Embed Size (px)
Citation preview

Looked after Children Annual Report 2016-17 Item 18h
Governing Body meeting
11 January 2018
Author(s) Nikki Shepherd, Designated Nurse Looked after Children Dr Lorraine Pearson, Designated Doctor Looked after Children
Sponsor Director Mandy Philbin, Acting Chief Nurse Purpose of Paper
To provide the Governing Body an annual report and assurance with regards the CCG responsibilities for Looked after Children
Key Issues
The benchmarking exercise has enabled significant improvements in CCG compliance to the commissioning standards for Looked after Children. Out of 34 standards only one remains Red.
In order to ensure full compliance to the benchmarking standards a Named Doctor LAC needs to be in post in the provider service and the Designated Doctor Looked after Children post should be brought into the CCG equivalent to the Designated Doctor for Safeguarding post.
Successful implementation of the Payment by Results tariff for statutory health assessments. It should be noted that no looked after child placed in Sheffield has a delayed health assessment due to invoicing arrangements.
Overall completion of statutory health assessments for children looked after for 12 months was 94% (March 2017) although there needs to be significant improvement in meeting the 20 working day deadline for initial health assessments.
GP’s have received training and information regarding looked after children through the GP training events and a PLI event. A guidance paper on the change in the NHS number at adoption and health records has been produced.
Is your report for Approval / Consideration / Noting
Noting
Recommendations / Action Required by Governing Body
The Governing Body is asked to endorse the above report and note the progress made.
Governing Body Assurance Framework
Which of the CCG’s objectives does this paper support? Organisational development to ensure CCG meets organisational health and capability requirements.
1
Are there any Resource Implications (including Financial, Staffing etc)?
No
Have you carried out an Equality Impact Assessment and is it attached?
Please attach if completed. Please explain if not, why not Not applicable
Have you involved patients, carers and the public in the preparation of the report?
No
2
Looked after Children Annual Report 2016-17
Governing Body meeting
11 January 2018
1. Introduction.
The purpose of this report is to provide NHS Sheffield Clinical Commissioning Group (CCG) an overview of the progress and challenges in supporting and improving the health of children looked after by Sheffield City Council (SCC) and those placed by other authorities in Sheffield. It is produced in line with duties and responsibilities outlined in the ‘Statutory Guidance on Promoting the Health of Looked after Children: Statutory Guidance for local authorities, clinical commissioning groups and NHS England’ (2015).
1.1 Accountability and role of Designated Professionals.
Accountability for Designated Professionals for Looked after Children is set out within the 2015 NHS England Safeguarding Vulnerable People in the NHS Accountability and Assurance Framework. The Designated Nurse is hosted within the CCG but is accountable also to NHS England and the Nursing and Midwifery Council. The Designated Doctor LAC is currently employed by Sheffield Children’s NHS Foundation Trust.
1.2 Role of Designated Nurse and Doctor for Looked after Children.
The Designated Professionals for Looked after Children role takes a strategic and professional lead across the whole health community on all aspects of Looked after Children. They provide clinical expertise to Clinical Commissioning Groups and partner agencies on the specific health needs of the cohort of looked after children and care leavers in fulfilling their responsibilities to improve the health of looked after children and care leavers. Audit and quality assurance are key roles for both designated professionals.
1.3 Statutory Framework, Legislation and Guidance.
There are a number of pieces of legislation and guidance which inform responsibilities and requirements with regard to working with looked after children and the key documents are summarised below.
Promoting the Health and Wellbeing of Looked After Children(Department of Education and Department of Health, 2015) stipulates that all commissioners of health services should have appropriate arrangements and resources in place to meet the physical and mental health needs of looked after children. CCGs must be able to access the expertise of a designated doctor and nurse for looked after children; the
3

CCG must retain responsibility for looked after children who are placed out of area and ensure that their care continues uninterrupted and they must ensure that arrangements are in place for smooth transitions into adult care.
Children’s Act (2004) requires local authorities; CCG and NHS England to cooperate to promote the health and welfare of looked after children (section 10).
Looked After Children: knowledge, skills and competence of healthcare staff (Intercollegiate Role Framework, 2015): this sets out the specific knowledge, skills and competencies which health staff require in order to work with looked after children.
Special educational needs and disability code of practice: 0-25 years (Department of Education and Department of Health 2015) is a statutory code of practice which outlines the duties of local authorities, health bodies, schools and colleges to provide for those with a special educational need (SEN) under part 3 of the Children and Families Act 2014. Approximately 70% of looked after children have some form of special educational need.
NICE Guideline PH28: Looked after Children and Young People (2010updated 2015) aims to enable children’s health and social care services to meet their obligations to improve the health and well- being of looked after children. The recommendations cover local commissioning, multiagency working, care planning, placements and timely access to appropriate health and mental health services.
Who Pays? Determining Responsibility for payments to providers (NHS England, 2013) provides guidance on how to determine who pays for health services for looked after children who are placed out of area.
NICE Quality Standard QS31: Looked after children & young people (2013) gives specific measureable statements around the health and wellbeing of looked after children and young people and care leavers for all services.
The Care Planning, Placement and Case Review (England) Regulations (2010) This guidance sets out the functions and responsibilities of local authorities and partner agencies under Part 3 of the Children Act 1989 (‘the 1989 Act’), which concerns the provision of local authority support for children and families. In particular it describes how local authorities should carry out their responsibilities in relation to care planning, placement and case review for looked after children.
4
Future in Mind: Promoting, protecting and improving our children and young people’s mental health and wellbeing (2015)
1.4 Corporate Parenting.
Corporate parenting is the term used to describe the responsibility of the local authority towards looked after children and young people. Accountability and scrutiny for the services provided to looked after children from multi- agency partners is directed through the Corporate Parenting Board. The Designated Nurse for LAC represents Sheffield CCG along with the Designated Doctor LAC (SC NHS FT) on Sheffield’s Corporate Parenting Board and are key members of the local authority Corporate Parenting Strategy Board as well as the Priority 3 Health and Wellbeing Group. These meetings are currently held quarterly.
