Embed Size (px)
Citation preview
Low Back Pain:Myths and Science
Robert Baldor, MD, FAAFP
Robert Baldor, MD, FAAFPProfessor and Vice Chair, Department of Family Medicine and Community Health/Director, Community-Based Education, Office of Undergraduate Medical Education/Director of Health Policy Education, Meyers Primary Care Institute/Medical Director, Center for Developmental Disabilities Evaluation and Research at the Eunice Kennedy Shriver Center, University of Massachusetts (UMass) Medical School, Worcester
Dr. Baldor has been teaching for 30 years and practices family medicine at the UMass Memorial Medical Center, Worcester. A member of the Massachusetts Governor’s Commission on Intellectual Disability, he has been recognized in The Best Doctors in America: Northeast Region and is a past-president of the Massachusetts Academy of Family Physicians. He publishes and presents regularly on a variety of family medicine topics and is an associate editor for The 5-Minute Clinical Consult. Dr. Baldor practices family medicine with a special interest in developmental and intellectual disabilities. Throughout the years, he has spoken on a variety of primary care topics at the AAFP's annual meeting.

LEARNING GOALS
1. Perform history and physical examination utilizing multidimensional pain, functional, psychological and opioid assessment tools to evaluate patients presenting with back pain. 2. Select appropriate diagnostic imaging tests, as necessary, for patients with back pain. 3. Identify red flags that indicate a need for immediate aggressive treatment or referral to a spine specialist, and coordinate referral and follow-up as necessary. 4. Develop collaborative care plans with appropriate pharmacologic, non-pharmacologic, or combination treatment plan for a patient with low back pain.
Low Back Pain…• Pain, muscle tension, or stiffness• Localized below the costal margin &
above the inferior gluteal folds• With or without sciatica/radicular
symptoms
Risk Factors for Developing LBP• Prolonged static posture including sitting• Heavy physical work• Frequent, repeated bending, twisting, lifting• Psychosocial risk factors
§ Anxiety, depression§ Mental stress at work
Epidemiology…• SECOND most common FM office complaint
§ 5th most common for all physician visits • First episode usually between ages 20-40• High recurrence rate
Symptoms, pathology and radiological images in LBP are POORLY correlated
An anatomical source of pain CANNOT be identified in 80-85% of people

Anatomical Considerations• Bones – Vertebrae, Joints• Muscles, Ligaments, & Tendons• Fascia, Connective Tissue• Spinal Cord & Nerve Roots• Discs• Mind-body Connection
Acute, Chronic & Non-specific LBP…
Acute: up to 6 weeks§ Early acute phase – acute LBP lasting < 2 weeks§ Late acute phase – acute LBP lasting 2 – 6 weeks
Subacute: 6 – 12 weeksChronic: > 12 weeks, cyclical, intermittent exacerbation
§ Significant enough to impact function or quality of life
Non-specific: Not attributable to recognizable pathology § No tumor, osteoporosis, arthritis, fracture, cord compression
LBP Etiology…
• Muscle Strain, Myositis
• Osteoarthritis/Facet Join Arthritis
• Compression Fractures
• Degenerative Disc Disease
• Spinal Stenosis
• Spondylolisthesis
• Spondylolysis
• Sacroiliac Joint Dysfunction/Pain
• Cancer/Neoplasms/Masses
• Infection (e.g., Epidural Abscess)
• Scoliosis
• Obesity
• Poor Posture
Non-back Origin (2%)• Pelvic organs: prostatitis, endometriosis, chronic PID• Renal disease: nephrolithiasis, pyelonephritis, perinephric abcess• Aortic aneurysm• GI disease: pancreatitis, cholecystitis, penetrating ulcer• Cardiac or pericardial disease• Pulmonary or pleural disease• Pregnancy
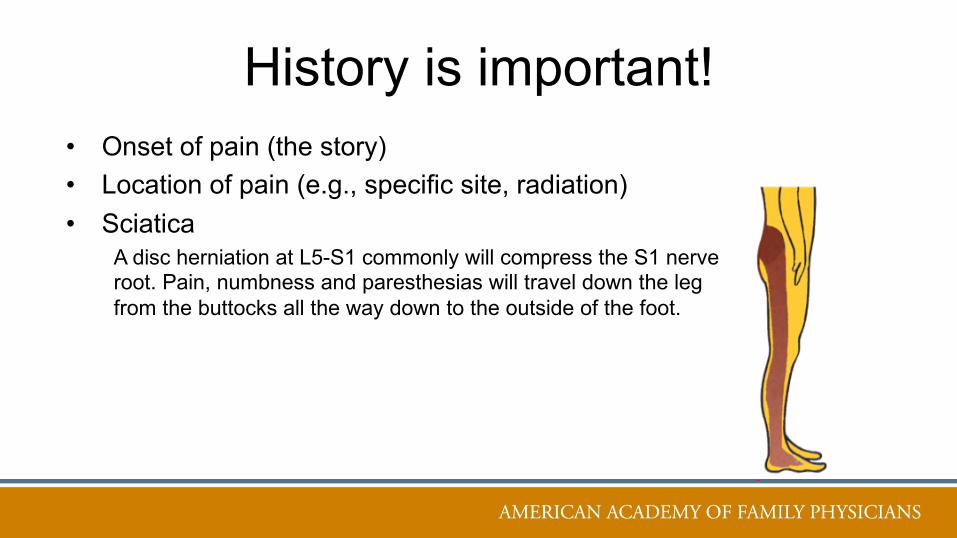
History is important!• Onset of pain (the story)• Location of pain (e.g., specific site, radiation)• Sciatica
A disc herniation at L5-S1 commonly will compress the S1 nerve root. Pain, numbness and paresthesias will travel down the leg from the buttocks all the way down to the outside of the foot.

