Embed Size (px)
Citation preview

Love-ins,Lobsters &Racing CarsGreat living in late adulthood
RADICAL REDESIGN
RADICAL REDESIGN
RADICAL REDESIGN

1. Productivity Commission, 2011, Caring for Older Australians, Report No.
53, Final Inquiry Report, Canberra, p. 9.
2. McGrath, D. 2011, ‘Carer support is not only about Respite.’ Presentation
to Transforming Respite Summit, Morphettville, SA.
3. Commonwealth Department of Health and Ageing, 2003, Review of
Pricing Arrangements in Residential Aged Care, Canberra, p. 2.
4. Productivity Commission, 2011, Caring for Older Australians, Report No.
53, Final Inquiry Report, Canberra.
“Better advances would be nice”Technical innovations in science and medicine prolonging
life long ago outpaced social innovations in providing care.
We package care up into efficient bits and bobs - showering,
preparing meals, transport, and social contact - and try
to fulfil basic needs. Indeed, in the discussion about living
longer, we’ve focused mostly on who will do and pay for the
care, rather than on the meaning of care. Caring has come to
mean the provision of what is neccessary for wealfare and
maintenance. In this project we want to find ways to enable
care in the deeper sense - as an expression of interest,
concern and meaning.
“I don’t know what to do when I get older”What if we took the opportunity to reshape late adulthood and
redefined how systems, services, families and friends give
and get care? What if we saw late adulthood as a lifestage
as important and worthy of investment as childhood? What if
late adulthood wasn’t just about managing decline, but about
building capabilities and connections? What if we saw caring
as we saw parenting - an experience that’s tough, rewarding
and wholly transformative?
We want to rethink and reshape:
• Who cares - from a focus on individuals and services to
a focus on relationships and networks
• What care is for - from a focus on dependency and
fulfilling basic needs to a focus on interdependency and
living well
• How to do care - from doing things for the person being
cared for to maintaining and building capabilities and
connections.
It’s a good time to be thinking differently about the policy
and practice of care. In 2011, funding and administration of
aged care services in Australia moved from state to federal
government. The Productivity Commission released a weighty
report on the the financial future of aged care services.4 The
report talks a lot about increasing ‘consumer choice’ and
improving the ‘quality’ of care. Our work with people in the
cities of Salisbury and Unley, South Australia has given these
buzz words a richer definition.
Rather than start with statistics and numbers, this project
starts with people’s lived experiences and imagined futures.
In the pages that follow, we share people’s stories and ideas
for a new kinds of caring. Caring that moves beyond servicing
basic needs to enabling great living in late adulthood - be that
having love-ins, eating lobster, or racing cars.
Opening words
“I’ve outlived all my friends and enemies”At 86 and 91, Dudley and Daphne are living beyond the
average life expectancy. Over the last century, our life
expectancy has risen by 30 years - but, it’s not just years
we’ve added, it’s a whole new phase of life. There’s childhood,
adolescence, adulthood, late adulthood, and now, even
later adulthood.
“I suppose I could learn new things”If childhood is seen as a period of learning and growth, late
adulthood has typically been seen as a period of loss and
decline. In late adulthood, the independence we’ve gained as
adults can give way to the kind of dependency we experienced
as children. And yet our return to dependency in later life is
rarely coupled with a renewed focus on learning and growth.
“The girls come in to help for 30 minutes every morning”Just as ‘parenting’ supports children through dependency in
childhood, ‘caring’ supports older people with dependency in
older age. Once we turn 65, about a third of us will need care
to get by. And by the time, we hit our 80s, 86% of us will rely
on extra help and care, most provided by friends and family.1
“The kids can’t stand to be around sickness”
Giving that extra help and care isn’t easy. 2.6 million
Australians have a caring role - and a third of them are
severely depressed.2 Carers have worse health outcomes
than nearly any other group. Increasingly, we look to
professional carers to supplement, and in some cases, take
over caring roles. With more families living far apart, more
divorced and blended families, and more older people living
alone than ever before, demand for professional care is rising.
By 2042, aged care services are estimated to cost the state
106.8 billion dollars.3
Daphne
Dudley

How to read this report
Start wide
Focus in
Go wide again
Introduction: That’s where you are right now. It sets the big picture: What this project aims to achieve, who made it, what we stand for and how
we work.
Stories: We zoom in and profile a selection of ten of the 130 people in caring roles and relationships we met in
Salisbury and Unley, South Australia.
Patterns: After the profiles, we identify the reoccurring themes and answer the
questions: How do people in caring roles and relationships define great living?
Who is experiencing great living? What can we learn from these
positive examples that could be applied more broadly?
Opportunities: We set out 7 opportunities to enable more
people to experience great living.
Why Invest? Then, we look at the economic opportunities and moral imperative for pursuing
the 7 opportunities.
What’s next: The next phase of the project is to spend time co-designing with people, practioners and policymakers.
To move from conceptual opportunities to desirable solutions.
04 Working Backwards
05 Finding & meeting
06 Conversations & observations
08 The Salisbury & Unley 40
10 The eligibility lens
11 The connections lens
14 Barbara
16 Suzie
18 Thia, Mick & Soula
20 Dudley & Daphne
22 Leon
24 Mike & Liz
26 What is great living?
30 Great living behaviours
32 Moving towards great living
36 Opportunities for great living
39 Shaping minds
40 Rebalancing relationships
41 Activating family & friends 42 Starting relationships
43 (Re)Starting networks
44 Caring services
45 Diversify help networks
46 Economic opportunities
48 The moral imperative
52 Learning and working
53 The Working Backwards approach
54 Finding people
56 Talking with people
58 Service shadowing
60 Reflections from people we met
61 More about the people we met
66 Reflections from the team
68 International examples
72 What we read
74 Bibliography
76 Glossary
77 Contributors
79 We love feedback!
Introduction Stories Patterns Opportunities Why Invest?
Appendix

PAGE 5PAGE 4
We’re not a think tank and this report isn’t a provocative think
piece, it’s the first step in a year long process. We work with
people to co-design, prototype, and spread new solutions to
complex social challenges. We’re The Australian Centre for
Social Innovation’s Radical Redesign Team. We define solutions
as programs, platforms, networks, or principles that change
behaviours and shift outcomes. We believe the best solutions
come from people, and draw on their time, skills, experiences,
motivations, and aspirations. That’s why we Work Backwards
from people to policy. In 7 phases.
Projects begin by naming a tough social challenge, bringing
together governmental and non-governmental partners, and
assembling an interdisciplinary project team. We call this the
Get Ready phase.
This project began with the challenge: as our population
ages, how can we improve outcomes for older people in
caring roles and relationships? The project brings together
South Australia’s Office of the Ageing, the cities of Salisbury
and Unley, and two not-for-profit service providers - Helping
Hand Aged Care and ACH Group. Our project team includes a
secondee from the city of Salisbury, two interaction designers,
a graphic designer, an educator, a business analyst and a
community organiser.
In the Look and Listen phase, we spend time with people
to understand what a good outcome is, and the behaviours
that contribute to those outcomes. Our goal is to identify
opportunities for enabling more people to experience great
living. Over the past 2 months, we’ve spent time with 40
people in caring roles and relationships. Husbands, wives,
daughters, sons-in-law, grandchildren, and friends.
In the pages that follow we’ll share their stories, their versions
of great living, and what their day-to-day life actually looks
like. We’ll also introduce you to 7 opportunities for shifting
behaviours and enabling more people to experience great
living. In the Create phase we’ll go back out to people’s
kitchens and living rooms to build on the opportunity areas.
We’ll take our ideas out of the conceptual space and into the
tangible.
Working BackwardsWe’re a group of designers, social scientists, community developers and business analysts who co-design new solutions to tough social challenges.
In the Prototype Interactions phase, we’ll move from the
tangible to the practical - testing and iterating our ideas at a
small scale. In the Prototype Systems phase, we develop and
test out the back-end systems and procedures required to run
the emergent solutions. And we work with policymakers to
influence the broader policy context.
In the Value phase, we craft the business case and tell the
story of the solutions. In the Grow phase, we look to scale and
spread the solutions. Success for us are solutions that change
how people and systems behave, at scale.
This isn’t the first time we’ve Worked Backwards. In 2010, we
worked with 100 South Australian families to co-design a new
response to family stress called Family by Family. Now in
2012 Family by Family is now growing to two areas.
Introduction
New opportunties
Potential solutions
During the Look and Listen phase we searched for people on the streets of Unley and Salisbury, at supermarkets, in centres, cafes, libraries, and homes.
Finding & meeting
“Do you know of anyone who helps out or cares for a family
member, friend, or neighbour?” We met 130 people who cared
- through door knocking, at pharmacies, shopping centres and
supermarkets.
Most did not identify with the word ‘carer.’ Some wanted to
share the challenges - the anxiety, dependency, and sleep
deprivation. Others wanted to share the rewards - care as a
proud source of identity, a reinforcement of character, and a
continuation of family tradition.
We moved beyond street conversations to more in-depth
explorations with a 40 of these folks, stepping inside their
homes, accompanying them on errands and just hanging out
and observing. We spent time with people who were isolated
and alone, in close knit couples, with friends and in larger
networks.
Peoples’ experiences ran the full spectrum - from depression
and hand-to-mouth survival to optimism and thriving. We
developed tools to uncover hopes and fears. It was often
the little things (the photo on the mantle, the magnet on the
fridge, the book by the bedside) that revealed the most. That
dug beneath stoic facades, and unearthed worries about
death, forgotten ambitions, and dormant interests in activities
like cupcake decorating and bushwalking.
From top left: Door knocking, Parrahills Woolworths, Crossroads Woolworths, Goodwood Road, Jack Young Centre Salisbury

PAGE 7PAGE 6
Tea & Cake | First Visit Interaction
Topic Guide & Script - Caring Relationship
_________________________________________________________________
What are our opportunities?
RoutinesWe’re interested in people’s everyday routines and rituals
Stresses
Networks, Connections and Services
We’re interested in understanding the types of networks and services that people in caring
relationships rely on to make things work. Do friends provide more support than families? Do they
have a particularly strong neighbourhood network where everyone keeps an eye out for each
other - what are some of the interesting relationships?. Or do they not have a network at all, and is
this a good or bad thing? Exploring “happy” and “sad” networks will allow us to see how we can
build and support what already exists and also figure out how people who have no current
network can begin to build one around them. We want to understand what are the existing people
resources out there we might draw on, and what are some of the existing interaction out there we
might improve or build on.
Interests and Capabilities
We’re interested in discovering what people are interested in doing and where they get and
maintain motivation. We’re curious about why some people give up their interests, while others
keep going or building them. In particular we want to understand if there’s a gap between
people’s perception of their capabilities and the reality. We also want to map changing
capabilities, interests and ability levels over time to see patterns of change, and be able to
understand if people adjust their aspirations to match their perceived levels of capability. We are
thinking about capabilities in a broad sense - physical, mental, social and emotional capabilities.
We might hang solutions from here ...
Outlook and Aspirations
Understanding the gaps | discrepancies between ... | what is doing well for you?
We want to learn more about how people see themselves, how their outlook impacts their
wellbeing, what influences this, and what motivates them, what are people’s goals, aspirations or
versions of a good life, and how have they shifted or adapted over time. We also want to find out
what people want in their lives, their values, what they do well, and what’s missing.
Changes, Transitions and Directions
We’d like to understand the key moments when things change in people’s lives and the coping
strategies they have. What are the life skills and resources which help people reach the other
side? How do people plan, make decisions and learn from previous experience of pivotal times?
How do people change and adapt in altering circumstances? The event that preceded/caused
change is important but we are more interested in the journey through the period of change. Is
there something about people’s attitudes to change that influences how they deal with it? (fear,
excited apprehensive, wishing for change?) ... what happens at different life stages?
Things to think about BEFORE the meeting
IDentify lead person (drive structure of conversation and focus on carer)
ID support (focus on cared for and keep an eye on time)
Conversations & observationsWe developed a set of tools that helped guide and deepen our conversations and observations. We wanted to understand people’s day-to-day lives and what great living meant to them.
The starting point for our questions came from diving into the
literature and identifying frameworks we wanted to test and
explore. And because we start with people, we also drew on what
we learned whilst recruiting on the streets of Salisbury and Unley.
These insights informed our topic guides.
Over the course of a month we talked to people in a range of
ways and settings. Structured interviews in homes and cafes. Day
long ethnographies at the shops, at the caravan park or in front
of the TV. Sharing a cuppa, shortbread or lingering over Sunday
lunch.
We conducted structured interviews
using a detailed topic guide inspired by
research and recruitment conversations.
Visual tools made conversations about
big or abstract ideas- like great living
and outlook- richer and more concrete.
During ethnographies, we used a more
general topic guide that focussed on
observation of people, behaviour and
environment.
Introduction
Ethnography Tips
•What do they do?•When?
•Variety?
•Planning?
•Together/alone?•Decisions?
•Who’s around? •Groups? Neighbors? •Objects?
•Roles?
•Spirit of interactions?•Services?
•Media/calls/books
•What type of care?•Indep vs need help? •Roles?
•Spirit of give and take? •Communication?
•Money?
•Home environment? •Energy levels?•What energizes/drains?
•Language talking about past/present/future
•Goals? Wishes?•Carer/caree differences?
•Who or what brightens their day?
•What’s prioritized?•Emotions?
Note: Contradictions - Repetitions - Gaps - Hooks
PROBING THE LITERATURE
47% of people rely solely on their family
for day-to-day care5—care that is
valued at up to 40 billion dollars a year.6
Research told us that family plays a
critical role in caring situations, so we
focused part of our interviews on the
topic of family to find out more.
The absence of family stood out to us.
We expected geography to be a big
reason why families played a limited
role in peoples’ caring networks
and lives. Instead it was divorce,
fractured relationships, and complete
estrangement that weakened family
ties. Far from being a resource, family
was too often a deficit seen as being
past repair: “My children disowned me...
I haven’t seen my granddaughter for 11
years.”
EXPLORING EMOTIONS In interviews and ethnography we
weren’t only exploring what people did,
we were also listening for the outlook
and emotions behind what people did.
For example, fear.
Fear was an undercurrent in nearly
every conversation. People’s view of the
future was often clouded by a sense of
impending loss: loss of loved ones, loss
of brain power, loss of independence,
loss of control over how one died.
Ending up in a residential care facility
was uniformly frightening.
Fear manifested differently. For some it
led to denial and resignation. “I wouldn’t
want to even think about needing
more care.” For others, fear became
a motivator to live differently. “We’re
just going to have to start living in the
present. Now is as good a time as any.”
For others, fear was mere background
noise. Something that was there, but
didn’t need to be listened to or acted
upon.
IDENTIFYING STRATEGIES
Being in people’s homes and asking
open questions about lives, not just
services, enabled to us to uncover the
strategies people use day-to-day to get
to great living.
By hanging out, we learnt so much
about how people adapt to live well with
dependency. How to have a romantic
date in a hospital cubical. How to turn
meal services into a gastronomic
experience. How to volunteer from
home. How to fix trailers without being
able to see. How to make sex a daily
activity.
It’s unpacking these strategies and the
attitudes and perceptions behind them
that ultimately led us to identifying great
living and what it will take to get more
people on the track.
1. Productivity Commission, 2011, Caring for Older Australians, Report No.
53, Final Inquiry Report, Canberra, p. 9.
2. McGrath, D. 2011, ‘Carer support is not only about Respite.’ Presentation
to Transforming Respite Summit, Morphettville, SA.
3. Commonwealth Department of Health and Ageing, 2003, Review of

PAGE 9PAGE 8
The Salisbury & Unley 40
Introduction
Thanks to: Eleanor / Barbara / Soula, Mick and Thia / Muriel and Norm / Deirdre and Jean / Joan and Don / Dudley and Daphne
Lance and Meredith / Eddie and Pam / Eileen / Glad / Helen and Jayne / Bob and Jean / Julie / Karen and Lou
Leon / Manajeh / Eddy / Mike and Liz / Joyce / Beryl and Jon / Suzie

PAGE 11PAGE 10
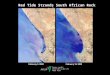
5 10 15 20 25 30
5 10 15 20 25 30 35 40
The eligibility lensMost ‘aged care’ services focus on individuals, determining eligibility by age, health and care needs.
LEVEL OF CARE
High Care
Mid Care
Low Care
= Struggling
= Getting by
= Great Living
AGE
THE 41 PEOPLE WE MET
THE 27 CARED FOR PEOPLE WE MET
Under 65
Carers
Over 65
Cared for
CULTURALLY & LINGUISTICALLY DIVERSE
CALD
Not CALD
TYPE OF SUPPORT
Managing Alone
Manages with Care
TYPE OF CARE
Mostly physical
Mostly cognitive
Mostly emotional
GENDER
Male
Female
Introduction
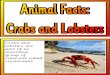
In their map we can see that Mick, Soula and Thia have limited support from their extended family, the broader community or from services.
In their map we can see Mike and Liz have multiple connections that all contribute strongly to great living.
The connections lensWe found it more instructive to look beyond the individual to who was around the individual. The type and quality of people’s connections told us more about great living than their age, health or care needs.
Fam
ily
Community
Services Fam
ily
Community
Services
Barbara Mick, Soula & Thia Mike & Liz
Fam
ily
Community
Services
In Barbara’s map we see family are only present at the network level and the only relationship she has is with services. Her limited connections weakly contribute to great living.
Knowing Liz needs help to dress and
remember faces doesn’t tell us why she
is living well.
Knowing Barbara has physical needs
doesn’t tell us how engaged members
of her family are in her day-to-day life.
Knowing Mick and Soula are classified
as CALD isn’t as telling as the fact they
manage care for Thia alone.
The ‘Connections Map’ used in this report shows the makeup
of an individual’s connections and how strongly they contribute
to great living:
Familyconnections
Communityconnections
Strong
Servicesconnections
Weak None
Reationships level connections
Network level connections
You can read more about how we define great living in ‘Patterns’ p. 26-35.
Barbara Thia LizMick
& S
oula
Mik
e

