Embed Size (px)
Citation preview

Eleni Korompoki PhDFilippos T Filippidis
PhDPeter B Nielsen PhDAngela Del Giudice MDGregory Y H Lip MDJoji B Kuramatsu MDHagen B Huttner PhDJiming Fang PhDSam Schulman PhDJoan Martiacute-Fagravebregas PhDCeline S Gathier MDAnand Viswanathan PhDAlessandro Biffi MDDaniela Poli MDChristian Weimar MDUwe Malzahn PhDPeter Heuschmann MDRoland Veltkamp MD
Correspondence toDr Veltkamprveltkampimperialacuk
Supplemental dataat Neurologyorg
Long-term antithrombotic treatment inintracranial hemorrhage survivors withatrial fibrillation
ABSTRACT
Objective To perform a systematic review and meta-analysis of studies reporting recurrent intra-cranial hemorrhage (ICH) and ischemic stroke (IS) in ICH survivors with atrial fibrillation (AF) duringlong-term follow-up
Methods A comprehensive literature search including MEDLINE EMBASE Cochrane libraryclinical trials registry was performed following the Preferred Reporting Items for Systematic Re-views and Meta-Analyses (PRISMA) statement We considered studies capturing outcome events(ICH recurrence and IS) for $3 months and treatment exposure to vitamin K antagonists (VKAs)antiplatelet agents (APAs) or no antithrombotic medication (no-ATM) Corresponding authorsprovided aggregate data for IS and ICH recurrence rate between 6 weeks after the event and1 year of follow-up for each treatment exposure Meta-analyses of pooled rate ratios (RRs) wereconducted with the inverse variance method
Results Seventeen articles met inclusion criteria Seven observational studies enrolling 2452patients were included in the meta-analysis Pooled RR estimates for IS were lower for VKAs com-pared to APAs (RR 5 045 95 confidence interval [CI] 027ndash074 p 5 0002) and no-ATM(RR 5 047 95 CI 029ndash077 p 5 0002) Pooled RR estimates for ICH recurrence were notsignificantly increased across treatment groups (VKA vs APA RR 5 134 95 CI 079ndash230p 5 028 VKA vs no-ATM RR 5 093 95 CI 045ndash190 p 5 084)
Conclusions In observational studies anticoagulation with VKA is associated with a lower rate ofIS than APA or no-ATM without increasing ICH recurrence significantly A randomized controlledtrial is needed to determine the net clinical benefit of anticoagulation in ICH survivors with AFNeurologyreg 201789687ndash696
GLOSSARYAF 5 atrial fibrillation APA 5 antiplatelet agent APACHE-AF 5 Apixaban Versus Antiplatelet Drugs or no AntithromboticDrugs After Anticoagulation-Associated Intracerebral Haemorrhage in PatientsWith Atrial FibrillationATM5 antithromboticmedication AVERROES 5 A Phase III Study of Apixaban in Patients With Atrial Fibrillation CI 5 confidence intervalDOAC 5 direct oral anticoagulant ICD-10 5 International Classification of Diseases 10th revision ICH 5 intracranialhemorrhage IS 5 ischemic stroke OAC 5 oral anticoagulant PRISMA 5 Preferred Reporting Items for Systematic Reviewsand Meta-Analyses RR 5 rate ratio VKA 5 vitamin K antagonist
Antithrombotic stroke prevention in patients with previous intracranial hemorrhage (ICH) andatrial fibrillation (AF) is challenging because ICH related to oral anticoagulant (OAC-ICH) isthe most lethal complication of long-term anticoagulation and OACs are contraindicated afterICH1 In this setting clinicians have to weigh the risk of thromboembolism against the risk ofanother ICH Thromboembolic risk in patients with AF can be estimated with the CHA2DS2VAScscore2 In contrast there is only limited evidence on factors influencing the risk of recurrent
These authors contributed equally to this work
From the Division of Brain Sciences (EK ADG RV) Department of Stroke Medicine and Department of Primary Care and Public Health(FTF) Imperial College London UK Aalborg Thrombosis Research Unit (PBN GYHL) Department of Clinical Medicine Faculty ofMedicine Aalborg University Denmark Institute of Cardiovascular Sciences (GYHL) University of Birmingham UK Department ofNeurology (JBK HBH) University of Erlangen-Nuremberg Erlangen Germany Institute for Clinical Evaluative Sciences (JF) TorontoThrombosis and Atherosclerosis Research Institute (SS) Department of Medicine McMaster University Hamilton Ontario Canada Stroke Unit(JM-F) Department of Neurology Hospital de la Santa Creu i Sant Pau IIB-Sant Pau Barcelona Spain Department of Neurology andNeurosurgery (CSG) Brain Center Rudolf Magnus University Medical Center Utrecht the Netherlands Department of Neurology (AV AB)Massachusetts General Hospital Harvard Medical School Boston Thrombosis Center (DP) Careggi Hospital Florence Italy Department ofNeurology (CW) University Hospital of Duisburg-Essen Essen Clinical Trial Center Wuumlrzburg (UM PH) University Hospital Wuumlrzburgand Institute of Clinical Epidemiology and Biometry (PH) Comprehensive Heart Failure Center University Wuumlrzburg Germany
Go to Neurologyorg for full disclosures Funding information and disclosures deemed relevant by the authors if any are provided at the end of the article
copy 2017 American Academy of Neurology 687
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
ICH with and without anticoagulation34 andclinical scores provide only modest help25 Norandomized controlled trial has studied theefficacy and safety of anticoagulation in pa-tients with AF and ICH yet The paucity ofhigh-grade evidence is reflected in clinicalguidelines which refrain from making strongor even any recommendations for stroke pre-vention in patients with ICH and AF67
The latest systematic review of the use ofATM after intracerebral hemorrhage focusedon the risks of recurrent bleeding and throm-boembolic events3 However AF was not theonly indication for ATM and only intracere-bral hemorrhage was considered In the mean-time several large cohort studies have beenpublished that explored antithrombotic therapyresumption after ICH
We performed a systematic review and meta-analysis of studies reporting ischemic stroke (IS)and recurrent ICH in survivors of ICHwith AF
METHODS We performed a systematic review consistent with
Preferred Reporting Items for Systematic Reviews and Meta-
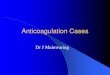
Analyses (PRISMA) guidelines (figure 1) following a pre-
specified protocol8 Our search strategy and data extraction are
described in the e-supplement and table e-1 at Neurologyorg
Exposure and outcome measures To calculate treatment
exposure the beginning of the observation period was set at 6
weeks after the index ICH This 6-week landmark approach has
been used in a large Danish nationwide registry9 and may reduce
selection bias derived from a nonrandomized allocation because
very ill patients or patients at high risk for ICH recurrence could
be considered unsuitable for OAC early after ICH Data were
requested and obtained from the corresponding authors of the
studies because originally published data were not consistent with
our 6-week quarantine period Because treatment exposure was
considered a time-dependent variable a patient could contribute
person-time to each of the groups at different times This approach
allowed us to calculate incidence rates and rate ratios (RRs)
For the purpose of our meta-analysis we considered 3 different
types of ATM exposure vitamin K antagonists (VKAs) antiplatelet
agents (APAs) or no antithrombotic medication (no-ATM) We
also combined the APA and the no-ATM group into a no-VKA
group We assessed 2 primary endpoints IS occurring between 6
weeks and 1 year of follow-up and ICH occurring between 6 weeks
and 1 year of follow-up For each endpoint data on the number of
events and the respective person-time of follow-up in each of the
treatment groups were extracted All investigators were asked to fill
out prespecified tables with aggregate data based on individual data
at study level
Unadjusted incidence rates were calculated for each group
and endpoint as well as the respective incidence RRs for each pair
of treatments Only the first event during the follow-up contrib-
uted to the risk estimate We conducted meta-analyses for the fol-
lowing pairs (1) VKA vs no-VKA (ie APA and no-ATM
combined) (2) VKA vs APA (3) VKA vs no-ATM and (4)
APA vs no-ATM
Finally we calculated crude pooled event rates with associated
95 confidence intervals (CIs) for IS and ICH by pooling the
total number of events (IS and ICH recurrences respectively)
and the respective cumulative follow-up expressed in person-
time across all studies
Risk of bias assessment The quality of the studies was assessedaccording to the Cochrane handbook10 We used funnel plots for
illustration of asymmetry and Egger regression test to get hints for
publication bias For the funnel plot we plotted the standard
error of the natural logarithm of the RR against the RR A value
of p 01 was considered significant for publication bias
Statistical analysis The relative incidence rates of ICH and IS
among the different groups in included studies were expressed as
RR The inverse variance method was used to conduct the meta-
analysis and pooled effects are presented as RR with 95 CI
Expecting considerable heterogeneity among studies because
there was wide variation in study populations and study designs
we used random-effects models for the meta-analysis11
The I2 statistic was calculated to quantify heterogeneity
among included studies as low (30) moderate (30ndash
50) or high (50) Single-variable meta-regression was used
to explore whether mean age sex timing of ATM exposure and
type of hemorrhage (all ICH vs intracerebral hemorrhage only)
were potential sources of significant heterogeneity The lnRR
weighted by inverse variance for each study was considered the
dependent variable Small study effects including publication bias
were assessed with the Egger test and funnel plots
All meta-analyses were performed with the Cochrane Review
Manager 53 software (RevMan53) The Egger test and meta-
regression analyses were conducted with Comprehensive Meta-
Analysis 30 Statistical significance levels were set at 005
RESULTS Seventeen articles 14 full manuscripts and3 conference abstracts12e1e2 of 3455 originally identi-fied citations met our inclusion criteria Among includedstudies 6 were prospective observational13e1e3ndashe6 and11 were retrospective studies91214ndash17e2e7ndashe10 Theindex event was intracerebral hemorrhage in 11studies912ndash1517e2e6ndashe8 and ICH in 6 studies16e1e3ndashe5e10
Regarding the underlying cause 11 studies addressedICH related to ATM914ndash17e1e3e6e7e9e11 and 6 studiesaddressed a mixture of spontaneous and posttraumaticICH1213e3e5e6e9 Of all index ICH events 97 occurredin anticoagulated patients 3 were VKA naive Theinclusion criteria and the type of ATM used after theindex event for each study are presented in table e-2
Ten studies were excluded from the meta-analysisbecause of missing data or the absence of a comparisongroup Seven studies were deemed suitable for inclu-sion in the meta-analysis912ndash17 A total of 2452 patients(mean age 76 years 41 female) were eligible Char-acteristics of included studies are presented in table 1
Pooled annual event rates for ICH recurrence andIS by antithrombotic strategy followed after the indexICH are presented in table 2
Publication bias and quality assessmentThe funnel plotsshowed asymmetry suggesting possible publicationbias (figures e-1 and e-2) No small study effects weredetected by Egger test for either IS or ICH recurrence
688 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
in all comparisons All studies had possible selectionbias Overall 71 of studies reported consecutiverecruitment Blinding of outcome assessment was per-formed in only one study Attrition bias was found in29 of studies No funding bias was found in any ofthe included studies Risk of reporting bias was low inall studies because data were provided directly by thecorresponding authors Other potential risks of biasare presented in table e-3
VKAs vs no-VKAs A total of 6 studies compared the ratesof IS and ICH between patients who started a VKA andpatients who did not start a VKA (no-VKA) The pooled
RR of IS was significantly lower for VKA vs no-VKApatients (RR 5 046 95 CI 029 to 072 p 5
00008 I2 5 0) (figure 2A) The rate of recurrentICH was not significantly increased in VKA-treatedcompared to no-VKA patients (pooled RR 5 12395 CI 080 to 187 p5 053 I2 5 0) (figure 3A)
VKAs vs APAs Five studies provided data for compar-ison of VKAs and APAs The pooled data showed a sig-nificant decrease in the rate of IS in patients treatedwith VKA vs APA (pooled RR 5 045 95 CI027 to 074 p5 0002 I2 5 0) (figure 2B) Againthe rate of ICH recurrence was not significantly higher
Figure 1 PRISMA flowchart Study selection
AF 5 atrial fibrillation PRISMA 5 Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Neurology 89 August 15 2017 689
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
for VKA than for APA (pooled RR 5 134 95 CI079 to 230 p 5 028 I2 5 0) (figure 3B)
VKAs vs no-ATM Five studies compared the rate of ISand ICH in patients started on VKA vs no-ATM Thepooled rate for IS was significantly lower in VKA-treatedpatients (pooled RR 5 047 95 CI 029ndash077 p 50002 I25 0) (figure 2C) The comparison of the rateof ICH recurrence revealed no significant differencebetween VKA and no-ATM (pooled RR 5 093 95CI 045 to 190 p 5 084 I2 5 20) (figure 3C)
APAs vs no-ATM Five studies compared incidencerates in APA vs no-ATM The pooled RR estimatedid not differ significantly for IS (RR 5 106 95CI 072ndash154 p 5 078 I2 5 0) or for ICHrecurrence (RR5 077 95CI 047ndash125 p5 028I2 5 0) (figures 2D and 3D respectively)
Assessing the relationship between study-level covariates
and effect size Meta-regression analyses exploring theimpact of mean age sex timing of ATM exposureand type of ICH showed no statistically significantresults across all groups (table e-4)
DISCUSSION This meta-analysis compared the ratesof ICH recurrence and IS after different antith-rombotic therapies in VKA-associated ICH survivorswith AF Our main findings are that (1) treatmentwith VKA was associated with a significantly lowerrate of IS compared to no anticoagulation (2) APAconferred no benefit for prevention of IS over noantithrombotic therapy and (3) anticoagulated pa-tients did not have a statistically significantly higherrate of ICH recurrence
AF is present in a substantial proportion of ICHsurvivors with a prevalence of 12 to 14 innational registries and 30 in tertiary stroke cen-ters1819 There is limited evidence on whether ATMshould be started or withheld in this context20 ICH isthe most feared complication of antithrombotic ther-apy and the risk of ICH is higher in ICH survivors(3ndash5 per year)21e5e6e9 compared to patients with-out previous ICH (03ndash25 per year)22ndash24 Thepaucity of evidence for efficacy and safety results invariation in restarting antithrombotic drugs in ICHsurvivors ranging from 11 to 45 across differenthealth systems25 For example although patients ofAsian ethnicity have a higher risk of ICH than whitepatients a nationwide survey in Japan reported thatthe majority of physicians support the resumption ofOACs after ICH26 Our meta-analysis shows that pre-scribing VKA after VKA-associated ICH is associatedwith a reduction of IS by 45 to 47 compared toAPA or no-ATM therapy This effect size is similar tothat in patients with AF without previous ICH27 Ourresults are supported by additional studies suggestingthat ICH survivors with AF who do not start OACtreatment are at high risk of IS and mortality both ofwhich are significantly reduced by VKA915
Table 2 Pooled annual event rates for ICH recurrence and IS in differenttreatment strategies expressed as pooled event rates with 95 CI
IS event rate(95 CI)
ICH recurrenceevent rate (95 CI)
VKA 32 (20ndash49) 46 (31ndash66)
Antiplatelets 95 (73ndash120) 37 (25ndash54)
No antithrombotics 61 (49ndash76) 42 (32ndash55)
No VKA(antiplatelets or no antithrombotics)
73 (62ndash85) 40 (32ndash50)
Abbreviations CI 5 confidence interval ICH 5 intracranial hemorrhage IS 5 ischemicstroke VKA 5 vitamin K antagonist
Table 1 Characteristics of the studies included in the meta-analysis
Study Patients n Type of hemorrhage Comparison groupsAge mean(SD) y
Female
CHADS2median(IQR)
FUmedianmo
Time intervalto resumptiona
median (IQR)
Gathier et al14 18 VKA-associatedintracerebral hemorrhage
VKA vs APA vsno-ATM
745 (10$6) 39 2 (1ndash3) 32 21 (9ndash35) d
Kuramatsuet al15
566 VKA-associatedintracerebral hemorrhage
Warfarin (VKA) vs nowarfarin (no-VKA)
75 39 2 12 32 (20ndash69) d
Majeed et al16 84 VKA-associated ICH Warfarin (VKA) vs nowarfarin (no-VKA)
75 (9) 33 2 (2ndash4) 17 92 (56ndash34) wk
Nielsen et al9 1545 VKA-associated ICH OAC vs APA vsno-ATM
78 38 2 12 34 d
Stamplecoskiet al12
199 Intracerebral hemorrhage(57 VKA associated)
Warfarin (VKA) vs nowarfarin (no-VKA)
804 (69) 54 4 (3ndash4) 12 24 (12ndash83) d
Vidal-Jordanaet al17
25 VKA-associatedintracerebral hemorrhage
VKA vs APA 752 (4) 40 2 (1ndash4) 55 NR
Viswanathanet al13
15 Spontaneous intracerebralhemorrhage
APA vs no- APA 736 (89) 47 2 (1ndash3) 32 NR
Abbreviations APA5 antiplatelet agent ATM5 antithrombotic medication FU5 follow-up ICH5 intracranial hemorrhage IQR5 interquartile range NR5
not reported OAC 5 oral anticoagulant VKA 5 vitamin K antagonista Reflects time to treatment resumption among individuals who resumed treatment
690 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
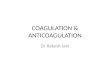
Figure 2 Pooled RR meta-analyses for IS that occurred between 6 weeks and 1 year of follow-up afterexposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval IS 5 ischemic stroke IV 5 inverse variance RR 5 rate ratio VKA 5
vitamin K antagonist
Neurology 89 August 15 2017 691
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 3 Pooled RRmeta-analyses for ICH recurrence that occurred between 6 weeks and 1 year of follow-upafter exposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval ICH 5 intracranial hemorrhage IV5 inverse variance RR 5 rate ratioVKA 5 vitamin K antagonist
692 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reinitiation of warfarin in Taiwanese ICH survivorswith AF was beneficial One study modeling risks andbenefits calculated a net benefit of VKA for Asianpatients with ICH with a CHA2DS2-VASc score$6 but this threshold was likely to be lower withdirect OACs (DOACs)28 In our analysis whichincluded mainly white patients with ICH the medianCHADS2 score was 2 suggesting that starting OACafter ICH may be beneficial with only moderatethromboembolic risk
We found no significantly increased risk for recur-rent ICH with VKA although the point estimate forthe pooled RR was 23 to 32 higher compared tono-VKA and no-ATM Previous research showed thatICH survivors carry a significant risk of recurrentICHe5e7e8 whereas studies found no increased riskof ICH recurrencee10 when they were treated withanticoagulants after the index event Only earlyresumption of VKAs after warfarin-associated ICHincreased the risk of recurrent ICH16 A recent Swed-ish nationwide cohort study suggests that anticoagu-lant treatment may be initiated 7 to 8 weeks afterICH in intracerebral hemorrhage survivors with AFto balance benefit from treatment against the risk ofrebleeding29 In our meta-regression analysis the tim-ing of resumption failed to explain the lack of a sig-nificant difference for recurrent ICH betweenanticoagulated and nonanticoagulated patients butearly recurrent bleeding events were not captured inour study design
OAC has a net clinical benefit in patients with AFwithout ICH30 Considering the significant decreasein the rate of IS with anticoagulants a treatmentoption that provides a better safety profile thanVKA may provide a net clinical benefit also topatients with ICH DOACs have a favorable risk-benefit profile compared to VKA resulting in a reduc-tion in stroke and mortality31 In particular DOACsare uniformly associated with a 50 reduced risk ofICH compared to VKA32 Limited information froma recent study based on national Danish registriessupports this assumption33 Moreover apixaban sig-nificantly reduced the risk of stroke and systemicembolism compared to aspirin without increasingthe risk of ICH in A Phase III Study of Apixabanin Patients With Atrial Fibrillation (AVERROES)34
Therefore DOACs could be a better alternative forpatients with ICH and AF The ongoing ApixabanVersus Antiplatelet Drugs or no AntithromboticDrugs After Anticoagulation-Associated IntracerebralHaemorrhage in Patients With Atrial Fibrillation(APACHE-AF) pilot study (ClinicalTrialsgovNCT02565693) addresses stroke prevention withDOACs in ICH survivors with AF Nonpharmaco-logic prevention strategies including left atrialappendage occlusion could be an alternative but
the evidence for this intervention in ICH survivorswith AF is limited13536
