Embed Size (px)
Citation preview

Long-Term Consistency in Speech/Language Profiles:1. Developmental and Academic Outcomes
JOSEPH H. BEITCHMAN, M.D., BETH WILSON, B.Se, I.B. BROWNLIE, B.Sc., HEATHER WALTERS, B.Se,
AND WILLIAM LANCEE, PH.D.
ABSTRACT
Objective: This study examined the 7-year developmental and academic outcome of speech/language-impaired and
control children selected from a community sample. Method: Speech/language and psychiatric measures were adminis
tered to the children at ages 5 and 12.5 years. Using children's age 5 speech/language test results, a cluster analysis
was performed to ascertain whether specific linguistic subgroups would emerge. The long-term consistency of these
subgroups was explored. The association between time 1 speech/language clusters and linguistic, cognitive, and
academic measures at time 2 were examined. Results: Four groups were identified in the cluster analysis: high overall,
poor articulation, poor comprehension, and low overall. Children with peNasive language problems continued to perform
poorly on linguistic, cognitive, and academic measures, while those with comprehension problems fared slightly better
but still had more difficulties than those with normal language. The poor articulation cluster had few articulation errors
at follow-up. Conclusions: Empirically supported speech/language classifications identified as early as age 5 continued
to be relevant into late childhood. PeNasive speech/language impairment in early childhood was associated with
increased risk of poor linguistic and academic outcome at follow-up, while isolated articulatory problems improved over
time. These findings reveal the urgent need for early inteNention among children with peNasive speech/language
impairment. J. Am. Acad. Child Ado/esc. Psychiatry, 1996,35(6):804-814. Key Words: speech/language impairment,
empirical classification, longitudinal study, academic outcomes, speech/language outcomes.
Given the heterogeneous nature of speechllanguagedisorders (Beitchman et aI., I989b), establishing anempirically based classification system is an importantinitial step toward a conceptualization of such disorders.An empirical classification system of linguistic profileswill provide a means for testing the associations betweenclinically relevan t variables and various speechllanguage competencies.
While many researchers have demonstrated the association between demographic, cognitive, behavioral,and academic measures and psychiatric status, few
Aeei'ptn/ No/)embl'l' 2. '995.lJr. Beitdmltln is Chief Child and Family Studies. Clarke Institute 0/
'''yehially. '1oronto. Ms. Wi/sou, Ms. Brownlie, and Ms. Walters are withthe Child find Family Studies Celltre, find Dr. IJII/el'e is with the lJepartment
0/ Culture. Community find Hertlth Studii's, Clarke IlIStitute of Psyehifilly.
'fIJis study W(/S supported by gmnt 6606-3812-42 jiwn the Depmtment 0/
Health and We!jf/l'(' Cimada.Reprillt req/{i'sts to Dr. Beitehman, Chief Child lind hlmily Studies, Clarke
Institute o/P,]ehially, 250 Colle."e Street, '1oronto, Ontario, Canada M5T I R8.OH90-H567/96/.'\506-0H04$O.'\.OO/O© 1996 by the American Academy
of Child and Adolescent Psychiatry.
804
attempts have been made to examine the relationshipbetween these variables and specific speech/languagecompetencies. Beitchman et al. 0989b), Fundudiset al. (979), and Wolfus et al. (980) have examinedthe association between empirically derived speech/language profiles and concurrent cognitive, developmental, and academic measures. However, with theexception of Beitchman et al. 0989b), no investigators have explored the long-term outcome of early
childhood speechllanguage competencies in terms oflate childhood speech/language, cognitive, and academic measures.
In the initial study, Beitchman et al. 0989b) identified four speech/language clusters in a communitysample of speech/language-impaired 5-year-old children and normal controls. On the basis of the children's
scores on measures of articulation and expressive andreceptive language and tests of auditory comprehensionand auditoty memOlY, four clusters were identified:high overall, poor comprehension, poor articulation,and low overall. Children in the high overall cluster
J. AM. ACAD. CHILD ADOI.FSC. PSYCHIATRY, 35:6, JUNE 1996

scored significantly higher than the other clusters onall speech/language measures. Children in the lowoverall cluster scored significantly lower than the otherclusters on all speech/language measures except the testof articulation. Children in the poor articulation clusterscored significantly lower than all other groups on thearticulation measure but had higher scores than the
poor comprehension and low overall clusters on theother measures. Children in the poor comprehensioncluster scored in the low range on most of the tests,especially the auditory comprehension measure.
Significant differences were found among the clustersin IQ and visual-motor integration scores. Childrenin the high overall cluster scored highest on the IQmeasure, followed by the poor articulation, poor comprehension, and low overall clusters. All groups scoredsignificantly higher than the low overall cluster on theBeery test of visual-motor integration.
As part of a 7-year follow-up study, this reportcompares the age 12.5 speechllanguage, cognitive, andacademic functioning of children in the four speech/language clusters identified at age 5 years. The results ofthese comparisons will address a number of theoreticalissues pertaining to the nature of speech/language delays. By determining whether these groups still distinguish children on speech/language and other variables,the stability of the original profiles can be assessed.The analysis of changes in speech/language functioningacross time allows us to understand better the development of speechllanguage functioning. Do specificspeechllanguage skills develop at different rates? Dodelayed groups "catch up" in speech/language functioning? To date these remain unanswered questions.
In practical terms, this study will provide informationabout the outcome of specific speech/language problems and related factors. This information can be usedto better inform parents and children not only of theoutcomes of speech/language disorder but also howother factors such as academic performance are likelyto be affected. By providing parents and other caregiverswith a full account of the likely effecl~ of childrcll'~
speech/language problems, practitioners can improvethe chances that the source of children's deficits inrelated areas will be understood and not be misattributed to other factors such as lack of motivation. Understanding the long-term outcome of specific speech/language deficits will also provide practitioners withempirically based rationales for a more effective use of
]. AM. ACAD. CHILD ADOLFSc:. PSYCHIATRY • .1');(" ]LJNF I')'J(,
DEVEI.OPMENTAI. AND ACADEMIC OUTCOMES
speechllanguage intervention. If children with partiClllar speech/language profiles recover by late childhoodfrom their early childhood deficits, the need for speech/language intervention may be less urgent than for thosechildren whose deficits remain in late childhood.