PAGE 13PAGE 12Stories:10 people we met
Suzie
Barbara
Leon
Thank you to our wonderful collaborators - Leon, Mike & Liz, Suzie, Mick, Soula, Thia, Dudley, Daphne and Barbara - who gave their time and permission for us to share their stories with you.
Mick, Soula & Thia
Dudley & Daphne
Mike & Liz

PAGE 15PAGE 14 Stories
A BIT ABOUT HERBarbara is a proud Scot living in Salisbury. She celebrates
Burns Night every year with a Tartan display in her backyard
and dreams of the rolling hills of St. Andrews.
She’s 75 years old and lives in a one-bedroom council flat
with her two pet budgies. Barbara suffers from lung cancer
but smokes half a pack a day: “The more I worry, the more
I smoke. I’d rather spend money on food, but I’m buying my
cigarettes. If I cannae sleep during the night, I smoke.” She has
diabetes, but still loves her ginger beer and short bread.
She moved to Australia 30 years ago with her husband “for a
fresh start” after he had several affairs. This didn’t work out,
and they separated a decade ago. Since then, her husband
died and her kids haven’t been in contact with her.
On days she’s well enough to get out of bed she cooks, reads
fiction books or calls relatives in Scotland. Her nephew, a
cab driver, stops by some days for a cigarette. Other than
the cleaner from the state provided Domiciliary Care, her
neighbour Diana is her only regular contact every few days.
HOW SHE SAYS SHE’S DOINGBarbara lives from one pension day to the next. Her health
is deteriorating with heart, lung and stomach conditions. She
says she can’t quit some of her habits - smoking and eating
sweets daily with diabetes. Her health also fluctuates a lot -
from being up and full of energy to bed bound within an hour.
She needs pain killers, insulin and 10 different tablets each
morning. Despite this, she likes a good laugh.
WHAT GREAT LIVING LOOKS LIKEBarbara says she’d like to re-establish connections with her
children, who she hasn’t seen since her divorce 10 years ago,
but that this is hard: “My children disowned me... I haven’t seen
my grand daughter for 11 years.” She’d also like to be more
mobile and meet new people.
She gets pleasure from talking and sharing memories with
others over the phone, like her cousin Rosy in Scotland. She
likes baking shortbread and other treats to share with people.
At the shops she bought small gifts for the children of people
who visit her, even though finances are tight. She cancelled
seeing anyone at Christmas, as she’s ashamed she can’t
afford gifts.
HER DAY TO DAYBarbara spends most of her days at home except for the
shopping trip for groceries with neighbour Diana or for
doctor’s appointments. She sometimes walks over to Diana’s
for a chat or to give Diana cooked chicken bones for her dog.
Other days she leaves the flat only to water the garden or
check the mail box.
If she is well enough to sit up in bed, or be in her living room,
she reads novels for a short while until her eyes need a break.
She also spends time with her budgies teaching them new
cheeky words.
Her cleaner comes every fortnight. Barbara enjoys the
short chats they have. She thinks the cleaner could be more
thorough though: “She spends time cleaning where it’s already
clean, like in the bathroom, and cleans the kitchen floor with
water, not detergent.”
Barbara gets frozen meals delivered from the City of
Salisbury’s Jack Young Centre every second Monday. She has
a chat with staff at the centre to order the meals and reheats
them in her kitchen at lunch time. Barbara goes shopping with
her neighbour Diana about once every fortnight. In return she
cooks chicken bones for Diana’s dog.
Barbara“It’s not a life this, it’s not a life. I thinks that’s why I shut people out.”
CONNECTIONS MAP
Fam
ily
Community
Getting by Great Living
Services
Network R.ship
Barbara

PAGE 17PAGE 16 Stories
A BIT ABOUT HERSuzie is not quite sure how old she is. She thinks she’s 52.
She is a member of the Stolen Generation and doesn’t have
contact with her biological family. Her adoptive mother lives
in a nursing home. At the moment she doesn’t see a lot of her
because of a train line upgrade.
In 2002, Suzie underwent brain surgery to remove a
tumour, leaving her with severe disabilities. She talks
about experiencing paranoia, hallucinations and periods of
depression. Left blind in one eye and deaf in one ear, she
walks with a limp and tires easily. When she’s tired everything
gets hard: moving, talking, thinking.
Prior to her tumour Suzie worked out bush, cooking in
roadhouses. She went caving, played computer games and
enjoyed photography and painting. Nowadays Suzie spends
a lot of time alone watching horror movies, reading and
drinking. She volunteers a few times a week at an Indigenous
arts centre, and has a cleaner and a care worker.
HOW SHE SAYS SHE’S DOINGWhen we asked if there were any points in her week where
she would like things to be different Suzie replied, “Yeah, all
of it.” Since her brain injury Suzie has had a found it tough to
keep doing the activities she loves. For example, she used to
spend a lot of time in the bush and doing outdoor activities;
this has been replaced by watching movies. She says not
being able to go out bushwalking “scares the hell out of [me].”
Suzie wants to keep learning and developing her skills. She
says, “The day you stop learning is the day you die.” Suzie tells
us she has a history of drinking, and last weekend she drank
half a bottle of scotch on her own. While she likes time alone,
a magnet on her fridge reads, “I cannot be lonely if I like the
person I’m alone with”. She takes medication for depression,
but says the “depression tablets aren’t working... I’ve been on
them for 7 years and that’s a long time to be on one tablet. I
have to be on them for the rest of my life”.
WHAT GOOD LIVING LOOKS LIKESuzie is not really happy with how things are going in her
life; she is not doing many of the activities she enjoys. Her
networks are limited and are mainly service providers. She
tells us that she wants to be able to do things on her own:
“I’ve always been independent; I want to stay as long as I
can.” Good food is important to Suzie: “My perfect meal is
lobster. I have had kangaroo. I have had shark. Being out in
the bush, I’ve had abalone.” Now her staple is tinned tuna and
mayonnaise bought every two weeks at Woolies. She has
started acupuncture treatment to help her stop smoking and
drinking.
HER DAY TO DAYAs well as time alone at home, Suzie works as a volunteer at
a local Indigenous art centre where she answers the phones
and does general office work. Suzie has met some friends
there. Occasionally she has lunch at the City of Salisbury’s
Jack Young Centre but usually only when her carer comes
along. She says: “I don’t go much - I should go more often.”
Suzie’s basic needs are mostly provided for through
professional care services. A carer visits for two hours a week
to help with shopping and organising doctors appointments.
Suzie trusts her because “she knows when I start getting
stressed - and I do get stressed.” She also has a cleaner that
comes fortnightly.
Suzie“A lot goes on in your head when you go through something traumatic” Getting by Great Living
Fam
ily
Community
Services
Network R.ship
Suzie
CONNECTIONS MAP

PAGE 19PAGE 18 Stories
A BIT ABOUT THEMSoula and husband Mick care for Soula’s mother Thia (90),
who lives with them. Thia was born in Greece, and Greek
culture remains a pillar of the family’s day-to-day life. She
speaks little english. Soula and Mick have 3 kids who they
see for lunch on the weekends. Their fourth daughter lives
in Greece with their only grandson. They have never been to
Greece themselves.
Mick had a workplace accident in the late 80’s, and hasn’t
been able to work since. Soula works full time at a call
centre. She sees looking after her mum as her responsibility:
“If I don’t do it, who will? She’s my mother.” Mick and Soula
live on Soula’s wage and Mick’s disability pension. They cook
for Thia, take her to medical appointments, help her take a
bathe and try not to ever leave her alone, “even to go to the
shops.”
HOW THEY SAY THEY’RE DOINGMick and Soula are doing their best to make things work,
balancing the care of Thia between them. They’ve adapted
to Thia’s changing needs by bringing her to live with them
after her husband passed away. They don’t get any support
in looking after Thia: their children drop in for a meal, but
aren’t involved in Thia’s care. They tried using a Greek respite
service, but Thia didn’t like being left with people she didn’t
know. During the week, Mick and Thia don’t leave the house
because Thia finds it hard to get around. Mick and Soula don’t
have much time for themselves, but feel “There’s nothing we
can do, we’re just going down the direction with her now.”
WHAT GOOD LIVING LOOKS LIKEWhen we asked Mick and Soula about what they’d like to
be doing more of, they said they’d love to have some time
alone as a couple. The last holiday they had was four years
ago, and they’ve given up their weekly trips to the movies
together so Thia isn’t left alone. Spending time with their
extended family is something they used to do more of, but
it’s dropped off since they’ve been caring for Thia.
Mick would like to be in better health. Soula tells us that she
worries: “What if Mick gets sick and I have to stop and look
after them both?” Mick would like to feel like he did when he
was working; he says that back then he was his “own man”.
Now he asks himself: “What would I be doing if I wasn’t
looking after the old girl?” Via a translator Thia told us good
living for her means, “Being with my kids and being looked
after. And doing whatever they do.”
THEIR DAY TO DAYThere is a gap between Mick, Soula and Thia’s current
behaviours and their aspirations. Mick cares for Thia during
work hours Monday to Friday. They mainly watch television -
watching the wrestling together is their favourite - and Mick
prepares Greek food or looks after his fruit trees. Mick and
Thia often share a laugh about their small dog who likes to sit
on Thia’s lap.
When she gets home from work, Soula takes over looking
after Thia. Mick then generally eats dinner and spends the
evening in another room. Soula also looks after Thia on the
weekends, while Mick and his son “go for a long drive or to
Harvey Norman.” On Saturdays, Soula and her Mum spend
the day at Thia’s old house in inner city Adelaide. During the
week, Thia’s house isn’t used. Soula tells us that one of Thia’s
childhood friends “lives a street away but they never see each
other” as it’s hard for Thia to climb stairs.
Soula, Mick & Thia“If I don’t do it, who will? She’s my mother.” Getting by Great Living
Fam
ily
Community
Services
Network R.ship
ThiaMick
&
Soul
a
CONNECTIONS MAP

PAGE 21PAGE 20 Stories
A BIT ABOUT THEMDudley and Daphne have been together for over 70 years.
They met in the final year of high school and worked together
for many years in rural South Australia, doing everything
together, from wood cutting to mechanics.
Dudley and Daphne have led very active lives. Just 10 years
ago, Dudley was famed internationally as Australia’s oldest
racing car driver, and Daphne was his one woman pit crew for
over 50 years at races across the country. Now Daphne finds it
hard to even get around in the house because of chronic pains
in her lower abdomen and knee surgery prevents her from
walking far. Dudley had open heart surgery three years ago
and feels like he’s lost all his energy. Dudley plays a big part
in looking after Daphne, and says he’s a “bloody doctor... I test
her blood pressure, give her shots.”
They used to like to hit the road and travel across Australia
together. Now Daphne doesn’t make any plans since she
“doesn’t know if [she]’ll be dead tomorrow.” Some days Dudley
tells us he wishes his wife would “die to put her out of her
misery”. His biggest fear is dying first.
HOW THEY SAY THEY’RE DOINGWhilst Dudley and Daphne’s basic needs are being met with
Dudley’s support and formal services, there are still lots of
things they’d like more of in their lives. Their support network
is getting smaller: “We’ve outlived our friends and enemies”.
They have 3 children living close by, but they don’t see them
much. They’d like to have more fun, and not let their health
limit their enjoyment of life. It’s been hard for them to pursue
their interests—like car racing—given their current situation.
WHAT GOOD LIVING LOOKS LIKEDudley would like to have more energy to do things. He tells
us: “I want to get around again.” Dudley liked being recognised
as an expert in his motor racing days ( “They called me the
Legend, Deadly Dud”), and would like a chance to share his
skills again. Daphne would like to do and learn more: “I used
to do cake decorating, I am still interested.” She says that when
volunteers from the local community centre drop by, she’d like
it if they did activities together, but “they just sit and talk.”
As a couple, there are also lots of things Dudley and Daphne
would like more of. When talking about intimacy they say,
“Sex. Let’s just say we’d like it.” Both Dudley and Daphne
talk about wanting to meet people to share intelligent
conversation, new experiences, and to have a good laugh
with. They’d like to see more of their children, but tell us
that their kids “can’t stand sickness.” Daphne tells us “being
respected would sure be nice. But you can’t be respected if
you can’t enjoy life.”
THEIR DAY TO DAYA care worker, provided by a not-for-profit service provider,
comes in every morning to shower Daphne and help her get
dressed. Dudley gives Daphne her medication and morphine
shots throughout the day. She spends most of the day in the
living room, but doesn’t watch TV as “there’s not much on.”
Sometimes a care worker pops by in the afternoon to spend
an hour with Daphne, but she says, “there’s nothing to talk
about.” Their grandson pops in every afternoon—they pay him
$100 a week to provide them with meals.
Dudley is still an avid driver (he owns three cars), yet they go
few places. Once a week or so, they go the community centre
for a meal but Dudley complains that “there’s no intelligent
conversation there, no laughter.”
Dudley & Daphne“I want to get around again”
Getting by Great Living
DaphneDud
ley
Fam
ily
Community
Services
Network R.ship
CONNECTIONS MAP

PAGE 23PAGE 22 Stories
A BIT ABOUT HIMLeon is the kind of man you would turn to if you needed help.
Ask him a question or where to find something and he’ll offer
to “put [his] feelers out.” He has lived alone in a SA Housing
Trust house in Salisbury North since his wife died from
cancer in 2006. When this happened, Leon went into a deep
depression and his eyesight deteriorated rapidly. He now only
sees light and dark, and is effectively blind.
Leon is a joker, and has a broad network of people with whom
he can share a laugh. He keeps in contact with people over
the phone, catches up with them at social gatherings, and
over mutual interests like fixing trailers in his workshop and
sourcing bits and pieces for people’s homes.
HOW HE SAYS HE’S DOINGAs a friend to many, Leon fixes trailers and repairs things for
people he knows. He describes his home as a “distribution
centre.” His network has grown since his wife passed
away, taking part in events at the Country Music Club and
in the Gawler Low Vision Support Group. Leon has several
people on speed dial who he calls daily. He is close with his
neighbour, and goes next door every morning for “comedy
hour” and shared banter. He says “I can’t complain at all—I’ve
got friends I can share a laugh with.” His motto is “caring and
sharing” and says “I scratch your back, you scratch mine.”
He uses his talents of sourcing and fixing things for people
and they help him in return with meals and lifts. He has
adapted his interests and skills to his sight loss, and makes
use of both formal services and his own network of friends.
WHAT GOOD LIVING LOOKS LIKE“I hope one day she’ll park her shoes under my bed”. Leon
tells us he’s recently met a woman, but is taking things slowly.
Being independent is important to Leon: “I don’t want to be
a burden to anyone.” Leon places items in his house, like his
kitchen wares and tools in exactly the same spot so he is able
to manage his day-to-day activities himself. Sharing stories
with friends is really important to Leon, and he is a colourful
story teller. He had a son with his first wife, who now only
occasionally comes around, but Leon doesn’t dwell so much
on people missing from his life.
HIS DAY TO DAYLeon keeps very busy. When we spent time with him, trailers
of different sizes were parked on the front lawn along with a
wide variety of scrap metals, wood and even an old washing
machine for his fixing, sourcing and making projects.
He is also busy thinking up and preparing pranks for the next
time he sees a particular friend. Things like a collection of
paddle pop sticks for the one friend who believes he’s up “shit
creek without a paddle”, or sourcing a box of vegemite chips
to give the committee members at the country music club a
very special Aussie Christmas—tongue firmly in cheek.
Leon receives food from the City of Salisbury’s Jack Young
Centre meal service topped up by meals that friends bring
him. A cleaner from Community Support Inc. also comes by
once a fortnight.
Neighbours drop by each day to catch up with groceries in
tow, to share the latest stories, or just to fix together that
barbeque. Friends come over to stay at his place or take Leon
to theirs for a day or the weekend.
When asked how he does all of this minus his eye sight, he
shrugs and says: “You can do anything you want, you’re only
limited by your own imagination. You need to broaden your
outlook on life.”
Leon‘Great friends and company around me, I can’t complain at all” Getting by Great Living
Fam
ily
Community
Services
Network R.ship
Leon
CONNECTIONS MAP

PAGE 25PAGE 24 Stories
Mike & Liz
A BIT ABOUT THEMMike and Liz met 23 years ago and have been inseparable
since. Together, they’ve enjoyed adventures like scuba diving,
flying planes and travel to the more personal: celebrating the
birth of grand children, renovating and gardening.
Theirs is a home with systems in place - a notice board
bursting with photos to aide memory, and space for Liz’s
wheelchair - a result of her 31 years with multiple sclerosis.
They tackle the progressive decline in capabilities MS brings
using some effective strategies.
Tricks like pooling strengths to work together, where Liz is
the planner, and Mike makes it happen. It’s also important to
them to find ways to give back: getting to know neighbours,
volunteering, and even setting up a community bank.
HOW THEY SAY THEY’RE DOINGDespite tough times (losing family, Mike’s cancer, Liz’s near
death), they describe themselves as “glass half full people”
and much of their focus is geared towards the brighter side
of life - appreciating the time they are together, doing things
that challenge them, and building new friendships. A weekly
highlight is rehearsing with the recently formed caring choir,
where they find “bonds of affection and mutual support.”
They’ve learnt to navigate complex bureaucratic systems,
and have even shaped services to better fit them. Sometimes
it’s fighting against discrimination (such as lack of choice and
disabled access) - “it’s the squeaky wheel that gets the oil.”
Other times, it’s refusing to accept services until they work as
they envision - insisting that respite be something for the two
of them, rather than a break away from each other. Mike says,
“I don’t want respite away from Liz I wanna be with Liz... if we
have respite we’ll have it together.”
WHAT GOOD LIVING LOOKS LIKELiz’s wish is for a “happy old age.” She would like to see
her grandchildren more than the every fortnight as it is
now. Mike thinks it’s important to have “someone to love,
something worthwhile, and something to look forward to”.
He occasionally misses the buzz that work gave him and his
loss of fitness due to his cancer, but he’s doing a few freelance
projects, and the cancer has helped them live in the moment.
That said they do plan for the future and have a plan in place
with a close friend should anything happen to either of them.
THEIR DAY TO DAYBeing close is very important to Mike and Liz and they start
each day with a two hour ‘love-in’ - for intimacy, planning the
day, newspapers and drinking coffee in bed. Three times a
week, a carer, provided by Domiciliary Care, visits and helps
get Liz showered and dressed. One of these is regular carer
Mary, who goes with Liz to the Central Market to shop for
their weekly ‘cooking experience’ where they produce dishes
from different cultures together—Liz does all the chopping,
Mary does the mixing.
Mornings often involve an exercise class for Liz, and Mike
will get on with work in the home, or goes on his regular
second-hand book hunt. Liz will take a nap every afternoon
“to give the neurons a chance to switch off”, and they also fit
in their weekly choir practice. Friends often pop round - like
Bronny, who they met through her mowing service, and have
developed a friendship with over the years. Most weekends
involve visits or outings to family and friends, or a creative
project—Liz has just finished painting mugs as presents for
the grandchildren.
“somebody to love, something worthwhile to do, and something to look forward to” Getting by Great Living
Fam
ily
Community
Services
Network R.ship
LizMik
e
CONNECTIONS MAP

Patterns:What is great living?
Barbara, Suzie, Dudley, Daphne, Soula, Mick, Thia and most of the other people we met are getting by. They have their basic needs met: they have food, a roof over their head, access to health care, and professional carers who help with shopping and cleaning. They are getting by in spite of brain tumours, diabetes, MS, dementia, and cancer.
Only a handful of people we met were close to great living - people like Leon, Mike and Liz. That left us wondering: What’s different about the people who are experiencing great living? How could we help more people lead great lives?
These are the questions we set out to answer as we looked for patterns across the 40 stories we heard. First, we compiled people’s definitions of great living. Then, we analysed what people actually did - in other words, how they behaved - to move towards great living. Finally, we identified what enabled people to adopt those behaviours: the mindsets, relationships, and networks that seem to support great living.
Here’s what we discovered.

