Embed Size (px)
Citation preview
Los Angeles Society Of PathologistsLos Angeles Society Of Pathologists
Dr. Shobha Castelino PrabhuDr. Shobha Castelino PrabhuLoma Linda University Medical CenterLoma Linda University Medical Center
June 12, 2007June 12, 2007
CASE 1CASE 176 year-old gentleman
Status post right parotidectomy 1 year ago for a
“rare tumor”
Presents with a right 5 cm pre-auricular and a 3 cm post-auricular mass - both are firm and immobile
Right facial nerve partial paralysis with tingling sensations
Fine needle aspiration was performed
Followed by excision of both masses
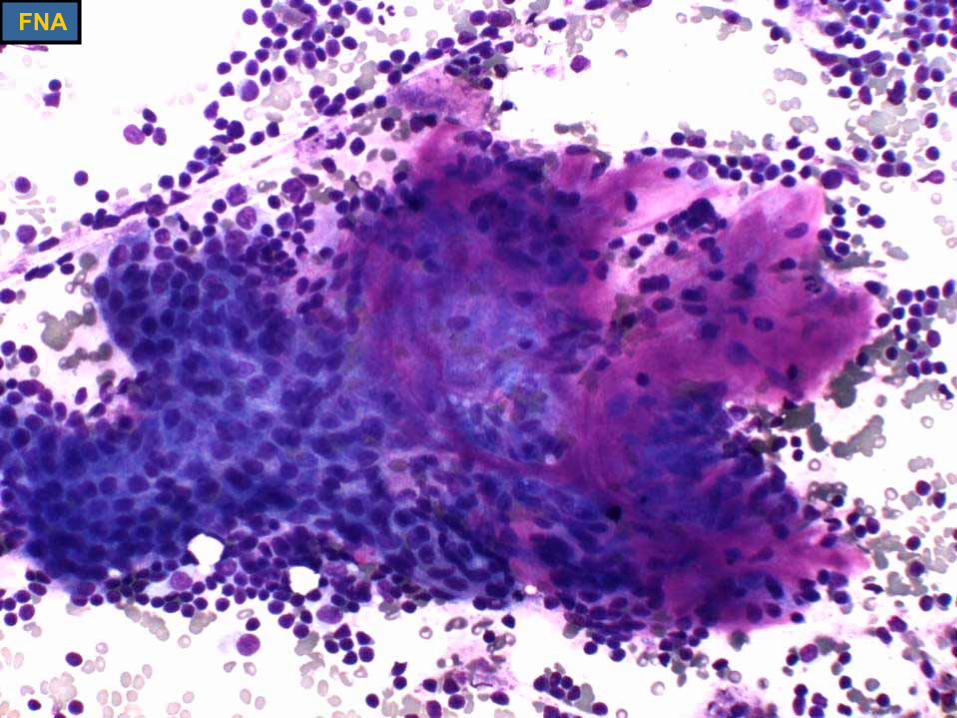
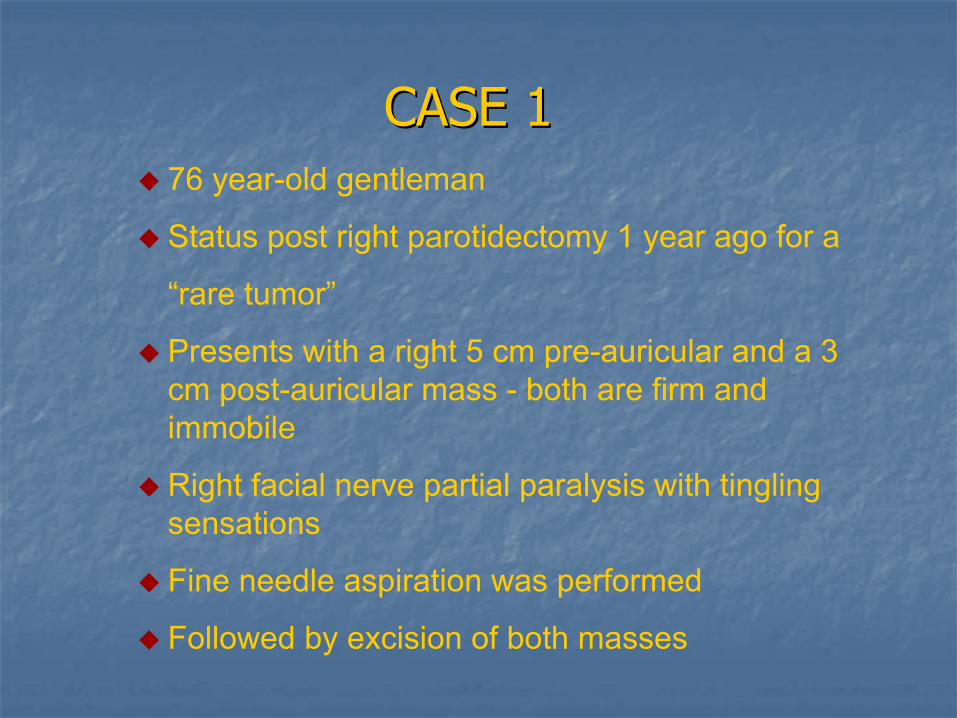
FNA
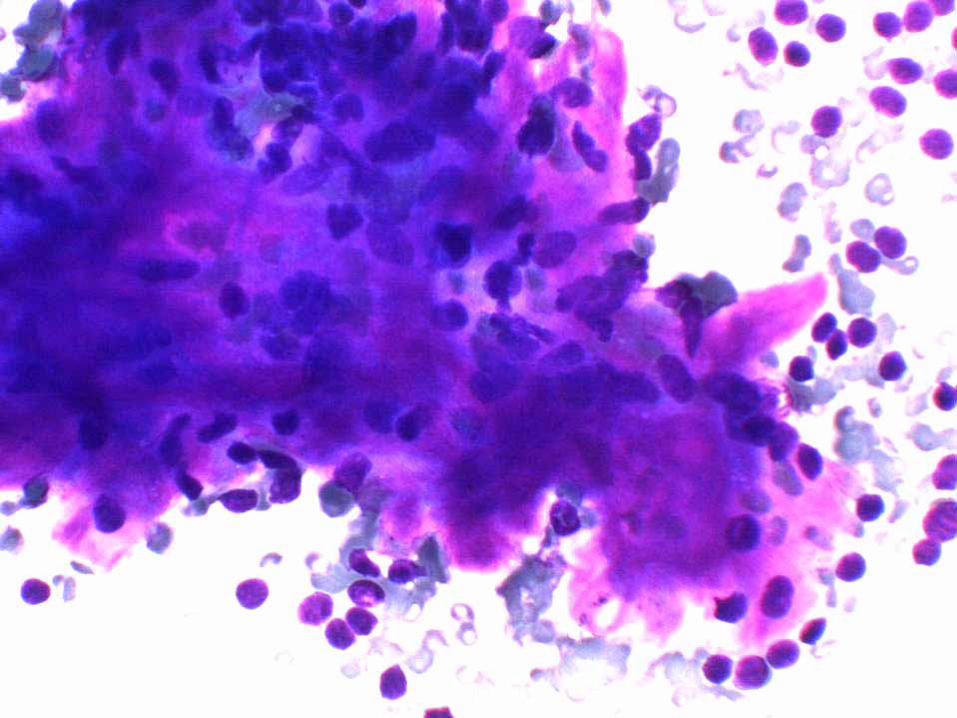
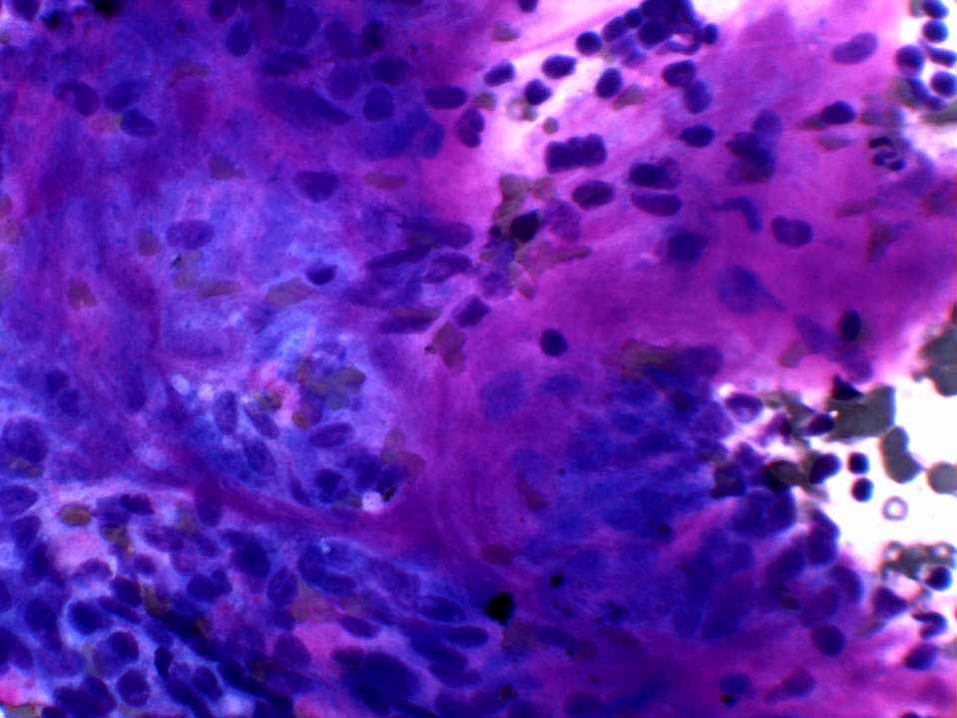
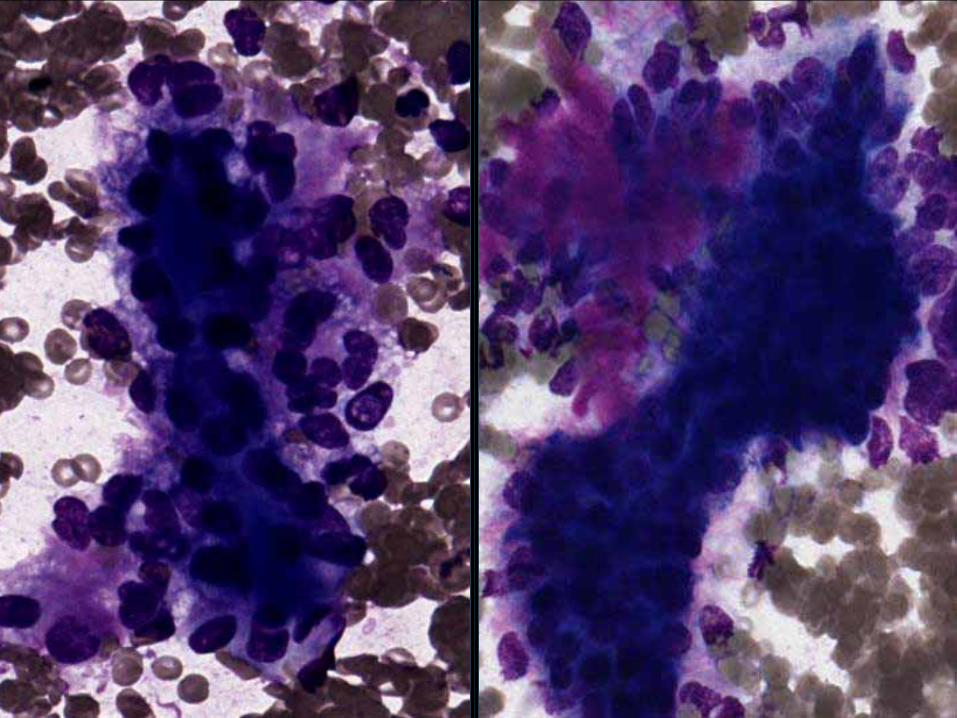
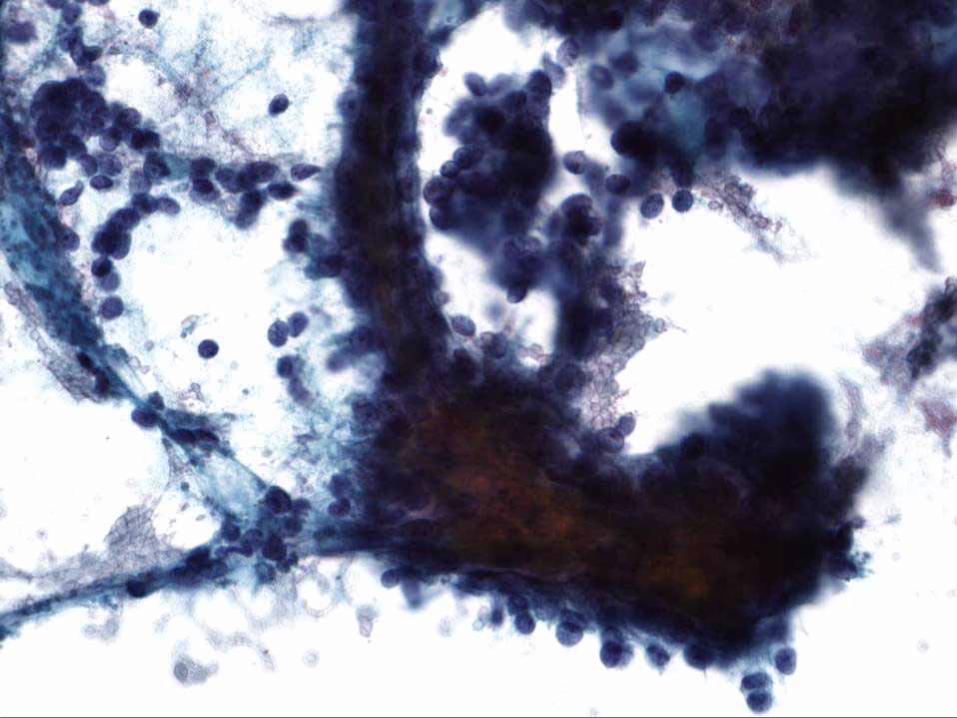
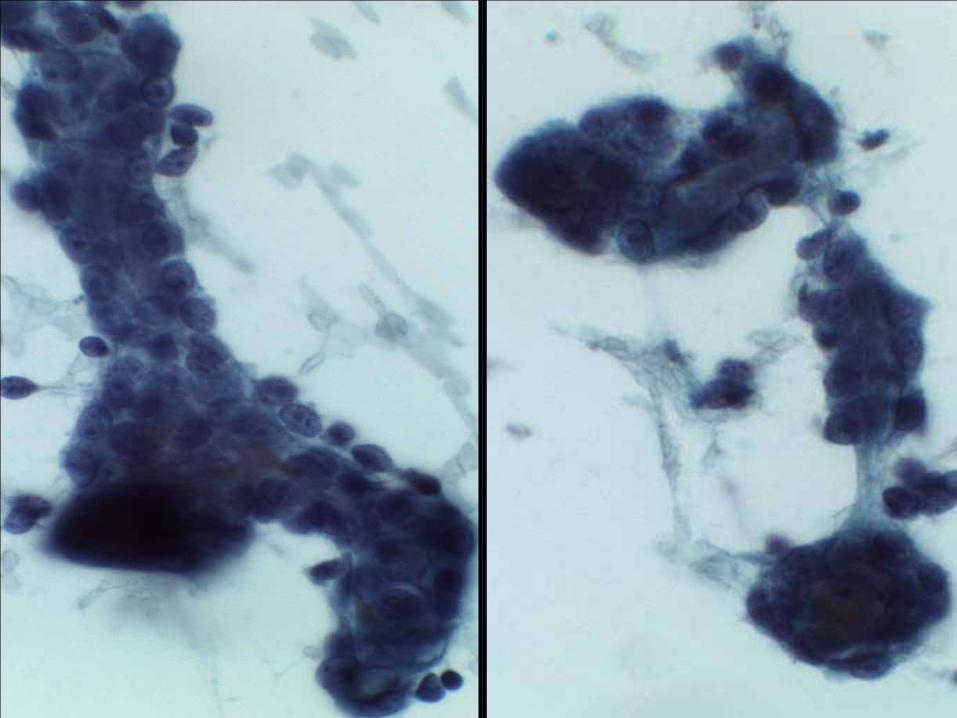
FNA CYTOLOGYFNA CYTOLOGY
