Embed Size (px)
Citation preview
Long-term retrospectiveevaluation of short implants inthe posterior areas: clinicalresults after 10–12 yearsAnitua E, Pi~nas L, Bego~na L, Orive G. Long-term retrospective evaluation of shortimplants in the posterior areas: clinical results after 10–12 years. J ClinPeriodontol 2014; 41: 404–411. doi: 10.1111/jcpe.12222.
AbstractAim: To evaluate the long-term clinical results of short implants in the posteriorareas and analyse the possible influence of different variables on implant successrate and marginal bone loss (MBL).Methods: A retrospective study design was used. Patients were included if theyhad received one or more short implants (≤8.5 mm long) in the posterior jaws atleast 10 years earlier. All implants were embedded in plasma rich in growth fac-tors (PRGF). The cumulative success rate was the primary outcome. MBL andthe influence of different variables as secondary outcomes were assessed.Results: A total of 111 short implants (7.0, 7.5 and 8.5 mm in length) placed in75 patients met the inclusion criteria. Of which, 94 were splinted to longer ones.The mean follow-up was 123.3 months (SD = 10.4 months). The mean crown-implant ratio was 1.4 (SD = 0.3). The mean MBL was 1.0 mm at mesial(SD = 0.7) and 0.9 mm (SD = 0.6) at distal aspect. One short implant failed. Suc-cess rate was 98.9% and 98.2% for the implant and patient-based analysis respec-tively. No relationship was observed between the studied variables and the MBL.Conclusions: These clinical results support the use of short implants as an effec-tive and safe long-term treatment option.
Eduardo Anitua1,2, Laura Pinas1,Leire Begona2 and Gorka Orive2
1Private Practice in Implantology and Oral
Rehabilitation in Vitoria, Vitoria, Spain;2Foundation Eduardo Anitua, Vitoria, Spain
Key words: long-term; PRGF; short implants
Accepted for publication 12 December 2013
In patients with long-standing eden-tulous arches, alveolar bone resorp-tion (both vertical and horizontal orcombined defects) is frequently
observed (Reich et al. 2011). Theinsertion of dental implants inpatients with reduced alveolar boneheight is challenging and mayrequire additional invasive bone aug-mentation procedures (Tonetti &Hammerle 2008, Esposito et al.2009). By modifying patient’s anat-omy, it is possible to insert longerimplants, but an extra surgical inter-vention may also lead to greaterpatient morbidity, higher costs andlonger treatment periods (Espositoet al. 2010, Telleman et al. 2011).
The introduction of shortimplants has represented a veryimportant progress in the implant
dentistry field and a new therapeuticalternative for these cases (Anitua2010). Situations including the pos-terior mandibular and maxillaryregions, which are characterized bythe difficult access, limited visibility,reduced space, poor bone qualityand the risk of affecting the inferioralveolar nerve candidate for treat-ment with short implants. However,the predictability of short implantswas initially controversial. In fact,some studies using short implantsreported lower survival rates thanlonger ones (Romeo et al. 2010).These results were explained bydifferent reasons including less bone
Conflict of interest and source offunding statement
This study was funded by FoundationEduardo Anitua (Vitoria, Spain). Edu-ardo Anitua is the president of thisfoundation. EA and LB are scientistsat Biotechnology Institute, the com-pany that produces the dentalimplants used in the present study.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd404
J Clin Periodontol 2014; 41: 404–411 doi: 10.1111/jcpe.12222

to implant contact associated withshort implants; the fact that shortimplants are mostly placed in poster-ior areas where the quality of thealveolar bone is relatively poor, andthe fact that often a very outsizedcrown has to be made to achieveproper occlusion, which causes ahigher crown to implant (C/I) ratio.
Recent systematic reviews havereported that short implants havesimilar long-term prognosis as stan-dard-length dental implants (Kotsov-ilis et al. 2009, Menchero-Cantalejoet al. 2011, Sun et al. 2011, Tellemanet al. 2011, Annibali et al. 2012,Atieh et al. 2012, Karthikeyan et al.2012, Srinivasan et al. 2012). Cur-rent scientific knowledge suggests theuse of short implants as an alterna-tive to more invasive bone augmen-tation techniques (Esposito et al.2009, 2010, 2011, Felice et al. 2010).Furthermore, short implants mayprovide additional advantages andcause fewer complications thanlonger implants when combined withmore complex techniques (Espositoet al. 2010). These evidences havebeen reinforced by the different bio-mechanical studies suggesting thatmaximum bone stress is practicallyindependent of implant length (Pier-risnard et al. 2003) and even thatimplant width is more importantthan the additional length (Anituaet al. 2010).
Interestingly, although there is anincreasing body of literature onshort implants and on their short-and medium-term predictability, veryfew studies have properly evaluatedtheir long-term clinical results. Theobjective of this retrospective studywas to evaluate the safety and long-term predictability (10–12 years offollow-up after implant installation)of short implants (≤8.5 mm) placedin posterior regions of maxillae andmandible. The main leading questionto address was: for short implantsplaced in the posterior jaws, areimplant success rate and marginalbone loss (MBL) after 10 years offunction affected by prosthetic andimplant variables?
Material and methods
This article was written followingthe Strengthening the Reporting ofObservational studies in Epidemiologyguidelines (von Elm et al. 2007) and
included patients treated at theCl�ınica Dental Eduardo Anitua atVitoria, Spain.
A retrospective case series studydesign was used. To achieve theobjectives of the study, the patient’smedical records database of theclinic was reviewed to find poten-tially eligible patients.
Patients were included in thestudy if fulfilled they all of the fol-lowing criteria:
• Patients over 18 years old.
• Presence of partial or complete e-dentulism requiring treatmentwith dental implants.
• One or more short implants(≤8.5 mm in length) were placedin the posterior areas of maxillaor mandible.
• Implants were inserted at least10 years earlier (before Septem-ber 2002).
