Embed Size (px)
Citation preview
Long-term in vivo survival of Rh(D)-negative donor red cells in a patient with anti-LW
H. CHAPI . IS . v. L. HUNTER. M. E. ROSCHE. A N D R . s. SHIREY
The present study documents immediate and long-term survival of crossmatch-incom- patible Rh(D)-negative donor red cells in a patient with anti-LW. A 67-year-old group A Rh(D)-positive man was admitted for urgent coronary artery bypass surgery. The direct antiglobulin test (DAT) was weakly positive in two of five laboratories. His se rum contained anti-LW (two laboratories); his red cells were LW negative (three antisera). Two siblings were LW-positive. Surgery was delayed, and 3 ml Rh(D)-negative crossmatch-incompatible red cellsstored in citrate-phosphate-dextrose-adenine-one were labeled with 25pCi of 51Cr and injected. Immediate survival was approximately 100 percent with 92 percent survival at 20 hours . Six daily blood samples showed a decreased red cell lifespan, (T 1/2 = 14 days). Because of medical complications, 4 units of Rh(D)-negative crossmatch-incompatible blood were then transfused without clinical or hemolytic reaction. The anti-lgG DAT became stronger. In vivo survival of the remaining 51Cr-RBCs became normal (T 1/2 28 days over t h e succeeding 20 days). Following transfusion, no change in serum antibody strength was demonstrated by double-blind titration of seven coded samples. The observations support modest reduction of lifespan for 3 ml of LW-positive red cells, but normal survival following subsequent transfusion of approximately 700 ml of LW-positive red cells. TRANSFUSION 1985;25:39-43.
ANTI-I.W IS A rarely encountered al loant ibody first described in h u m a n s by Levine e t al.' Its clinical significance h a s been considered negligible, based primarily on a single report in 1977' of failure of multi-unit transfusions of LW-positive red cells (RBCs) t o evoke f rank evidence of in vivo hemolysis in a hemorrhaging pat ient whose serum contained anti- LW. M o r e recently. Cummings e t al.' reported t w o
' I Cr survival studies of R h (D)-nega t ive L W-posi tive d o n o r R B C s followed f o r 20 h o u r s af ter infusion (>95% survival a t I hour . 78% a t 20 hours on both occasions).
T h e present report describes t h e in vivo survival of 3 ml of "Cr-labeled Rh( D)-negative crossmatch- incompatible d o n o r RBCs. followed f o r 27 d a y s in a patient with anti-LW'b in his serum. Modestly shortened survival was observed over the initial 6 d a y s . After t ransfusion of 4 units of unlabeled R h ( D ) -
From the Department of Laboratory Medicine and the Barnes Hospital Blood Bank. Washington University Medical Center. St. Louis. Missouri and the Blood Bank. Johns Hopkins Hospital. Baltimore. Maryland.
Supported in part by Research Grant CA02918 from the National Institutes of Health. Department of Health and Human Sciences.
Submitted for publication March 17. 1984; revision received May 12. 1984. and accepted May 23. 1984.
negative crossmatch-incompatible RBCs, survival of t h e remaining labeled RBCs was normal over the succeeding 3 weeks.
