Embed Size (px)
Citation preview
45
SECTION II — Preventive CardiologySECTION II — Coronary Artery DiseaseSECTION III — Interventional CardiologySECTION IV — Cardiac ImagingSECTION V — Valvular Heart DiseaseSECTION VI — Heart FailureSECTION VII — Cardiac ElectrophysiologySECTION VIII — Right Heart and Pulmonary CirculationSECTION IX — Pediatric CardiologySECTION X — Cardiac SurgerySECTION XI — Miscellaneous
Chapter 6Long-Term Cardiovascular Outcomes with PCSK9 InhibitorsPREMCHAND RAJENDRA KUMAR • GEETESH MANIK
cholesterol in patients with FH but 79% of pa-tients with heterozygous familial hypercholes-terolaemia in the Netherlands did not achieve their goal for LDL cholesterol (,2.5 mmol/L [100 mg/dL]), despite 96% receiving a statin. A second study showed that 81% of patients with familial hypercholesterolaemia did not achieve LDL cholesterol ,2.6 mmol/L (100 mg/dL) de-spite maximal statin treatment plus a second lipid-modifying agent. In general, monotherapy with a statin is not usually sufficient to get a patient with familial hypercholesterolaemia to goal LDL choles-terol and adding further therapies (ezetimibe, a bile acid sequestrant and possibly nicotinic acid or a fibrate) will provide an additional reduction in LDL cholesterol2.
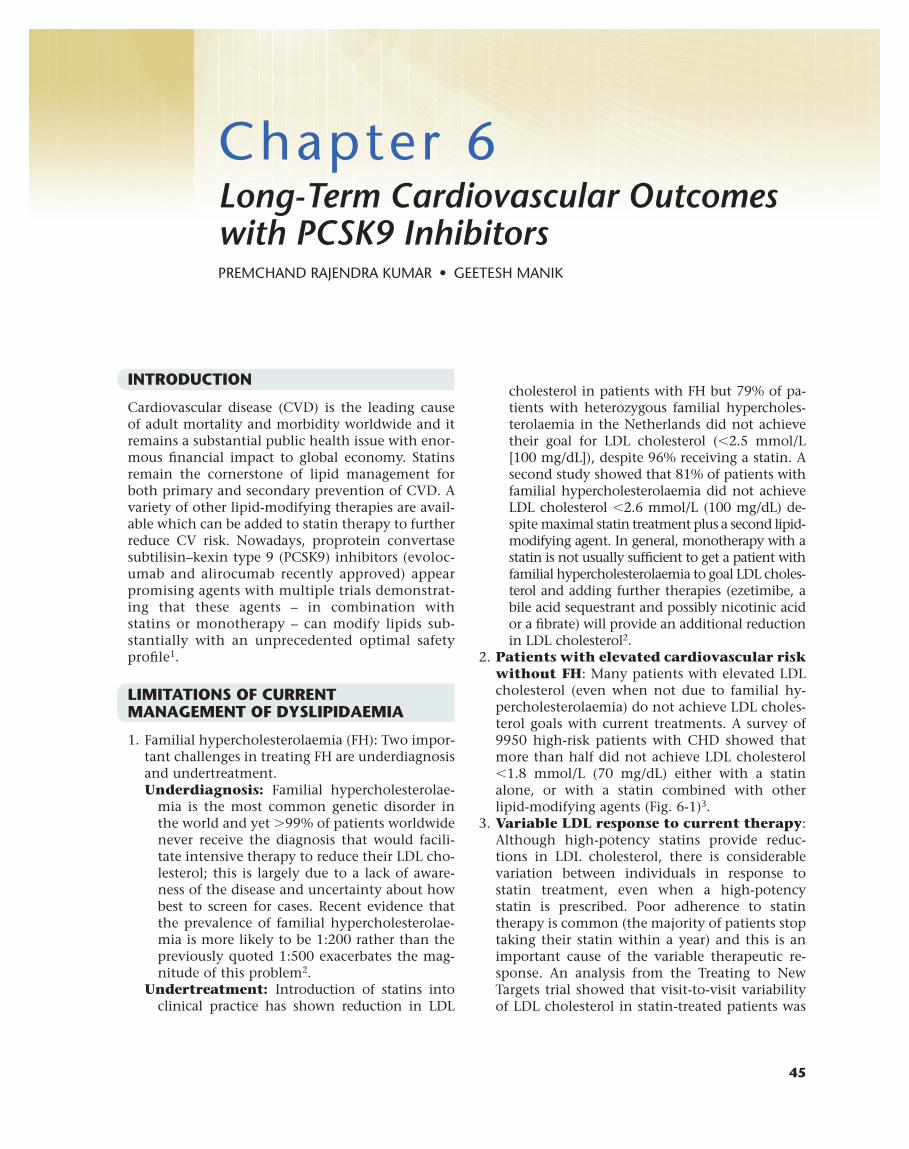
2. Patients with elevated cardiovascular risk without FH: Many patients with elevated LDL cholesterol (even when not due to familial hy-percholesterolaemia) do not achieve LDL choles-terol goals with current treatments. A survey of 9950 high-risk patients with CHD showed that more than half did not achieve LDL cholesterol ,1.8 mmol/L (70 mg/dL) either with a statin alone, or with a statin combined with other lipid-modifying agents (Fig. 6-1)3.
3. Variable LDL response to current therapy: Although high-potency statins provide reduc-tions in LDL cholesterol, there is considerable variation between individuals in response to statin treatment, even when a high-potency statin is prescribed. Poor adherence to statin therapy is common (the majority of patients stop taking their statin within a year) and this is an important cause of the variable therapeutic re-sponse. An analysis from the Treating to New Targets trial showed that visit-to-visit variability of LDL cholesterol in statin-treated patients was
INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of adult mortality and morbidity worldwide and it remains a substantial public health issue with enor-mous financial impact to global economy. Statins remain the cornerstone of lipid management for both primary and secondary prevention of CVD. A variety of other lipid-modifying therapies are avail-able which can be added to statin therapy to further reduce CV risk. Nowadays, proprotein convertase subtilisin–kexin type 9 (PCSK9) inhibitors (evoloc-umab and alirocumab recently approved) appear promising agents with multiple trials demonstrat-ing that these agents – in combination with statins or monotherapy – can modify lipids sub-stantially with an unprecedented optimal safety profile1.
LIMITATIONSOFCURRENTMANAGEMENTOFDYSLIPIDAEMIA
1. Familial hypercholesterolaemia (FH): Two impor-tant challenges in treating FH are underdiagnosis and undertreatment.Underdiagnosis: Familial hypercholesterolae-
mia is the most common genetic disorder in the world and yet .99% of patients worldwide never receive the diagnosis that would facili-tate intensive therapy to reduce their LDL cho-lesterol; this is largely due to a lack of aware-ness of the disease and uncertainty about how best to screen for cases. Recent evidence that the prevalence of familial hypercholesterolae-mia is more likely to be 1:200 rather than the previously quoted 1:500 exacerbates the mag-nitude of this problem2.