After case selection, each of thepatient’s medical records was care-fully reviewed to obtain the neces-sary clinical data and the predefinedvariables for each implant-patient toachieve the objectives of the study.A total of 111 short BTI acid-etchedsurface implants (Biotechnology Ins-titute BTI, Vitoria, Spain) placed in75 patients in maxilla and mandiblewere included and evaluated.
The cumulative success rate wasconsidered the primary outcome.MBL and the possible influence ofdifferent patients, implant and pros-thetic variables as secondary end-points were also assessed.
Implant placement-surgical protocol
In all patients the same surgical pro-tocol and treatment plan was fol-lowed. Before surgery, patientsunderwent a routine dental scaling tostart the implant treatment with anadequate gingival status. A conebeam computed tomography scanwas carried out to all patients priorto the intervention to assess bonequality and quantity and to measurethe ridge height and width of the sup-porting bone using specialized soft-ware for implant surgery planning(BTI Scan�; Biotechnology InstituteBTI). Panoramic X-rays were alsotaken prior and after surgery for allpatients to allow careful planning ofthe treatment. Rehabilitations were
made by three equally experiencedprosthodontists.
During the days prior to the inter-vention, all patients received ade-quate prophylaxis and oral hygieneinstructions. Patients received 1 g ofamoxicillin and 1 g of acetaminophenas prophylactic medication 1 h beforethe intervention. Antibiotic adminis-tration continued during 5 days aftersurgery. At the time prior to the inter-vention, all patients performed 1-minrinses with chlorhexidine digluconate0.20%. Lips and perioral area werealso cleaned with chlorhexidine. Aninfiltrative anaesthesia was appliedto all patients and incisions weremade to elevate a full-thickness flap.Implant sites were prepared usinga low-speed drilling procedure(125 rpm) without irrigation (Anituaet al. 2007a). Before installation,implants were carefully embedded inliquid plasma rich in growth factors(PRGF-Endoret�; BiotechnologyInstitute BTI) with the aim of bioacti-vating the implant surface (Anituaet al. 2007b). PRGF was preparedfrom each patient by taking blood byvenipuncture before surgery andplacing it directly into 9-ml blood-collecting tubes� (BiotechnologyInstitute BTI) that contain 3.8% (wt/vol) sodium citrate as anticoagulant.Liquid PRGF was prepared by centri-fugation (PRGF System�, BTI) at580 g for 8 min at room temperature.The 2 ml plasma fraction located justabove the red cell fraction, but notincluding the buffy coat, was col-lected and deposited in a glass dish.To initiate clotting, formation of athree-dimensional fibrin matrix andthe release of growth factors andproteins, PRGF activator� (calciumchloride) was added to the liquidPRGF preparation (50 ll PRGFactivator per millilitre of preparation)(Anitua et al. 2007b). In general,healing was allowed for a minimumof 3 months, after which the surgi-cal abutments were fixed. Shortlythereafter, the suprastructure wasplaced.
Most implants (74.9%) wereloaded between 3 and 7 months afterinsertion [mean value 4.91 months(SD = 2.12)]. Prior to the final pros-thesis placement, implants wereloaded with a provisional screwedprosthesis to promote a progressiveimplant loading. The provisionalprosthesis was made of titanium and
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Long-term evaluation of short implants 405

composite resin. The final prosthesis,also made of a titanium structure,was placed after 6–9 months. Occlu-sion was always checked and themajority of implants were splinted.
After the intervention, patientswere encouraged to take in case ofpain, acetaminophen (1 g/8 h) or Ib-uprofen (600 mg/8 h). Patients werealso instructed how to maintainproper oral hygiene around implants.In addition, just after the interven-tion, a panoramic radiograph wastaken to verify the adequate place-ment of the implant.
Once the surgical phase was con-ducted patients were referred to peri-odic evaluations, consisting of: oneevaluation 5–10 days after interven-tion, at 1 month, at 3 months, at6 months and from this momentahead, once a year. The post-implantassessment included at each follow-up visit different clinical assessmentsto verify the status of the implant(gingival health, prosthesis mobility,pain, infection, alveolar ridge resorp-tion and any complications) as wellas periodic panoramic radiographsto verify the appropriate state of theimplant in the follow-up period.
For success rate calculation, theimplant was considered to be success-ful if it complied with the followingsuccess criteria: a stable prosthe-sis, absence of pain, infections orany other pathology related to theimplants, absence of a radiolucentline around the implant and if noneof the following events occur: implantloss, fracture that makes support ofthe prosthesis impossible, significantbone loss (>2–3 mm) and lack ofosseointegration.
For survival rate calculation,implant failure was considered anyimplant lost due to any cause, eitherbiological (failure to achieve osseoin-tegration or loss of acquired osseoin-tegration) or biomechanical causes.
For MBL quantifications, mar-ginal bone levels were measured onthe panoramic radiograph made justafter the surgery and the lastpatient’s available radiograph.
All panoramic radiographs wereperformed using a positioning pin(with patient’s chin resting on astandard device) and with the Frank-furt plane parallel to the ground.Measurements on the panoramicradiographs were performed bycomputer software (Sidexis XG;
Sirona Dental Systems, Bensheim,Germany), which conducts a calibra-tion of the X-ray by a known length(implant length). Once the radio-graph was calibrated to a 1:1 mea-sure, eliminating the possiblepresence of magnification, measure-ments were made mesially and dis-tally to the implants, calculating thedistance between the uppermostpoint of the implant platform andthe most coronal contact betweenthe bone and the implant. The bonelevel recorded just after the surgicalinsertion of the implant was thebasal value to compare with subse-quent measurements over time.
Demographic, surgery and imp-lant dependent variables, as wellother prosthetic-biomechanical vari-ables were also registered frompatient’s clinical records.