This is the first of two articles reporting on the 7-yearoutcome of children's empirically classified speech/language functioning. The present article describes theassociation between children's speechllanguage classification at age 5 years and late childhood outcomeat age 12.5 years. Associated cognitive variables suchas IQ and visual-motor skills are examined, as well asdemographic factors such as socioeconomic status(SES). The second article (Beitchman et a!', 1996)explores the association between the speech/languagegroups based on children's age 5 linguistic functioningand their behavioral, emotional, and social outcomes atage 12.5 according to teacher, mother, and self-reports.
METHOD
Subjects
A detailed account of subject selection procedures is ourlinedelsewhere (lkitchman et aI., 1994). BrieRy, in 1982 the first stageof a three-stage language-screening procedure was administered toa one-in-three random sample (N = 1,655) of all 5-year-old Englishspeaking kindergarten children in the Ottawa-Carleton schoolregion. Children who Eli led the screening participated in fiu·therspeech/language testing, and children who r;liled the second stageof speech/language testing participated in the third stage of testing,which included cognitive, developmental, and psychiatric assessments, A total of 169 children, including a subsample of childrenwho passed the speech/language tests, participated in the threestages of testing and were included in the cluster analysis. For afull description of the 1982 study methodology, see lkitchmanet a1. (1989a,b). Subjects were recontacted in 1989 and invitedto participate in follow-up language, cognitive, and psychiatricassessments. Of the 169 time I participants (110 boys, 59 girls),124 (85 boys, 39 girls) participated in speech/language assessmentsat follow-up.
Attrition
To examine the continuity of speech/language perf<lrll1ance overtime, it was necessary to ensure that the sample discussed in thisarticle did not represent a radically differcnt group from thatdiscussed in lkitchman et al. (I 'JI)'Jb). A total of 45 children(26.7%) who participatcd in the time 1 study did not participatcin the follow-up speech/language assessment. The attrition groupwas compared with thc 124 continuing participants on the timeI language, cognitive, and developmental measures reported inBeitchman et a1. (1989b). No differences were found between thegroups on any of these measures. No differences in time 1 SESwere found between the artrition and participating groups; however,children who participated at time 2 were statistically more likelyto have had two-parent homes at time I.
805

BEITCHMAN ET At.
Measures
Table I shows the speechllanguage, cognitive, developmental,and academic measures used at time I and time 2.
Speech/Language Measures. Speech functioning was measured attime I and time 2 using the Photo Articulation Test (PAT)(Pendergast et aI., 1969) and a nonstandardized clinical assessmentof voice and Auency problems. Since no artiClllation errors areexpected in normally developing speech by age 12.5 years, andnorms for the PAT were unavailable for children older than ageI I years, raw error totals were used to measure articulation at time2. For repeated-measures analyses, raw error totals were also usedfor the time I PAT.
Language functioning was measured at time I and time 2 usingseveral standardized instruments. The Peabody Picture VocabularyTest-Revised (PPVT-R) (Dunn and Dunn, 1981) and the Content(C) and Sequence (S) subscales of the Goldman-Fristoe-WoodcockAuditory Memory Test (GFW) (Goldman et aI., 1974) were usedto measure receptive comprehension and memory at time I andtime 2. The two language-screening instruments-Screening Testfor Auditory Comprehension of Language (STACL) (Carrow, 1973)and Bankson Language Screening Test (BLST) (Bankson, 1977)were used to measure auditory comprehension and expressivelanguage at time I only. At follow-up, auditory comprehension wasmeasured by the Clinical Evaluation of l.anguage FundamentalsRevised (Semel et aI., 1986). Expressive and receptive languagewere measured by the Test of Language Development (TOLD) atboth time I and time 2. At time I, the TOLD (Primary) (Newcomerand Hammill, 1977) was used and at time 2 the TOLD-2 (Intermediate) (Newcomer and Hammill, 1988), which is designed for
TABLE 1Tests and Measures at Time I and Time 2
Time I Speech/Language Tests• Photo Articulalion Test"• Peabody Picture Vocabulary Test-Revised"• Goldman-Fristoe-Woodcock Auditory Memory Test-Content"• Goldman-Fristoe-Woodcock Auditory Memory Test-Sequence"• Screening Test for Auditory Comprehension of Language"• Bankson Language Screening Test"• Test of Language Development-Primary
Time 2 Speech/Language Tests• Photo Articulation Test• Peabody Picture Vocabulary Test-Revised• Goldman-Fristoe-Woodcock Auditory Memory Test-Content• Goldman-Fristoe-Woodcock AuditOlY Memory Test-Sequence• Test of Language Development-2-lntermediate• Clinical Evaluation of Language Fundamentals-Revised• Prutting & Kirchner Pragmatics Scale
Time I Cognitive and Developmental Measures• Wechsler Preschool and Primary Scale of Intelligence• Beery Developmental Test of Visual-Motor Integration• Audiometly screening
Time 2 Cognitive, Developmental, and Academic Measures• Wechsler Intelligence Scale for Children-Revised• Beery Developmental Test of Visual-Motor Integration• Kaufman Test of Educational Achievement• Audiometry screening
"Test was used in time 1 cluster analysis.
806
older children, was used. The TOLD Listening Quotient subtestmeasured receptive language, while the TOLD Speaking Quotientsubtest measured expressive language. The TOLD Spoken LanguageQuotient subtest measured both receptive and expressive language.In addition, a IO-minute conversational sample was scored usinga nonstandardized checklist (P-K) to assess pragmatic skills (Pruttingand Kirchner, 1987).