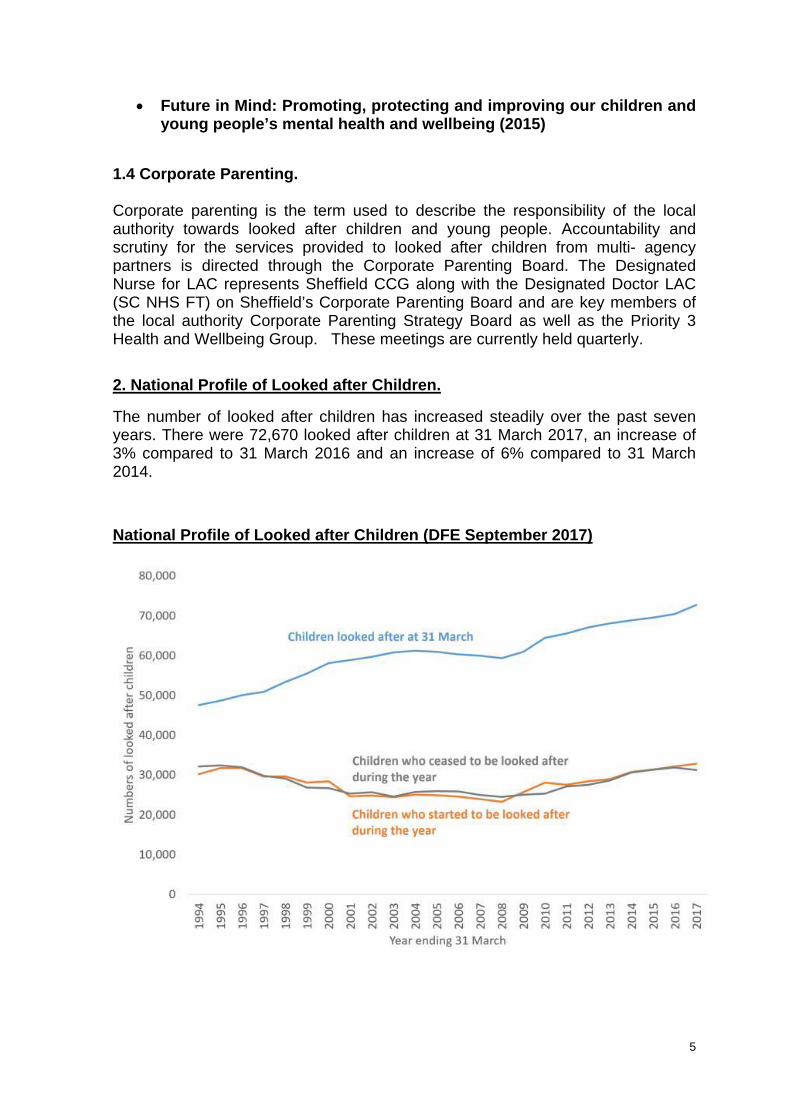
2. National Profile of Looked after Children.
The number of looked after children has increased steadily over the past seven years. There were 72,670 looked after children at 31 March 2017, an increase of 3% compared to 31 March 2016 and an increase of 6% compared to 31 March 2014.
National Profile of Looked after Children (DFE September 2017)
5
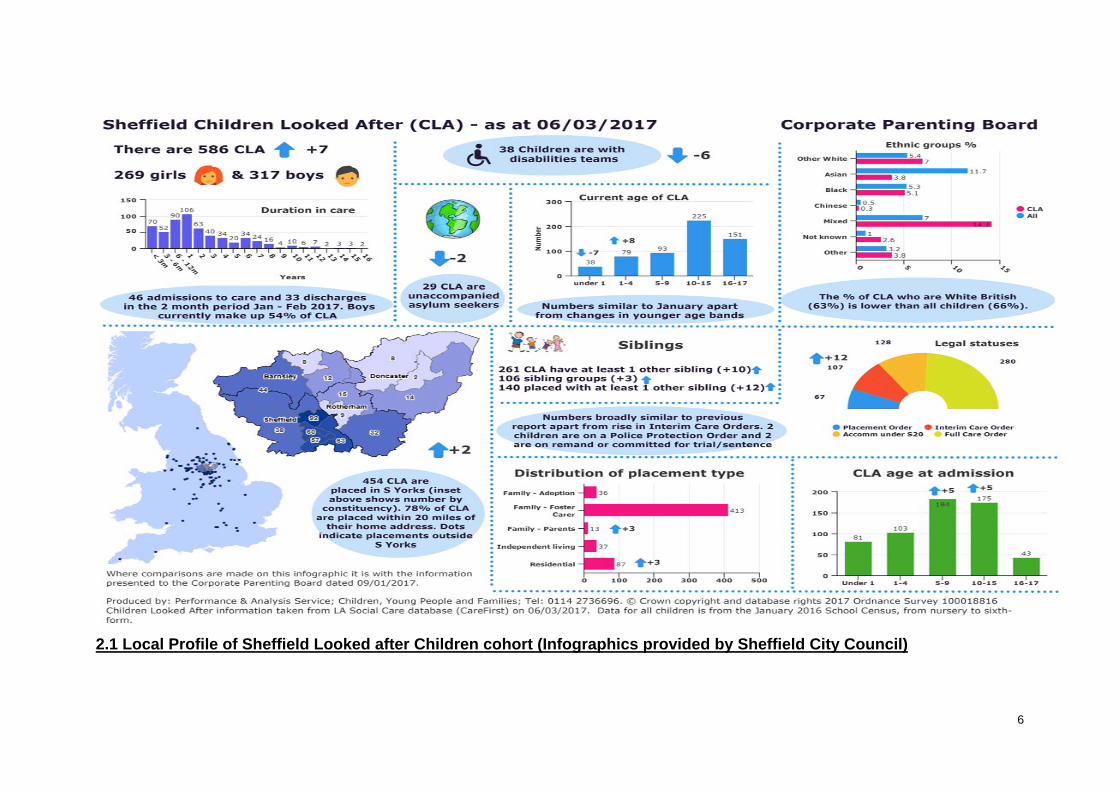
2.1 Local Profile of Sheffield Looked after Children cohort (Infographics provided by Sheffield City Council)
6

2.2 Local Profile of Sheffield Looked after Children cohort (Infographics provided by Sheffield City Council)
7

3. Achievements 2016-2017.
3.1 NHS England CCG Benchmarking Exercise.
NHS England North commissioned a benchmarking exercise to provide insight into commissioning practice across the North of England in relation to Looked after Children. The benchmarking tool was created by the designated nurses for looked after children from Sheffield and Calderdale and is now being piloted in the Midlands within the electronic safeguarding assurance tool.
The aim was to gain further understanding with the knowledge that differing commissioning practice adds further complexity in addressing the health of this most vulnerable cohort. The compliance tool was rolled out across the North of England and 68 CCG’s were benchmarked. (NHS England North acknowledged that the rankings were not an indicator around performance or outcomes for Looked after Children within individual CCGs but of compliance with the standards only.)
Since initial completion in February 2015 the benchmarking tool has provided a working document to monitor compliance with the standards outlined in the tool and to making improvements in the health and wellbeing of looked after children.