Statistical analysis
Data collection and analysis were per-formed by two independent examin-ers (other than restorative dentists).Descriptive statistics were performedwhen necessary considering theimplant and the patient as the unit ofanalysis. Absolute and relative fre-quency distributions were calculatedfor qualitative variables (either nomi-nal as patient’s gender, implant’smaxilla type or ordinals as prosthesistype) and mean values and standarddeviations for quantitative variables(either discrete or continuous as MBLor crown height). Survival and successrate were estimated both by animplant-based and subject-basedanalysis. In the patient-based analy-sis, the patient was considered theunit of analysis if they had at leastone short implant inserted that metthe study selection criteria. For thesecalculations, the dates of the firstimplant inserted and the first to fail ornot meet the criteria of success (evenif they were the same one or not) wereconsidered. In both types of analysis,the cumulative survival rate as a func-tion of the time was analysed using alife-table analysis (Actuarial method).Mann–Whitney non-parametric testwas used to evaluate the possible dif-ferences in bone loss in both mesialand distal points in categorical vari-ables. To assess the possible associa-tion between quantitative variablesand bone loss, linear regression analy-sis was used. The potential influence
of different variables on implantsuccess rate was evaluated using Coxregression analysis. Statistical level ofsignificance was set at p < 0.05. SPSSv15.0 for Windows statistical softwarepackage (SPSS Inc., Chicago, IL,USA) was used for statistical analysis.
Results
A total of 111 short implants and 97prostheses placed in 75 patients wereincluded and evaluated. The diameterof short implants ranged between3.30 and 5.00 mm, and the lengthsbetween 7.0 and 8.5 mm. Thefrequency of the lengths and diame-ters of the included short implants isshown in Table 1. A total of 134implants of standard size (from 3.30and 5 mm diameter and from 10 to15 mm length) were also used incombination with short implants in94 rehabilitations (78 fixed partialbridges and 16 complete overden-tures). Sixty-one patients werefemales (81.3%) and the mean age atinsertion time was 58.2 years(SD = 9.8, range 28–84). Twenty-onepatients were smokers (28.0%).
On implant basis, the meanfollow-up time since insertion was123.3 months (SD = 10.4; range86–141 months), more than 10 years,while the mean follow-up time sinceloading was 118.0 months (SD =11.0; range 83–137 months). On apatient basis the mean follow-up timesince insertion was 122.6 months(SD = 12.4 months) and it was117.5 months (SD = 12.2 months)from loading.
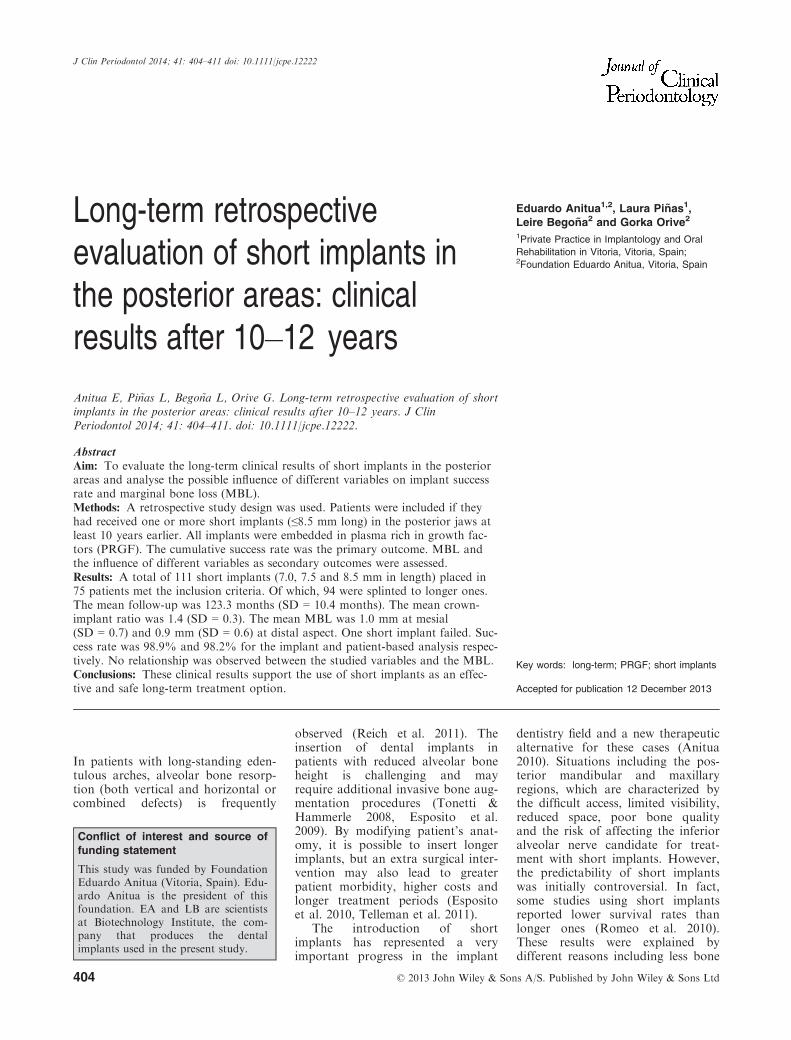
A total of 67 implants (60.4%)were placed in the posterior areas ofthe mandible, whereas 44 were placedin the posterior maxilla (39.6%). Fig-ure 1 shows the anatomical locationof short implants. Eleven implants(9.9%) were placed using special tech-
Table 1. Distribution of diameters andlengths of included short implants
Length (mm) Total
7.00 7.50 8.50
Diameter(mm)
3.30 0 0 15 153.75 2 0 43 454.00 0 0 29 294.50 0 7 12 195.00 0 0 3 3
Total 2 7 102 111
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
406 Anitua et al.
niques (sinus elevation, immediatepost-extraction or crest-split expan-sion). Only three implants (2.7%)were submitted to immediate loadingprotocol, whereas 33 implants(29.7%) underwent two surgicalphases.
Regarding the type of prosthesis,87 (78.4%) implants were involvedin a total of 78 fixed partial bridgessupported by two to four splintedimplants, 75 of them cemented,whereas 21 implants were involvedin 16 screwed complete overdentures(18.9%), and the three remainingimplants were cemented singlecrowns (2.7%).
