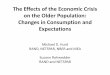
Ophthalmology Volume 120, Number 10, October 2013Figure 1. Blue
Mountains Eye Study (BMES) population ow chart.Mountains area, west
of Sydney. Prospective follow-up of thispopulation-based sample
enabled us to assess the longer-termincidence of vision loss and
common eye diseases and the riskfactors associated with increased
risks of these common diseasesamong older people.
Detailed methods of the baseline survey were reported
previ-ously.20 In summary, at baseline we recruited and examined
3654participants between 1992 and 1994. Surviving
baselineparticipants were invited to participate in the 5-, 10-,
and 15-yearfollow-up examinations. Of these, 2334 returned after 5
years(75.8% of survivors), 1952 returned after 10 years (76.7%
ofsurvivors), and 1149 returned after 15 years (56.1% of
survivors).Over the period between the 10- and 15-year visits, 364
hadmoved, 81 were admitted to a nursing home and were too frail
toparticipate, 454 declined re-examination, and 496 had died (Fig
1).
All baseline and follow-up examinations of the BMES wereapproved
by the Human Research Ethics Committees of theUniversity of Sydney
and the Western Sydney Area Health Serviceand were conducted
adhering to the tenets of the Declaration ofHelsinki. Signed
informed consent was obtained from all partici-pants at each
examination visit.
Study Procedures
The 15-year follow-up examination methods were similar to
thoseused at baseline.20 Participants underwent a comprehensive
eyeexamination after pupil dilation and completed a detailed
mainquestionnaire during a face-to-face interview. Additional
ques-tionnaires were completed at home by study participants.
Visual acuity was measured using a retroilluminated logarithmof
the minimum angle of resolution chart (VectorVision CSV-
2092100TM; VectorVision, Inc., Daytona, OH). Distance VA
wasmeasured at 8 feet (244 cm) for each eye with current spectacles
ifworn, followed by pinhole acuity. Either a previous
spectacleprescription or an autorefraction (Humphrey automatic
refractor,model 597; Humphrey-Zeiss, Oberkochen Germany) provided
thebaseline for a subjective refraction. Subjective refraction was
per-formed using the Beaver Dam Eye Study (BDES) modication ofthe
Early Treatment Diabetic Retinopathy Study protocol.21 Visualacuity
was recorded as the number of letters read correctly in eacheye
(from 0e70). If no letters could be read from the chart at 8
feet(244 cm), VA was assessed further at 2 feet (61 cm) and
wasrecorded as counting ngers, hand movements, light perception,or
no light perception. Visual acuity used in this report refers
tobest-corrected VA after subjective refraction.
Peripheral visual elds were assessed via automated perimetryin
both eyes using Humphrey 24-2 Swedish interactive
thresholdalgorithm standard tests (Humphrey-Zeiss, model 530).
Pupilswere dilated with tropicamide 1% and phenylephrine 10%.
Eyeexaminations that were performed included a slit lamp
(HaagStreit, Koeniz, Switzerland) and retroillumination (Neitz
CT-Rcataract camera; Neitz Instruments, Tokyo, Japan) camera to
assessthe lens. Retinal photographs were obtained using a Canon
funduscamera (CF-60DSi, EOS 1Ds Mk III; Canon, Tokyo, Japan) witha
digital back.
Denitions
Visual impairment was dened as VA worse than 20/40 (fewerthan 41
letters read), and blindness was dened as VA worse than20/200 (0e5
letters read). The denition for VI was in keepingwith the denitions
used in previous BMES reports, and it was the
minimum VA requirement to obtain and maintain an Australian
development of VI or death. Persons eligible for inclusion in
increasing age in either gender. Of these 34 persons, 20 (59%)
had
Hong et al Long-term Changes in VA in Older Populationdrivers
license. An eye was considered to be at risk of VI devel-oping if
VA was 20/40 or better and was considered to be at risk ofblindness
developing if VA was 20/200 or better at baseline.Incident
unilateral VI was dened as development of VI in only1 eye (the
worse eye) at follow-up visits where both eyes were atrisk of VI at
baseline. Similarly, incident bilateral VI was denedas development
of VI in both eyes when at least 1 eye was at risk ofdeveloping VI
at baseline and was dened based on VA in thebetter eye at
follow-up. In addition, any incident VI was dened ashaving at least
1 eye at risk of VI developing at baseline where theat-risk eye was
found to have VI at the follow-up examination.Incidence of any
blindness was dened as having at least 1 eye atrisk of blindness
developing at baseline and the at-risk eye beingfound to be blind
at the follow-up examination.