Undertreatment: Introduction of statins into clinical practice has shown reduction in LDL
46 SECTION II — Preventive Cardiology
a significant predictor of subsequent events (16% increase in risk for each additional standard de-viation increase in LDL cholesterol variability)4. A number of reports have identified a possible genetic basis for this variable treatment response, although the magnitude of effect of common genetic variants has been questioned5,6.
4. Intolerance to statins: The incidence of ad-verse events attributable to statins in random-ized clinical trials is low. However, side effects in muscle occurred in up to 29% of statin-treated patients in observational studies, presenting a potential barrier to treatment. A switch to a dif-ferent agent in the same class, or to a lower statin dose as part of a combination regimen, helps most patients to remain on statin-based therapy. Pharmacogenetic studies have detected a gene that may identify patients at risk of statin-induced myopathy (SLCO1B1, a member of the solute carrier organic anion transporter family)7.
PCSK9ANDPATHOPHYSIOLOGYOFCHOLESTEROLMETABOLISM
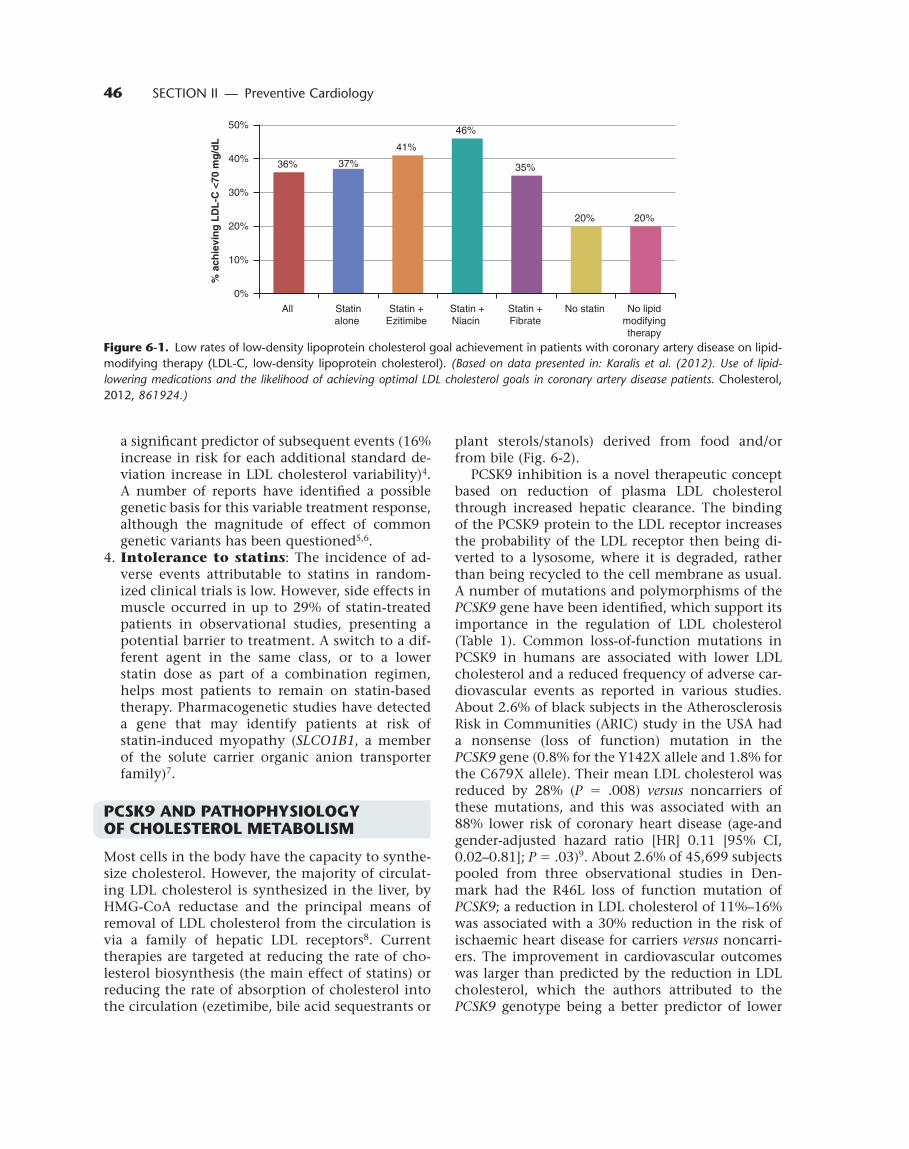
Most cells in the body have the capacity to synthe-size cholesterol. However, the majority of circulat-ing LDL cholesterol is synthesized in the liver, by HMG-CoA reductase and the principal means of removal of LDL cholesterol from the circulation is via a family of hepatic LDL receptors8. Current therapies are targeted at reducing the rate of cho-lesterol biosynthesis (the main effect of statins) or reducing the rate of absorption of cholesterol into the circulation (ezetimibe, bile acid sequestrants or
plant sterols/stanols) derived from food and/or from bile (Fig. 6-2).
PCSK9 inhibition is a novel therapeutic concept based on reduction of plasma LDL cholesterol through increased hepatic clearance. The binding of the PCSK9 protein to the LDL receptor increases the probability of the LDL receptor then being di-verted to a lysosome, where it is degraded, rather than being recycled to the cell membrane as usual. A number of mutations and polymorphisms of the PCSK9 gene have been identified, which support its importance in the regulation of LDL cholesterol (Table 1). Common loss-of-function mutations in PCSK9 in humans are associated with lower LDL cholesterol and a reduced frequency of adverse car-diovascular events as reported in various studies. About 2.6% of black subjects in the Atherosclerosis Risk in Communities (ARIC) study in the USA had a nonsense (loss of function) mutation in the PCSK9 gene (0.8% for the Y142X allele and 1.8% for the C679X allele). Their mean LDL cholesterol was reduced by 28% (P 5 .008) versus noncarriers of these mutations, and this was associated with an 88% lower risk of coronary heart disease (age-and gender-adjusted hazard ratio [HR] 0.11 [95% CI, 0.02–0.81]; P 5 .03)9. About 2.6% of 45,699 subjects pooled from three observational studies in Den-mark had the R46L loss of function mutation of PCSK9; a reduction in LDL cholesterol of 11%–16% was associated with a 30% reduction in the risk of ischaemic heart disease for carriers versus noncarri-ers. The improvement in cardiovascular outcomes was larger than predicted by the reduction in LDL cholesterol, which the authors attributed to the PCSK9 genotype being a better predictor of lower
36% 37%
41%
46%
35%
20% 20%
0%
10%
20%
30%
40%
50%
All Statinalone
Statin + Ezitimibe
Statin +Niacin
Statin + Fibrate
No statin No lipid modifying therapy
% a
chie
vin
g L
DL
-C <
70 m
g/d
L
Figure6-1. Low rates of low-density lipoprotein cholesterol goal achievement in patients with coronary artery disease on lipid-modifying therapy (LDL-C, low-density lipoprotein cholesterol). (Based on data presented in: Karalis et al. (2012). Use of lipid-lowering medications and the likelihood of achieving optimal LDL cholesterol goals in coronary artery disease patients. Cholesterol, 2012, 861924.)