Most implants (108 implants,97.3%) were splinted to otherimplants (to one or two implants).Specifically, 14 of these implants weresplinted only to other short implants(12.6%, 10 implants to one shortimplant and four implants to twoshort implants). The remaining 94implants were splinted to one or morelong implants (84.7%, 12 implants toone short and one long implants, 42implants to only one long implantand 40 implants to two longimplants).
The mean length of the crownwas 11.9 mm (SD = 2.7; rangebetween 7.2 and 19.4 mm). The cal-culated crown to implant ratio (C/Iratio) ranged between 0.9 and 2.5,showing a mean C/I ratio of 1.4(SD = 0.3). The C/I ratio of nineimplants (8.1%) was less than one,whereas it was ≥1 in 102 implants(91.9%). Table 2 shows mean C/Iratio values by implant length andjaw (maxilla and mandible).
In the opposing jaw, implant-sup-ported bridge was the most frequentantagonist prostheses (in 33 prosthe-ses, 34.0%), followed by naturaltooth (28 prostheses, 28.9%) andimplant-supported complete prosthe-ses (15 prostheses, 15.5%).
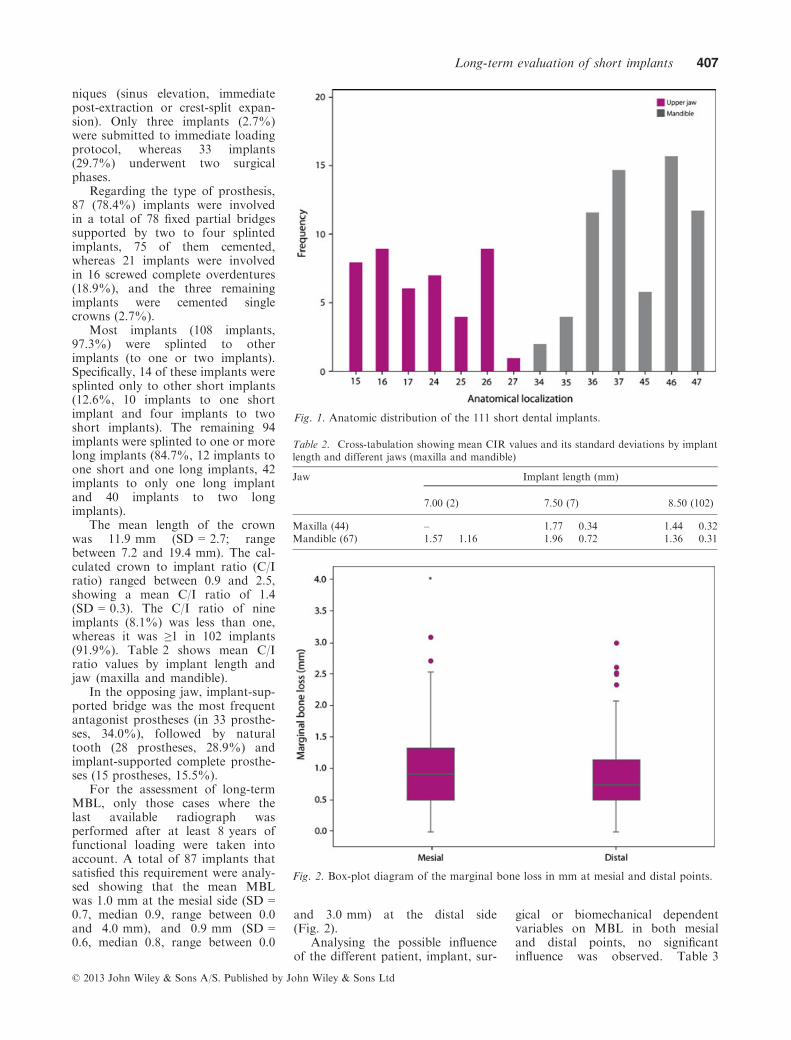
For the assessment of long-termMBL, only those cases where thelast available radiograph wasperformed after at least 8 years offunctional loading were taken intoaccount. A total of 87 implants thatsatisfied this requirement were analy-sed showing that the mean MBLwas 1.0 mm at the mesial side (SD =0.7, median 0.9, range between 0.0and 4.0 mm), and 0.9 mm (SD =0.6, median 0.8, range between 0.0
and 3.0 mm) at the distal side(Fig. 2).
Analysing the possible influenceof the different patient, implant, sur-
gical or biomechanical dependentvariables on MBL in both mesialand distal points, no significantinfluence was observed. Table 3
Fig. 1. Anatomic distribution of the 111 short dental implants.
Table 2. Cross-tabulation showing mean CIR values and its standard deviations by implantlength and different jaws (maxilla and mandible)
Jaw Implant length (mm)
7.00 (2) 7.50 (7) 8.50 (102)
Maxilla (44) – 1.77 � 0.34 1.44 � 0.32Mandible (67) 1.57 � 1.16 1.96 � 0.72 1.36 � 0.31
Fig. 2. Box-plot diagram of the marginal bone loss in mm at mesial and distal points.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Long-term evaluation of short implants 407
shows the different mean values ofMBL in both mesial and distalpoints and its statistical significance(p values) for qualitative and quanti-tative variables.
Biological complications (a peri-implantitis) occurred in one implant(0.9%). No mechanical or technicalcomplications were registered.