PAGE 29PAGE 28
Q: What do people say is great living? A: Personal development, close connections, compelling experiences, and not being held back.
Patterns
Dudley wants intelligent conversation. Daphne wants to feel respected. Suzie wants to eat lobster and kangaroo, from her days out in bush. Barbara wants financial security, and to not have to worry about paying for her funeral. Liz wants to keep learning new things. Mike wants to be surrounded by driven, passionate people. Mick and Soula want to travel interstate. Leon wants to build new relationships. Thia wants to never be alone.
The ‘living great’ cards in action
When we asked people to sort through our ‘living great’ cards
and assemble their version of great living, we got a real range
of responses. Not surprising, really. People in caring roles and
relationships are about as diverse as they come.
We wondered what great living meant as people’s roles
and relationships shifted over time. The literature on great
living—on wellbeing, to be more precise—talks a lot about
independence and control.* These aren’t static concepts—as
our capabilities change, so too does our independence and
control.
What does great living mean when we are no longer as
independent as we once were, and rely on others to get by?
What does great living mean when our relationships require
more of us than they once did?
GREAT LIVING IS TANGIBLEWe learned was that people’s versions of great living were
rooted in past experiences . They weren’t extravagant or
fantastical. Dudley values intelligent conversation because
he’s always been a witty conversationalist. Suzie sees the
great living as good food because she’s savored it before.
People weren’t downgrading their aspirations based on their
caring needs and responsibilities - but they were downgrading
their sense of possibility. For Daphne, great living was about
feeling respected. Respect wasn’t a fuzzy concept for her:
it meant people seeing you, not your ailments. Yet Daphne
saw respect as completely out of reach, something no longer
possible given her ailments.
Great living, even where it felt out of reach, was tangible. It
was made up of at least four component parts, which people
sequenced and prioritised differently. Some people saw
great living as all about personal development; other people
saw great living as a blend between close connections and
compelling experiences; still other people saw great living as
not being held back.
* Valliant (2002) and Burgener
(2005), amongst others, informed
our thinking about great living.
To see what we read head to page 72.

PAGE 31PAGE 30
Q: What behaviours underpin great living?A: Exchanging, adapting, shaping, enjoying, initiating.
Whilst few people we met wanted any less for themselves because of their caring situation, many are living with less. Barbara’s diabetes is worsening; she rarely gets out of the house. Daphne has debilitating stomach pain; Dudley spends most of his day at Daphne’s side. Eileen was recently diagnosed with emphysema; most of her week is spent alone, reading postings and playing games on Facebook.
The gap between people’s aspirations and their behaviours is wide. By behaviours, we mean what people do, say, think, and feel on a day-to-day basis.
People moving towards their versions of great living do, say, and think some similar things. They may have different versions of great living and different capabilities, but they have adopted a common set of behaviours.
Patterns
Top: Leon and his friends eating Alison’s lamb stew.
Bottom: Liz and one of her ESL students.
GREAT LIVING BEHAVIOURS The individuals we met close to their version of great living:
• Exchange: Swap stories, skills, resources, and different
kinds of care.*
• Adapt: Continually (re)shape how they live and what they
do, measuring success in terms of what they can do†
• Shape: Explore potential futures, plan forward, shape
expectations and systems to work for them.
• Enjoy: Infuse fun, enjoyment, and humour into most
everything they do; Don’t see health as a prerequisite of
happiness.
• Initiate: Actively seek out new people and places.
Mike and Liz’s version of great living is constant learning,
being in stimulating environments with passionate people,
and having a close relationship with each other. Liz is losing
muscle control, and yet she’s still taking on new projects,
learning to cook new recipes and painting. Mike and Liz have
helped to initiate a carers choir and Liz tutors ESL students
at home, enabling them to constantly meet new and different
people.
Leon’s version of great living is about reciprocal friendships,
fixing trailers, and building new connections. Far from being
an obstacle, Leon’s blindness has brought new meaning to
the notion of reciprocity. He still fixes trailers. He tells lots
of (off-colour) jokes. He laughs a lot. He’s open to meeting
friends of friends - and takes an interest in their interests. This
enables him to build new connections - including romantic
relationships.
People who are farther away from their versions of great
living also do, say, and think similar things. They too have
different versions of great living, and different capabilities, but
their behaviours aren’t facilitating great living.
THE INDIVIDUALS WE MET FARTHER AWAY FROM THEIR VERSION OF GREAT LIVING• Don’t think they have much to give.
• Stick with the familiar and convenient; measuring
success in terms of what they can no longer do.
• Fear a negative future; wait for it to happen.
• Make decisions according to what they see as
‘appropriate’; accept limitations of age and health.
• Avoid asking for or accepting help.
Barbara’s version of great living is financial security, closer
relationships with family, and travel to Scotland. Since her
divorce 10 years ago, Barbara hasn’t had any contact with
her 4 kids. She sees her diabetes and poor health as a barrier
to doing much. She eats lollies and shortbread in bed. She
hasn’t accepted her neighbour’s invitation to Christmas dinner.
Money is so tight she struggles to pay for subsided frozen
meals, but she’s not told anyone about her financial situation.
Dudley’s version of great living is about intelligent
conversation, competition and challenge, Daphne’s version
of great living is about being respected and doing projects
with Dudley. Until 8 years ago, Dudley was the world’s oldest
speedway racer. Daphne was his pit crew. Now, Daphne’s
unwell more days that she’s well. She sits in her special
chair and waits for the hours to pass. Dudley rides his bicycle
every morning, plays with his dog, reads a textbook about
prescription drugs, and occasionally watches videos of his
speedway days. A recently widowed neighbour comes by
most nights for company. There’s not much new to talk about.
RELATIONSHIPS INFLUENCE GREAT LIVINGDudley and Daphne’s behaviours are interlinked. What one
does, says, and feels affects the other. We found that for
people giving and receiving nearly full-time care from each
other, we needed to look at the distribution of behaviours
across the relationship. Dudley doesn’t go to the speedway
track because he thinks Daphne is too unwell. Daphne doesn’t
ask to do projects with Dudley because she thinks she is too
unwell. Neither is getting what they want: in fact, they seem
stuck in a self-perpetuating downward cycle. We met another
caring couple where the husband was “sacrificing” his great
living to try and keep his wife, suffering from dementia, at
home. They too are stuck in a self-perpetuating downward
cycle, where neither is getting any closer to great living. The
demands of caring has supplanted anything else.
* Fine’s (2004) work gave us
a lens to look at care relationships
more broadly.
† Freund’s (1998) selection,
optimisation and compensation
(SOC) framework influenced how we
thought about adaptation.
To see what we read head to page 72.

PAGE 33PAGE 32
What enables Mike, Liz, and Leon to adopt behaviours that get them closer to great living? Why haven’t the demands of caring supplanted everything else? The short answer seems to be balance. They’ve got a ‘knock-down, get-back-up’ attitude. They’ve got relationships that aren’t just about caring. They’ve got networks that both alleviate the pressures on their relationships and bring new energy and experiences into the fold. Individual mindsets, relationships, and networks are what appear to be critical.
Q: What enables people to adopt behaviours that move them towards great living? A: Mindsets, relationships, and networks.
OPEN MINDSETSMindset, attitude, personality, outlook, self-perception. Call it
what you will, but the people who are moving towards great
living are able to truly appreciate being alive - even whilst
acknowledging the indignities and setbacks of getting older
and needing care. They don’t live in denial. They live with an
understanding of what is happening to them and those around
them - but don’t see it as taking away from the essence of
them. Leon knows he is a funny and blindness won’t change
that, if anything it gives him new material.
In psychological words, the people doing really well seem
to have a strong sense of self. They know who they are, and
are secure enough with their own identity that they find ways
to keep expressing themselves even when circumstances
change. A change in circumstance isn’t something to be
feared, avoided, or succumbed to but just a new reality they
have to adjust to.
Patterns
Irene
MOTIVATIONAL RELATIONSHIPS Solid, trusting, comforting, active, fun. These were some
of the words people who were doing well used to describe
relationships that brought the best out of them. Relationships
that made them want to exchange stories, skills and
resources; focus on what they can still do; plan forward; do fun
things; and seek out new opportunities. Good relationships
seemed to motivate people to get on with living, as well as
help them to actually do that.
Good relationships weren’t just a ‘means’ to an individual’s
‘ends’, but an ‘end’ in and of themselves. Liz’s relationship
with Mike isn’t just helping Liz get by and live well, but
something she puts continual energy into. That’s also true
for another couple we met, Lou and Karen. When Lou was in
hospital receiving treatment for leukemia, Karen planned and
orchestrated a weekly date night- complete with table clothes,
candles, and non-hospital food. Lou even gently chided Karen
for not remembering his dress shoes.
VIBRANT NETWORKSAbundant and varied. That’s how we’d describe the networks
that surround the people living well. What separates networks
from relationships is the frequency with which people see
them - and the functions they perform. Individuals and groups
in a network might be connected to a particular interest (e.g.
sewing friends), or a particular time (e.g. friends from work),
or a particular need (e.g. plumbing, cooking).
Academics refer to networks with a range of individuals and
groups as ‘multiplex.’ That means there is some redundancy
built in - there are multiple people in the network that could
fulfill a function if needed. That also means there is task
distribution - and the tasks are not all about caring. Indeed, we
learned that having individuals & groups in the network who
don’t play a physical caring role helps people maintain their
interests and practice adaptive behaviours.
Take, Leon, for example. He’s got a cleaner and he gets meals
delivered every week - but he also has mates with whom he
repairs trailers, neighbours with whom he shares a good joke,
and community groups he visits to get out of the house. Were
some of his mates and neighbours to no longer be around,
Leon has other people in his network who could play similar
roles. We’d predict that Leon’s network could bounce back if
there were some changes and unpredicted shocks.
* To read more about Knoke
and Kuklinski’s (1982) concept of
multiplexity head to page 72.
Eddy Leon

PAGE 35PAGE 34
Open mindsets, motivational relationships and vibrant networks were common features across the people doing really well, though the makeup of their relationships and networks varied widely. Leon’s got mates, neighbours, and community groups. Mike and Liz have each other - as well as friends and a professional carer. For those doing well, friends, family, services and community groups take on a variety of roles. Over time, as capabilities shift, so too can the relationships and networks. People in the network layer can take on more intensive roles, and people in the relationship layer can distribute tasks to the network. This flexible mix of people helps to maintain great living.
Q: Who enables people to adopt behaviours that move them towards great living? A: A mix of friends and family, services, and community groups
FRIENDS & FAMILY MAKE AN EFFORTFor relationships to be motivational and networks to be
abundant, partners, parents, children, grandchildren, and
friends also have to do, say, think, and feel different things.
Partners who are in great relationships and networks keep
doing the things that make their relationship tick - whether
that’s going for drives, reading the newspaper, or having date
nights - even as capabilities shift. They also find ways to keep
the intimacy alive - whether that’s sex or just physical touch.
And they don’t shy away from the difficult conversations.
Parents and children who are in great relationships and
networks work hard to treat each other as adults. They are
mindful & respectful of boundaries, acknowledge and express
appreciation for what the other is doing.
Friends who are in great relationships and networks keep
up with each other regularly. They call to check-in, and are a
regular presence in each other’s lives even if they see each
other infrequently. They are also not afraid of sickness and
age. They can reminisce about the past, but also suggest
things to do together - be it watching a film, reading a book
aloud, cooking something, or going on an outing.
COMMUNITY GROUPS REACH OUTChoirs, country clubs, sewing circles, lawn bowls, bridge
groups, dancing groups, community centres, cancer support
groups. The people experiencing great living are plugged into
community organisations and groups that help them to keep
learning, stay active, and meet new people.
These are community organisations and groups that are
flexible and reach out to people. They don’t have a ‘Build it
and they will come’ mentality. Instead, they actively cultivate
new members and do everything they can to close logistical
gaps - even for the non-joiners and people who have said ‘no’
in the past. Every couple of weeks, Leon takes part in a group
suggested to him by the Royal Society for the Blind. They had
to work hard to sign him up. Now they pick him up, and head
to the Gawler Country Music Club Inc. for an afternoon of live
music. The people he’s met have become so close they throw
each other birthday parties, and see each other between
events. That stands in stark contrast to the speedway circuit
that Dudley and Daphne were a part of. Once they stopped
participating, the group stopped calling. They are disconnected
from their former network.
Patterns
SERVICES ARE DEVELOPMENTAL Carers, doctors, cleaners, and gardeners. Nearly everyone
we met interfaced with these services. For people far away
from their versions of great living, weekly visits with service
providers were their relationships and networks. For people
closer to their version of great living, service providers were
only one node on the network. Usage didn’t seem to be
the differentiating factor. It was the quality of those service
interactions.
Every other week, Inga spends two hours with Suzie helping
her restock her kitchen. They shop and put away cans of food
together. Inga is a professional carer whose salary is paid for
by the state and a welcome helper to Suzie when she’s there.
Many nights, Suzie just opens up a tin of tuna for dinner.
Every Friday, Mary spends the morning with Liz cooking food
from around the world. They plan, shop, chop, mix, pour,
simmer, and bake together. Mary is a professional carer,
whose salary is paid for by the state, but when in Liz’s kitchen,
she’s a creative sous chef.
Both Liz and Suzie have their essential food needs met.
But, for Liz, food isn’t merely a functional experience. It’s
a developmental experience. Shopping and cooking aren’t
chores to be ticked off a list, but opportunities to learn, build
new capabilities, and enjoy.
Nearly all of the services we heard about and saw were
good quality, functional experiences. Beryl and Jon really
like their cleaner. Barbara likes the driver who delivers her
frozen meals. Daphne likes the girls that keep her company.
In fact, older people’s services consistently receive customer
satisfaction rates of 95%!
But, satisfaction shouldn’t be the only marker of success. After
all, such statistics are based on people’s prior experiences
with services of those kind, rather than an understanding of the
kinds of services that could be. Few of the services we heard
about or saw were good quality, developmental experiences.
They weren’t building capabilities. If anything, many of these
services inadvertently took away people’s capabilities.
Dudley loves to garden, but he felt pressured to accept
gardening help in order to get more support for Daphne. Now,
he’s not gardening as much. Barbara watches Nigella Lawson
and enjoys making good Scottish food, but gets frozen meals
delivered to eat alone. It’s just easier. Then, there are people
who avoid services in order to maintain their skills. Another
person we met, Eddy, actively avoids going to the Citizens
Centre because he wants to keep up his cooking skills, and
not “get lazy”. When his wife was alive, she did all the cooking,
so Eddy’s asked his carer to teach him how to cook. Now
Eddy’s churning out cookies and cakes.
More than building skills, though, services could help build
relationships. We haven’t yet encountered a service that
intentionally brokers or facilitates informal relationship and
network building. Yes, we’ve seen services that help take the
strain off of existing relationships- services like respite and
holiday planning- but we haven’t seen services that act as
matchmakers, facilitators or mediators for building new or
repairing old relationships & networks.
Services that build skills and relationships are services that
enable people to change their behaviour. People like Eddy and
Mike and Liz teach us behaviour change is not only possible,
it’s critical to continuing to do well. But behaviour change
isn’t a concept we’ve encountered much when out and about
observing services and groups.
SHIFTING BEHAVIOUR The big question, then, is what could we do to shift older
people’s behaviours? How could we shape individual’s
mindsets, relationships and networks? How could we help
services, community groups, and friends and family function
as the sorts of relationships and networks that enable great
living? These are the questions we asked ourselves as we
moved from analysing people’s stories to brainstorming
opportunities for things to be different.
Pricing Arrangements in Residential Aged Care, Canberra, p. 2.
4. Productivity Commission, 2011, Caring for Older Australians, Report No.
53, Final Inquiry Report, Canberra.