47Chapter 6 — Long-Term Cardiovascular Outcomes with PCSK9 Inhibitors
lifetime LDL cholesterol levels than a point mea-surement of LDL cholesterol made in adulthood10. These observations have fuelled considerable inter-est among researchers in cardiovascular medicine in the prospect of pharmacological inhibition of
PCSK9 as a therapeutic strategy for the manage-ment of dyslipidaemia and cardiovascular risk.
CLINICALEXPERIENCEWITHPCSK9INHIBITORS
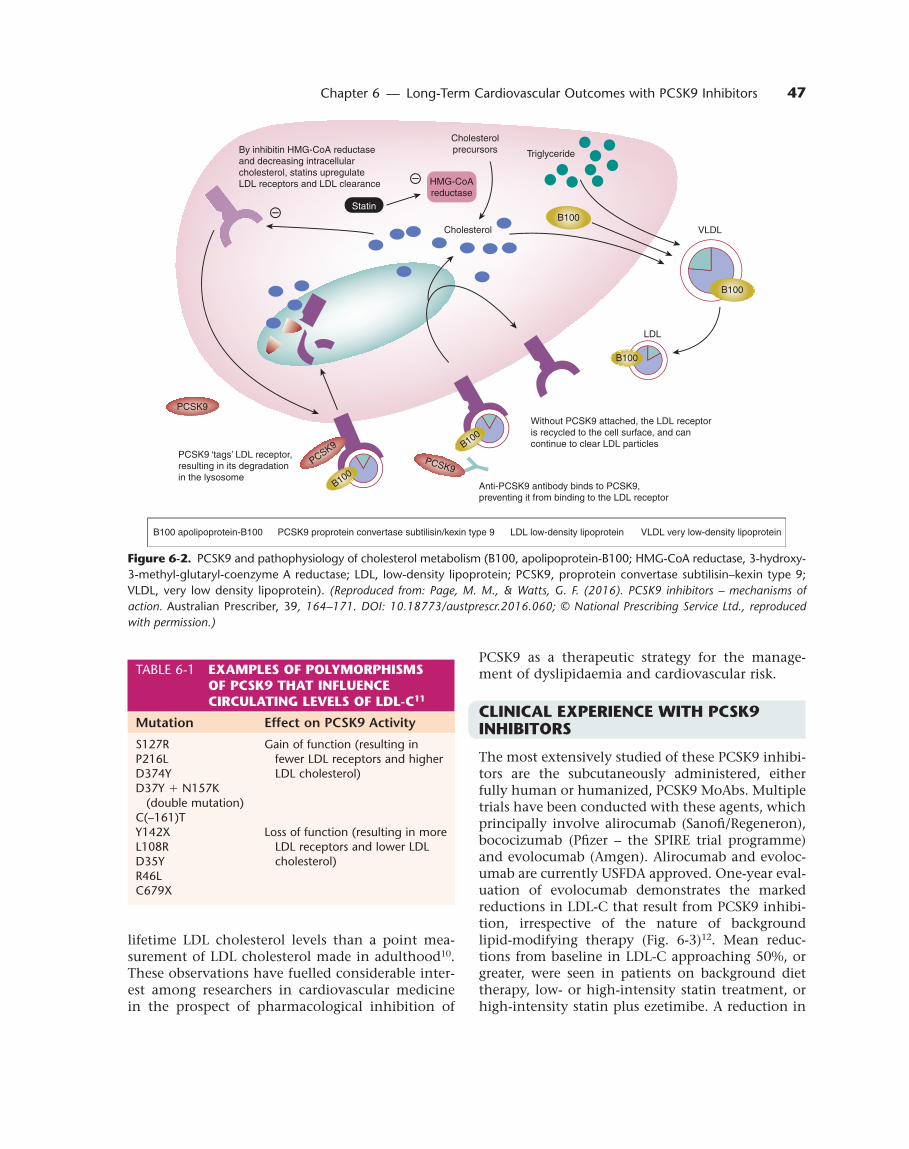
The most extensively studied of these PCSK9 inhibi-tors are the subcutaneously administered, either fully human or humanized, PCSK9 MoAbs. Multiple trials have been conducted with these agents, which principally involve alirocumab (Sanofi/Regeneron), bococizumab (Pfizer – the SPIRE trial programme) and evolocumab (Amgen). Alirocumab and evoloc-umab are currently USFDA approved. One-year eval-uation of evolocumab demonstrates the marked reductions in LDL-C that result from PCSK9 inhibi-tion, irrespective of the nature of background lipid-modifying therapy (Fig. 6-3)12. Mean reduc-tions from baseline in LDL-C approaching 50%, or greater, were seen in patients on background diet therapy, low- or high-intensity statin treatment, or high-intensity statin plus ezetimibe. A reduction in
TABLE 6-1 EXAMPLESOFPOLYMORPHISMSOFPCSK9THATINFLUENCECIRCULATINGLEVELSOFLDL-C11
Mutation Effect on PCSK9 Activity
S127RP216LD374Y D37Y 1 N157K
(double mutation)C(–161)T
Gain of function (resulting in fewer LDL receptors and higher LDL cholesterol)
Y142XL108RD35YR46LC679X
Loss of function (resulting in more LDL receptors and lower LDL cholesterol)
Figure6-2. PCSK9 and pathophysiology of cholesterol metabolism (B100, apolipoprotein-B100; HMG-CoA reductase, 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase; LDL, low-density lipoprotein; PCSK9, proprotein convertase subtilisin–kexin type 9; VLDL, very low density lipoprotein). (Reproduced from: Page, M. M., & Watts, G. F. (2016). PCSK9 inhibitors – mechanisms of action. Australian Prescriber, 39, 164–171. DOI: 10.18773/austprescr.2016.060; © National Prescribing Service Ltd., reproduced with permission.)