History is important!• Onset of pain (the story)• Location of pain (e.g., specific site, radiation)• Quality, severity, timing (sharp/dull, numeric scale, etc.)• Aggravating & relieving factors; activities impaired
PEG Scale – fast & easyPain (how much?)Enjoyment (how little?)General Activity (how impacted?)

History is important!• Onset of pain (the story)• Location of pain (e.g., specific site, radiation)• Quality, severity, timing (sharp/dull, numeric scale, etc.)• Aggravating & relieving factors; activities impaired• Medical and social history: injuries, trauma, surgeries, tobacco use,
IVDA, malignancy, psychiatric disorders• “Red flags”
Red FlagsPotential indicators of serious spinal pathology
• Age of onset < 20 years or > 50 years• Severe or progressive neurologic deficits• History of malignancy• Fever or unexplained weight loss• Bladder of bowel dysfunction• Disturbed gait and saddle anesthesia
Cauda Equina SyndromePrevalence 1-3/ 100,000 population.
Signs/Symptoms• Urinary retention
– if no retention, the likelihood is < 1 in 10,000
• Fecal incontinence• Saddle anesthesia• Motor deficits at multiple levels
Physical examination…• Observation: posture, expressions, pain behavior• Full PE on initial evaluation
§ Focused PE subsequently• Neurologic evaluation on initial evaluation
§ Repeat each visit if radicular symptoms