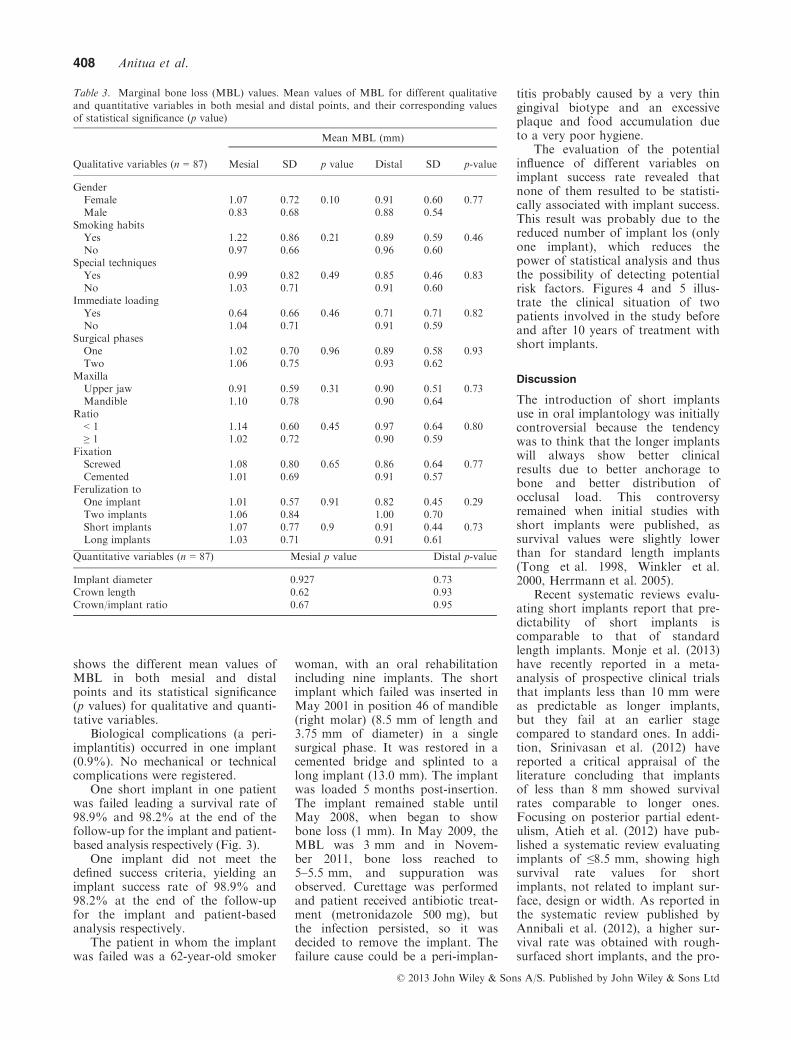
One short implant in one patientwas failed leading a survival rate of98.9% and 98.2% at the end of thefollow-up for the implant and patient-based analysis respectively (Fig. 3).
One implant did not meet thedefined success criteria, yielding animplant success rate of 98.9% and98.2% at the end of the follow-upfor the implant and patient-basedanalysis respectively.
The patient in whom the implantwas failed was a 62-year-old smoker
woman, with an oral rehabilitationincluding nine implants. The shortimplant which failed was inserted inMay 2001 in position 46 of mandible(right molar) (8.5 mm of length and3.75 mm of diameter) in a singlesurgical phase. It was restored in acemented bridge and splinted to along implant (13.0 mm). The implantwas loaded 5 months post-insertion.The implant remained stable untilMay 2008, when began to showbone loss (1 mm). In May 2009, theMBL was 3 mm and in Novem-ber 2011, bone loss reached to5–5.5 mm, and suppuration wasobserved. Curettage was performedand patient received antibiotic treat-ment (metronidazole 500 mg), butthe infection persisted, so it wasdecided to remove the implant. Thefailure cause could be a peri-implan-
titis probably caused by a very thingingival biotype and an excessiveplaque and food accumulation dueto a very poor hygiene.
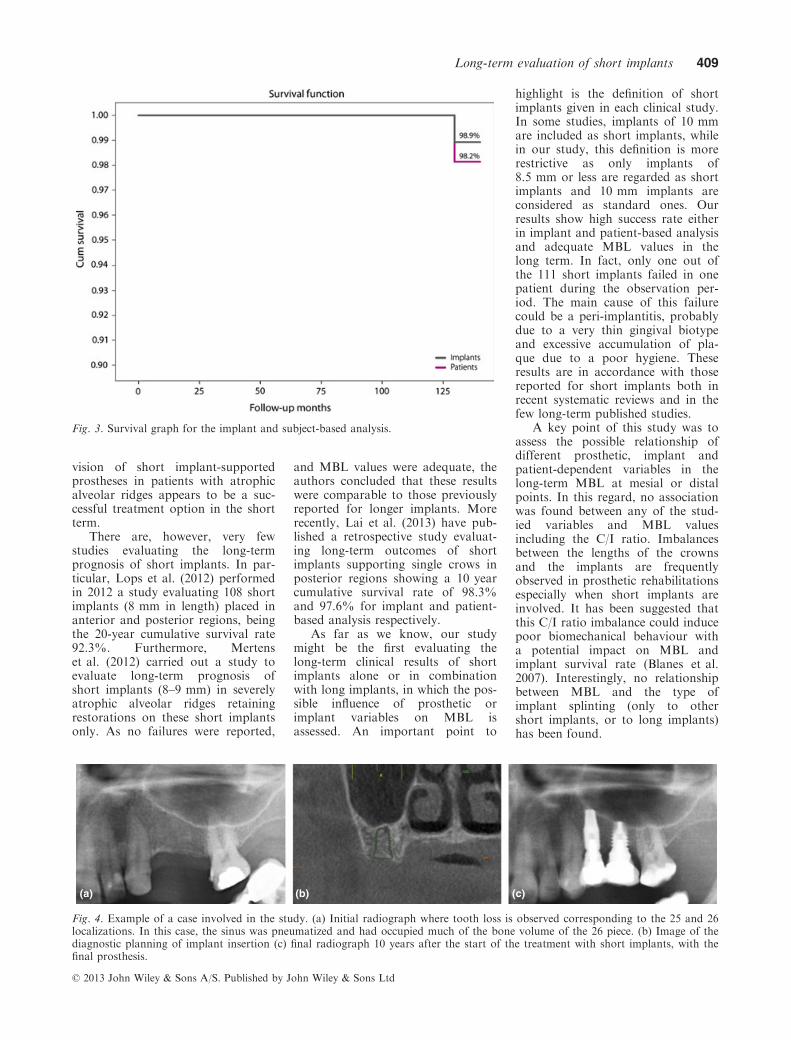
The evaluation of the potentialinfluence of different variables onimplant success rate revealed thatnone of them resulted to be statisti-cally associated with implant success.This result was probably due to thereduced number of implant los (onlyone implant), which reduces thepower of statistical analysis and thusthe possibility of detecting potentialrisk factors. Figures 4 and 5 illus-trate the clinical situation of twopatients involved in the study beforeand after 10 years of treatment withshort implants.
