use standard
treatment dosing
(ie, 175 units/kg
once daily based
on ABW).
Not indicated. BMI 30 to 39
kg/m : For
orthopedic surgery
use standard
prophylaxis dosing
(ie, 50 or 75 anti-
factor Xa units/kg
based on ABW
once daily) for
general surgery
use standard fixed
dosing (ie, 3500
anti-factor Xa
units once daily).
BMI 40
kg/m : For
orthopedic surgery
use standard
prophylaxis dosing
(ie, 50 or 75 anti-
factor Xa units/kg
based on ABW
once daily) for
general surgery
empirically
increase fixed dose
by 30 percent (ie,
increase to 4500
anti-factor Xa
Safety and efficacy
in patients
weighing >120 kg
has not been fully
determined.
Individualized
clinical and
laboratory
monitoring is
recommended
(Canada product
monograph).
[4]
2
2
[2]
[7]
2
2
[8]
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
18/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
18
units once
daily).
All doses shown are for patients with normal renal function and
are for subcutaneous
administration (except initial intravenous bolus of enoxaparin
for treatment of STEMI in
patients
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
19/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
19
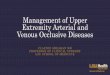
Suggested dose adjustments of low molecular weight heparins
in
renal insufficiency for adults
VTE treatment VTE prophylaxis*
Dalteparin Cl 30 mL/min : No adjustment
Cl 20 to 29 mL/min: Due to
variable response, adjust dose based
upon anti-factor Xa levels
Cl 20 mL/min: No adjustment
En oxaparin Cl 30 mL/min : No adjustment
Cl 20 to 29 mL/min: Reduce to 1
mg/kg once daily
Cl 30 mL/min: No adjustment
Cl 20 to 29 mL/min: Reduce to
30 mg once daily (medical or surgical
patients)
Nadroparin
(not available in
US)
Cl 50 mL/min: No adjustment
Cl 30 to 50 mL/min: Reduce dose
by 25 to 33 percent (optional)
Cl
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
20/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
20
(Garcia et al. Chest 2012 141:e24S)
Dosing suggested in prescribing information other approaches
including dose adjustment based on
anti-factor Xa activity are discussed in UpToDate topics on use
of LMW heparin.
Data from:
1. Dalteparin sodium injection. US FDA approved prescribing
information (revised January, 2015).
Available at
http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/020287s062lbl.pdf
2. Enoxaparin sodium injection. US FDA approved prescribing
information (revised October, 2013).
Available at: at:
http://www.accessdata.fda.gov/drugsatfda_docs/label/2013/020164s102lbl.pdf
3. Nadroparin calcium injection. Canada product monograph
(revised February, 2015). Available at
http://webprod5.hc-sc.gc.ca/dpd-bdpp/index-eng.jsp
4. Tinzaparin sodium injection. Canada product monograph
(revised May, 2014). Available at
http://webprod5.hc-sc.gc.ca/dpd-bdpp/index-eng.jsp
Graphic 90258 Version 3.0
http://webprod5.hc-sc.gc.ca/dpd-bdpp/index-eng.jsphttp://webprod5.hc-sc.gc.ca/dpd-bdpp/index-eng.jsphttp://www.accessdata.fda.gov/drugsatfda_docs/label/2013/020164s102lbl.pdfhttp://www.accessdata.fda.gov/drugsatfda_docs/label/2015/020287s062lbl.pdf
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
21/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
2
Example of a weight-based nomogram for intravenous
unfractionated heparin infusion for treatment of venous
thromboembolism and/or pulmonary embolism
Initial dose 80 units/kg bolus, then 18 units/kg per hour*
aPTT result Action Next aPTT
aPTT 3.0 x control)
Hold infusion 1 hour, then
decrease infusion rate by 3
units/kg per hour
6 hours
aPTT: activated partial thromboplastin time.
This table is provided as an example of a locally developed and
validated
unfractionated heparin weight-based dose adjustment nomogram. It
reflects the
original aPTT ranges, bolus sizes, and suggested changes in
infusion rate that were present at
the time the study was performed. The therapeutic ranges (ie,
relationship between the
aPTT and anti-factor Xa activity), initial and subsequent bolus
sizes, and sizes of the infusion
rate changes, as well as dosing differences depending on the
disorder under treatment (eg,
venous thromboembolism, stroke, acute coronary syndrome) should
be established separately
for each institution.