In addition to relative risks decision making fora specific antithrombotic therapy has to take the abso-lute risks for ischemic and hemorrhagic events intoaccount A previous meta-analysis reported an annualrisk of recurrent intracerebral hemorrhage of 13 to744 whereas a prospective cohort study of patientswith AF on VKA after ICH reported an ICH recur-rence rate of 185 per person-year and no ISe5 In ourstudy VKA users had a 04 to 09 higher pooledannual rate of ICH recurrence compared to the othertreatment groups On the contrary the pooled annualevent rate for IS was much lower in patients on VKA(32 per 100 patient-years) compared to the othertreatment groups (APA 95 per 100 patient-yearsno-ATM 61 per 100 patient-years) Although thesedata suggest a reduction of combined ischemic andhemorrhagic stroke event rates by VKA they do notaccount for the different mortality and morbidity re-sulting from these different types of stroke
Current American Heart Association guidelinesrecommend that APA monotherapy after any ICHmight be considered and can be a reasonable alterna-tive in patients with lobar hemorrhage in whomOAC should be avoided6 The findings of the presentmeta-analysis do not support the use of APA for ISprevention because no effect on prevention of throm-boembolic events was observed in patients with AFand ICH Although older research found a smallerbleeding risk on APAs compared to VKAs37 the rateof ICH on aspirin was similar to that of well-managedVKAs38 or DOACs34 However the risk-benefit ratioof APA in ICH survivors with AF was unclear Thecurrent analysis suggests that APAs do not increasethe risk of ICH recurrence compared to VKAs or no-ATM
Our systematic review and meta-analysis wasbased on a comprehensive search strategy that aimedto provide pooled estimates for IS and ICH recur-rence in ICH survivors with AF after different preven-tion strategies Thus we can anticipate a low rate ofunderdetection An important limitation of this largemeta-analysis is the limited data quality of the mostlyretrospective studies For example 3 studies relied oncohorts of patients derived from large national regis-tries that use ICD-10 codes for medical diagnosisand Anatomical Therapeutic Chemical classificationsystem codes to identify ATM Because some deathsmay be due to undiagnosed stroke and some minorstrokes may have remained undetected the risk ofIS may be underreported Using a 6-week landmarkapproach we did not take into account bleeding com-plications related to the index ICH that may havebeen misclassified as ICH recurrences Likewise itis uncertain how many of the early recurrences were
Neurology 89 August 15 2017 693
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
truly new events or just an extension of the initialbleeding site9 The included studies are highly proneto selection bias and confounding by indicationbecause treating physicians may have avoided theuse of VKAs in patients perceived to be at higher riskof recurrence Hence unmeasured selection bias islikely in that we were unable to calculate adjustedincidence RRs because individual patient data werenot available in all studies We summarized aggre-gated treatment group differences (baseline character-istics and comorbidities) (table e-5) for each studythat may facilitate the interpretation of the results(table e-6) As previously shown baseline adjustmentin the setting of time-dependent exposure of treat-ment regimens only marginally affects outcomes asso-ciated with treatment9 This may indicate that otherreasons (besides the measure and included variables)have affected the decision of resuming OAC treat-ment This highlights the importance of meticulousinterpretation of the associations because indicationbias was likely present in all of the included studiesAnother limitation is that we did not have informationon either the time in therapeutic range for patientstaking VKAs or the quality of blood pressure control39
We also did not have data on dropout and rates anddirections of switch between different antithrombotictreatment strategies The number of studies includedin the meta-analysis was small therefore meta-regression and publication bias assessments may havebeen underpowered and should be interpreted withcaution Our study focused on IS and ICH as the mainoutcome events This approach may not provide thefull picture of outcome events and other factors affect-ing the net clinical benefit The 2 largest includedstudies showed a significant decrease of mortality inpatients treated with VKAs915 Because we censoredpatients after either IS or ICH we did not capturepotential multiple outcome events in individual pa-tients although ICH and IS are competing riskAnother limitation is that further subgroup analysesin terms of risk factors for ICH recurrence such aslobar vs deep hemorrhage topography leukoaraiosisand cerebral microbleed burden were not feasiblebecause this information was missing in several studiesIn addition comorbidities apart from AF (eg coro-nary artery disease) indicating the use of antiplateletswere not addressed
This meta-analysis of antithrombotic treatment inVKA-associated ICH survivors with AF suggests thatanticoagulation with VKA is associated with a lowerrate of IS compared to other or no antithromboticswithout causing a major increase of the risk of ICHrecurrence whereas antiplatelets fail to prevent ISBecause of the limitations of observational studiesa randomized controlled trial of antithrombotictherapy preferably with DOACs used as the
anticoagulants is needed to better guide decision mak-ing for antithrombotic therapy in patients with ICHand AF
AUTHOR CONTRIBUTIONSEleni Korompoki study concept data collection drafting and critical revi-
sion of manuscript Filippos T Filippidis study concept statistical analysis
data collection drafting and critical revision of manuscript Peter B Nielsen
study concept data collection and critical revision of manuscript
Angela Del Giudice Gregory Y Lip Joji Kuramatsu Hagen Huttner
Jiming Fang Sam Schulman Joan Martiacute-Fagravebregas Celine S Gathier
Anand Viswanathan Alessandro Biffi Daniela Poli and Christian
Weimar data collection and critical revision of manuscript Uwe
Malzahn and Peter Heuschmann critical review of manuscript Roland
Veltkamp study concept and financial support drafting and critical
revision of manuscript All authors have read and approved the final form
of the manuscript and have agreed to conditions noted on the authorship
agreement The principal author has taken full responsibility for the data
the analyses and the interpretation and the conduct of the research The
statistical analysis has been contacted by Dr Filippidis (Department of
Primary Care and Public Health Imperial College London UK) All
authors had full access to all the data in the study and had final respon-
sibility for the decision to submit for publication Contributor Torben
Bjerregaard Larsen his institution has received payment for enrolling trial
participants from Janssen Scientific Affairs LLC and Boehringer Ingelheim
and he has been on the speaker bureaus for Bayer BMSPfizer Roche
Diagnostics Boehringer Ingelheim and Takeda Pharma
ACKNOWLEDGMENTContributor Torben Bjerregaard Larsen Aalborg University Hospital
Department of Cardiology Aalborg Thrombosis Research Unit Denmark
(data collection)
STUDY FUNDINGSupported by Imperial College London St Maryrsquos development fund
and National Institute for Health Research Imperial Biomedical Research
Centre The sponsor of the study had no role in study design data
collection data analysis data interpretation or writing of the report
Celine S Gathier was supported by the Dutch Heart Foundation grant
2009B046 Joan Martiacute-Fagravebregas was supported by the Spanish Ministry
of Health-Instituto de Salud Carlos III Redes temaacuteticas de Investigacioacuten
Cooperativa INVICTUS RD01200140002 and Fondo Europeo de
Desarrollo Regional Jiming Fang the Ontario Stroke Registry is funded
by the Canadian Stroke Network (CSN) and the Ontario Ministry of
Health and Long-Term Care (MOHLTC) This study was supported by
the Institute for Clinical Evaluative Sciences (ICES) which is funded by
an annual grant from the Ontario MOHLTC The opinions results and
conclusions reported in this paper are those of the authors and are inde-
pendent from the funding sources No endorsement by ICES or the
Ontario MOHLTC is intended or should be inferred
DISCLOSUREE Korompoki and F Filippidis report no disclosures relevant to the man-
uscript P Nielsen speaker for Boehringer Ingelheim consultant for
Bayer Pharma AS and BMSPfizer unrestricted research grant from
BMSPfizer A Del Giudice reports no disclosures relevant to the man-
uscript G Lip consultant for BayerJanssen BMSPfizer Biotronik
Medtronic Boehringer Ingelheim Microlife and Daiichi-Sankyo
speaker for Bayer BMSPfizer Medtronic Boehringer Ingelheim Micro-
life Roche and Daiichi-Sankyo J Kuramatsu reports no conflicts of
interest related to manuscript Unrelated potential conflicts of interest
travel grants from EMCools Otsuka and Boehringer Ingelheim and
speaker honoraria from Otsuka H Huttner reports no conflicts of inter-
est related to manuscript Unrelated potential conflicts of interest consul-
ting speaker honoraria and research support from Boehringer Ingelheim
Pfizer Biogen Medtronic and Novartis J Fang reports no disclosures
relevant to the manuscript S Schulman reports no conflicts of interest
related to manuscript Unrelated potential conflicts of interest honoraria
research support from Baxter Bayer Boehringer Ingelheim Daichii
694 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Sankyo Octapharma and Sanofi J Martiacute-Fagravebregas C Gathier
A Viswanathan A Biffi D Poli C Weimar and U Malzahn report
no disclosures relevant to the manuscript P Heuschmann research
grants from BMBF European Union Chariteacute Berlin Chamber of Physi-
cians German Parkinson Society University Hospital Wuumlrzburg
Robert-Koch-Institute German Heart Foundation Chariteacutendash
Universitaumltsmedizin Berlin (MonDAFIS unrestricted research grant to
Chariteacute from Bayer) University Goumlttingen (FIND-AFrandomized
unrestricted research grant to University Goumlttingen from Boehringer
Ingelheim) and University Hospital Heidelberg (RASUNOA-prime
unrestricted research grant to University Hospital Heidelberg from Bayer
BMS Boehringer Daiichi Sankyo) R Veltkamp consulting speaker
honoraria research support from Bayer Boehringer Daiichi Sankyo
BMS Pfizer Portola Biogen Amgen Morphosys Medtronic and
Apoplex Medical Technologies Go to Neurologyorg for full disclosures
Received December 29 2016 Accepted in final form May 23 2017
REFERENCES1 Camm AJ Lip GY De Caterina R et al 2012 Focused
update of the ESC guidelines for the management of atrial
fibrillation an update of the 2010 ESC guidelines for the
management of atrial fibrillation developed with the spe-
cial contribution of the European Heart Rhythm Associa-
tion Eur Heart J 2012332719ndash2747
2 Olesen JB Lip GY Hansen ML et al Validation of risk
stratification schemes for predicting stroke and thrombo-
embolism in patients with atrial fibrillation nationwide
cohort study BMJ 2011342d124
3 Flynn RW MacDonald TM Murray GD Doney AS
Systematic review of observational research studying the
long-term use of antithrombotic medicines following
intracerebral hemorrhage Cardiovasc Ther 201028
177ndash184
4 Poon MT Fonville AF Al-Shahi Salman R Long-term
prognosis after intracerebral haemorrhage systematic
review and meta-analysis J Neurol Neurosurg Psychiatry
201485660ndash667
5 Pisters R Lane DA Nieuwlaat R de Vos CB Crijns HJ
Lip GY A novel user-friendly score (HAS-BLED) to assess
1-year risk of major bleeding in patients with atrial fibrilla-
tion the Euro Heart Survey Chest 20101381093ndash1100
6 Hemphill JC III Greenberg SM Anderson CS et al
Guidelines for the management of spontaneous intracere-
bral hemorrhage a guideline for healthcare professionals
from the American Heart AssociationAmerican Stroke
Association Stroke 2015462032ndash2060
7 Steiner T Al-Shahi Salman R Beer R et al European
Stroke Organisation (ESO) guidelines for the management
of spontaneous intracerebral hemorrhage Int J Stroke
20149840ndash855
8 Liberati A Altman DG Tetzlaff J et al The PRISMA state-
ment for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions explanation
and elaboration J Clin Epidemiol 200962e1ndashe34
9 Nielsen PB Larsen TB Skjoth F Gorst-Rasmussen A
Rasmussen LH Lip GY Restarting anticoagulant treat-
ment after intracranial haemorrhage in patients with atrial
fibrillation and the impact on recurrent stroke mortality
and bleeding a nationwide cohort study Circulation
2015132517ndash525
10 Higgins JPT Altman DG Assessing Risk of Bias in
Included Studies Chichester Wiley 2008
11 DerSimonian R Laird N Meta-analysis in clinical trials
Control Clin Trials 19867177ndash188
12 Stamplecoski M Fang J Kapral MK Silver FL Long-term
outcomes of elderly patients with intracerebral hemorrhage
and atrial fibrillation Stroke 201445(s1)ATMP103
13 Viswanathan A Rakich SM Engel C et al Antiplatelet use
after intracerebral hemorrhage Neurology 200666206ndash209
14 Gathier CS Algra A Rinkel GJ van der Worp HB Long-
term outcome after anticoagulation-associated intracerebral
haemorrhage with or without restarting antithrombotic
therapy Cerebrovasc Dis 20133633ndash37
15 Kuramatsu JB Gerner ST Schellinger PD et al Antico-
agulant reversal blood pressure levels and anticoagulant
resumption in patients with anticoagulation-related intra-
cerebral hemorrhage JAMA 2015313824ndash836
16 Majeed A Kim YK Roberts RS Holmstrom M Schulman
S Optimal timing of resumption of warfarin after intracranial
hemorrhage Stroke 2010412860ndash2866
17 Vidal-Jordana A Barroeta-Espar I Sainz Pelayo MP
Mateo J Delgado-Mederos R Marti-Fabregas J Intracerebral
hemorrhage in anticoagulated patients what do we do after-
wards [in Spanish] Neurologia 201227136ndash142
18 Horstmann S Rizos T Jenetzky E Gumbinger C Hacke W
Veltkamp R Prevalence of atrial fibrillation in intracerebral
hemorrhage Eur J Neurol 201421570ndash576
19 Andersen KK Olsen TS Dehlendorff C Kammersgaard LP
Hemorrhagic and ischemic strokes compared stroke severity
mortality and risk factors Stroke 2009402068ndash2072
20 Paciaroni M Agnelli G Should oral anticoagulants be
restarted after warfarin-associated cerebral haemorrhage
in patients with atrial fibrillation Thromb Haemost
201411114ndash18
21 Eckman MH Rosand J Knudsen KA Singer DE
Greenberg SM Can patients be anticoagulated after
intracerebral hemorrhage A decision analysis Stroke
2004341710ndash1716
22 Lip GY Andreotti F Fauchier L et al Bleeding risk assess-
ment and management in atrial fibrillation patients a position
document from the European Heart Rhythm Association
endorsed by the European Society of Cardiology Working
Group on Thrombosis Europace 201113723ndash746
23 Goldstein JN Greenberg SM Should anticoagulation be
resumed after intracerebral hemorrhage Cleve Clin J Med
201077791ndash799
24 Molina CA Selim MH The dilemma of resuming anti-
coagulation after intracranial hemorrhage little evidence
facing big fears Stroke 2011423665ndash3666
25 Pasquini M Charidimou A van Asch CJ et al Variation in
restarting antithrombotic drugs at hospital discharge after
intracerebral hemorrhage Stroke 2014452643ndash2648
26 Maeda K Koga M Okada Y et al Nationwide survey of
neuro-specialistsrsquo opinions on anticoagulant therapy after
intracerebral hemorrhage in patients with atrial fibrillation
J Neurol Sci 201231282ndash85
27 Hart RG Pearce LA Aguilar MI Meta-analysis antith-
rombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation Ann Intern Med 2007146
857ndash867
28 Chao TF Liu CJ Liao JN et al Use of oral anticoagulants
for stroke prevention in patients with atrial fibrillation who
have a history of intracranial hemorrhage Circulation
20161331540ndash1547
29 Pennlert J Overholser R Asplund K et al Optimal timing
of anticoagulant treatment after intracerebral hemorrhage
in patients with atrial fibrillation Stroke 201748
314ndash320
Neurology 89 August 15 2017 695
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

ICH with and without anticoagulation34 andclinical scores provide only modest help25 Norandomized controlled trial has studied theefficacy and safety of anticoagulation in pa-tients with AF and ICH yet The paucity ofhigh-grade evidence is reflected in clinicalguidelines which refrain from making strongor even any recommendations for stroke pre-vention in patients with ICH and AF67
The latest systematic review of the use ofATM after intracerebral hemorrhage focusedon the risks of recurrent bleeding and throm-boembolic events3 However AF was not theonly indication for ATM and only intracere-bral hemorrhage was considered In the mean-time several large cohort studies have beenpublished that explored antithrombotic therapyresumption after ICH
We performed a systematic review and meta-analysis of studies reporting ischemic stroke (IS)and recurrent ICH in survivors of ICHwith AF
METHODS We performed a systematic review consistent with
Preferred Reporting Items for Systematic Reviews and Meta-
Analyses (PRISMA) guidelines (figure 1) following a pre-
specified protocol8 Our search strategy and data extraction are
described in the e-supplement and table e-1 at Neurologyorg
Exposure and outcome measures To calculate treatment
exposure the beginning of the observation period was set at 6
weeks after the index ICH This 6-week landmark approach has
been used in a large Danish nationwide registry9 and may reduce
selection bias derived from a nonrandomized allocation because
very ill patients or patients at high risk for ICH recurrence could
be considered unsuitable for OAC early after ICH Data were
requested and obtained from the corresponding authors of the
studies because originally published data were not consistent with
our 6-week quarantine period Because treatment exposure was
considered a time-dependent variable a patient could contribute
person-time to each of the groups at different times This approach
allowed us to calculate incidence rates and rate ratios (RRs)
For the purpose of our meta-analysis we considered 3 different
types of ATM exposure vitamin K antagonists (VKAs) antiplatelet
agents (APAs) or no antithrombotic medication (no-ATM) We
also combined the APA and the no-ATM group into a no-VKA
group We assessed 2 primary endpoints IS occurring between 6
weeks and 1 year of follow-up and ICH occurring between 6 weeks
and 1 year of follow-up For each endpoint data on the number of
events and the respective person-time of follow-up in each of the
treatment groups were extracted All investigators were asked to fill
out prespecified tables with aggregate data based on individual data
at study level
Unadjusted incidence rates were calculated for each group
and endpoint as well as the respective incidence RRs for each pair
of treatments Only the first event during the follow-up contrib-
uted to the risk estimate We conducted meta-analyses for the fol-
lowing pairs (1) VKA vs no-VKA (ie APA and no-ATM
combined) (2) VKA vs APA (3) VKA vs no-ATM and (4)
APA vs no-ATM
Finally we calculated crude pooled event rates with associated
95 confidence intervals (CIs) for IS and ICH by pooling the
total number of events (IS and ICH recurrences respectively)
and the respective cumulative follow-up expressed in person-
time across all studies
Risk of bias assessment The quality of the studies was assessedaccording to the Cochrane handbook10 We used funnel plots for
illustration of asymmetry and Egger regression test to get hints for
publication bias For the funnel plot we plotted the standard
error of the natural logarithm of the RR against the RR A value
of p 01 was considered significant for publication bias
Statistical analysis The relative incidence rates of ICH and IS
among the different groups in included studies were expressed as
RR The inverse variance method was used to conduct the meta-
analysis and pooled effects are presented as RR with 95 CI
Expecting considerable heterogeneity among studies because
there was wide variation in study populations and study designs
we used random-effects models for the meta-analysis11
The I2 statistic was calculated to quantify heterogeneity
among included studies as low (30) moderate (30ndash
50) or high (50) Single-variable meta-regression was used
to explore whether mean age sex timing of ATM exposure and
type of hemorrhage (all ICH vs intracerebral hemorrhage only)
were potential sources of significant heterogeneity The lnRR
weighted by inverse variance for each study was considered the
dependent variable Small study effects including publication bias
were assessed with the Egger test and funnel plots
All meta-analyses were performed with the Cochrane Review
Manager 53 software (RevMan53) The Egger test and meta-
regression analyses were conducted with Comprehensive Meta-
Analysis 30 Statistical significance levels were set at 005
RESULTS Seventeen articles 14 full manuscripts and3 conference abstracts12e1e2 of 3455 originally identi-fied citations met our inclusion criteria Among includedstudies 6 were prospective observational13e1e3ndashe6 and11 were retrospective studies91214ndash17e2e7ndashe10 Theindex event was intracerebral hemorrhage in 11studies912ndash1517e2e6ndashe8 and ICH in 6 studies16e1e3ndashe5e10