Case Report A 67-year-old white man was admitted to Barnes Hospital
because of rapidly progressive angina pectoris. Emergency cardiac catheterization revealed severe three-vessel coronary artery disease. and coronary artery bypass surgery was scheduled for the next day. Eight units of blood were ordered. The patient was typed as group A Rh(D)-positive. with a negative direct antiglobulin test. A routine antibody screen using enhancement medium (Lo-Ion. Gamma Bio- logicals, Houston, TX) was positive in the antiglobulin phase. Tests with a differential RBC panel were positive with all of the panel cells. and all crossmatch results were incompatible. There was no history of prior transfusion. Antiglobulin reactions were strongest against cord RBCs. and results against adult Rh(D)-positive RBCs were stronger than against adult Rh(D)-negative cells. Consultation with the Johns Hopkins Hospital Reference Laboratory sug- gested anti-LW specificity. Because of the urgency to proceed with surgery, a "Cr-labeled "in vivo crossmatch" was undertaken using group A Rh( D)-negative crossmatch- incompatible RBCs (see below). The immediate survival was 100 percent of the expected value, with 90 percent survival still evident a t 20 hours. The surgeons were informed that there was no reason to delay surgery because of transfusion needs. However, on the following day. the patient experi- enced recurrent pulmonary emboli. surgery was postponed,
39

40 CHAPLIN ET A1
and he was anticoagulated. Within 48 hours. the patient had hemoptysis and hematuria and his stools became weakly guaic positive. By the fifth day of the cell survival study. the hematocrit had declined from 35 percent on admission to 27 percent. and transfusion of packed RBCs was necessary. Between the evening of the fifth day and midnight on the sixth day, four units of Rh(D)-negative. crossmatch- incompatible RBCs were transfused without incident. The serum bilirubin concentration did not rise above I .4 mg per dl. and the hematocrit rose a s expected. Bleeding diminished and the patient stabilized. but he never developed the reticulocytosis necessary to bring his hematocrit into the normal range. Two units of Rh(D)-negative crossmatch- incompatible RBCs were transfused on both the 18th and 25th days of the study. Shortly thereafter. he was discharged from the hospital. He remained comfortable a t home on limited activity for 6 months, when recurrent angina and two episodes of syncope and unconsciousness led to his readmis- sion. A triple coronary artery bypass was performed. during which he received 5 units of Rh(D)-negative crossmatch- incompatible RBCs uneventfully. His postoperative course was uncomplicated. and he was discharged 9 days later. As of this writing. his condition remains improved.
Materials and Methods Loboratory tests
Hematocrits. reticulocyte counts. and serum bilirubin concentrations were measured by standard methods. Direct and indirect antiglobulin tests were carried out by conven- tional methods employing polyspecific and monospecific anti-y and anti-C3d anti-human globulin reagents supplied by several manufacturers. Direct antiglobulin tests also employed ten serial dilutions (1:2 t o 1:1024) of potent polyclonal monospecific anti-y and anti-C3d sera prepared by one of the authors (HC). Indirect antiglobulin tests and crossmatches were performed using enhancement media (Lo-Ion) and were tested a t immediate spin. after 10 minutes incubation a t 37OC. and by the antiglobulin test using commercial polyspecific anti-human globulin reagents. For antibody titrations. 22 percent bovine serum albumin was substituted for the Lo-Ion diluent. Titration scores were calculated according t o lssitt and Issilt.' Ether elution was performed by a modification of the Rubin method: Definition of the LW specificity of the antibody and the LW phenotyping of the patient and family members was
generously performed for us by colleagues a t four diffcrcnt reference laboratories: the Johns Hopkins Hospital Blood Bank in Baltimore. Maryland: thc Missouri-Illinois Red Cross Regional Blood Centcr in St. I.ouis. Missouri: the South Florida Blood Service in Miami. Florida: and the Medical Research Council Blood Group Unit in I.ondon. England.
'' Cr in vivo RBC survival Three ml of group A Rh(D)-negativc crossmatch-incom-
patible RBCs stored for 5 days in citrate-phosphate- dextrose-adenine (CPDA-I) were incubated with 25 pCi of "Cr for 30 minutes a t 37°C. washcd three times. and diluted to a total volume of 10 ml with stcrile pyrogen-free saline. Eight milliliters of the well-mixed suspension was injected a t time zero. and samples were obtained a t 30 minutes. 3 and 20 hours. and daily thereafter l o r the next 5 days. "Cr was determined in plasma. a s well a s in whole blood in samples obtained during the first 24 hours and in whole blood samples thereafter. Furthcr samplcs were obtained at approximately 5 d a y intervals for the subsequent 3 weeks. Initial 100 percent expected survival was calculated on the basis of total blood volumc estimated a s 70 ml per kg body weight. A standard was prepared from the residual of the injected labeled RBC suspension. a t a dilution equivalent to dilution of the injected volume in the patient's estimated blood volume.