* Use of total body weight (TBW) is suggested for calculating
the initial bolus dose and infusion rate for
most obese patients. For additional information refer to
"Management of the critically ill obese patient",
section "Anticoagulants".
Therapeutic aPTT range of 46 to 70 seconds corresponded to
anti-Xa activity of 0.3 to 0.7 units/mL.
The target aPTT range in a particular institution should reflect
what is known about the local reagentsand equipment to perform the
assay .
The first aPTT should be obtained 4 to 6 hours after the initial
heparin bolus.
References:
1. Raschke RA, Reilly BM, Guidry JR, et al. The weight-based
heparin dosing nomogram compared
with a "standard care" nomogram. A randomized controlled trial.
Ann Intern Med 1993 119:874.
2. Garcia DA, Baglin TP, Weitz JI A, et al. Parenteral
Anticoagulants: Antithrombotic therapy and
Prevention of Thrombosis, American College of Chest Physicians
Evidence-Based Clinical Practice
Guidelines (9th Edition). Chest 2012 141:e24S-e43S.
Graphic 58483 Version 8.0
[1]
[2]
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
22/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
22
Example of a non-weight-based intravenous heparin protocol: Part
I
Initial intravenous heparin bolus: 5000 units.
Continuous intravenous heparin infusion: commence at 42 mL/hour
of 20,000 units (1680
units/hour) in 500 mL of two-thirds dextrose and one-third
saline (a 24-hour heparin dose of
40,320 units), except in the following patients, in whom heparin
infusion will be commenced at a
rate of 31 mL/hour (1240 units/hour) (ie, a 24-hour dose of
29,760 units).
Patients who have undergone surgery within the previous two
weeks.
Patients with a previous history of peptic ulcer disease,
gastrointestinal or genitourinary bleeding.
Patients with (thrombotic) stroke within the previous two
weeks.
Patients with a platelet count
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
23/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
23
Example of a non-weight-based intravenous heparin protocol:
Part
II titration based upon the activated partial thromboplastin
time
IV infusion
aPTT Rate change,
mL/hour*
Dose change,
units/24-hour Additional action
45 +6 +5760 Repeated aPTT in 4
to 6 hours
46 to 54 +3 +2880 Repeated aPTT in 4 to
6 hours
55 to 85 0 0 None
86 to 110 3 2880 Stop heparin sodium
treatment for 1 hour
repeated aPTT 4 to 6
hours after restarting
heparin treatment
>110 6 5760 Stop heparin
treatment for 1 hour
repeated aPTT 4 to 6
hours after restarting
heparin treatment
NOTE: This table reflects the original aPTT ranges, bolus sizes,
and suggested changes in
infusion rate that were present at the time this study was
performed. The therapeutic ranges
(ie, relationship between the aPTT and anti-factor Xa activity),
initial and subsequent bolus
sizes, and sizes of the infusion rate changes, as well as dosing
differences depending on thedisorder under treatment (eg, venous
thromboembolism, stroke, acute coronary syndrome)
should be established separately for each institution.
aPTT: activated partial thromboplastin time IV: intravenous.
* Heparin sodium concentration, 20,000 units in 500 mL = 40
units/mL.
With the use of Actin-FS thromboplastin reagent (Dade,
Mississauga, Ontario).
During the first 24 hours, repeated aPTT in 4 to 6 hours.
Thereafter, the aPTT will be determined once
daily, unless subtherapeutic.
Redrawn from: Hull RD, Raskob GE, Rosenbloom D, et al. Optimal
therapeutic level of heparin therapy in
patients with venous thrombosis. Arch Intern Med 1 992
152:1589.