Regarding the underlying cause 11 studies addressedICH related to ATM914ndash17e1e3e6e7e9e11 and 6 studiesaddressed a mixture of spontaneous and posttraumaticICH1213e3e5e6e9 Of all index ICH events 97 occurredin anticoagulated patients 3 were VKA naive Theinclusion criteria and the type of ATM used after theindex event for each study are presented in table e-2
Ten studies were excluded from the meta-analysisbecause of missing data or the absence of a comparisongroup Seven studies were deemed suitable for inclu-sion in the meta-analysis912ndash17 A total of 2452 patients(mean age 76 years 41 female) were eligible Char-acteristics of included studies are presented in table 1
Pooled annual event rates for ICH recurrence andIS by antithrombotic strategy followed after the indexICH are presented in table 2
Publication bias and quality assessmentThe funnel plotsshowed asymmetry suggesting possible publicationbias (figures e-1 and e-2) No small study effects weredetected by Egger test for either IS or ICH recurrence
688 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
in all comparisons All studies had possible selectionbias Overall 71 of studies reported consecutiverecruitment Blinding of outcome assessment was per-formed in only one study Attrition bias was found in29 of studies No funding bias was found in any ofthe included studies Risk of reporting bias was low inall studies because data were provided directly by thecorresponding authors Other potential risks of biasare presented in table e-3
VKAs vs no-VKAs A total of 6 studies compared the ratesof IS and ICH between patients who started a VKA andpatients who did not start a VKA (no-VKA) The pooled
RR of IS was significantly lower for VKA vs no-VKApatients (RR 5 046 95 CI 029 to 072 p 5
00008 I2 5 0) (figure 2A) The rate of recurrentICH was not significantly increased in VKA-treatedcompared to no-VKA patients (pooled RR 5 12395 CI 080 to 187 p5 053 I2 5 0) (figure 3A)
VKAs vs APAs Five studies provided data for compar-ison of VKAs and APAs The pooled data showed a sig-nificant decrease in the rate of IS in patients treatedwith VKA vs APA (pooled RR 5 045 95 CI027 to 074 p5 0002 I2 5 0) (figure 2B) Againthe rate of ICH recurrence was not significantly higher
Figure 1 PRISMA flowchart Study selection
AF 5 atrial fibrillation PRISMA 5 Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Neurology 89 August 15 2017 689
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
for VKA than for APA (pooled RR 5 134 95 CI079 to 230 p 5 028 I2 5 0) (figure 3B)
VKAs vs no-ATM Five studies compared the rate of ISand ICH in patients started on VKA vs no-ATM Thepooled rate for IS was significantly lower in VKA-treatedpatients (pooled RR 5 047 95 CI 029ndash077 p 50002 I25 0) (figure 2C) The comparison of the rateof ICH recurrence revealed no significant differencebetween VKA and no-ATM (pooled RR 5 093 95CI 045 to 190 p 5 084 I2 5 20) (figure 3C)
APAs vs no-ATM Five studies compared incidencerates in APA vs no-ATM The pooled RR estimatedid not differ significantly for IS (RR 5 106 95CI 072ndash154 p 5 078 I2 5 0) or for ICHrecurrence (RR5 077 95CI 047ndash125 p5 028I2 5 0) (figures 2D and 3D respectively)
Assessing the relationship between study-level covariates
and effect size Meta-regression analyses exploring theimpact of mean age sex timing of ATM exposureand type of ICH showed no statistically significantresults across all groups (table e-4)
DISCUSSION This meta-analysis compared the ratesof ICH recurrence and IS after different antith-rombotic therapies in VKA-associated ICH survivorswith AF Our main findings are that (1) treatmentwith VKA was associated with a significantly lowerrate of IS compared to no anticoagulation (2) APAconferred no benefit for prevention of IS over noantithrombotic therapy and (3) anticoagulated pa-tients did not have a statistically significantly higherrate of ICH recurrence
AF is present in a substantial proportion of ICHsurvivors with a prevalence of 12 to 14 innational registries and 30 in tertiary stroke cen-ters1819 There is limited evidence on whether ATMshould be started or withheld in this context20 ICH isthe most feared complication of antithrombotic ther-apy and the risk of ICH is higher in ICH survivors(3ndash5 per year)21e5e6e9 compared to patients with-out previous ICH (03ndash25 per year)22ndash24 Thepaucity of evidence for efficacy and safety results invariation in restarting antithrombotic drugs in ICHsurvivors ranging from 11 to 45 across differenthealth systems25 For example although patients ofAsian ethnicity have a higher risk of ICH than whitepatients a nationwide survey in Japan reported thatthe majority of physicians support the resumption ofOACs after ICH26 Our meta-analysis shows that pre-scribing VKA after VKA-associated ICH is associatedwith a reduction of IS by 45 to 47 compared toAPA or no-ATM therapy This effect size is similar tothat in patients with AF without previous ICH27 Ourresults are supported by additional studies suggestingthat ICH survivors with AF who do not start OACtreatment are at high risk of IS and mortality both ofwhich are significantly reduced by VKA915
Table 2 Pooled annual event rates for ICH recurrence and IS in differenttreatment strategies expressed as pooled event rates with 95 CI
IS event rate(95 CI)
ICH recurrenceevent rate (95 CI)
VKA 32 (20ndash49) 46 (31ndash66)
Antiplatelets 95 (73ndash120) 37 (25ndash54)
No antithrombotics 61 (49ndash76) 42 (32ndash55)
No VKA(antiplatelets or no antithrombotics)
73 (62ndash85) 40 (32ndash50)
Abbreviations CI 5 confidence interval ICH 5 intracranial hemorrhage IS 5 ischemicstroke VKA 5 vitamin K antagonist
Table 1 Characteristics of the studies included in the meta-analysis
Study Patients n Type of hemorrhage Comparison groupsAge mean(SD) y
Female
CHADS2median(IQR)
FUmedianmo
Time intervalto resumptiona
median (IQR)
Gathier et al14 18 VKA-associatedintracerebral hemorrhage
VKA vs APA vsno-ATM
745 (10$6) 39 2 (1ndash3) 32 21 (9ndash35) d
Kuramatsuet al15
566 VKA-associatedintracerebral hemorrhage
Warfarin (VKA) vs nowarfarin (no-VKA)
75 39 2 12 32 (20ndash69) d
Majeed et al16 84 VKA-associated ICH Warfarin (VKA) vs nowarfarin (no-VKA)
75 (9) 33 2 (2ndash4) 17 92 (56ndash34) wk
Nielsen et al9 1545 VKA-associated ICH OAC vs APA vsno-ATM
78 38 2 12 34 d
Stamplecoskiet al12
199 Intracerebral hemorrhage(57 VKA associated)
Warfarin (VKA) vs nowarfarin (no-VKA)
804 (69) 54 4 (3ndash4) 12 24 (12ndash83) d
Vidal-Jordanaet al17
25 VKA-associatedintracerebral hemorrhage
VKA vs APA 752 (4) 40 2 (1ndash4) 55 NR
Viswanathanet al13
15 Spontaneous intracerebralhemorrhage
APA vs no- APA 736 (89) 47 2 (1ndash3) 32 NR
Abbreviations APA5 antiplatelet agent ATM5 antithrombotic medication FU5 follow-up ICH5 intracranial hemorrhage IQR5 interquartile range NR5
not reported OAC 5 oral anticoagulant VKA 5 vitamin K antagonista Reflects time to treatment resumption among individuals who resumed treatment
690 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 2 Pooled RR meta-analyses for IS that occurred between 6 weeks and 1 year of follow-up afterexposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval IS 5 ischemic stroke IV 5 inverse variance RR 5 rate ratio VKA 5
vitamin K antagonist
Neurology 89 August 15 2017 691
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 3 Pooled RRmeta-analyses for ICH recurrence that occurred between 6 weeks and 1 year of follow-upafter exposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval ICH 5 intracranial hemorrhage IV5 inverse variance RR 5 rate ratioVKA 5 vitamin K antagonist
692 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reinitiation of warfarin in Taiwanese ICH survivorswith AF was beneficial One study modeling risks andbenefits calculated a net benefit of VKA for Asianpatients with ICH with a CHA2DS2-VASc score$6 but this threshold was likely to be lower withdirect OACs (DOACs)28 In our analysis whichincluded mainly white patients with ICH the medianCHADS2 score was 2 suggesting that starting OACafter ICH may be beneficial with only moderatethromboembolic risk
We found no significantly increased risk for recur-rent ICH with VKA although the point estimate forthe pooled RR was 23 to 32 higher compared tono-VKA and no-ATM Previous research showed thatICH survivors carry a significant risk of recurrentICHe5e7e8 whereas studies found no increased riskof ICH recurrencee10 when they were treated withanticoagulants after the index event Only earlyresumption of VKAs after warfarin-associated ICHincreased the risk of recurrent ICH16 A recent Swed-ish nationwide cohort study suggests that anticoagu-lant treatment may be initiated 7 to 8 weeks afterICH in intracerebral hemorrhage survivors with AFto balance benefit from treatment against the risk ofrebleeding29 In our meta-regression analysis the tim-ing of resumption failed to explain the lack of a sig-nificant difference for recurrent ICH betweenanticoagulated and nonanticoagulated patients butearly recurrent bleeding events were not captured inour study design
OAC has a net clinical benefit in patients with AFwithout ICH30 Considering the significant decreasein the rate of IS with anticoagulants a treatmentoption that provides a better safety profile thanVKA may provide a net clinical benefit also topatients with ICH DOACs have a favorable risk-benefit profile compared to VKA resulting in a reduc-tion in stroke and mortality31 In particular DOACsare uniformly associated with a 50 reduced risk ofICH compared to VKA32 Limited information froma recent study based on national Danish registriessupports this assumption33 Moreover apixaban sig-nificantly reduced the risk of stroke and systemicembolism compared to aspirin without increasingthe risk of ICH in A Phase III Study of Apixabanin Patients With Atrial Fibrillation (AVERROES)34
Therefore DOACs could be a better alternative forpatients with ICH and AF The ongoing ApixabanVersus Antiplatelet Drugs or no AntithromboticDrugs After Anticoagulation-Associated IntracerebralHaemorrhage in Patients With Atrial Fibrillation(APACHE-AF) pilot study (ClinicalTrialsgovNCT02565693) addresses stroke prevention withDOACs in ICH survivors with AF Nonpharmaco-logic prevention strategies including left atrialappendage occlusion could be an alternative but
the evidence for this intervention in ICH survivorswith AF is limited13536
In addition to relative risks decision making fora specific antithrombotic therapy has to take the abso-lute risks for ischemic and hemorrhagic events intoaccount A previous meta-analysis reported an annualrisk of recurrent intracerebral hemorrhage of 13 to744 whereas a prospective cohort study of patientswith AF on VKA after ICH reported an ICH recur-rence rate of 185 per person-year and no ISe5 In ourstudy VKA users had a 04 to 09 higher pooledannual rate of ICH recurrence compared to the othertreatment groups On the contrary the pooled annualevent rate for IS was much lower in patients on VKA(32 per 100 patient-years) compared to the othertreatment groups (APA 95 per 100 patient-yearsno-ATM 61 per 100 patient-years) Although thesedata suggest a reduction of combined ischemic andhemorrhagic stroke event rates by VKA they do notaccount for the different mortality and morbidity re-sulting from these different types of stroke
Current American Heart Association guidelinesrecommend that APA monotherapy after any ICHmight be considered and can be a reasonable alterna-tive in patients with lobar hemorrhage in whomOAC should be avoided6 The findings of the presentmeta-analysis do not support the use of APA for ISprevention because no effect on prevention of throm-boembolic events was observed in patients with AFand ICH Although older research found a smallerbleeding risk on APAs compared to VKAs37 the rateof ICH on aspirin was similar to that of well-managedVKAs38 or DOACs34 However the risk-benefit ratioof APA in ICH survivors with AF was unclear Thecurrent analysis suggests that APAs do not increasethe risk of ICH recurrence compared to VKAs or no-ATM
Our systematic review and meta-analysis wasbased on a comprehensive search strategy that aimedto provide pooled estimates for IS and ICH recur-rence in ICH survivors with AF after different preven-tion strategies Thus we can anticipate a low rate ofunderdetection An important limitation of this largemeta-analysis is the limited data quality of the mostlyretrospective studies For example 3 studies relied oncohorts of patients derived from large national regis-tries that use ICD-10 codes for medical diagnosisand Anatomical Therapeutic Chemical classificationsystem codes to identify ATM Because some deathsmay be due to undiagnosed stroke and some minorstrokes may have remained undetected the risk ofIS may be underreported Using a 6-week landmarkapproach we did not take into account bleeding com-plications related to the index ICH that may havebeen misclassified as ICH recurrences Likewise itis uncertain how many of the early recurrences were
Neurology 89 August 15 2017 693
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
truly new events or just an extension of the initialbleeding site9 The included studies are highly proneto selection bias and confounding by indicationbecause treating physicians may have avoided theuse of VKAs in patients perceived to be at higher riskof recurrence Hence unmeasured selection bias islikely in that we were unable to calculate adjustedincidence RRs because individual patient data werenot available in all studies We summarized aggre-gated treatment group differences (baseline character-istics and comorbidities) (table e-5) for each studythat may facilitate the interpretation of the results(table e-6) As previously shown baseline adjustmentin the setting of time-dependent exposure of treat-ment regimens only marginally affects outcomes asso-ciated with treatment9 This may indicate that otherreasons (besides the measure and included variables)have affected the decision of resuming OAC treat-ment This highlights the importance of meticulousinterpretation of the associations because indicationbias was likely present in all of the included studiesAnother limitation is that we did not have informationon either the time in therapeutic range for patientstaking VKAs or the quality of blood pressure control39
We also did not have data on dropout and rates anddirections of switch between different antithrombotictreatment strategies The number of studies includedin the meta-analysis was small therefore meta-regression and publication bias assessments may havebeen underpowered and should be interpreted withcaution Our study focused on IS and ICH as the mainoutcome events This approach may not provide thefull picture of outcome events and other factors affect-ing the net clinical benefit The 2 largest includedstudies showed a significant decrease of mortality inpatients treated with VKAs915 Because we censoredpatients after either IS or ICH we did not capturepotential multiple outcome events in individual pa-tients although ICH and IS are competing riskAnother limitation is that further subgroup analysesin terms of risk factors for ICH recurrence such aslobar vs deep hemorrhage topography leukoaraiosisand cerebral microbleed burden were not feasiblebecause this information was missing in several studiesIn addition comorbidities apart from AF (eg coro-nary artery disease) indicating the use of antiplateletswere not addressed
This meta-analysis of antithrombotic treatment inVKA-associated ICH survivors with AF suggests thatanticoagulation with VKA is associated with a lowerrate of IS compared to other or no antithromboticswithout causing a major increase of the risk of ICHrecurrence whereas antiplatelets fail to prevent ISBecause of the limitations of observational studiesa randomized controlled trial of antithrombotictherapy preferably with DOACs used as the
anticoagulants is needed to better guide decision mak-ing for antithrombotic therapy in patients with ICHand AF
AUTHOR CONTRIBUTIONSEleni Korompoki study concept data collection drafting and critical revi-
sion of manuscript Filippos T Filippidis study concept statistical analysis
data collection drafting and critical revision of manuscript Peter B Nielsen
study concept data collection and critical revision of manuscript
Angela Del Giudice Gregory Y Lip Joji Kuramatsu Hagen Huttner
Jiming Fang Sam Schulman Joan Martiacute-Fagravebregas Celine S Gathier
Anand Viswanathan Alessandro Biffi Daniela Poli and Christian
Weimar data collection and critical revision of manuscript Uwe
Malzahn and Peter Heuschmann critical review of manuscript Roland
Veltkamp study concept and financial support drafting and critical
revision of manuscript All authors have read and approved the final form
of the manuscript and have agreed to conditions noted on the authorship
agreement The principal author has taken full responsibility for the data
the analyses and the interpretation and the conduct of the research The
statistical analysis has been contacted by Dr Filippidis (Department of
Primary Care and Public Health Imperial College London UK) All
authors had full access to all the data in the study and had final respon-
sibility for the decision to submit for publication Contributor Torben
Bjerregaard Larsen his institution has received payment for enrolling trial
participants from Janssen Scientific Affairs LLC and Boehringer Ingelheim
and he has been on the speaker bureaus for Bayer BMSPfizer Roche
Diagnostics Boehringer Ingelheim and Takeda Pharma
ACKNOWLEDGMENTContributor Torben Bjerregaard Larsen Aalborg University Hospital
Department of Cardiology Aalborg Thrombosis Research Unit Denmark
(data collection)
STUDY FUNDINGSupported by Imperial College London St Maryrsquos development fund
and National Institute for Health Research Imperial Biomedical Research
Centre The sponsor of the study had no role in study design data
collection data analysis data interpretation or writing of the report
Celine S Gathier was supported by the Dutch Heart Foundation grant
2009B046 Joan Martiacute-Fagravebregas was supported by the Spanish Ministry
of Health-Instituto de Salud Carlos III Redes temaacuteticas de Investigacioacuten
Cooperativa INVICTUS RD01200140002 and Fondo Europeo de
Desarrollo Regional Jiming Fang the Ontario Stroke Registry is funded
by the Canadian Stroke Network (CSN) and the Ontario Ministry of
Health and Long-Term Care (MOHLTC) This study was supported by
the Institute for Clinical Evaluative Sciences (ICES) which is funded by
an annual grant from the Ontario MOHLTC The opinions results and
conclusions reported in this paper are those of the authors and are inde-
pendent from the funding sources No endorsement by ICES or the
Ontario MOHLTC is intended or should be inferred
DISCLOSUREE Korompoki and F Filippidis report no disclosures relevant to the man-
uscript P Nielsen speaker for Boehringer Ingelheim consultant for
Bayer Pharma AS and BMSPfizer unrestricted research grant from
BMSPfizer A Del Giudice reports no disclosures relevant to the man-
uscript G Lip consultant for BayerJanssen BMSPfizer Biotronik
Medtronic Boehringer Ingelheim Microlife and Daiichi-Sankyo
speaker for Bayer BMSPfizer Medtronic Boehringer Ingelheim Micro-
life Roche and Daiichi-Sankyo J Kuramatsu reports no conflicts of
interest related to manuscript Unrelated potential conflicts of interest
travel grants from EMCools Otsuka and Boehringer Ingelheim and
speaker honoraria from Otsuka H Huttner reports no conflicts of inter-
est related to manuscript Unrelated potential conflicts of interest consul-
ting speaker honoraria and research support from Boehringer Ingelheim
Pfizer Biogen Medtronic and Novartis J Fang reports no disclosures
relevant to the manuscript S Schulman reports no conflicts of interest
related to manuscript Unrelated potential conflicts of interest honoraria
research support from Baxter Bayer Boehringer Ingelheim Daichii
694 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Sankyo Octapharma and Sanofi J Martiacute-Fagravebregas C Gathier
A Viswanathan A Biffi D Poli C Weimar and U Malzahn report
no disclosures relevant to the manuscript P Heuschmann research
grants from BMBF European Union Chariteacute Berlin Chamber of Physi-
cians German Parkinson Society University Hospital Wuumlrzburg
Robert-Koch-Institute German Heart Foundation Chariteacutendash
Universitaumltsmedizin Berlin (MonDAFIS unrestricted research grant to
Chariteacute from Bayer) University Goumlttingen (FIND-AFrandomized
unrestricted research grant to University Goumlttingen from Boehringer
Ingelheim) and University Hospital Heidelberg (RASUNOA-prime
unrestricted research grant to University Hospital Heidelberg from Bayer
BMS Boehringer Daiichi Sankyo) R Veltkamp consulting speaker
honoraria research support from Bayer Boehringer Daiichi Sankyo
BMS Pfizer Portola Biogen Amgen Morphosys Medtronic and
Apoplex Medical Technologies Go to Neurologyorg for full disclosures
Received December 29 2016 Accepted in final form May 23 2017
REFERENCES1 Camm AJ Lip GY De Caterina R et al 2012 Focused
update of the ESC guidelines for the management of atrial
