Embed Size (px)
Citation preview
(2007) 1104–1107
Clinical Biochemistry 40Long-term stability of endogenous B-type natriuretic peptide during storageat −20 °C for later measurement with Biosite Triage assay
Marta Pereira ⁎, Ana Azevedo, Milton Severo, Henrique Barros
Department of Hygiene and Epidemiology, University of Porto Medical School, Alameda Prof Hernâni Monteiro, 4200-319 Porto, Portugal
Received 2 April 2007; received in revised form 29 May 2007; accepted 7 June 2007Available online 20 July 2007
Abstract
Objective: To evaluate the long-term stability of B-type natriuretic peptide (BNP) in frozen samples at −20 °C.Design and methods: During a health and nutrition survey of a representative sample of the adult population of Porto, Portugal, blood samples
were collected in EDTA tubes. Aliquots of plasma were frozen at −20 °C until measurement. Subjects with cardiac structural or functionalabnormalities or renal dysfunction were excluded. BNP was assessed using a commercial immunofluorescence assay (Triage BNP Test®) as acontinuous variable (n=340) and in four subgroups selected according to different storage periods: ≤1 month (n=35), 6–12 months (n=80), 20–24 months (n=18) and ≥36 months (n=21).
Results: Age- and sex-adjusted BNP values, analyzed as a continuous variable, decreased significantly over time of storage. When westratified in four intervals of storage time, the median BNP value (25th–75th percentile, p value) was: 22.6 pg/mL (8.9–76.2, reference group) for≤1 month, 19.8 pg/mL (9.5–48.4, p=0.055) for 6–12 months, 15.3 pg/mL (7.5–35.0, p=0.037) for 20–24 months, and 2.5 pg/mL (2.5–10.5,pb0.001) for ≥36 months.
Conclusions: BNP is stable at −20 °C for 1 year, without protease inhibitors.© 2007 The Canadian Society of Clinical Chemists. Published by Elsevier Inc. All rights reserved.
Keywords: B-type natriuretic peptide; Stability; Immunoassay; Temperature
Introduction
B-type natriuretic peptide (BNP) is a biochemical markersynthesized and secreted in the ventricular myocardium inresponse to pressure or volume overload [1]. The biologicalactions of BNP are the reduction of blood pressure and plasmavolume, as a result of natriuresis, vasodilatation, suppression ofrenin and aldosterone actions, suppression of sympatheticactivity and inhibition of vascular smooth muscle growth [2].Plasma concentrations of BNP are different when comparinghealthy individuals with heart failure patients. This makes BNP auseful biomarker for diagnosis and prognosis of heart failure andfor its precursor, left ventricular systolic dysfunction [3]. Severalphysiological and clinical conditions explain the biological
Abbreviations: BNP, B-type natriuretic peptide; EDTA, ethylenediaminete-traacetic acid.⁎ Corresponding author. Fax: +351 22 551 36 53.E-mail address: [email protected] (M. Pereira).
0009-9120/$ - see front matter © 2007 The Canadian Society of Clinical Chemistsdoi:10.1016/j.clinbiochem.2007.06.014
variation of the natriuretic peptides, such as increasing age,female sex, systemic hypertension and renal failure [4–8].
In routine clinical practice BNP measurements are doneshortly after blood withdrawal, usually within hours. Samplestorage is not an issue in that context. In contrast, in researchprojects, it is usual to store samples for variable periods andperform measurements in batches. The storage could be done atdifferent temperatures (usually −20 °C or −80 °C), using aprotease inhibitor or not, in whole blood or in plasma samples.
Using information obtained from healthy subjects as part of apopulation survey, we compared BNP plasma levels in samplesfrozen at −20 °C, without protease inhibitors, according to theduration of storage.
Methods
As part of a health and nutrition survey of the adult populationof Porto, Portugal, we measured parameters of cardiac structureand function in 653 randomly selected participants aged ≥45
. Published by Elsevier Inc. All rights reserved.