The Benchmarking Tool was updated in 2016 adding in an additional key area which was ensuring compliance with the Statutory Guidance and the intercollegiate document on Designated and Named professional roles. With regards to having a Named LAC Doctor in the provider service Sheffield CCG ranks as Red. This is a key priority for 2018/19. Additionally establishing the wider influence/role of the Designated Doctor for LAC within the CCG should be made more robust.
The tool is constantly under review by the Designated Nurse LAC and is used for seeking assurance in some areas from the provider Looked after and Adoptive Children’s Health Team. For Sheffield CCG there has been a decrease of amber ratings from 16 to 6, and an increase in green ratings from 17 to 27. There is only one Red rating which is identified above. (Appendix 1)
3.2 The Responsible Commissioner.
NHS Sheffield CCG is the responsible commissioner of health services for children looked after who are taken into the care of Sheffield Local Authority. When children looked after are placed out of area it is the responsibility of Sheffield Local Authority as lead agency to advise health as stakeholders to ensure that children maintain access to relevant health services. This includes the originating CCG and the receiving CCG where the child or young person has been placed (DOH 2015).
3.3 Payment by Results.
The Department of Health, with NHS England, Monitor, the Royal Colleges and other partners, has developed a mandatory national currency and tariff for statutory health assessments for looked-after children placed out of area. In November 2015, a standard letter was devised informing all CCGs across England that Sheffield CCG would charge for statutory health assessments in line with national tariff. The tariff is not applied to the
8
South Yorkshire and Bassetlaw footprint. The Payment by Results tariff was aimed at improving quality, access to services and providing resources into local areas to meet the demand. However, in view of the way each CCG has commissioned services this, in some instances, has caused further delay in accessing services prior to invoicing arrangements being confirmed.
Sheffield CCG has a process in place whereby prior to payment of invoices for Sheffield LAC placed outside, assurance is provided both through the provider service via the Lead Nurse LAC. All looked after children placed into Sheffield from other authorities have a health assessment completed as priority and is not delayed due to invoicing arrangements. A quarterly audit by the Designated Nurse LAC (CCG) provides further assurance that health assessments meet quality requirements.
3.4 NHS England National LAC Forum (was Sub Group)
Since the benchmarking exercise was completed NHS England has commissioned work on unwarranted variation and this is part of the work of the National LAC Forum (formally National LAC Sub Group). A Standard Approach document is expected to be published in the autumn and aims to reduce the complexity that is apparent nationally.
3.5 Expert Reference Group
The National LAC Sub group split into the National LAC Forum and the Expert Reference Group in July 2017. The Designated Nurse LAC is a member of both groups and will be the chair of the Expert Reference Group.
4. Children and Young people placed out of Sheffield.
Assurance around health needs being addressed for those children and young people is sought via the implementation of the quality assurance tool within provider services, further audit and scrutiny. Escalation processes are embedded within the LAC health team to the Designated Nurse for LAC if experiencing difficulties in accessing health services and the annual health assessment for Sheffield looked after children placed out of area.
4.1 Children and Young people placed in Sheffield via other Authorities
There are, at the time of writing this report, around 150 looked after children placed into Sheffield from other local authorities.
Due to the variation in notification procedures from other local authorities it has been unknown for a significant time how many looked after children are placed into Sheffield who are under the care of other local authorities. The Designated Nurse and the Lead Nurse LAC have spent a considerable amount of time during the year ensuring that all data is checked and correct. We will be working further with the local authority to ensure that data held by both agencies is accurate and up to date.
5. Statutory Health Assessments.
The ‘Promoting the health and well-being of looked after children: Statutory guidance for local authorities, clinical commissioning groups and NHS England’ (March 2015) along with the ‘Children Act’ 1989, sets out the statutory requirements for health assessments. The initial health assessments should be completed within 20 working days of a child coming into care. Following this for children less than 5 years require 6 monthly review
9

health assessments and for children and young people over 5 years the review health assessment should be yearly.
5.1 Key Performance Indicator for 2016/2017
The KPI’s on timely health assessments for all Sheffield looked after children are reported quarterly via the Designated Safeguarding Nurse as part of a suite of safeguarding reporting from provider services.
2016 /2017 Quarter 1 Quarter 2 Quarter 3 Quarter 4
Initial Health assessments
17% 64% 56% 69%
Review Health assessments – children under 5 years
100% 90% 93% 92%
Review Health Assessments – children over 5 years.
75% 73% 89% 78%
The compliance of achieving the 20 day working deadline for initial health assessments has improved over the year due to close working with the local authority although the issues of delayed or incomplete consent forms remains a significant issue. This has been the case for a number of years and is monitored through the corporate parenting strategy group. It should be noted also that the reasons for not meeting the 20 day deadline can also be due to other issues for example, a young person being place out of city. The issue of delayed consent for health assessments has been a long standing issue for Sheffield and remains to be an area that requires further work and significant improvement.
The local authority are required to report annually on children looked after continuously for 12 months and have had a statutory health assessment. As at March 2017 this was reported as 94%.
6. Care leavers.
The DoH document ‘Promoting the Health of Looked after Children’ (March 2015) states that CCG’s have a role in commissioning health provision taking into account the specific requirements for young people identified as care leavers in the Leaving Care Act (2000). They are required to ensure that plans are in place to enable children leaving care to continue to obtain the healthcare they need and that arrangements are in place to ensure a smooth transition for looked-after children and care leavers moving from child to adult health services.
On leaving care Sheffield young people are provided with a leaving care health summary, providing details of their medical history and advice on navigating universal health services and their health provision is then with primary care services. CCG and Local Authority responsibility for the transition arrangements of young people leaving care to adult services is set out in the NICE Guidance Transition for Young People
10
using health and social care services and Statutory Guidance on promoting the health of LAC and Care leavers (2015). Going forward, a robust health transition pathway for care leavers needs to be established for young people up to the age of 25 years. Currently a specialist LAC nurse works with looked after young people up to their 19th birthday.
7. Role of Primary Care.
The Department of Health (2015) Statutory Guidance on Promoting the Health of Looked After Children and care leavers states that Primary Care providers have a vital role in the identification of the health care needs of children and young people who are looked after or leaving care. They have prior knowledge of the child/young person and have statutory responsibilities to:
Accept the LAC child as a registered patient seeking the urgent transfer of the medical records.
Act as advocate for the child, contribute and provide summaries of the health history of a child who is LAC, including their family history to inform the Statutory Health Assessment process and legal proceedings e.g. Adoption
Ensure that referrals to specialist services are timely, taking into account the needs and high mobility of children who are looked after.