Opportunities for great living
We found...People farthest from great living often
have closed mindsets that get in the
way of great living.
The opportunty1: Shaping MindsHow can we help people shift their
mindset so that isn’t a barrier to great
living?
We’ve identified what adds up to great living - but what about the people who are far from great living and those who are only part of the way there. What can we do for them?
Getting people closer to great living will mean creating more open mindsets, more motivational relationships and vibrant networks. To do that will require shaping the behaviour of individuals, family, friends, communities as well as providers of help and care. This section sets out 7 opportunities for shaping behaviour based on our work on the ground, theory and international practice.
Exactly what these opportunities will look, sound, and feel like, we don’t yet know. That will come from the next stage of our project, when we sit back down with the people and practitioners we’ve met to co-design and prototype solutions they want to be part of.
Shaping individuals
3 2
We found...People far from great living were often
estranged from family, disconnected
from friends, or part of a caring
relationship that was strained.
The opportunities 2: Rebalancing RelationshipsHow could we reduce the strain
of caring relationships on family
and friends?
3: Activating Family & FriendsHow can we activate family and friends
at the periphery?
We found...People far from great living lived in
settings with few opportunties to build
new caring relatinships or networks.
The opportunities4: Starting Relationships How can we help people to form
caring relationships ?
5: (Re)Starting NetworksHow can we enable people in caring
situations to build networks in the
community?
We found...People far from great living often
relied on services that struggled to
provide genuine caring relationships,
developmental experiences and diverse
forms of help.
The opportunities6: Caring Services How can services be part of a caring
relationship?
7: Diversifying Help Networks How can we diversify networks of help?
Shaping family & friends
Shapingcommunities
Shaping providers
1 6
4
5
7

PAGE 39PAGE 38 Opportunities
Reshaping late adulthood into it’s ‘never too late’ adulthood.
1. Shaping minds
Developing mindsets open to living and caring differently.
WHAT’S THE OPPORTUNITY?We tend to look as late adulthood as a
period of declining capabilities. That is
only one reality there are many other
realities: learning, intimacy, fitness,
good food, zesty times. The people we
met closest to great living saw a loss
of capabilities as a challenge. One to be
tackled with resilience, creative thinking,
adapted goals, and sometimes a little
bit of help.
In contrast, the people we met who
were furthest from great living felt
stuck, unable to modify things around
them, and sometimes resentful of help.
They didn’t adapt but maintained goals
beyond their reach, then felt down when
they couldn’t achieve them. To prevent
further disappointment they stopped
setting goals.
This opportunity is not about relentlessly
positive outlooks in late adulthood, it’s
about developing mindsets that are
open to living differently.
Most existing solutions for shifting
mindsets are talk-based professional to
client therapies. Our hunch is that we
can use them - but to appeal to people
in caring situations, we will have to
take these therapeutic approaches into
different contexts - making them both
less clinical and less new-age.
STARTING POINTSThe Reader Organisation (TRO) uses
therapy through books to shift older
people’s wellbeing, at a relatively low
cost. How else could therapeutic
approaches look at home, on the radio,
at the shopping centre, online or over
the phone? What about therapy through
film, music, news, magazines, humour?
Rather than professional-to-client
interactions, what about peer-to-peer
interactions that draw on the lived
experience of older people?
WHAT COULD THIS LEAD TO?Imagine a new suite of therapeutic
approaches based on things people love
doing e.g. knitting or mechanics; new
organisations promoting open mindsets
With & For: - People whose mindset gets in the
way of great living.
Behaviour change:- From a closed mindset to an open
mindset. Rebalancing fear and
widening sense of self.
at key transition points (e.g. retirement)
and in late adulthood; new coaching
roles for older people who have open
outlooks; new kinds of training for social
workers and psychologists; and new
spaces for therapeutic sessions: public
libraries, for example.
HOW IS THIS DIFFERENT?In contrast to social marketing used to
promote ‘positive ageing’ and ‘active
retirement’ to whole populations, we
propose focussing on individuals and
caring relationships. Whereas social
marketing approaches often avoid
issues of dependency, dealing with the
realities and possibilities of changing
capabilities will be core to this approach.
To complement targeted therapeutic
approaches focussing on grief and
loss, we propose an approach that is
proactive and open to anyone in a caring
relationship.
For more about TRO go to page 68.

PAGE 41PAGE 40
2. Rebalancing RelationshipsReducing the strain of caring by actively (re)balancing relationships.
WHAT’S THE OPPORTUNITY? Most caring we saw happened between
partners. For those close to great
living, relationships were balanced and
motivating. The ‘tough stuff’ was talked
about, when help was given it was
recognised with positive feedback, and
people found ways to keep doing what
they loved - together and apart.
For people far from great living,
caring responsibilities dominated
the relationship, leaving it strained
and stretched. Family members had
begun loosing respect for each other,
avoided asking for or giving help and
dodged difficult conversations. Partners
had often lost the common pursuits
and intimacy that their relationship
was founded on. People directly and
indirectly talked to us about the lack of
sex and touch.
The stress, depression and poor
health outcomes associated with
caring was what got this project off
the ground. Our hunch is that the
With & For:- Partners and family members in
strained caring relationships.
Behaviour change:- From caring dominated
relationships to motivational
relationships.
Opportunities
strain of caring could be alleviated
by actively rebalancing relationships
and encouraging exchange. Like
in Opportunity 1, recontextualising
therapeutic approaches could provide a
starting point.
STARTING POINTSPremarital classes, sex therapy for
couples, mediation, retreats, and family
counselling can help us to learn how to
repair and improve broken and strained
relationships.
WHAT COULD THIS LEAD TOImagine new kinds of family counselling
specific to late adulthood or new kinds
of intimacy & sex therapy specific to
older couples. What would relationship
therapy look like at home, in person,
or over the phone? Could they spread
in a way that didn’t always rely on
professional therapists? Could we
tap into existing respite dollars? Or
capitalise on savings to government,
who currently pitch in approximately
$40,000 per annum for publicly funded
places in low level residential care?8
HOW IS THIS DIFFERENT?Respite is designed to provide someone
in a caring situation with a short term
break from a relationship. We propose
to work on the caring relationships itself
and broaden our unit of focus from an
individual carer to all partners, family
members, friends and even services
who are part of caring relationships.
5. Australian Institute of Health and Welfare,
2004, Carers in Australia: assisting frail older
people and people with a disability, AIHW Cat
3. Activating Family & Friends
WHAT’S THE OPPORTUNITY.Adult children, grandchildren and
extended family played a limited role
in many of the homes we visited, more
often appearing at a network level
rather than as part of a core caring
relationships.
Sometimes family members were
emotionally close yet geographically
far away, but in many of the situations
we saw family were geographically
close yet emotionally distant. Stories of
estranged relationships were common.
Families and friend networks that
actively contributed to great living had
a good understanding of what was
needed, distributed tasks evenly across
the network, and provided relief to those
at the centre of the caring relationship.
What’s more, they got something out
of helping out: emotional closeness, a
feeling of reward, a stronger sense of
identity.
With & For:- People who have family in their
network who could do more.
- Family members who would like
to do more.
- Family members who’ve become
estranged.
Behaviour change:- From disengaged networks to
active networks and relationships.
We see an opportunity to activate willing
family members who are part of the
network and help them contribute to a
motivational caring relationship.
STARTING POINTSPlanned Lifetime Advocacy Network
(PLAN) have been supporting network
building around people with disabilities
in Canada for over 20 years. They aim
to create a good life for families living
with disability and provide training for
parents in building networks. PLAN
also supports “community coordinators”
who actively catalyse caring networks
around individuals. More recently
they developed Tyze, an online social
networking tool for families to identify
and distribute tasks amongst a family
and friend network. Families pay a
membership fee to be part of PLAN and
additional fees for training events and to
use Tyze.
WHAT COULD THIS LEAD TOImagine PLAN’s training, roles and
online networks adapted to support
older people and family networks
in Australia. The approach could be
spread by a new kind of membership
organisation or become a new offer for
organisations already working in the
relationships space.
PLAN’s tools focus on building networks
amongst those who want to help.
Reaching out to more disconnected
family members will require different
roles and tools, such as a new kind of
family arbitrator to address complex
family histories.
HOW IS THIS DIFFERENT?Whilst there are organisations
supporting family relationships, we’ve
not come across services that focus
on building and repairing family
networks around caring situations in
late adulthood. In many cases, we see
networks as an untapped resource.
Activating family as part of the network and building caring relationships.
To read more about PLAN, go to page 69.

PAGE 43PAGE 42
4. Starting relationships
WHAT’S THE OPPORTUNITY?We met a number of people who didn’t
have caring relationships, but wanted
to form some. They often lived alone -
separated from partners by divorce or
death and from family by estrangement
or geographical distance. Most talked
about not wanting to be a burden on
others and feared residential care.
Those closest to great living were
working to build caring relationships
from their existing network. Others,
who had a home they could sell, saw
moving to a retirement villages as
a way to build caring relationships.
Currently more than 160,000 Australians
live in retirement villages, but from what
we’ve seen they do little to build new
relationships or move people towards
great living. 9
We see an opportunity to support
people without caring relationships to
build a more varied, intentional and
caring communities around themselves
- whether they choose to move from
home or stay put.
STARTING POINTSCo-housing is an international
movement of people building supportive
communities. Whilst co-housing for
older people shares some features
with conventional retirement villages,
such as small homes arranged
around common facilities, there is a
big difference. In co-housing homes,
facilities and activities are all designed
and run according to the requirements
of residents. Explicit social contracts
setting out expectations of the kind
of help and care to be exchanged
between residents are common. The
collective design process plays a big
role in developing the community and
is sometimes facilitated by experienced
organisations like US based Co-housing
Partners.
WHAT COULD THIS LEAD TO?Imagine new collective living
arrangements, between people
with common interests that actively
contribute to great living, are easy to be
part of and share resources including
With & For:- People looking to form caring
relationships in advance of late
adulthood.
- People without caring
relationships.
- Retirement villages, social
housing for older people,
centre based services.
Behaviour change:- From passive aged communities
to caring communities.
care and help. These communities
could be centralised or distributed local
networks: people living in their own
homes but connected.
Building diverse links in these
communities could involve a ‘dating
service’ or a ‘find old friends’ service.
These new kinds of services could also
activate relationships within existing
communities such as retirement
villages, centre based groups or aged
housing.
HOW IS THIS DIFFERENT?The retirement communities we’ve
seen are not developmental. They do
little to intentionally open minds, form
relationships or diversify networks and
are only accessible to people who can
sell their home.
Supporting people to live in settings where they can build caring relationships.
Opportunities
No. AGE 41, Canberra, p. 16.
6. Access Economics, 2010, The Economic
To read more about co-housing,
go to page 70.
5. (Re)Starting Networks
WHAT’S THE OPPORTUNITYMany of the people we met with weak
networks once had rich ones. They used
to meet friends in their homes, go to
clubs, go fishing and volunteer - but
illness got in the way. Now finding the
energy to leave the house and take part
is just too much.
We see an opportunity to catalyse new
connections and rebuild old ones from
home. This could mean:
1) Creating at-home networks around
existing community groups, interest
based clubs, religious groups, learning
institutions and places of work.
2) Catalysing new distributed networks
that draw on people’s passions,
knowledge and latent assets - such as
unused workshops, untended gardens,
and spare rooms.
STARTING POINTSThe Alice Springs School of the Air
provides education to children in remote
outback settings, and is an example of
a centre based institution reimagined
as a distributed network. Initiated with
a radio broadcast from Adelaide in
With & For:- People looking to start or
restart social networks.
- Community groups, interest
based clubs, religious groups,
learning institutions and places
of work.
Behaviour change:- From ‘come to us’ to
‘we hook you up.’
1951, the school today enables learning
for 120 children spread over 1 million
square kilometres. The platform has
evolved to provide learning experiences
through video, audio, materials send
by post and whole school events 3 or 4
times a year.
US church Saddleback provides an
example of how to supporting the
development of at-home networks.
Nearly all of the 20, 000 members are
part of one of the 3,000 ‘cells’ - groups
of 6 or 7 that meet in each other’s
homes. Saddleback’s core business is
the recruitment, training and retention
of volunteer leaders who start and run
these groups.10
WHAT COULD THIS LEAD TO?Imagine providing staff and members
of existing centre based groups with
the training and technology to re-
connect former members and shape
activities so that they provide value to
distributed members. The community
care provision market is estimated to
be worth more than $1.8 billion a year.11
Could a small share of this market be
drawn on to re-start networks?
Imagine new roles and technology to
identify and initiate latent groups in
the community, and then to run those
groups in people’s living rooms, gardens
and sheds - making use of common
interests and underutilised resources.
HOW IS THIS DIFFERENT?In contrast to centre based groups
which convene only for specific
activities, this opportunity focuses on
building and maintaining relationships in
varied contexts. Whilst there are many
examples of video and the internet
being used to reach older people, we’ve
found few examples of solutions that
actively build and maintain distributed
networks of older people.
Catalysing new connections and rebuilding old ones from home.
Value of Informal Care in 2010, Report for
Carers Australia, October, p. 3.
7. Family and Community Services, 2010,
Home care client satisfaction survey results.
Available: http://www.adhc.nsw.gov.au/
individuals/help_at_home/home_care_
service/your_feedback/

PAGE 45PAGE 44
6. Caring servicesShifting professional carers and services from providing help to enabling development.
WHAT’S THE OPPORTUNITY?The people we met furthest from
great living were dependent on formal
services for their caring relationships.
Getting these people closer to great
living will mean services becoming one
part of a motivational realtionship.
Where services were motivational,
workers didn’t only provide practical
help, they provided developmental
experiences aligned to what people
loved but thought they could no longer
do. They didn’t just cook - they made
meals an event; they learnt languages
together; they visited exciting places.
What’s more there was reciprocity:
workers did things with people, not for
them, and had a good time.
Mos of the services we saw, though,
simply provided help in an efficient and
friendly way. And whilst people liked
their professional carers, in some cases,
the relationships were inadvertently
creating greater dependency. To move
people to great living, care services
will need to shift from providing help to
enabling ongoing development.
STARTING POINTSThe Green House Nursing Home
Alternative has improved outcomes for
residents and staff of residential care
by adopting a set of developmental
principles, redesigning the physical
space and creating a new role - the
Shahbaz. Shahbazim provide personal
care, cook and clean and because of a
different organisational model, spend
more time with residents building
personal bonds. All this at a cost
comparable to traditional residential
care.
WHAT COULD THIS LEAD TO?How could we turn in-home workers
into something closer to the Shahbaz
role? How could we apply the principles
and practice of Green Homes to in-home
care? Imagine a new set of protocols
and roles for in-home workers. Or
new kinds of training and accreditation,
professional development, pay scales,
and matching processes between
‘workers’ and people requiring care.
With & For: - People who rely on services for
caring relationships.
- Providers of domestic and
residential care services.
Behaviour change: - From helpers to enablers.
Making all this happen at scale
will be dependant on shifting the
federal policies which tightly control
the type and quantity of care. A
significant amount of resources goes
into residential care. In 2009-10 the
government provided $7.1 billion to
residential care.12 Could a small part
of these resources be the start-up
capital for new, more developmental
solutions?
HOW IS THIS DIFFERENT?Existing models of in-home
and residential ‘care’ are in-fact
transactional help, albeit often provided
in a warm and friendly way. This
opportunity looks at how we can shift
the role of care workers so that it is
more developmental for older people
and more rewarding for workers.
Opportunities
8. Commonwealth of Australia Treasury, 2009,
Australia’s Future Tax System - Part Two
To read more about Green House,
go to page 71.
7. Diversifying Help Networks
WHAT’S THE OPPORTUNITY?The innovative services we’ve seen
don’t start with formal assessments,
but with conversations about older
people’s aspirations. But when it
came to connecting those people to
services to achieve these aspirations,
things broke down. Despite the
rhetoric of ‘consumer choice’ there
is a limited breadth of services
available - contrained by government
funding - and these are not necessarily
what older people themselves want.
This limited choice provides a direct
challenge to innovations like consumer
directed care.
People closer to great living found and
shaped help into unconventional forms
- cooking experiences, pagoda building
help and travel buddies. People further
from great living were happy with any
service they were offered and didn’t
think to shape it to better fit their needs
and aspirations.
We see an opportunity to increase the
quantity, diversity and quality of help
available and to shape demand for
different kinds of support that is more
developmental - a particular challenge
for people who are risk adverse and
want to stick with what they know.
STARTING POINTSJag, which translates as ‘I’, is a
co-operative of disabled people in
Sweden who hire their own personal
assistants - including friends, family,
or recommended carers. Jag shapes
demand for help, makes it easier for
disabled people and their families
to shape what help they get and has
created a new market for would be
personal assistants.
The Amazings is a supply driven
platform for retirees to find a market for
their skills, knowledge and passions.
You can use it to go on history walks,
learn to knit or dance. The platform
uses advertising to find a market
for experiences retirees want to run
and then handles payments from
attendees.13
With & For:- People looking for practical help
and new opportunities to learn.
- People looking to help others
- People looking for new business
opportunties
Behaviour change:- From latent help to active help.
WHAT COULD THIS LEAD TOImagine a new platform for identifying,
training, and hosting new kinds of
developmental services. Imagine a
new industry of computer fixers, cake
decorators, dog trainers and armchair
travellers. Or new ways for people close
to great living to share their strategies
with families and the younger old.
Imagine something that tapped into
disposable income and state provided
funds to enable great living for all.
HOW IS THIS DIFFERENT?Innovations we’ve seen in consumer
directed care have focused on creating
the means to purchase different
services and on brokerage to existing
services rather than catalysing new
markets of help and shaping demand
toward developmental experiences.
Increasing the quantity, and quality of help available and shaping demand for diverse kinds of developmental support.
Detailed Analysis, p. 634.
To read more about JAG,
go to page 68.