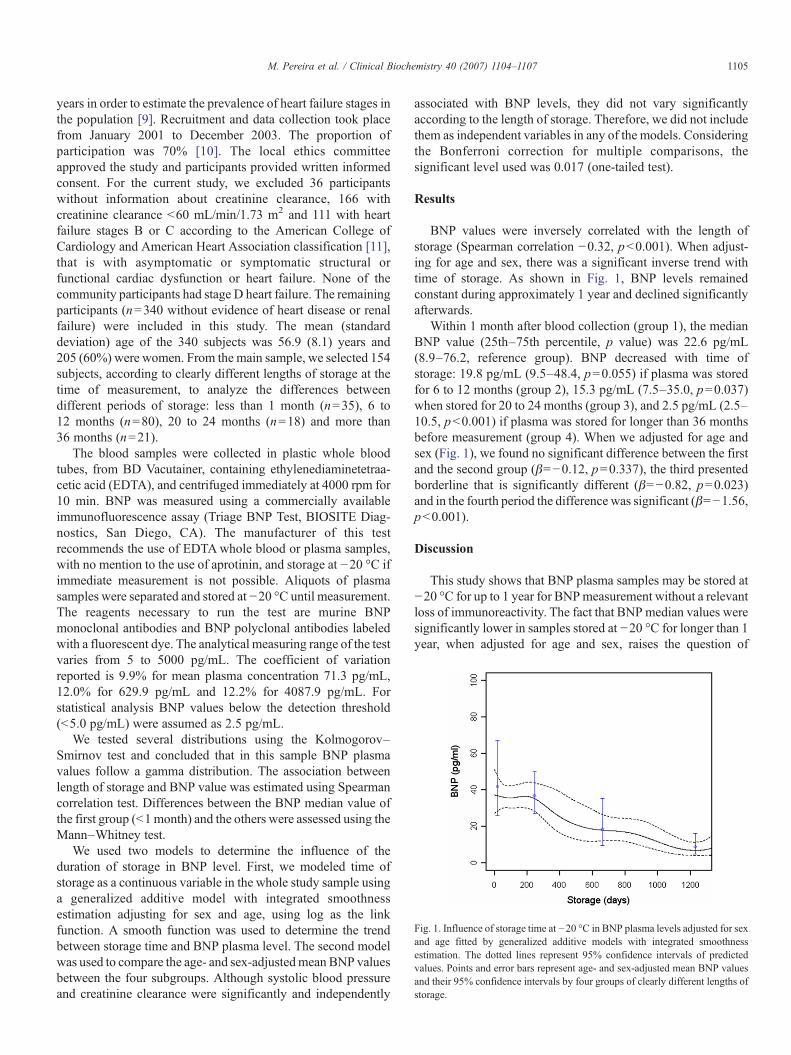
Fig. 1. Influence of storage time at −20 °C in BNP plasma levels adjusted for sexand age fitted by generalized additive models with integrated smoothnessestimation. The dotted lines represent 95% confidence intervals of predictedvalues. Points and error bars represent age- and sex-adjusted mean BNP valuesand their 95% confidence intervals by four groups of clearly different lengths ofstorage.
1105M. Pereira et al. / Clinical Biochemistry 40 (2007) 1104–1107
years in order to estimate the prevalence of heart failure stages inthe population [9]. Recruitment and data collection took placefrom January 2001 to December 2003. The proportion ofparticipation was 70% [10]. The local ethics committeeapproved the study and participants provided written informedconsent. For the current study, we excluded 36 participantswithout information about creatinine clearance, 166 withcreatinine clearance b60 mL/min/1.73 m2 and 111 with heartfailure stages B or C according to the American College ofCardiology and American Heart Association classification [11],that is with asymptomatic or symptomatic structural orfunctional cardiac dysfunction or heart failure. None of thecommunity participants had stage D heart failure. The remainingparticipants (n=340 without evidence of heart disease or renalfailure) were included in this study. The mean (standarddeviation) age of the 340 subjects was 56.9 (8.1) years and205 (60%) were women. From the main sample, we selected 154subjects, according to clearly different lengths of storage at thetime of measurement, to analyze the differences betweendifferent periods of storage: less than 1 month (n=35), 6 to12 months (n=80), 20 to 24 months (n=18) and more than36 months (n=21).