A change in the number of letters read correctly was dened asthe
difference in the numbers of letters read between the 15-yearand
baseline examinations. Deterioration or doubling of thevisual angle
was dened as a loss of 15 letters or more readcorrectly in the
better eye from baseline to the 15-year visits.Improvement in
vision (halving of the visual angle) was dened ifthere was an
improvement of 15 letters or more read correctly overthe same
period. Eyes were at risk of deteriorating or improvingVA (doubling
or halving the visual angle) if their baseline VA waslight
perception or better, or if the baseline VA was 55 letters orfewer,
respectively.
Causes of Visual Impairment
Cataract was diagnosed during the dilated slit-lamp
examinationsand alsowas recorded during lens photographic
grading.Age-relatedmacular degeneration (AMD) was diagnosed at the
time of thedilated fundus examination and was conrmed by retinal
photo-graphic grading. Glaucoma was diagnosed when glaucomatous
eldloss was detected, based on repeated visual eld tests in which
thevisual eld defect corresponded to optic disc changes,
consistentwith typical glaucomatous cupping.22 Previously
undiagnosedocular conditions detected during the study examinations
werereferred to ophthalmologists, who provided regular eye
clinicservices to the population of the study area. A survey report
of thendings for each participants examination was sent to
theparticipant, treating general practitioner, and ophthalmologist
forthose with ongoing care of pre-existing conditions by their
doctorsor to assist in treatment of newly diagnosed conditions.
The primary cause of VI was dened as the single conditionthat
explained at least 50% of the vision loss. It was assessed at
allexaminations by the same ophthalmologist (P.M.), who assessedall
VI cases and the severity of each eyes pathologic
conditions.Estimating the causes of measured vision loss was based
either onpersonal examination by the same ophthalmologist (P.M.) or
by hisassessment of photographic images or other data. Based on
theseverity of the condition and its likely effect on vision,
theophthalmologist estimated and allocated the proportion of
visionloss resulting from each individual pathological condition,
totaling100%. Most of the causes were responsible for less than 90%
ofreduced vision (e.g., cases with coexisting dense cataract
andglaucoma, or cataract and early AMD).
Statistical Analysis
SAS software version 9 (SAS Inc, Cary, NC) was used for
allanalyses, and age was dened as age at baseline.
Cumulative15-year incidence was calculated while considering the
competingrisk of death.23 The competing risk regression model is
anadaptation of the Kaplan-Meier method that takes into account2
competing events; in this case, the events would be eitherundergone
cataract surgery during the follow-up period.Table 4 shows a
comparison of the incidence of VI between our
study and BDES1 ndings using the modied denition of VI
andblindness, after direct standardization to the age distribution
of theBMES population. Incidences of VI were higher in the
BDESpopulation (11.1%) compared with our population (6.4%),
afteradjusting for competing risk of death. However, the
incidencesof blindness were similar among the BDES population
(1.2%)
2093analyses contributed information up to the time when either
ofthese 2 events occurred. Persons were considered as censored
whenreasons other than death prevented them from participation in
thefollow-up examinations.
The incidence rates of VI and blindness reported by the BDESwere
age standardized to the BMES population for comparison.For this
comparison, we used modied denitions of VI (VA 20/40) and blindness
(VA 20/200) following the denitions used inthe BDES.
Results
The mean age of participants at baseline was 64.5 years, and
57.9%were female. Table 1 shows the baseline characteristics of the
2501participants who attended at least 1 follow-up examination
afterbaseline with complete data for analysis. The main reasons
fornot returning for follow-up examination were participant
frailtyresulting from multiple comorbidities and relocation.