Discussion
The introduction of short implantsuse in oral implantology was initiallycontroversial because the tendencywas to think that the longer implantswill always show better clinicalresults due to better anchorage tobone and better distribution ofocclusal load. This controversyremained when initial studies withshort implants were published, assurvival values were slightly lowerthan for standard length implants(Tong et al. 1998, Winkler et al.2000, Herrmann et al. 2005).
Recent systematic reviews evalu-ating short implants report that pre-dictability of short implants iscomparable to that of standardlength implants. Monje et al. (2013)have recently reported in a meta-analysis of prospective clinical trialsthat implants less than 10 mm wereas predictable as longer implants,but they fail at an earlier stagecompared to standard ones. In addi-tion, Srinivasan et al. (2012) havereported a critical appraisal of theliterature concluding that implantsof less than 8 mm showed survivalrates comparable to longer ones.Focusing on posterior partial edent-ulism, Atieh et al. (2012) have pub-lished a systematic review evaluatingimplants of ≤8.5 mm, showing highsurvival rate values for shortimplants, not related to implant sur-face, design or width. As reported inthe systematic review published byAnnibali et al. (2012), a higher sur-vival rate was obtained with rough-surfaced short implants, and the pro-
Table 3. Marginal bone loss (MBL) values. Mean values of MBL for different qualitativeand quantitative variables in both mesial and distal points, and their corresponding valuesof statistical significance (p value)
Mean MBL (mm)
Qualitative variables (n = 87) Mesial SD p value Distal SD p-value
GenderFemale 1.07 0.72 0.10 0.91 0.60 0.77Male 0.83 0.68 0.88 0.54
Smoking habitsYes 1.22 0.86 0.21 0.89 0.59 0.46No 0.97 0.66 0.96 0.60
Special techniquesYes 0.99 0.82 0.49 0.85 0.46 0.83No 1.03 0.71 0.91 0.60
Immediate loadingYes 0.64 0.66 0.46 0.71 0.71 0.82No 1.04 0.71 0.91 0.59
Surgical phasesOne 1.02 0.70 0.96 0.89 0.58 0.93Two 1.06 0.75 0.93 0.62
MaxillaUpper jaw 0.91 0.59 0.31 0.90 0.51 0.73Mandible 1.10 0.78 0.90 0.64
Ratio< 1 1.14 0.60 0.45 0.97 0.64 0.80≥ 1 1.02 0.72 0.90 0.59
FixationScrewed 1.08 0.80 0.65 0.86 0.64 0.77Cemented 1.01 0.69 0.91 0.57
Ferulization toOne implant 1.01 0.57 0.91 0.82 0.45 0.29Two implants 1.06 0.84 1.00 0.70Short implants 1.07 0.77 0.9 0.91 0.44 0.73Long implants 1.03 0.71 0.91 0.61
Quantitative variables (n = 87) Mesial p value Distal p-value
Implant diameter 0.927 0.73Crown length 0.62 0.93Crown/implant ratio 0.67 0.95
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
408 Anitua et al.
vision of short implant-supportedprostheses in patients with atrophicalveolar ridges appears to be a suc-cessful treatment option in the shortterm.
There are, however, very fewstudies evaluating the long-termprognosis of short implants. In par-ticular, Lops et al. (2012) performedin 2012 a study evaluating 108 shortimplants (8 mm in length) placed inanterior and posterior regions, beingthe 20-year cumulative survival rate92.3%. Furthermore, Mertenset al. (2012) carried out a study toevaluate long-term prognosis ofshort implants (8–9 mm) in severelyatrophic alveolar ridges retainingrestorations on these short implantsonly. As no failures were reported,
and MBL values were adequate, theauthors concluded that these resultswere comparable to those previouslyreported for longer implants. Morerecently, Lai et al. (2013) have pub-lished a retrospective study evaluat-ing long-term outcomes of shortimplants supporting single crows inposterior regions showing a 10 yearcumulative survival rate of 98.3%and 97.6% for implant and patient-based analysis respectively.
As far as we know, our studymight be the first evaluating thelong-term clinical results of shortimplants alone or in combinationwith long implants, in which the pos-sible influence of prosthetic orimplant variables on MBL isassessed. An important point to
highlight is the definition of shortimplants given in each clinical study.In some studies, implants of 10 mmare included as short implants, whilein our study, this definition is morerestrictive as only implants of8.5 mm or less are regarded as shortimplants and 10 mm implants areconsidered as standard ones. Ourresults show high success rate eitherin implant and patient-based analysisand adequate MBL values in thelong term. In fact, only one out ofthe 111 short implants failed in onepatient during the observation per-iod. The main cause of this failurecould be a peri-implantitis, probablydue to a very thin gingival biotypeand excessive accumulation of pla-que due to a poor hygiene. Theseresults are in accordance with thosereported for short implants both inrecent systematic reviews and in thefew long-term published studies.
A key point of this study was toassess the possible relationship ofdifferent prosthetic, implant andpatient-dependent variables in thelong-term MBL at mesial or distalpoints. In this regard, no associationwas found between any of the stud-ied variables and MBL valuesincluding the C/I ratio. Imbalancesbetween the lengths of the crownsand the implants are frequentlyobserved in prosthetic rehabilitationsespecially when short implants areinvolved. It has been suggested thatthis C/I ratio imbalance could inducepoor biomechanical behaviour witha potential impact on MBL andimplant survival rate (Blanes et al.2007). Interestingly, no relationshipbetween MBL and the type ofimplant splinting (only to othershort implants, or to long implants)has been found.
Fig. 3. Survival graph for the implant and subject-based analysis.
