Embed Size (px)
Citation preview

Wvmccatb
M
TbCaPwitmcb
vN2
0d
Long-Term Outcomes After Percutaneous Coronary Intervention ofBifurcation Narrowings
Nicholas Collins, MD, Peter H. Seidelin, MB, Paul Daly, MD, Joan Ivanov, PhD,Alan Barolet, MD, PhD, Karen Mackie, RN, Sanh Bui, BSc,
Leonard Schwartz, MD, and Vladimír Džavík, MD*
The optimal approach to percutaneous coronary intervention (PCI) of bifurcation lesionsremains unclear, reflecting lack of long-term follow-up and heterogeneity of lesions en-countered. We evaluated the long-term outcome of patients undergoing bifurcation PCIfollowed in the prospective bifurcation registry at the University Health Network, Toronto,Ontario, Canada. Of 526 patients undergoing bifurcation PCI between November 2003 andMarch 2005, most (n � 406) were treated by main vessel stenting only (n � 266) orcrush/culotte stenting (n � 140). After median follow-up of 26.5 months, major adversecardiac events (MACEs) and Canadian Cardiovascular Society class >2 angina occurredin 28.5% and 22.3% of patients in these groups, respectively (p � 0.190), whereas MACErates were 20.8% for main vessel stenting and 18.7% for crush/culotte stenting (p � 0.670).A low bifurcation angle was associated with better outcomes in the crush/culotte group buthad no effect on outcome of patients treated with main vessel stenting only. Use ofcrush/culotte techniques independently predicted freedom from MACEs or CanadianCardiovascular Society class >2 angina compared with main vessel stenting only (oddsratio 0.55, 95% confidence interval 0.32 to 0.94, p � 0.029). In conclusion, the use ofcrush/culotte stenting is safe, with efficacy and MACE rates being similar to main vesselstenting alone. Our observations regarding the effect of lesion characteristics such asbifurcation angle and extent of side branch disease on outcome underscore the need forrandomized trials that are inclusive of patients with complex side branch disease. © 2008
Elsevier Inc. All rights reserved. (Am J Cardiol 2008;102:404–410)mapstwpagoad
cpidkcnnthofti
e compared characteristics of patients undergoing mainessel stenting only and crush or culotte stenting, com-only used bifurcation stenting techniques, to determine if
ertain patient or lesion characteristics were associated withhoice of technique and subsequent long-term outcome. Welso compared long-term clinical outcomes associated withhese techniques to treat the main vessel and side branch inifurcation percutaneous coronary intervention (PCI).
ethods
he study protocol was approved by the research ethicsoard of the University Health Network, Toronto, Ontario,anada. All patients identified as having undergone PCI ofbifurcation lesion in the prospective PCI Registry,1,2 at theeter Munk Cardiac Centre, University Health Network,ere selected for screening. Procedural angiographic stud-
es of all screened patients were then reviewed to identifyhose who had a target bifurcation with a side branch �2m in diameter by visual assessment. Bifurcations were
lassified according to the Medina classification, a simpleinary system, in which the proximal main vessel, distal
Interventional Cardiology Program, Peter Munk Cardiac Centre, Uni-ersity Health Network, Toronto, Ontario, Canada. Manuscript receivedovember 9, 2007; revised manuscript received and accepted March 20,008.
*Corresponding author: Tel: 416-340-4800, ext. 6265; fax: 416-340-3390.
uE-mail address: [email protected] (V. Džavík).002-9149/08/$ – see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2008.03.075
ain vessel, and side branch components of the bifurcationre, in that order, each assigned 1 or 0 depending on theresence or absence of �50% stenosis.3,4 Thus a vessel withignificant lesions in the proximal main vessel and ostium ofhe side branch but with an unaffected distal main vesselould be classified 1,0,1. For this analysis, we combinedatients with 1,1,1 and 0,1,1 bifurcation classifications intosingle “true bifurcation” group because in the 2 groups a
reater likelihood of the need to treat the distal continuationf the main vessel and the origin of the side branch could benticipated. Clinical, procedural, and in-hospital outcomeata were extracted from the registry.