Results Pretransfusion serological studies
The most relevant data are summarized in Table I . The revised nomenclature used is that yf Sistonen and Tippett.h a s further summarized by Tippett . ' The patient typed a s 1.W (a-b-): the specificity of the antibody was anti-LWah.
The direct antiglobulin test results on freshly obtained pretransfusion blood samples drawn into EDTA were negative with polyspecific and monospecific commercial reagents in our own blood bank. and in samples shipped to the Missouri-Illinois Red Crossand the South Florida Blood Service. A weakly positive D A T was reported for the sample shipped t o the Johns Hopkins Hospital Reference Labora- tory and was very weakly positive with a marked prozone employing 10 serial dilutions of a potent polyspecific rabbit anti-serum prepared in the author's laboratory (HC). unaffected by neutralization of the serum with IgG: however.
Table 1. Serological studies of the patient and members of his family
Antibody Identification Test Cells
LW(a+b-) LW(a-b+) LW(a-b-) Interpretation
Patient serum positive positive negative Anti-LWab
Phenotyping Results
Antisera
Anti-LW Anti-LW Anti-LW ab Interpretation
Patient cells negative negative negative LW(a-b-) Brother cells positive LW(a+) Sister cells positive LW(a+) Daughter cells (group AB - unable to type)
TRANSFUSION 1985--Vol 25. No I
CI-INICAI. SIGNIFICANCE OF ANTI-I W 41
Q 4
1 1 1 1 Tr
E 3l 5 n V *t
' 1 2 3 4 5 6 7 8 DAY 5
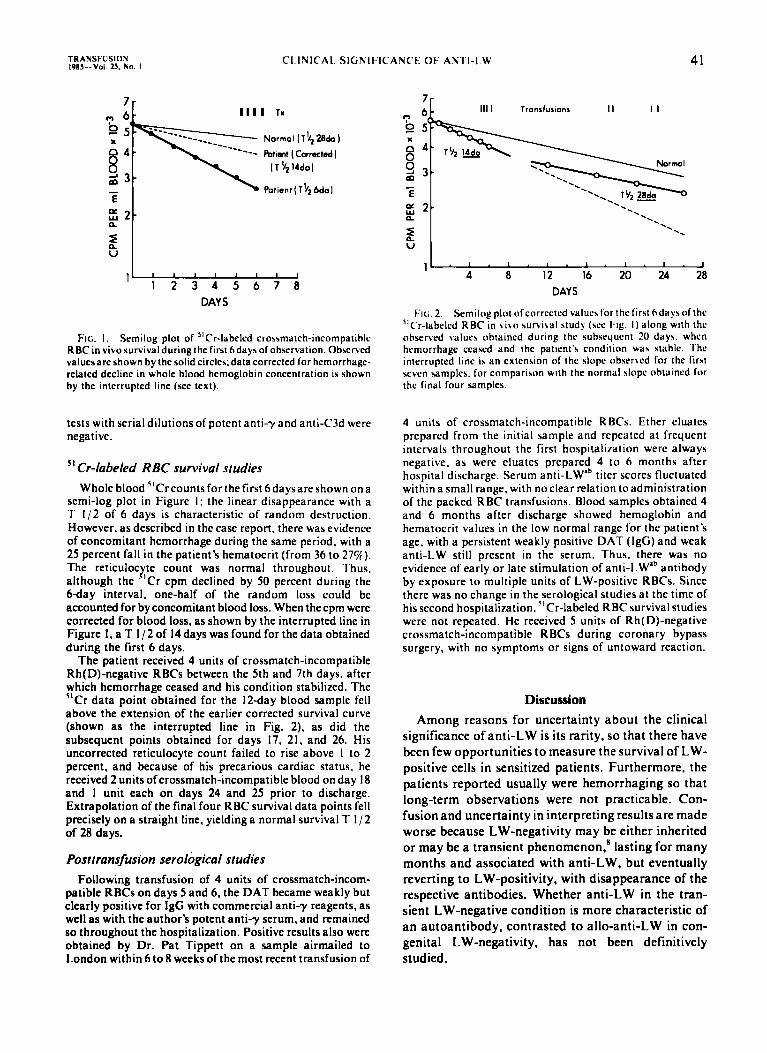
FIG. I , Semilog plot of "Cr-labeled crossmatch-incompatihle RBC in vivosurvivalduringthe first hdaysof observation. Obrerwd valuesare shown by the solid circles data corrected for hemorrhage- related decline in whole blood hemoglobin concentration is shown by the interrupted line (see text).
tests with serial dilutions of potent anti-y and anti-C3d were negative.