Focused Back/Neuro Examination
• Observe: Stance and posture
• Gait and mobility: transitions between sitting, laying and standing
• Range of motion: flexion, extension, lateral flexion, axial rotation
• Palpation: localized tenderness, tightness, trigger points
§ Dermatomes …
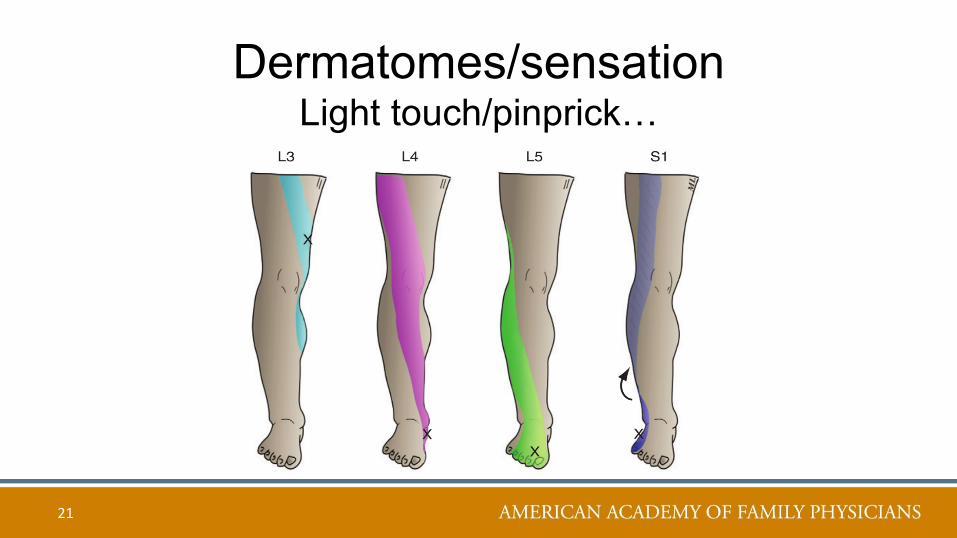
Dermatomes/sensationLight touch/pinprick…
21
Focused Back/Neuro Examination• Observe: Stance and posture• Gait and mobility: transitions between sitting, laying and standing• Range of motion: flexion, extension, lateral flexion, axial rotation• Palpation: localized tenderness, tightness, trigger points• Strength: stand on toes, heels, squat
Tip Toeing….The S1 nerve root exits L5-S1 disc space to innervate the gastroc-soleus group (calf muscles) • An L5-S1disc herniation can compress this root.• Patient will have difficulty walking on toes…
23
Foot Drop…• Inability to flex foot
“catching toe on carpet”• L4-5 nerve root (primarily L5)
§ Tibialis Anterior innervation• Difficult to walk on heels
24

SquatsL3 & 4 Nerve roots supply the Quadriceps• Difficult to do squats…
25
Focused Back/Neuro Examination• Observe: Stance and posture• Gait and mobility: transitions between sitting, laying and standing• Palpation: localized tenderness, tightness, trigger points• Range of motion: flexion, extension, lateral flexion, axial rotation• Strength: stand on toes, heels; ? Squat• Reflexes: knee, ankle

Knee (Patellar) jerk reflex: L3 & L4 nerve rootsAnkle (Achilles) jerk reflex: L5 & S1 nerve roots

Focused Back/Neuro Examination• Observe: Stance and posture• Gait and mobility: transitions between sitting, laying and standing• Palpation: localized tenderness, tightness, trigger points• Range of motion: flexion, extension, lateral flexion, axial rotation• Strength: stand on toes, heels; ? Squat• Reflexes: knee, ankle• Straight leg raise test: aka bilateral neural tension test