All patients were treated with dual antiplatelet therapyonsisting of aspirin and clopidogrel at time of PCI; ticlo-idine was substituted for clopidogrel in cases of patientntolerance. Glycoprotein IIb/IIIa inhibitors were used at theiscretion of the treating interventional cardiologist. Finalissing balloon inflation was performed routinely in cases ofrush stenting after July 2004 because previously we wereot mandating this based on an initial report of the tech-ique by Colombo et al.5 We previously reported that pa-ients undergoing crush stenting especially in the case ofigh-angle bifurcations had significantly worse long-termutcome if a final kissing balloon inflation was not per-ormed.6 Patients undergoing left main coronary arteryreatment and treatment in the setting of acute myocardialnfarction were not excluded from analysis. Intravascular
ltrasound was not used routinely. Based on the techniquewww.AJConline.org
urwcluobotccsm2en
gofcihmawipbopc
TB
V
AWDHDSKPPCEAE
EM
S
B
5 (1.2
405Coronary Artery Disease/Outcome After Bifurcation Percutaneous Coronary Intervention
sed to treat the bifurcation lesion, patients were catego-ized as undergoing main vessel stenting alone, with orithout balloon angioplasty of the side branch, or crush and
ulotte techniques, with the similarity of multiple stentayers resulting from the procedure, the most commonlysed complex stenting techniques used during this period inur program. Most crush cases were performed using thealloon crush technique.7 Patients undergoing PCI usingther techniques, including T-stenting (n � 40) and simul-aneous kissing stenting or V-stenting (n � 18), were ex-luded due to the small numbers treated, rendering statisti-al comparisons difficult. In addition, those undergoingtenting of the proximal main vessel only (n � 4), distalain vessel only (n � 14), or side branch ostium only (n �
7) were excluded because these patients were not consid-red to have true bifurcation lesions and generally would
able 1aseline characteristics of bifurcation percutaneous coronary intervention
ariable
ge 6omeniabetesypertension 2yslipidemia 3moking history 2nown family history of coronary artery disease 1revious PCIrevious coronary artery bypass surgeryreatinine (mg/dl) 1stimated creatinine clearancecute myocardial infarction (primary, facilitated, rescue, shock)xtent of coronary artery disease1 vessel 12 vessels 13 vesselsLeft mainstimated left ventricular ejection fraction �40%ain bifurcation coronary artery
Left mainLeft anterior descending 2CircumflexObtuse marginalRight coronary arterySaphenous vein graftide branchDiagonal 2Left anterior descendingSeptalObtuse marginalCircumflexPosterior descendingPosterolateralRight ventricularifurcation type1,1,1 21,1,01,0,00,1,10,1,00,0,1
ot be considered for a multistent approach. Patients under- a
oing balloon angioplasty (n � 10), brachytherapy (n � 2),r Frontier stent deployment (n � 2) were also excludedrom further analysis. Study groups were also divided ac-ording to bifurcation angle, which has found to have anmpact on long-term outcome after crush stenting6 intoigh-angle (�50°) and low-angle (�50°) groups, approxi-ating the median cutpoint of the study population; low-
ngle bifurcations can be considered to have a Y shape,hereas high-angle bifurcations are more likely to approx-
mate a T shape. Procedural success was defined as finalercent diameter stenosis �30 in the main vessel as definedy the operator at the end of the PCI procedure in the absencef in-hospital major adverse cardiac events (MACEs). Post-rocedural myocardial infarction was defined as an increase inreatine kinase �2 times the upper limit of normal.
All procedural cineangiograms were acquired digitally
of main vessel stenting only and crush/culotte stenting
ents Main Vessel Stent Crush/Culotte p Value06) (n � 266) (n � 134/6)
11.8 62.7 � 11.7 63.4 � 11.8 0.533.6%) 64 (24.1%) 32 (22.9%) 0.807.2%) 62 (23.3%) 28 (20.0%) 0.530.1%) 151 (56.8%) 89 (63.6%) 0.203.9%) 203 (76.0%) 110 (78.6%) 0.621.1% 154 (57.9%) 78 (55.7%) 0.673.4) 114 (42.9%) 46 (32.9%) 0.146.0%) 50 (18.8%) 27 (19.3%) 0.895%) 18 (6.8%) 14 (10.0%) 0.2520.95 1.08 � 0.79 1.21 � 1.20 0.18736 89 � 35 85 � 37 0.224%) 14 (5.3%) 4 (2.9%) 0.319
.9%) 108 (40.6%) 62 (44.3%)
.5%) 101 (38.0%) 43 (30.7%) 0.534
.0%) 43 (16.2%) 26 (18.6%)%) 14 (5.3%) 9 (6.4%).3%) 33 (14.3%) 17 (14.3%) 1.00
%) 15 (5.6%) 8 (5.7%).6%) 144 (54.1%) 94 (67.1%).7%) 50 (18.8%) 30 (21.4%) 0.004%) 8 (3.0%) 1 (0.7%).6%) 48 (18.0%) 7 (5.0%)%) 1 (0.4%) 0
.1%) 130 (49.4%) 92 (65.7%)%) 4 (1.5%) 7 (5.0%)%) 8 (3.0%) 0.8%) 34 (12.8%) 26 (18.6%) �0.0001.4%) 37 (14.0%) 5 (3.6%)%) 11 (4.1%) 4 (2.9%)%) 22 (8.3%) 3 (2.1%)%) 17 (6.4%) 0
.9%) 132 (50.6%) 111 (80.4%)%) 25 (9.6%) 3 (2.2%)%) 36 (13.8%) 2 (1.4%) �0.0001%) 15 (5.8%) 18 (13.0%).0%) 50 (19.2%) 2 (1.4%)%) 3 (1.2%) 2 (1.4%)
groups
All Pati(n � 4
2.9 �96 (2390 (2240 (5912 (7632 (5760 (3977 (1932 (7.9.13 �88 �18 (4.4