By inhibitin HMG-CoA reductaseand decreasing intracellularcholesterol, statins upregulateLDL receptors and LDL clearance
PCSK9 ‘tags’ LDL receptor,resulting in its degradationin the lysosome
B100 apolipoprotein-B100 PCSK9 proprotein convertase subtilisin/kexin type 9 LDL low-density lipoprotein VLDL very low-density lipoprotein
Anti-PCSK9 antibody binds to PCSK9,preventing it from binding to the LDL receptor
Without PCSK9 attached, the LDL receptoris recycled to the cell surface, and cancontinue to clear LDL particles
Cholesterolprecursors Triglyceride
Cholesterol
StatinB100
B100
LDL
VLDL
B100
PCSK9
PCSK9
HMG-CoAreductase
B100
B100PCSK9
48 SECTION II — Preventive Cardiology
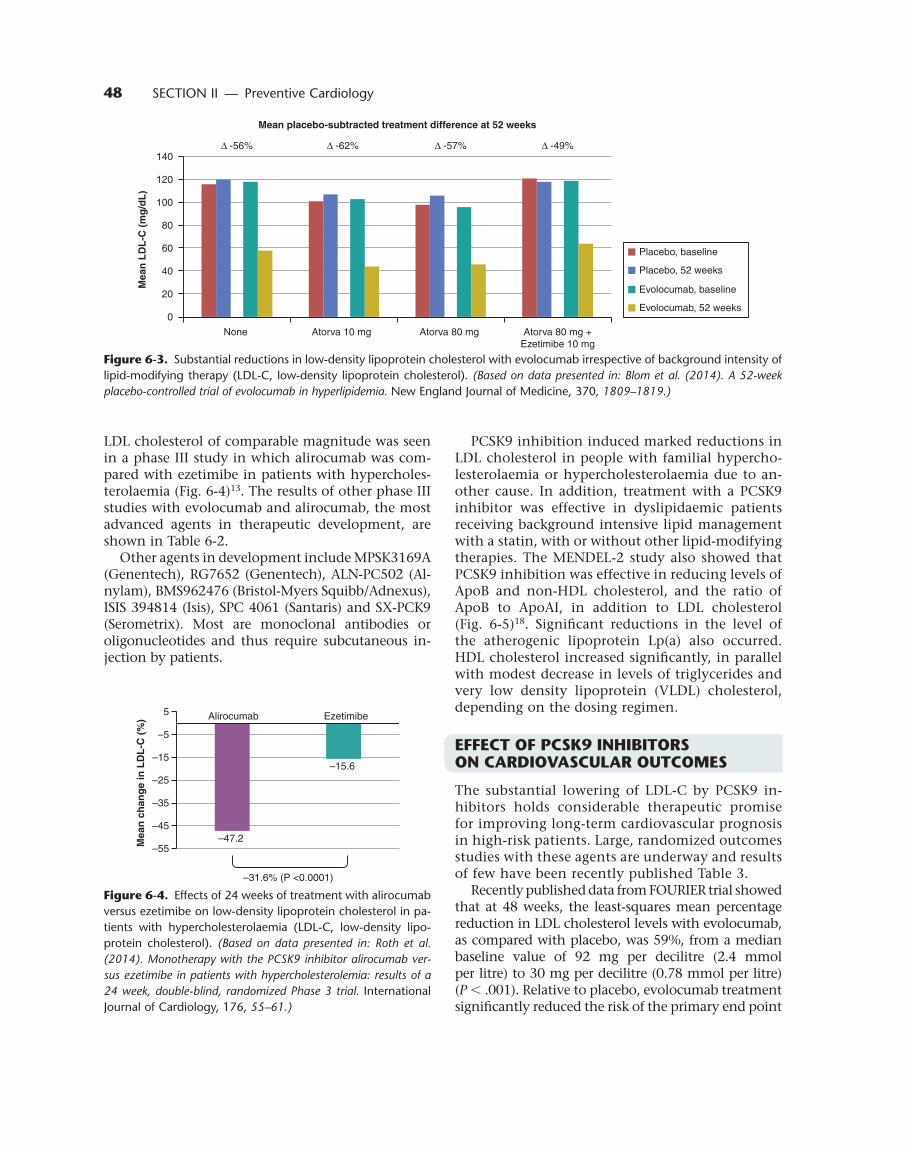
LDL cholesterol of comparable magnitude was seen in a phase III study in which alirocumab was com-pared with ezetimibe in patients with hypercholes-terolaemia (Fig. 6-4)13. The results of other phase III studies with evolocumab and alirocumab, the most advanced agents in therapeutic development, are shown in Table 6-2.
Other agents in development include MPSK3169A (Genentech), RG7652 (Genentech), ALN-PC502 (Al-nylam), BMS962476 (Bristol-Myers Squibb/Adnexus), ISIS 394814 (Isis), SPC 4061 (Santaris) and SX-PCK9 (Serometrix). Most are monoclonal antibodies or oligonucleotides and thus require subcutaneous in-jection by patients.
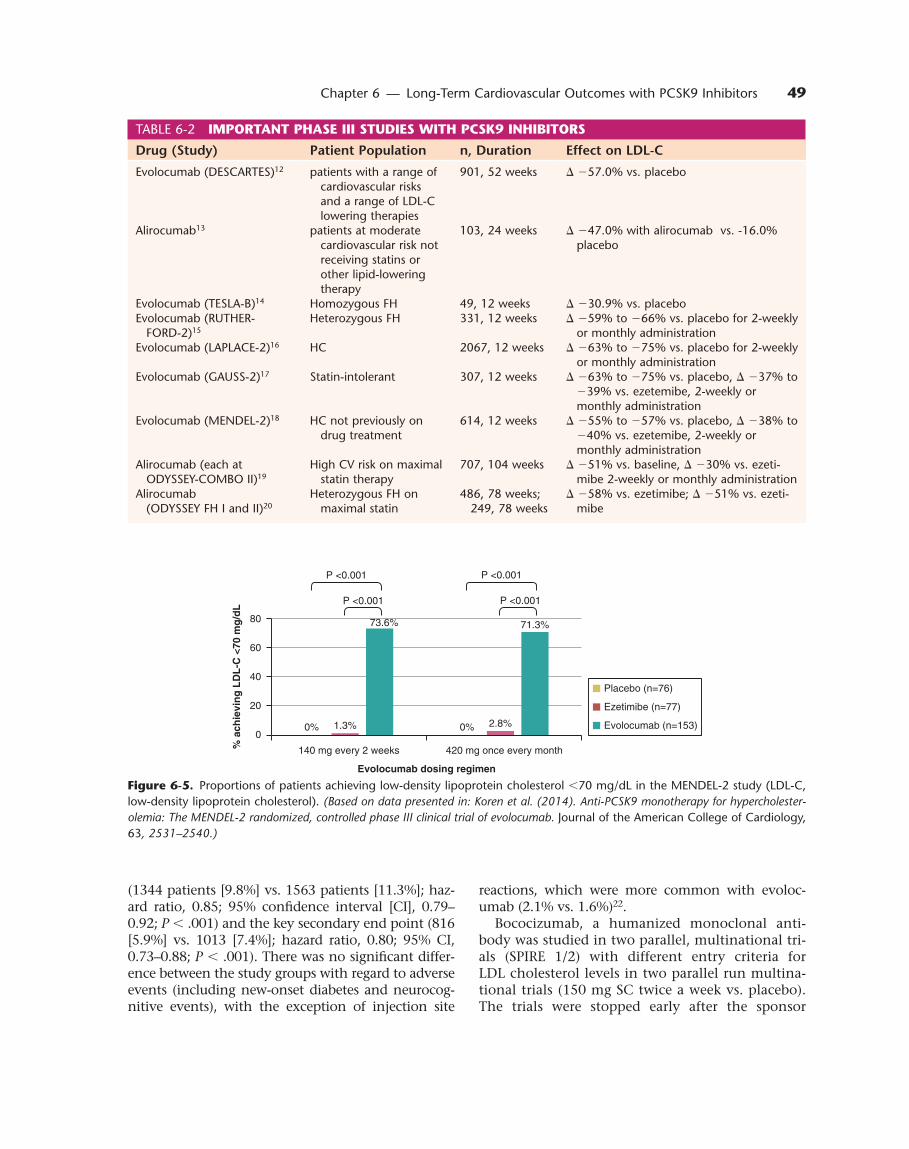
PCSK9 inhibition induced marked reductions in LDL cholesterol in people with familial hypercho-lesterolaemia or hypercholesterolaemia due to an-other cause. In addition, treatment with a PCSK9 inhibitor was effective in dyslipidaemic patients receiving background intensive lipid management with a statin, with or without other lipid-modifying therapies. The MENDEL-2 study also showed that PCSK9 inhibition was effective in reducing levels of ApoB and non-HDL cholesterol, and the ratio of ApoB to ApoAI, in addition to LDL cholesterol (Fig. 6-5)18. Significant reductions in the level of the atherogenic lipoprotein Lp(a) also occurred. HDL cholesterol increased significantly, in parallel with modest decrease in levels of triglycerides and very low density lipoprotein (VLDL) cholesterol, depending on the dosing regimen.