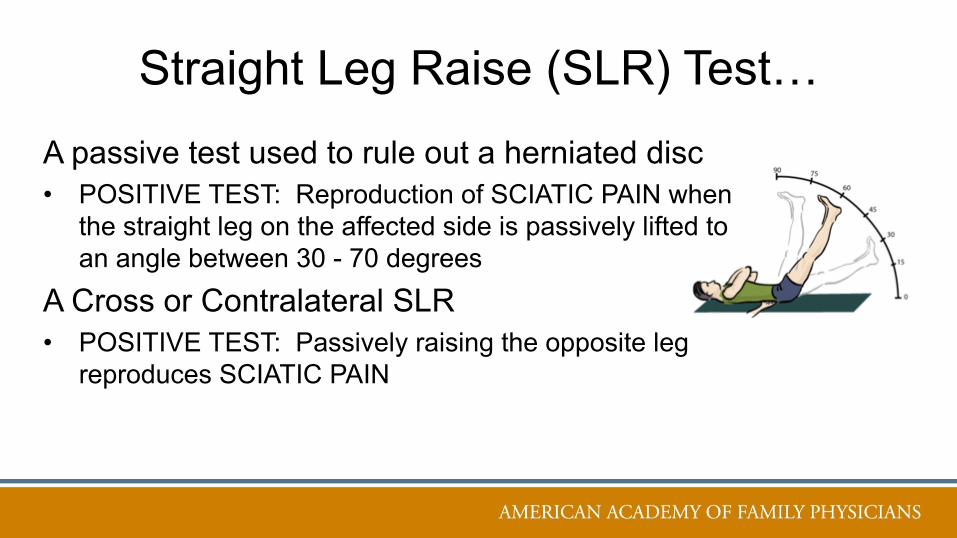
Straight Leg Raise (SLR) Test…A passive test used to rule out a herniated disc• POSITIVE TEST: Reproduction of SCIATIC PAIN when
the straight leg on the affected side is passively lifted to an angle between 30 - 70 degrees
A Cross or Contralateral SLR• POSITIVE TEST: Passively raising the opposite leg
reproduces SCIATIC PAIN
The differential is WIDE and COMPLEXCategorize Time
§ Acute§ Subacute§ Chronic
Classify the patient’s condition:§ Nonspecific Pain ?§ Radiculopathic pain or possibly related to spinal stenosis ?§ Pain from another specific cause ?
Spinal Stenosis ?Difficult to diagnose and treat …..
Symptoms: Numbness, weakness, cramping pain in legs, thighs or feet making ambulation difficult; radicular pain, abnormal bowel/bladder function, loss of sexual function, partial or complete leg paralysisRadiating leg pain: high quality studies show a trade-off between sensitivity & specificities, resulting in poor to modest likelihood ratios.Pain relieved by sitting: ranges from poor to high to predict stenosisDownhill treadmill testing: changing symptoms are associated with the highest positive likelihood ratios
Imaging????BOTTOM LINE: DO NOT obtain any imaging studies or diagnostic testing in patients with non-specific LBP
In patients with LBP that cannot be attributed to a specific disease or spinal abnormality following Hx & PE, imaging with plain radiography, CT scan, or MRI does not improve outcomes
(Strong recommendation, Moderate-quality evidence)
DO NOT ORDER imaging studies within 6 weeks UNLESS:
You performed a thorough physical exam and• There is concern for infection, fracture, cauda equina syndrome• The patient with radicular pain has Sx concerning for specific disc herniationDemonstrable leg weakness that is disabling or progressively worsening
Imaging is required before invasive intervention