70 (4144 (3569 (1723 (5.750 (14
23 (5.738 (5880 (199 (2.2
55 (131 (0.2
23 (5511 (2.78 (1.5
60 (1442 (1015 (3.725 (6.217 (4.2
43 (6028 (7.038 (9.533 (8.352 (13
nd stored in Digital Imaging and Communication in Med-
iplldw
aiscactvgpdab
ScovsStccMcl
bmfla
TP
V
BM
S
TP
V
N
V
DGFTFTP 2
406 The American Journal of Cardiology (www.AJConline.org)
cine format. Quantitative coronary angiographic analysis,erformed using the Medis system (Leiden, The Nether-ands), was used to assess the main vessel and side branchesion length and the reference vessel and minimum lumeniameter before and after the procedure. Bifurcation angleas measured as previously described.6
Patients were contacted by mailed questionnaire on annnual basis during follow-up, with subsequent telephonenterviews as required. Medical records and angiographictudies were reviewed where appropriate. Follow-up dataollected included Canadian Cardiovascular Society (CCS)ngina class, myocardial infarction and cerebrovascular ac-ident, duration of dual antiplatelet therapy with aspirin andhienopyridine, repeat cardiac catheterization, repeat targetessel revascularization by PCI, coronary artery bypassrafting, and death. Routine angiographic follow-up was noterformed. Stent thrombosis was defined according Aca-emic Research Consortium criteria,8 and its presence orbsence was categorized as (1) none, (2) definite or proba-
able 2re- and postprocedural quantitative coronary angiographic analyses
ariable All Patients(n � 406)
ifurcation angle 52.1 � 16.9ain vessel
Reference diameter before 3.24 � 0.41Lesion length (mm) 15.84 � 7.75Minimal luminal diameter before 0.70 � 0.37Percent stenosis before 78.3 � 10.6Minimal luminal diameter after 2.98 � 0.40Percent stenosis after 7.83 � 5.20ide branchReference diameter before 2.76 � 0.40Lesion length (mm) 9.15 � 4.77Minimal luminal diameter before 1.21 � 0.74Percent stenosis before 56.22 � 24.99Minimal luminal diameter after 1.99 � 0.72Percent stenosis after 29.2 � 21.1
able 3rocedural variables and outcomes
ariable All Patients(n � 526)
o. of intervened vessels1 283 (69.7%)2 93 (22.9%)3 9 (2.2%)Left main 21 (5.2%)ascular access siteFemoral 326 (80.3%)Radial 78 (19.2%)Brachial 2 (0.5%)ES deployed 254 (62.7%)lycoprotein IIb/IIIa inhibitor 338 (83.2)inal kissing balloon inflation 230 (56.8%)otal procedure time (min) 96.3 � 39.8luoroscopic time (min) 25.5 � 16.0otal contrast volume (ml) 409 � 182rocedural success (%) 390 (96.1%)
le, and (3) possible. d
Statistical analysis was performed using JMP 5.0 andAS 8.2 (SAS Institute, Cary, North Carolina). The primaryomparison variable was the composite end point consistingf MACEs defined as death, myocardial infarction, targetessel revascularization by PCI or coronary artery bypassurgery, or recurrence of anginal symptoms CCS class �2.econdary outcomes included the individual components of
he composite primary end point. Continuous variables wereompared using Student’s t test, with categorical variablesompared using chi-square and Fisher’s exact tests. Kaplan-eier curves were generated to compare long-term out-
omes of study groups, which also were stratified by high orow bifurcation angle.
To assess the possibility of an independent associationetween bifurcation technique and occurrence of the pri-ary composite end point in the 2 study groups, we per-
ormed Cox multivariable analysis using all important base-ine and procedural variables. For the purposes of thisnalysis, interquartile ranges (25%, 50%, 75%) were used to
Main Vessel Stent Crush/Culotte p Value(n � 266) (n � 134/6)
52.5 � 17.6 51.3 � 15.5 0.485
3.21 � 0.42 3.29 � 0.38 0.08215.70 � 7.85 16.12 � 7.56 0.600
0.67 � 0.37 0.77 � 0.36 0.01679.1 � 10.7 76.7 � 10.3 0.0382.95 � 0.41 3.05 � 0.38 0.0198.31 � 4.42 6.93 � 6.34 0.011
2.67 � 0.41 2.91 � 0.31 �0.00017.91 � 3.95 11.47 � 5.30 �0.00011.46 � 0.76 0.75 � 0.40 �0.000146.6 � 24.5 74.3 � 13.0 �0.00011.63 � 0.59 2.69 � 0.32 �0.000140.5 � 17.3 7.6 � 4.0 �0.0001
in Vessel Stent Crush/Culotte p Value(n � 266) (n � 134/6)
81 (68.0%) 102 (72.9%)68 (25.6%) 25 (17.9%)5 (1.9%) 4 (2.9%) 0.292
12 (4.5%) 9 (6.4%)
00 (75.2%) 126 (90.0%)65 (24.4%) 13 (9.3%) 0.0011 (0.4%) 1 (0.7%)
30 (48.9%) 124 (89.2%) �0.000108 (78.2%) 130 (92.9%) 0.000124 (47.0%) 105 (75.0%) �0.000187 � 37 114 � 39 �0.00012.9 � 15.2 30.7 � 16.4 �0.0001374 � 173 474 � 182 �0.000156 (96.2%) 134 (95.7%) 0.793
Ma
1
2
121
2
efine quartiles of the main vessel baseline reference diam-
e(dlity
tcc(mimtdsbv(elawpww
R
O2
bwsgdvatumg
Fs
TI
V
I
F
%)
407Coronary Artery Disease/Outcome After Bifurcation Percutaneous Coronary Intervention
ter (2.96, 3.22, and 3.48 mm), main vessel lesion length10.1, 14.63, and 20.0 mm), side branch baseline referenceiameter (2.51, 2.76, and 3.0 mm), and side branch lesionength (5.52, 8.33, and 11.73 mm). Age was categorizednto decades �49 years (age/decade 0 � �50 years, 1 � 50o 59 years, 2 � 60 to 69 years, 3 � 70 to 79 years, 4 � �80ears).