Ensure that any health needs identified within a Looked after Children Health Assessment are met and monitored.
Copies of the full statutory health assessment and health plans are sent to GP practices via the Sheffield Looked after Children’s Health Team to ensure that the lead clinical record is updated and health needs followed up within the Primary Care setting.
Training has been provided to GPs on about looked after children both at GP locality training during 2016-2017 and at the PLI in 2016.
8. Adoption and NHS numbers.
Current adoption legislation requires that adopted children are given a new NHS number and that previous medical information relating to the child is put into a newly created health record. The new NHS number is allocated by the National Back office following confirmation by the General Register Office that adoption order has been granted.
It was proposed that the practice of issuing a new NHS number when a child is adopted should be brought to an end, but did not receive Parliamentary approval. This is because important medical records are being lost due to the introduction of new NHS numbers. There is still no national policy on this matter. Hospital records, General Practitioner and community records are all treated separately by different agencies. The designated professionals have produced an interim guidance document for GPs that has been agreed until national guidelines have been sanctioned.
8.1 Regionalisation of adoption
The Government’s Adoption Reform Agenda requires all adoption services to be reorganised under regional arrangements. Due to close working and collaboration the 15 Adoption Agencies and 8 Voluntary Agencies in the Yorkshire and Humber area are acting as a National performance lead. There is an expectation that local authorities and voluntary adoption agencies will collaborate to provide services in a newly formed
11
Yorkshire and Humber ‘One Adoption’ service with a central hub co-ordinating 3 Regional Adoption Agencies (RAAs) and the Voluntary Adoption Agencies Group. The driver for this proposed change is to improve outcomes for children with a plan of adoption – timelier placements, increased recruitment of appropriate adopters and improved matching of children with families. There is also an expectation that support provided to children and adopters throughout the adoption process is timely and of a standardised high quality.
The Adoption Panel contributes to the running and quality assurance of the Agencies adoption service. It has an overriding responsibility to promote good practice, consistency of approach and fairness in all aspects of the adoption service, in accordance with its procedures and values. Historically both nationally and across the region, adoption panels have been inconsistent in their ability to contribute to the delivery of timely outcomes for children and adopters.
The four adoption services within the South Yorkshire Regional Adoption Agency (SYRAA) wish to build on the individual success of the local agencies and improve performance to meet the needs of children requiring permanency through adoption in the three Local Authorities (Barnsley, Rotherham and Sheffield) and Doncaster Children’s Services Trust comprising the SY RAA and are working together to develop standardisation in infrastructure.
9. Key Priorities for 2017-2018.
Care leaver offer – establish a health pathway for young people leaving care.
Designated Doctor and Named Doctor – ensure that Sheffield CCG is complaint with the NHS England Benchmarking and work with the provider service to ensure a Named Doctor LAC is in post and strengthen the role of the Designated Doctor within the CCG.
To develop a robust assurance framework with provider organisations in relation to looked after children who cover leadership, training and quality.
Improve health links and commissioning across the SY &Bassetlaw footprint to improve care across the region in line with the Accountable Care System.
Notification and Consents – ensure that partnership working is continued to improve the timely provision of consent forms in order to meet the statutory deadline.
With the relevance of Future in Mind and in alignment with the Expert Working Group (SCIE) a more holistic health assessment process and mental health therapeutic support should be considered as a priority.
Action for Governing Body / Recommendations
The Governing Body is asked to endorse the above report and note the progress made.
Paper prepared by: Nikki Shepherd and Dr Lorraine Pearson On behalf of: Mandy Philbin, Chief Nurse 14 December 2017
12
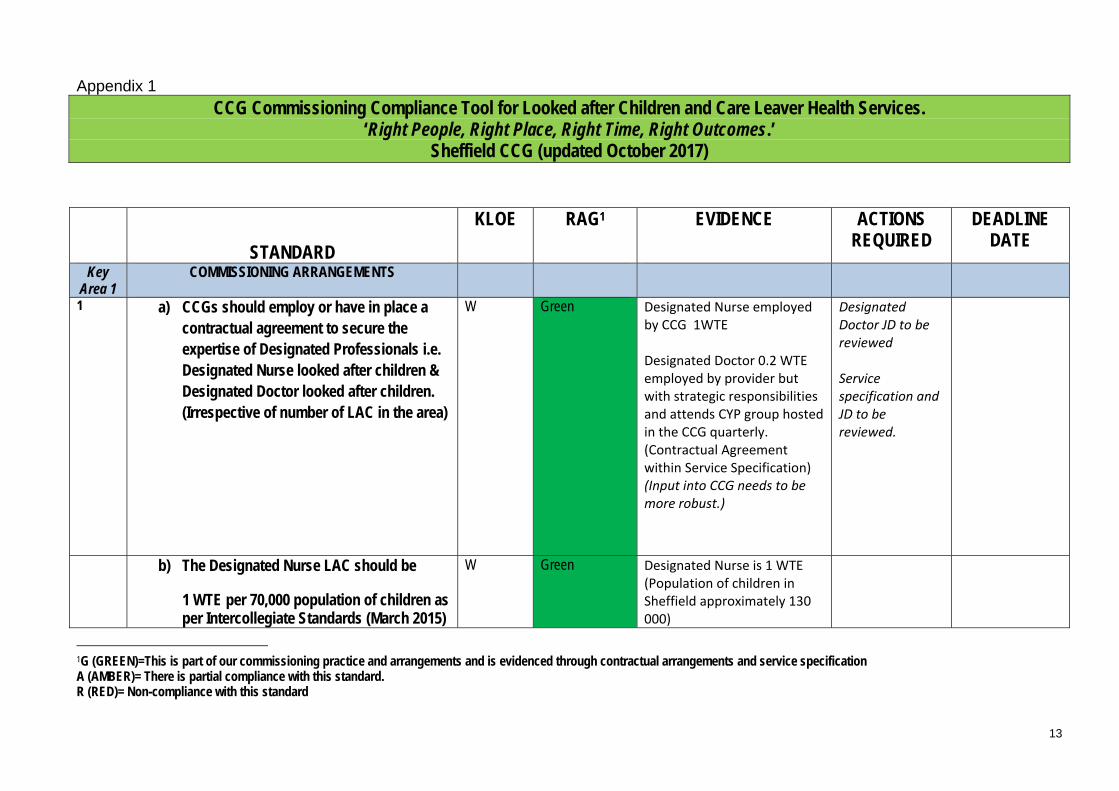
Appendix 1
CCG Commissioning Compliance Tool for Looked after Children and Care Leaver Health Services. ‘Right People, Right Place, Right Time, Right Outcomes.’