fibrillation an update of the 2010 ESC guidelines for the
management of atrial fibrillation developed with the spe-
cial contribution of the European Heart Rhythm Associa-
tion Eur Heart J 2012332719ndash2747
2 Olesen JB Lip GY Hansen ML et al Validation of risk
stratification schemes for predicting stroke and thrombo-
embolism in patients with atrial fibrillation nationwide
cohort study BMJ 2011342d124
3 Flynn RW MacDonald TM Murray GD Doney AS
Systematic review of observational research studying the
long-term use of antithrombotic medicines following
intracerebral hemorrhage Cardiovasc Ther 201028
177ndash184
4 Poon MT Fonville AF Al-Shahi Salman R Long-term
prognosis after intracerebral haemorrhage systematic
review and meta-analysis J Neurol Neurosurg Psychiatry
201485660ndash667
5 Pisters R Lane DA Nieuwlaat R de Vos CB Crijns HJ
Lip GY A novel user-friendly score (HAS-BLED) to assess
1-year risk of major bleeding in patients with atrial fibrilla-
tion the Euro Heart Survey Chest 20101381093ndash1100
6 Hemphill JC III Greenberg SM Anderson CS et al
Guidelines for the management of spontaneous intracere-
bral hemorrhage a guideline for healthcare professionals
from the American Heart AssociationAmerican Stroke
Association Stroke 2015462032ndash2060
7 Steiner T Al-Shahi Salman R Beer R et al European
Stroke Organisation (ESO) guidelines for the management
of spontaneous intracerebral hemorrhage Int J Stroke
20149840ndash855
8 Liberati A Altman DG Tetzlaff J et al The PRISMA state-
ment for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions explanation
and elaboration J Clin Epidemiol 200962e1ndashe34
9 Nielsen PB Larsen TB Skjoth F Gorst-Rasmussen A
Rasmussen LH Lip GY Restarting anticoagulant treat-
ment after intracranial haemorrhage in patients with atrial
fibrillation and the impact on recurrent stroke mortality
and bleeding a nationwide cohort study Circulation
2015132517ndash525
10 Higgins JPT Altman DG Assessing Risk of Bias in
Included Studies Chichester Wiley 2008
11 DerSimonian R Laird N Meta-analysis in clinical trials
Control Clin Trials 19867177ndash188
12 Stamplecoski M Fang J Kapral MK Silver FL Long-term
outcomes of elderly patients with intracerebral hemorrhage
and atrial fibrillation Stroke 201445(s1)ATMP103
13 Viswanathan A Rakich SM Engel C et al Antiplatelet use
after intracerebral hemorrhage Neurology 200666206ndash209
14 Gathier CS Algra A Rinkel GJ van der Worp HB Long-
term outcome after anticoagulation-associated intracerebral
haemorrhage with or without restarting antithrombotic
therapy Cerebrovasc Dis 20133633ndash37
15 Kuramatsu JB Gerner ST Schellinger PD et al Antico-
agulant reversal blood pressure levels and anticoagulant
resumption in patients with anticoagulation-related intra-
cerebral hemorrhage JAMA 2015313824ndash836
16 Majeed A Kim YK Roberts RS Holmstrom M Schulman
S Optimal timing of resumption of warfarin after intracranial
hemorrhage Stroke 2010412860ndash2866
17 Vidal-Jordana A Barroeta-Espar I Sainz Pelayo MP
Mateo J Delgado-Mederos R Marti-Fabregas J Intracerebral
hemorrhage in anticoagulated patients what do we do after-
wards [in Spanish] Neurologia 201227136ndash142
18 Horstmann S Rizos T Jenetzky E Gumbinger C Hacke W
Veltkamp R Prevalence of atrial fibrillation in intracerebral
hemorrhage Eur J Neurol 201421570ndash576
19 Andersen KK Olsen TS Dehlendorff C Kammersgaard LP
Hemorrhagic and ischemic strokes compared stroke severity
mortality and risk factors Stroke 2009402068ndash2072
20 Paciaroni M Agnelli G Should oral anticoagulants be
restarted after warfarin-associated cerebral haemorrhage
in patients with atrial fibrillation Thromb Haemost
201411114ndash18
21 Eckman MH Rosand J Knudsen KA Singer DE
Greenberg SM Can patients be anticoagulated after
intracerebral hemorrhage A decision analysis Stroke
2004341710ndash1716
22 Lip GY Andreotti F Fauchier L et al Bleeding risk assess-
ment and management in atrial fibrillation patients a position
document from the European Heart Rhythm Association
endorsed by the European Society of Cardiology Working
Group on Thrombosis Europace 201113723ndash746
23 Goldstein JN Greenberg SM Should anticoagulation be
resumed after intracerebral hemorrhage Cleve Clin J Med
201077791ndash799
24 Molina CA Selim MH The dilemma of resuming anti-
coagulation after intracranial hemorrhage little evidence
facing big fears Stroke 2011423665ndash3666
25 Pasquini M Charidimou A van Asch CJ et al Variation in
restarting antithrombotic drugs at hospital discharge after
intracerebral hemorrhage Stroke 2014452643ndash2648
26 Maeda K Koga M Okada Y et al Nationwide survey of
neuro-specialistsrsquo opinions on anticoagulant therapy after
intracerebral hemorrhage in patients with atrial fibrillation
J Neurol Sci 201231282ndash85
27 Hart RG Pearce LA Aguilar MI Meta-analysis antith-
rombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation Ann Intern Med 2007146
857ndash867
28 Chao TF Liu CJ Liao JN et al Use of oral anticoagulants
for stroke prevention in patients with atrial fibrillation who
have a history of intracranial hemorrhage Circulation
20161331540ndash1547
29 Pennlert J Overholser R Asplund K et al Optimal timing
of anticoagulant treatment after intracerebral hemorrhage
in patients with atrial fibrillation Stroke 201748
314ndash320
Neurology 89 August 15 2017 695
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

in all comparisons All studies had possible selectionbias Overall 71 of studies reported consecutiverecruitment Blinding of outcome assessment was per-formed in only one study Attrition bias was found in29 of studies No funding bias was found in any ofthe included studies Risk of reporting bias was low inall studies because data were provided directly by thecorresponding authors Other potential risks of biasare presented in table e-3
VKAs vs no-VKAs A total of 6 studies compared the ratesof IS and ICH between patients who started a VKA andpatients who did not start a VKA (no-VKA) The pooled
RR of IS was significantly lower for VKA vs no-VKApatients (RR 5 046 95 CI 029 to 072 p 5
00008 I2 5 0) (figure 2A) The rate of recurrentICH was not significantly increased in VKA-treatedcompared to no-VKA patients (pooled RR 5 12395 CI 080 to 187 p5 053 I2 5 0) (figure 3A)
VKAs vs APAs Five studies provided data for compar-ison of VKAs and APAs The pooled data showed a sig-nificant decrease in the rate of IS in patients treatedwith VKA vs APA (pooled RR 5 045 95 CI027 to 074 p5 0002 I2 5 0) (figure 2B) Againthe rate of ICH recurrence was not significantly higher
Figure 1 PRISMA flowchart Study selection
AF 5 atrial fibrillation PRISMA 5 Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Neurology 89 August 15 2017 689
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
for VKA than for APA (pooled RR 5 134 95 CI079 to 230 p 5 028 I2 5 0) (figure 3B)
VKAs vs no-ATM Five studies compared the rate of ISand ICH in patients started on VKA vs no-ATM Thepooled rate for IS was significantly lower in VKA-treatedpatients (pooled RR 5 047 95 CI 029ndash077 p 50002 I25 0) (figure 2C) The comparison of the rateof ICH recurrence revealed no significant differencebetween VKA and no-ATM (pooled RR 5 093 95CI 045 to 190 p 5 084 I2 5 20) (figure 3C)
APAs vs no-ATM Five studies compared incidencerates in APA vs no-ATM The pooled RR estimatedid not differ significantly for IS (RR 5 106 95CI 072ndash154 p 5 078 I2 5 0) or for ICHrecurrence (RR5 077 95CI 047ndash125 p5 028I2 5 0) (figures 2D and 3D respectively)
Assessing the relationship between study-level covariates
and effect size Meta-regression analyses exploring theimpact of mean age sex timing of ATM exposureand type of ICH showed no statistically significantresults across all groups (table e-4)
DISCUSSION This meta-analysis compared the ratesof ICH recurrence and IS after different antith-rombotic therapies in VKA-associated ICH survivorswith AF Our main findings are that (1) treatmentwith VKA was associated with a significantly lowerrate of IS compared to no anticoagulation (2) APAconferred no benefit for prevention of IS over noantithrombotic therapy and (3) anticoagulated pa-tients did not have a statistically significantly higherrate of ICH recurrence
AF is present in a substantial proportion of ICHsurvivors with a prevalence of 12 to 14 innational registries and 30 in tertiary stroke cen-ters1819 There is limited evidence on whether ATMshould be started or withheld in this context20 ICH isthe most feared complication of antithrombotic ther-apy and the risk of ICH is higher in ICH survivors(3ndash5 per year)21e5e6e9 compared to patients with-out previous ICH (03ndash25 per year)22ndash24 Thepaucity of evidence for efficacy and safety results invariation in restarting antithrombotic drugs in ICHsurvivors ranging from 11 to 45 across differenthealth systems25 For example although patients ofAsian ethnicity have a higher risk of ICH than whitepatients a nationwide survey in Japan reported thatthe majority of physicians support the resumption ofOACs after ICH26 Our meta-analysis shows that pre-scribing VKA after VKA-associated ICH is associatedwith a reduction of IS by 45 to 47 compared toAPA or no-ATM therapy This effect size is similar tothat in patients with AF without previous ICH27 Ourresults are supported by additional studies suggestingthat ICH survivors with AF who do not start OACtreatment are at high risk of IS and mortality both ofwhich are significantly reduced by VKA915
Table 2 Pooled annual event rates for ICH recurrence and IS in differenttreatment strategies expressed as pooled event rates with 95 CI
IS event rate(95 CI)
ICH recurrenceevent rate (95 CI)
VKA 32 (20ndash49) 46 (31ndash66)
Antiplatelets 95 (73ndash120) 37 (25ndash54)
No antithrombotics 61 (49ndash76) 42 (32ndash55)
No VKA(antiplatelets or no antithrombotics)
73 (62ndash85) 40 (32ndash50)
Abbreviations CI 5 confidence interval ICH 5 intracranial hemorrhage IS 5 ischemicstroke VKA 5 vitamin K antagonist
Table 1 Characteristics of the studies included in the meta-analysis
Study Patients n Type of hemorrhage Comparison groupsAge mean(SD) y
Female
CHADS2median(IQR)
FUmedianmo
Time intervalto resumptiona
median (IQR)
Gathier et al14 18 VKA-associatedintracerebral hemorrhage
VKA vs APA vsno-ATM
745 (10$6) 39 2 (1ndash3) 32 21 (9ndash35) d
Kuramatsuet al15
566 VKA-associatedintracerebral hemorrhage
Warfarin (VKA) vs nowarfarin (no-VKA)
75 39 2 12 32 (20ndash69) d
Majeed et al16 84 VKA-associated ICH Warfarin (VKA) vs nowarfarin (no-VKA)
75 (9) 33 2 (2ndash4) 17 92 (56ndash34) wk
Nielsen et al9 1545 VKA-associated ICH OAC vs APA vsno-ATM
78 38 2 12 34 d
Stamplecoskiet al12
199 Intracerebral hemorrhage(57 VKA associated)
Warfarin (VKA) vs nowarfarin (no-VKA)
804 (69) 54 4 (3ndash4) 12 24 (12ndash83) d
Vidal-Jordanaet al17
25 VKA-associatedintracerebral hemorrhage
VKA vs APA 752 (4) 40 2 (1ndash4) 55 NR
Viswanathanet al13
15 Spontaneous intracerebralhemorrhage
APA vs no- APA 736 (89) 47 2 (1ndash3) 32 NR
Abbreviations APA5 antiplatelet agent ATM5 antithrombotic medication FU5 follow-up ICH5 intracranial hemorrhage IQR5 interquartile range NR5
not reported OAC 5 oral anticoagulant VKA 5 vitamin K antagonista Reflects time to treatment resumption among individuals who resumed treatment
690 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 2 Pooled RR meta-analyses for IS that occurred between 6 weeks and 1 year of follow-up afterexposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval IS 5 ischemic stroke IV 5 inverse variance RR 5 rate ratio VKA 5
vitamin K antagonist
Neurology 89 August 15 2017 691
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 3 Pooled RRmeta-analyses for ICH recurrence that occurred between 6 weeks and 1 year of follow-upafter exposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval ICH 5 intracranial hemorrhage IV5 inverse variance RR 5 rate ratioVKA 5 vitamin K antagonist
692 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reinitiation of warfarin in Taiwanese ICH survivorswith AF was beneficial One study modeling risks andbenefits calculated a net benefit of VKA for Asianpatients with ICH with a CHA2DS2-VASc score$6 but this threshold was likely to be lower withdirect OACs (DOACs)28 In our analysis whichincluded mainly white patients with ICH the medianCHADS2 score was 2 suggesting that starting OACafter ICH may be beneficial with only moderatethromboembolic risk
We found no significantly increased risk for recur-rent ICH with VKA although the point estimate forthe pooled RR was 23 to 32 higher compared tono-VKA and no-ATM Previous research showed thatICH survivors carry a significant risk of recurrentICHe5e7e8 whereas studies found no increased riskof ICH recurrencee10 when they were treated withanticoagulants after the index event Only earlyresumption of VKAs after warfarin-associated ICHincreased the risk of recurrent ICH16 A recent Swed-ish nationwide cohort study suggests that anticoagu-lant treatment may be initiated 7 to 8 weeks afterICH in intracerebral hemorrhage survivors with AFto balance benefit from treatment against the risk ofrebleeding29 In our meta-regression analysis the tim-ing of resumption failed to explain the lack of a sig-nificant difference for recurrent ICH betweenanticoagulated and nonanticoagulated patients butearly recurrent bleeding events were not captured inour study design
OAC has a net clinical benefit in patients with AFwithout ICH30 Considering the significant decreasein the rate of IS with anticoagulants a treatmentoption that provides a better safety profile thanVKA may provide a net clinical benefit also topatients with ICH DOACs have a favorable risk-benefit profile compared to VKA resulting in a reduc-tion in stroke and mortality31 In particular DOACsare uniformly associated with a 50 reduced risk ofICH compared to VKA32 Limited information froma recent study based on national Danish registriessupports this assumption33 Moreover apixaban sig-nificantly reduced the risk of stroke and systemicembolism compared to aspirin without increasingthe risk of ICH in A Phase III Study of Apixabanin Patients With Atrial Fibrillation (AVERROES)34
Therefore DOACs could be a better alternative forpatients with ICH and AF The ongoing ApixabanVersus Antiplatelet Drugs or no AntithromboticDrugs After Anticoagulation-Associated IntracerebralHaemorrhage in Patients With Atrial Fibrillation(APACHE-AF) pilot study (ClinicalTrialsgovNCT02565693) addresses stroke prevention withDOACs in ICH survivors with AF Nonpharmaco-logic prevention strategies including left atrialappendage occlusion could be an alternative but
the evidence for this intervention in ICH survivorswith AF is limited13536
In addition to relative risks decision making fora specific antithrombotic therapy has to take the abso-lute risks for ischemic and hemorrhagic events intoaccount A previous meta-analysis reported an annualrisk of recurrent intracerebral hemorrhage of 13 to744 whereas a prospective cohort study of patientswith AF on VKA after ICH reported an ICH recur-rence rate of 185 per person-year and no ISe5 In ourstudy VKA users had a 04 to 09 higher pooledannual rate of ICH recurrence compared to the othertreatment groups On the contrary the pooled annualevent rate for IS was much lower in patients on VKA(32 per 100 patient-years) compared to the othertreatment groups (APA 95 per 100 patient-yearsno-ATM 61 per 100 patient-years) Although thesedata suggest a reduction of combined ischemic andhemorrhagic stroke event rates by VKA they do notaccount for the different mortality and morbidity re-sulting from these different types of stroke
Current American Heart Association guidelinesrecommend that APA monotherapy after any ICHmight be considered and can be a reasonable alterna-tive in patients with lobar hemorrhage in whomOAC should be avoided6 The findings of the presentmeta-analysis do not support the use of APA for ISprevention because no effect on prevention of throm-boembolic events was observed in patients with AFand ICH Although older research found a smallerbleeding risk on APAs compared to VKAs37 the rateof ICH on aspirin was similar to that of well-managedVKAs38 or DOACs34 However the risk-benefit ratioof APA in ICH survivors with AF was unclear Thecurrent analysis suggests that APAs do not increasethe risk of ICH recurrence compared to VKAs or no-ATM
Our systematic review and meta-analysis wasbased on a comprehensive search strategy that aimedto provide pooled estimates for IS and ICH recur-rence in ICH survivors with AF after different preven-tion strategies Thus we can anticipate a low rate ofunderdetection An important limitation of this largemeta-analysis is the limited data quality of the mostlyretrospective studies For example 3 studies relied oncohorts of patients derived from large national regis-tries that use ICD-10 codes for medical diagnosisand Anatomical Therapeutic Chemical classificationsystem codes to identify ATM Because some deathsmay be due to undiagnosed stroke and some minorstrokes may have remained undetected the risk ofIS may be underreported Using a 6-week landmarkapproach we did not take into account bleeding com-plications related to the index ICH that may havebeen misclassified as ICH recurrences Likewise itis uncertain how many of the early recurrences were
Neurology 89 August 15 2017 693
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
truly new events or just an extension of the initialbleeding site9 The included studies are highly proneto selection bias and confounding by indicationbecause treating physicians may have avoided theuse of VKAs in patients perceived to be at higher riskof recurrence Hence unmeasured selection bias islikely in that we were unable to calculate adjustedincidence RRs because individual patient data werenot available in all studies We summarized aggre-gated treatment group differences (baseline character-istics and comorbidities) (table e-5) for each studythat may facilitate the interpretation of the results(table e-6) As previously shown baseline adjustmentin the setting of time-dependent exposure of treat-ment regimens only marginally affects outcomes asso-ciated with treatment9 This may indicate that otherreasons (besides the measure and included variables)have affected the decision of resuming OAC treat-ment This highlights the importance of meticulousinterpretation of the associations because indicationbias was likely present in all of the included studiesAnother limitation is that we did not have informationon either the time in therapeutic range for patientstaking VKAs or the quality of blood pressure control39
We also did not have data on dropout and rates anddirections of switch between different antithrombotictreatment strategies The number of studies includedin the meta-analysis was small therefore meta-regression and publication bias assessments may havebeen underpowered and should be interpreted withcaution Our study focused on IS and ICH as the mainoutcome events This approach may not provide thefull picture of outcome events and other factors affect-ing the net clinical benefit The 2 largest includedstudies showed a significant decrease of mortality inpatients treated with VKAs915 Because we censoredpatients after either IS or ICH we did not capturepotential multiple outcome events in individual pa-tients although ICH and IS are competing riskAnother limitation is that further subgroup analysesin terms of risk factors for ICH recurrence such aslobar vs deep hemorrhage topography leukoaraiosisand cerebral microbleed burden were not feasiblebecause this information was missing in several studiesIn addition comorbidities apart from AF (eg coro-nary artery disease) indicating the use of antiplateletswere not addressed
This meta-analysis of antithrombotic treatment inVKA-associated ICH survivors with AF suggests thatanticoagulation with VKA is associated with a lowerrate of IS compared to other or no antithromboticswithout causing a major increase of the risk of ICHrecurrence whereas antiplatelets fail to prevent ISBecause of the limitations of observational studiesa randomized controlled trial of antithrombotictherapy preferably with DOACs used as the
anticoagulants is needed to better guide decision mak-ing for antithrombotic therapy in patients with ICHand AF
AUTHOR CONTRIBUTIONSEleni Korompoki study concept data collection drafting and critical revi-
sion of manuscript Filippos T Filippidis study concept statistical analysis
data collection drafting and critical revision of manuscript Peter B Nielsen
study concept data collection and critical revision of manuscript
Angela Del Giudice Gregory Y Lip Joji Kuramatsu Hagen Huttner
Jiming Fang Sam Schulman Joan Martiacute-Fagravebregas Celine S Gathier
Anand Viswanathan Alessandro Biffi Daniela Poli and Christian
Weimar data collection and critical revision of manuscript Uwe
Malzahn and Peter Heuschmann critical review of manuscript Roland
Veltkamp study concept and financial support drafting and critical
revision of manuscript All authors have read and approved the final form