The following variables were selected for submission tohe Cox model: age/decade, gender, diabetes, creatininelearance, left ventricular function, previous PCI, previousoronary artery bypass grafting surgery, multivessel diseasemajor epicardial vessel �70% diameter stenosis or leftain artery �50% diameter stenosis), acute myocardial
nfarction indication for PCI, multivessel PCI, PCI of leftain or left anterior descending coronary arteries, bifurca-
ion angle �50°, quartiles of main vessel baseline referenceiameter, quartiles of main vessel lesion length, quartiles ofide branch baseline reference diameter, quartiles of sideranch lesion length, crush/culotte technique versus mainessel stenting only, deployment of a drug-eluting stentDES) in the bifurcation, and true bifurcation as definedarlier. A second model was tested, eliminating the 6 cu-otte-treated patients to compare the crush technique alonegainst the main vessel stent only technique. A third modelas used to determine independent predictors of the com-osite outcome variable in those patients whose bifurcationsere treated exclusively with DESs. An alpha value of 0.1as defined for retention of a variable in the Cox model.
esults
f the 2,879 PCI procedures performed between November
able 4n-hospital complications and long-term events
ariable All Pa(n �
n hospitalAbrupt closure 2 (0.5Myocardial infarction by enzyme criteria 11 (2.7Myocardial infarction by electrocardiographic criteria 1 (0.2Side branch occlusion 7 (1.7Urgent coronary artery bypass surgery 1 (0.2Death 2 (0.5MACEs 15 (3.7Acute renal dysfunction 3 (0.7ollow-upMonths, median (interquartile range) 26.4 (22.Completeness of follow-up 400 (98.Months of dual antiplatelet therapy (n � 196, 124) 17.6 �MACEs or CCS class �2 angina 104 (26.MACEs 80 (20.Death 17 (4.3Myocardial infarction 14 (3.6Target vessel PCI or coronary artery bypass surgery 49 (12.
Target vessel PCI 37 (9.5Coronary artery bypass surgery 16 (4.1
CCS class �2 angina 38 (10.Stent thrombosis
Definite or probable 11 (2.7Possible 4 (1.0
003 and March 2005, 526 were in patients with a target l
ifurcation lesion fulfilling study criteria, of which 120ere excluded as described in Methods. There were no
ignificant differences between treatment groups in demo-raphic features, extent and severity of coronary arteryisease, or nature of clinical presentation (Table 1). Mainessel stenting only was used to treat all bifurcation types,bout 1/2 of which were true bifurcations (1,1,1 accordingo Medina classification). Crush/culotte techniques weresed almost exclusively in patients with disease in the distalain vessel and side branch, such that most patients under-
oing crush/culotte stenting had true Medina bifurcation
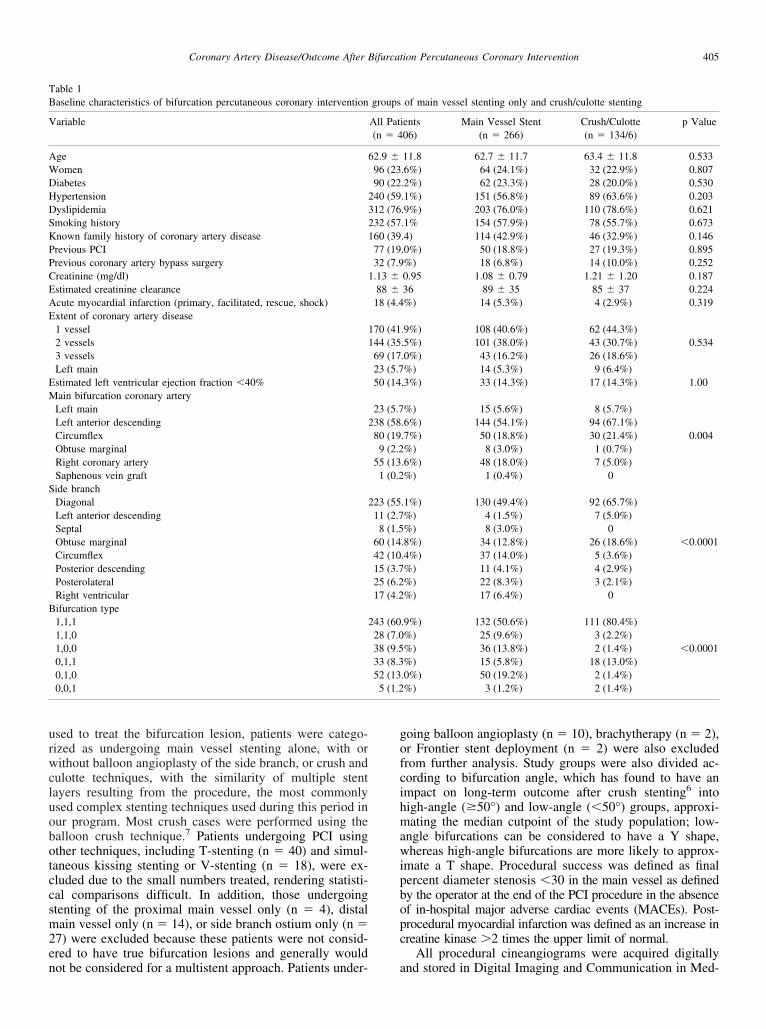
igure 1. Kaplan-Meier curves for MACEs or CCS class �2 angina-freeurvival according to bifurcation technique.