Sheffield CCG (updated October 2017)
STANDARD
KLOE RAG1 EVIDENCE ACTIONS REQUIRED
DEADLINE DATE
Key Area 1
COMMISSIONING ARRANGEMENTS
1 a) CCGs should employ or have in place a contractual agreement to secure the expertise of Designated Professionals i.e. Designated Nurse looked after children & Designated Doctor looked after children. (Irrespective of number of LAC in the area)
W Green Designated Nurse employed by CCG 1WTE
Designated Doctor 0.2 WTE employed by provider but with strategic responsibilities and attends CYP group hosted in the CCG quarterly. (Contractual Agreement within Service Specification) (Input into CCG needs to be more robust.)
Designated Doctor JD to be reviewed
Service specification and JD to be reviewed.
b) The Designated Nurse LAC should be
1 WTE per 70,000 population of children as per Intercollegiate Standards (March 2015)
W Green Designated Nurse is 1 WTE (Population of children in Sheffield approximately 130 000)
1G (GREEN)=This is part of our commissioning practice and arrangements and is evidenced through contractual arrangements and service specification A (AMBER)= There is partial compliance with this standard. R (RED)= Non-compliance with this standard
13
Sheffield CCG Designated nurse LA
c) The Designated Doctor LAC should be 2 PA’s per 400 LAC (excluding IHA activity) as per Intercollegiate Document (March 2015)
W Light Green Designated Doctor is 2 PAs.
Job description Consultant Designate
Designated Doctor JD to be reviewed
Service specification and JD to be reviewed.
April 2018
d) The designated role should be strategic, having the authority and autonomy to act in order to embed clinical decision making to influence local thinking and practice and provide advice in complex cases.
W Green Strategic role embedded in Quality Team in Sheffield CCG
DD role is strategic and written in Service Specification 15/16 although this is being reviewed to make the role more robust within the CCG
e) The designated role should be separate from any responsibilities for individual looked after children.
E,W Green Designated Nurse Role in commissioning from January 2015
f) Designated health professionals should have job description and personal specifications in line with the intercollegiate framework document.
W Green See JDs above
14
g) The Designated and Named professional are distinct roles and as such should ideally be separate post holders to avoid potential conflict of interest.
W Amber Named nurse role in provider. No named doctor in post.
Designated Doctor employed in Provider but has strategic function.
Need to ensure DD LAC is embedded into CCG. DN /DD to work with commissioners to
April 2018
ensure a Named Doctor is in post
JD lead Nurse LAC.doc
as per Intercollegiate and Statutory Guidance documents.
h) A Designated Nurse and Doctor for looked after children are members of their
W Green DN attends as required (DD is invited and gets minutes )
regional NHS England Safeguarding Network.
DN is part of the National & Regional Sub Group for LAC NHSE. Attend the Y&H Commissioner Safeguarding Network also.
2 CCG’s must ensure they have a commissioner in post with responsibility for looked after children.
W,R Green DN meets regularly DD meets as required via CYP Commissioning Group Meeting.
3 The CCG lead commissioner for looked after children meets on a quarterly (minimum) basis with designated professionals looked after children.
W,R Green DN/DD attend CYP meetings & at other relevant times and are able to raise LAC issues.
4 Designated professionals, as clinical experts & strategic leaders, advise the Board of Executives, CCG, NHS England, LA (Corporate Parenting Panel) and the LSCB, on all matters relating to looked after children including regulation and inspection.
W,R Green
Priority 3 Health Wellbeing Annual Rep
Designated Nurse LAC to ensure for 2017/18: First CCG Annual Report (2016/17) to GB Jan 2018
April 2018
15
Corporate Parenting Strategy 2015-17.pdf
Corporate Parenting
Strategy Board
member.
Attends Corporate
Parenting.
Service Specification
Briefing papers
Minutes from above
Designated Nurse LAC to write CCG LAC Strategy to be written 2017/8.
Ensure LAC is included on the CCG Safeguarding page
April 2018
Gap analysis provided
through
benchmarking (2016)
against new Statutory
Guidance
Not part of the LSCB
but reports through
the Designated Nurse
Safeguarding
16
CCG Annual report to
be completed 2017
5 Designated professionals looked after children advise CCG commissioners, providers andpartners on the direction and performance monitoring of looked after children health services.
W,R,E Green Monthly performance
figures from LAACH
Team are analysed
and discussed as
required through
Quality Team
meeting.
Priority 3 bi monthly
reporting raised
through Corporate
Parenting Strategy
DNLAC updates
service specification
and liaises with
commissioner with
regards resource
including CQC
compliance.
NHSE Benchmarking
tool updated
regularly.
17
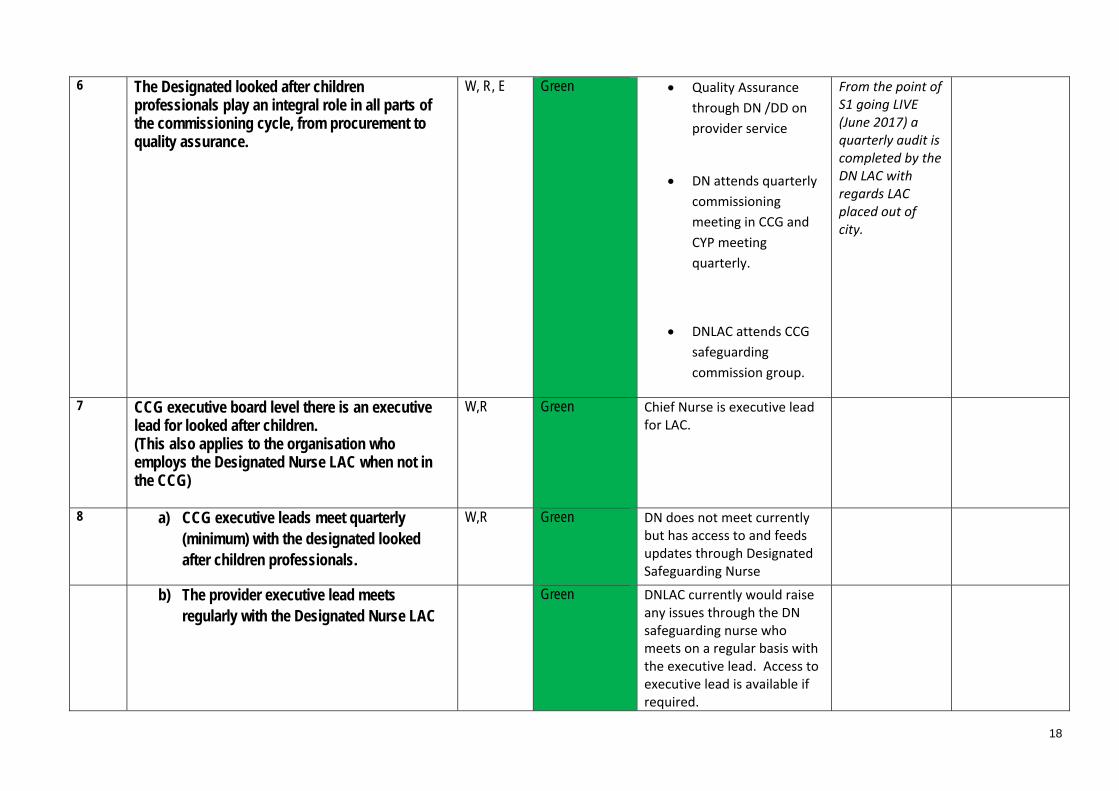
6 The Designated looked after children professionals play an integral role in all parts of the commissioning cycle, from procurement to quality assurance.