Same for persistent LBP Imaging…• ONLY order an MRI (or CT) for CHRONIC LBP with
radiculopathy or possible spinal stenosis IF the patient is a potential candidate for surgery or epidural steroid injection
(strong recommendation, moderate-quality evidence)
Cancer???
Risk factors:
§ History of cancer with New onset LBP
§ Age > 50 years or older
§ Unexplained weight loss
§ Failure to improve after 4 – 6 weeks of conservative LBP therapy
If all 4 of these risk factors are absent, studies suggest that cancer can be ruled out with nearly 100% sensitivity
Spinal/Vertebral Infection?
Risk factors for possible spinal/vertebral infection:• Fever > 38°C (100.4°F) for > 48 hours• Intravenous drug use• Immunosuppression• History of tuberculosis or active tuberculosis
Other ConsiderationsVertebral compression fracture: § Risk Factors – osteoporosis, history of steroid use, ageAnkylosing Spondylitis: § Morning stiffness, improves with exercise, alternating buttock pain,
awakening due to BP during 2nd part of the night, younger ageUnrelenting night pain or pain at rest shows increased incidence of clinically significant pathology

Treatment Considerations..
38
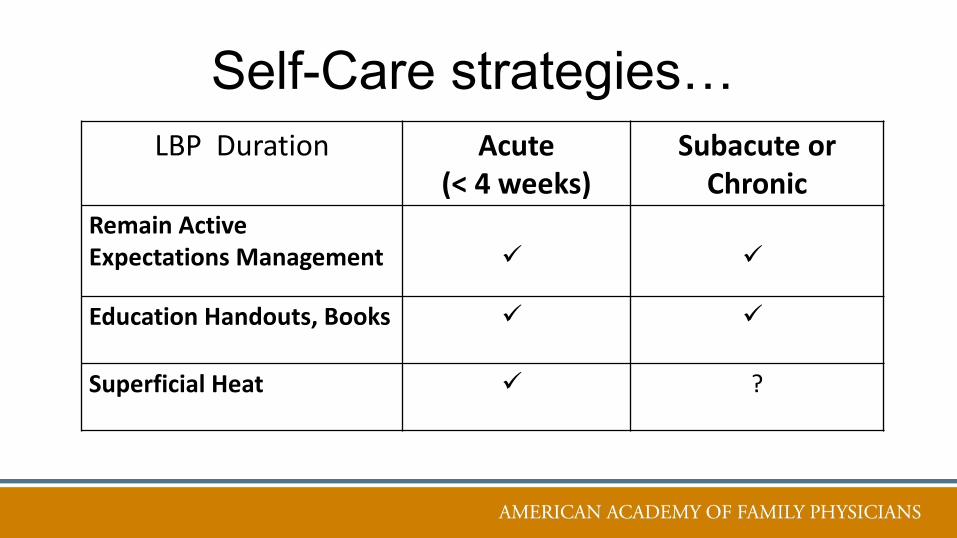
Self-Care strategies…LBP Duration Acute
(< 4 weeks)Subacute or