of the manuscript and have agreed to conditions noted on the authorship
agreement The principal author has taken full responsibility for the data
the analyses and the interpretation and the conduct of the research The
statistical analysis has been contacted by Dr Filippidis (Department of
Primary Care and Public Health Imperial College London UK) All
authors had full access to all the data in the study and had final respon-
sibility for the decision to submit for publication Contributor Torben
Bjerregaard Larsen his institution has received payment for enrolling trial
participants from Janssen Scientific Affairs LLC and Boehringer Ingelheim
and he has been on the speaker bureaus for Bayer BMSPfizer Roche
Diagnostics Boehringer Ingelheim and Takeda Pharma
ACKNOWLEDGMENTContributor Torben Bjerregaard Larsen Aalborg University Hospital
Department of Cardiology Aalborg Thrombosis Research Unit Denmark
(data collection)
STUDY FUNDINGSupported by Imperial College London St Maryrsquos development fund
and National Institute for Health Research Imperial Biomedical Research
Centre The sponsor of the study had no role in study design data
collection data analysis data interpretation or writing of the report
Celine S Gathier was supported by the Dutch Heart Foundation grant
2009B046 Joan Martiacute-Fagravebregas was supported by the Spanish Ministry
of Health-Instituto de Salud Carlos III Redes temaacuteticas de Investigacioacuten
Cooperativa INVICTUS RD01200140002 and Fondo Europeo de
Desarrollo Regional Jiming Fang the Ontario Stroke Registry is funded
by the Canadian Stroke Network (CSN) and the Ontario Ministry of
Health and Long-Term Care (MOHLTC) This study was supported by
the Institute for Clinical Evaluative Sciences (ICES) which is funded by
an annual grant from the Ontario MOHLTC The opinions results and
conclusions reported in this paper are those of the authors and are inde-
pendent from the funding sources No endorsement by ICES or the
Ontario MOHLTC is intended or should be inferred
DISCLOSUREE Korompoki and F Filippidis report no disclosures relevant to the man-
uscript P Nielsen speaker for Boehringer Ingelheim consultant for
Bayer Pharma AS and BMSPfizer unrestricted research grant from
BMSPfizer A Del Giudice reports no disclosures relevant to the man-
uscript G Lip consultant for BayerJanssen BMSPfizer Biotronik
Medtronic Boehringer Ingelheim Microlife and Daiichi-Sankyo
speaker for Bayer BMSPfizer Medtronic Boehringer Ingelheim Micro-
life Roche and Daiichi-Sankyo J Kuramatsu reports no conflicts of
interest related to manuscript Unrelated potential conflicts of interest
travel grants from EMCools Otsuka and Boehringer Ingelheim and
speaker honoraria from Otsuka H Huttner reports no conflicts of inter-
est related to manuscript Unrelated potential conflicts of interest consul-
ting speaker honoraria and research support from Boehringer Ingelheim
Pfizer Biogen Medtronic and Novartis J Fang reports no disclosures
relevant to the manuscript S Schulman reports no conflicts of interest
related to manuscript Unrelated potential conflicts of interest honoraria
research support from Baxter Bayer Boehringer Ingelheim Daichii
694 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Sankyo Octapharma and Sanofi J Martiacute-Fagravebregas C Gathier
A Viswanathan A Biffi D Poli C Weimar and U Malzahn report
no disclosures relevant to the manuscript P Heuschmann research
grants from BMBF European Union Chariteacute Berlin Chamber of Physi-
cians German Parkinson Society University Hospital Wuumlrzburg
Robert-Koch-Institute German Heart Foundation Chariteacutendash
Universitaumltsmedizin Berlin (MonDAFIS unrestricted research grant to
Chariteacute from Bayer) University Goumlttingen (FIND-AFrandomized
unrestricted research grant to University Goumlttingen from Boehringer
Ingelheim) and University Hospital Heidelberg (RASUNOA-prime
unrestricted research grant to University Hospital Heidelberg from Bayer
BMS Boehringer Daiichi Sankyo) R Veltkamp consulting speaker
honoraria research support from Bayer Boehringer Daiichi Sankyo
BMS Pfizer Portola Biogen Amgen Morphosys Medtronic and
Apoplex Medical Technologies Go to Neurologyorg for full disclosures
Received December 29 2016 Accepted in final form May 23 2017
REFERENCES1 Camm AJ Lip GY De Caterina R et al 2012 Focused
update of the ESC guidelines for the management of atrial
fibrillation an update of the 2010 ESC guidelines for the
management of atrial fibrillation developed with the spe-
cial contribution of the European Heart Rhythm Associa-
tion Eur Heart J 2012332719ndash2747
2 Olesen JB Lip GY Hansen ML et al Validation of risk
stratification schemes for predicting stroke and thrombo-
embolism in patients with atrial fibrillation nationwide
cohort study BMJ 2011342d124
3 Flynn RW MacDonald TM Murray GD Doney AS
Systematic review of observational research studying the
long-term use of antithrombotic medicines following
intracerebral hemorrhage Cardiovasc Ther 201028
177ndash184
4 Poon MT Fonville AF Al-Shahi Salman R Long-term
prognosis after intracerebral haemorrhage systematic
review and meta-analysis J Neurol Neurosurg Psychiatry
201485660ndash667
5 Pisters R Lane DA Nieuwlaat R de Vos CB Crijns HJ
Lip GY A novel user-friendly score (HAS-BLED) to assess
1-year risk of major bleeding in patients with atrial fibrilla-
tion the Euro Heart Survey Chest 20101381093ndash1100
6 Hemphill JC III Greenberg SM Anderson CS et al
Guidelines for the management of spontaneous intracere-
bral hemorrhage a guideline for healthcare professionals
from the American Heart AssociationAmerican Stroke
Association Stroke 2015462032ndash2060
7 Steiner T Al-Shahi Salman R Beer R et al European
Stroke Organisation (ESO) guidelines for the management
of spontaneous intracerebral hemorrhage Int J Stroke
20149840ndash855
8 Liberati A Altman DG Tetzlaff J et al The PRISMA state-
ment for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions explanation
and elaboration J Clin Epidemiol 200962e1ndashe34
9 Nielsen PB Larsen TB Skjoth F Gorst-Rasmussen A
Rasmussen LH Lip GY Restarting anticoagulant treat-
ment after intracranial haemorrhage in patients with atrial
fibrillation and the impact on recurrent stroke mortality
and bleeding a nationwide cohort study Circulation
2015132517ndash525
10 Higgins JPT Altman DG Assessing Risk of Bias in
Included Studies Chichester Wiley 2008
11 DerSimonian R Laird N Meta-analysis in clinical trials
Control Clin Trials 19867177ndash188
12 Stamplecoski M Fang J Kapral MK Silver FL Long-term
outcomes of elderly patients with intracerebral hemorrhage
and atrial fibrillation Stroke 201445(s1)ATMP103
13 Viswanathan A Rakich SM Engel C et al Antiplatelet use
after intracerebral hemorrhage Neurology 200666206ndash209
14 Gathier CS Algra A Rinkel GJ van der Worp HB Long-
term outcome after anticoagulation-associated intracerebral
haemorrhage with or without restarting antithrombotic
therapy Cerebrovasc Dis 20133633ndash37
15 Kuramatsu JB Gerner ST Schellinger PD et al Antico-
agulant reversal blood pressure levels and anticoagulant
resumption in patients with anticoagulation-related intra-
cerebral hemorrhage JAMA 2015313824ndash836
16 Majeed A Kim YK Roberts RS Holmstrom M Schulman
S Optimal timing of resumption of warfarin after intracranial
hemorrhage Stroke 2010412860ndash2866
17 Vidal-Jordana A Barroeta-Espar I Sainz Pelayo MP
Mateo J Delgado-Mederos R Marti-Fabregas J Intracerebral
hemorrhage in anticoagulated patients what do we do after-
wards [in Spanish] Neurologia 201227136ndash142
18 Horstmann S Rizos T Jenetzky E Gumbinger C Hacke W
Veltkamp R Prevalence of atrial fibrillation in intracerebral
hemorrhage Eur J Neurol 201421570ndash576
19 Andersen KK Olsen TS Dehlendorff C Kammersgaard LP
Hemorrhagic and ischemic strokes compared stroke severity
mortality and risk factors Stroke 2009402068ndash2072
20 Paciaroni M Agnelli G Should oral anticoagulants be
restarted after warfarin-associated cerebral haemorrhage
in patients with atrial fibrillation Thromb Haemost
201411114ndash18
21 Eckman MH Rosand J Knudsen KA Singer DE
Greenberg SM Can patients be anticoagulated after
intracerebral hemorrhage A decision analysis Stroke
2004341710ndash1716
22 Lip GY Andreotti F Fauchier L et al Bleeding risk assess-
ment and management in atrial fibrillation patients a position
document from the European Heart Rhythm Association
endorsed by the European Society of Cardiology Working
Group on Thrombosis Europace 201113723ndash746
23 Goldstein JN Greenberg SM Should anticoagulation be
resumed after intracerebral hemorrhage Cleve Clin J Med
201077791ndash799
24 Molina CA Selim MH The dilemma of resuming anti-
coagulation after intracranial hemorrhage little evidence
facing big fears Stroke 2011423665ndash3666
25 Pasquini M Charidimou A van Asch CJ et al Variation in
restarting antithrombotic drugs at hospital discharge after
intracerebral hemorrhage Stroke 2014452643ndash2648
26 Maeda K Koga M Okada Y et al Nationwide survey of
neuro-specialistsrsquo opinions on anticoagulant therapy after
intracerebral hemorrhage in patients with atrial fibrillation
J Neurol Sci 201231282ndash85
27 Hart RG Pearce LA Aguilar MI Meta-analysis antith-
rombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation Ann Intern Med 2007146
857ndash867
28 Chao TF Liu CJ Liao JN et al Use of oral anticoagulants
for stroke prevention in patients with atrial fibrillation who
have a history of intracranial hemorrhage Circulation
20161331540ndash1547
29 Pennlert J Overholser R Asplund K et al Optimal timing
of anticoagulant treatment after intracerebral hemorrhage
in patients with atrial fibrillation Stroke 201748
314ndash320
Neurology 89 August 15 2017 695
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

for VKA than for APA (pooled RR 5 134 95 CI079 to 230 p 5 028 I2 5 0) (figure 3B)
VKAs vs no-ATM Five studies compared the rate of ISand ICH in patients started on VKA vs no-ATM Thepooled rate for IS was significantly lower in VKA-treatedpatients (pooled RR 5 047 95 CI 029ndash077 p 50002 I25 0) (figure 2C) The comparison of the rateof ICH recurrence revealed no significant differencebetween VKA and no-ATM (pooled RR 5 093 95CI 045 to 190 p 5 084 I2 5 20) (figure 3C)
APAs vs no-ATM Five studies compared incidencerates in APA vs no-ATM The pooled RR estimatedid not differ significantly for IS (RR 5 106 95CI 072ndash154 p 5 078 I2 5 0) or for ICHrecurrence (RR5 077 95CI 047ndash125 p5 028I2 5 0) (figures 2D and 3D respectively)
Assessing the relationship between study-level covariates
and effect size Meta-regression analyses exploring theimpact of mean age sex timing of ATM exposureand type of ICH showed no statistically significantresults across all groups (table e-4)
DISCUSSION This meta-analysis compared the ratesof ICH recurrence and IS after different antith-rombotic therapies in VKA-associated ICH survivorswith AF Our main findings are that (1) treatmentwith VKA was associated with a significantly lowerrate of IS compared to no anticoagulation (2) APAconferred no benefit for prevention of IS over noantithrombotic therapy and (3) anticoagulated pa-tients did not have a statistically significantly higherrate of ICH recurrence
AF is present in a substantial proportion of ICHsurvivors with a prevalence of 12 to 14 innational registries and 30 in tertiary stroke cen-ters1819 There is limited evidence on whether ATMshould be started or withheld in this context20 ICH isthe most feared complication of antithrombotic ther-apy and the risk of ICH is higher in ICH survivors(3ndash5 per year)21e5e6e9 compared to patients with-out previous ICH (03ndash25 per year)22ndash24 Thepaucity of evidence for efficacy and safety results invariation in restarting antithrombotic drugs in ICHsurvivors ranging from 11 to 45 across differenthealth systems25 For example although patients ofAsian ethnicity have a higher risk of ICH than whitepatients a nationwide survey in Japan reported thatthe majority of physicians support the resumption ofOACs after ICH26 Our meta-analysis shows that pre-scribing VKA after VKA-associated ICH is associatedwith a reduction of IS by 45 to 47 compared toAPA or no-ATM therapy This effect size is similar tothat in patients with AF without previous ICH27 Ourresults are supported by additional studies suggestingthat ICH survivors with AF who do not start OACtreatment are at high risk of IS and mortality both ofwhich are significantly reduced by VKA915
Table 2 Pooled annual event rates for ICH recurrence and IS in differenttreatment strategies expressed as pooled event rates with 95 CI
IS event rate(95 CI)
ICH recurrenceevent rate (95 CI)
VKA 32 (20ndash49) 46 (31ndash66)
Antiplatelets 95 (73ndash120) 37 (25ndash54)
No antithrombotics 61 (49ndash76) 42 (32ndash55)
No VKA(antiplatelets or no antithrombotics)
73 (62ndash85) 40 (32ndash50)
Abbreviations CI 5 confidence interval ICH 5 intracranial hemorrhage IS 5 ischemicstroke VKA 5 vitamin K antagonist
Table 1 Characteristics of the studies included in the meta-analysis
Study Patients n Type of hemorrhage Comparison groupsAge mean(SD) y
Female
CHADS2median(IQR)
FUmedianmo
Time intervalto resumptiona
median (IQR)
Gathier et al14 18 VKA-associatedintracerebral hemorrhage
VKA vs APA vsno-ATM
745 (10$6) 39 2 (1ndash3) 32 21 (9ndash35) d
Kuramatsuet al15
566 VKA-associatedintracerebral hemorrhage
Warfarin (VKA) vs nowarfarin (no-VKA)
75 39 2 12 32 (20ndash69) d
Majeed et al16 84 VKA-associated ICH Warfarin (VKA) vs nowarfarin (no-VKA)
75 (9) 33 2 (2ndash4) 17 92 (56ndash34) wk
Nielsen et al9 1545 VKA-associated ICH OAC vs APA vsno-ATM
78 38 2 12 34 d
Stamplecoskiet al12
199 Intracerebral hemorrhage(57 VKA associated)
Warfarin (VKA) vs nowarfarin (no-VKA)
804 (69) 54 4 (3ndash4) 12 24 (12ndash83) d
Vidal-Jordanaet al17
25 VKA-associatedintracerebral hemorrhage
VKA vs APA 752 (4) 40 2 (1ndash4) 55 NR
Viswanathanet al13
15 Spontaneous intracerebralhemorrhage
APA vs no- APA 736 (89) 47 2 (1ndash3) 32 NR
Abbreviations APA5 antiplatelet agent ATM5 antithrombotic medication FU5 follow-up ICH5 intracranial hemorrhage IQR5 interquartile range NR5
not reported OAC 5 oral anticoagulant VKA 5 vitamin K antagonista Reflects time to treatment resumption among individuals who resumed treatment
690 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 2 Pooled RR meta-analyses for IS that occurred between 6 weeks and 1 year of follow-up afterexposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval IS 5 ischemic stroke IV 5 inverse variance RR 5 rate ratio VKA 5
vitamin K antagonist
Neurology 89 August 15 2017 691
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 3 Pooled RRmeta-analyses for ICH recurrence that occurred between 6 weeks and 1 year of follow-upafter exposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval ICH 5 intracranial hemorrhage IV5 inverse variance RR 5 rate ratioVKA 5 vitamin K antagonist
692 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reinitiation of warfarin in Taiwanese ICH survivorswith AF was beneficial One study modeling risks andbenefits calculated a net benefit of VKA for Asianpatients with ICH with a CHA2DS2-VASc score$6 but this threshold was likely to be lower withdirect OACs (DOACs)28 In our analysis whichincluded mainly white patients with ICH the medianCHADS2 score was 2 suggesting that starting OACafter ICH may be beneficial with only moderatethromboembolic risk
We found no significantly increased risk for recur-rent ICH with VKA although the point estimate forthe pooled RR was 23 to 32 higher compared tono-VKA and no-ATM Previous research showed thatICH survivors carry a significant risk of recurrentICHe5e7e8 whereas studies found no increased riskof ICH recurrencee10 when they were treated withanticoagulants after the index event Only earlyresumption of VKAs after warfarin-associated ICHincreased the risk of recurrent ICH16 A recent Swed-ish nationwide cohort study suggests that anticoagu-lant treatment may be initiated 7 to 8 weeks afterICH in intracerebral hemorrhage survivors with AFto balance benefit from treatment against the risk ofrebleeding29 In our meta-regression analysis the tim-ing of resumption failed to explain the lack of a sig-nificant difference for recurrent ICH betweenanticoagulated and nonanticoagulated patients butearly recurrent bleeding events were not captured inour study design
OAC has a net clinical benefit in patients with AFwithout ICH30 Considering the significant decreasein the rate of IS with anticoagulants a treatmentoption that provides a better safety profile thanVKA may provide a net clinical benefit also topatients with ICH DOACs have a favorable risk-benefit profile compared to VKA resulting in a reduc-tion in stroke and mortality31 In particular DOACsare uniformly associated with a 50 reduced risk ofICH compared to VKA32 Limited information froma recent study based on national Danish registriessupports this assumption33 Moreover apixaban sig-nificantly reduced the risk of stroke and systemicembolism compared to aspirin without increasingthe risk of ICH in A Phase III Study of Apixabanin Patients With Atrial Fibrillation (AVERROES)34
Therefore DOACs could be a better alternative forpatients with ICH and AF The ongoing ApixabanVersus Antiplatelet Drugs or no AntithromboticDrugs After Anticoagulation-Associated IntracerebralHaemorrhage in Patients With Atrial Fibrillation(APACHE-AF) pilot study (ClinicalTrialsgovNCT02565693) addresses stroke prevention withDOACs in ICH survivors with AF Nonpharmaco-logic prevention strategies including left atrialappendage occlusion could be an alternative but
the evidence for this intervention in ICH survivorswith AF is limited13536
In addition to relative risks decision making fora specific antithrombotic therapy has to take the abso-lute risks for ischemic and hemorrhagic events intoaccount A previous meta-analysis reported an annualrisk of recurrent intracerebral hemorrhage of 13 to744 whereas a prospective cohort study of patientswith AF on VKA after ICH reported an ICH recur-rence rate of 185 per person-year and no ISe5 In ourstudy VKA users had a 04 to 09 higher pooledannual rate of ICH recurrence compared to the othertreatment groups On the contrary the pooled annualevent rate for IS was much lower in patients on VKA(32 per 100 patient-years) compared to the othertreatment groups (APA 95 per 100 patient-yearsno-ATM 61 per 100 patient-years) Although thesedata suggest a reduction of combined ischemic andhemorrhagic stroke event rates by VKA they do notaccount for the different mortality and morbidity re-sulting from these different types of stroke
Current American Heart Association guidelinesrecommend that APA monotherapy after any ICHmight be considered and can be a reasonable alterna-tive in patients with lobar hemorrhage in whomOAC should be avoided6 The findings of the presentmeta-analysis do not support the use of APA for ISprevention because no effect on prevention of throm-boembolic events was observed in patients with AFand ICH Although older research found a smallerbleeding risk on APAs compared to VKAs37 the rateof ICH on aspirin was similar to that of well-managedVKAs38 or DOACs34 However the risk-benefit ratioof APA in ICH survivors with AF was unclear Thecurrent analysis suggests that APAs do not increasethe risk of ICH recurrence compared to VKAs or no-ATM
Our systematic review and meta-analysis wasbased on a comprehensive search strategy that aimedto provide pooled estimates for IS and ICH recur-rence in ICH survivors with AF after different preven-tion strategies Thus we can anticipate a low rate ofunderdetection An important limitation of this largemeta-analysis is the limited data quality of the mostlyretrospective studies For example 3 studies relied oncohorts of patients derived from large national regis-tries that use ICD-10 codes for medical diagnosisand Anatomical Therapeutic Chemical classificationsystem codes to identify ATM Because some deathsmay be due to undiagnosed stroke and some minorstrokes may have remained undetected the risk ofIS may be underreported Using a 6-week landmarkapproach we did not take into account bleeding com-plications related to the index ICH that may havebeen misclassified as ICH recurrences Likewise itis uncertain how many of the early recurrences were
Neurology 89 August 15 2017 693
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
truly new events or just an extension of the initialbleeding site9 The included studies are highly proneto selection bias and confounding by indicationbecause treating physicians may have avoided theuse of VKAs in patients perceived to be at higher riskof recurrence Hence unmeasured selection bias islikely in that we were unable to calculate adjustedincidence RRs because individual patient data werenot available in all studies We summarized aggre-gated treatment group differences (baseline character-istics and comorbidities) (table e-5) for each studythat may facilitate the interpretation of the results(table e-6) As previously shown baseline adjustmentin the setting of time-dependent exposure of treat-ment regimens only marginally affects outcomes asso-ciated with treatment9 This may indicate that otherreasons (besides the measure and included variables)have affected the decision of resuming OAC treat-ment This highlights the importance of meticulousinterpretation of the associations because indicationbias was likely present in all of the included studiesAnother limitation is that we did not have informationon either the time in therapeutic range for patientstaking VKAs or the quality of blood pressure control39