W, R, E Green Quality Assurance
through DN /DD on
provider service
DN attends quarterly
commissioning
meeting in CCG and
CYP meeting
quarterly.
From the point of S1 going LIVE (June 2017) a quarterly audit is completed by the DN LAC with regards LAC placed out of city.
DNLAC attends CCG
safeguarding
commission group.
7 CCG executive board level there is an executive lead for looked after children. (This also applies to the organisation who employs the Designated Nurse LAC when not in the CCG)
W,R Green Chief Nurse is executive lead for LAC.
8 a) CCG executive leads meet quarterly (minimum) with the designated looked after children professionals.
W,R Green DN does not meet currently but has access to and feeds updates through Designated Safeguarding Nurse
b) The provider executive lead meets Green DNLAC currently would raise
regularly with the Designated Nurse LAC any issues through the DN safeguarding nurse who meets on a regular basis with the executive lead. Access to executive lead is available if required.
18

9 Designated LAC professionals submit a paper that sets out the health needs of LAC within the local health economy to the Provider, CCG executive leads and to NHS England.
W,R Green Previous Priority 3
Health & Wellbeing
report
Annual report by DN
/DD LAC to be
submitted 2017
DN circulates to Chief
Nurse CCG
DD circulates to
Provider
10 There is 1.0 WTE Named Nurse for looked after children in post per provider organisation(s), witha maximum caseload of 50 LAC.
E,R,W Amber 0.8 WTE Lead Nurse in post in Provider
Ensure that the job description and WTE meets the Intercollegiate Framework Standards (2015) and Statutory Guidance (2015)
April 2018
11 The Named Nurse is responsible for the delivery of the operational level of service; Ensuring that high standards of care are
achieved and maintained
Demonstrating effective performance management and leadership skills.
C,E,W Green Lead nurse LAC with operational / nurse manager role (maximum case load of 50 YP)
Provide oversight of PIs / processes attends Priority 3 multi agency meeting (LA)
Specialist nurses in post for residential and post 16 years
19
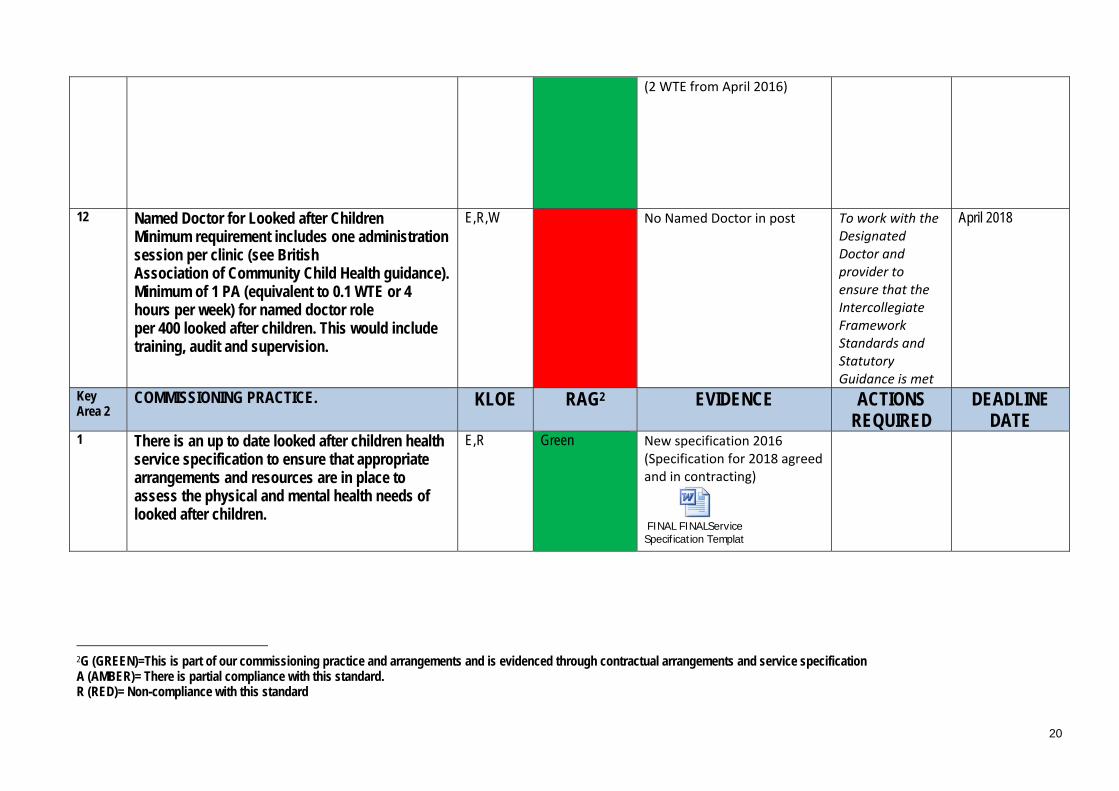
(2 WTE from April 2016)
12 Named Doctor for Looked after Children Minimum requirement includes one administration session per clinic (see British Association of Community Child Health guidance). Minimum of 1 PA (equivalent to 0.1 WTE or 4 hours per week) for named doctor role per 400 looked after children. This would include training, audit and supervision.
E,R,W No Named Doctor in post To work with the Designated Doctor and provider to ensure that the Intercollegiate Framework Standards and Statutory Guidance is met
April 2018
Key Area 2
COMMISSIONING PRACTICE. KLOE RAG2 EVIDENCE ACTIONS REQUIRED
DEADLINE DATE
1 There is an up to date looked after children health service specification to ensure that appropriate arrangements and resources are in place to assess the physical and mental health needs of looked after children.