ChronicRemain ActiveExpectations Management ü ü
Education Handouts, Books ü ü
Superficial Heat ü ?
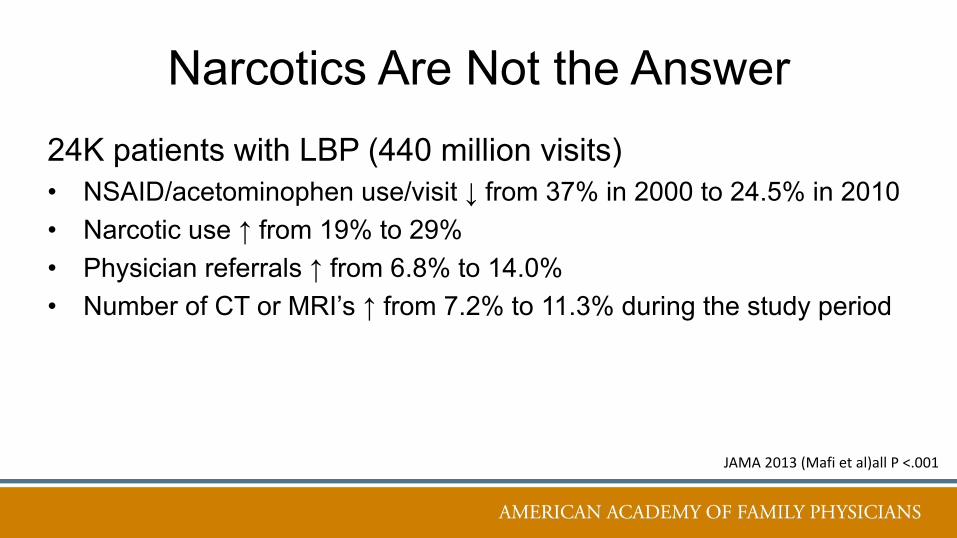
Narcotics Are Not the Answer24K patients with LBP (440 million visits)• NSAID/acetominophen use/visit ↓ from 37% in 2000 to 24.5% in 2010• Narcotic use ↑ from 19% to 29%• Physician referrals ↑ from 6.8% to 14.0% • Number of CT or MRI’s ↑ from 7.2% to 11.3% during the study period
JAMA 2013 (Mafi et al)all P <.001
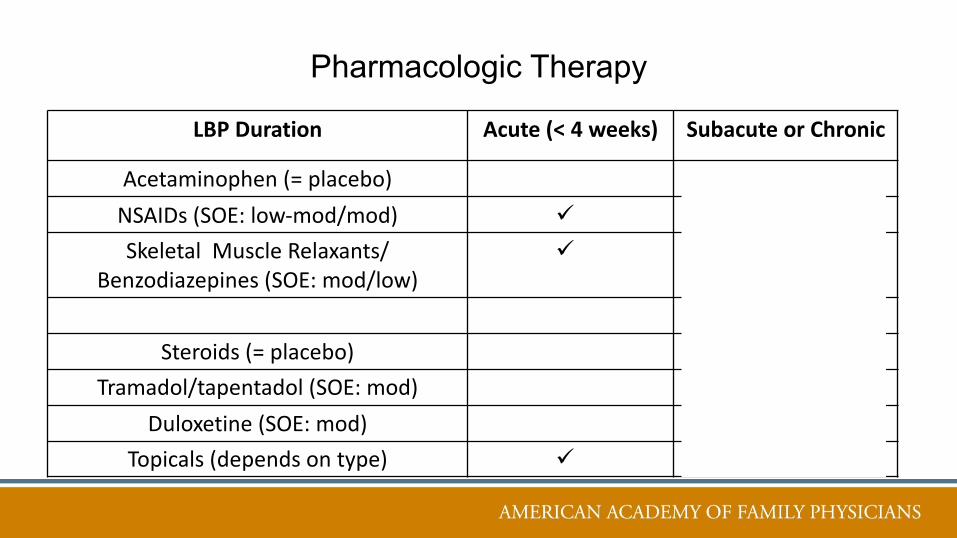
Pharmacologic Therapy
LBP Duration Acute (< 4 weeks) Subacute or Chronic
Acetaminophen (= placebo)NSAIDs (SOE: low-mod/mod) ü ü
Skeletal Muscle Relaxants/Benzodiazepines (SOE: mod/low)
ü ü
Steroids (= placebo)Tramadol/tapentadol (SOE: mod) ü
Duloxetine (SOE: mod) ü
Topicals (depends on type) ü ü
Other Medications…• Gabapentin, pregabalin• Topiramate• SSRIs, SNRIs, other antidepressants• Trazodone• TCAs• Lidocaine patches• Capsaicin• Other topicals – menthol/camphor agents; arnica; salves
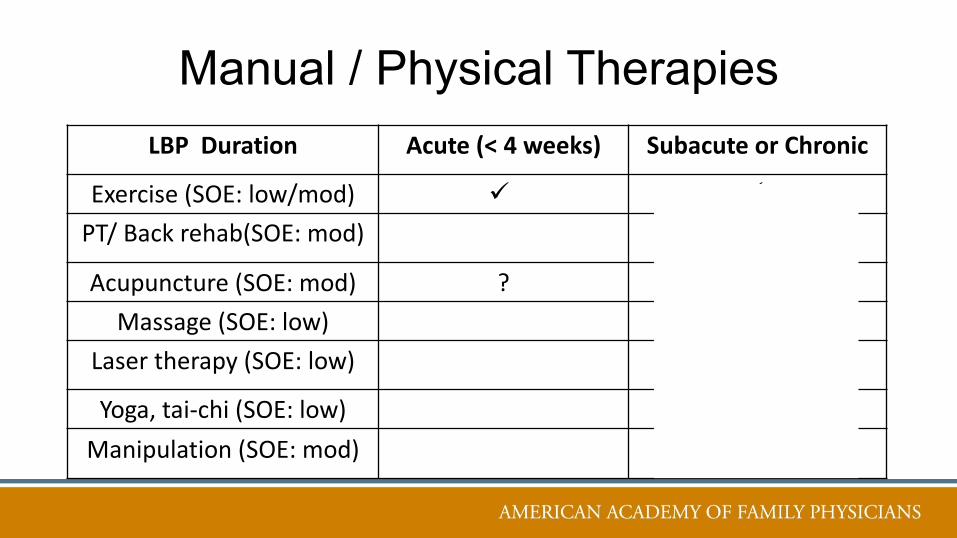
Manual / Physical TherapiesLBP Duration Acute (< 4 weeks) Subacute or Chronic
Exercise (SOE: low/mod) ü ü
PT/ Back rehab(SOE: mod) ü
Acupuncture (SOE: mod) ? ü
Massage (SOE: low) ü
Laser therapy (SOE: low) ü
Yoga, tai-chi (SOE: low) ü
Manipulation (SOE: mod) ü