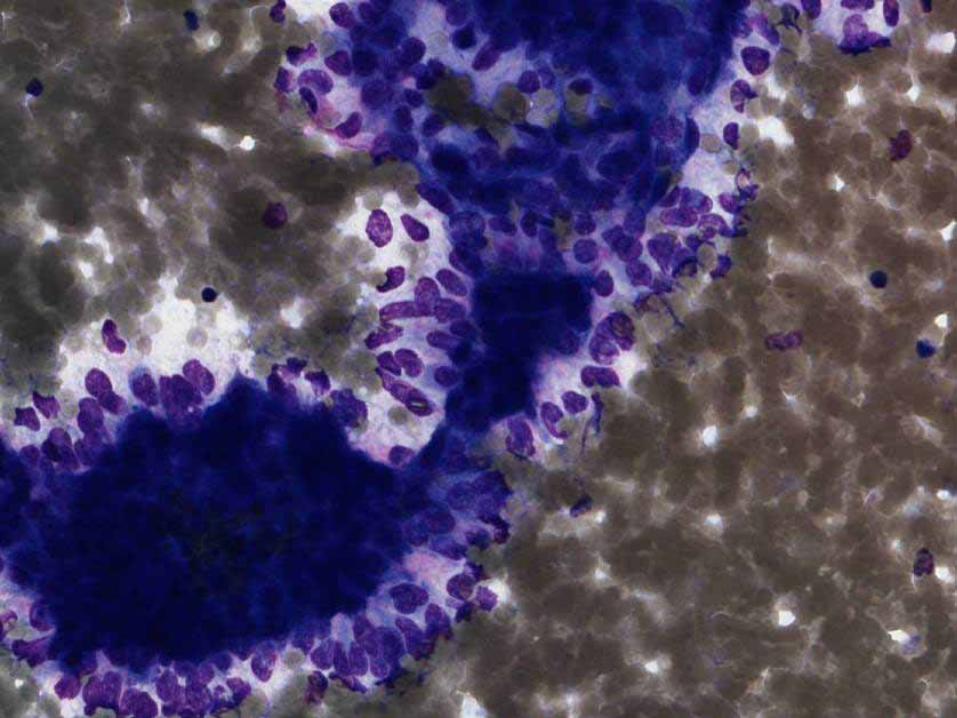
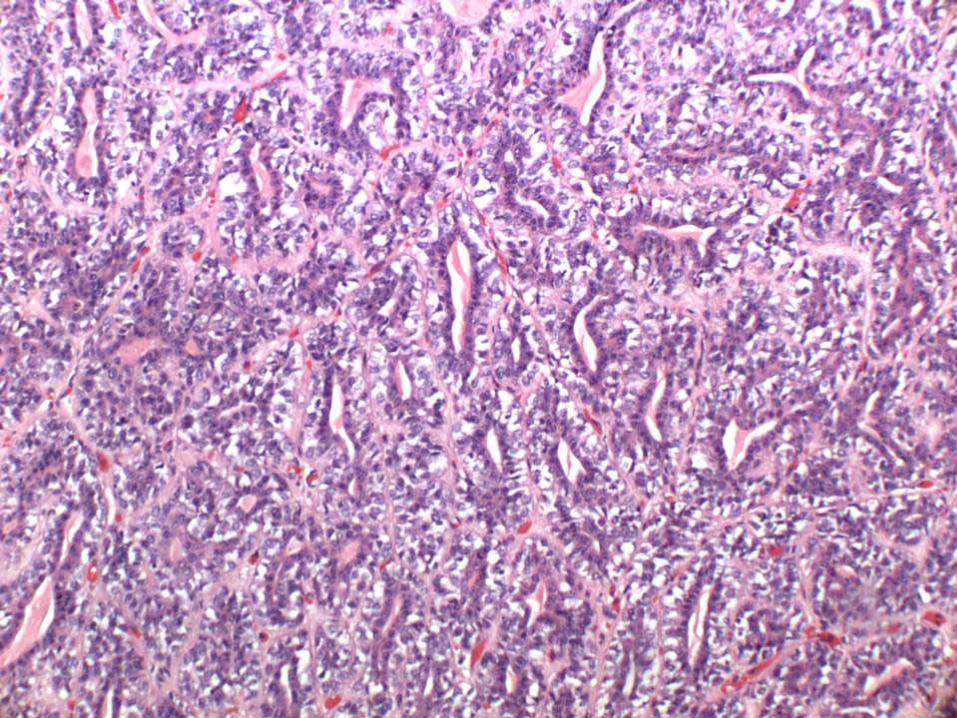
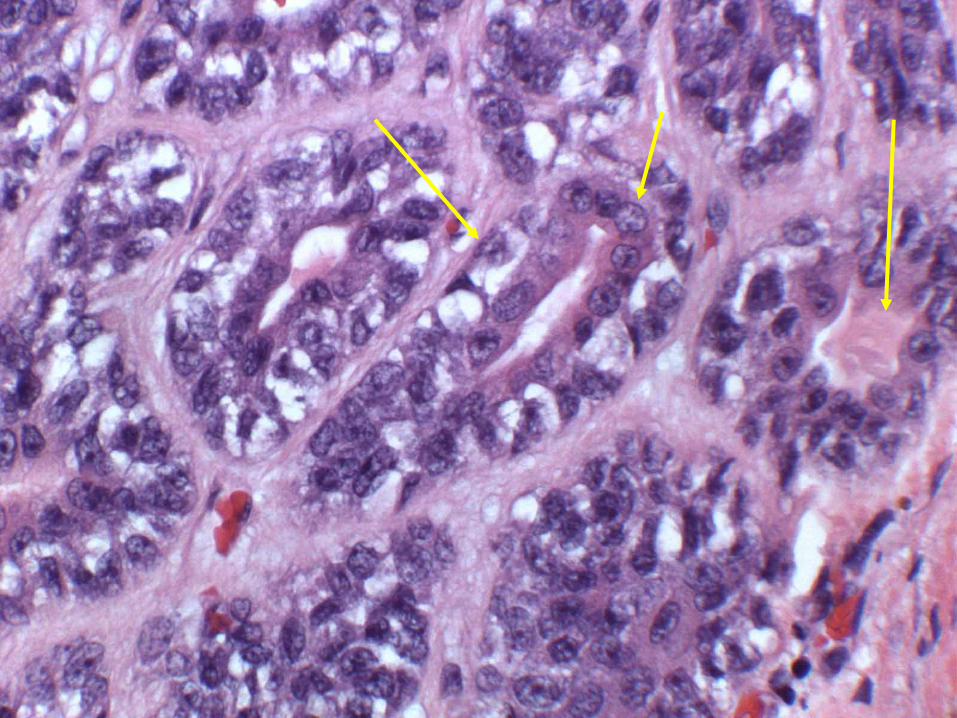
Biphasic cell population around tubule-like structures: inner small dark cells
outer large pale cells
Dense refractile ground substance within tubules
Acellular myxoid/hyaline material present
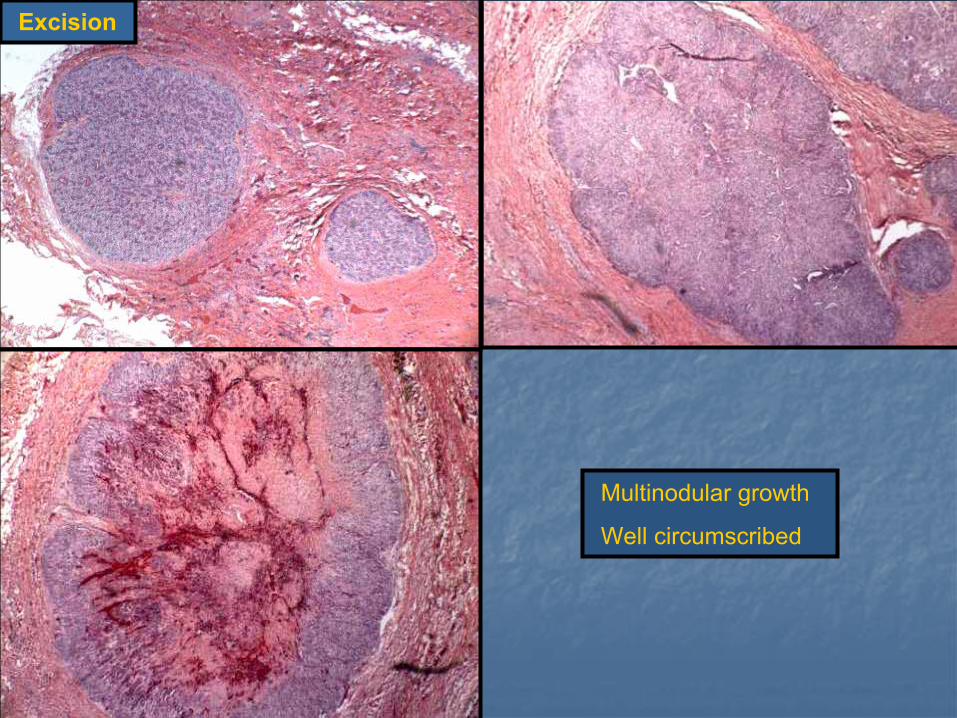
Multinodular growth
Well circumscribed
Excision

DIAGNOSISDIAGNOSIS
Recurrent epithelial-myoepithelial carcinoma of the parotid gland,
intermediate grade
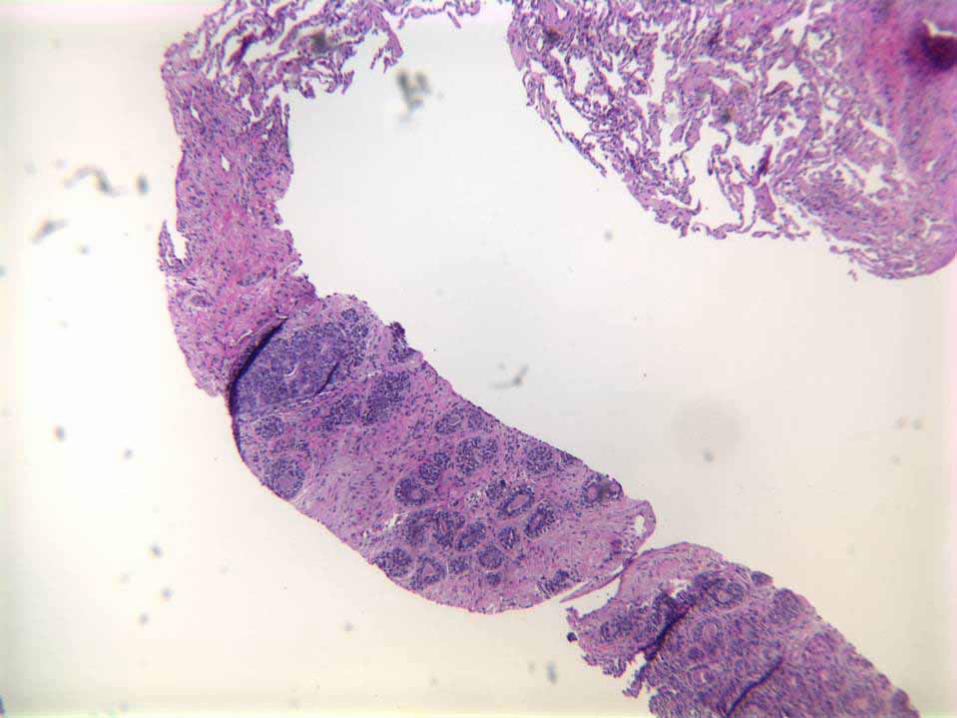
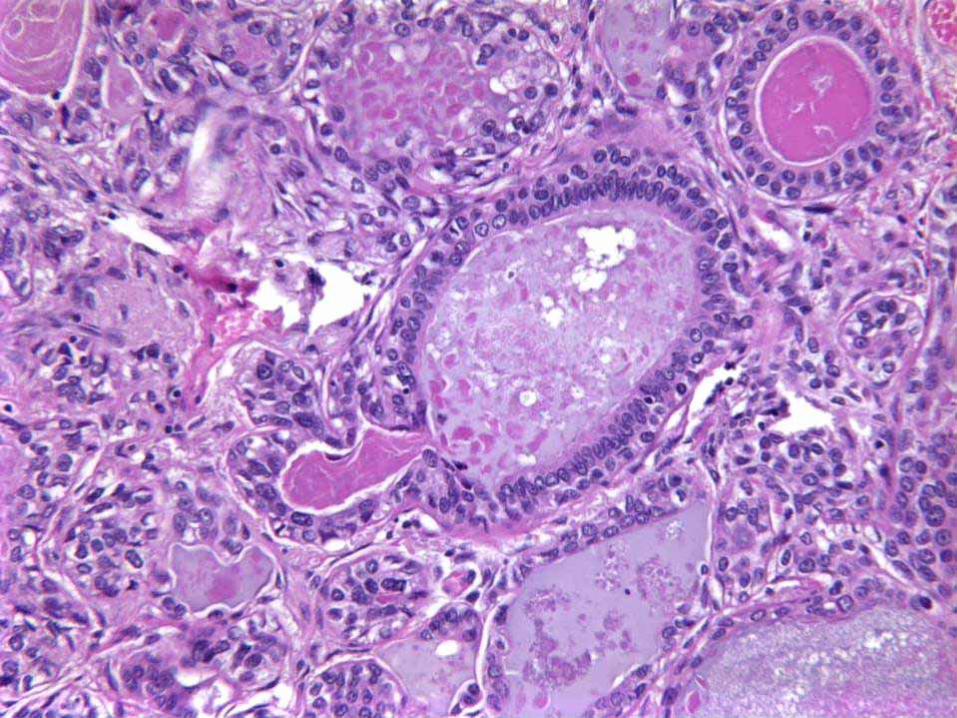
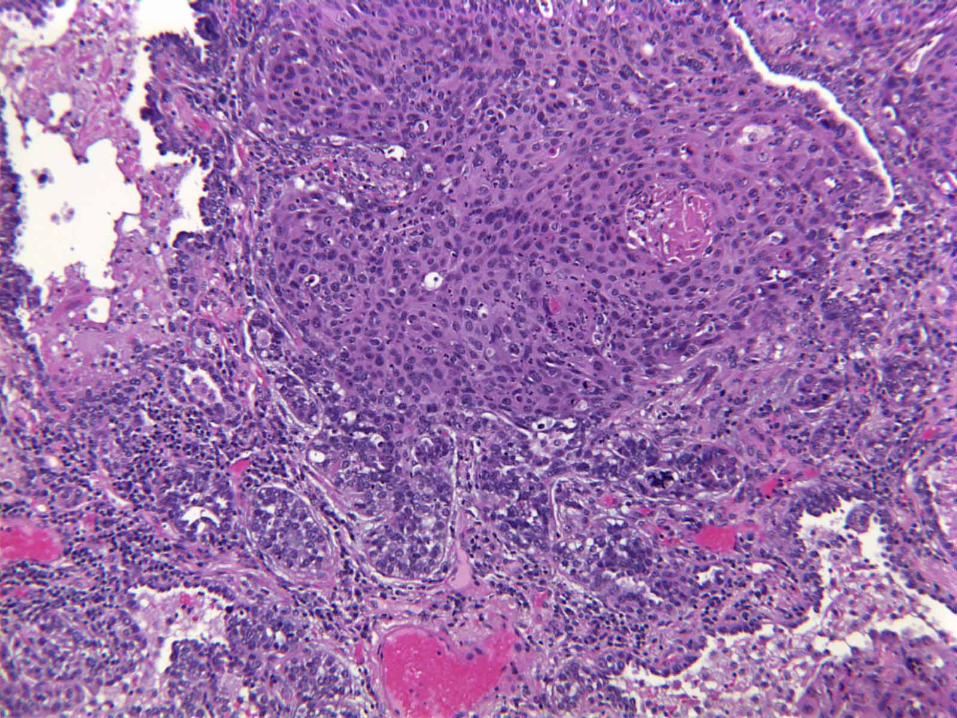
CASE 2CASE 271 year-old lady awaiting renal transplant
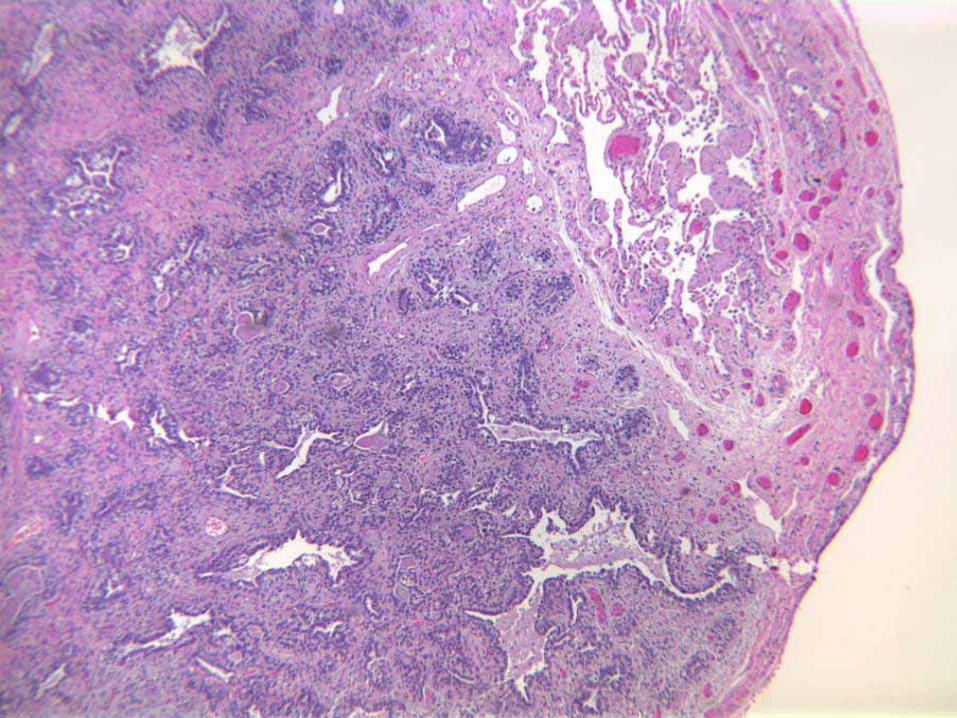
Found to have an irregular spiculated soft tissue density in the left upper lungCT guided needle core biopsy followed by left lung resection