We also did not have data on dropout and rates anddirections of switch between different antithrombotictreatment strategies The number of studies includedin the meta-analysis was small therefore meta-regression and publication bias assessments may havebeen underpowered and should be interpreted withcaution Our study focused on IS and ICH as the mainoutcome events This approach may not provide thefull picture of outcome events and other factors affect-ing the net clinical benefit The 2 largest includedstudies showed a significant decrease of mortality inpatients treated with VKAs915 Because we censoredpatients after either IS or ICH we did not capturepotential multiple outcome events in individual pa-tients although ICH and IS are competing riskAnother limitation is that further subgroup analysesin terms of risk factors for ICH recurrence such aslobar vs deep hemorrhage topography leukoaraiosisand cerebral microbleed burden were not feasiblebecause this information was missing in several studiesIn addition comorbidities apart from AF (eg coro-nary artery disease) indicating the use of antiplateletswere not addressed
This meta-analysis of antithrombotic treatment inVKA-associated ICH survivors with AF suggests thatanticoagulation with VKA is associated with a lowerrate of IS compared to other or no antithromboticswithout causing a major increase of the risk of ICHrecurrence whereas antiplatelets fail to prevent ISBecause of the limitations of observational studiesa randomized controlled trial of antithrombotictherapy preferably with DOACs used as the
anticoagulants is needed to better guide decision mak-ing for antithrombotic therapy in patients with ICHand AF
AUTHOR CONTRIBUTIONSEleni Korompoki study concept data collection drafting and critical revi-
sion of manuscript Filippos T Filippidis study concept statistical analysis
data collection drafting and critical revision of manuscript Peter B Nielsen
study concept data collection and critical revision of manuscript
Angela Del Giudice Gregory Y Lip Joji Kuramatsu Hagen Huttner
Jiming Fang Sam Schulman Joan Martiacute-Fagravebregas Celine S Gathier
Anand Viswanathan Alessandro Biffi Daniela Poli and Christian
Weimar data collection and critical revision of manuscript Uwe
Malzahn and Peter Heuschmann critical review of manuscript Roland
Veltkamp study concept and financial support drafting and critical
revision of manuscript All authors have read and approved the final form
of the manuscript and have agreed to conditions noted on the authorship
agreement The principal author has taken full responsibility for the data
the analyses and the interpretation and the conduct of the research The
statistical analysis has been contacted by Dr Filippidis (Department of
Primary Care and Public Health Imperial College London UK) All
authors had full access to all the data in the study and had final respon-
sibility for the decision to submit for publication Contributor Torben
Bjerregaard Larsen his institution has received payment for enrolling trial
participants from Janssen Scientific Affairs LLC and Boehringer Ingelheim
and he has been on the speaker bureaus for Bayer BMSPfizer Roche
Diagnostics Boehringer Ingelheim and Takeda Pharma
ACKNOWLEDGMENTContributor Torben Bjerregaard Larsen Aalborg University Hospital
Department of Cardiology Aalborg Thrombosis Research Unit Denmark
(data collection)
STUDY FUNDINGSupported by Imperial College London St Maryrsquos development fund
and National Institute for Health Research Imperial Biomedical Research
Centre The sponsor of the study had no role in study design data
collection data analysis data interpretation or writing of the report
Celine S Gathier was supported by the Dutch Heart Foundation grant
2009B046 Joan Martiacute-Fagravebregas was supported by the Spanish Ministry
of Health-Instituto de Salud Carlos III Redes temaacuteticas de Investigacioacuten
Cooperativa INVICTUS RD01200140002 and Fondo Europeo de
Desarrollo Regional Jiming Fang the Ontario Stroke Registry is funded
by the Canadian Stroke Network (CSN) and the Ontario Ministry of
Health and Long-Term Care (MOHLTC) This study was supported by
the Institute for Clinical Evaluative Sciences (ICES) which is funded by
an annual grant from the Ontario MOHLTC The opinions results and
conclusions reported in this paper are those of the authors and are inde-
pendent from the funding sources No endorsement by ICES or the
Ontario MOHLTC is intended or should be inferred
DISCLOSUREE Korompoki and F Filippidis report no disclosures relevant to the man-
uscript P Nielsen speaker for Boehringer Ingelheim consultant for
Bayer Pharma AS and BMSPfizer unrestricted research grant from
BMSPfizer A Del Giudice reports no disclosures relevant to the man-
uscript G Lip consultant for BayerJanssen BMSPfizer Biotronik
Medtronic Boehringer Ingelheim Microlife and Daiichi-Sankyo
speaker for Bayer BMSPfizer Medtronic Boehringer Ingelheim Micro-
life Roche and Daiichi-Sankyo J Kuramatsu reports no conflicts of
interest related to manuscript Unrelated potential conflicts of interest
travel grants from EMCools Otsuka and Boehringer Ingelheim and
speaker honoraria from Otsuka H Huttner reports no conflicts of inter-
est related to manuscript Unrelated potential conflicts of interest consul-
ting speaker honoraria and research support from Boehringer Ingelheim
Pfizer Biogen Medtronic and Novartis J Fang reports no disclosures
relevant to the manuscript S Schulman reports no conflicts of interest
related to manuscript Unrelated potential conflicts of interest honoraria
research support from Baxter Bayer Boehringer Ingelheim Daichii
694 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Sankyo Octapharma and Sanofi J Martiacute-Fagravebregas C Gathier
A Viswanathan A Biffi D Poli C Weimar and U Malzahn report
no disclosures relevant to the manuscript P Heuschmann research
grants from BMBF European Union Chariteacute Berlin Chamber of Physi-
cians German Parkinson Society University Hospital Wuumlrzburg
Robert-Koch-Institute German Heart Foundation Chariteacutendash
Universitaumltsmedizin Berlin (MonDAFIS unrestricted research grant to
Chariteacute from Bayer) University Goumlttingen (FIND-AFrandomized
unrestricted research grant to University Goumlttingen from Boehringer
Ingelheim) and University Hospital Heidelberg (RASUNOA-prime
unrestricted research grant to University Hospital Heidelberg from Bayer
BMS Boehringer Daiichi Sankyo) R Veltkamp consulting speaker
honoraria research support from Bayer Boehringer Daiichi Sankyo
BMS Pfizer Portola Biogen Amgen Morphosys Medtronic and
Apoplex Medical Technologies Go to Neurologyorg for full disclosures
Received December 29 2016 Accepted in final form May 23 2017
REFERENCES1 Camm AJ Lip GY De Caterina R et al 2012 Focused
update of the ESC guidelines for the management of atrial
fibrillation an update of the 2010 ESC guidelines for the
management of atrial fibrillation developed with the spe-
cial contribution of the European Heart Rhythm Associa-
tion Eur Heart J 2012332719ndash2747
2 Olesen JB Lip GY Hansen ML et al Validation of risk
stratification schemes for predicting stroke and thrombo-
embolism in patients with atrial fibrillation nationwide
cohort study BMJ 2011342d124
3 Flynn RW MacDonald TM Murray GD Doney AS
Systematic review of observational research studying the
long-term use of antithrombotic medicines following
intracerebral hemorrhage Cardiovasc Ther 201028
177ndash184
4 Poon MT Fonville AF Al-Shahi Salman R Long-term
prognosis after intracerebral haemorrhage systematic
review and meta-analysis J Neurol Neurosurg Psychiatry
201485660ndash667
5 Pisters R Lane DA Nieuwlaat R de Vos CB Crijns HJ
Lip GY A novel user-friendly score (HAS-BLED) to assess
1-year risk of major bleeding in patients with atrial fibrilla-
tion the Euro Heart Survey Chest 20101381093ndash1100
6 Hemphill JC III Greenberg SM Anderson CS et al
Guidelines for the management of spontaneous intracere-
bral hemorrhage a guideline for healthcare professionals
from the American Heart AssociationAmerican Stroke
Association Stroke 2015462032ndash2060
7 Steiner T Al-Shahi Salman R Beer R et al European
Stroke Organisation (ESO) guidelines for the management
of spontaneous intracerebral hemorrhage Int J Stroke
20149840ndash855
8 Liberati A Altman DG Tetzlaff J et al The PRISMA state-
ment for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions explanation
and elaboration J Clin Epidemiol 200962e1ndashe34
9 Nielsen PB Larsen TB Skjoth F Gorst-Rasmussen A
Rasmussen LH Lip GY Restarting anticoagulant treat-
ment after intracranial haemorrhage in patients with atrial
fibrillation and the impact on recurrent stroke mortality
and bleeding a nationwide cohort study Circulation
2015132517ndash525
10 Higgins JPT Altman DG Assessing Risk of Bias in
Included Studies Chichester Wiley 2008
11 DerSimonian R Laird N Meta-analysis in clinical trials
Control Clin Trials 19867177ndash188
12 Stamplecoski M Fang J Kapral MK Silver FL Long-term
outcomes of elderly patients with intracerebral hemorrhage
and atrial fibrillation Stroke 201445(s1)ATMP103
13 Viswanathan A Rakich SM Engel C et al Antiplatelet use
after intracerebral hemorrhage Neurology 200666206ndash209
14 Gathier CS Algra A Rinkel GJ van der Worp HB Long-
term outcome after anticoagulation-associated intracerebral
haemorrhage with or without restarting antithrombotic
therapy Cerebrovasc Dis 20133633ndash37
15 Kuramatsu JB Gerner ST Schellinger PD et al Antico-
agulant reversal blood pressure levels and anticoagulant
resumption in patients with anticoagulation-related intra-
cerebral hemorrhage JAMA 2015313824ndash836
16 Majeed A Kim YK Roberts RS Holmstrom M Schulman
S Optimal timing of resumption of warfarin after intracranial
hemorrhage Stroke 2010412860ndash2866
17 Vidal-Jordana A Barroeta-Espar I Sainz Pelayo MP
Mateo J Delgado-Mederos R Marti-Fabregas J Intracerebral
hemorrhage in anticoagulated patients what do we do after-
wards [in Spanish] Neurologia 201227136ndash142
18 Horstmann S Rizos T Jenetzky E Gumbinger C Hacke W
Veltkamp R Prevalence of atrial fibrillation in intracerebral
hemorrhage Eur J Neurol 201421570ndash576
19 Andersen KK Olsen TS Dehlendorff C Kammersgaard LP
Hemorrhagic and ischemic strokes compared stroke severity
mortality and risk factors Stroke 2009402068ndash2072
20 Paciaroni M Agnelli G Should oral anticoagulants be
restarted after warfarin-associated cerebral haemorrhage
in patients with atrial fibrillation Thromb Haemost
201411114ndash18
21 Eckman MH Rosand J Knudsen KA Singer DE
Greenberg SM Can patients be anticoagulated after
intracerebral hemorrhage A decision analysis Stroke
2004341710ndash1716
22 Lip GY Andreotti F Fauchier L et al Bleeding risk assess-
ment and management in atrial fibrillation patients a position
document from the European Heart Rhythm Association
endorsed by the European Society of Cardiology Working
Group on Thrombosis Europace 201113723ndash746
23 Goldstein JN Greenberg SM Should anticoagulation be
resumed after intracerebral hemorrhage Cleve Clin J Med
201077791ndash799
24 Molina CA Selim MH The dilemma of resuming anti-
coagulation after intracranial hemorrhage little evidence
facing big fears Stroke 2011423665ndash3666
25 Pasquini M Charidimou A van Asch CJ et al Variation in
restarting antithrombotic drugs at hospital discharge after
intracerebral hemorrhage Stroke 2014452643ndash2648
26 Maeda K Koga M Okada Y et al Nationwide survey of
neuro-specialistsrsquo opinions on anticoagulant therapy after
intracerebral hemorrhage in patients with atrial fibrillation
J Neurol Sci 201231282ndash85
27 Hart RG Pearce LA Aguilar MI Meta-analysis antith-
rombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation Ann Intern Med 2007146
857ndash867
28 Chao TF Liu CJ Liao JN et al Use of oral anticoagulants
for stroke prevention in patients with atrial fibrillation who
have a history of intracranial hemorrhage Circulation
20161331540ndash1547
29 Pennlert J Overholser R Asplund K et al Optimal timing
of anticoagulant treatment after intracerebral hemorrhage
in patients with atrial fibrillation Stroke 201748
314ndash320
Neurology 89 August 15 2017 695
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Figure 2 Pooled RR meta-analyses for IS that occurred between 6 weeks and 1 year of follow-up afterexposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval IS 5 ischemic stroke IV 5 inverse variance RR 5 rate ratio VKA 5
vitamin K antagonist
Neurology 89 August 15 2017 691
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Figure 3 Pooled RRmeta-analyses for ICH recurrence that occurred between 6 weeks and 1 year of follow-upafter exposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval ICH 5 intracranial hemorrhage IV5 inverse variance RR 5 rate ratioVKA 5 vitamin K antagonist
692 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reinitiation of warfarin in Taiwanese ICH survivorswith AF was beneficial One study modeling risks andbenefits calculated a net benefit of VKA for Asianpatients with ICH with a CHA2DS2-VASc score$6 but this threshold was likely to be lower withdirect OACs (DOACs)28 In our analysis whichincluded mainly white patients with ICH the medianCHADS2 score was 2 suggesting that starting OACafter ICH may be beneficial with only moderatethromboembolic risk
We found no significantly increased risk for recur-rent ICH with VKA although the point estimate forthe pooled RR was 23 to 32 higher compared tono-VKA and no-ATM Previous research showed thatICH survivors carry a significant risk of recurrentICHe5e7e8 whereas studies found no increased riskof ICH recurrencee10 when they were treated withanticoagulants after the index event Only earlyresumption of VKAs after warfarin-associated ICHincreased the risk of recurrent ICH16 A recent Swed-ish nationwide cohort study suggests that anticoagu-lant treatment may be initiated 7 to 8 weeks afterICH in intracerebral hemorrhage survivors with AFto balance benefit from treatment against the risk ofrebleeding29 In our meta-regression analysis the tim-ing of resumption failed to explain the lack of a sig-nificant difference for recurrent ICH betweenanticoagulated and nonanticoagulated patients butearly recurrent bleeding events were not captured inour study design
OAC has a net clinical benefit in patients with AFwithout ICH30 Considering the significant decreasein the rate of IS with anticoagulants a treatmentoption that provides a better safety profile thanVKA may provide a net clinical benefit also topatients with ICH DOACs have a favorable risk-benefit profile compared to VKA resulting in a reduc-tion in stroke and mortality31 In particular DOACsare uniformly associated with a 50 reduced risk ofICH compared to VKA32 Limited information froma recent study based on national Danish registriessupports this assumption33 Moreover apixaban sig-nificantly reduced the risk of stroke and systemicembolism compared to aspirin without increasingthe risk of ICH in A Phase III Study of Apixabanin Patients With Atrial Fibrillation (AVERROES)34
Therefore DOACs could be a better alternative forpatients with ICH and AF The ongoing ApixabanVersus Antiplatelet Drugs or no AntithromboticDrugs After Anticoagulation-Associated IntracerebralHaemorrhage in Patients With Atrial Fibrillation(APACHE-AF) pilot study (ClinicalTrialsgovNCT02565693) addresses stroke prevention withDOACs in ICH survivors with AF Nonpharmaco-logic prevention strategies including left atrialappendage occlusion could be an alternative but
the evidence for this intervention in ICH survivorswith AF is limited13536
In addition to relative risks decision making fora specific antithrombotic therapy has to take the abso-lute risks for ischemic and hemorrhagic events intoaccount A previous meta-analysis reported an annualrisk of recurrent intracerebral hemorrhage of 13 to744 whereas a prospective cohort study of patientswith AF on VKA after ICH reported an ICH recur-rence rate of 185 per person-year and no ISe5 In ourstudy VKA users had a 04 to 09 higher pooledannual rate of ICH recurrence compared to the othertreatment groups On the contrary the pooled annualevent rate for IS was much lower in patients on VKA(32 per 100 patient-years) compared to the othertreatment groups (APA 95 per 100 patient-yearsno-ATM 61 per 100 patient-years) Although thesedata suggest a reduction of combined ischemic andhemorrhagic stroke event rates by VKA they do notaccount for the different mortality and morbidity re-sulting from these different types of stroke
Current American Heart Association guidelinesrecommend that APA monotherapy after any ICHmight be considered and can be a reasonable alterna-tive in patients with lobar hemorrhage in whomOAC should be avoided6 The findings of the presentmeta-analysis do not support the use of APA for ISprevention because no effect on prevention of throm-boembolic events was observed in patients with AFand ICH Although older research found a smallerbleeding risk on APAs compared to VKAs37 the rateof ICH on aspirin was similar to that of well-managedVKAs38 or DOACs34 However the risk-benefit ratioof APA in ICH survivors with AF was unclear Thecurrent analysis suggests that APAs do not increasethe risk of ICH recurrence compared to VKAs or no-ATM
Our systematic review and meta-analysis wasbased on a comprehensive search strategy that aimedto provide pooled estimates for IS and ICH recur-rence in ICH survivors with AF after different preven-tion strategies Thus we can anticipate a low rate ofunderdetection An important limitation of this largemeta-analysis is the limited data quality of the mostlyretrospective studies For example 3 studies relied oncohorts of patients derived from large national regis-tries that use ICD-10 codes for medical diagnosisand Anatomical Therapeutic Chemical classificationsystem codes to identify ATM Because some deathsmay be due to undiagnosed stroke and some minorstrokes may have remained undetected the risk ofIS may be underreported Using a 6-week landmarkapproach we did not take into account bleeding com-plications related to the index ICH that may havebeen misclassified as ICH recurrences Likewise itis uncertain how many of the early recurrences were
Neurology 89 August 15 2017 693
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
truly new events or just an extension of the initialbleeding site9 The included studies are highly proneto selection bias and confounding by indicationbecause treating physicians may have avoided theuse of VKAs in patients perceived to be at higher riskof recurrence Hence unmeasured selection bias islikely in that we were unable to calculate adjustedincidence RRs because individual patient data werenot available in all studies We summarized aggre-gated treatment group differences (baseline character-istics and comorbidities) (table e-5) for each studythat may facilitate the interpretation of the results(table e-6) As previously shown baseline adjustmentin the setting of time-dependent exposure of treat-ment regimens only marginally affects outcomes asso-ciated with treatment9 This may indicate that otherreasons (besides the measure and included variables)have affected the decision of resuming OAC treat-ment This highlights the importance of meticulousinterpretation of the associations because indicationbias was likely present in all of the included studiesAnother limitation is that we did not have informationon either the time in therapeutic range for patientstaking VKAs or the quality of blood pressure control39
We also did not have data on dropout and rates anddirections of switch between different antithrombotictreatment strategies The number of studies includedin the meta-analysis was small therefore meta-regression and publication bias assessments may havebeen underpowered and should be interpreted withcaution Our study focused on IS and ICH as the mainoutcome events This approach may not provide thefull picture of outcome events and other factors affect-ing the net clinical benefit The 2 largest includedstudies showed a significant decrease of mortality inpatients treated with VKAs915 Because we censoredpatients after either IS or ICH we did not capturepotential multiple outcome events in individual pa-tients although ICH and IS are competing riskAnother limitation is that further subgroup analysesin terms of risk factors for ICH recurrence such aslobar vs deep hemorrhage topography leukoaraiosisand cerebral microbleed burden were not feasiblebecause this information was missing in several studiesIn addition comorbidities apart from AF (eg coro-nary artery disease) indicating the use of antiplateletswere not addressed