Statistical Classification of Speech/Language Categories. Clusteranalysis was used at time I to determine whether homogeneousgroups ofchildren with similar linguistic profiles could be identified.Speechllanguage measures used for these analyses were STACLand BLST percentiles, PAT percent scores, PPVT standard scores,and GFWC and GFWS scores. The McQueen's k-means clusteringmethod was used for this analysis, and a four-cluster solutionwas indicated.
Cognitive, Developmental, and Academic Measures. Cognitivefunctioning was measured at time I and time 2 using the ageappropriate Wechsler intelligence scale: WPPSI (Wechsler, 1%7)at time I and WISC-R (Wechsler, 1981) at time 2. The Developmental Test ofVisual-Motor Integration (VMI) (Beery and Buktenica, 1967) was administered at time I and the revised version(Beery, 1982) was administered at time 2. Academic functioningwas measured at time 2 using the Kaufman Test of EducationalAchievement (KTEA) (Kaufman and Kaufman, 1985). Items froma teacher report form measured use of special education services.To be considered a consumer of special education services, a child'steacher had to report that the child had been referred for specialclass placement, services, or tutoring. To verifY that placementsreAected remedial aid services rather than enhancement programsfor gifted children, teachers were asked to describe the kind ofservices rendered and their responses were coded accordingly.Unfottunately, only a determination of the general category ofspecial education services was obtained rather than a morespecific measure.
Demographics. Demographic measures included marital and common law status from the parent's interview and Blishen ratings ofSES. The Blishen Scale is a 7-point ordinal coding scalc ofemployment status with I as unemployed or never employed and7 as the highest status occupation. The scale was developed usingcensus data based on persons in the male labor force. Employmentstatus is based on prestige scores, income, and educational requirements (Blishen and McRoberts, 1976). SES was assessed for eachparent. The occupation of the parent with the highest SES wasused to calculate the Blishen code. Because of the variation ofstudents' economic positions, parents with the highest SES in thefamily who also identified as students were omitted from thisanalysis (n = 3). Blishen ratings below 3 were classified as low,Blishen ratings at or above 5 were classified as high, and theremaining ratings were classified as medium SES. Issues of genderwith reference to the linguistic clusters will be explored in a futurepublication. Since there were very few nonwhite participants inthis study, race was not recorded.
Analyses
Analyses of variance (ANOVAs) and X2 tests were conductedto ascertain whether time 2 demographic, linguistic, cognitive,developmental, and educational outcomes were associated with thechildren's time I linguistic profiles. Where possible, repeatedmeasures analyses were conducted with demographic, linguistic,cognitive, and developmental measures to determine the extent towhich the children's scores remained stable over time within theirrespective clusters and the extent to which changes between clusters
J. AM. ACAD, CHIl.D ADOl.ESC. PSYCHIATRY, 35:6, JUNF 1996

occurred. Tukey Honestly Significant Difference post hoc comparisons with a valucs set at .01 and .05 were used to test for significantdifferences among specific clustcrs when significant cluster effectswerc found. It was not possible to conduct repcated-measuresanalyses using educational tests since the KTEA was administeredat time 2 only, and no comparable educational measure was takenwhen the children were 5 years old.
RESULTS
Four linguistic groups emerged from the clusteranalysis: high overall, poor comprehension, poor articulation, and low overall. Children in the high overallcluster were characterized by higher performance onall speechllanguage tests used in the cluster analysis.Members of the poor comprehension cluster obtainedscores that were within the normal range on all ofthese tests except for the STACL, a measure of auditorycomprehension. Children in the poor articulation cluster were impaired on the PAT, a measure ofarticulation,but they scored within the normal range on all othertests used in the cluster analysis. Finally, children inthe low overall cluster obtained low scores on all ofthese speech/language measures.
The time 1 sample (n = 169) included 16 childrenfrom the high overall cluster, 30 from the poor comprehension cluster, 56 from the poor articulation cluster,and 67 from the low overall cluster. The time 2 sampleused in the analyses presented in this article (n = 124)were similarly distributed, with 13 children from thehigh overall cluster, 24 from the poor comprehensioncluster, 46 from the poor articulation cluster, and 41from the low overall cluster. Children who participatedat time 2 did not necessarily complete every test inthe battery or may have had incomplete demographicinformation, causing the sample size per measure tovalY slightly.
Demographics
No significant differences between linguistic clusterswere found when examining parental marital status ormarital/common law status at time 2. This resultdiffered from our time 1 finding that linked maritalstatus with children's linguistic cluster membership(Beitchman et aI., 1989b). While post hoc tests werenot significant, there appeared to be a higher percentageof unmarried parents among children from the lowoverall cluster than among those from the otherthree clusters.
There was a significant relationship between time 2SES and time 1 cluster membership (X2 [6] = 12.76,
J, AM, ACAD, CHII.D ADOI.ESC, PSYCHIATRY, 35:6, JUNE 1996
DEVELOPMENTAL AND ACADEMIC OUTCOMES
p < .05). Only 7.7% of children from the high overallcluster had families with low SES at time 2, with theremaining high overall children equally divided betweenmedium and high SES families. Similarly, only 13.4%of children from the poor articulation cluster hadfamilies with low SES at time 2, with the greatestproportion coming from high SES families. Amongchildren in the poor comprehension cluster, familySES was more evenly distributed at time 2, with morethan one fourth from low SES families. Among lowoverall cluster children, 42.2% had families with lowSES at time 2, with the remainder divided betweenmedium and high SES families.
To determine the extent to which family SESchanged over time by cluster membership, a repeatedmeasures analysis was conducted using Blishen codesat time 1 and time 2. No linguistic cluster by timeinteraction effect was found.