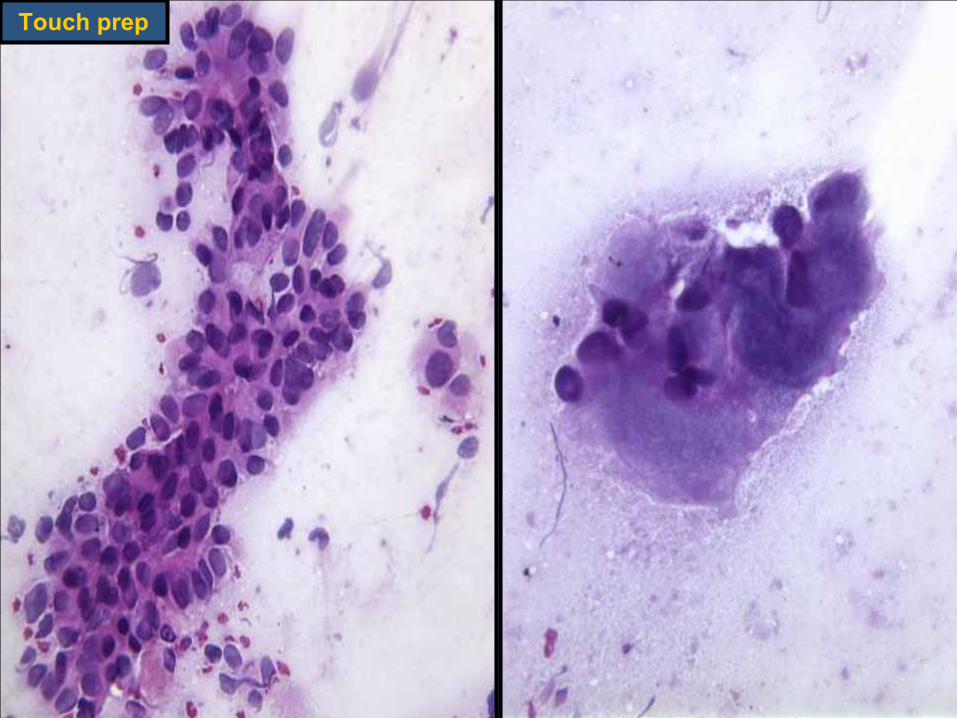
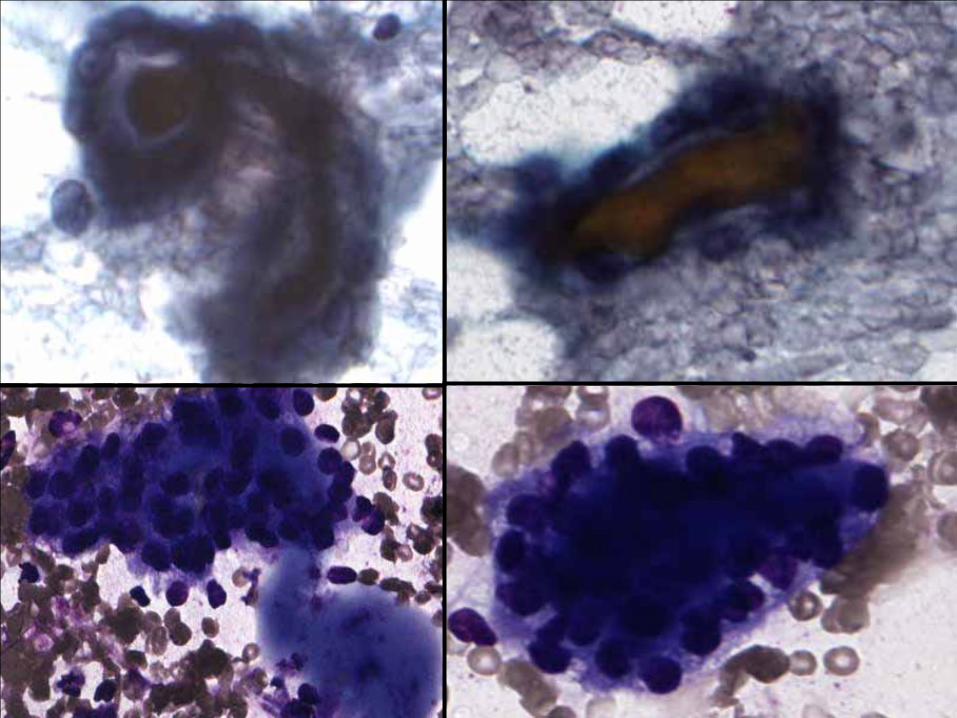
Touch prep
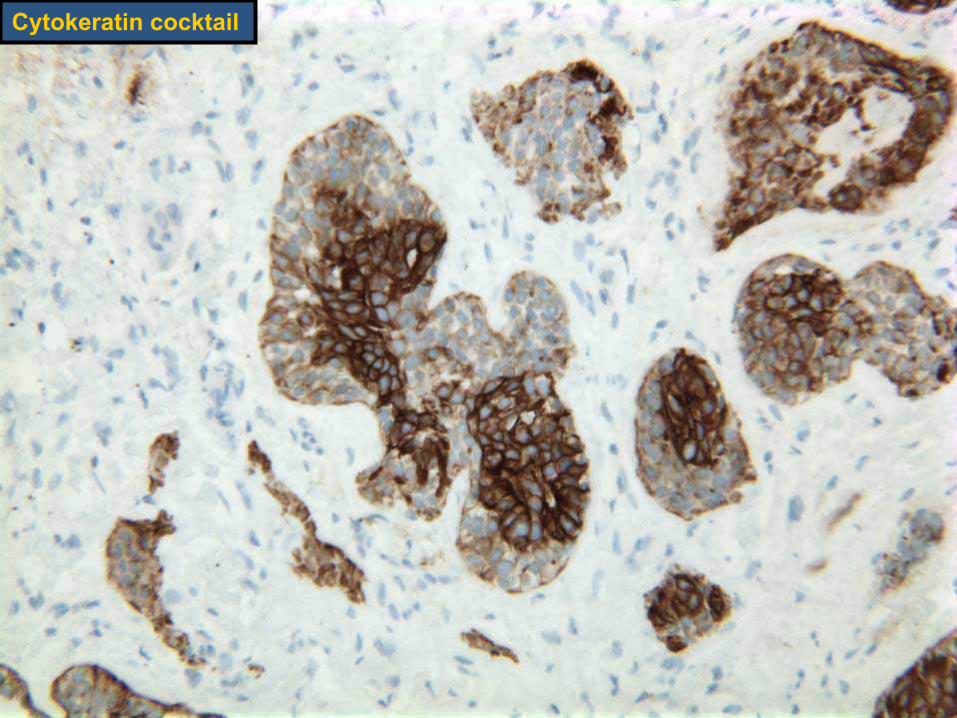
Cytokeratin cocktail
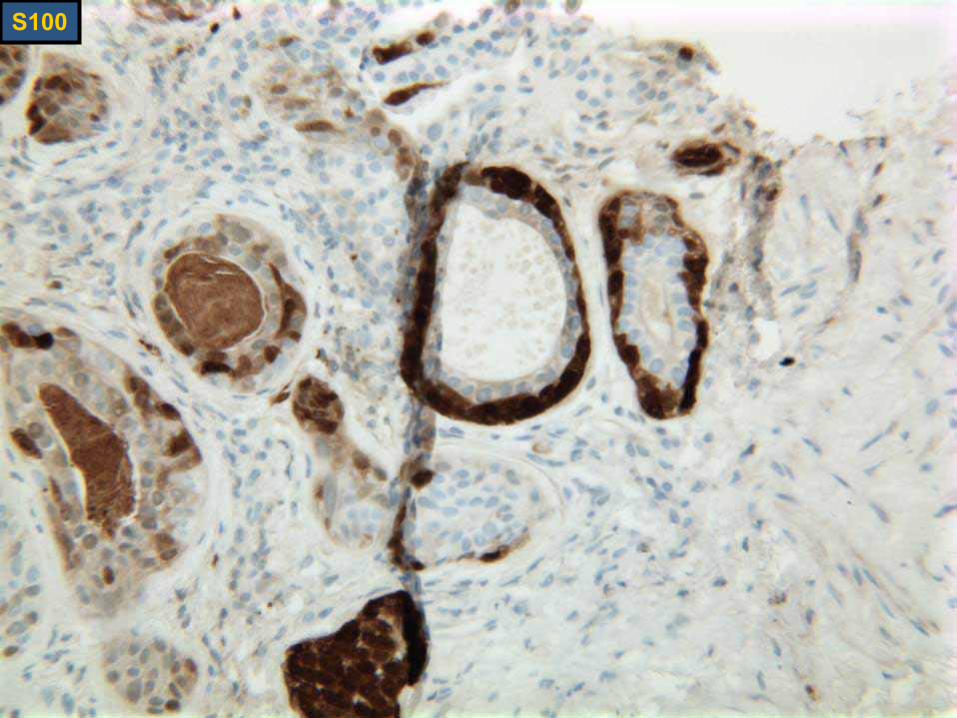
S100
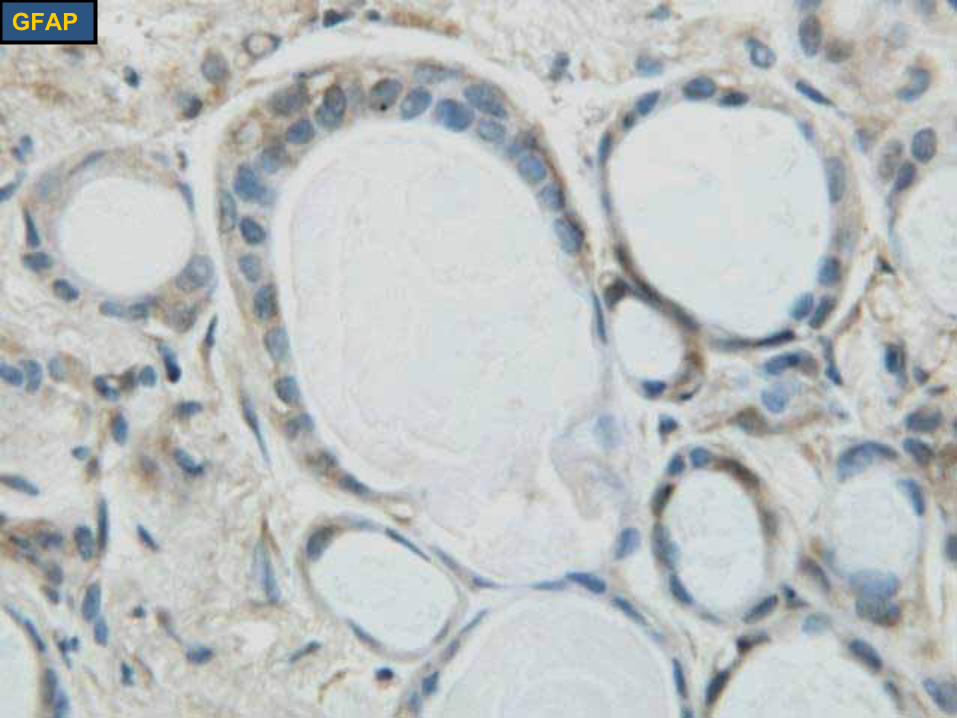
GFAP

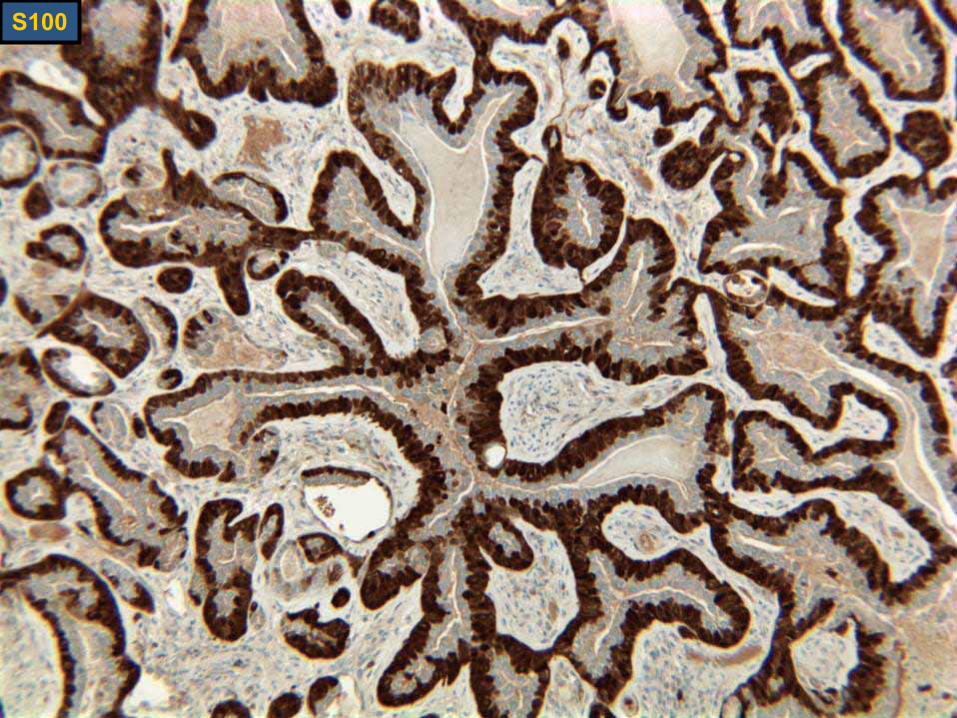
S100
DIAGNOSISDIAGNOSIS
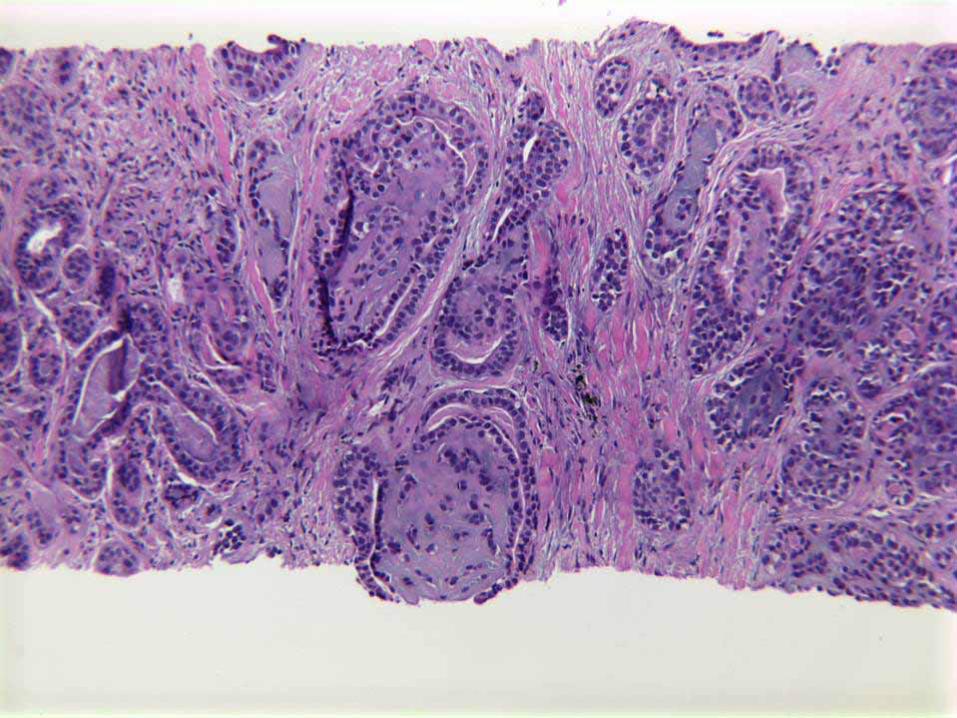
Epithelial-myoepithelial carcinoma of salivary gland type, arising in the lung
CASE 3CASE 3
57 year-old gentleman
History of radiation for lung cancer, 2003
Now with large heterogenous liver massCT guided liver biopsy was performed
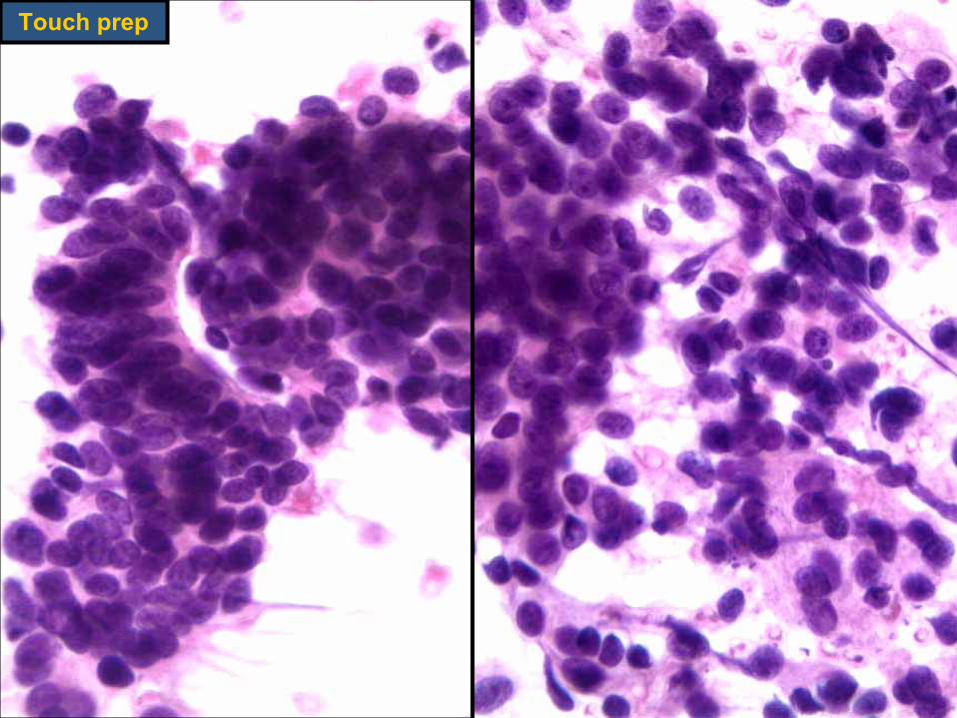
Touch prep
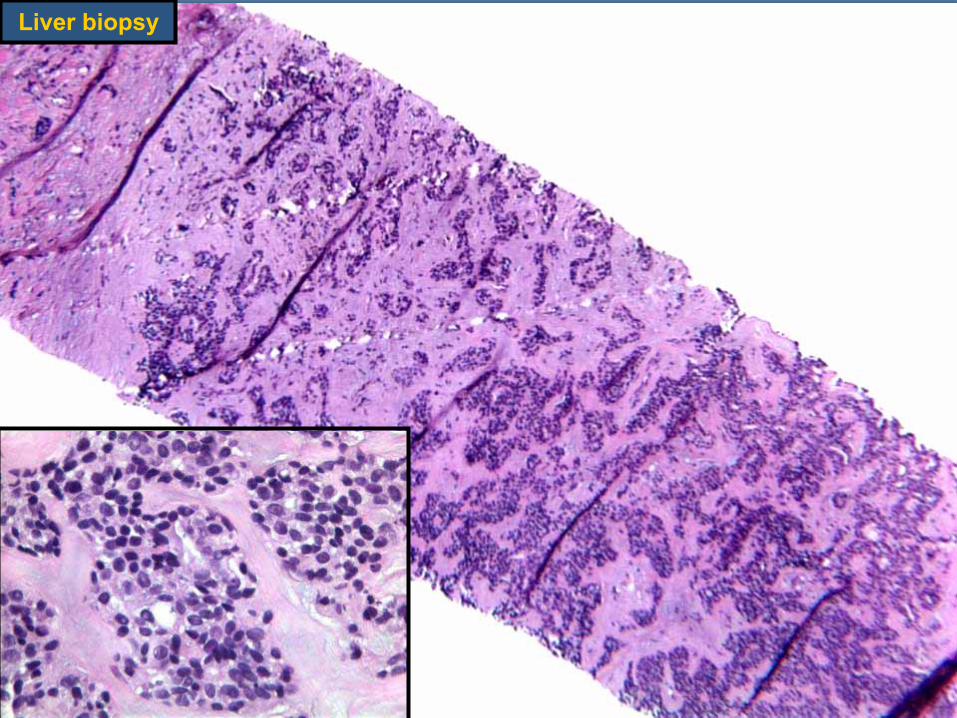
Liver biopsy
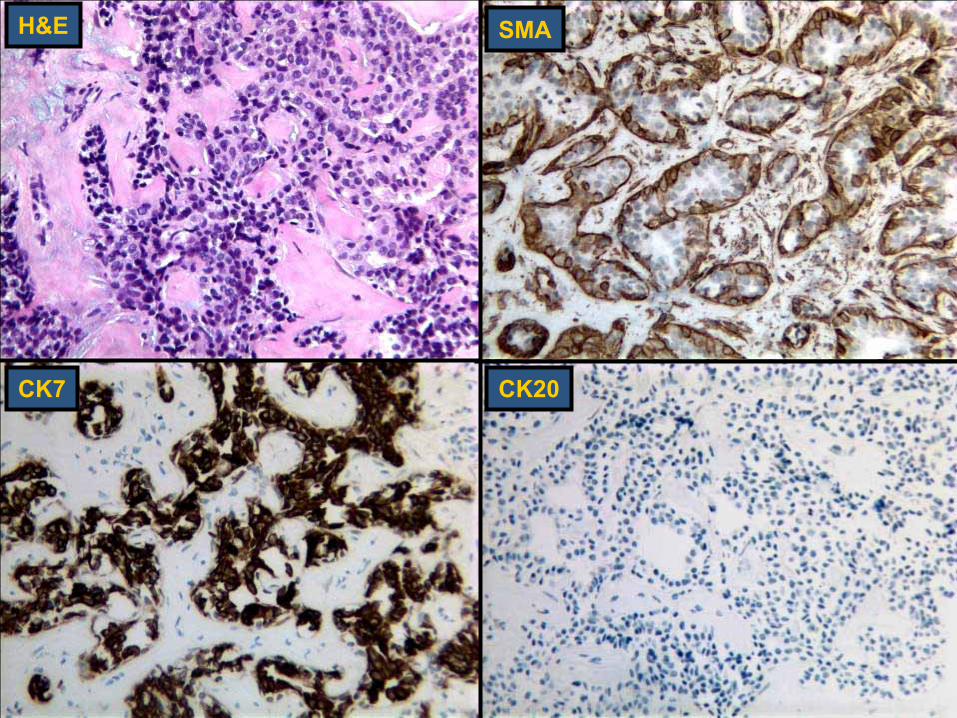
H&E SMA
CK20CK7
DIAGNOSISDIAGNOSIS
Metastatic carcinoma consistent with epithelial-myoepithelial carcinoma
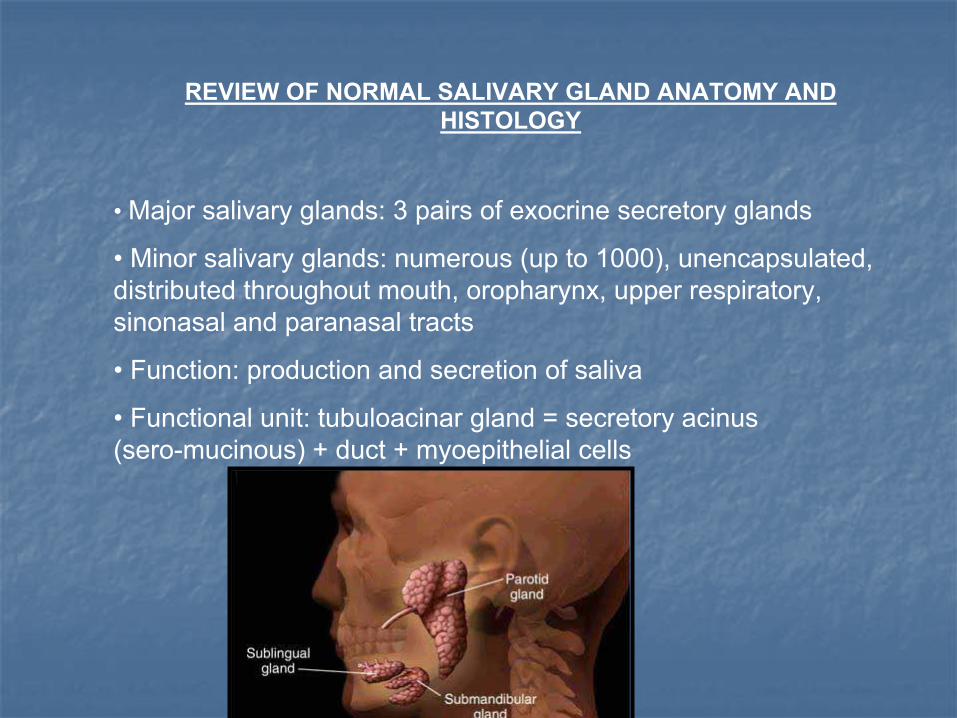
REVIEW OF NORMAL SALIVARY GLAND ANATOMY AND HISTOLOGY