EFFECTOFPCSK9INHIBITORSONCARDIOVASCULAROUTCOMES
The substantial lowering of LDL-C by PCSK9 in-hibitors holds considerable therapeutic promise for improving long-term cardiovascular prognosis in high-risk patients. Large, randomized outcomes studies with these agents are underway and results of few have been recently published Table 3.
Recently published data from FOURIER trial showed that at 48 weeks, the least-squares mean percentage reduction in LDL cholesterol levels with evolocumab, as compared with placebo, was 59%, from a median baseline value of 92 mg per decilitre (2.4 mmol per litre) to 30 mg per decilitre (0.78 mmol per litre) (P , .001). Relative to placebo, evolocumab treatment significantly reduced the risk of the primary end point
0
20
40
60
80
100
120
140
None
∆ -56% ∆ -62% ∆ -57% ∆ -49%
Atorva 10 mg
Mean placebo-subtracted treatment difference at 52 weeks
Atorva 80 mg Atorva 80 mg +Ezetimibe 10 mg
Mea
n L
DL
-C (
mg
/dL
)
Placebo, baseline
Placebo, 52 weeks
Evolocumab, baseline
Evolocumab, 52 weeks
Figure6-3. Substantial reductions in low-density lipoprotein cholesterol with evolocumab irrespective of background intensity of lipid-modifying therapy (LDL-C, low-density lipoprotein cholesterol). (Based on data presented in: Blom et al. (2014). A 52-week placebo-controlled trial of evolocumab in hyperlipidemia. New England Journal of Medicine, 370, 1809–1819.)
–47.2
–15.6
–55
–45
–35
–25
–15
–5
5 Alirocumab Ezetimibe
Mea
n c
han
ge
in L
DL
-C (
%)
–31.6% (P <0.0001)
Figure6-4. Effects of 24 weeks of treatment with alirocumab versus ezetimibe on low-density lipoprotein cholesterol in pa-tients with hypercholesterolaemia (LDL-C, low-density lipo-protein cholesterol). (Based on data presented in: Roth et al. (2014). Monotherapy with the PCSK9 inhibitor alirocumab ver-sus ezetimibe in patients with hypercholesterolemia: results of a 24 week, double-blind, randomized Phase 3 trial. International Journal of Cardiology, 176, 55–61.)
49Chapter 6 — Long-Term Cardiovascular Outcomes with PCSK9 Inhibitors
reactions, which were more common with evoloc-umab (2.1% vs. 1.6%)22.
Bococizumab, a humanized monoclonal anti-body was studied in two parallel, multinational tri-als (SPIRE 1/2) with different entry criteria for LDL cholesterol levels in two parallel run multina-tional trials (150 mg SC twice a week vs. placebo). The trials were stopped early after the sponsor
0%1.3% 2.8%
73.6% 71.3%
0
20
40
60
80
140 mg every 2 weeks 420 mg once every month% a
chie
vin
g L
DL
-C <
70 m
g/d
L
Evolocumab dosing regimen
P <0.001
P <0.001
P <0.001
P <0.001
0%
Placebo (n=76)
Ezetimibe (n=77)
Evolocumab (n=153)
Figure6-5. Proportions of patients achieving low-density lipoprotein cholesterol ,70 mg/dL in the MENDEL-2 study (LDL-C, low-density lipoprotein cholesterol). (Based on data presented in: Koren et al. (2014). Anti-PCSK9 monotherapy for hypercholester-olemia: The MENDEL-2 randomized, controlled phase III clinical trial of evolocumab. Journal of the American College of Cardiology, 63, 2531–2540.)