Speech/Language Measures
To ascertain whether children's time 1 speechllanguage clusters differed significantly on their time 2language test scores, one-way ANOVAs were conducted. Results are shown in Table 2.
With the exception of the PAT, all time 2 linguistictest results significantly differentiated among the time1 speech/language clusters. Post hoc tests revealed thatthe low overall cluster continued to perform poorlyrelative to their peers on tests of language proficiency.Children from the poor comprehension cluster alsoshowed continued language deficits compared withchildren without early receptive language impairment.These children experienced difficulties in expressiveand receptive language and pragmatics. In contrast,the poor articulation cluster performed similarly to thehigh overall cluster on many time 2 linguistic measures.
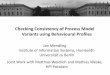
To determine the extent to which children's scoreschanged over time by speech/language cluster, repeatedmeasures analyses were conducted with the PPVT,PAT, TOLD, and the GFW speechllanguage tests attime 1 and time 2. Repeated-measures analyses usingmean .score.s from the PAT and the crwc .speech/
language tests revealed significant linguistic cluster bytime interaction effects. These results are graphed inFigure 1 and Figure 2. On the PAT, children in thehigh overall and poor comprehension clusters had slightdecreases in the number of errors made from time 1to time 2, but there were very large decreases for thepoor articulation cluster (21.65 to 3.61) and for the
807

llEITCHMAN ET AI..
TABLE 2Mean Time 2 Speech/Language 'I'esr Scores by Time I Speech/Language C1usrer
CI C2 C3 C4High Poor Poor Low
Overall Comprehension Anicularion Overall(n = 13) (n= 24) (n = 46) (n = 41)
Time 2 Spccch/Language Test Mean SD Mean SD Mean SO Mean SO
PAT raw crror rotal" (n = 124) 1.54 4.98 0.58 1.98 3.61 7.27 2.51 4.75PPVT-R standard scorc;' (n = 123) 116.85 19.05 97.58 13.67 106.78 15.79 81.63 14.91(;FWC standard score" (n = 119) 52.23 7.75 48.21 7.27 49.78 7.37 43.47 8.31(; FWS standard scored (n = 121) 50.85 11.65 43.71 9.15 46.76 10.95 39.39 9.53TOLD Listening QuotielH" (n = 123) 108.62 14.55 95.58 16.58 107.13 11.27 90.65 11.16TOLD Spcaking Quoriemf(n = 123) 102.00 8.40 85.33 14.89 97.37 20.20 75.60 15.58TOLD Spokcn Language Quoticnt"
(n = 120) 106.62 10.84 94.33 11.89 101.15 12.47 80.48 14.47CELF-R rcccprivc languagc" (It = 12.'3) 109.85 14.09 95.17 12.68 102.09 14.32 79.85 14.47Pruning & Kirchncr; (n = 121) 1.85 2.41 5.09 4.93 2.04 2.94 5.05 4.96
Note: PAT = Phow Aniculation 'I'csr; PPVT-R = Pcabody Picture Vocabulary Tesr-Revised; GFWC = GoldmanFriswc-Woodcock Audiwry Memory Test, COlHelH Subscalc; GFWS = GFW, Sequence Subscalc; TOLD = Tesr ofLanguage Developmcnt; CELF-R = Clinical Evaluarion of Language Fundamentals-Reviscd.
" 1-'(3,120) = 1.70, not signflcant.;, 1-'(3,119) = 26.25, P < .0001, C4 < C1, C2, C3, P < .01; C2 < Cl, P < .01.'F(3,115) = 6.29, P < .001, C4 < C3, P < .05; C4 < Cl, P < .01.d F(3,117) = 5.57, P < .005, C4 < CI p < .01" F(3,119) = 14.81, P < .0001, C2 < C3, P < .05; C4 < C1, C3, P < .01; C2 < CI, p < .01.fF(3,119) = 15.13, P < .0001, C4 < C1, C3, P < .01; C2 < Cl, P < .01."F(3,119) = 24.21, P < .0001, C4 < Cl, C2, C3, P < .01; C2 < CI, P < .01.h F(3,119) = 24.17, P < .0001, C4 < CI, C2, C3, P < .01; C2 < C1, P < .01.; F(3,117) = 5.70, P < .005, CI < C2, C4, P < .05.
low overall cluster (14.65 to 2.51). Score decreases onthe GFWC were most pronounced for the high overall,poor articulation, and poor comprehension dustersfrom time 1 to time 2, whereas scores for the lowoverall cluster stayed at the same very low level.
Cognitive and Developmental Measures
At time 2, the WISC-R and the YMI were used ascognitive and developmental measures. To ascertainwhether children's cognitive and developmental scoresat time 2 differed by linguistic cluster, one-wayANOYAs were conducted. The results of these analysesare shown in Table 3. Post hoc tests revealed that thelow overall cluster had significantly lower mean scoresthan the other three clusters on these cognitive anddevelopmental measures. However, no differences werefound berween mean IQ scores of the poor articulationand high overall clusters.
Repeated-measures analyses were conducted on thesecognitive and developmental measures. No linguisticcluster by time interaction effects were found. Cognitiveand developmental disadvantages experienced at time
808
1 by the low overall cluster appeared to continue at time2. Furthermore, children in the poor comprehensioncluster, while obtaining higher scores than the lowoverall cluster, continued to perform at a significantlylower cognitive level than children in the high overallcluster. The poor articulation cluster performed similarly to the high overall cluster on the WISC-R andthe VMI.
At time 1, the results on the audiomeuy test significantly discriminated among the four clusters. Of thechildren in the low overall cluster, 25% failed theaudiometry test, while fewer than 10% of children inthe poor comprehension and poor articulation groupsfailed, and no children in the high overall group failed.The time 2 audiometry test results, however, did notdiscriminate among the four time 1 clusters (Xl [3] =
2.72, not significant).