This meta-analysis of antithrombotic treatment inVKA-associated ICH survivors with AF suggests thatanticoagulation with VKA is associated with a lowerrate of IS compared to other or no antithromboticswithout causing a major increase of the risk of ICHrecurrence whereas antiplatelets fail to prevent ISBecause of the limitations of observational studiesa randomized controlled trial of antithrombotictherapy preferably with DOACs used as the
anticoagulants is needed to better guide decision mak-ing for antithrombotic therapy in patients with ICHand AF
AUTHOR CONTRIBUTIONSEleni Korompoki study concept data collection drafting and critical revi-
sion of manuscript Filippos T Filippidis study concept statistical analysis
data collection drafting and critical revision of manuscript Peter B Nielsen
study concept data collection and critical revision of manuscript
Angela Del Giudice Gregory Y Lip Joji Kuramatsu Hagen Huttner
Jiming Fang Sam Schulman Joan Martiacute-Fagravebregas Celine S Gathier
Anand Viswanathan Alessandro Biffi Daniela Poli and Christian
Weimar data collection and critical revision of manuscript Uwe
Malzahn and Peter Heuschmann critical review of manuscript Roland
Veltkamp study concept and financial support drafting and critical
revision of manuscript All authors have read and approved the final form
of the manuscript and have agreed to conditions noted on the authorship
agreement The principal author has taken full responsibility for the data
the analyses and the interpretation and the conduct of the research The
statistical analysis has been contacted by Dr Filippidis (Department of
Primary Care and Public Health Imperial College London UK) All
authors had full access to all the data in the study and had final respon-
sibility for the decision to submit for publication Contributor Torben
Bjerregaard Larsen his institution has received payment for enrolling trial
participants from Janssen Scientific Affairs LLC and Boehringer Ingelheim
and he has been on the speaker bureaus for Bayer BMSPfizer Roche
Diagnostics Boehringer Ingelheim and Takeda Pharma
ACKNOWLEDGMENTContributor Torben Bjerregaard Larsen Aalborg University Hospital
Department of Cardiology Aalborg Thrombosis Research Unit Denmark
(data collection)
STUDY FUNDINGSupported by Imperial College London St Maryrsquos development fund
and National Institute for Health Research Imperial Biomedical Research
Centre The sponsor of the study had no role in study design data
collection data analysis data interpretation or writing of the report
Celine S Gathier was supported by the Dutch Heart Foundation grant
2009B046 Joan Martiacute-Fagravebregas was supported by the Spanish Ministry
of Health-Instituto de Salud Carlos III Redes temaacuteticas de Investigacioacuten
Cooperativa INVICTUS RD01200140002 and Fondo Europeo de
Desarrollo Regional Jiming Fang the Ontario Stroke Registry is funded
by the Canadian Stroke Network (CSN) and the Ontario Ministry of
Health and Long-Term Care (MOHLTC) This study was supported by
the Institute for Clinical Evaluative Sciences (ICES) which is funded by
an annual grant from the Ontario MOHLTC The opinions results and
conclusions reported in this paper are those of the authors and are inde-
pendent from the funding sources No endorsement by ICES or the
Ontario MOHLTC is intended or should be inferred
DISCLOSUREE Korompoki and F Filippidis report no disclosures relevant to the man-
uscript P Nielsen speaker for Boehringer Ingelheim consultant for
Bayer Pharma AS and BMSPfizer unrestricted research grant from
BMSPfizer A Del Giudice reports no disclosures relevant to the man-
uscript G Lip consultant for BayerJanssen BMSPfizer Biotronik
Medtronic Boehringer Ingelheim Microlife and Daiichi-Sankyo
speaker for Bayer BMSPfizer Medtronic Boehringer Ingelheim Micro-
life Roche and Daiichi-Sankyo J Kuramatsu reports no conflicts of
interest related to manuscript Unrelated potential conflicts of interest
travel grants from EMCools Otsuka and Boehringer Ingelheim and
speaker honoraria from Otsuka H Huttner reports no conflicts of inter-
est related to manuscript Unrelated potential conflicts of interest consul-
ting speaker honoraria and research support from Boehringer Ingelheim
Pfizer Biogen Medtronic and Novartis J Fang reports no disclosures
relevant to the manuscript S Schulman reports no conflicts of interest
related to manuscript Unrelated potential conflicts of interest honoraria
research support from Baxter Bayer Boehringer Ingelheim Daichii
694 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Sankyo Octapharma and Sanofi J Martiacute-Fagravebregas C Gathier
A Viswanathan A Biffi D Poli C Weimar and U Malzahn report
no disclosures relevant to the manuscript P Heuschmann research
grants from BMBF European Union Chariteacute Berlin Chamber of Physi-
cians German Parkinson Society University Hospital Wuumlrzburg
Robert-Koch-Institute German Heart Foundation Chariteacutendash
Universitaumltsmedizin Berlin (MonDAFIS unrestricted research grant to
Chariteacute from Bayer) University Goumlttingen (FIND-AFrandomized
unrestricted research grant to University Goumlttingen from Boehringer
Ingelheim) and University Hospital Heidelberg (RASUNOA-prime
unrestricted research grant to University Hospital Heidelberg from Bayer
BMS Boehringer Daiichi Sankyo) R Veltkamp consulting speaker
honoraria research support from Bayer Boehringer Daiichi Sankyo
BMS Pfizer Portola Biogen Amgen Morphosys Medtronic and
Apoplex Medical Technologies Go to Neurologyorg for full disclosures
Received December 29 2016 Accepted in final form May 23 2017
REFERENCES1 Camm AJ Lip GY De Caterina R et al 2012 Focused
update of the ESC guidelines for the management of atrial
fibrillation an update of the 2010 ESC guidelines for the
management of atrial fibrillation developed with the spe-
cial contribution of the European Heart Rhythm Associa-
tion Eur Heart J 2012332719ndash2747
2 Olesen JB Lip GY Hansen ML et al Validation of risk
stratification schemes for predicting stroke and thrombo-
embolism in patients with atrial fibrillation nationwide
cohort study BMJ 2011342d124
3 Flynn RW MacDonald TM Murray GD Doney AS
Systematic review of observational research studying the
long-term use of antithrombotic medicines following
intracerebral hemorrhage Cardiovasc Ther 201028
177ndash184
4 Poon MT Fonville AF Al-Shahi Salman R Long-term
prognosis after intracerebral haemorrhage systematic
review and meta-analysis J Neurol Neurosurg Psychiatry
201485660ndash667
5 Pisters R Lane DA Nieuwlaat R de Vos CB Crijns HJ
Lip GY A novel user-friendly score (HAS-BLED) to assess
1-year risk of major bleeding in patients with atrial fibrilla-
tion the Euro Heart Survey Chest 20101381093ndash1100
6 Hemphill JC III Greenberg SM Anderson CS et al
Guidelines for the management of spontaneous intracere-
bral hemorrhage a guideline for healthcare professionals
from the American Heart AssociationAmerican Stroke
Association Stroke 2015462032ndash2060
7 Steiner T Al-Shahi Salman R Beer R et al European
Stroke Organisation (ESO) guidelines for the management
of spontaneous intracerebral hemorrhage Int J Stroke
20149840ndash855
8 Liberati A Altman DG Tetzlaff J et al The PRISMA state-
ment for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions explanation
and elaboration J Clin Epidemiol 200962e1ndashe34
9 Nielsen PB Larsen TB Skjoth F Gorst-Rasmussen A
Rasmussen LH Lip GY Restarting anticoagulant treat-
ment after intracranial haemorrhage in patients with atrial
fibrillation and the impact on recurrent stroke mortality
and bleeding a nationwide cohort study Circulation
2015132517ndash525
10 Higgins JPT Altman DG Assessing Risk of Bias in
Included Studies Chichester Wiley 2008
11 DerSimonian R Laird N Meta-analysis in clinical trials
Control Clin Trials 19867177ndash188
12 Stamplecoski M Fang J Kapral MK Silver FL Long-term
outcomes of elderly patients with intracerebral hemorrhage
and atrial fibrillation Stroke 201445(s1)ATMP103
13 Viswanathan A Rakich SM Engel C et al Antiplatelet use
after intracerebral hemorrhage Neurology 200666206ndash209
14 Gathier CS Algra A Rinkel GJ van der Worp HB Long-
term outcome after anticoagulation-associated intracerebral
haemorrhage with or without restarting antithrombotic
therapy Cerebrovasc Dis 20133633ndash37
15 Kuramatsu JB Gerner ST Schellinger PD et al Antico-
agulant reversal blood pressure levels and anticoagulant
resumption in patients with anticoagulation-related intra-
cerebral hemorrhage JAMA 2015313824ndash836
16 Majeed A Kim YK Roberts RS Holmstrom M Schulman
S Optimal timing of resumption of warfarin after intracranial
hemorrhage Stroke 2010412860ndash2866
17 Vidal-Jordana A Barroeta-Espar I Sainz Pelayo MP
Mateo J Delgado-Mederos R Marti-Fabregas J Intracerebral
hemorrhage in anticoagulated patients what do we do after-
wards [in Spanish] Neurologia 201227136ndash142
18 Horstmann S Rizos T Jenetzky E Gumbinger C Hacke W
Veltkamp R Prevalence of atrial fibrillation in intracerebral
hemorrhage Eur J Neurol 201421570ndash576
19 Andersen KK Olsen TS Dehlendorff C Kammersgaard LP
Hemorrhagic and ischemic strokes compared stroke severity
mortality and risk factors Stroke 2009402068ndash2072
20 Paciaroni M Agnelli G Should oral anticoagulants be
restarted after warfarin-associated cerebral haemorrhage
in patients with atrial fibrillation Thromb Haemost
201411114ndash18
21 Eckman MH Rosand J Knudsen KA Singer DE
Greenberg SM Can patients be anticoagulated after
intracerebral hemorrhage A decision analysis Stroke
2004341710ndash1716
22 Lip GY Andreotti F Fauchier L et al Bleeding risk assess-
ment and management in atrial fibrillation patients a position
document from the European Heart Rhythm Association
endorsed by the European Society of Cardiology Working
Group on Thrombosis Europace 201113723ndash746
23 Goldstein JN Greenberg SM Should anticoagulation be
resumed after intracerebral hemorrhage Cleve Clin J Med
201077791ndash799
24 Molina CA Selim MH The dilemma of resuming anti-
coagulation after intracranial hemorrhage little evidence
facing big fears Stroke 2011423665ndash3666
25 Pasquini M Charidimou A van Asch CJ et al Variation in
restarting antithrombotic drugs at hospital discharge after
intracerebral hemorrhage Stroke 2014452643ndash2648
26 Maeda K Koga M Okada Y et al Nationwide survey of
neuro-specialistsrsquo opinions on anticoagulant therapy after
intracerebral hemorrhage in patients with atrial fibrillation
J Neurol Sci 201231282ndash85
27 Hart RG Pearce LA Aguilar MI Meta-analysis antith-
rombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation Ann Intern Med 2007146
857ndash867
28 Chao TF Liu CJ Liao JN et al Use of oral anticoagulants
for stroke prevention in patients with atrial fibrillation who
have a history of intracranial hemorrhage Circulation
20161331540ndash1547
29 Pennlert J Overholser R Asplund K et al Optimal timing
of anticoagulant treatment after intracerebral hemorrhage
in patients with atrial fibrillation Stroke 201748
314ndash320
Neurology 89 August 15 2017 695
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Figure 3 Pooled RRmeta-analyses for ICH recurrence that occurred between 6 weeks and 1 year of follow-upafter exposure to different treatment strategies
(A) VKA vs no-VKA (B) VKA vs APA (C) VKA vs no-ATM and (D) APA vs no-ATM APA 5 antiplatelet agent ATM 5
antithrombotic medication CI 5 confidence interval ICH 5 intracranial hemorrhage IV5 inverse variance RR 5 rate ratioVKA 5 vitamin K antagonist
692 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reinitiation of warfarin in Taiwanese ICH survivorswith AF was beneficial One study modeling risks andbenefits calculated a net benefit of VKA for Asianpatients with ICH with a CHA2DS2-VASc score$6 but this threshold was likely to be lower withdirect OACs (DOACs)28 In our analysis whichincluded mainly white patients with ICH the medianCHADS2 score was 2 suggesting that starting OACafter ICH may be beneficial with only moderatethromboembolic risk
We found no significantly increased risk for recur-rent ICH with VKA although the point estimate forthe pooled RR was 23 to 32 higher compared tono-VKA and no-ATM Previous research showed thatICH survivors carry a significant risk of recurrentICHe5e7e8 whereas studies found no increased riskof ICH recurrencee10 when they were treated withanticoagulants after the index event Only earlyresumption of VKAs after warfarin-associated ICHincreased the risk of recurrent ICH16 A recent Swed-ish nationwide cohort study suggests that anticoagu-lant treatment may be initiated 7 to 8 weeks afterICH in intracerebral hemorrhage survivors with AFto balance benefit from treatment against the risk ofrebleeding29 In our meta-regression analysis the tim-ing of resumption failed to explain the lack of a sig-nificant difference for recurrent ICH betweenanticoagulated and nonanticoagulated patients butearly recurrent bleeding events were not captured inour study design
OAC has a net clinical benefit in patients with AFwithout ICH30 Considering the significant decreasein the rate of IS with anticoagulants a treatmentoption that provides a better safety profile thanVKA may provide a net clinical benefit also topatients with ICH DOACs have a favorable risk-benefit profile compared to VKA resulting in a reduc-tion in stroke and mortality31 In particular DOACsare uniformly associated with a 50 reduced risk ofICH compared to VKA32 Limited information froma recent study based on national Danish registriessupports this assumption33 Moreover apixaban sig-nificantly reduced the risk of stroke and systemicembolism compared to aspirin without increasingthe risk of ICH in A Phase III Study of Apixabanin Patients With Atrial Fibrillation (AVERROES)34
Therefore DOACs could be a better alternative forpatients with ICH and AF The ongoing ApixabanVersus Antiplatelet Drugs or no AntithromboticDrugs After Anticoagulation-Associated IntracerebralHaemorrhage in Patients With Atrial Fibrillation(APACHE-AF) pilot study (ClinicalTrialsgovNCT02565693) addresses stroke prevention withDOACs in ICH survivors with AF Nonpharmaco-logic prevention strategies including left atrialappendage occlusion could be an alternative but
the evidence for this intervention in ICH survivorswith AF is limited13536
In addition to relative risks decision making fora specific antithrombotic therapy has to take the abso-lute risks for ischemic and hemorrhagic events intoaccount A previous meta-analysis reported an annualrisk of recurrent intracerebral hemorrhage of 13 to744 whereas a prospective cohort study of patientswith AF on VKA after ICH reported an ICH recur-rence rate of 185 per person-year and no ISe5 In ourstudy VKA users had a 04 to 09 higher pooledannual rate of ICH recurrence compared to the othertreatment groups On the contrary the pooled annualevent rate for IS was much lower in patients on VKA(32 per 100 patient-years) compared to the othertreatment groups (APA 95 per 100 patient-yearsno-ATM 61 per 100 patient-years) Although thesedata suggest a reduction of combined ischemic andhemorrhagic stroke event rates by VKA they do notaccount for the different mortality and morbidity re-sulting from these different types of stroke
Current American Heart Association guidelinesrecommend that APA monotherapy after any ICHmight be considered and can be a reasonable alterna-tive in patients with lobar hemorrhage in whomOAC should be avoided6 The findings of the presentmeta-analysis do not support the use of APA for ISprevention because no effect on prevention of throm-boembolic events was observed in patients with AFand ICH Although older research found a smallerbleeding risk on APAs compared to VKAs37 the rateof ICH on aspirin was similar to that of well-managedVKAs38 or DOACs34 However the risk-benefit ratioof APA in ICH survivors with AF was unclear Thecurrent analysis suggests that APAs do not increasethe risk of ICH recurrence compared to VKAs or no-ATM
Our systematic review and meta-analysis wasbased on a comprehensive search strategy that aimedto provide pooled estimates for IS and ICH recur-rence in ICH survivors with AF after different preven-tion strategies Thus we can anticipate a low rate ofunderdetection An important limitation of this largemeta-analysis is the limited data quality of the mostlyretrospective studies For example 3 studies relied oncohorts of patients derived from large national regis-tries that use ICD-10 codes for medical diagnosisand Anatomical Therapeutic Chemical classificationsystem codes to identify ATM Because some deathsmay be due to undiagnosed stroke and some minorstrokes may have remained undetected the risk ofIS may be underreported Using a 6-week landmarkapproach we did not take into account bleeding com-plications related to the index ICH that may havebeen misclassified as ICH recurrences Likewise itis uncertain how many of the early recurrences were
Neurology 89 August 15 2017 693
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
truly new events or just an extension of the initialbleeding site9 The included studies are highly proneto selection bias and confounding by indicationbecause treating physicians may have avoided theuse of VKAs in patients perceived to be at higher riskof recurrence Hence unmeasured selection bias islikely in that we were unable to calculate adjustedincidence RRs because individual patient data werenot available in all studies We summarized aggre-gated treatment group differences (baseline character-istics and comorbidities) (table e-5) for each studythat may facilitate the interpretation of the results(table e-6) As previously shown baseline adjustmentin the setting of time-dependent exposure of treat-ment regimens only marginally affects outcomes asso-ciated with treatment9 This may indicate that otherreasons (besides the measure and included variables)have affected the decision of resuming OAC treat-ment This highlights the importance of meticulousinterpretation of the associations because indicationbias was likely present in all of the included studiesAnother limitation is that we did not have informationon either the time in therapeutic range for patientstaking VKAs or the quality of blood pressure control39
We also did not have data on dropout and rates anddirections of switch between different antithrombotictreatment strategies The number of studies includedin the meta-analysis was small therefore meta-regression and publication bias assessments may havebeen underpowered and should be interpreted withcaution Our study focused on IS and ICH as the mainoutcome events This approach may not provide thefull picture of outcome events and other factors affect-ing the net clinical benefit The 2 largest includedstudies showed a significant decrease of mortality inpatients treated with VKAs915 Because we censoredpatients after either IS or ICH we did not capturepotential multiple outcome events in individual pa-tients although ICH and IS are competing riskAnother limitation is that further subgroup analysesin terms of risk factors for ICH recurrence such aslobar vs deep hemorrhage topography leukoaraiosisand cerebral microbleed burden were not feasiblebecause this information was missing in several studiesIn addition comorbidities apart from AF (eg coro-nary artery disease) indicating the use of antiplateletswere not addressed
This meta-analysis of antithrombotic treatment inVKA-associated ICH survivors with AF suggests thatanticoagulation with VKA is associated with a lowerrate of IS compared to other or no antithromboticswithout causing a major increase of the risk of ICHrecurrence whereas antiplatelets fail to prevent ISBecause of the limitations of observational studiesa randomized controlled trial of antithrombotictherapy preferably with DOACs used as the
anticoagulants is needed to better guide decision mak-ing for antithrombotic therapy in patients with ICHand AF
AUTHOR CONTRIBUTIONSEleni Korompoki study concept data collection drafting and critical revi-
sion of manuscript Filippos T Filippidis study concept statistical analysis
data collection drafting and critical revision of manuscript Peter B Nielsen
study concept data collection and critical revision of manuscript
Angela Del Giudice Gregory Y Lip Joji Kuramatsu Hagen Huttner
Jiming Fang Sam Schulman Joan Martiacute-Fagravebregas Celine S Gathier
Anand Viswanathan Alessandro Biffi Daniela Poli and Christian
Weimar data collection and critical revision of manuscript Uwe
Malzahn and Peter Heuschmann critical review of manuscript Roland
Veltkamp study concept and financial support drafting and critical
revision of manuscript All authors have read and approved the final form
of the manuscript and have agreed to conditions noted on the authorship
agreement The principal author has taken full responsibility for the data
the analyses and the interpretation and the conduct of the research The
statistical analysis has been contacted by Dr Filippidis (Department of