(a) (b) (c)
Fig. 4. Example of a case involved in the study. (a) Initial radiograph where tooth loss is observed corresponding to the 25 and 26localizations. In this case, the sinus was pneumatized and had occupied much of the bone volume of the 26 piece. (b) Image of thediagnostic planning of implant insertion (c) final radiograph 10 years after the start of the treatment with short implants, with thefinal prosthesis.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Long-term evaluation of short implants 409

Data showed herein may bepartially explained due to thebiomechanical configuration of theshort implants and also due the cor-rect choice of implant diameter. Afterthe detailed diagnostic study of thecases, and the assessment of thepatients’ baseline situation, choosingthe most appropriate treatment plan isthe key for the final success of theimplant treatment. On the other hand,correct selection of the implant surfaceand deep analysis of the biomechani-cal properties of the implant-supported prosthesis also result essen-tial. Last but not least, it is importantto mention that the vast majority ofthe short implants were splinted tolonger ones.
As it has been reported, the effectof implant diameter on stress distri-bution in bone is more significant
than the effect of the implant’slength or its geometry. In addition,the maximum stress is locatedaround the neck of the implant andthe majority of the stress is distrib-uted in the bone adjacent to initialimplant threads (Isidor 2006).
In general and especially in pos-terior areas, the advantages thatshort implants can offer are clear.When additional bone augmentationsurgery procedures are necessary,there is a risk of involving the infe-rior alveolar nerve or penetrating themaxillary sinus during implant place-ment when alveolar bone is deficient.Furthermore, the posterior maxillaepresents additional challenges forimplant placement including difficultand challenging access, limited visi-bility, reduced space and poor bonequality.
When interpreting the results fromthe present study, some limitationsshould be considered. One importantissue is that results come from a ret-rospective study. This type of studyhas less validity than randomizedprospective clinical trials, due toissues of selection bias and confound-ing factors. Furthermore, it alsoshould be taken into considerationthat most of the short implants stud-ied were splinted to long implantsand the number of short implantsstanding alone or splinted to othershort implants was reduced. More-over, although the Authors believethat the standardized method ofMBL calibrated measurement onpanoramic radiographs is reliable, itis true that intra-oral periapicalradiographs is still the most advisablemethod to minimize measurementerrors. Finally, one should also takeinto consideration that a lack of arelationship between studied vari-ables on MBL could be due to a lackof statistical power in the study.
Conclusions
This study reports the long-termclinical evaluation of short dentalimplants humidified with PRGFwith 10–12 years of follow-up. Mostof the short implants were splintedto longer ones. High cumulative suc-cess rates of 98.9% and 98.2% wereobtained for the implant andpatient-based analysis, respectively,at the end of follow-up. Mean MBLvalues were very small for the long-term assessment. Prosthetic andimplant variables did not affectimplant success rate nor MBL.
References
Anitua, E. (2010) The use of short and extrashortBTI implants in the daily clinical practice. TheJournal of Implant and Advanced Clinical Den-tistry 2, 19–29.
Anitua, E., Carda, C. & Andia, I. (2007b) Anovel drilling procedure and subsequent boneautograft preparation: a technical note. Interna-tional Journal of Oral and MaxillofacialImplants 22, 138–145.
Anitua, E., Sanchez, M., Orive, G. & Andia, I.(2007a) The potential impact of the preparationrich in growth factors (PRGF) in differentmedical fields. Biomaterials 28, 4551–4560.
Anitua, E., Tapia, R., Luzuriaga, F. & Orive,G. (2010) Influence of implant length, diame-ter, and geometry on stress distribution: afinite element analysis. The International Jour-nal of Periodontics & Restorative Dentistry 30,89–95.
(a) (b)
(c) (d)
(e) (f)
Fig. 5. Example of a case treated with short implants. (a–b) Image of CT-scan pre-operative planning where the implant is planning to be located just above the dentalnerve and radiograph showing existing vertical bone atrophy in the molar region. (c)Intra-oral photography of the surgery. The implant is placed supracrestally in vestibu-lar location (1 mm). (d) Placement of particulate bone graft consisting of a mixture ofbone from drilling + plasma rich in growth factors (PRGF) on the area being treated.(e) Coverage with a fibrin membrane obtained from the PRGF-Endoret and posteriorsuture with a non-absorbable monofilament 5/0. (f) Panoramic radiograph of thedefinitive prosthesis at 10 years of implant placement.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
410 Anitua et al.

Annibali, S., Cristalli, M. P., Dell’Aquila, D., Big-nozzi, I., La Monaca, G. & Pilloni, A. (2012)Short dental implants: a systematic review.Journal of Dental Research 91, 25–32.
Atieh, M. A., Zadeh, H., Stanford, C. M. & Coo-per, L. F. (2012) Survival of short dentalimplants for treatment of posterior partial e-dentulism: a systematic review. InternationalJournal of Oral and Maxillofacial Implants 27,1323–1331.
Blanes, R. J., Bernard, J. P., Blanes, Z. M. & Bel-ser, U. C. (2007) A 10-year prospective studyof ITI dental implants placed in the posteriorregion. II: influence of the crown-to-implantratio and different prosthetic treatment modali-ties on crestal bone loss. Clinical Oral ImplantsResearch 18, 707–714.
von Elm, E., Altman, D. G., Egger, M., Pocock,S. J., Gotzsche, P. C. & Vandenbroucke, J. P.(2007) The Strengthening the Reporting ofObservational Studies in Epidemiology(STROBE) statement: guidelines for reportingobservational studies. Lancet 370, 1453–1457.
Esposito, M., Grusovin, M. G., Felice, P., Ka-ratzopoulos, G., Worthington, H. V. & Coult-hard, P. (2009) Interventions for replacingmissing teeth: horizontal and vertical boneaugmentation techniques for dental implanttreatment. Cochrane Database SystematicReview, CD003607.
Esposito, M., Grusovin, M. G., Rees, J., Karaso-ulos, D., Felice, P., Alissa, R., Worthington,H. V. & Coulthard, P. (2010) Interventions forreplacing missing teeth: augmentation proce-dures of the maxillary sinus. Cochrane Data-base Systematic Review, CD008397.