(1344 patients [9.8%] vs. 1563 patients [11.3%]; haz-ard ratio, 0.85; 95% confidence interval [CI], 0.79–0.92; P , .001) and the key secondary end point (816 [5.9%] vs. 1013 [7.4%]; hazard ratio, 0.80; 95% CI, 0.73–0.88; P , .001). There was no significant differ-ence between the study groups with regard to adverse events (including new-onset diabetes and neurocog-nitive events), with the exception of injection site
TABLE 6-2 IMPORTANTPHASEIIISTUDIESWITHPCSK9INHIBITORS
Drug (Study) Patient Population n, Duration Effect on LDL-C
Evolocumab (DESCARTES)12 patients with a range of cardiovascular risks and a range of LDL-C lowering therapies
901, 52 weeks D 257.0% vs. placebo
Alirocumab13 patients at moderate cardiovascular risk not receiving statins or other lipid-lowering therapy
103, 24 weeks D 247.0% with alirocumab vs. -16.0% placebo
Evolocumab (TESLA-B)14 Homozygous FH 49, 12 weeks D 230.9% vs. placeboEvolocumab (RUTHER-
FORD-2)15Heterozygous FH 331, 12 weeks D 259% to 266% vs. placebo for 2-weekly
or monthly administrationEvolocumab (LAPLACE-2)16 HC 2067, 12 weeks D 263% to 275% vs. placebo for 2-weekly
or monthly administrationEvolocumab (GAUSS-2)17 Statin-intolerant 307, 12 weeks D 263% to 275% vs. placebo, D 237% to
239% vs. ezetemibe, 2-weekly or monthly administration
Evolocumab (MENDEL-2)18 HC not previously on drug treatment
614, 12 weeks D 255% to 257% vs. placebo, D 238% to 240% vs. ezetemibe, 2-weekly or monthly administration
Alirocumab (each at ODYSSEY-COMBO II)19
High CV risk on maximal statin therapy
707, 104 weeks D 251% vs. baseline, D 230% vs. ezeti-mibe 2-weekly or monthly administration
Alirocumab (ODYSSEY FH I and II)20
Heterozygous FH on maximal statin
486, 78 weeks; 249, 78 weeks
D 258% vs. ezetimibe; D 251% vs. ezeti-mibe

50 SECTION II — Preventive Cardiology
elected to discontinue the development of bococi-zumab owing in part to the development of high rates of antidrug antibodies, as seen in data from other studies in the programme. At 14 weeks, pa-tients in the combined trials had a mean change from baseline in LDL cholesterol levels of –56.0% in the bococizumab group and 12.9% in the placebo group, for a between-group difference of –59.0 % (P , .001). In the lower risk, shorter duration trial (in which the patients had a baseline LDL choles-terol level of 70 mg per decilitre [1.8 mmol per li-tre] and the median follow-up was 7 months), major cardiovascular events occurred in 173 patients each in the bococizumab group and the placebo group (hazard ratio, 0.99; 95% confidence interval [CI], 0.80–1.22; P 5 .94). In the higher risk, longer dura-tion trial (in which the patients had a baseline LDL cholesterol level of 100 mg per decilitre [2.6 mmol per litre] and the median follow-up was 12 months), major cardiovascular events occurred in 179 and 224 patients, respectively (hazard ratio, 0.79; 95% CI, 0.65–0.97; P 5 .02). The hazard ratio for the primary
end point in the combined trials was 0.88 (95% CI, 0.76–1.02; P 5 .08). Injection site reactions were more common in the bococizumab group than in the placebo group (10.4% vs. 1.3%, P , .001)23.
An exploratory analysis (pooled analysis of the randomized OSLER-1 and OSLER-2 trials) evaluated the effects of evolocumab on cardiovascular out-comes (Fig. 6-6). The addition of evolocumab versus standard care alone reduced the incidence of a pre-specified composite of adjudicated cardiovascular outcomes over a median follow-up of 11 months.
LONG-TERMSAFETYPROFILEOFPCSK9INHIBITORS
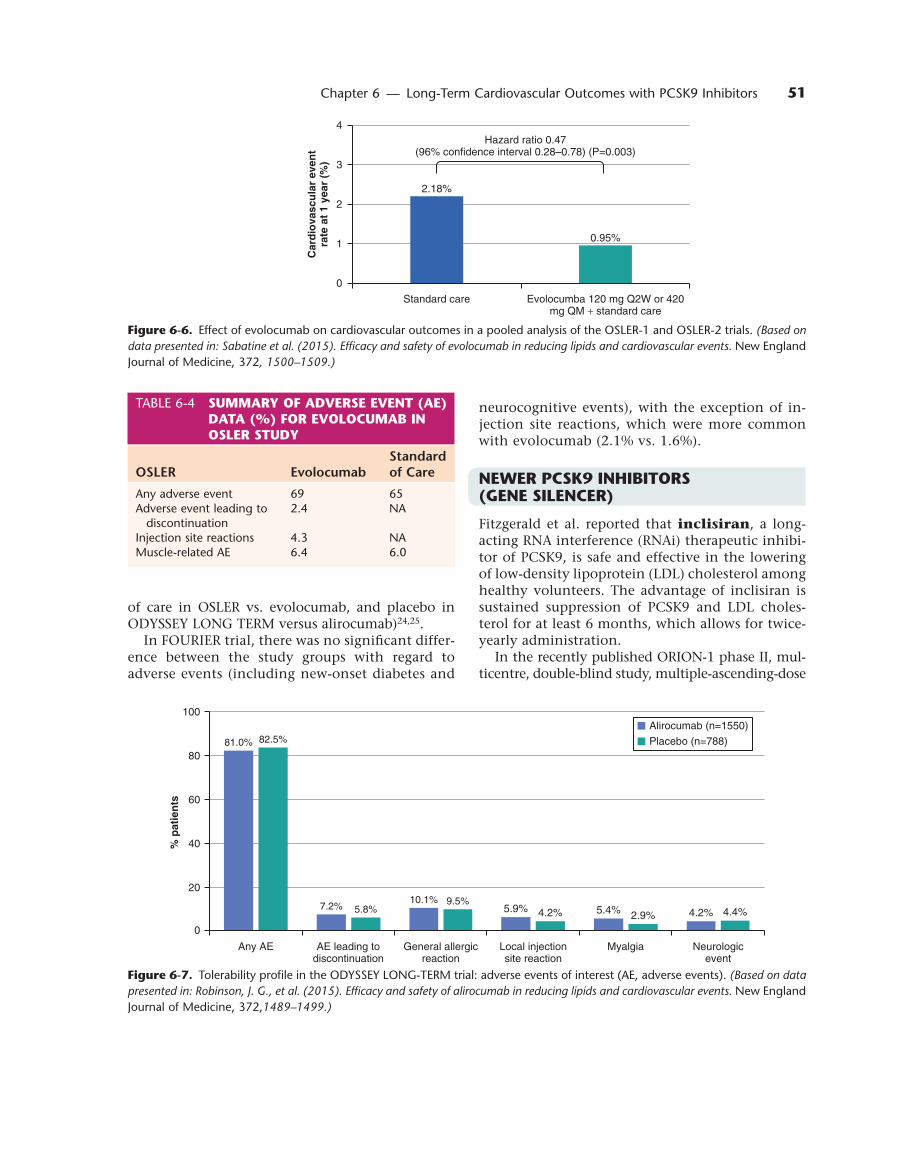
Long-term safety data are available from the OSLER trials (Table 6-4) with evolocumab (n 5 4465, me-dian follow-up 11.1 months) and ODYSSEY LONG TERM (Fig. 6-7) with alirocumab (n 5 2341, 78-week treatment duration). In both reports, adverse events were reported with similar frequency with the PCSK9 inhibitor compared with the comparator (standard
TABLE 6-3 CLINICALOUTCOMETRIALSOFPCSK9INHIBITORS21
Trial Name Study Drug Patient PopulationPrimary Outcome Measure Follow-Up Result
FOURIER NCT01764633
Evolocumab (140 mg every 2 weeks or 420 mg monthly)
n 5 27,564; history of CVD – at high risk of recurrent event; LDL-C 70 mg/dL or non-HDL-C 100 mg/dL; background statin therapy
Time to cardiovascular death, myocardial in-farction, hospitalization for unstable angina, stroke, or coronary revascularization
2.2 years ∆ 259 %; Sig ( primary end points (P , .05)
ODYSSEY OUTCOMES NCT01663402
Alirocumab n 5 18,000; acute coro-nary syndrome ,52 weeks earlier; LDL-C 70 mg/dL or non-HDL-C 100 mg/dL; background statin therapy
Time to cardiovascular death, nonfatal myocar-dial infarction, hospital-ization for unstable angina, or stroke
64 months Ongoing
SPIRE-1 NCT01975376
Bococizumab n 5 17,000; high risk of CVD event, primary and secondary preven-tion; background lipid- lowering treatment; LDL-C 70–100 mg/dL or non-HDL-C 100–130 mg/dL
Time to composite major cardiovascular event (cardiovascular death, nonfatal myocardial in-farction, nonfatal stroke and hospitalization for unstable angina)
10 months (prema-turely stopped – antidrug antibody formation)
∆ 256 %; NS (P 5 .94)
SPIRE-2 NCT01975389
Bococizumab n 5 9000; high risk of CVD event; back-ground lipid-lowering treatment; LDL-C 100 mg/dL or non-HDL-C 130 mg/dL
Time to composite major cardiovascular event (cardiovascular death, nonfatal myocardial in-farction, nonfatal stroke and hospitalization for unstable angina)
10 months (prema-turely stopped – antidrug antibody formation)
∆ 256 %; S (P 5 .02)
51Chapter 6 — Long-Term Cardiovascular Outcomes with PCSK9 Inhibitors
neurocognitive events), with the exception of in-jection site reactions, which were more common with evolocumab (2.1% vs. 1.6%).