The blood samples were collected in plastic whole bloodtubes, from BD Vacutainer, containing ethylenediaminetetraa-cetic acid (EDTA), and centrifuged immediately at 4000 rpm for10 min. BNP was measured using a commercially availableimmunofluorescence assay (Triage BNP Test, BIOSITE Diag-nostics, San Diego, CA). The manufacturer of this testrecommends the use of EDTAwhole blood or plasma samples,with no mention to the use of aprotinin, and storage at −20 °C ifimmediate measurement is not possible. Aliquots of plasmasamples were separated and stored at −20 °C until measurement.The reagents necessary to run the test are murine BNPmonoclonal antibodies and BNP polyclonal antibodies labeledwith a fluorescent dye. The analytical measuring range of the testvaries from 5 to 5000 pg/mL. The coefficient of variationreported is 9.9% for mean plasma concentration 71.3 pg/mL,12.0% for 629.9 pg/mL and 12.2% for 4087.9 pg/mL. Forstatistical analysis BNP values below the detection threshold(b5.0 pg/mL) were assumed as 2.5 pg/mL.
We tested several distributions using the Kolmogorov–Smirnov test and concluded that in this sample BNP plasmavalues follow a gamma distribution. The association betweenlength of storage and BNP value was estimated using Spearmancorrelation test. Differences between the BNP median value ofthe first group (b1month) and the others were assessed using theMann–Whitney test.
We used two models to determine the influence of theduration of storage in BNP level. First, we modeled time ofstorage as a continuous variable in the whole study sample usinga generalized additive model with integrated smoothnessestimation adjusting for sex and age, using log as the linkfunction. A smooth function was used to determine the trendbetween storage time and BNP plasma level. The second modelwas used to compare the age- and sex-adjustedmean BNP valuesbetween the four subgroups. Although systolic blood pressureand creatinine clearance were significantly and independently
associated with BNP levels, they did not vary significantlyaccording to the length of storage. Therefore, we did not includethem as independent variables in any of the models. Consideringthe Bonferroni correction for multiple comparisons, thesignificant level used was 0.017 (one-tailed test).
Results
BNP values were inversely correlated with the length ofstorage (Spearman correlation −0.32, pb0.001). When adjust-ing for age and sex, there was a significant inverse trend withtime of storage. As shown in Fig. 1, BNP levels remainedconstant during approximately 1 year and declined significantlyafterwards.
Within 1 month after blood collection (group 1), the medianBNP value (25th–75th percentile, p value) was 22.6 pg/mL(8.9–76.2, reference group). BNP decreased with time ofstorage: 19.8 pg/mL (9.5–48.4, p=0.055) if plasma was storedfor 6 to 12 months (group 2), 15.3 pg/mL (7.5–35.0, p=0.037)when stored for 20 to 24 months (group 3), and 2.5 pg/mL (2.5–10.5, pb0.001) if plasma was stored for longer than 36 monthsbefore measurement (group 4). When we adjusted for age andsex (Fig. 1), we found no significant difference between the firstand the second group (β=−0.12, p=0.337), the third presentedborderline that is significantly different (β=−0.82, p=0.023)and in the fourth period the difference was significant (β=−1.56,pb0.001).
Discussion
This study shows that BNP plasma samples may be stored at−20 °C for up to 1 year for BNPmeasurement without a relevantloss of immunoreactivity. The fact that BNP median values weresignificantly lower in samples stored at −20 °C for longer than 1year, when adjusted for age and sex, raises the question of

1106 M. Pereira et al. / Clinical Biochemistry 40 (2007) 1104–1107
validity of BNP measurements when obtained with thisimmunofluorescence assay (Triage BNP Test, Biosite) undersuch conditions. The recommendation of the manufacturer isvalid for up to 1 year of storage at −20 °C.