• Major salivary glands: 3 pairs of exocrine secretory glands
• Minor salivary glands: numerous (up to 1000), unencapsulated, distributed throughout mouth, oropharynx, upper respiratory, sinonasal and paranasal tracts
• Function: production and secretion of saliva
• Functional unit: tubuloacinar gland = secretory acinus (sero-mucinous) + duct + myoepithelial cells
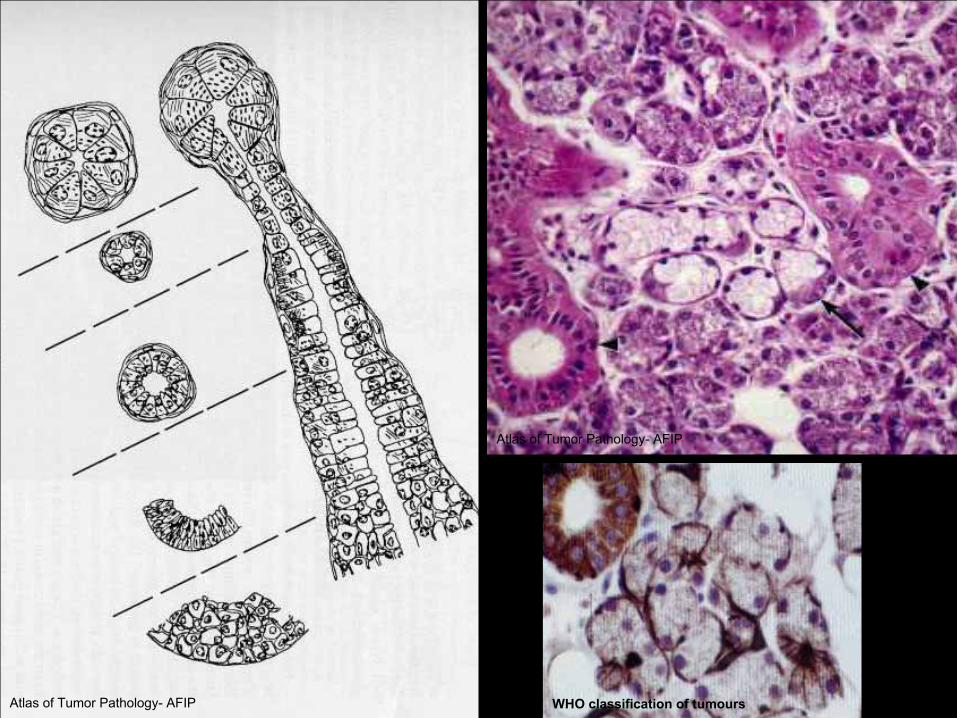
Atlas of Tumor Pathology- AFIP
WHO classification of tumoursAtlas of Tumor Pathology- AFIP
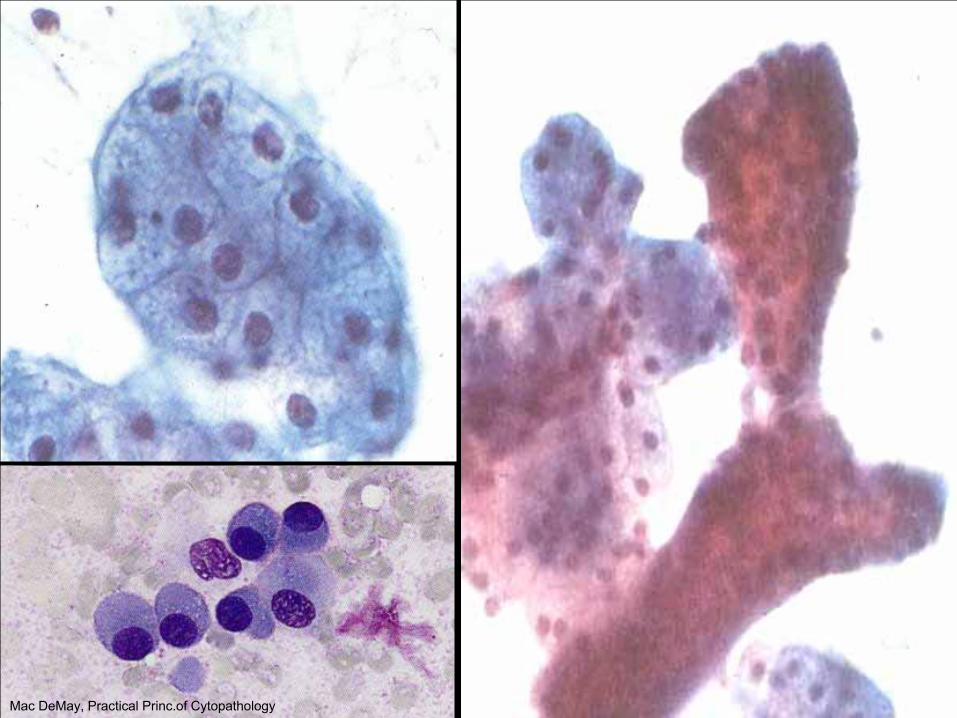
Mac DeMay, Practical Princ.of Cytopathology
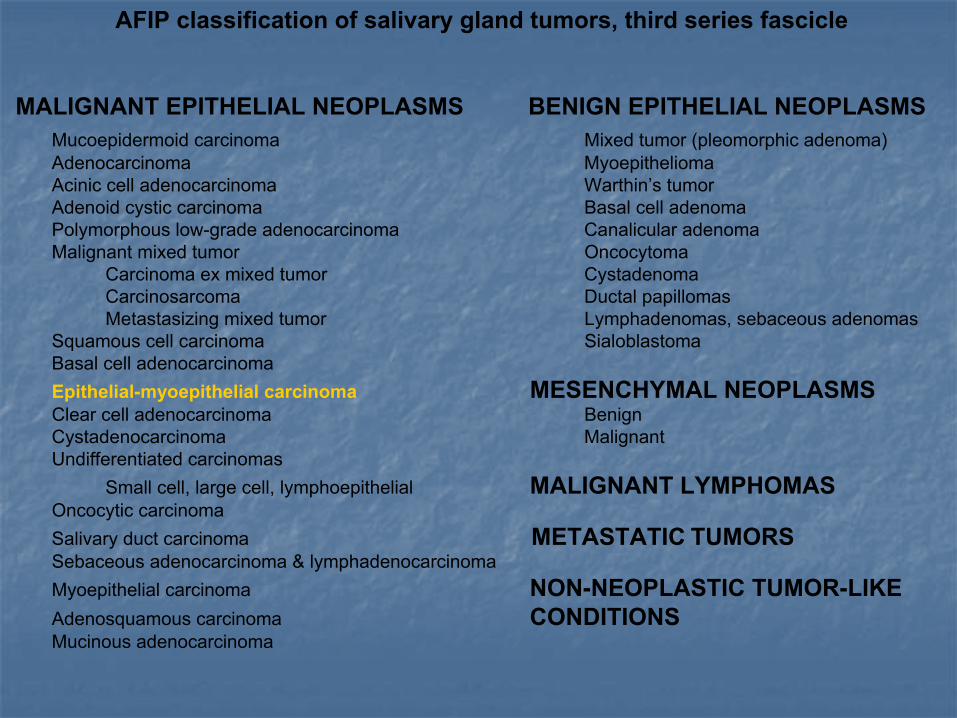
AFIP classification of salivary gland tumors, third series fascicle
MALIGNANT EPITHELIAL NEOPLASMS BENIGN EPITHELIAL NEOPLASMSMucoepidermoid carcinoma Mixed tumor (pleomorphic adenoma)Adenocarcinoma MyoepitheliomaAcinic cell adenocarcinoma Warthin’s