Other Manual/Physical Therapies
• Myofascial techniques– Rolfing, Anatomy Trains, etc.
• Other approaches (cupping, gua sha, moxa)
• TENS, heat/cold/stretch
• Temperature treatments (short-wave, diathermy, US)
• Back schools• Tools such as acu-balls, foam rolling

Psycho-Behavioral Therapies• Cognitive Behavioral Therapy (CBT)• Acceptance and Commitment Therapy (ACT)• Mindfulness Based Stress Reduction (MBSR)• Meditation• Treat Mood/trauma issues• Address substances• Electromyographic Feedback/Biofeedback

ProceduresCan be done by the family physician
– Trigger point injections– Acupuncture
Others, done by specialists– Nerve blocks/Epidural steroid injections/pumps– Prolotherapy (5% dextrose)– Stimulators– Surgery
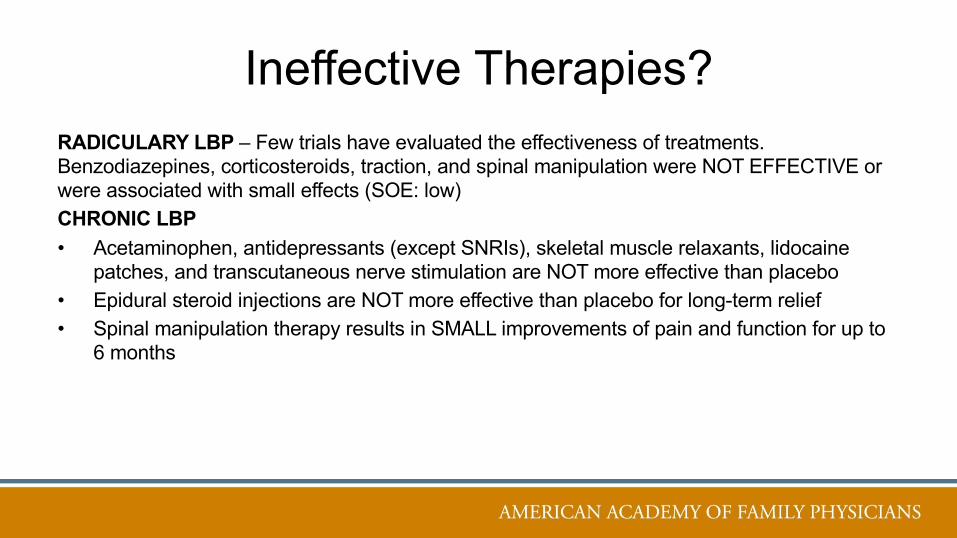
Ineffective Therapies?
RADICULARY LBP – Few trials have evaluated the effectiveness of treatments. Benzodiazepines, corticosteroids, traction, and spinal manipulation were NOT EFFECTIVE or were associated with small effects (SOE: low)
CHRONIC LBP• Acetaminophen, antidepressants (except SNRIs), skeletal muscle relaxants, lidocaine
patches, and transcutaneous nerve stimulation are NOT more effective than placebo
• Epidural steroid injections are NOT more effective than placebo for long-term relief
• Spinal manipulation therapy results in SMALL improvements of pain and function for up to 6 months
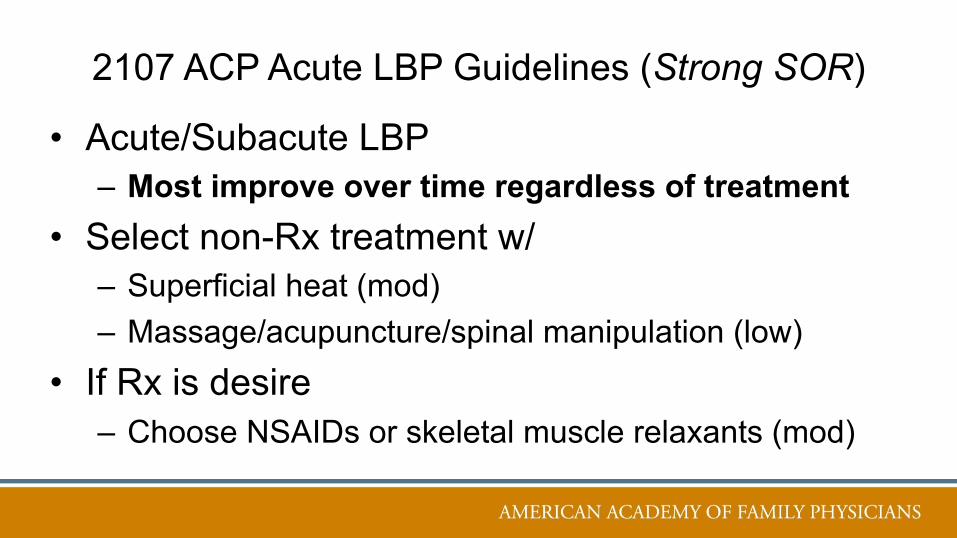
2107 ACP Acute LBP Guidelines (Strong SOR)
• Acute/Subacute LBP– Most improve over time regardless of treatment
• Select non-Rx treatment w/– Superficial heat (mod)– Massage/acupuncture/spinal manipulation (low)
• If Rx is desire– Choose NSAIDs or skeletal muscle relaxants (mod)
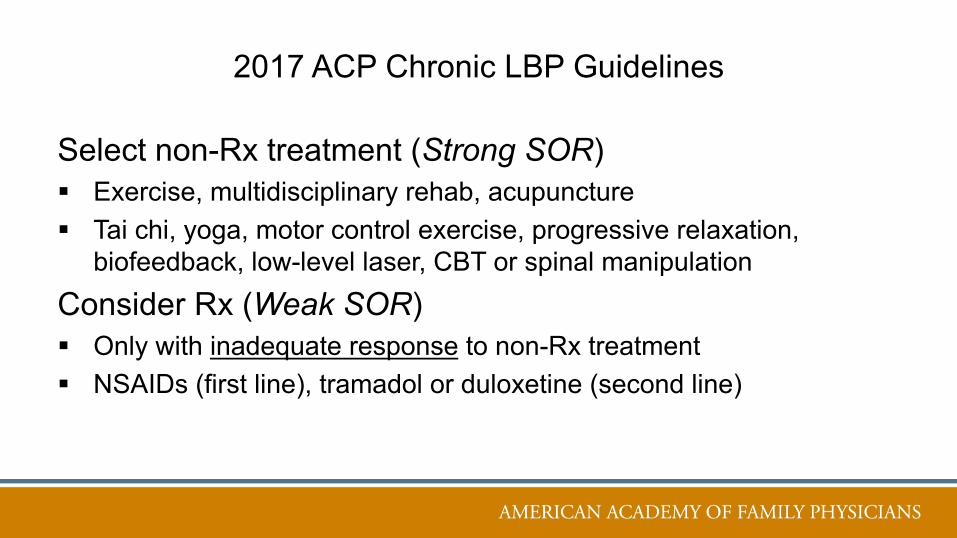
2017 ACP Chronic LBP Guidelines
Select non-Rx treatment (Strong SOR)§ Exercise, multidisciplinary rehab, acupuncture§ Tai chi, yoga, motor control exercise, progressive relaxation,