Main Vessel Stent Crush/Culotte p Value(n � 266) (n � 134/6)
1 (0.4%) 1 (0.7%) 0.6447 (2.6%) 4 (2.9%) 1.000
0 1 (0.7%) 0.3445 (1.9%) 2 (1.4%) 1.0001 (0.4) 0 1.0001 (0.4%) 1 (0.7%) 1.0009 (3.4%) 6 (4.3%) 0.7831 (0.4) 2 (1.4) 0.274
26.1 (22.8–30.1) 26.9 (22.9–31.9)261 (98.1%) 139 (99.3%) 0.355
17.4 � 8.8 16.7 � 8.8 0.50673 (28.5%) 31 (22.3%) 0.19054 (20.8%) 26 (18.7%) 0.67011 (4.2%) 6 (4.3%) 1.00010 (4.0%) 4 (3.0%) 0.77832 (12.6%) 17 (12.4%) 1.00026 (10.2%) 11 (8.0%) 0.588
8 (3.2%) 8 (5.8%) 0.28429 (11.7%) 9 (6.8%) 0.113
7 (2.7%) 4 (2.9%) 0.8072 (0.8%) 2 (1.4%)
tients406)
%)%)%)%)%)%)%)%)
7–30.5)5%)
9.13%)1%)%)%)5%)%)%)0%)
%)
esions (1,1,1).
gp
mtlbl
svTtob(w
(mttug
Fsc
Ftu
TCcl
V
C
C
0
408 The American Journal of Cardiology (www.AJConline.org)
Table 2 presents results of quantitative coronary angio-raphic analysis. Patients undergoing main vessel stenting
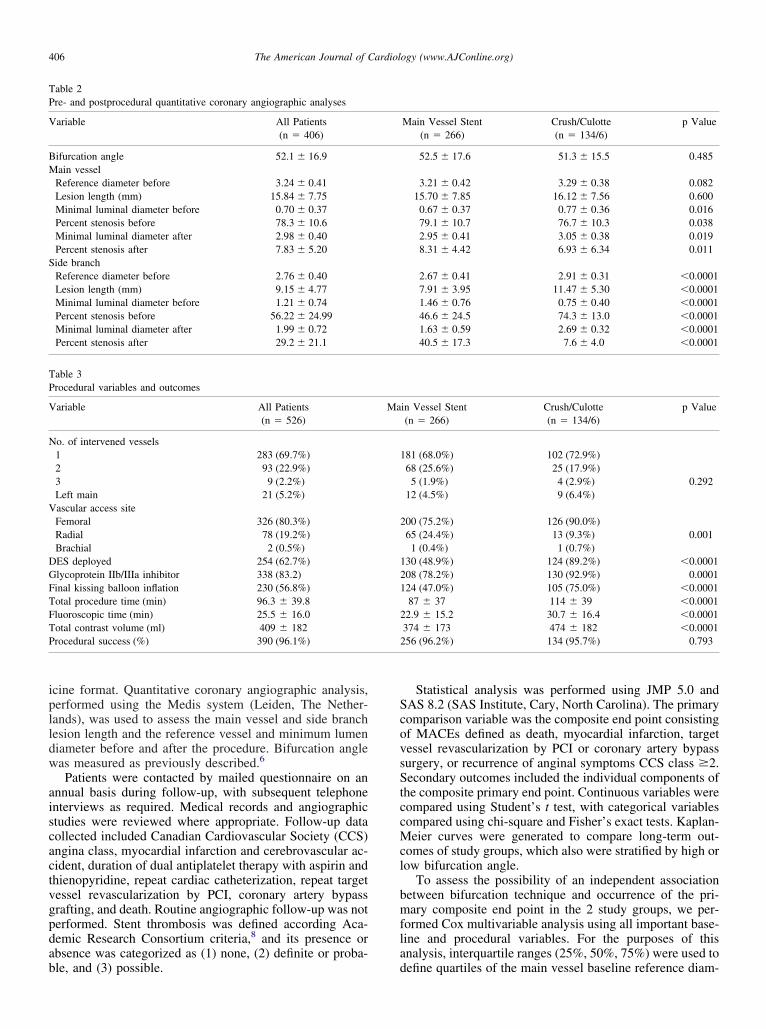
igure 2. Kaplan-Meier curves for MACEs or CCS class �2 angina-freeurvival in (A) patients with main vessel stenting only and (B) those withrush/culotte stenting stratified according to bifurcation angle.
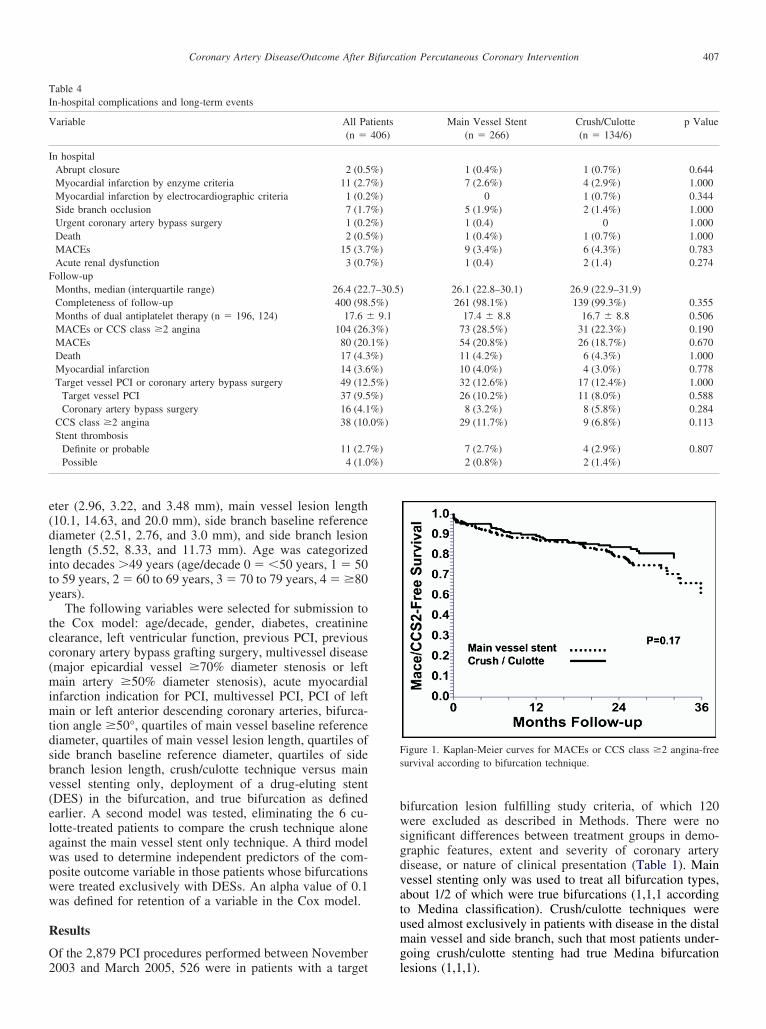
igure 3. Kaplan-Meier curve comparing DES with BMS deployment inhe bifurcation on MACEs or CCS class �2 angina-free survival in patientsndergoing main vessel stenting only.