PAGE 47PAGE 46
Economic oppportunitiesInvesting in developmental solutions could reduce future costs. Leveraging people and money already invested in aged care and activating new resources in the community requires different practice, not neccessarily more money.
Over the coming decades, government spending on aged care is projected to draw even with other big ticket items such as education and defence.14
With such massive spending, even small innovations could have a significant impact on the public purse. For instance, a 1% reduction in use of the aged care system would free $110 million per year.15 That’s $110 million that could be used to enable great living.
Our work with people, with services and our analysis of financial projections suggest five economic opportunities:
We could save money(1) We could reduce entry into expensive residential care.
We could get more from existing resource(2) We could sustain and increase contributions of family and friends.
(3) We could get more from existing investment in community and aged care services.
We could activate new resources(4) We could increase disposable income spent on aged care.
(5) We could activate non-financial resources in the community.
Why invest?
(1) WE COULD SAVE MONEY The research is clear: keeping people in their own home,
doing well, for longer, saves money. The average cost of a
person staying at home with the help of community services
is less than a quarter the annual cost of a place in residential
care. If an intervention can keep just one person out of high
level residential care for an additional two years it would save
the state well over $100,000.16
(2) WE COULD SUSTAIN AND INCREASE THE CONTRIBUTION OF FRIENDS AND FAMILY Friends and family across Australia provide an estimated 1.32
billion care hours per year. Low estimates value this at $6.5
billion per year.17 Keeping friends and family healthy, and
experiencing great living, is critical to the aged care system’s
financial solvency. Increasing the number of friends and family
taking on a caring role would create significant cost savings
for the state.
(3) WE COULD GET MORE FROM EXISTING INVESTMENT IN AGED CAREIndeed, in the decades to come, more and more Australians
will rely on services. By 2050 it is estimated that over 3.5
million Australians will use aged care services.18 Yet rigid
funding and accountability requirements mean few of the
services we saw actively contributed to great living. Few
worked to activate family and friends and few worked well at
the relationships level. Many could.
(4) WE COULD INCREASE DISPOSABLE INCOME SPENT ON AGED CARE User-pay solutions in the ageing space are controversial and
rightly debated. We are not interested in for-profit services,
but we are interested in exploring the potential for greater
personal contribution within not-for-profit models.
Whilst we spent time with people for whom money is a daily
concern, many of the people we got to know could afford to
contribute more to services than they currently do. This is
backed up by the research that shows a significant proportion
of retired people have disposable income. Whilst government
pensions are the dominant source of income in half of
households aged over 65, in the other half of households the
majority of income comes from other sources.19
In services we saw a vast disparity between actual costs,
prices charged and what people would be willing to pay. One
service we came across provides cleaning to older people
for $7.50 an hour. The fee is reduced or waived dependent on
ability to pay, but never increased. The real cost of the service
is close to $33 an hour.
9. Productivity Commission, 2011, Caring for Older Australians, p. 29.
10. http://saddleback.com/
11. Value based on government expenditure estimates for aged care
packages at home [HACC, CACP, EACH, EACHD, TCP, MPS] in 2006-07
only. Excluding expenditure for respite care and financial support for
carers valued at an additional $1.2 billion per year.
12. Productivity Commission, 2011, Caring for Older Australians, p. 30.
13. http://theamazings.org
14. Commonwealth of Australia Treasury, 2011, Intergenerational Report
2010, p. 47.
15. Total cost of aged care 2009-10 is $11 billion. Australian Institute of
Health and Welfare, 2011, Residential Aged Care in Australia 2009-10:
a statistical overview, p. 20.
16. Calculation based on comparison of the total cost per recipient in
(5) WE COULD ACTIVATE N0N-FINANCIAL RESOURCES IN THE COMMUNITYThe current aged care system treats older people as passive
recipients of resources, but most of the older people we’ve
met have resources to give. Leon can repair trailers, Dudley
has a fully equipped car workshop collecting dust. Barbara
knows how to make delicious shortbread, Liz can teach
English and Mike makes films.
Finding ways to systematically identify and exchange the
resources of older people and others in the community means
moving to co-produced service models. Models where people
not just professionals design services, make decisions and
share resources. Isn’t that what the ‘personalisation’ and
‘consumer choice’ agenda in aged care should be all about?

PAGE 49PAGE 48
There is another reason to invest in the 7 opportunity areas, and it has little to do
with cost savings or resource generation. It has to do with our morals, our values
and our own future.
Western society values children for their freshness and potential. One of our pillars
is equal opportunity - the notion that every child should have the same chance to
succeed and grow no matter their background.
Well, we believe the same should be true for older people. That every older person
should have the same chance to succeed no matter their illness, dependencies,
or even their past decisions. And that we should value older people for their lived
experience and potential.
Success, we think, is great living. It’s doing things you love, being close to people
around you, eating great food and having a laugh, and not letting too many things
get in the way.
We don’t think it is too tall an order. After all, isn’t it what we would want for
ourselves? For our friends? Thanks to science and modern technology, most of us
can expect to live into our late 70’s and 80’s. But we shouldn’t expect to just be alive
- we should expect to thrive. Knock on wood, one day we will all be in the shoes of
people we spent time with in this project. And our hunch is we’ll want to add life to
our years, not just years to our life.
A society with thriving older adults wouldn’t erase the inevitabilities of age - the
natural shifting of our capabilities and dependencies. But a society with thriving
older adults would mean that dependencies don’t just go up as capabilities go down.
It would mean building on what people can do, want to do and love. It would mean
recognising that older adults deserve experiences as developmental as society
expects for all children. Whilst there is a strong financial argument for this, we also
believe that it would make late adulthood a chapter of life to be excited about. Surely
that’s an investment we all have cause to get behind.
The moral imperative
“We have to think in a new way about care. We have to think through the mystique of age...”- Betty Friedan
Why invest?
What’s next?
In the next 2 months, we’ll move from broad opportunity areas to concrete ideas.
We’ll once again spend time with people, in their living rooms and kitchens, co-
designing solutions they want to be part of. Then, we’ll prototype, and iterate those
solutions. All along the way, we’ll be looking for partners & investors to help us
launch the most compelling solutions later in 2012.
Now that we’ve looked, listened and understood our next chapter is about creating.

Appendix:Behind the scenes
Index52 Learning and working
53 The Working Backwards approach
54 Finding people
56 Talking with people
58 Service shadowing
60 Reflections from people we met
61 More people we met
66 Reflections from the team
68 International examples
72 What we read
74 Bibliography
76 Glossary
77 Contributors
79 How to share this report

PAGE 53PAGE 52
Learning and working
By Radical Redesign Co-leads
Chris Vanstone & Sarah Schulman
A little over two years ago we moved to Adelaide to set-up
The Australian Centre for Social Innovation’s Radical Redesign
Team. Few people in Australia were blending design, social
science, community development, and business methods to
solve social problems. TACSI wanted many more teams to be
able to do so. The question was how?
During our first project in Australia, Family by Family, we ran
workshops and events to spread our approach. We found they
didn’t shift practice. Attendees often left understanding what
it meant to Work Backwards, but were not equipped to Work
Backwards.
That’s why we’re developing a curriculum to equip
interdisciplinary teams to Work Backwards. Rather than focus
on methods and tools, we’re focussing on the behaviours that
enable teams to co-design and prototype new solutions.
One of our hunches is that the best way to adopt these
behaviours is to combine live project work with structured
learning. We’re prototyping a new hybrid ‘work & learn’ model
with the Radical Redesign Team. Indeed, the curriculum is
a project running parallel to the caring project. Learning
experiences include: camps, classes, workshops, and new
models of reflection and feedback.
We’re also prototyping this hybrid ‘work & learn’ model within
the public sector. With the Department of Human Services,
we’re working on a project to improve outcomes for children
starting school and build civil servants’ capacity to think and
work differently.
In this Appendix, learn more about the approach, the
behaviours underpinning Working Backwards, and what is
has looked like to apply the behaviours & the approach in this
project.
Appendix
The Working Backwards approachEarlier on, you read about and saw the tools we used to talk to
people about their lives and aspirations [see p. 8]. Where the
Look and Listen phase was all about understanding people’s
versions of great living, in the upcoming Create phase, we’ll
work with people, practitioners, and policymakers to generate
and visualise ideas for enabling great living.
Our approach to working with people, practitioners, and
policymakers comes from a critique of traditional social
problem-solving. Rather than move from problems to policy
to practice to people, we Work Backwards. We build from
problems to outcomes, from outcomes to practice, and from
practice to policy.
To do that, we bring together critical policy thinking with
people-driven design, supported by social science, community
development, and business expertise. It’s not just different
disciplines we bring together but a different set of behaviours.
Behaviours for Working Backwards:Analytic behaviour - Identifying patterns and trends; breaking
complex concepts into component parts; asking why and how
questions.
Generative behaviour - Identifying and exploiting
opportunities; developing new ideas; applying concepts from
one field to another; thinking visually and laterally.
People behaviour - Talking with; observing; listening;
understanding, respecting and contextualising people.
Making behaviour - Turning abstract ideas into real, tangible
products; using your hands.
Feedback behaviour - Showing work; making improvements;
offering constructive suggestions to others; failing;
persistently iterating.
Storytelling behaviour - Developing rational and emotive
arguments; using different mediums; bringing ideas to life for
people versus practice versus policy audiences
Finding people, talking with people, service shadowing,
reviewing literature, analysing, identifying opportunities
Co-designing, brainstorming,
visualising
Testing new uer
interactions, materials and
roles
Testing policies,
procedures, back-end
systems
Developing the business case,
telling the project story
New opportunities
Potential solutions

PAGE 55PAGE 54
Finding people
But what convinces people to get involved?
We wanted to meet as many people as we could in as wide
a variety of caring roles as possible - the full time stay at
home carer, the person who pops in on a neighbour, a person
managing alone, the husband and wife who help each other
out. We had a hunch that many people’s voices are not heard
because they don’t engage in spaces, groups or conversations
that typically feed into research.
THINGS WE CONSIDERED THINGS THAT FAILED
THINGS THAT WORKED:
That’s why we spread our net broadly - heading to shopping
centres, libraries, public spaces and knocking on peoples’
doors. Meeting strangers out and about, who were busy
and going places, meant we had to develop an offer & value
proposition that would persuade people to stop, chat, and
want to meet with us again.
1. ‘Hug-a-bear’: a friendly way to get people’s attention.
2. A game experience with questions about caring.
3. An old vintage style cafe
We didn’t pursue these since in the end they seemed too gimmicky, lacked intentionality, and didn’t have a clear value proposition.
1. Asking people if they were a carer.
2. Using clipboards to collect people’s details.
3. Free flowers as an incentive to talk with us.
The caring question was too specific, the clipboards were too formal and flowers didn’t help us attract or stop people.
A table and posters offering free
bicuits & bananas for a chat. People
were curious, but still comfortable.
We felt people responded openly because we created an experience that was warm and inviting - but not over the top - and used language that was conversational and clear.
Giving examples, with illustrations, of
who we wanted to meet.
Using language around “helping out”
rather than around “caring.”
Appendix
“So what we’re doing today is collecting people’s contact details.”
“Do you know
someone who is doing
this kind of thing, or
perhaps you’re doing
it yourself?”
“We’re doing a
project with the local
Council about people
helping others out.”
THREE PHRASES THAT WORK
People were happier getting
involved when they believed
other people were too.
It put people less on the spot
about their experiences and let
them volunteer to help more.
Including a reference to our
project partners gave us
legitimacy with people.
Whilst we found certain words and phrases helpful, on reflection, we think our success came down to an ability to talk about the project from multiple angles until something resonated and kick-started a conversation.
Top: Recruiting at a community centre, Left: Filling out interest sheets on John Road, Salisbury. Right: Recruiting outside a Woolies in Kingspark, Unley.

PAGE 57PAGE 56
Talking with peopleWe find the best way to get to know people is to spend lots
of time with them in their own environment. It’s an approach
based on anthropological methods like ethnography. Often
it starts with a chat - some time for everyone to get familiar
with each other, and then continues into more unstructured
time doing everyday things like going shopping, visiting the
hairdresser, or going on a caravan holiday. These immersive
experiences help us to gain a better understanding of people’s
lives. They bring to light interesting disconnects between
what people say they want and do and what they actually do.
In other words, they get underneath mismatches between
people’s perceptions and reality.
But how did we know what to ask? And what to look for?
CREATING A TOPIC GUIDEBefore we met people, we created a list of topics we had
a hunch might be valuable to explore:
• Looking at the current lives of people and seeing
their everyday contexts and networks.
• Discussing hopes and aspirations for the future, and
discovering if they are on track or far from it.
• Focussing on relationships, looking at power
balance, use of language, roles and what was
exchanged.
KEEPING OPEN & CURIOUSHaving an unstructured approach led us us down
interesting paths with people:
• We used the topic guide as a prompt not a survey.
• Introducing topics fluidly, asking questions
opportuniticly, and going with the flow of conversation
rather than trying to overly direct the conversation.
Appendix
Tea & Cake | First Visit Interaction
Topic Guide & Script - Caring Relationship
_________________________________________________________________
What are our opportunities?
RoutinesWe’re interested in people’s everyday routines and rituals
Stresses
Networks, Connections and Services
We’re interested in understanding the types of networks and services that people in caring
relationships rely on to make things work. Do friends provide more support than families? Do they
have a particularly strong neighbourhood network where everyone keeps an eye out for each
other - what are some of the interesting relationships?. Or do they not have a network at all, and is
this a good or bad thing? Exploring “happy” and “sad” networks will allow us to see how we can
build and support what already exists and also figure out how people who have no current
network can begin to build one around them. We want to understand what are the existing people
resources out there we might draw on, and what are some of the existing interaction out there we
might improve or build on.
Interests and Capabilities
We’re interested in discovering what people are interested in doing and where they get and
maintain motivation. We’re curious about why some people give up their interests, while others
keep going or building them. In particular we want to understand if there’s a gap between
people’s perception of their capabilities and the reality. We also want to map changing
capabilities, interests and ability levels over time to see patterns of change, and be able to
understand if people adjust their aspirations to match their perceived levels of capability. We are
thinking about capabilities in a broad sense - physical, mental, social and emotional capabilities.
We might hang solutions from here ...
Outlook and Aspirations
Understanding the gaps | discrepancies between ... | what is doing well for you?
We want to learn more about how people see themselves, how their outlook impacts their
wellbeing, what influences this, and what motivates them, what are people’s goals, aspirations or
versions of a good life, and how have they shifted or adapted over time. We also want to find out
what people want in their lives, their values, what they do well, and what’s missing.
Changes, Transitions and Directions
We’d like to understand the key moments when things change in people’s lives and the coping
strategies they have. What are the life skills and resources which help people reach the other
side? How do people plan, make decisions and learn from previous experience of pivotal times?
How do people change and adapt in altering circumstances? The event that preceded/caused
change is important but we are more interested in the journey through the period of change. Is
there something about people’s attitudes to change that influences how they deal with it? (fear,
excited apprehensive, wishing for change?) ... what happens at different life stages?
Things to think about BEFORE the meeting
IDentify lead person (drive structure of conversation and focus on carer)
ID support (focus on cared for and keep an eye on time)
The ‘Tea and Cake’ topic guide. Jess and Lou having tea at Rosey’s in Unley.
TOP 3 EXPERIENCES WE HAD WITH PEOPLE• Joining a family caravan holiday for a day helped us
see how an extended family comes together, what
that means for people and what makes it work.
• Having a cigarette with someone despite being a
nonsmoker built rapport and created a whole new
atmosphere.
• Observing how people interacted with professional
services - like cleaners - helped us see the
importance of the chat that happens first.
But isn’t it tricky to have such personal conversations with people?
THINGS THAT MOVED CONVERSATIONS ALONG
“So can you tell me a little bit more about ....”Prompts that dug deeper into the subject, letting unexpected
things rise to the surface.
“How long have you lived here?”“What have you been up to today?”
Using friendly questions that open up further pathways for
conversation.
“Why?”Getting at the meaning behind an action or thought was more
revealing than the original story.
TOOLS THAT HELPED GET AT INTERESTING STUFF
• A blank week planner that helped us get an overview of
the routines and regular connections that people have.
• A card sorting exercise that asked people to identify the
things that it would be wonderful to have more of in their
lives.
• A set of idiom cards gave us a way to discuss people’s
mindset & attitudes.
All these tools helped us to start meaningful conversations
around topics that might have been difficult to bring up
otherwise. Topics like sex and intimacy, estranged families,
planning for death, feeling lonely and stressed.
Dan and Dudley choosing his ‘living great’ cards. Barbara’s ‘living great’ cards.
Susan with Muriel and Norm on their caravan trip.