Esposito, M., Pellegrino, G., Pistilli, R. & Felice,P. (2011) Rehabilitation of postrior atrophicedentulous jaws: prostheses supported by 5 mmshort implants or by longer implants in aug-mented bone? One-year results from a pilotrandomised clinical trial. European Journal ofOral Implantology 4, 21–30.
Felice, P., Pellegrino, G., Checchi, L., Pistilli, R. &Esposito, M. (2010) Vertical augmentation withinterpositional blocks of anorganic bovine bonevs. 7-mm-long implants in posterior mandibles:1-year results of a randomized clinical trial.Clinical Oral Implants Research 21, 1394–1403.
Herrmann, I., Lekholm, U., Holm, S. & Kultje,C. (2005) Evaluation of patient and implantcharacteristics as potential prognostic factorsfor oral implant failures. International Journalof Oral and Maxillofacial Implants 20, 220–230.
Isidor, F. (2006) Influence of forces on peri-implantbone. Clinical Oral Implants Research 17(Suppl.2), 8–18.
Karthikeyan, I., Desai, S. R. & Singh, R. (2012)Short implants: a systematic review. Journal ofIndian Society of Periodontology 16, 302–312.
Kotsovilis, S., Fourmousis, I., Karoussis, I. K. &Bamia, C. (2009) A systematic review andmeta-analysis on the effect of implant length onthe survival of rough-surface dental implants.Journal of Periodontology 80, 1700–1718.
Lai, H. C., Si, M. S., Zhuang, L. F., Shen, H.,Liu, Y. L. & Wismeijer, D. (2013) Long-termoutcomes of short dental implants supportingsingle crowns in posterior region: a clinical ret-rospective study of 5–10 years. Clinical OralImplants Research 24, 230–237.
Lops, D., Bressan, E., Pisoni, G., Cea, N., Coraz-za, B. & Romeo, E. (2012) Short implants inpartially edentuolous maxillae and mandibles: a10 to 20 years retrospective evaluation. Interna-tional Journal of Dentistry 2012, 351793.
Menchero-Cantalejo, E., Barona-Dorado, C., Can-tero-Alvarez, M., Fernandez-Caliz, F. & Marti-nez-Gonzalez, J. M. (2011) Meta-analysis on thesurvival of short implants. Medicina oral, pato-log�ıa oral y cirug�ıa bucal 16, e546–e551.
Mertens, C., Meyer-Baumer, A., Kappel, H.,Hoffmann, J. & Steveling, H. G. (2012) Use of8-mm and 9-mm implants in atrophic alveolarridges: 10-year results. International Journal ofOral and Maxillofacial Implants 27, 1501–1508.
Monje, A., Chan, H. L., Fu, J. H., Suarez, F.,Galindo-Moreno, P. & Wang, H. L. (2013) Areshort dental implants (<10 mm) effective? Ameta-analysis on prospective clinical trials.Journal of Periodontology 84, 895–904.
Pierrisnard, L., Renouard, F., Renault, P. & Bar-quins, M. (2003) Influence of implant lengthand bicortical anchorage on implant stress dis-tribution. Clinical Implant Dentistry andRelated Research 5, 254–262.
Reich, K. M., Huber, C. D., Lippnig, W. R.,Ulm, C., Watzek, G. & Tangl, S. (2011) Atro-
phy of the residual alveolar ridge followingtooth loss in an historical population. Oral Dis-eases 17, 33–44.
Romeo, E., Bivio, A., Mosca, D., Scanferla, M.,Ghisolfi, M. & Storelli, S. (2010) The use ofshort dental implants in clinical practice: litera-ture review. Minerva Stomatologica 59, 23–31.
Srinivasan, M., Vazquez, L., Rieder, P., Mora-guez, O., Bernard, J. P. & Belser, U. C. (2012)Efficacy and predictability of short dentalimplants (<8 mm): a critical appraisal of therecent literature. International Journal of Oraland Maxillofacial Implants 27, 1429–1437.
Sun, H. L., Huang, C., Wu, Y. R. & Shi, B.(2011) Failure rates of short (≤ 10 mm) dentalimplants and factors influencing their failure: asystematic review. International Journal of Oraland Maxillofacial Implants 26, 816–825.
Telleman, G., Raghoebar, G. M., Vissink, A., denHartog, L., Huddleston Slater, J. J. & Meijer,H. J. (2011) A systematic review of the progno-sis of short (<10 mm) dental implants placed inthe partially edentulous patient. Journal ofClinical Periodontology 38, 667–676.
Tonetti, M. S. & Hammerle, C. H. (2008)Advances in bone augmentation to enable den-tal implant placement: Consensus Report ofthe Sixth European Workshop on Periodontol-ogy. Journal of Clinical Periodontology 35, 168–172.
Tong, D. C., Rioux, K., Drangsholt, M. & Bei-rne, O. R. (1998) A review of survival rates forimplants placed in grafted maxillary sinusesusing meta-analysis. International Journal ofOral and Maxillofacial Implants 13, 175–182.
Winkler, S., Morris, H. F. & Ochi, S. (2000)Implant survival to 36 months as related tolength and diameter. Annals of Periodontology/the American Academy of Periodontology 5, 22–31.
Address:Eduardo AnituaInstituto Eduardo Anituac/ Jose Maria Cagigal 19, 01005 VitoriaSpainE-mail: [email protected]
Clinical Relevance
Scientific rationale for the study:There are few published studiesevaluating short implants in thelong term.Principal findings: Results are sofar comparable to those reportedfor longer implants.
Practical implications: the use ofshort implants self-standing orsplinted to longer implants shouldbe considered as an effective andsafe long-term treatment option inpatients with partial or – totallyedentulous jaws whenever the place-ment of longer implants may require
additional and more invasive boneaugmentation procedures.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Long-term evaluation of short implants 411





