rocedures and those undergoing crush/culotte stenting had d
ore severe lesions in the main vessel. Crush or culotteechniques were more likely to be used in cases with aarger-diameter side branch and with greater severity of sideranch disease as reflected in percent stenosis and lesionength. Mean bifurcation angle was similar in the 2 groups.
DESs were deployed in most cases of crush or culottetenting strategies, whereas 1/2 of patients treated with mainessel stenting alone received bare metal stents (BMSs;able 3). Procedure duration, fluoroscopic time, and con-
rast volume were significantly decreased in main vesselnly stenting procedures. Angiographic results in the sideranch were superior in the crush/culotte stenting groupTable 2). Procedural success and in-hospital outcomesere similar in the 2 study groups.Median duration of clinical follow-up was 26.5 months
Table 4), with the longest follow-up period being 49.2onths. Duration of dual antiplatelet therapy was similar in
he 2 groups. At follow-up, the primary composite end pointended to occur somewhat less frequently in patientsndergoing crush/culotte procedures than in those under-oing main vessel stenting only (Figure 1). Patients un-
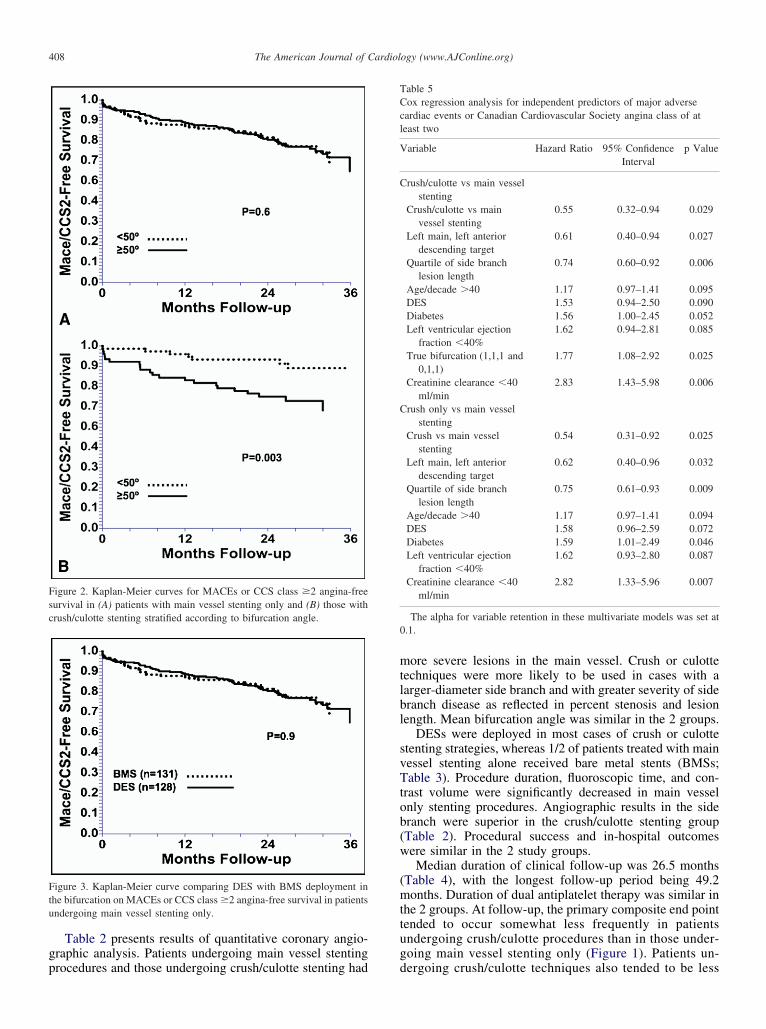
able 5ox regression analysis for independent predictors of major adverseardiac events or Canadian Cardiovascular Society angina class of ateast two
ariable Hazard Ratio 95% ConfidenceInterval
p Value
rush/culotte vs main vesselstenting
Crush/culotte vs mainvessel stenting
0.55 0.32–0.94 0.029
Left main, left anteriordescending target
0.61 0.40–0.94 0.027
Quartile of side branchlesion length
0.74 0.60–0.92 0.006
Age/decade �40 1.17 0.97–1.41 0.095DES 1.53 0.94–2.50 0.090Diabetes 1.56 1.00–2.45 0.052Left ventricular ejection
fraction �40%1.62 0.94–2.81 0.085
True bifurcation (1,1,1 and0,1,1)
1.77 1.08–2.92 0.025
Creatinine clearance �40ml/min
2.83 1.43–5.98 0.006
rush only vs main vesselstenting
Crush vs main vesselstenting
0.54 0.31–0.92 0.025
Left main, left anteriordescending target
0.62 0.40–0.96 0.032
Quartile of side branchlesion length
0.75 0.61–0.93 0.009
Age/decade �40 1.17 0.97–1.41 0.094DES 1.58 0.96–2.59 0.072Diabetes 1.59 1.01–2.49 0.046Left ventricular ejection
fraction �40%1.62 0.93–2.80 0.087
Creatinine clearance �40ml/min
2.82 1.33–5.96 0.007
The alpha for variable retention in these multivariate models was set at.1.