Educational Measures
One-way ANOYAs were conducted to determinewhether children's time 1 linguistic clusters were associated with time 2 performance on the KTEA, an aca-
J. AM. ACAD. CHII.I) AI)OI.ESC. PSYCHIATRY. 35:6. JUNE 19%

DEVELOPMENTAL AND ACADEMIC OUTCOMES
25 -------- 65
[:~:::::-<>--- High Overall
Poor Comp
"* Poor Arlie -;>C Poor Arlie
20 a- Low Overall 60 a Low Overall
-----------
In
~0 x()l/)
Cil 15 ~ 55e t1l... 'tlW c:- t1l0 en~ 1:
"~I- 2~ 10 c: 500
u:;:u.e"
5 45
---~- a
~------~ '00
~~.------
0 40 _.. _"-----
Time 1 Time 2 Time 1 Time 2
Fig. 1 Photo Articulation Test (PAT) taw error mean scores by time 1
linguistic clusters. Cluster by time interaction effect: F(3,120) = 19.63, P< .000 I. Comp = Comprehension; Artic = Articulation.
demic measure. Results are presented in Table 4. Time2 mean KTEA subscale scores significantly differentiated among time 1 linguistic clusters. On each KTEAsubscale and the overall composite, the low overallcluster had significantly lower mean scores than theother three clusters according to post hoc tests. Thepoor comprehension cluster had significantly lowermean scores than the high overall cluster on each ofthe KTEA subscales and the overall composite. Whilethe high overall clusters appeared to have slightly highermean scores on all educational measures than thepoor articulation cluster, these differences were notsignificant on post hoc tests. Repeated-measures analyses could not be conducted because the KTEA wasadministered only at time 2.
Children's time 2 use of special education servicesdiffered significantly by their time 1 linguistic clustermembership (X 2 [3] = 11.84, P < .01). Children inthe high overall cluster differed significantly from children in the other three clusters on special education
]. AM. ACAD. CHI!.D ADO!.ESC. PSYCIIIATRY. 35J,. IUNI·: \9%
Fig.2 C;oldman-Frisroe-Woodcock (C;FW) COlllelll mean standard scores
by time 1 linguistic clusters. Cluster by time interaction ell"ct: 1'(3,1 1'5) =4.71, P < .005. Comp = Comprehension; Artic = Articulation.
placement. None of the children from thc high ovcrallcluster received special education. In contrast, 64()lo ofthc low overall cluster, 50% of the poor comprehensioncluster, and 46.3% of the poor articulation clustcrreceived special education.
DISCUSSION
These results reveal that childhood speechllanguagecompetence assessed as early as age 5 is associated withdemographic characteristics, linguistic skills, IQ, visualmotor skills, and academic achievement measures 7years later. In general, the high overall cluster had thebest scores followed by the poor articulation, poorcomprehension, and low overall clusters, respectively.This pattern of results was found across language,cognitive, developmental, and academic measures. Language differences among clusters were found on timc2 measures of receptivc vocabulary, auditory memory,rcceptive language, expressive languagc, and pragmatics.
809

llEITCHMAN ET AI..
TABLE 3Mean Time 2 Cognitive and Developmental Scores by Time I Speech/Language Cluster
CI C2 C3 C4High Poor Poor Low
Overall Comprehension Articulation Overall
Cognitive and (n = 13) (n = 22) (n = 46) (n = 40)
Developmental Measures Mean SD Mean SD Mean SD Mean SD
WISC-R (n = 121)Full Scale IQ" 115.46 12.89 102.23 7.72 106.65 11.18 86.40 13.37Performance IQ" 118.54 10.82 107.50 9.40 108.83 11.72 90.58 14.60VerbalIQ" 109.77 13.62 97.77 9.80 103.98 11.14 84.70 13.07
VMI standard scored (n = 116) 109.85 8.67 104.00 13.24 102.25 9.86 90.16 11.61
Note: WISC-R = Wechsler Intelligence Scale for Children-Revised; VMI = Developmental Test of Visual-MotorIntegration.
"F(3,1 17) = 31.15, P < .0001, C4 < C3, C2, CI, P < .01; C2 < CI, P < .01."FO,117) = 24.78, p < .0001, C2, C3 < CI, P < .05; C4 < C3, C2, CI, P < .01.'FO,117) = 24.65, P < .0001, C4 < C3, C2, CI, P < .01; C2 < CI, P < .01.d F(3,112) = 14.79, P < .0001, C4 < C3, C2, CI, P < .01.
Full Scale, Performance, and Verbal IQ mean scoresall differed by speechllanguage cluster. Speechllanguagegroups were differentiated by time 2 math, spelling,and reading educational measures.
One possible interpretation of these results is thatchildren's linguistic, cognitive, developmental, and academic skills and competencies develop in parallel overtime. With few exceptions, linguistic deficits wereaccompanied by deficits of a similar degree in theother areas of functioning. Although published researchexamining all of these areas of functioning together isscarce, researchers such as Beitchman et al. (1989b),Powell and Bishop (1992), Locke (1994), and Bishopand Edmundson (1987) have speculated on the natureof linguistic delays.
In an earlier report, Beitchman et al. (1989b) suggested that neurodevelopmental delay may be the underlying cause of linguistic deficiencies. If this werethe case we would expect to see delays or deficienciesin other areas of functioning. In fact, the results demonstrate continuing deficits in IQ, visual-motor skills,and academic achievement among these children. Theseresults are consistent with a neurodevelopmental immaturity model of language impairment.