Cr-labeled R BC survival studies 51
Whole blood "Cr counts for the first 6 days are shown on a semi-log plot in Figure I ; the linear disappearance with a T 1/2 of 6 days is characteristic of random destruction. However, as described in the case report. there was evidence of concomitant hemorrhage during the same period. with a 25 percent fall in the patient's hematocrit (from 36 to 27%). The reticuloc te count was normal throughout. Thus. although the . ' C r cpm declined by 50 percent during the M a y interval. one-half of the random loss could be accounted for by concomitant blood loss. When the cpm were corrected for blood loss, as shown by the interrupted line in Figure I , a T I / 2 of 14 days was found for the data obtained during the first 6 days.
The patient received 4 units of crossmatch-incompatible Rh(D)-negative RBCs between the 5th and 7th days. after which hemorrhage ceased and his condition stabilized. The "Cr data point obtained for the 12day blood sample fell above the extension of the earlier corrected survival curve (shown as the interrupted line in Fig. 2). as did the subsequent points obtained for days 17, 21. and 26. His uncorrected reticulocyte count failed to rise above I to 2 percent, and because of his precarious cardiac status. he received 2 units of crossmatch-incompatible blood on day I8 and I unit each on days 24 and 25 prior to discharge. Extrapolation of the final four RBC survival data points fell precisely on a straight line. yielding a normal survival T I / 2 of 28 days.
Posttransfusion serological studies Following transfusion of 4 units of crossmatch-incom-
patible RBCs on days 5 and 6, the DAT became weakly but clearly positive for IgG with commercial anti-y reagents. as well as with the author's potent anti-y serum, and remained so throughout the hospitalization. Positive results also were obtained by Dr. Pat Tippett on a sample airmailed to London within 6 to 8 weeks of the most recent transfusion of
Y
" - ; 8 12 16 20 24 . J 28 DAYS
FIG. 2. Semilog plot of corrected valuer for the l'irrt h d a y of the "Cr-lahclrd RBC in \ i \ o survibal study (rce Fig. I ) along with the ohserved valuer obtained during the suhrcqucnt 20 days. when hemorrhage ceased and the patient'\ condition war stahle. The interrupted line ir an extension of the slope obserbcd for the first reven umples. for comparison with the normal rlopc ohtaincd for the final four samples.
4 units of crossmatch-incompatible RBCs. Ether eluates prepared from the initial sample and repeated at frequent intervals throughout the first hospitali~ation werc always negative, as were eluates prepared 4 to 6 months after hospital discharge. Serum anti-LWab titer scores fluctuated within a small range. with no clear relation to administration of the packed RBC transfusions. Blood samples obtained 4 and 6 months after discharge showed hemoglobin and hematocrit values in the low normal range for the patient's age, with a persistent weakly positive DAT (IgG) and weak anti-LW still present in the serum. Thus. there was no evidence of early or late stimulation of anti-LW'b antibody by exposure to multiple units of LW-positive RBCs. Since there was no change in the serological studies at the time of his second hospitalization. "Cr-labeled RBC survival studies were not repeated. He received 5 units of Rh(D)-negative crossmatch-incompatible RBCs during coronary bypass surgery, with no symptoms or signs of untoward reaction.
Discussion Among reasons for uncertainty about the clinical
significance of anti-LW is its rarity, so that there have been few opportunities to measure the survival of LW- positive cells in sensitized patients. Furthermore, the patients reported usually were hemorrhaging so that long-term observations were not practicable. Con- fusion and uncertainty in interpreting results are made worse because LW-negativity may be either inherited or may be a transient phenomenon,' lasting for many months and associated with anti-LW. but eventually reverting to LW-positivity. with disappearance of the respective antibodies. Whether anti-LW in the tran- sient LW-negative condition is more characteristic of an autoantibody, contrasted to allo-anti-LW in con- genital LW-negativity. has not been definitively studied .