PAGE 59PAGE 58
Service shadowingWe wanted to get an idea of what happens in the organisations
and services within the ageing and caring space. But we find
that often the bits we learn the most from aren’t the things you
can read about on their website but the day-to-day structures,
interactions and goings on. So we acted as a fly-on-wall to
various services observing, experiencing and understanding.
6 THINGS WE LOOKED OUT FOR1. Rituals and Routines - the daily behaviour and
actions of people that signal acceptable behaviour.
2. Stories - the events that people talk about inside
and outside the organisation.
3. Symbols - the visual representation of the
organisation.
4. Control Systems - the ways that the organisation
and its resources are controlled and distributed.
5. Organisational Structure - the structure defined
by the organisation chart versus the unwritten
lines of power and influence that indicate whose
contributions are most valued.
6. Power Structures - the pockets of real power in the
organisation.
TOP 3 SURPRISING THINGS WE DISCOVERED1. The services we encountered were overwhelmingly
positive about us coming along, and open to thinking
about how to shift practice & improve outcomes.
2. Staff in organisations willingly shared their frustrations,
and had many strategies for doing good work in spite of
rigid systems & structures. Many were hungry for more.
3. Lots of services provide more than what they say they do
in their promotional materials, like the maintenance man
who doesn’t just change light bulbs but provides a good
chat and is beloved by the people he visits regularly.
Appendix
From the top left: Mandy from Carers Support, Salisbury; Ryan with Muriel and Norm’s cleaner @ their home in Unley; The Mens Shed at Edinburgh in
Salisbury; Northern Carers Network Support Group; Dave from Unley Maintenance.
AnalysingAfter meeting such interesting people, we needed to
make sense of it all. First, we described people’s current
situations and realities.Then we worked to understand
their behaviours, motivations, and any contradictions.
Next, we segmented people according to wants &
capabilities. Finally, we generated ideas for what could be.
TOP 3 WONDERFUL WAYS WE CAPTURED OUR EXPERIENCES:• Immediately after leaving a house / chat / service we’d
record ourselves on a dictaphone, dumping all our
recollections and initial thoughts so we didn’t lose any
with time and distance.
• We’d pore over notes and recordings and highlight
people’s language, repetition of concepts, and anything
that was jaring or out of the norm.
• When writing our experiences, we’d capture both the
conversation and context but also group recurring themes
to make it easier to process and compare.
3 LENSES WE USED DURING ANALYSIS:• We compared the existence of relationships and
networks with how much those relationships &
networks contributed to great living.
• We compared people’s openness to adapting to change
with their ability to build new relationships & networks.
• We compared people’s reliance on others with the
reciprocity and balance in their relationships.
The Radical Redesign team on analysis day.

PAGE 61PAGE 60
It’s been good actually - cause it just
shows you how positive I am, through
the cards. Even though I have my ups
and downs it shows that I’ve got that
positive attitude.
Suzanne
Carers and carees are frequently called upon to be
practice subjects for allied health students. Occasionally
we see the outcomes as pie charts and bar graphs in
disability magazines. Sometimes we get trotted out to
be photographed with a politician or new a CEO because
Liz and I present well.
And so it was with some trepidation and wariness that
we responded to the handout from TACSI.
This actually became a therapeutic process and a
reexamination of ourselves and our relationship, and
processes as we articulated them to Adele.
A personal relationship developed between Adele
and us, not surprisingly with the close proximity and
personal exchanges.
It has been a very positive experience.
Mike and Liz
I hope that the experience was of some
help to you and thank you for giving me
the opportunity to be part of the project.
It was just a day in the life of Irene
Barker and I feel so lucky and privileged
to be able to live my life the way I do.
Irene
Reflections from people we met
Appendix
Dear Jess,
We are all sitting back watching our golden oldies now dwindle down in numbers (from the village our parents came from and were the 1st to migrate in the 1950 & 60’s).
From a simple talk around the table at the little cafe with Mary, Helen, David at Hyde Park to come to this so far has been overwhelming for me.
It was not something I was expecting for some-one to take interest in what we are doing out here with our loved ones.
Soula
More people we met
EILEENEileen is sixty-nine. She laughs a lot and tells lots of stories.
She goes dancing every Sunday, reads horror books regularly,
and most evenings plays a bit of Bubble Witch or another
game on Facebook. Through dancing, she met her boyfriend
of four years, a fifty-five year old who shares her love of
ridiculous costumes.
She has three children in their forties with her former
husband, a bricklayer who died twelve years ago.
Eileen has lived with a heart condition since she was
nineteen:“I have sleep apnea and high blood pressure, I had
my first heart surgery at age 19, and a valve replacement
in 1988, and now I have a bulge on my ventricle. I have
osteoporosis. And now the emphysema.” Her boyfriend’s
father died of emphysema, and recently he said “don’t grow
old on me.”
Eileen, by her own admission, is bored. “I don’t do anything
during the week. Hardly see anyone.” She spends most
weekdays at home. She goes to the library every couple of
weeks.
“There is nothing to do in Salisbury. I would like to use the
soccer fields for entertainment. Maybe a comedian.” She says
that she used to be a social committee in the neighbourhood
years ago, but that a neighbour had it shut down.
She and Robert see each other on the weekends, which they
pack with dancing, doing things around the house, and driving
over to visit the youngest of Eileen’s three grown children.
Eileen says that she’d like to have better health, and places
a premium on keeping sharp: “Keeping me brain intact...I
don’t want to get Alzheimer’s.” She would like “people being
concerned about [her] feelings” and dreads the thought of a
nursing home.
CHLOE AND GRACEChloe is 35 yaers old. In 1999, she was in a car accident that
resulted in a brain injury and loss of mobility, restricting her
to a wheelchair. When we met her she happily chatted with us
and came across as very socially capable. Mum Grace later
explained that she has issues with short term memory and
finds herself emotionally disconnected from others.
Grace has been the main carer for her daughter for the last
13 years. She spends all of her time with Chloe except for
when she is with her Dad on the weekends, or Grace’s sister
Deb who looks after her one day a week. Deb registered as
an official carer and so gets paid for her time with Chloe, an
arrangement which Grace thinks is critical for the family’s
ability to have some time each for themselves.
Grace tries to create a world around Chloe that is interesting
and varied. They have students who lodge in their house and
occasionally they have an evening of pizza and Pictionary.
They also have people who work with Chloe from various
university programmes - some of the skills they work on
benefit Chloe, like physiotherapy, but others are less helpful
overall. Initiating activities for her like growing plants actually
causes extra work for Grace - she has to remind her about
watering and care because of Chloe’s extreme memory
deficits - and in fact Chloe gets little from the experience. Also
every time someone new comes to work with them Grace has
to spend energy training them in and getting them familiar
with Chloe’s needs. Still though, Grace’s wish for making
things better would be for Chloe to have more contact with
young people.
They share a number of activities. Grace enjoys writing, which
started with letters to Chloe when she was first in hospital in
a coma after the accident. She has since written a book about
her experiences which she is considering publishing. Chloe
writes poetry and some small pieces of prose with Grace’s
intuitive encouragement. When Chloe meets new people they
give them a poem she has written to enable them to become
aware of the clarity of Chloe’s thoughts. They are also aiming
to publish this collection of work. A highlight that they talked
about was having her poems read at a local cafe and how this
enabled them to meet new people.
Grace also works part-time and enjoys gardening. She knows
that she should see friends more often but sometimes when
she has time to herself she just finds herself needing to ‘glaze
over’ and be by herself. For Grace the physical side of Chloe’s
care isn’t the tough part, rather it’s the emotional aspect of
everything.

PAGE 63PAGE 62 Appendix
JEAN & DEIRDREDeirdre has four people she identifies as her “caring
relationships.” There’s Chuck, a friend who has been recently
widowed and comes over once a week for dinner. And Ivy, a
90 year old widow who lives next door who she occasionally
checks up on. Dalcy, her cousin who she recently put in a
nursing home because of her dementia and Jean, a 90 year
old friend who she sees most days of the week.
Jean and Deirdre met nine years ago at a quilting group.
Initially Deirdre had just been driving Jean and her husband
around a few times a week, but when Jean’s husband passed
away a few years ago there was a need to provide greater
social support for Jean.
Jean is 90 years old and still lives in her own home, which is
7 minutes away from Deirdre. She is part of an online quilting
community and likes to play games on the computer to keep
her mind sharp. Jean uses a walker and cooks for herself
frequently: she particularly likes to make pies.
Deirdre’s week revolves around different social activities
and spending time with Jean. With occasional variation of
weekend activities, Deirdre’s week is very structured. She
“doesn’t do things by halves.” Highlights of her week include
“coffee with the girls” where they “solve the problems of
the world” and spending time with Jean. Deirdre and Jean
go shopping, watch “Letters and Numbers” among other
programs, and do different craft or quilting activities together.
When talking about herself Deirdre tells us, “I come in about
third- my husband, my friends and then me.” Her values are
inherited from her mum who always used to welcome “the
waifs and strays” to dinner. When Deirdre broke her two wrists
a few months ago she was able to rely on Bernie, her kids
and friends to take care of her. A friend came and helped her
shower in the mornings, and Bernie took over the household
duties.
Deirdre’s husband Bernie is “counting down the months” to
retirement. They’re planning to go overseas and Deirdre notes
how she will have to “organise someone to help Jean and
Chuck” at that time.
BERYL AND JONBeryl and Jon are “old worldly and independent.” They get the
bus everywhere and never get lifts from older friends as they
don’t trust drivers who can “barely get into their car.”
Jon was diagnosed with Multiple Sclerosis four years ago.
In the same week, Beryl was diagnosed with bowel cancer.
At the time Beryle wished, “somebody could have come and
talked to me.” Instead she had to “just soldier on” on her own.
Beryl also has glaucoma but she tells me her new pair of
glasses allow her to see better than she has in a long time.
Beryl thinks the secret of old age is “being in the right place
at the right time.” They describe their move to a retirement
village as the “best move we ever made.” When Beryl was
in the hospital two weeks ago Jon could still see her at the
hospital “next door here every morning, every day, twice or
three times.”
In their 50’s they lived in a “fastidiously maintained” house
Victor Harbour where they both worked as carers: Jon with
psychiatric patients and Beryl in a nursing home. They both
say the experience “changed [their] lives” because they “saw
the other side... a lot of suffering... a lot of hardship.”
Currently they’re both “getting on fine.” Jon’s MS is still in its
early stages; he tells me he has constant “pins and needles” in
his feet. They mainly get by on their own with the help of a few
selected services: a shopper that helps with a fortnightly shop
and a cleaner that helps with the bathroom floors.
Beryl’s son is the only other family member who remains in
good contact with them.
Beryl’s hopes to “grow old gracefully and take it slowly and
carry on as best as I can.” She fears being a “burden” to others
and people coming round out of obligation.
LANCELance, by anyone’s standards, has had his share of difficulty
and misfortune in life. Despite everything, he’s upbeat and
friendly and open about his misfortune. He’s also chatty. “I talk
to every man and the tree, the dog, the cat, the budgie, I talk to
everybody!”
Lance is married to Meredith, who he met through a Carer
Cert IV course four years ago. “I’m on my third wife... I wear
them out.” Lance says he and Meredith are “both the same,
we’re both injured but we probably worry about helping other
people than helping ourselves.”
Lance lives off of a disability pension, but he works as a
handyman to “get out of the house. You can sit at home and
be miserable or you can go out and create pain and know
that you’re alive.” Lance used to golf and ride a Harley, but
had to give those up after breaking his back in 2008. He still
watches golf, and he’s replaced the social aspect of it with the
handyman work he does.
Lance has also started writing poetry in the past few years.
When “my sister passed away of cancer and I wrote poems
for her and I stood in front of congregation of 70 people and
I stood there and I [could] talk to them about other people’s
feelings... I wrote poems about how heaven’s got a phone, all
you gotta do is connect it, connect it with your heart.”
After his back injury, he also became more earnestly
interested in WWII research. He has an entire miniature
museum full of Anzac memorabilia and travelled to New
Guinea this year.
He says the visit helped to give more perspective. He spent a
lot of time in the local villages talking to people, and he’s now
involved in sending back medical supplies to the people he
met.
“This is what we’ve always done. We’ve always wanted to go
out and help people.”
JOAN AND DON“They make them tough, Yorkshire girls,” Joan tells us,
and she would know as she grew up there before moving
to Adelaide with husband Don and their young children in
1963. Now their children are all grown up and living around
Australia.
Don has suffered a succession of strokes and health worries
which began soon after his retirement in 1995. For over
10 years they managed and adapted, making use of stuff
like respite and local Council maintenance support, but the
last incident meant Don had to move into full time care in a
nursing home. Joan visits every weekend and despite the fact
that there isn’t much conversation for Don, and he can’t have
a beer, we hear he’s adaptable and making the best of things.
He did used to ask when he was going to be able to come
home though.
Soon he’ll possibly be moving as Joan is going to live down
south with her daughter and grand daughters in a new home
they have bought together. Hopefully Don can be moved to
a place closer to this house. They already know some of the
nursing facilities in that area from when Joan got respite
support, although it’s a different experience now. Joan hopes
that the move will mean more company for Don and he’ll get
to see the grand children and old friends more than he does
currently.
BOB AND JEANFor childhood sweethearts Bob and Jean, “life’s been doctor’s
appointments” for the last few years. It was Bob’s health (a
severe stroke in 1999 and a number of falls since then) that’s
led to a recent move to an assisted living unit. “Last time he
fell, I couldn’t pick him up,” says Jean. It doesn’t feel quite like
home just yet- lots of their furniture wouldn’t fit into the new
space and had to be given away, but they are slowly starting
to explore their surroundings (like bingo, and happy hour), and
Jean has started gardening again (although gardening is also
provided as part of their services).
They struggle sometimes with “being in each others pockets”
and our great living cards revealed they think it’s important
to have time alone, and that you can’t teach an old dog new
tricks. Bob says, “my walking’s not the best - can’t hurry
myself” and so he does need to rely on Jean’s help for the day-
to-day stuff. He’s the designated driver still.
Despite once active networks as keen lawn bowlers and
members at the RSL club, now there are barriers to them
enjoying these activities. They are currently working out
whether their Crows membership will be too much trouble
to manage this year. They do enjoy seeing their daughter and
grand daughter (a trainee nurse) who live locally and speak
with their son, who lives in Melbourne, weekly.
KAREN AND LOU Karen and Lou got together three years ago. Karen is an
environmental law professor. Lou was an accountant for
community organisations and an avid cyclist. He also ran a
successful bike and kayak hire business, and a love of the
environment is something that he and Karen share. In 2007
Lou had testicular cancer. In January 2011, he was diagnosed
with leukemia and spent much of the year in and out of
hospital. Karen took leave from work in Sydney to care for
Lou and has just started a new job now at UniSA. She feels
like she’s lost a lot of her professional network in the past
year. Lou is starting to get back on his feet health wise. He
attends a Men’s Group for people with blood diseases which
he finds helpful, and has a friend who is two weeks ahead with
the same condition who he gets a lot of support and comfort
from. Lou would like to do some worthwhile work but he’s not
sure what yet.