tumorAdenoid cystic carcinoma Basal cell adenomaPolymorphous low-grade adenocarcinoma Canalicular adenomaMalignant mixed tumor Oncocytoma
Carcinoma ex mixed tumor CystadenomaCarcinosarcoma Ductal papillomasMetastasizing mixed tumor Lymphadenomas, sebaceous adenomas
Squamous cell carcinoma SialoblastomaBasal cell adenocarcinomaEpithelial-myoepithelial carcinoma MESENCHYMAL NEOPLASMSClear cell adenocarcinoma BenignCystadenocarcinoma MalignantUndifferentiated carcinomas
Small cell, large cell, lymphoepithelial MALIGNANT LYMPHOMASOncocytic carcinomaSalivary duct carcinoma METASTATIC TUMORSSebaceous adenocarcinoma & lymphadenocarcinomaMyoepithelial carcinoma NON-NEOPLASTIC TUMOR-LIKEAdenosquamous carcinoma CONDITIONSMucinous adenocarcinoma
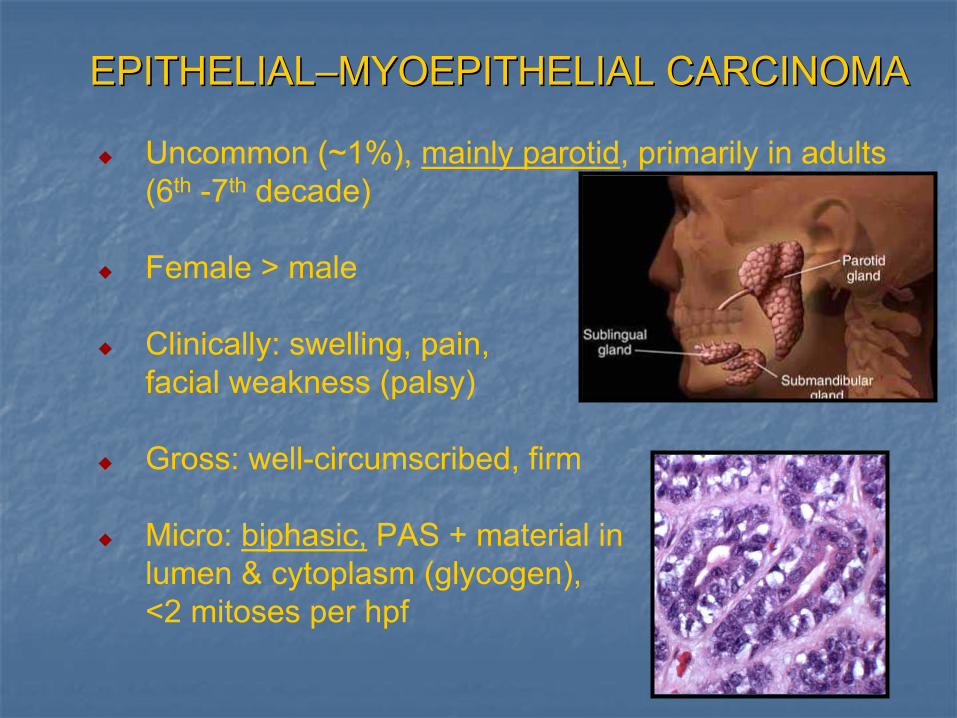
EPITHELIALEPITHELIAL––MYOEPITHELIAL CARCINOMAMYOEPITHELIAL CARCINOMA
Uncommon (~1%), mainly parotid, primarily in adults (6th -7th decade)