The overall mean decrease in number of letters read
correctlyover the 15 years was similar in right and left eyes (6.9
and 6.8letters, respectively); there was an inverse relationship
betweenreduction in the mean number of letters read correctly from
base-line to the 15-year examination and increasing age, as shownin
Figure 2. There was no signicant gender difference in thechanges in
numbers of letters read correctly in either right or lefteyes (P
0.97 and P 0.25, respectively).
The 15-year cumulative incidence of bilateral VI was 5.2%(119
persons) and varied from 0.4% in those younger than 55 yearsto
10.5% in those 75 years of age or older at baseline. The inci-dence
of bilateral blindness was 0.9% (21 persons) and varied from0% in
those younger than 55 years to 1.7% in those 75 years of ageor
older at baseline. Women were more likely than men to havebilateral
VI (6.8% vs. 3.4%; age-adjusted P 0.02) and bilateralblindness
(1.2% vs. 0.5%; age-adjusted P 0.09). The incidencesof VI and
blindness were strongly age related in both men andwomen (P
whereas our study samples had a higher mortality rate,a
competing risk to VI development. Our study showed that
Botucatu Eye Study. BMC Ophthalmol [serial online] 2009;9:8.
Available at: http://www.biomedcentral.com/1471-2415/
Ophthalmology Volume 120, Number 10, October 2013age was
associated strongly with the development of VI inthis older
population, likely because of the increasingprevalence of many
common ocular diseases associated withaging. Women were twice as
likely as men to have VI andblindness, even after adjusting for
age, which is likelya result of different age-specic mortality
rates between menand women.
Findings from this report may help to establish
effectiveallocation of resources toward vision-related
treatment,rehabilitation, and prevention. Based on the
populationestimates from the Australian Bureau of Statistics33
(2006),the United States Census Bureau34 (2000), and the VIincident
rates from our data, we estimate the number ofolder persons 50
years of age or older with VI willincrease from 480 000 to 1
million in Australia and from3 million to 18 million in the United
States. Thistranslates to an estimated demand for approximately23
000 and 180 000 additional cataract surgical proceduresin the 2
countries, respectively, to treat new unilateral andbilateral cases
of VI and blindness caused by cataract.However, caution should be
applied to these estimates,given that the BMES population was
slightly older andhad a slightly higher socioeconomic status at
baselinecompared with the overall Australian population.14
References
1. Klein R, Klein BE, Lee KE, et al. Changes in visual acuity
ina population over a 15-year period: the Beaver Dam EyeStudy. Am J
Ophthalmol 2006;142:53949.
2. Klein R, Klein BE, Lee KE, et al. Changes in visual acuity
ina population over a 10-year period: the Beaver Dam EyeStudy.
Ophthalmology 2001;108:175766.
3. Zhao J, Ellwein LB, Cui H, et al. Prevalence of
visionimpairment in older adults in rural China: the China
Nine-Province Survey. Ophthalmology 2010;117:40916.
4. Tielsch JM, Javitt JC, Coleman A, et al. The prevalence
ofblindness and visual impairment among nursing home resi-dents in
Baltimore. N Engl J Med 1995;332:12059.
5. Cedrone C, Ricci F, Nucci C, et al. Age-specic changes in
theprevalence of best-corrected visual impairment in an
Italianpopulation. Ophthalmic Epidemiol 2007;14:3206.
6. Hyman L, Wu SY, Connell AM, et al; Barbados Eye StudyGroup.
Prevalence and causes of visual impairment in TheBarbados Eye
Study. Ophthalmology 2001;108:17516.
7. Huang S, Zheng Y, Foster PJ, et al. Prevalence and causes
ofvisual impairment in Chinese adults in urban southern China:the
Liwan Eye Study. Arch Ophthalmol 2009;127:13627.
8. Evans JR, Fletcher AE, Wormald RP. Age-related
maculardegeneration causing visual impairment in people 75 years
orolder in Britain: an add-on study to the Medical ResearchCouncil
Trial of Assessment and Management of Older Peoplein the Community.
Ophthalmology 2004;111:5137.
9. Chong EW, Lamoureux EL, Jenkins MA, et al. Sociodemo-graphic,
lifestyle, and medical risk factors for visual impair-ment in an
urban Asian population: the Singapore Malay EyeStudy. Arch
Ophthalmol 2009;127:16407.