42 CHAPLIN ET AL. TRANSFUSION Vol. 25. No. I - 1985
Table 2. Transfusions of LW-positive blood in presence of anti-LW
Present Authors
Antibody specificity Anti-LW titer Posttransfusion DCT: Pretransfusion
Posttransfusion (3-4 units) 51Cr-labeled RBC survival at 1-3 hrs
at 20-24 hrs at 6 days
Macrophage assay (Schanfield)
Anti-LWab no rise
negative (3 labs) weakly positive (2 labs)
positive (IgG) 95% 900/0 73%
not tested
Cummings et al.'
Anti-LWa 128 - 2048
negative
negative 95% 78%
not tested predicted acceptable survival
The relative safety of transfusing Rh( D)-negative LW-incompatible blood was strongly supported by Tregallas et a]..' whose continuously bleeding patient with ulcerative colitis received 50 units of unlabeled crossmatch-incompatible donor RBCs without appar- ent acute o r late untoward effects. More recently. Cummings et al.' reported two 20-hour "Cr-labeled LW-positive RBC survival studies in a bleeding patient with anti-LW' in her serum and a negative DAT. Table 2 compares selected features of our patient with the patient reported by Cummings et al.' There are some similarities and some differences. In Cummings' patient, the antibody specificity was anti-LW'. con- trasted to anti-LWab in our patient. The pretransfusion D A T was negative in Cummings' patient compared to the equivocal initial results in ours, and weak positivity for IgG in Tregallas' patient.' Most striking is the posttransfusion rise in anti-LW' titer from 128 to 2048 in Cummings' patient in contrast t o no evidence for anti-LWab stimulation either early or late (over 6 months of repeated testing) following transfusion of 8 units of Rh(D)-negative crossmatch-incompatible blood. Whether this could be related to a difference between auto- and allo-anti-LW is unknown. Cum- mings et al.' considered their patient's anti-LW' to be a n alloantibody. although definitive evidence for that position was not given. We d o not know whether our patient's anti-LWab is a n auto- o r alloantibody. He consistently typed as LW(a-b-) during 8 months of observation. We plan to follow him to determine whether his RBC phenotype reverts to LW-positive, with concurrent disappearance of anti-LW antibody, as occurred in the patient reported by Tregallas. Regardless of the above speculation. it is significant that even when the anti-LW titer in Cummings'patient reached 2048. there was no evidence of markedly accelerated hemolysis. suggesting either low affinity of the antibody o r paucity o r inaccessibility of the LW' antigens in that instance.
That anti-LW antibodies are not totally "insignifi- cant" is attested by the 14 day T 1 / 2 exhibited by the small volume (3 ml) of labeled cells studied in our
patient during the first 6 days of observation. It is notable that the 20-hour survival was 78 percent in both of Cummings' mea~uremen t s ,~ consistent with modest shortening of RBC lifespan assuming the RBCs were stored less than 1 week and that there was little o r no blood loss. A normal T 1 / 2 of 28 days was obtained for the 35 percent of labeled cells remaining in our patient's circulation after transfusion of 4 units of crossmatch-incompatible RBCs. The likely expla- nation for the improved survival is that the limited amount of anti-LW became distributed on the much larger LW-positive red cell mass following transfusions and therefore was a t so low a concentration on individual RBC membranes a s not t o prejudice survival. In the present instance, low affinity of the anti-LWab antibody may well have contributed to the normal survival: first, because the initial effect on survival of 3 ml was so modest (T 1 / 2 14 days), and second, free anti-LW was always demonstrable in the serum, even after the administration of 4 whole units of RBCs.