NEWERPCSK9INHIBITORS(GENESILENCER)
Fitzgerald et al. reported that inclisiran, a long-acting RNA interference (RNAi) therapeutic inhibi-tor of PCSK9, is safe and effective in the lowering of low-density lipoprotein (LDL) cholesterol among healthy volunteers. The advantage of inclisiran is sustained suppression of PCSK9 and LDL choles-terol for at least 6 months, which allows for twice-yearly administration.
In the recently published ORION-1 phase II, mul-ticentre, double-blind study, multiple-ascending-dose
2.18%
0.95%
0
1
2
3
4
Standard care Evolocumba 120 mg Q2W or 420mg QM + standard care
Car
dio
vasc
ula
r ev
ent
rate
at
1 ye
ar (
%)
Hazard ratio 0.47(96% confidence interval 0.28–0.78) (P=0.003)
Figure6-7. Tolerability profile in the ODYSSEY LONG-TERM trial: adverse events of interest (AE, adverse events). (Based on data presented in: Robinson, J. G., et al. (2015). Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. New England Journal of Medicine, 372,1489–1499.)
Figure6-6. Effect of evolocumab on cardiovascular outcomes in a pooled analysis of the OSLER-1 and OSLER-2 trials. (Based on data presented in: Sabatine et al. (2015). Efficacy and safety of evolocumab in reducing lipids and cardiovascular events. New England Journal of Medicine, 372, 1500–1509.)
TABLE 6-4 SUMMARYOFADVERSEEVENT(AE)DATA(%)FOREVOLOCUMABINOSLERSTUDY
OSLER EvolocumabStandard of Care
Any adverse event 69 65Adverse event leading to
discontinuation2.4 NA
Injection site reactions 4.3 NAMuscle-related AE 6.4 6.0
81.0%
7.2%10.1%
5.9% 5.4% 4.2%
82.5%
5.8%9.5%
4.2% 2.9% 4.4%
0
20
40
60
80
100
Any AE AE leading todiscontinuation
General allergicreaction
Local injectionsite reaction
Myalgia Neurologicevent
% p
atie
nts
Alirocumab (n=1550)
Placebo (n=788)
of care in OSLER vs. evolocumab, and placebo in ODYSSEY LONG TERM versus alirocumab)24,25.
In FOURIER trial, there was no significant differ-ence between the study groups with regard to adverse events (including new-onset diabetes and

52 SECTION II — Preventive Cardiology
statin, people at high cardiovascular risk who are not at their LDL cholesterol goal.
9. Inclisiran, RNAi of PCSK9, is relatively safe and effective in reducing LDL cholesterol.
trial of inclisiran administered as a subcutaneous injection in patients at high risk for CVD who had elevated LDL cholesterol levels26. Patients were ran-domly assigned to receive a single dose of placebo or 200, 300 or 500 mg of inclisiran or two doses (at days 1 and 90) of placebo or 100, 200 or 300 mg of inclisiran. A total of 501 patients underwent randomization. Patients who received inclisiran had dose-dependent reductions in PCSK9 and LDL cholesterol levels. At day 180, the least-squares mean reductions in LDL cholesterol levels were 27.9%–41.9% after a single dose of inclisiran and 35.5%–52.6% after two doses (P , .001 for all com-parisons vs. placebo). The two-dose 300-mg incli-siran regimen produced the greatest reduction in LDL cholesterol levels: 48% of the patients who received the regimen had an LDL cholesterol level below 50 mg per decilitre (1.3 mmol per litre) at day 180. At day 240, PCSK9 and LDL cholesterol levels remained significantly lower than at baseline in association with all inclisiran regimens. Serious adverse events occurred in 11% of the patients who received inclisiran and in 8% of the patients who received placebo. Injection site reactions oc-curred in 5% of the patients who received injec-tions of inclisiran.
SUMMARY(KEYPOINTS)
1. Familial hypercholesterolaemia is the most com-mon genetic disorder in the world and yet .99% of patients worldwide never receive the diagnosis that would facilitate intensive therapy to reduce their LDL cholesterol.
2. Reducing the activity or expression of PCSK9 in-creases the number of LDL receptors, which re-duces circulating LDL cholesterol.
3. PCSK9 inhibitors reduced LDL cholesterol by .50% in randomized trials in patients with hypercholes-terolaemia.
4. Preliminary data from the ODYSSEY study sug-gest a reduced frequency of adverse cardiovascu-lar outcomes associated with a PCSK9 inhibitor in patients with hypercholesterolaemia.
5. PCSK9 inhibitors have been generally well toler-ated in clinical trials.
6. The main side effects associated with these agents are injection site reactions, which is unsurprising for an injectable treatment.
7. The tolerability and safety profiles of these agents so far support long-term administration for life-long conditions such as hypercholesterolaemia.
8. Current indications of PCSK9 inhibitors: People with familial hypercholesterolaemia, people with
RefeRences
1. Centers for Disease Control and Prevention, Heart Dis-ease facts and statistics (2013). (2015). Deaths: Final data for 2013. National Vital Statistics Report, 64(2).
2. Nordestgaard, B. G., Chapman, M. J., Humphries, S. E., Ginsberg, H. N., Masana, L., & Descamps, O. S., et al. (2013). Familial hypercholesterolaemia is underdiag-nosed and undertreated in the general population: Guidance for clinicians to prevent coronary heart dis-ease: Consensus statement of the European Atheroscle-rosis Society. European Heart Journal, 34, 3478–3490a.