PAGE 65PAGE 64
IRENE Divorce changes things. After having a 3 bedroom house,
caravan and holiday home, Irene now lives in a 1 bedroom
unit. Her divorce was 30 years ago and much has changed
since then. Irene describes her life as anything but over: “I’m
happy with my life, my friends and volunteering.”
Irene’s world is centred around spending time with and
keeping in contact with different groups of people. She speaks
to her son Michael on the phone several times per week,
volunteers 3 days per week at a local senior’s centre and
catches up with neighbours on a daily basis. She also keeps in
contact with friends and family via email.
Irene keeps up with what is going on around her. She does
this by watching the news nightly, checking the news online
and listening to talkback radio. Once a week, she and her
friend Judy travel across Adelaide via buses to different
shopping centres. She loves to get out and about.
Learning new things and sharing skills features strongly in
Irene’s life. At the moment the focus is card making. She has
friends who are also interested in this. Irene buys magazines
and scans the internet for new ideas, products and ways of
doing things.
Good health and being independent are really important to
Irene. She cared for her parents in her home for 13 years and
has an understanding of what that is like. She talked about
there being a positive side as well as a negative one to caring.
Irene plans to find a nursing home to move into if she is
unable to live at home alone. Irene wonders about the impact
of her health on plans that she has for the future - to continue
volunteering, maybe going on an overseas trip and to continue
getting out and about.
EDDYEddy lives in a spotless two bedroom independent living unit.
He and his wife moved into the unit 14 years ago, and he now
lives there alone after his wife died a few years ago. Eddy had
two heart operations when he was 58 which meant he had to
retire. He has a package of services, which includes cleaning
and cooking help, provided by a girl called Sammy. Eddy is
fond of Sammy and “treats her like a grandchild.” He likes
planning his evening meals and doesn’t want to have meals
at the Citizen’s Centre because it would make him “lazy.” He
is also very handy- his most recent project is making folding
wooden card tables. Eddy shows us a trophy that he won
for bowls at a family competition last year, but tells us he
doesn’t really like bowling because you have to go the club
Appendix
“every day.” Eddy lives on the pension and keeps an Excel
spreadsheet of his expenses, which is detailed to the level of
yearly expenditure on clothes and Christmas dinner. Eddy’s
daughter Mandy is an experienced nurse, and comes over for
dinner once a week. He says, “I don’t know what I’d do without
her.” He has a son who lives in Adelaide, but he doesn’t drop in
much as much. Up until this year, Eddy has taken the girls at
the chemist out for dinner once a year. He mentions one friend
he’s fond of - who he helps with financial advice- but says that
friends are only good if you do something with them: “playing
ludo or something- not just sitting around.” “Getting out” is
important to him: “sitting wrapped up in your chair is why
people get depressed.”
PAM & EDDIEPam and Eddie found love on the golf course 12 years ago and
they married soon after. Eddie’s first wife passed away after
a battle with cancer a few years prior to that and Pam’s first
marriage had left her unhappy and unfulfilled. She left to move
in with Eddie.
Around 5 years ago Pam was diagnosed with Alzheimer’s
Disease. Every aspect of Eddie’s life revolves around caring
for Pam. Pam’s scoliosis and decreasing ability to effectively
communicate mean they no longer go to the golf club or
dancing - “We’ve lost connection with all our friends”. Eddie
tends to finish Pam’s sentences. They go to the Para Hills Club
Monday’s and Tuesdays for a few hours. Eddie rarely leaves
Pam’s side.
Eddie also has his own health problems. He has a severe
tremor from a work place accident years ago that has left him
unable to do things like write or prepare food. They get meals
on wheels a couple of times a week and they have a hot meal
at the Para Hills Club a couple of times a week.
For a couple of years now they have received services as
part of a package of care from Helping Hand. 3 mornings a
fortnight a carer takes Pam out to give Eddie some respite. He
usually does the washing, shopping or other things around the
house. A cleaner comes in weekly to take care of the basics
and fortnightly a gardener helps out with cutting the lawn and
tending the front yard - he also makes time for a cup of coffee
and chat with both Eddie and Pam.
Eddie focuses on making the most of life for Pam sometimes
makes it difficult for him to sleep. He worries alot about the
impact he has on the desire or willingness of Pam’s children
to spend time with their mother. Eddie just wishes they would
spend some time with her, take her out every now and then.
He also worries about what might happen to Pam if
something happens to him. A week ago Eddie was rushed to
hospital with pains in his chest. Pam had to come along in the
ambulance. Eddies not sure how it was arranged but Pam’s
son came and collected her. Eddie once promised Pam that
she would never go into a nursing home. He is desperately
trying to avoid this.
MURIEL AND NORMMuriel and Norm have been happily married for around 40
years, live in a nice house, and have a big family of children,
grandchildren, brothers and sisters who often pop in. They
love travelling, and have 2 big maps in their house with pins
showing the places they’ve visited - one of Australia which
they toured in their caravan, the other of the world. Norm
retired early 22 years ago when he developed a degenerative
bone disease which made it harder for him to get about.
Muriel has been caring for him since then and they’ve had to
adjust everything they want to do to whatever pace Norm can
manage.
Last year Norm had a stroke and heart surgery, and since has
needed far greater levels of care. Muriel has tried to make
everything easier, but is stressed by all the extra stuff she has
to do. They managed their first caravan holiday in a year last
week - to McLaren Vale. Norm feels bad that he cannot share
the driving with Muriel anymore, but she seemed happy to
have managed to make the trip at all. They spent the weekend
with her extended family - 3 sisters and their husbands- who
are all getting on in age but still attend the four annual get-
togethers.
Their big love in life is travelling and meeting new people -
they tell many happy stories of making new and temporary
connections on all their travels. They don’t have the social life
that they would like - they don’t often get out in the evenings
though Muriel would like to - and they go mainly to the casino
because its the easiest and safest social option for them.
CATHYCathy ended up for a time helping out a friend, Evelyn, now
aged 92. However, she became stressed out by the experience
which eventually became more than she could cope with.
She met Evelyn many years ago through a distant connection
who introduced them since both are British in Adelaide. For
many years she kept in touch with Evelyn via social situations,
mostly around a shared love of music.
As time went on Cathy could see that Evelyn, who has no
family in Australia, was becoming increasingly frail and
isolated and needed more and more help. Unfortunately she
would not allow strangers into her home - her “haven”. The
only people that Evelyn was prepared to call upon for help
were Cathy and one helpful neighbour.
Cathy found herself driving Evelyn to meals twice a week,
taking her home-prepared food, helping her with shopping,
banking, numerous medical appointments, liasing with her
daughter and her GP, and being almost her only point of social
contact. During this period Evelyn refused to consider asking
for any of the help with shopping or cleaning etc to which
she would have been entitled. When Cathy suggested any
kind of change involving outside help, Evelyn would either
cry and become very distressed and short of breath, or else
go completely silent and freeze Cathy out. Cathy felt that she
was being manipulated into giving so much time to Evelyn. An
additional difficulty was that Evelyn’s hearing had deteriorated
so much that she couldn’t hear the phone or door bell ring.
As a result, Cathy sometimes feared that Evelyn might have
fallen, or could even have died. This possibility always worried
Cathy when she went away on holiday. A couple of times it
became necessary to break into Evelyn’s house to check if she
was still alive, only to discover that she just hadn’t hear them
at the door. Despite Cathy and the neighbour’s best efforts
Evelyn ended up so malnourished at times that she had to be
admitted to hospital, but each time she was discharged with
no additional support and the pattern that got her there was
repeated.
Eventually Cathy went away for a long stretch of time and
during her absence the neighbour managed to persuade
Evelyn to accept some other help. Now she has people from a
local aged-care agency to bring her to the lunch place where
she goes five days a week. A nurse also visits every morning
to check up on her and help her with taking medication. Cathy
seems very relieved to be free of the full responsibility for
Evelyn, and now sees her more occasionally and in a much
more social role.

PAGE 67PAGE 66
JESS DE CAMPOSOCIAL SCIENCE HATWhen I got the job at RR, I explained to
friends and family that it was all about a
new way of getting ideas to address big
social issues: I’d be asking rather than
telling people what they need more of.
The response to this was: ‘Of course.
That makes sense!’ Asking people who
care or are cared for what’s hard and
what’d make life better- it sounds
pretty sensible.
But I don’t think I realised what genuinely
working with people meant until I started
at RR. It means standing outside Woolies,
sharing cups of Greek coffee, helping
CHRIS VANSTONEDESIGN HAT (CO-LEAD)Being let into homes and lives is always
a privilege. The warmth with which
people shared time, stories and tea has
been elevating.
This is the third project I’ve worked on
to improve outcomes for ‘oldies’. Each
with a new team and fresh perspectives.
This feels like the first to get close to the
complexity of caring.
My biggest contribution to this report
has been wrestling the opportunities.
They should be simpler and clearer than
they are, but by Round Four it became
apparent that opportunities to promote
great living are, inconveniently, nearly
everywhere. The next challenge for this
project is to find the best place to start..
SARAH SCHULMANSOCIAL SCIENCE HAT (CO-LEAD)Novel. Surprising. Challenging. Fun.
That’s what it’s felt like to shift from
Working Backwards to facilitating others
to Work Backwards. When Chris and
I first moved to Adelaide to build the
Radical Redesign Team, it was just us.
A few months later, we added Carolyn
to the team - then a secondee from
the state’s child protection agency and
now the Director of Family by Family.
DAN MOHR
BUSINESS HAT“...radical redesign, ey?”
Look & Listen - A myriad of bits to learn
or share that then thicken and lead to
an aha moment: the one highly relevant
line in a research paper, the one crucial
variable in a HACC formula, the moment
of silence in a story.
Interdisciplinary - The wealth of know-
how within the team enriches and
complicates. My inner homo economicus
expands and becomes human again. My
left and right brain play high speed ping
pong of understanding and creating.
Rapid & Precise - Put my best effort into
fleshing out ideas quickly. Make ideas
tangible. Then just start from scratch
again if they don’t fly.
Now I can’t wait to start turning the
bittersweet emotions of aha moments
into solutions that suit people and matter
to them.
Reflections from the team
She transformed our thinking and
whet the appetite - how could we be
more systematic and intentional about
building teams? Instead of trial by fire,
how could we embed a trial-and-error
mindset and enable people to problem-
solve with people, from the ground-up?
Doing so has meant codifying what we
know, figuring out how to transfer our
experiences, and letting go. Ultimately,
we want the new Radical Redesign Team
to take ownership over the project, and
to apply the methods to other social
challenges. That means as we move
forward with the project and enter the
Create phase, I’ll have to keep practicing
stepping back, and helping curate an
environment that’s all about making
ideas tangible and testable. No doubt it
will be novel, surprising, challenging, and
fun.
people prune fruit trees, sitting with
people who are very upset and seeing
their eyes light up talking about family
members who’ve drifted out of their
lives. It’s doing your best to really listen to
peoples stories and what they’re saying.
It means taking off your professional hat
and trying to understand how day-to-day
stuff is for people, before you think of
what could be. People have been warm,
honest, candid and we’ve been privileged
to be invited into their home and lives.
Appendix
ADELE LIDDLE COMMUNITY HATIt’s exciting to visualise our next stage,
which will see us building on hunches,
testing findings, revising what we
think we know about relationships,
and rethinking new ways to treat and
appreciate each other. No doubt once
more massively frustrating, messy,
insightful, somewhat glorious.
JENNA ROMAINESECONDEEIt’s exciting, it’s exhausting, it’s
sometimes frustrating! We work really
closely together and we are learning to
challenge each others ideas more and
more everyday. I am really enjoying
the structure of learning and working
in parallel. Conscious iteration and the
intentionality behind every step in our
process has really pushed us to produce
better work.
The RR process has allowed the space
and given me the tools to do much
more than just scratch the surface when
spending time with people. Spending
time with people in their own context
has enabled us to peer into their lives.
We have got to understand what their life
is really like, what they do, who they do it
with and why they do it.
SANDHYA SHARMADESIGN HATMoving to Adelaide to be a part of the RR
Team feels like, in the words of Beryl and
Jon, being in the right place at the right
time. It’s been surprising, interesting and
touching to be let inside people’s lives
and have the time and space to hear
their stories in their own words.
The best part is these stories don’t just
end with this report. Instead they’re the
starting to point to the next phase where
we will leap into making things tangible.
We’ll prototype, test and repeat until we
find something that resonates and has a
positive impact on people’s lives.
Learning what this thing called ‘Social
Innovation’ is and extending my skills
as a thinker, do-er and designer is an
amazing added bonus.
SUSAN BUTLERDESIGN HATThe RR Team experience is a bit like
lasagne - all the component parts alone
are a little odd, but put them all together
and you get tasty goodness. The team
around me is a bit like the sauce, running
through everything with some spice, and
stickiness. The project, curriculum for
learning and the day to day bits are the
layers of pasta, giving form. The people
RYAN HUBBARDDESIGN HATTACSI’s really ahead of the game. No
one else in the world is working in this
way on this scale. We have a great crew
of people on the design team, and it’s a
pleasure to be part of it.
We’re about to get into making things
real, and that’s always really exciting. We
get to talk to people and have all of these
ideas, which is great fun, but this next
phase is where the rubber meets the
road and we prove whether our ideas are
any good. It’ll be really rewarding to see
tangible results from our work.
SHOUT OUT FROM THE TEAMSpecial thanks to David Kelly for your
warmth, insights, advice and charm.
we meet are the filling - without them
the whole dish would be tasteless - it’s
the people that give the real texture. A
delicious combination - I can’t wait for
dessert - I have a feeling it’s going to be
tiramisu!
One of the most surprising things I’ve
found has been just how emotional it’s
been - from the sadder stories to the
brave and hopeful tales. Joining the
project I expected to get to know many
people, but I never expected to care this
much about them. I thought I’d be more
detached, but all the moments stay with
me and driven me on to discovering
better stuff. And that’s a good thing.

PAGE 69PAGE 68
Get Into Reading by The Reader Organisation (UK)
thereader.org.ukUKOpportunity 1: Shaping minds
WHAT IS IT?The Reader Organisation (TRO) supports regular Get into
Reading (GIR) groups- in residential care homes and older
people’s houses. Facilitators choose books that explore
personal challenges like mood swings or low self-confidence.
About 70 GIR meet once a week all over the world, including
Australia.
WHAT CAN WE TAKE AWAY?How to create and grow alternative kinds of therapy.GIR is a form of bibliotherapy that is more generative than
traditional book clubs where people read selected books in
their own space. GIR facilitators guide people into reading
meaningful literature outloud in an active and social way.
Members of reading groups noticed how the weekly get
togethers improved their wellbeing. Their mood improved and
they felt more inspired in planning their days. Their cognitive
abilities to recollect and concentrate improved as well.
Jämlikhet, Assistans och Gemenskap (Equality, Assistance and Community)jag.seSwedenOpportunity 7: Diversifying help networks
WHAT IS IT?JAG - Swedish for “I” is run, i.e. staffed, by and for people with
multiple physical or intellectual impairments. Members hire
their own care “personal assistant” (PA) and network through
JAG.
The JAG cooperative has 400 members in the Stockholm area.
Together they employ some 3,000 personal assistants (PAs).
About 40 persons work directly for JAG. The JAG cooperative
disposes of nearly 70 million Euro (c.$100 million) per year
from state funded personal care budgets. Members use it
to organise their personal assistance and to resource JAG
support staff. Personal assistants come from the circles of
family, friends or JAG’s recommended professional carers.
WHAT CAN WE TAKE AWAY?How to blend care from family, friends and professionalsJAG is a model that enables members to build their own care
networks with advice from other co-op members. They pick
suitable assistants and pay them from their personal budgets,
which they spend at their discretion. That means members
can use the funds to support their friends and family for their
efforts or attract PAs from outside their personal network. The
personal blend of PAs, friends and family has been working
for members for over 15 years.
Evaluations suggest that the quality of life is higher than
in institutional settings at lower cost. Whether the model
can inspire solutions from the context of disability care in a
different political context remains to be seen.
International examples
Appendix
Planned Lifetime Advocacy Network (PLAN)
plan.caCanadaOpportunity 3 - Activating Family & Friends
WHAT IS IT?PLAN is a network led by families who want to secure a future
for family members of all ages living with disabilities. PLAN
was founded by parents who acknowledged that one day they
would need to pass on their caring responsibility to someone
else. It operates throughout Canada and has inspired over 40
similar organisations across the world. PLAN wants everyone
to have access to a good life: (1) friends and family who
love them, (2) a place of one’s own, (3) financial security, (4)
participating in decision making, (5) and the ability to make a
contribution to society.
WHAT CAN WE LEARN?How to build capabilities through trainingCourses and workshops spread the best ways to develop and
maintain a personal network for children with disabilities, and
teach how to structure finances and wills.
How to build connections through new rolesCommunity Connectors are the linchpins who help families to
create and expand their networks. They help family members
to make connections with new people. Once these friendships
are built, the Community Connector formalises a group of
three to five people who help ensure a safe and secure future
for their child or sibling.
How to maintain connections onlineTyze Personal Networks (tyze.com) is a social networking
service that revolves around a specific person and their
network. Members use shared calendars, goal and task lists,
stories and photos to build community, share information and
coordinate support for someone needing care.
It remains to be tested whether interactions and supporting
systems used by PLAN can be built that help plan a good life
for people in late adulthood.
WHAT CAN WE TAKE AWAY?Sustainable Business Model. Members contribute to PLAN in kind as well as financially. All
member families pay the network a small annual subscription
fee of $29 to use general planning tools and to be connected
to other families. Families that tap into personalised services,
such as the Community Connector, contribute through higher
valued Lifetime Memberships. Participants of specific courses
pay fees that recover the running costs. PLAN’s business
model is an example of a network people are willing to
support financially in return for the value that they receive.

PAGE 71PAGE 70
The Cohousing Company
cohousingco.comLocation: USAOpportunity 4 - Starting Relationships
WHAT IS IT?The Cohousing Company (“TCC”) is an architecture firm that
specialises in helping people of all ages design and build their
own cohousing communities. It acts (1) as the facilitator of
the participatory design process that enables people to build
the community together “not brick by brick, but decision by
decision”, and (2) as advisor on building and architectural
issues including on how to design sustainable and affordable
houses.
TCC has advised over 50 cohousing communities across
the US (5 specifically for older residents such as Silver Sage
Village in Boulder, Colorado).
Cohousing communities are similar to other types of
intentional communities like co-ops or communes but differ
in that common areas, such as kitchen or gardens, are
interspersed among private homes. The aim is to invest in
a socially rich and interconnected community where people
are happy to give each other a helping hand. They are self-
managed with a non-hierarchical structure and consensus
decision-making by all residents.
TCC’s approach draws from the cohousing communities
first designed in Denmark in the 1960s. Communities have
been developed by local people in many countries, most
in Northern Europe. There are more than 300 cohousing
communities (about 70 mixed-generation and 230 senior
cohousing) in the Netherlands alone.
TCC’s services to senior co-housing communities include
specific design features that let people age in their
community, such as barrier-free access, and future-proof
support features, such as common guest rooms for relatives
or nurses to live.
WHAT CAN WE TAKE AWAY?
How to create and build community. Know-how about designing a co-housing development with a
strong community spirit tends to dispersed by word of mouth.
TCC has aggregated its lessons learnt from facilitating the
collaborative development process and created a blueprint. Its
set of interactions has turned diverse groups of like-minded
people into residents that are passionate about having a
community rich in relationships. Our hunch is that a similar
blueprint can be prototyped for the Australian context and be
used to spread co-housing commiunities for older people. We
can learn from examples like Apartments for Life in Sydney.
Sustaining Community. Co-housing communities that endure keep running based on
the principles of their development: decisions by consensus
and non-hierarchical organisation. Residents look out for each
other and help each other to stay in the community for as
long as they wish for. Enduring communities with seniors are
run flexibly as people’s circumstances change. Private homes
and common spaces can be redesigned and paid helpers can
top up help among residents. Yet we wonder whether the
communities can also run on an intergenerational compact
between younger, newer members that can give a helping
hand and older, decorated members of the community who
can contribute in a different way.
International Examples
Appendix
thegreenhouseproject.orgUSAOpportunity 6: Caring Services
WHAT IS IT?A Green House home is an independent, self-contained
home for 6-12 people, designed to look like a private home
or apartment in the surrounding community. Each person
who lives in a Green House home has a private bedroom and
bathroom, opening to a central living area and an open kitchen
and dining area. Elders, as residents are called, share meals at
a common table.
The Green House concept was developed by Dr. Bill Thomas,
an expert on geriatric medicine and elder care, as a model
for residential care that rethinks the philosophy of care,
architecture, and organisational structure of long-term care.
There are 113 Green Houses in 29 states with 227 in
development. Each home is staffed by a team known as
Shahbazim (which is a midwives of elderhood). The staff
has core training as certified nursing assistants and share
personal care, meal preparation, and light housekeeping
responsibilities among their team.
The elders and Shahbazim collaborate to create a daily routine
that meets elders individual needs. If they wish, elders
can help cook, and assist around the home. There is no
predetermined routine. The aim of shahbazim is to facilitate
independence and the ability to pursue individual interests.
WHAT CAN WE TAKE AWAY?How to create caring services Green Houses have clear principles operating in their homes.
[See: edenalt.org/our-10-principles]. The principles put good
outcomes for the elders at the forefront of any interaction.
Green Homes reinforces these values in the daily interaction
through peer observation and feedback. New Shabahzim go
on a short but intense course on the principles, and structured
training on the job with mentor Shahbaz. What if we took
the Shabahz role out of residential settings and into people’s
homes?
Sustainable model for enabling services. The Green House homes model is built around supporting
direct care workers in their interactions with elders. A
clinical support team of nurses, social workers, therapists,
physicians, activities and dietary professionals, and
pharmacists assist the Shabahzim. This reversal of roles with
resources geared towards direct carers creates a model of
high quality care that is sustainable. Shabahzim constantly
learn from mentors on the job, have longer care times and
engagement with elders. This in turn ensures a high quality of
personal care that is financially viable. Turnover of staff is only
10%, which adds to the sustainability of the care model.
Green House Nursing Home Alternative