ergoing crush/culotte techniques also tended to be less

llog
fNvattb
2astwv
Dty11(rw
5w6matra(0
D
TPsblmmd
vcrowwaam
otclbtdaevsiafsmpimnl
cortshibdc
rcpphOpbismtpmbt
agtstdafiw
409Coronary Artery Disease/Outcome After Bifurcation Percutaneous Coronary Intervention
ikely to have CCS class �2 angina at long-term fol-ow-up than were those undergoing main vessel stentingnly (Table 4). MACE rates were similar in the 2 mainroups.
The association between bifurcation angle and freedomrom the primary composite end point is shown in Figure 2.o association was observed in patients undergoing mainessel stenting alone. However, a low bifurcation angle wasssociated with a significantly better outcome in patientsreated with crush and culotte techniques compared withhose treated with these techniques that had high-angleifurcations.
Stent thrombosis occurred with similar frequency in thestudy groups (Table 4) and in patients treated with DESs
nd BMSs. Within the crush/culotte group, however, alltent thrombosis events occurred in patients with a bifurca-ion angle �50° (�50°, 8.6%, vs �50°, 0%, p � 0.048),hereas no such association was observed in the mainessel stenting only group (4.3% vs 2.8%, p � 0.787).
Patients with main vessel stenting only were treated withESs and BMSs in approximately equal proportions. Patients
reated with DESs were younger (60.9 � 11.5 vs 64.4 � 11.7ears of age, p � 0.014), more likely to be diabetic (30.0% vs6.9%, p � 0.011), to have had a previous PCI (26.2% vs1.8%, p � 0.003), and had a longer main vessel lesion17.03 � 8.33 vs 14.41 � 7.16 mm, p � 0.007). MACEates were similar in DES-treated patients and those treatedith BMSs (Figure 3).Results of multivariable analysis are presented in Table
. Treatment by crush/culotte techniques was associatedith a significant risk decrease (p � 0.029). Excluding thepatients who underwent culotte stenting from the secondultivariable model had no effect on this result. Multivari-
ble analysis of patients whose bifurcation lesions werereated exclusively with DESs, not presented in Table 5,evealed the crush/culotte strategy to be an independentlyssociated with a lower risk of the composite end pointodds ratio 0.53, 95% confidence interval 0.31 to 0.92, p �.023).
iscussion
his is the first report of long-term outcome of patients afterCI of coronary bifurcation lesions using crush/culottetenting compared with main vessel stenting alone. Com-ined crush/culotte treatment tended to be associated with aower rate of MACEs and CCS class �2 angina than treat-ent with a single main vessel stent. Indeed, multivariableodeling revealed crush/culotte stenting to be indepen-
ently associated with better outcome.Outcome after crush/culotte stenting was particularly fa-
orable in patients with a low bifurcation angle (�50°),onfirming our previous observations.6 The less favorableesults in those with high-angle bifurcations are likely sec-ndary to the presence of adjacent areas of high shear stress,here platelet activation can occur, and low shear stress,here platelets can be deposited, mechanisms that are ex-
ggerated under high-angle bifurcation conditions9 and thatre likely further exacerbated by multiple layers of stent
aterial that may not be optimally deployed.10 rWe cannot necessarily ascribe these findings from anbservational registry setting to a treatment effect. Thereatment groups studied differed in a number of importantharacteristics. The main vessel stent group had shorteresion length in the side branch and a smaller mean sideranch diameter. Furthermore, the main vessel group con-ained a larger proportion of patients without side branchisease, which may also explain the increased use of BMSslone in this subgroup. Although a small side branch diam-ter might be consistent with a smaller and less importantessel subtending less myocardium, it may also be that themall-caliber vessel is more likely to undergo hemodynam-cally significant restenosis after stenting. This may lead togreater likelihood of recurrence of symptoms and the need
or repeat revascularization in patients treated by main ves-el stenting only. Although the crush/culotte technique re-ained an independent predictor of better outcome com-
ared with the main vessel stent only group, it is likelympossible to capture all important factors in a multivariableodel that are used by clinicians to select a stenting tech-
ique and that may well have a bearing on short- andong-term outcomes.
Our data suggest that crush and culotte stenting strategiesan be used to treat bifurcation stenoses with a high degreef safety and long-term efficacy. This is reassuring given theeported association between bifurcation PCI and late stenthrombosis.11 By selecting patients with more extensiveide branch disease for a complex stenting strategy, we mayave provided more appropriate percutaneous revascular-zation to these patients. An individualized approach towardifurcation PCI based on extent of side branch disease andegree of bifurcation angle may potentially optimize out-omes.