Powell and Bishop (1992) argued that the motor andperceptual deficits that co-occur with specific languageimpairment arise from a common etiology, as yetunspecified. Locke (1994) believed that neuromaturational delay is responsible for many of the children'sauditory, visual, and tactile perceptual deficits, a view
TABLE 4Mean Time 2 KTEA Subscale Scores by Time I Speech/Language Cluster (n = 120)
CI C2 C3 C4High Poor Poor Low
Overall Comprehension Articulation Overall(n = 13) (n = 21) (n = 46) (n = 40)
Time 2 KTEA Subscale Mean SD Mean SD Mean SD Mean SD
Battery Com SS by age" 116.23 11.68 97.38 12.82 106.72 16.37 84.03 14.54Spelling SS by age" 114.77 14.48 99.95 11.77 103.50 15.43 87.35 14.70Reading Com S5 by a7ec 116.54 12.73 98.71 13.66 106.76 15.92 86.43 14.25Math Com SS by age' 113.77 9.56 97.05 12.92 107.89 15.27 84.75 14.48
Note: KTEA = Kaufman Test of Academic Achievement; Com = Composite; 5S = standard score."FO,116) = 23.91, P < .0001, C4 < C2, P < .05; C4 < CI, C3, P < .01; C2 < CI, P < .01."F(3,116) = 15.20, P < .0001, C3 < CI, p < .05; C4 < C2, P < .05; C4 < Cl, C3, P < .01; C2 < CI, P < .01."F(3,116) = 20.18, P < .0001, C4 < C2, P < .05; C4 < CI, C3, P < .01; C2 < CI, P < .01.,I F(3,116) = 24.55, P < .0001, C3 < C2, p < .05; C4 < C2, P < .05; C4 < CI, C3, P < .01; C2 < CI, P < .01.
810 J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY. 35:6, JUNE 1996

similar to our neurodevelopmental immaturity hypothesis and consistent with the follow-up scores of childrenfrom the low overall cluster. The idea that languagedelayed children's brains develop more slowly thanothers and that language-delayed children performpoorly on tasks that, like language, require cognitiveor motor sophistication is also similar to Bishop andEdmundson's (1987) notion of maturational lag. Intheir 2-year follow-up study, Bishop and Edmundsonreported that while language-delayed and normal-language youngsters developed linguistically at similarrates, language-delayed children maintained their original level of delay.
Repeated-measures analyses on available linguistic,cognitive, and developmental scores for the four clustersdemonstrated similar rates of development across clusters over the 7-year follow-up period. Only two significant time by cluster interactions, one involvingarticulation and the other involving memory for content, were found. No other language or cognitivemeasure showed a significant time by cluster interaction, indicating that developmental rates were similaracross clusters.
Why did performance on articulation and memoryfor content measures progress at different rates acrossthe four clusters? Children from the poor articulationcluster had the greatest number of articulation errorsat time 1, but their rapid rate of improvement suggeststhat their articulation skills may have been followinga different developmental time course than were thearticulation skills of children from the other clusters,with more rapid progress between the ages of 5 and12.5 rather than prior to the age of 5. This findingof improved articulation at time 2 is not surprisinggiven results from Baker and Cantwell's (1987) followup study of speech/language-impaired youngsters.These researchers reported that the percentage of purespeech problems found in their sample had the mostdramatic decline at follow-up, in comparison to purelanguage and mixed speech and language problems,which appeared resistant to change.
In the case of memory for content, it appears thatthe low overall cluster had continued deficits over time.The other three clusters showed decreases in their meanscores on auditory memOlY for content over time. Thestability in the performance of the low overall clustermay actually reflect an improvement for this group.Mean scores of the other three clusters decreased by
J. AM. ACAD. CHIl.D ADOLESc:. PSYCHIATRY, .15:6, JUNE 1996
DEVELOPMENTAL AND ACADEMIC OUTCOMES
approximately 10 standard score points from time 1to time 2. These decreases may reflect the increasedskill level required by the age 12.5 measure of auditorymemory compared with the age 5 measure of auditorymemory. If so, we would expect all groups to show adecrease over time. Instead, the mean auditory memOlYfor content scores for the low overall cluster wererelatively similar at both time points. However, anyimprovements these children did experience were notsufficient to allow them to "catch up" with their peers.As demonstrated by the overall results, the low overallcluster continued to have marked deficits in several areasoflanguage competence including auditory memory forcontent.
These results illustrate how early detection of specificlanguage problems can help to identify children most atrisk and in need of interventions. The poor articulationcluster did not appear to be at risk in terms of linguisticand educational performance at follow-up. It is unclearwhether their articulation improved spontaneously orthrough successful speech interventions over the 7-yearperiod. Other study data revealed that half of thechildren from the poor articulation cluster receivedsome form of speech/language intervention. However,the impact of intervention cannot be adequately assessed owing to the nature of this study. That is,because this longitudinal study did not seek to evaluatethe efficacy of speech/language intervention, childrenwere not randomly assigned to treatment and notreatment control groups.
In contrast to the performance of the poor articulation cluster, the low overall cluster showed the leastprogress over time and was most at risk educationally.Early intervention for these youngsters must be apriority. Furthermore, it is apparent that their deficitsextend beyond simply that of language but includevisual-motor skills and educational achievement.
Similar to the low overall cluster, the poor comprehension cluster had significantly lower mean scores onseveral language, cognitive, developmental, and academic measures compared with the high overall cluster.
However, the poor comprehension cluster's mean scoreswere within the normal range on most of these measures. Still, differences between the poor comprehensionand high overall clusters suggest that children fromthe poor comprehension cluster may appear somewhatimpaired, particularly in academic settings, where linguistic skills are most likely to be taxed. It may be
811

IlEITCHMAN ET AI..
that specific interventions would improve the skill leveland abilities of these children as well. Despite meanscores within the notmal range at follow-up, analysesrevealed that half of the poor comprehension clusterhad participated in some special education service,suggesting some degree of impairment.
It is also of interest that there was a significantassociation between speech/language cluster and SES.The vast majority of children from the high overalland poor articulation clusters were from middle to
high SES families at time 2, whereas more than onequarter of the children from the poor comprehensioncluster and almost half of the children from the lowoverall cluster were from low SES families at time 2.While SES for children in each of the clusters improvedover time, there was no significant difference in theamount of change in SES among the clusters.