The present results demonstrate the safety and effectiveness of transfusing Rh(D)-negative LW- positive blood to our patient with anti-LWab in his serum. This was demonstrated during his initial hospitalization, while the "Cr-labeled RBC survival study was in progress, and was confirmed during his second hospitalization 6 months later, when he again received 5 units of crossmatch-incompatible Rh(D)- negative RBCs a t the time of coronary artery bypass surgery. These results, added to the reports by Tregallas et al.4 and by Cummings et al.,s support the concept that when transfusing Rh(D)-negative RBCs, anti-LW antibodies may be considered clinically "insignificant." However, the total number of patients studied has been small, and the importance of inherited versus transient LW-negative status of the patient has not been assessed fully. Additional in vivo RBC survival data should be obtained when oppor- tunity permits, but life-saving transfusion should not be withheld because of in vitro anti-LW "incom- pat i bili t y . "
TRANSFUSION CLINICAL SIGNIFICANCE OF ANTI-LW 43 I985 Vol 25. No I
Acknowledgments The authors acknowledge their appreciation of the gracious and
cxemplary cooperation of the patient and his family. without which this study would have been impossible. Weareespcciallygrateful to the following individuals for their invaluableassistance in character- i7ing the patient's serological findings: Ms. Mary Wallhermfechtel. Missouri-Illinois Red Cross Regional Blood Center. St. Louis. MO: Mr. Peter Issitt. South Florida Blood Service. Miami, FL: Dr. Patricia Tippett and Ms. C. L. Lomas. Medical Research Council Blood Group Unit. London. England. We also thank Mr. Donald Rernier. Chief Technologist. Division of Nuclear Medicine. Washington University School of Medicine. for assistance with the "Cr-labeled RBC survival studies.
4. lssitt PD. lssitt C H . Applied blood group serology. 2nd ed. Oxnard: Spectra Biologicals. 1977:36.
5. Miller WV.ed. Technical manual. 7thed. Washington: American Association of Blood Banks 1977:391.
6. Sistonen P. Tippett P. A'new'allele givingfurther insight into the 1.W blood group system. Vox Sang 1982:42:252 5.
7. Tippett. P. Low frequency antigens associated with the Rh system. Perspectives in Blood Group Serology. Houston: Gamma Biologicals. Inc. 1983:3:5 8.
8. Giles CM. The LW blood group: a review. lmmunol Commun 1980:9:225 42.
References I . Levine P. Celano MJ. Wallace J. Sanger R. A human 'D-like'
antibody. Nature 1963:198:596 7. 2. Tregallas WM. Moulds JJ . South SF. Successful transfusion o f a
patient with anti-LW and LW positive blood (abstract). Trans- fusion 197X:IX:384.
3. Cummings E. Pisciotto P. Roth G . Normal survival of Rho ( D ) negative. LW(a+) red cells in a patient with allo-anti LW'. Vox Sang 1984:46:286-90.
Hugh Chaplin. Jr.. MD. Professor of Medicine and Pathology. Washington University School of Medicine. Box 81 18 f60 South Euclid, sI, ~ ~ ~ i ~ . MO 631 10, [Reprint
Mary Ellen Rosche. MT(ASCP)SBB. MBA. Chief Technologist. Barnes Hospital Blood Bank. St. Louis. M O 631 10.
Vicki L. Hunter. MT(ASCP)SBB. Asst. Chief Technologist. Barnes
Rosetta Sue Shirey. MS. MT(ASCP)SBB. Technical Specialist. Johns Hopkins Hospital. Baltimore. M D 21205.
Blood Bank.
Announcement
EIGHTH SUMMER PROGRAM IN METHODS OF IMMUNOLOGIC RESEARCH AND DIAGNOSIS
The Ernest Witebsky Center for Immunology of the State University of New York at Buffalo is offering this summer program on June 9-22, 1985. The 2-week program consists of combinations of core and elective lectures, demonstrations, discussions, and practical laboratory exercises. Participants personally carry out techniques at the bench. The program is open to postdoctoral level, supervisory senior technologists, and graduate students beyond the master's level.
For detailed program description, contact James F. Mohn, MD, Director, The Ernest Witebsky Center for Immunology, 210 Sherman Hall, Buffalo, New York 14214, or call (716) 831-2848. Inquiries should be received by February 15, 1985.