An important finding relates to the favorable results withespect to CCS angina class noted in patients undergoingomplex bifurcation stenting procedures. Despite anginaersisting in up to 26% of patients after PCI,12 only 1 of therevious studies comparing bifurcation stenting strategiesad specifically addressed the issue of ongoing symptoms.13
ur finding of decreased angina may reflect the more com-lete revascularization conferred by stenting of the sideranch; inadequate treatment of the side branch may notnfluence MACEs during short term follow-up, but residualide branch disease may contribute to ongoing symptomaticyocardial ischemia. This result may also reflect, in part,
he larger side branch vessel in the groups receiving multi-le stents. The larger-caliber side branches, which may beore likely to contribute to angina, are also more likely to
e suitable for stenting, incorporating the crush or culotteechniques.
Although this is a large, prospective analysis, our datare limited by the nonrandomized nature of the comparisonroups in which all possible confounders cannot be con-rolled for. Although the main vessel only stenting groupuggested that deployment of DESs offers no benefit overhe period of follow-up even after adjustment for baselineifferences, it is quite possible that other differences notccounted for in our database may have contributed to thisnding. An adequately powered randomized study would bearranted to validate these observations. The relatively low
ate of occurrence of stent thrombosis after complex bifur-

crprbp
1
1
1
1
410 The American Journal of Cardiology (www.AJConline.org)
ation lesion stenting in this study, although encouraging,equires the corroboration of follow-up of larger numbers ofatients and a longer follow-up period. This study alsoepresents a single-center experience with the procedureseing performed by experienced high-volume operators,ossibly affecting generalizability of the data.
1. Blackman DJ, Pinto R, Ross JR, Seidelin PH, Ing D, Jackevicius C,Mackie K, Chan C, Dzavik V. Impact of renal insufficiency on out-come after contemporary percutaneous coronary intervention. AmHeart J 2006;151:146–152.
2. Jackevicius CA, Pinto R, Daly P, Mackie K, Dzavik V. Routine use ofglycoprotein IIb/IIIa inhibitor therapy is associated with an improvedin-hospital outcome after percutaneous coronary intervention: Insightsfrom a large, prospective, single-centre registry. Can J Cardiol 2005;21:27–32.
3. Medina A, Suarez de Lezo J, Pan M. [A new classification of coronarybifurcation lesions]. Rev Esp Cardiol 2006;59:183.
4. Louvard Y, Thomas M, Dzavik V, Hildick-Smith D, Galassi AR, PanM, Burzotta F, Zelizko M, Dudek D, Ludman P, et al. Classification ofcoronary artery bifurcation lesions and treatments: time for a consen-sus! Catheter Cardiovasc Interv 2007;71:175–183.
5. Colombo A, Stankovic G, Orlic D, Corvaja N, Liistro F, Airoldi F,Chieffo A, Spanos V, Montorfano M, Di Mario C. Modified T-stentingtechnique with crushing for bifurcation lesions: immediate results and30-day outcome. Catheter Cardiovasc Interv 2003;60:145–151.
6. Dzavik V, Kharbanda R, Ivanov J, Ing DJ, Bui S, Mackie K, Ram-
samujh R, Barolet A, Schwartz L, Seidelin PH. Predictors of long-termoutcome after crush stenting of coronary bifurcation lesions:importance of the bifurcation angle. Am Heart J 2006;152:762–769.
7. Lim PO, Dzavik V. Balloon crush: treatment of bifurcation lesionsusing the crush stenting technique as adapted for transradial approachof percutaneous coronary intervention. Catheter Cardiovasc Interv2004;63:412–416.
8. Mauri L, Hsieh WH, Massaro JM, Ho KK, D’Agostino R, Cutlip DE.Stent thrombosis in randomized clinical trials of drug-eluting stents.N Engl J Med 2007;356:1020–1029.
9. Miyazaki Y, Nomura S, Miyake T, Kagawa H, Kitada C, Taniguchi H,Komiyama Y, Fujimura Y, Ikeda Y, Fukuhara S. High shear stress caninitiate both platelet aggregation and shedding of procoagulant con-taining microparticles. Blood 1996;88:3456–3464.
0. Ormiston JA, Currie E, Webster MW, Kay P, Ruygrok PN, Stewart JT,Padgett RC, Panther MJ. Drug-eluting stents for coronary bifurcations:insights into the crush technique. Catheter Cardiovasc Interv 2004;63:332–336.
1. Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM, Stankovic G,Airoldi F, Chieffo A, Montorfano M, Carlino M, et al. Incidence,predictors, and outcome of thrombosis after successful implantation ofdrug-eluting stents. JAMA 2005;293:2126–2130.
2. Holubkov R, Laskey WK, Haviland A, Slater JC, Bourassa MG,Vlachos HA, Cohen HA, Williams DO, Kelsey SF, Detre KM.Angina 1 year after percutaneous coronary intervention: a reportfrom the NHLBI Dynamic Registry. Am Heart J 2002;144:826 –833.
3. Steigen TK, Maeng M, Wiseth R, Erglis A, Kumsars I, Narbute I,Gunnes P, Mannsverk J, Meyerdierks O, Rotevatn S, et al. Random-ized study on simple versus complex stenting of coronary arterybifurcation lesions: the Nordic bifurcation study. Circulation 2006;
114:1955–1961.




