It appears that children with more pervasive languageproblems were also more likely to live in economicallydisadvantaged circumstances. The importance of SEShas also been revealed in literature linking child povertyto poor nutrition, inadequate housing, and, in general,restricted f:1mily access to necessary resources (Centrefor International Statistics on Economic and SocialWelfare, 1993). Researchers have also found that children exposed to environments rich in language stimulation acquire language competence earlier than dochildren deprived of such environments (Puckering
and Rutter, 1987). It is clear that economic conditionsplay a role in children's speech/language development. The degree of influence social class exacts onchildren's speech/language development requires further investigation.
Speech/Language Clusters and the DSM-IV Classification
System for Communication Disorders
In addition to the issues discussed in the previoussection, these empirically derived clusters provide abasis for critically examining the validity of the DSMIV classification system for communication disorders(American Psychiatric Association, 1994). The DSMIV has classified communication disorders under thefollowing categories: mixed receptive-expressive language disorder, phonological disorder, stuttering disorder, expressive language disorder, and language disordernot otherwise specified. A brief examination of thesimilarities and differences between our empirically
812
based subgroups and the DSM-IV classificationsfollows.
Characteristics distinct to the low overall clusterappeared most similar to the description of mixedreceptive-expressive language disorder from the DSMIV. Similar to the DSM-IV criterion for the mixedreceptive-expressive language disorder, children fromthe low overall cluster had scores on receptive andexpressive language tests that were substantially belowthose obtained from standardized measures of theirnonverbal intellectual capacity. As well, we found evidence of disturbances in their academic achievementand social communication, another DSM-IVcriterion.
In contrast, characteristics of the poor articulationcluster appeared most similar to the DSM-IVphonological disorder and stuttering disorder categories. Similarto the DSM-IVcriteria for both stuttering and phonological disorders, these children showed age-inappropriate speech sounds and fluency problems at time 1.However, in contrast to the criteria for both of thesedisorders, children from the poor articulation clustershowed high academic performance and strong socialcommunication skills. It may be that the poor articulation cluster represents children with the least severe ofthe phonological or stuttering disorder categories. Theirimproved articulation scores at follow-up provide support for this notion.
The poor comprehension cluster was characterizedby impaired receptive language functioning but hadnormal scores on the BLST, a measure of expressivelanguage functioning, at time 1. The DSM-IV reponsthat children with purely receptive language disordersare "virtually never seen." It is unclear whether childrenin the poor comprehension cluster had undetectedexpressive language deficits or whether due to thenature of community samples a group of children wererevealed that would be very unlikely to be detectedand referred to clinicians for treatment. Evidence presented in this article's companion paper regardingbehavioral, emotional, and social outcomes demonstrates an association between early childhood poorcomprehension and behavioral problems (Beitchmanet aI., 1996). These behavioral problems may overshadow any language deficits children with poor comprehension experience.
It is interesting that none of the speech/languageclusters had a linguistic profile which resembled theDSM-IVexpressive language disorder classification. The
J. AM. ACAD. CHI!.D ADOLESc:. PSYCHIATRY, 35,(,. JUNE 1996

DSM-IV reports prevalence rates for developmentalexpressive language disorder between 3% and 5%. Yetno cluster clearly resembled this category despite theutilization of a community sample. In another report(Beitchman et aI., 1994), we have described a groupof children from this study with expressive languagedeficits only. The TOLD Spoken Language and Listening Quotients were used to define this group. Interms of distinguishing between expressive languagedeficits and normal functioning, it is possible that theTOLD Spoken Language Quotient is a more sensitiveinstrument than the BLST. Because the BLST is intended as a screening instrument, using more sensitivemeasures of expressive language functioning in similarcluster analyses may result in the identification of agroup with purely expressive language disorders.
Bishop and Rosenbloom (1987), using their clinicalexperience and findings from the relevant literature,proposed a classification system for speech and languagedisorders. They have described a category of disorderlabeled syntactic-pragmatic disorder, which loosely corresponds to delayed or disordered phonological andexpressive language. However, Bishop and Rosenbloomreported that studies of these children revealed deficitsof receptive language as well. The identification of acategory of children with expressive language impairment as described in the DSM-IVis clearly important,but the empirical data remain mixed at this point.
Conclusions
The predictability oflate childhood linguistic, cognitive, and academic outcomes based on early childhoodspeech/language competence supports the utility ofthese classifications. Many significant associations werefound between time 1 speechllanguage cluster membership and follow-up speechllanguage, cognitive, developmental, demographic, and academic measures.However, it should be stressed that these findingsare correlational and caution must be exercised ininterpreting them. Potentially important factors suchas speech/language intervention have not heen takeninto consideration in these analyses. While study datado reveal that a considerable number of children included in these analyses received speech/language treatment (n = 48), treatment was not randomly assignedand consequently its impact cannot be adequatelyassessed in this study. However, selectivity factors certainly playa role in who receives treatment, since the
J. AM. ACAD. CI-III.D ADOI.ESC. PSYCHIATRY, .l,):!>, JUNE 19%
DEVEI.OpMFNTAI. AND ACADFMIC OUTCOMES
most severely disordered children are most likely to
receive treatment and least likely to improve at followup (Beitchman et aI., 1993). This study provides oneof the first empirically grounded classification systemsfor early childhood speech/language impairment. Whileit provides a foundation from which to build, it isimportant in future work to take into account baselineand intermittent variables in accurately assessing theeffect of early childhood speech/language disorders onoutcome. Factors such as comprehensive preschoolintervention programs and psychosocial factors suchas the experience ofearly trauma have not been incorporated in these analyses. Taking into account suchvariables will provide a more elaborate model for understanding the association between early speech/languageimpairment and late childhood linguistic, cognitive,and academic outcome. In addition to these outcomes,early childhood speechllanguage profiles are discussedin terms of behavioral, social, and emotional outcomesin part II (Beitchman et aI., 1996).