Female > male
Clinically: swelling, pain, facial weakness (palsy)
Gross: well-circumscribed, firm
Micro: biphasic, PAS + material in lumen & cytoplasm (glycogen), <2 mitoses per hpf
EPITHELIALEPITHELIAL––MYOEPITHELIAL CARCINOMAMYOEPITHELIAL CARCINOMA
Immunostains: ductal cells are CK, EMA +clear cells are S100, SMA, HHF35,
GFAP, p63, calponin +EM: electron dense epithelial cells surrounded by electron lucent myoepithelial cellsBehavior: low grade malignancy
40% recurrence14% metastasize (periparotid and cervical nodes, lung, liver, kidney)
Margin statusPoor prognosis- minor salivary gland tumors, atypia (>20%), dedifferentiation, aneuploidy
Treatment: surgical excision +/- radiation
“Biphasic Tumors” :Pleomorphic adenomaAdenoid cystic CAPLGA
“Clear Cell Tumors”:Clear cell carcinoma, NOSMucoepidermoid CAAcinic cell CASebaceous CAOncocytomaMetastatic renal cell, thyroid CA
DIFFERENTIAL DAGNOSISDIFFERENTIAL DAGNOSIS
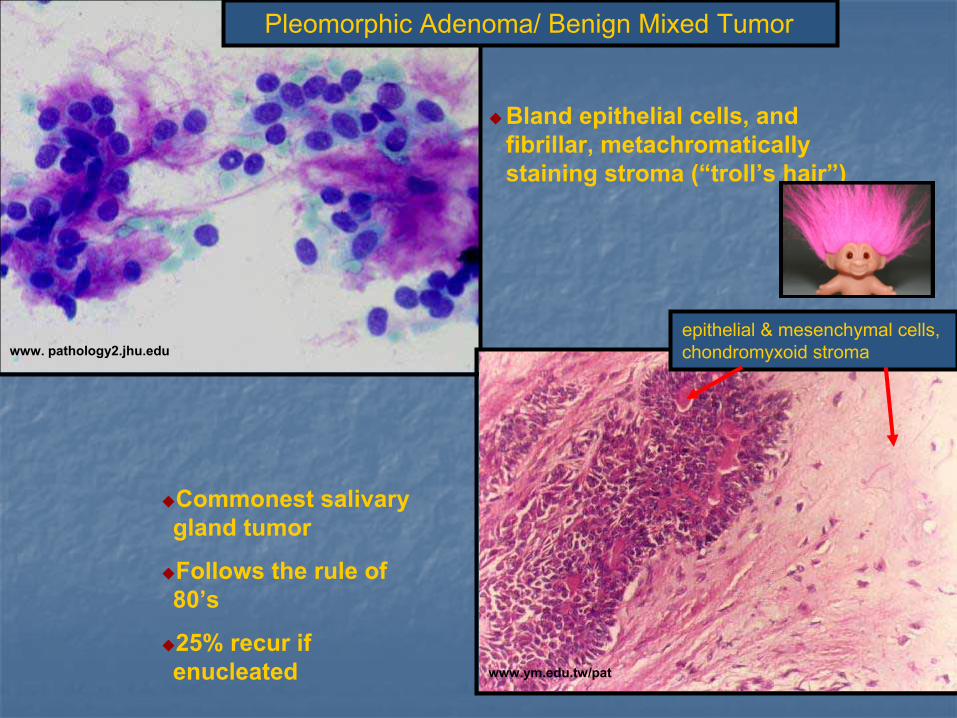
Bland epithelial cells, and fibrillar, metachromatically staining stroma (“troll’s hair”)
Pleomorphic Adenoma/ Benign Mixed Tumor
www.ym.edu.tw/pat
www. pathology2.jhu.eduepithelial & mesenchymal cells, chondromyxoid stroma
Commonest salivary gland tumor
Follows the rule of 80’s
25% recur if enucleated
www.pathology.uth.tmc.edu
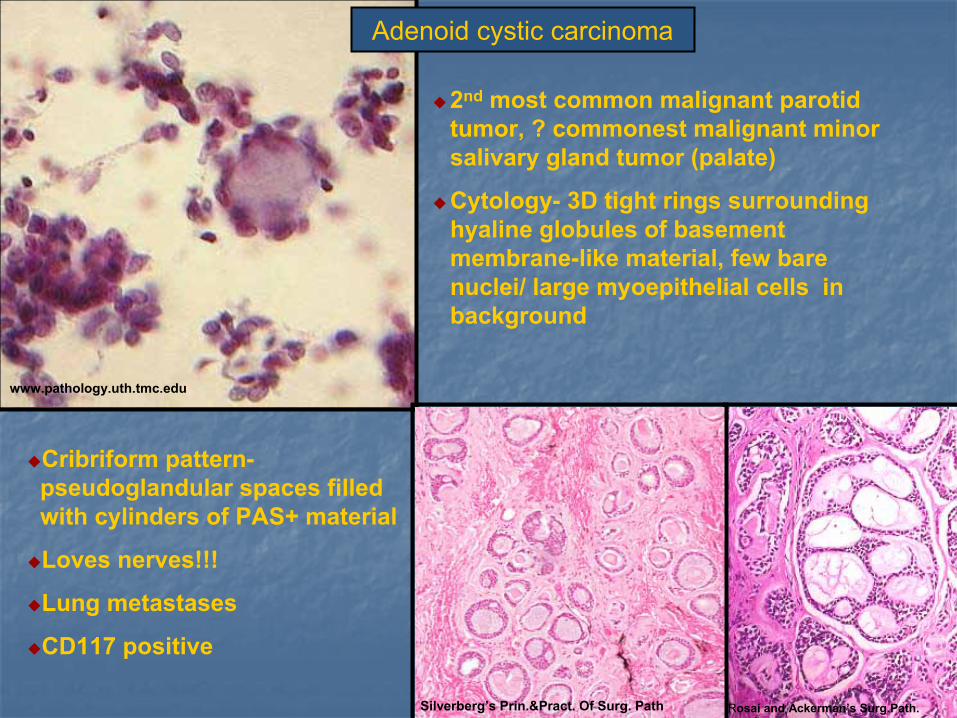
2nd most common malignant parotid tumor, ? commonest malignant minor salivary gland tumor (palate)
Cytology- 3D tight rings surrounding hyaline globules of basement membrane-like material, few bare nuclei/ large myoepithelial cells in background
Cribriform pattern-pseudoglandular spaces filled with cylinders of PAS+ material
Loves nerves!!!
Lung metastases
CD117 positive
Adenoid cystic carcinoma
Rosai and Ackerman’s Surg.Path.Silverberg’s Prin.&Pract. Of Surg. Path
SUMMARYSUMMARY
Rare, low grade carcinomaUsually arising in the parotid glandThree cases of EMC
One typical location (parotid)Two apparently primary in the lung
one metastatic to liver
Important to distinguish from: pleomorphic adenoma because of its potential for metastasisadenoid cystic carcinoma because of its less aggressive nature
REFERENCESREFERENCES
Atlas of Tumor Pathology (Tumors of the Salivary Glands)- AFIP WHO classification of tumours- Head and Neck tumoursElsevier Inc 2004 Rosai and Ackerman’s Surgical Pathology 9th ed.Sternberg's Diagnostic Surgical Pathology 4th ed.Silverberg's Principles and Practice of Surgical Pathology and CytopathologyPathologic Basis of Disease, 7th ed., Robbins and Cotran
Special thanksDr. Craig Zuppan
Dr. Anwar Sultana RazaDr. Wesley Stevens
Dr. Jeff CaoDr. Daniel BuxtonDr. Mingyi Chen
Loma Linda Histology