3. Karalis, D. G., Victor, B., Ahedor, L., & Liu, L. (2012). Use of lipid-lowering medications and the likelihood of achieving optimal LDL cholesterol goals in coronary artery disease patients. Cholesterol, 2012, 861924.
4. Bangalore, S., Breazna, A., DeMicco, D. A., Wun, C. C., & Messerli, F. H. (2015). Visit-to-visit low-density lipo-protein cholesterol variability and risk of cardiovascu-lar outcomes: Insights from the TNT Trial. Journal of the American College of Cardiology, 65, 1539–1548.
5. Bandolier. Patient compliance with statins. http://www.bandolier.org.uk/booth/cardiac/patcomp.html Accessed 20th October 2017
6. Mann, D. M., Glazer, N. L., Winter, M., Paasche-Or-low, M. K., Muntner, P., Shimbo, D., et al. (2013). A pilot study identifying statin nonadherence with visit-to-visit variability of low-density lipoprotein choles-terol. American Journal of Cardiology, 111, 1437–1442.
7. Hopewell, J. C., Reith, C., & Armitage, J. (2014). Phar-macogenomics of statin therapy: Any new insights in efficacy or safety? Current Opinion in Lipidology, 25, 438–445.
8. Go, G. W., & Mani, A. (2012). Low-density lipoprotein receptor (LDLR) family orchestrates cholesterol homeostasis. Yale Journal of Biology and Medicine, 85, 19–28.
9. Cohen, J. C., Boerwinkle, E., Mosley, T. H. Jr., & Hobbs, H. H. (2006). Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. New England Journal of Medicine, 354, 1264–1272.
10. Benn, M., Nordestgaard, B. G., Grande, P., Schnohr, P., & Tybjaerg-Hansen, A. (2010). PCSK9 R46L, low-den-sity lipoprotein cholesterol levels, and risk of ischemic heart disease: 3 independent studies and meta-analy-ses. Journal of the American College of Cardiology, 55, 2833–2842.
11. De Castro-Orós, I., Pocoví, M., & Civeira, F. (2010). The genetic basis of familial hypercholesterolemia: Inheri-tance, linkage, and mutations. Application of Clinical Genetics, 3, 53–64.
12. Blom, D. J., Hala, T., Bolognese, M., Lillestol, M. J., Toth, P. D., Burgess, L., et al. (2014). A 52-week placebo-controlled trial of evolocumab in hyperlipid-emia. New England Journal of Medicine, 370, 1809–1819.

53Chapter 6 — Long-Term Cardiovascular Outcomes with PCSK9 Inhibitors
13. Roth, E. M., Taskinen, M. R., Ginsberg, H. N., Kastelein, J. J., Colhoun, H. M., Robinson, J. G., et al. (2014). Monotherapy with the PCSK9 inhibitor alirocumab versus ezetimibe in patients with hypercholesterol-emia: Results of a 24 week, double-blind, randomized Phase 3 trial. International Journal of Cardiology, 176, 55–61.
14. Raal, F. J., Honarpour, N., Blom, D. J., Hovingh, G. K., Xu, F., Scott, R., et al. (2014). Inhibition of PCSK9 with evo-locumab in homozygous familial hypercholesterolae-mia (TESLA Part B): A randomised, double-blind, pla-cebo-controlled trial. Lancet, 385(9965), 341–350.
15. Raal, F. J., Stein, E. A., Dufour, R., Turner, T., Civeira, F., Burgess, L., et al. (2014). PCSK9 inhibition with evo-locumab (AMG 145) in heterozygous familial hyper-cholesterolaemia (RUTHERFORD-2): A randomised, double-blind, placebo-controlled trial. Lancet, 385(9965), 331–340.
16. Robinson, J. G., Nedergaard, B. S., Rogers, W. J., Fi-alkow, J., Neutel, J. M., Ramstad, D., et al. (2014). Effect of evolocumab or ezetimibe added to moderate- or high-intensity statin therapy on LDL-C lowering in patients with hypercholesterolemia: The LAPLACE-2 randomized clinical trial. JAMA, 311, 1870–1882.
17. Stroes, E., Colquhoun, D., Sullivan, D., Civeira, F., Ro-senson, R. S., Watts, G. F., et al. (2014). Anti-PCSK9 antibody effectively lowers cholesterol in patients with statin intolerance: The GAUSS-2 randomized, placebo-controlled phase 3 clinical trial of evolocumab. Journal of the American College of Cardiology, 63, 2541–2548.
18. Koren, M. J., Lundqvist, P., Bolognese, M., Neutel, J. M., Monsalvo, M. L., Yang, J., et al. (2014). Anti-PCSK9 monotherapy for hypercholesterolemia: The MEN-DEL-2 randomized, controlled phase III clinical trial of evolocumab. Journal of the American College of Cardiol-ogy, 63, 2531–2540.
19. Cannon, C. P., Cariou, B., Blom, D., McKenney, J. M., Lorenzato, C., Pordy, R., et al. (2015). Efficacy and safety
of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolemia on maxi-mal tolerated daily statin: Results from the ODYSSEY COMBO II study. European Heart Journal, 36(19), 1186–1194.
20. Kastelein JJ, Ginsberg HN, Langslet G, et al. (2015). ODYSSEY FH I and FH II: 78 week results with ali-rocumab treatment in 735 patients with heterozygous familial hypercholesterolaemia. Eur Heart J, 36, 2996–3003.
21. Stoekenbroek, R. M., Kastelein, J. J., & Huijgen, R. (2015). PCSK9 inhibition: The way forward in the treatment of dyslipidemia. BMC Medicine, 13, 258. doi:10.1186/s12916-015-0503-4
22. Sabatine, M. S., Giugliano, R. P., Keech, A. C., Honar-pour, N., Wiviott, S. D., Murphy, S. A., et al. (2017). Evolocumab and clinical outcomes in patients with cardiovascular disease. New England Journal of Medicine, 376, 1713–1722.
23. Ridker, P. M., Revkin, J., Amarenco, P., Brunell, R., Curto, M., Civeira, F., et al (2017). Cardiovascular effi-cacy and safety of bococizumab in high-risk patients. New England Journal of Medicine, 376, 1527–1539.
24. Sabatine, M. S., Giugliano, R. P., Wiviott, S. D., Raal, F. J., Blom, D. J., Robinson, J., et al. (2015). Efficacy and safety of evolocumab in reducing lipids and cardiovas-cular events. New England Journal of Medicine, 372, 1500–1509.
25. Robinson, J. G., Farnier, M., Krempf, M., Bergeron, J., Luc, G., Averna, M., et al. (2015). Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. New England Journal of Medicine, 372, 1489–1499.
26. Ray, K. K., Landmesser, U., Leiter, L. A., Kallend, D., Dufour, R., Karakas, M., et al. (2017). Inclisiran in pa-tients at high cardiovascular risk with elevated LDL cholesterol. New England Journal of Medicine, 376, 1430–1440.






