biofeedback, low-level laser, CBT or spinal manipulationConsider Rx (Weak SOR)§ Only with inadequate response to non-Rx treatment§ NSAIDs (first line), tramadol or duloxetine (second line)
Collaborative Care Pearls…
• Listen to the patient attentively
• Develop a trusting bond; who is the person behind the illness?
• Assess and manage patient’s expectations at every encounter
• Provide interventions in a step-wise fashion
• Every patient’s chemistry is different. Give the patient something that works
for him or her. If it is not working, stop it and try something else
• Treat depression and other mental illness actively
• See patient as often as they need you

Take Home – EBM Practice Changes• Perform a focused HX and PE to classify patients:
§ Non-specific pain§ Pain possibly associated with radiculopothy or spinal stenosis§ Due to another specific cause
• Order diagnostic imaging in patients with:§ Severe/progressive neurologic deficits§ HX/PE indicate severe underlying condition
• Provide patients with evidence-based info about their expected treatment course, advise them to remain active, give information about self-care options
References1. American Academy of Family Physicians (AAFP), American College of Physicians. LowBack Pain: Diagnosis and Treatment of Low Back Pain. Clinical Practice Guideline2017.2. Qaseem A, Wilt TJ, McLean RM, Forciea M, for the Clinical Guidelines Committee ofthe American College of P. Noninvasive treatments for acute, subacute, and chronic lowback pain: A clinical practice guideline from the American College of Physicians. Annalsof Internal Medicine. 2017;166(7):514-530.3. Shaughnessy AF. Opioid Analgesia Hard to Tolerate and Not Effective for Chronic LowBack Pain. American family physician. 2016;94(9):753-757.
52

























![Back Talk - Back Pain Rescue[1]](https://img.pdfslide.us/doc/110x75/577d35821a28ab3a6b90a19c/back-talk-back-pain-rescue1.jpg)