E,R Green New specification 2016 (Specification for 2018 agreed and in contracting)
FINAL FINALService Specification Template
2G (GREEN)=This is part of our commissioning practice and arrangements and is evidenced through contractual arrangements and service specification A (AMBER)= There is partial compliance with this standard. R (RED)= Non-compliance with this standard
20

2 In accordance with NHS England guidance ‘Who Pays? Determining responsibility for payments to providers’ CCGs and local authorities should have agreed mechanisms in place when making placement decisions and for resolving any funding disputes that may arise.
R Green Annex H used. PbR being established from April 2016
Premise is that a child is seen over any disputes over payment issues.
09/2016 Invoice process in place.
REVIEWED PROCESS (August 2017) based on recommendations from the National LAC Forum. New letters agreed with commissioner and new process via S1 agreed with Provider. Goes live November 2017.
3 On receipt of notification from the LA that a child has become looked after or moved placement, the CCG can give assurance that a robust mechanismin place to ensure that the child’s/ young person’s physical and mental health needs will be met including out of area placements.
R,E Green LAACH team are notified of new placements, change of placements and end of care although assurance that the information received is correct and up to date is needed.
Escalation to social care through the Priority 3 group and the Corporate Parenting Strategy Group. DN LAC is notified through SFX and informs the relevant provider services – STH and
Ensure notification process is robust now provider is on S1
April 2018
21

Dental.
Notification process established and in place. LAACH team will go ‘live’ on 1st October 2016
updated - PROCESS FINAL OLA notificatio
updated -PROCESS FINAL Notification of
Process for the LAACH team to be reviewed once S1 is live.
4 The CCG can give assurance that a robust system is in place to manage and escalate persistent none notification of placement / changes/ cease to belooked after by a placing LA.
S,R Green Escalated through CP Strategy Board if needed & Corporate Parenting Board via DN LAC / DDLAC. Robust pathway needs to be written
22
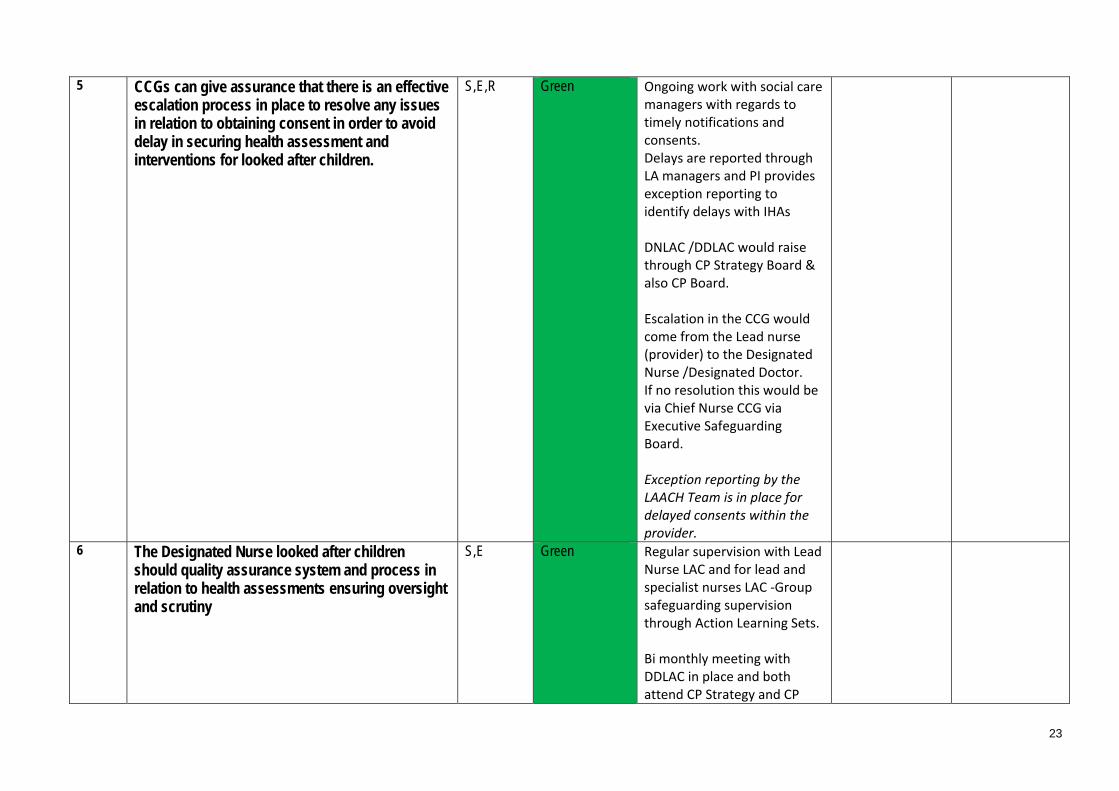
5 CCGs can give assurance that there is an effective escalation process in place to resolve any issuesin relation to obtaining consent in order to avoid delay in securing health assessment and interventions for looked after children.
S,E,R Green Ongoing work with social care managers with regards to timely notifications and consents. Delays are reported through LA managers and PI provides exception reporting to identify delays with IHAs
DNLAC /DDLAC would raise through CP Strategy Board & also CP Board.
Escalation in the CCG would come from the Lead nurse (provider) to the Designated Nurse /Designated Doctor. If no resolution this would be via Chief Nurse CCG via Executive Safeguarding Board.
Exception reporting by the LAACH Team is in place for delayed consents within the provider.
6 The Designated Nurse looked after childrenshould quality assurance system and process in relation to health assessments ensuring oversight and scrutiny
S,E Green Regular supervision with Lead Nurse LAC and for lead and specialist nurses LAC ‐Group safeguarding supervision through Action Learning Sets.
Bi monthly meeting with DDLAC in place and both attend CP Strategy and CP
23

Board.
Service specification places quality assurance role with the provider of the health assessments.
The Designated Nurse LAC completes quarterly audits to ensure compliance from June 2017 when S1 went live.
7 The Designated Nurse looked after children will ensure that health assessment data informs the health needs analysis of the looked after childrenpopulation.
E,R Amber Health data
questionnaire is
completed by
assessing health
professional at health
assessment.
Health Data collated
by LAACH team and
sent to Designated
Nurse in CCG. Final
report June 2017
Future plan in to
analyse this data by
the provider to
inform commissioning
and public health.
Ensure a robust data collection process is in place that ensures a health needs analysis is available and reported on. Health data analysis in draft format. To be presented to CCG and through CP Strategy Board / CP Board.