Mueller et al. [12] reported that mean recovery of BNP wasless than 70% after 1 day of storage at −20 °C and decreased toless than 50% after 2 to 4 months of storage. This could beexplained by their large ranging of recovery and the utilization ofa different assay (AxSYM). The differences between assayswere analyzed by Yeo et al. [13] who found that Biosite BNPassay showed worse analytical performance and larger degrada-tion in plasma samples stored at room temperature and 4 °C thanthe Roche NT-proBNP assay. This could be due to differences inthe stability of epitopes of BNP that are recognized by thedifferent antisera.
The utilization of a protease inhibitor could be one solutionfor the degradation of BNP. Belenky et al. [14] suggest the use ofa specific kallikrein protease inhibitor to eliminate BNPdegradation in patient samples for up to 6–10 days when storedat 2–8 °C. Gobinet-Georges et al. [15] demonstrated that the useof aprotinin prevents, in most cases, the degradation in wholeblood samples after 3 months at −20 °C, whereas BNP leveldecreases by 50% of subjects without aprotinin. Gruson et al.[16], using blood samples from 4 heart failure patients, could notdemonstrate a significant benefit with the use of aprotinin indecreasing degradation at room temperature for 24 h. However,the conditions in this small study were quite different from ours,precluding extrapolation to a longer storage time at lowertemperature. The tubes for blood collection might also influencestability. Shimizu et al. [17,18] reported that collection andstorage of BNP in plastic (polyethylene terephthalate, PET)resulted in increased recovery of BNP in comparison with glasstubes. Another potentially efficient way of preventing degrada-tion is to reduce the temperature of storage. Gobinet-Georges etal. [15] demonstrated that a freezing temperature of −70 °C candispense the use of aprotinin. The effect of the anticoagulant wasstudied by Evans et al. [19], who reported no significantdifferences in BNP level between EDTA plasma, heparin plasmaand serum at −20 °C. Additional studies are warranted to clarifyhow samples should be managed for long-term storage.
Our data result from the comparison of independent samples,that is, some individuals had their plasma stored for shorterperiods and others for longer periods with only onemeasurementavailable for each participant. The ideal design would compriseanalysis of samples obtained from the same individuals andassessed repeatedly at different storage periods. That wouldadditionally allow us to calculate the speed of degradation.Nevertheless, the probability of subjects whose plasma wasstored for a longer time having in fact lower BNP levels isminimal because the order of measurement was determined bythe consecutive recruitment to the study, which was obviouslyindependent of the natriuretic peptides system activation. Also,to avoid other sources of confounding, we restricted theevaluation to subjects without cardiac or renal dysfunction, themain determinants of BNP variation.
The fact that BNP and synthetic forms of the peptide areprone to relatively rapid decomposition in blood plasma and
serum as a result of proteolysis, by the intervention of activatedprotease [14], is a plausible explanation for our findings.
In order to formally test the effect of length of storage,ideally we should have the referent BNP concentrationmeasured immediately after blood withdrawal with no freezingat all and then performed repeated measurements in parts of thesame sample stored for progressively longer periods of time.Given the current observation, this will be the focus of a specificstudy designed to assess BNP degradation. Also by comparingstorage at different temperatures such as −20 °C and −80 °C wewould be able to assess whether it is worth investing ininfrastructures for storage at lower temperatures. The presentresults and those expected from experiments under the proposedconditions will help clarify at least partly some of theheterogeneous results regarding the role of BNP in the earlyidentification of systolic dysfunction or heart failure inpopulation surveys [20].
Acknowledgment
The authors gratefully acknowledge a grant from Fundaçãopara a Ciência e a Technologia (POCTI/SAU-ESP/61492/2004).
References
[1] Munagala VK, Burnett Jr JC, Redfield MM. The natriuretic peptides incardiovascular medicine. Curr Probl Cardiol 2004;29(12):707–69.
[2] Suttner SW, Boldt J. Natriuretic peptide system: physiology and clinicalutility. Curr Opin Crit Care 2004;10(5):336–41.
[3] Bettencourt PM. Clinical usefulness of B-type natriuretic peptidemeasurement: present and future perspectives. Heart 2005;91(11):1489–94.
[4] Cheung BM, Brown MJ. Plasma brain natriuretic peptide and C-typenatriuretic peptide in essential hypertension. J Hypertens 1994;12(4):449–54.