PAGE 73PAGE 72
What we readABOUT OUTCOMES
Traditionally, medical literature talks
about good outcomes for older people
in terms of having less bad health: less
illness, depression or disabilities,21 or in
terms of being independent.22
In the field of developmental
psychology, outcomes focus more
on social and emotional wellbeing for
individuals: meaningful relationships
and community involvement, making
a contribution, autonomy, control in
decision making and experiencing
positive emotions.23
SO WHAT?The people we met talked about great
living as having friends, being close, and
planning and learning new things. The
literature focuses on good outcomes
for individuals, whilst we think good
outcomes will focus on people’s
relationships and networks, and how
they can grow and develop over time.
ABOUT BEHAVIOURS
George Valliant’s Aging Well emphasises the importance of being
helpful to those around you, and
continuing to make new relationships
while deepening old friendships. It
also highlights retaining your sense
of humour and capacity for play while
accepting the “indignities of old age.”24
Freund and Baltes’s framework
explores differences in people who find
new ways to pursue their interests as
their capabilities change, from those
who forgo goals once things become
harder as they get older.25 Those who
found ways to adapt were more likely
to display attributes the researchers
define as successful ageing, like having
a positive outlook and feeling satisfied
with life.
SO WHAT?What if we can help others to improve
their ability to adapt as they get older
- and how might this help them get to
great living?
ABOUT NETWORKS
Knoke and Kuklinsky introduced us to
multiplexity: where people share roles
within a caring network. More resilient
networks spread caring roles across
more people, creating less pressure
on one person.26 Antonucci’s concept
of reciprocity is also useful: the idea of
both give and take, or a two way street,
within caring relationships.27
SO WHAT?This work helped us to see that we
need to look beyond the core caring
relationship to see what role the
broader network plays.
ABOUT CARING
Michael Fine writes that caring is ‘a
complex cluster of social activities,
behaviours and dispositions.’ Rather
than burden, as it’s often seen, he
says care is a ‘fundamental condition
of human experience.’28 Care comes
from the Latin, caritas, which means
to love. Fine says that rather than
something ‘done’ to you, care should be
defined more broadly, and be a social
process.
SO WHAT?Fine’s work gave us a lens through
which to look at perceptions of care.
Could we see care as a shared activity
rather than unidirectional?
2006-07 of HACC compared with Residential High Care Level. Data
in: Commonwealth of Australia Treasury, 2009, Australia’s Future Tax
System: Detailed Analysis, Vol. 2, p. 634.
17. Access Economics, 2010, The economic value of informal care in 2010,
Report for Carers Australia, p. i.
18. Productivity Commission 2011, Caring for Older Australians, Vol. 1, p. XXII.
19. Australian Bureau of Statistics, 2011, Household Income and Income
Distribution 2009-10, p. 32.
20. Chappell, N.L. & Reid, R.C. 2002, ‘Burden and well-being among
caregivers: examining the distinction,’ The Gerontologist, 42(6).
21. Burgener, S., Twigg, P. & Popovich, A. 2005, ‘Measuring psychological
well-being in cognitively impaired persons,’ Dementia, Vol. 4 (4).
22. Ryff, C. D. 1989, ‘Happiness is everything, or is it? Explorations on the
meaning of psychological well-being,’ Journal of Personality and Social
Psychology, Vol. 57(6).
23. Valliant, G. 2002, Aging Well: Surprising Guideposts to a Happier Life from
the Landmark Harvard Study of Adult Development, Little Brown, p. 346.
24. Freund, A.M. & Baltes, P.B. 1998, ‘Selection, optimization, and

PAGE 75PAGE 74
Freund, A.M. & Baltes, P.B. 1998, ‘Selection, optimization, and
compensation as strategies of life management: correlations
with subjective indicators of successful aging,’ Psychology and Aging, 13(4), pp. 531-543.
Roos, N.P. & Havens B. 1991, ‘Predictors of Successful Ageing:
A Twelve-Year Study of Manitoba Elderly,’ American Journal of Public Health, 81(1), pp. 63-68.
Rozario, P.A., Morrow-Howell, N. & Hinterlong, J.E. 2004, ‘Role
Enhancement or Role Strain: Assessing the Impact of Multiple
Productive Roles on Older Caregiver Well-Being,’ Research on Aging, 26 (4), pp. 413-428.
Ryff, C. D. 1989, ‘Happiness is everything, or is it? Explorations
on the meaning of psychological well-being,’ Journal of Personality and Social Psychology, 57(6), pp. 1069-1081.
Smerglia, V.L. & Deimling, G.T. 1997, ‘Care-related decision-
making satisfaction and caregiver well-being in families
caring for older members,’ The Gerontologist, 37(5), pp. 658-
65.
Stoltz, P., Udén, G. & Willman, A. 2004, ‘Support for family
carers who care for an elderly person at home - a systematic
literature review,’ Scandinavian Journal of Caring Sciences,
18(2), pp. 111-9.
Wright, D. & Aquilino, W. 1998, ‘Influence of emotional support
exchange in marriage on caregiving wives’ burden and marital
satisfaction’ Family Relations, 47 (2), pp. 195- 204.
ARTICLESAhmed, N. & Rees Jones, I. 2008, ‘Habitus and Bureaucratic
Routines: Cultural and Structural Factors in the Experience
of Informal Care: A Qualitative Study of Bangladeshi Women
Living in London,’ Current Sociology, 56(1), pp. 57-76.
Antonucci, T.C., Sherman, A.M. & Akiyama, H. 1996, ‘Social
Network, Support, and Integration,’ in Birren, J.E. (ed.),
Encyclopedia of Gerontology: Age, Aging and the Aged,
Academic, San Diego, pp. 505-15.
Aronson, J. 1998, ‘Lesbians Giving and Receiving Care:
Stretching Conceptualizations of Caring and Community,’
Science, 21(5), pp. 505-519.
Bowling, A. & Dieppe, P. 2004, ‘Thoughts for today: What is
successful ageing and who should define it?,’ British Medical Journal, 331(7531), pp. 1548-51.
Burgener, S., Twigg, P., & Popovich, A. 2005, ‘Measuring
psychological well-being in cognitively impaired persons,’
Dementia, 4 (4), pp. 463-485.
Chappell, N.L. & Reid, R.C. 2002, ‘Burden and well-
being among caregivers: examining the distinction,’ The Gerontologist, 42(6), pp. 772-780.
Cox, E.O. 2006, ‘Coping with late-life challenges: Development
and validation of the care-receiver efficacy scale,’ The Gerontologist, 46(5), pp. 640-649.
Fine, M. 2004, ‘Renewing the Social Vision of Care,’ Australian Journal of Social Issues, 39 (3), pp. 217-232.
Levy, B., Slade, M., & Kavi, S. 2002, ‘Longitudinal Benefit of
Positive Self-Perceptions of Aging on Functional Health,’ The Journals of Gerontology, 57 (5), pp. 409-17.
Lyonette, C. & Yardley, L. 2003, ‘The influence on carer
wellbeing of motivations to care for older people and the
relationship with the care recipient,’ Ageing and Society, 23(4),
pp. 487-506.
Appendix
Bibliography BibliographyBOOKSDurkin, K. 1995, Developmental social psychology: from infancy to old age, Blackwell Publishers.
Emerson, R., Fretz, R. & Shaw, L. 1995, Writing ethnographic fieldnotes, The University of Chicago Press, Chicago.
Fine, M. 2007, A Caring Society? Care and the Dilemmas of Human Service in the 21st Century, Palgrave Macmillan.
Forbat, L. 2005, Talking About Care, The Policy Press, UK.
Friedan, B. 1993, The Fountain of Age, Vintage, London.
Knoke, D. & Kuklinski, J. H. 1982, Network Analysis, Sage,
London.
Pascale, R., Sternin, J. & Sternin, M. 2010, The power of positive deviance: how unlikely innovators solve the world’s toughest problems, Harvard Business Press, Boston.
Piercy, K. 2010, Working with Aging Families, W.W. Norton,
New York.
Seligman, M. 2011, Flourish: A Visionary New Understanding of Happiness and Well-being, Free Press, New York.
Ritchie, J. & Lewis, J. 2003, Qualitative Research Practice: A Guide for Social Science Students and Researchers, Sage
Publications, London.
Ybema, S., Yanow, D., Wels, H. & Kamsteeg, F. (eds.) 2009,
Organizational Ethnography: Studying the Complexity of Everyday Life, Sage, London.
Valliant, G. 1995, Adaptation to Life, Harvard University Press,
Cambridge, Massachusetts.
Valliant, G. 2002, Aging Well: Surprising Guideposts to a Happier Life from the Landmark Harvard Study of Adult Development, Little Brown, New York.
REPORTSAccess Economics, 2010, The Economic Value of Informal Care in 2010, Report for Carers Australia, October.
Department of Health and Ageing, 2003, Review of Pricing Arrangements in Residential Aged Care, Canberra.
Department for Health and Ageing, 2010-11, Report on the Operation of the Aged Care Act 1997, Canberra.
Demos, 2007, Coming of Age. Available: http://www.demos.
co.uk/projects/comingofage/
Government of South Australia, 2006, Improving with Age: Our Ageing Plan for South Australia.
McGrath, D. 2011, ‘Carer support is not only about Respite.’ Presentation to Transforming Respite Summit, Morphettville,
SA.
Productivity Commission, 2011, Caring for Older Australians,
Report No. 53, Final Inquiry Report, Canberra.
South Australian Department of Families and Communities,
2006, SA Carers Policy.
IF YOU WANT TO KNOW MORE ABOUT WHERE THIS PROJECT CAME FROMSchulman, S. and Vanstone, C. (2011), How can we improve outcomes for caring & cared for older people? Ageing Project
Paper 00. Available: http://www.tacsi.org.au/our-projects/
caring/
Schulman, S. and Vanstone, C. (2011), If you could improve outcomes for one group of older people who would it be?
Ageing Project Paper 01. Available: http://www.tacsi.org.au/
our-projects/caring/

PAGE 77PAGE 76
GlossaryBehavioursWhat people say, feel, think and do.
Carer: official definitionsAccording to the National Respite for Carers Program
(NRCP), a carer is defined as “a person who, through family
relationship or friendship, looks after a frail older person or
someone with a disability or chronic illness. Carers look after
these people in the community or in their own homes”
(DoHA, 2006).
Carers Australia definition: Carers provide unpaid care and
support to family members and friends who have a disability,
mental illness, chronic condition, terminal illness or who are
frail aged.
Carer: Radical Redesign definition 1) A family member, friend or neighbour who provides
assistance in the provision of support (physical, emotional,
social or other) to another.
2) Being there for another person - playing a role and
contributing to great living.
Cared forPerson receiving support (including physical, emotional or
social support) from another.
Co-designWorking with people, practitioners and policymakers to
develop new kinds of solutions.
Consumer Directed Care
A system where care recipients and their carers have
greater control over the design and delivery of the care and
services they receive. Consumers are allocated a budget
and are able to ‘buy in’ services that meet their care needs.
Internationally there are several models currently in practice
with varying guidelines and boundaries around the amount
and management of funds and the types of services eligible to
be purchased.
DevelopmentalThe process of growing, progressing and intentionally
changing over time.
EthnographyExperiencing a day in the life of an individual, caring
partnership, group and culture.
HACC (Home and Community Care Program)Federally funded initiative. Local government, community
organisations, religious or charitable bodies, state and
territory government agencies and private (for profit)
organisations are eligible to receive HACC money to deliver
services. The HACC program supports older Australians,
younger people with a disability and their carers.
InteractionEngagement of individuals or groups with services,
programs or each other.
OutcomeThe end results; what changes for people and for systems.
PrototypingTrying out new ideas that have been co-created with carers
and those they care for.
Positive deviants
Individuals or groups of people who are doing well or thriving
despite the situation they are in. Characterised by specific
behaviours or sets of behaviours.
SolutionsA set of interactions and experiences that spread as
principles, platforms, organisational models, and programs.
ThrivingIndividuals who are thriving are actively developing
aspirations, capabilities, relationships and achievements.
They have lives where they feel good and in-control.
Working Backwards approachProcess used by the Radical Redesign team. Draws on
design thinking, social sciences, community development
and business to create solutions that enable change in
peoples lives.
Appendix
SOUNDING BOARD
Thanks to the Sounding Board for being critical friends.
Brenton Caffin Chief Executive, The Australian Centre for Social Innovation
David Kelly Deputy CEO, The Australian Centre for Social Innovation
Michael FineAssoc Professor and Head, Department of Sociology,
Macquarie University
Jane MussaredGeneral Manager Innovation, ACH Group
David CaudreyExecutive Director, Disability, Ageing and Carers
Karen GroganChief of Staff, Mark Butler MP
Megan CorlisDirector of Research & Development, Helping Hand Aged Care
Peter SparrowChief Executive, Carer Support & Respite Centre
Peter TsokasChief Executive, Unley Council
John HarryChief Executive, Salisbury Council
Greg MackieExecutive Director, Ageing SA Health
PEOPLE
Thank you to the people in Unley and Salisbury for letting us into your lives.
Glad
Leon
Bob and Jean
Norm and Muriel
Julie
Soula, Mick and Thia
Helen
Lou and Karen
Eddie and Pam
Susan, Wayne and Naomi
Eddy
Joan and Don
Pat and Dave
Beryl and Jon
Barbara
Mike and Liz
Eileen
Irene
Eleanor
Lance and Meredith
Helen and Jayne
Suzie
Deidre
Mary Skaltas
Contributors

PAGE 79PAGE 78
SERVICES
Thank you to the following people and services for your willingness to have us hang around and for being open in sharing what you do.
From Office of the Ageing, Department for Communities and Social Inclusion:Christopher Birtwistle-Smith
Myrana Wahlqvist
Lisette Clairdge
UnleyFranco Parenti - Aged Care Alternatives
Deb Oliver - Unley Council
Celine Luia - Unley Council
Chris Murray - Unley Council
Unley Council Home and Community Care team
Luke Say - ECH Inc.
Tracey Davis - Mental Health Coalition of SA
Mandy Toczek McPeake - Manager Carer Services,
Carer Support
Donna Musarella - PA to CEO, Carer Support
Mel Burge and Anne Higginson - ACH Group ‘Wyatt Holidays’
Antonietta Cardinale - Ethnic Ageing Officer,
Co-ordinating Italian Committee Inc.
Marjon Martin - Community Centre Co-ordinator,
Adelaide City Council
Kate Grivell - Community Centre Co-ordinator, Unley Council
Rima Chahoud - Team Leader Respite,
Mental Illness Fellowship
Simon McMahon - Programs Manager Respite,
Mental Illness Fellowship
Maureen Lewis -Team Leader of Family Support Services,
Mental Illness Fellowship
Ben Heyward - Program Manager for Education Awareness
and Training, Mental Illness Fellowship
SalisburyMaria Ross and Team - Northern Carers Network
Sue Phyllis - TAFE SA
Lyndal Gerrard - Access To Home Care Adelaide Metro
Pam Pindral - City of Salisbury Healthy Ageing & Access
Division
Craig Oswald - ‘The Shed’
Shannan Davis - ‘Gone to Seed’ Gardening Project
Bev Brooker and Team- Home Support Service
Robyn Mercierre and Team - Jack Young Centre and the Para
Hills Centre
Ashling O’Boyle - Living Well Program (ECH and City of
Salisbury)
Gail Sloane - Lyell McEwin Hospital Discharge Office
Megan Corlis - Helping Hand Aged Care
Sue Leckie - Northern Collaborative Project
Lui DiVenuto - Eastern Collaborative Project
Contributors
Appendix
We love feedback!Thanks so much for reading this report. Like versions of great living we discovered, we want this document to improve and evolve as more people add their perspective and insights.
Please share this report in any way that works for you, and feel free to use the questions below as discussion points. We’d love to hear about what’s been useful, and any questions the report has raised for you: in your work or current life situation.
Here’s some discussion starters. More information and opportunities to contribute your thoughts can be found at: tacsi.org.au/caring
• Which opportunity area is most exciting? Why?• Do you disagree with any of our findings? Tell us more.• What are some of the challenges or barriers we
haven’t anticipated?• What have we missed? • Or perhaps you have stories or ideas to support
our learnings? Please share.
Send us an email at [email protected]

People of all ages will live better lives when we succeed in bringing elders back to the heart of our society.
U.S. News and World Report, “The Greening of Aging.” Available:
http://www.usnews.com/usnews/biztech/articles/060619/19leader.htm
The Australian Centre for Social Innovation exists to identify and support the innovative ideas, methods and people that will contribute to and accelerate positive social change. tacsi.org.au
TACSI’s Radical Redesign team blends design thinking, policy thinking, social science and business to solve social problems and demonstrate new ways of working with and for social services. tacsi.org.au/design
TACSI’s Ageing & Caring project aims to improve outcomes for older people in caring roles and relationships. The project brings together TACSI; South Australia’s Office of the Ageing; the City of Salisbury; the City of Unley; ACH Group, and Helping Hand Aged Care. tacsi.org.au/caring
Contact [email protected]
© The Australian Centre for Social InnovationPublished February 2012Under Creative Commons Attribution 3.0Please share

PAGE 82