April 2018
8 The Health Needs Analysis in turn informs the annual report and commissioning agenda bycollating trends and themes for the JSNA.
R, E Amber CCG to work with Public health re this via the Priority 3 Health and Wellbeing Group.
April 2018
24

9 The CCG should ensure a system is in place to capture the voice of the looked after child in order to influence service design and delivery.
S,C,R Amber Voice of the child
captured in IHA
/RHAs and was
highlighted by CQC as
good practice.
Client satisfaction
forms developed by
Lead Nurse. To be
implemented April
2017
Information needs
disseminating
Included in Service
Specification 16/17
DDLAC has met with
the Care Leaver
Forum and has
received feedback
To work with the Children in Care Council and Care Leaver council to ensure the ‘voice of the child’ is represented in service design and delivery
To provide evidence of the voice of young people and how this influences service design.
April 2018
Key Area 3
COMMISSIONING CAMHS. KLOE RAG3 EVIDENCE ACTIONS REQUIRED
DEADLINE DATE
1 CCG’s should ensure that CAMHS and other therapeutic services provide targeted and dedicated support to looked after children
S,E,R Green Dedicated specialist
CAMHS service in
place for Sheffield
3G (GREEN)=This is part of our commissioning practice and arrangements and is evidenced through contractual arrangements and service specification A (AMBER)= There is partial compliance with this standard. R (RED)= Non-compliance with this standard
25
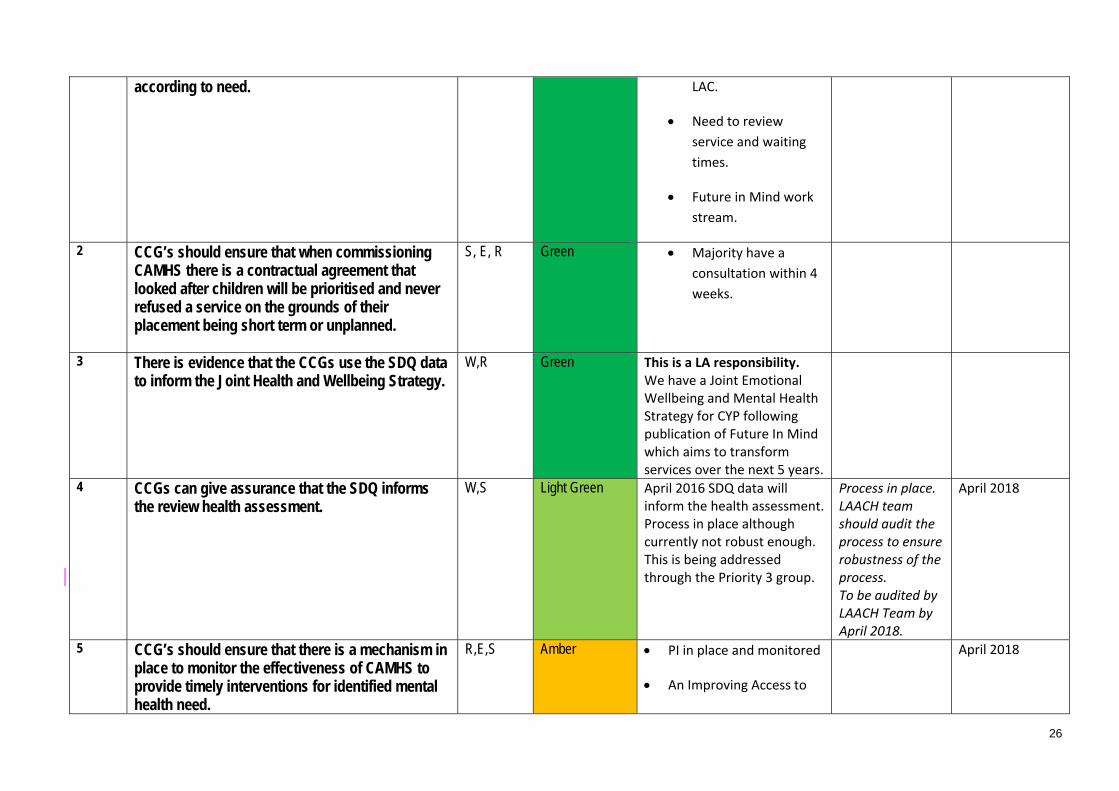
according to need. LAC.
Need to review
service and waiting
times.
Future in Mind work
stream.
2 CCG’s should ensure that when commissioning CAMHS there is a contractual agreement that looked after children will be prioritised and never refused a service on the grounds of their placement being short term or unplanned.
S, E, R Green Majority have a
consultation within 4
weeks.
3 There is evidence that the CCGs use the SDQ data to inform the Joint Health and Wellbeing Strategy.
W,R Green This is a LA responsibility. We have a Joint Emotional Wellbeing and Mental Health Strategy for CYP following publication of Future In Mind which aims to transform services over the next 5 years.
4 CCGs can give assurance that the SDQ informs the review health assessment.
W,S Light Green April 2016 SDQ data will inform the health assessment.
Process in place. LAACH team
April 2018
Process in place although should audit the currently not robust enough. process to ensure This is being addressed robustness of the through the Priority 3 group. process.
To be audited by LAACH Team by April 2018.
5 CCG’s should ensure that there is a mechanism in place to monitor the effectiveness of CAMHS to provide timely interventions for identified mental health need.
R,E,S Amber PI in place and monitored
An Improving Access to
April 2018
26
Services Sub‐Group is part
of the Governance
Structure for our service
transformation work and
is overseeing projects to
improve access and
waiting times
Immediate Identified Risks
Good Practice Group supervision of LAC nurse through action Learning Sets.Joint Health and Wellbeing report as part of the LAAC Strategy (LA)Health assessments forms updated and approved by CQC Visit from Derbyshire LAC TeamSY&B Named Nurse forum Young Person Clinic
27
CQC Key Lines of Enquiry (KLOE)
W – Well led R – Responsive S - Safe
E – Effective C – Caring
References
1. DoH/DfE. (2015). Promoting the Health and Well-Being of Looked After Children. Statutory guidance for local authorities, clinical commissioning groups & NHS England. London: DfE/DoH.
2. NHS England (2015). Safeguarding Vulnerable People in the NHS - Accountability and Assurance Framework. London: NHS England.
3. RCPCH, RCGP & RCN (2015). Looked After Children: Knowledge, Skills and Competences of health care staff. Intercollegiate Role Framework. London: RCPCH.
4. HM Government (2015). Working Togethether to Safeguard Children. A guide to inter-agency working to safeguard and promote the welfare of children. London: HM Government (2015).
28