Graphic 72792 Version 10.0
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
24/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
24
Pretest probability of deep vein thrombosis (Wells score)
Clinical feature Score
Active cancer (treatment ongoing or within the previous six
months or palliative) 1
Paralysis, paresis, or recent plaster immobilization of the
lower extremities 1
Recently bedridden for more than three days or major surgery,
within four weeks 1
Localized tenderness along the distribution of the deep venous
system 1
Entire leg swollen 1
Calf swelling by more than 3 cm when compared to the
asymptomatic leg (measured
below tibial tuberosity)
1
Pitting edema (greater in the symptomatic leg) 1
Collateral superficial veins (nonvaricose) 1
Alternative diagnosis as likely or more likely than that of deep
venous thrombosis -2
Score
High probability 3 or
greater
Moderate probability 1 or 2
Low probability 0 or less
Modification:
This clinical model has been modified to take one other clinical
feature into account: a previously
documented deep vein thrombosis (DVT) is given the score of 1.
Using this modified scoring
system, DVT is either likely or unlikely, as follows:DVT likely
2 or
greater
DVT unlikely 1 or less
Adapted from:
1. Wells PS, Anderson DR, Bormanis J, et al. Value of assessment
of pretest probability of deep-vein
thrombosis in clinical management. Lancet 1997 350:1795
2. Wells PS, Anderson,DR, Rodger M, et al. Evaluation of D-dimer
in the diagnosis of suspected deep-
vein thrombosis. N Engl J Med 2003 349:1227.
Graphic 75871 Version 2.0
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
25/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
25
Minimal requirements for early hospital discharge or
outpatient
therapy of venous thromboembolic disease
The responsible physician must ensure that all of the
following
conditions apply:
The patient is ambulatory and in stable condition, with normal
vital signs
There is a low a priori risk of bleeding in the patient
Severe renal insufficiency is not present
There is a practical system in place for the following:
Administration of LMW heparin and/or warfarin with appropriate
monitoring, and
Surveillance and treatment of recurrent VTE and bleeding
complications
VTE: venous thromboembolism LMW heparin: low molecular weight
heparin.
Adapted from Hyers, TM, Agnelli, G, Hu ll, RD, et al.
Antithrombotic therapy for venous thromboembolic
disease. Chest 2001 119:176S. (Sixth ACCP Consensus Conference
on Antithrombotic Therapy).
Graphic 70140 Version 2.0
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
26/28
3/6/2016 Lower extremity deep venous thrombosis: Initiation of
anticoagulation (first 10 days)
http://www.uptodate.com/contents/lower-extremity-
deep-venous-thrombosis-initiation-of-anticoagulation-first-10-days?topicKey=PULM%2F95336&elapsed
26
2012 ACCP recommended treatment of heparin-induced
thrombocytopenia (HIT)
The following non-heparin agents are recommended for use in
acute HIT whether or not
complicated by thrombosis: argatroban or danaparoid. Argatroban
is suggested over danaparoid
in those with renal insufficiency. (Editor's note: Lepirudin is
no longer available).
In pregnant patients with HIT, the use of danaparoid is
suggested over other non-heparin
anticoagulants. The use of fondaparinux is suggested only if
danaparoid is not available.
In patients with antibody-positive HIT who require urgent
cardiac surgery, the use of bivalirudin is
suggested over other non-heparin anticoagulants. In patients
with antibody-positive HIT who
require percutaneous coronary interventions, the use of
bivalirudin or argatroban is suggested over
other non-heparin anticoagulants.
Warfarin alone should not be used to treat HIT because of the
risk of causing venous limb
gangrene and/or skin necrosis.
Warfarin is safe to use when it is given to a patient adequately
and stably anticoagulated with a
drug that reduces thrombin generation (eg, danaparoid,
argatroban) it is prudent to delay use of
warfarin until the platelet count is >150,000/microL.
LMWH should not be given to patients with HIT, whether or not
complicated by thrombosis.
Prophylactic platelet transfusions should not be administered
for the treatment of patients with HIT
who do not have active bleeding.
ACCP: American College of Chest Physicians DVT: deep venous
thrombosis LMWH: low molecular weight
heparin.
Adapted from Linkins LA, et al. Treatment and prevention of
heparin-induced thrombocytopenia:
Antithrombotic therapy and prevention of thrombosis, 9th
edition: American College of Chest Physicians
Evidence-based clinical practice guidelines. Chest 2012
141:e495S.
Graphic 73727 Version 2.0
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
27/28
-
7/25/2019 Lower Extremity Deep Venous Thrombosis_ Initiation of
Anticoagulation (First 10 Days)
28/28