REFERENCES
American Psychiatric Association (1994), Dit/glloslic rllld Sirl/islil'll! Mtlllllft!ofMl'Illai Disordm, 1th edilioll (DSM-IV). Washington, DC: AmericanPsychiatric Association
Baker I., Cantwell Dp (I987), A prospective psychiatric f()lIow-up ofchildren with speechllanguage disorders. J Alii Actld CNId AdolescPsychitltry 26:546-553
Bankson NW (1977), Brlllksoll {rllIgurlgeSael'llilig 'f;'SI. Baltimore: University Park Press
Beery KE (1982), Thc f)mclo/'lIIcntrll 'f;'SI 0/ ViJllrll-Molor Ili/(Xm/ioli.Cleveland: Modern Curriculum Press
Beery KE, Buktenica NA (1967), 'fhc BCl'l)'-Bukll'llim f)CIICIO/,lIIl'Illrll 'f;'N0/ Visurll-Motor Integrrltioll. Chicago: Follett Publishing
Ikitchman )H, Browolie EB, loglis A et al. (I994), Seven-year f()lIow-upof speechllanguage stability and outcome. J Alii Amd Child AdolcscPsychirltry .')3: I322- I3.')0
Ikitchman )H, Ferguson B, Schachter D et al. (1993), A SClil'll Ymr hlilo/{)u/' Siudy o{)pecchHrtngllflgc IIII/'tlired tllld COlilrol Children. Final Report,Health and Welfare Canada, grant 6606-3812-42
Beitchman )H, Hood), Rochoo), Peterson M (I 989a), Empirical classification ofspeech/language impairment in children: II. Behavioral characteristics. J Alii Actld Child Adolesc Psychitlll)' 28: I 18-123
Beitchman )H, Hood ), Rochon ), Peterson M, Mantini '1', Majumdar S(I989b), Empirical classification of speechllanguage impairment inchildren: I. Identification of speech/language categories. J Am AmdChild Adolcsc Psychitl/l)' 28: 112- 117
Bcitt:hlll.lll )1 I, Wilsol1 H, Brownlie EB, Wallers I I, Inglis A, I.allu..'c W
(I 996), Long-term consistency in speech/language profiles: II. Behavioral, emotiona!, and social outcomes. J Am ACrid Child Adolcsc PsyrhirlII)' 35:815-825
Bishop DVM, Edmundson A (I987), Specific language impairment as amaturational lag: evidence from longitudinal data on language andmotor development. f)ClJ Mcd C/,ild NCllroI29:442-459
Bishop DVM, Rosenbloom L (1987), Childhood language disorders: classification and overview. In: languagc l)clJc/opmclll tlJu/ fJisorr!l'n, YuleW, Rutter M, cds. Netherhall Gardens, London: Mac Keith Press,PI' 16-41
813

BEITCHMAN ET AI..
Blishen BR, McRoberts HA (1976), A revised socioeconomic index foroccupations in Canada. Can Rev Sociol Allthropol13:7l-79
Carrow E (1973), Saeening Test fOr Allditory Comprehension of !.angllage,5th cd. Boston: Teaching Resources Corp
Centre for International Statistics on Economic and Social Welt,re (1993),COllntdown 93: Glmpaign2000 Child Poverty Indicator Report. Toronto:Canadian Council on Social Development
Dunn I.M, Dunn I.M (1981), Peabody Pictllre Vocabulfll] Test-Revised:Manila!. Nashville, TN: American Guidance Center
Fundudis T, Kolvin I, Garside R (1979), Speech Retarded and DeafChildren:'IlJeir Psychological DelJelopment. London: Academic Ptess
Goldman R, Fristoe M, Woodcock RW (1974), Goldman-Fristoe- WoodcockAuditory Memory Tests. Circle Pines, MN: American Guidance Services
Kaufman AS, Kaufman NL (1985), Kaufinan Test ofEducational Achievemerit. Circle Pines, MN: American Guidance Services
Locke JL (1994), Gradual emetgence of developmental language disorders.j Speech Heal' Res 37:608-616
Newcomer PL, Hammill DO (1977), The Test of !.anguage Development(I0!.D). Austin, TX: Empite Ptess
814
Newcomer PL, Hammill DO (1988), Test of !.anguage Development-2(TOLD-2). Austin, TX: Empire Press
Pendergast K, Dickey SE, Selmar JW, Soder AL (1969), Photo ArtiClllationTest. Danville, IL: Interstate Printers and Publishers
Powell RP, Bishop DVM (1992), Clumsiness and perceptual problems inchildren with specilic language impairment. Dev Med Child Neurol34:755-765
Prutting CA, Kirchner DM (1987), A clinical appraisal of the pragmaticaspects of language. j Speech Hear Disord 52:105-1 19
Puckering C, Rutter M (1987), Environmental inAuences on languagedevelopment. In: I.anguage Developmellt and Disorders, Yule W, RutterM, eds. Netherhall Gardens, London: Mac Keith Press, PI' 103-128
Semel E, Wiig EH, Secord W (1986), Clinical Eualuation of LanguageFundamelltals-Revised (CELF-R). San Antonio, TX: Psychological Corp
Wechsler 0 (1967), Manual fOr the Wechsler Preschool and Primary Scaleof IlItelligence. New York: Psychological Corp
Wechsler 0 (1981), Manllal fOr the Wechsler Intelligence Scale fOr ChildrenRelJised. San Antonio, TX: Psychological Corp
Wolfus B, Moscovitch M, Kinsbourne M (1980), Subgroups of developmental language impairment. Brain Lang 10:152-171
J. AM. ACAD. CHILD ADOl.ESC. PSYCHIATRY, 35:6, JUNE 1996