10. Schellini SA, Durkin SR, Hoyama E, et al. Prevalence
andcauses of visual impairment in a Brazilian population: the
20989/8. Accessed March 19, 2013.11. Varma R, Chung J, Foong AW,
et al, Los Angeles Latino Eye
Study Group. Four-year incidence and progression of
visualimpairment in Latinos: the Los Angeles Latino Eye Study. AmJ
Ophthalmol 2010;149:71327.
12. Wang JJ, Foran S, Mitchell P. Age-specic prevalence
andcauses of bilateral and unilateral visual impairment in
olderAustralians: the Blue Mountains Eye Study. Clin
ExperimentOphthalmol 2000;28:26873.
13. Karpa MJ, Mitchell P, Beath K, et al. Direct and
indirecteffects of visual impairment on mortality risk in older
persons:the Blue Mountains Eye Study. Arch Ophthalmol
2009;127:134753.
14. Wang JJ, Mitchell P, Smith W, Leeder SR. Factors
associatedwith use of community support services in an older
Australianpopulation. Aust N Z J Public Health 1999;23:14753.
15. Freeman EE, Egleston BL, West SK, et al. Visual acuitychange
and mortality in older adults. Invest Ophthalmol VisSci
2005;46:40405.
16. McCarty CA, Nanjan MB, Taylor HR. Vision impairmentpredicts
5 year mortality. Br J Ophthalmol 2001;85:3226.
17. Foong AW, Fong CW, Wong TY, et al. Visual acuity
andmortality in a Chinese population. The Tanjong Pagar
Study.Ophthalmology 2008;115:8027.
18. Nucci C, Cedrone C, Culasso F, et al. Incidence of visual
lossin the Ponza Eye Study, Italy. Eye (Lond) 2005;19:17582.
19. Cedrone C, Culasso F, Cesareo M, et al. Incidence of
blindnessand low vision in a sample population: the Priverno Eye
Study,Italy. Ophthalmology 2003;110:5848.
20. Attebo K, Mitchell P, Smith W. Visual acuity and the
causesof visual loss in Australia. The Blue Mountains Eye
Study.Ophthalmology 1996;103:35764.
21. Klein R, Klein BEK, Linton KLP, De Mets DL. The BeaverDam
Eye Study: Visual acuity. Ophthalmology 1991;98:13105.
22. Foran S, Wang JJ, Mitchell P. Causes of incident
visualimpairment: the Blue Mountains Eye Study. Arch
Ophthalmol2002;120:6139.
23. Berry SD, Ngo L, Samelson EJ, Kiel DP. Competing risk
ofdeath: an important consideration in studies of older adults.J Am
Geriatr Soc 2010;58:7837.
24. Hennis AJ, Wu SY, Nemesure B, et al, Barbados Eye
StudiesGroup. Nine-year incidence of visual impairment in
theBarbados Eye Studies. Ophthalmology 2009;116:14618.
25. Racette L, Wilson MR, Zangwill LM, et al. Primary open-angle
glaucoma in blacks: a review. Surv Ophthalmol2003;48:295313.
26. Kawasaki R, Yasuda M, Song SJ, et al. The prevalence of
age-related macular degeneration in Asians: a systematic reviewand
meta-analysis. Ophthalmology 2010;117:9217.
27. Smith W, Assink J, Klein R, et al. Risk factors for
age-relatedmacular degeneration: pooled ndings from three
continents.Ophthalmology 2001;108:697704.
28. Klein BE, Klein R, Lee KE. Incidence of age-related
cataract: theBeaver Dam Eye Study. Arch Ophthalmol
1998;116:21925.
29. Mitchell P, Cumming RG, Attebo K, Panchapakesan J.
Prev-alence of cataract in Australia: the Blue Mountains Eye
Study.Ophthalmology 1997;104:5818.
30. Hill DJ, Gray NJ. Patterns of tobacco smoking in
Australia.Med J Aust 1982;1:235.
31. Smith W, Mitchell P, Leeder SR. Smoking and
age-relatedmaculopathy. The Blue Mountains Eye Study. Arch
Oph-thalmol 1996;114:151823.