[5] Buckley MG, Markandu ND, Miller MA, Sagnella GA, MacGregor GA.Plasma concentrations and comparisons of brain and atrial natriureticpeptide in normal subjects and in patients with essential hypertension.J Hum Hypertens 1993;7(3):245–50.
[6] Wang TJ, Larson MG, Levy D, Leip EP, Benjamin EJ, Wilson PW, et al.Impact of age and sex on plasma natriuretic peptide levels in healthyadults. Am J Cardiol 2002;90(3):254–8.
[7] Almeida P, Azevedo A, Rodrigues R, Dias P, Frioes F, Vazquez B, et al.B-type natriuretic peptide and left ventricular hypertrophy in hypertensivepatients. Rev Port Cardiol 2003;22(3):327–36.
[8] Joffy S, Rosner MH. Natriuretic peptides in ESRD. Am J Kidney Dis2005;46(1):1–10.
[9] Azevedo A, Bettencourt P, Dias P, Abreu-Lima C, Hense H-W, Barros H.Population based study on the prevalence of the stages of heart failure.Heart 2006;92:1161–3.
[10] Ramos E, Lopes C, Barros H. Investigating the effect of nonparticipationusing a population-based case–control study on myocardial infarction.Ann Epidemiol 2004;14(6):437–41.
[11] Hunt SA, Baker DW, Chin MH, Cinquegrani MP, Feldman AM, FrancisGS, et al. ACC/AHA guidelines for the evaluation and management ofchronic heart failure in the adult: executive summary: a report of theAmerican College of Cardiology/American Heart Association Task Forceon Practice Guidelines (committee to revise the 1995 guidelines for theevaluation and management of heart failure). J Am Coll Cardiol 2001;38(7):2101–13.
[12] Mueller T, Gegenhuber A, Dieplinger B, Poelz W, Haltmayer M. Long-term stability of endogenous B-type natriuretic peptide (BNP) and amino

1107M. Pereira et al. / Clinical Biochemistry 40 (2007) 1104–1107
terminal proBNP (NT-proBNP) in frozen plasma samples. Clin Chem LabMed 2004;42(8):942–4.
[13] Yeo KT, Wu AH, Apple FS, Kroll MH, Christenson RH, LewandrowskiKB, et al. Multicenter evaluation of the Roche NT-proBNP assay andcomparison to the Biosite Triage BNP assay. Clin Chim Acta 2003;338(1–2):107–15.
[14] Belenky A, Smith A, Zhang B, Lin S, Despres N, Wu AH, et al. The effectof class-specific protease inhibitors on the stabilization of B-type natriureticpeptide in human plasma. Clin Chim Acta 2004;340(1–2): 163–72.
[15] Gobinet-Georges A, Valli N, Filliatre H, Dubernet MF, Dedeystere O,Bordenave L. Stability of brain natriuretic peptide (BNP) in human wholeblood and plasma. Clin Chem Lab Med 2000;38(6):519–23.
[16] Gruson D, Rousseau MF, de Coninck V, Ahn SA, Ketelslegers JM.Influence of sampling and storage conditions on B-type natriuretic
peptide immunoreactivity for 3 automated assays. Clin Chem 2006;52(4):766–7.
[17] Shimizu H, Aono K, Masuta K, Asada H, Misaki A, Teraoka H. Stability ofbrain natriuretic peptide (BNP) in human blood samples. Clin Chim Acta1999;285(1–2):169–72.
[18] Shimizu H, Aono K, Masuta K, Asada H, Misaki A, Teraoka H.Degradation of human brain natriuretic peptide (BNP) by contact activationof blood coagulation system. Clin Chim Acta 2001;305(1–2):181–6.
[19] Evans MJ, Livesey JH, Ellis MJ, Yandle TG. Effect of anticoagulantsand storage temperatures on stability of plasma and serum hormones.Clin Biochem 2001;34(2):107–12.
[20] Doust JA, Glasziou PP, Pietrzak E, Dobson AJ. A systematic review of thediagnostic accuracy of natriuretic peptides for heart failure. Arch InternMed 2004;164(18):1978–84.