Primary Care and Public Health Imperial College London UK) All
authors had full access to all the data in the study and had final respon-
sibility for the decision to submit for publication Contributor Torben
Bjerregaard Larsen his institution has received payment for enrolling trial
participants from Janssen Scientific Affairs LLC and Boehringer Ingelheim
and he has been on the speaker bureaus for Bayer BMSPfizer Roche
Diagnostics Boehringer Ingelheim and Takeda Pharma
ACKNOWLEDGMENTContributor Torben Bjerregaard Larsen Aalborg University Hospital
Department of Cardiology Aalborg Thrombosis Research Unit Denmark
(data collection)
STUDY FUNDINGSupported by Imperial College London St Maryrsquos development fund
and National Institute for Health Research Imperial Biomedical Research
Centre The sponsor of the study had no role in study design data
collection data analysis data interpretation or writing of the report
Celine S Gathier was supported by the Dutch Heart Foundation grant
2009B046 Joan Martiacute-Fagravebregas was supported by the Spanish Ministry
of Health-Instituto de Salud Carlos III Redes temaacuteticas de Investigacioacuten
Cooperativa INVICTUS RD01200140002 and Fondo Europeo de
Desarrollo Regional Jiming Fang the Ontario Stroke Registry is funded
by the Canadian Stroke Network (CSN) and the Ontario Ministry of
Health and Long-Term Care (MOHLTC) This study was supported by
the Institute for Clinical Evaluative Sciences (ICES) which is funded by
an annual grant from the Ontario MOHLTC The opinions results and
conclusions reported in this paper are those of the authors and are inde-
pendent from the funding sources No endorsement by ICES or the
Ontario MOHLTC is intended or should be inferred
DISCLOSUREE Korompoki and F Filippidis report no disclosures relevant to the man-
uscript P Nielsen speaker for Boehringer Ingelheim consultant for
Bayer Pharma AS and BMSPfizer unrestricted research grant from
BMSPfizer A Del Giudice reports no disclosures relevant to the man-
uscript G Lip consultant for BayerJanssen BMSPfizer Biotronik
Medtronic Boehringer Ingelheim Microlife and Daiichi-Sankyo
speaker for Bayer BMSPfizer Medtronic Boehringer Ingelheim Micro-
life Roche and Daiichi-Sankyo J Kuramatsu reports no conflicts of
interest related to manuscript Unrelated potential conflicts of interest
travel grants from EMCools Otsuka and Boehringer Ingelheim and
speaker honoraria from Otsuka H Huttner reports no conflicts of inter-
est related to manuscript Unrelated potential conflicts of interest consul-
ting speaker honoraria and research support from Boehringer Ingelheim
Pfizer Biogen Medtronic and Novartis J Fang reports no disclosures
relevant to the manuscript S Schulman reports no conflicts of interest
related to manuscript Unrelated potential conflicts of interest honoraria
research support from Baxter Bayer Boehringer Ingelheim Daichii
694 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Sankyo Octapharma and Sanofi J Martiacute-Fagravebregas C Gathier
A Viswanathan A Biffi D Poli C Weimar and U Malzahn report
no disclosures relevant to the manuscript P Heuschmann research
grants from BMBF European Union Chariteacute Berlin Chamber of Physi-
cians German Parkinson Society University Hospital Wuumlrzburg
Robert-Koch-Institute German Heart Foundation Chariteacutendash
Universitaumltsmedizin Berlin (MonDAFIS unrestricted research grant to
Chariteacute from Bayer) University Goumlttingen (FIND-AFrandomized
unrestricted research grant to University Goumlttingen from Boehringer
Ingelheim) and University Hospital Heidelberg (RASUNOA-prime
unrestricted research grant to University Hospital Heidelberg from Bayer
BMS Boehringer Daiichi Sankyo) R Veltkamp consulting speaker
honoraria research support from Bayer Boehringer Daiichi Sankyo
BMS Pfizer Portola Biogen Amgen Morphosys Medtronic and
Apoplex Medical Technologies Go to Neurologyorg for full disclosures
Received December 29 2016 Accepted in final form May 23 2017
REFERENCES1 Camm AJ Lip GY De Caterina R et al 2012 Focused
update of the ESC guidelines for the management of atrial
fibrillation an update of the 2010 ESC guidelines for the
management of atrial fibrillation developed with the spe-
cial contribution of the European Heart Rhythm Associa-
tion Eur Heart J 2012332719ndash2747
2 Olesen JB Lip GY Hansen ML et al Validation of risk
stratification schemes for predicting stroke and thrombo-
embolism in patients with atrial fibrillation nationwide
cohort study BMJ 2011342d124
3 Flynn RW MacDonald TM Murray GD Doney AS
Systematic review of observational research studying the
long-term use of antithrombotic medicines following
intracerebral hemorrhage Cardiovasc Ther 201028
177ndash184
4 Poon MT Fonville AF Al-Shahi Salman R Long-term
prognosis after intracerebral haemorrhage systematic
review and meta-analysis J Neurol Neurosurg Psychiatry
201485660ndash667
5 Pisters R Lane DA Nieuwlaat R de Vos CB Crijns HJ
Lip GY A novel user-friendly score (HAS-BLED) to assess
1-year risk of major bleeding in patients with atrial fibrilla-
tion the Euro Heart Survey Chest 20101381093ndash1100
6 Hemphill JC III Greenberg SM Anderson CS et al
Guidelines for the management of spontaneous intracere-
bral hemorrhage a guideline for healthcare professionals
from the American Heart AssociationAmerican Stroke
Association Stroke 2015462032ndash2060
7 Steiner T Al-Shahi Salman R Beer R et al European
Stroke Organisation (ESO) guidelines for the management
of spontaneous intracerebral hemorrhage Int J Stroke
20149840ndash855
8 Liberati A Altman DG Tetzlaff J et al The PRISMA state-
ment for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions explanation
and elaboration J Clin Epidemiol 200962e1ndashe34
9 Nielsen PB Larsen TB Skjoth F Gorst-Rasmussen A
Rasmussen LH Lip GY Restarting anticoagulant treat-
ment after intracranial haemorrhage in patients with atrial
fibrillation and the impact on recurrent stroke mortality
and bleeding a nationwide cohort study Circulation
2015132517ndash525
10 Higgins JPT Altman DG Assessing Risk of Bias in
Included Studies Chichester Wiley 2008
11 DerSimonian R Laird N Meta-analysis in clinical trials
Control Clin Trials 19867177ndash188
12 Stamplecoski M Fang J Kapral MK Silver FL Long-term
outcomes of elderly patients with intracerebral hemorrhage
and atrial fibrillation Stroke 201445(s1)ATMP103
13 Viswanathan A Rakich SM Engel C et al Antiplatelet use
after intracerebral hemorrhage Neurology 200666206ndash209
14 Gathier CS Algra A Rinkel GJ van der Worp HB Long-
term outcome after anticoagulation-associated intracerebral
haemorrhage with or without restarting antithrombotic
therapy Cerebrovasc Dis 20133633ndash37
15 Kuramatsu JB Gerner ST Schellinger PD et al Antico-
agulant reversal blood pressure levels and anticoagulant
resumption in patients with anticoagulation-related intra-
cerebral hemorrhage JAMA 2015313824ndash836
16 Majeed A Kim YK Roberts RS Holmstrom M Schulman
S Optimal timing of resumption of warfarin after intracranial
hemorrhage Stroke 2010412860ndash2866
17 Vidal-Jordana A Barroeta-Espar I Sainz Pelayo MP
Mateo J Delgado-Mederos R Marti-Fabregas J Intracerebral
hemorrhage in anticoagulated patients what do we do after-
wards [in Spanish] Neurologia 201227136ndash142
18 Horstmann S Rizos T Jenetzky E Gumbinger C Hacke W
Veltkamp R Prevalence of atrial fibrillation in intracerebral
hemorrhage Eur J Neurol 201421570ndash576
19 Andersen KK Olsen TS Dehlendorff C Kammersgaard LP
Hemorrhagic and ischemic strokes compared stroke severity
mortality and risk factors Stroke 2009402068ndash2072
20 Paciaroni M Agnelli G Should oral anticoagulants be
restarted after warfarin-associated cerebral haemorrhage
in patients with atrial fibrillation Thromb Haemost
201411114ndash18
21 Eckman MH Rosand J Knudsen KA Singer DE
Greenberg SM Can patients be anticoagulated after
intracerebral hemorrhage A decision analysis Stroke
2004341710ndash1716
22 Lip GY Andreotti F Fauchier L et al Bleeding risk assess-
ment and management in atrial fibrillation patients a position
document from the European Heart Rhythm Association
endorsed by the European Society of Cardiology Working
Group on Thrombosis Europace 201113723ndash746
23 Goldstein JN Greenberg SM Should anticoagulation be
resumed after intracerebral hemorrhage Cleve Clin J Med
201077791ndash799
24 Molina CA Selim MH The dilemma of resuming anti-
coagulation after intracranial hemorrhage little evidence
facing big fears Stroke 2011423665ndash3666
25 Pasquini M Charidimou A van Asch CJ et al Variation in
restarting antithrombotic drugs at hospital discharge after
intracerebral hemorrhage Stroke 2014452643ndash2648
26 Maeda K Koga M Okada Y et al Nationwide survey of
neuro-specialistsrsquo opinions on anticoagulant therapy after
intracerebral hemorrhage in patients with atrial fibrillation
J Neurol Sci 201231282ndash85
27 Hart RG Pearce LA Aguilar MI Meta-analysis antith-
rombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation Ann Intern Med 2007146
857ndash867
28 Chao TF Liu CJ Liao JN et al Use of oral anticoagulants
for stroke prevention in patients with atrial fibrillation who
have a history of intracranial hemorrhage Circulation
20161331540ndash1547
29 Pennlert J Overholser R Asplund K et al Optimal timing
of anticoagulant treatment after intracerebral hemorrhage
in patients with atrial fibrillation Stroke 201748
314ndash320
Neurology 89 August 15 2017 695
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Reinitiation of warfarin in Taiwanese ICH survivorswith AF was beneficial One study modeling risks andbenefits calculated a net benefit of VKA for Asianpatients with ICH with a CHA2DS2-VASc score$6 but this threshold was likely to be lower withdirect OACs (DOACs)28 In our analysis whichincluded mainly white patients with ICH the medianCHADS2 score was 2 suggesting that starting OACafter ICH may be beneficial with only moderatethromboembolic risk
We found no significantly increased risk for recur-rent ICH with VKA although the point estimate forthe pooled RR was 23 to 32 higher compared tono-VKA and no-ATM Previous research showed thatICH survivors carry a significant risk of recurrentICHe5e7e8 whereas studies found no increased riskof ICH recurrencee10 when they were treated withanticoagulants after the index event Only earlyresumption of VKAs after warfarin-associated ICHincreased the risk of recurrent ICH16 A recent Swed-ish nationwide cohort study suggests that anticoagu-lant treatment may be initiated 7 to 8 weeks afterICH in intracerebral hemorrhage survivors with AFto balance benefit from treatment against the risk ofrebleeding29 In our meta-regression analysis the tim-ing of resumption failed to explain the lack of a sig-nificant difference for recurrent ICH betweenanticoagulated and nonanticoagulated patients butearly recurrent bleeding events were not captured inour study design
OAC has a net clinical benefit in patients with AFwithout ICH30 Considering the significant decreasein the rate of IS with anticoagulants a treatmentoption that provides a better safety profile thanVKA may provide a net clinical benefit also topatients with ICH DOACs have a favorable risk-benefit profile compared to VKA resulting in a reduc-tion in stroke and mortality31 In particular DOACsare uniformly associated with a 50 reduced risk ofICH compared to VKA32 Limited information froma recent study based on national Danish registriessupports this assumption33 Moreover apixaban sig-nificantly reduced the risk of stroke and systemicembolism compared to aspirin without increasingthe risk of ICH in A Phase III Study of Apixabanin Patients With Atrial Fibrillation (AVERROES)34
Therefore DOACs could be a better alternative forpatients with ICH and AF The ongoing ApixabanVersus Antiplatelet Drugs or no AntithromboticDrugs After Anticoagulation-Associated IntracerebralHaemorrhage in Patients With Atrial Fibrillation(APACHE-AF) pilot study (ClinicalTrialsgovNCT02565693) addresses stroke prevention withDOACs in ICH survivors with AF Nonpharmaco-logic prevention strategies including left atrialappendage occlusion could be an alternative but
the evidence for this intervention in ICH survivorswith AF is limited13536
In addition to relative risks decision making fora specific antithrombotic therapy has to take the abso-lute risks for ischemic and hemorrhagic events intoaccount A previous meta-analysis reported an annualrisk of recurrent intracerebral hemorrhage of 13 to744 whereas a prospective cohort study of patientswith AF on VKA after ICH reported an ICH recur-rence rate of 185 per person-year and no ISe5 In ourstudy VKA users had a 04 to 09 higher pooledannual rate of ICH recurrence compared to the othertreatment groups On the contrary the pooled annualevent rate for IS was much lower in patients on VKA(32 per 100 patient-years) compared to the othertreatment groups (APA 95 per 100 patient-yearsno-ATM 61 per 100 patient-years) Although thesedata suggest a reduction of combined ischemic andhemorrhagic stroke event rates by VKA they do notaccount for the different mortality and morbidity re-sulting from these different types of stroke
Current American Heart Association guidelinesrecommend that APA monotherapy after any ICHmight be considered and can be a reasonable alterna-tive in patients with lobar hemorrhage in whomOAC should be avoided6 The findings of the presentmeta-analysis do not support the use of APA for ISprevention because no effect on prevention of throm-boembolic events was observed in patients with AFand ICH Although older research found a smallerbleeding risk on APAs compared to VKAs37 the rateof ICH on aspirin was similar to that of well-managedVKAs38 or DOACs34 However the risk-benefit ratioof APA in ICH survivors with AF was unclear Thecurrent analysis suggests that APAs do not increasethe risk of ICH recurrence compared to VKAs or no-ATM
Our systematic review and meta-analysis wasbased on a comprehensive search strategy that aimedto provide pooled estimates for IS and ICH recur-rence in ICH survivors with AF after different preven-tion strategies Thus we can anticipate a low rate ofunderdetection An important limitation of this largemeta-analysis is the limited data quality of the mostlyretrospective studies For example 3 studies relied oncohorts of patients derived from large national regis-tries that use ICD-10 codes for medical diagnosisand Anatomical Therapeutic Chemical classificationsystem codes to identify ATM Because some deathsmay be due to undiagnosed stroke and some minorstrokes may have remained undetected the risk ofIS may be underreported Using a 6-week landmarkapproach we did not take into account bleeding com-plications related to the index ICH that may havebeen misclassified as ICH recurrences Likewise itis uncertain how many of the early recurrences were
Neurology 89 August 15 2017 693
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
truly new events or just an extension of the initialbleeding site9 The included studies are highly proneto selection bias and confounding by indicationbecause treating physicians may have avoided theuse of VKAs in patients perceived to be at higher riskof recurrence Hence unmeasured selection bias islikely in that we were unable to calculate adjustedincidence RRs because individual patient data werenot available in all studies We summarized aggre-gated treatment group differences (baseline character-istics and comorbidities) (table e-5) for each studythat may facilitate the interpretation of the results(table e-6) As previously shown baseline adjustmentin the setting of time-dependent exposure of treat-ment regimens only marginally affects outcomes asso-ciated with treatment9 This may indicate that otherreasons (besides the measure and included variables)have affected the decision of resuming OAC treat-ment This highlights the importance of meticulousinterpretation of the associations because indicationbias was likely present in all of the included studiesAnother limitation is that we did not have informationon either the time in therapeutic range for patientstaking VKAs or the quality of blood pressure control39
We also did not have data on dropout and rates anddirections of switch between different antithrombotictreatment strategies The number of studies includedin the meta-analysis was small therefore meta-regression and publication bias assessments may havebeen underpowered and should be interpreted withcaution Our study focused on IS and ICH as the mainoutcome events This approach may not provide thefull picture of outcome events and other factors affect-ing the net clinical benefit The 2 largest includedstudies showed a significant decrease of mortality inpatients treated with VKAs915 Because we censoredpatients after either IS or ICH we did not capturepotential multiple outcome events in individual pa-tients although ICH and IS are competing riskAnother limitation is that further subgroup analysesin terms of risk factors for ICH recurrence such aslobar vs deep hemorrhage topography leukoaraiosisand cerebral microbleed burden were not feasiblebecause this information was missing in several studiesIn addition comorbidities apart from AF (eg coro-nary artery disease) indicating the use of antiplateletswere not addressed
This meta-analysis of antithrombotic treatment inVKA-associated ICH survivors with AF suggests thatanticoagulation with VKA is associated with a lowerrate of IS compared to other or no antithromboticswithout causing a major increase of the risk of ICHrecurrence whereas antiplatelets fail to prevent ISBecause of the limitations of observational studiesa randomized controlled trial of antithrombotictherapy preferably with DOACs used as the
anticoagulants is needed to better guide decision mak-ing for antithrombotic therapy in patients with ICHand AF
AUTHOR CONTRIBUTIONSEleni Korompoki study concept data collection drafting and critical revi-
sion of manuscript Filippos T Filippidis study concept statistical analysis
data collection drafting and critical revision of manuscript Peter B Nielsen
study concept data collection and critical revision of manuscript
Angela Del Giudice Gregory Y Lip Joji Kuramatsu Hagen Huttner
Jiming Fang Sam Schulman Joan Martiacute-Fagravebregas Celine S Gathier
Anand Viswanathan Alessandro Biffi Daniela Poli and Christian
Weimar data collection and critical revision of manuscript Uwe
Malzahn and Peter Heuschmann critical review of manuscript Roland
Veltkamp study concept and financial support drafting and critical
revision of manuscript All authors have read and approved the final form
of the manuscript and have agreed to conditions noted on the authorship
agreement The principal author has taken full responsibility for the data
the analyses and the interpretation and the conduct of the research The
statistical analysis has been contacted by Dr Filippidis (Department of
Primary Care and Public Health Imperial College London UK) All
authors had full access to all the data in the study and had final respon-
sibility for the decision to submit for publication Contributor Torben
Bjerregaard Larsen his institution has received payment for enrolling trial
participants from Janssen Scientific Affairs LLC and Boehringer Ingelheim
and he has been on the speaker bureaus for Bayer BMSPfizer Roche
Diagnostics Boehringer Ingelheim and Takeda Pharma
ACKNOWLEDGMENTContributor Torben Bjerregaard Larsen Aalborg University Hospital
Department of Cardiology Aalborg Thrombosis Research Unit Denmark
(data collection)
STUDY FUNDINGSupported by Imperial College London St Maryrsquos development fund
and National Institute for Health Research Imperial Biomedical Research
Centre The sponsor of the study had no role in study design data
collection data analysis data interpretation or writing of the report
Celine S Gathier was supported by the Dutch Heart Foundation grant
2009B046 Joan Martiacute-Fagravebregas was supported by the Spanish Ministry
of Health-Instituto de Salud Carlos III Redes temaacuteticas de Investigacioacuten
Cooperativa INVICTUS RD01200140002 and Fondo Europeo de
Desarrollo Regional Jiming Fang the Ontario Stroke Registry is funded
by the Canadian Stroke Network (CSN) and the Ontario Ministry of
Health and Long-Term Care (MOHLTC) This study was supported by
the Institute for Clinical Evaluative Sciences (ICES) which is funded by
an annual grant from the Ontario MOHLTC The opinions results and
conclusions reported in this paper are those of the authors and are inde-
pendent from the funding sources No endorsement by ICES or the
Ontario MOHLTC is intended or should be inferred
DISCLOSUREE Korompoki and F Filippidis report no disclosures relevant to the man-
uscript P Nielsen speaker for Boehringer Ingelheim consultant for
Bayer Pharma AS and BMSPfizer unrestricted research grant from
BMSPfizer A Del Giudice reports no disclosures relevant to the man-
uscript G Lip consultant for BayerJanssen BMSPfizer Biotronik
Medtronic Boehringer Ingelheim Microlife and Daiichi-Sankyo
speaker for Bayer BMSPfizer Medtronic Boehringer Ingelheim Micro-
life Roche and Daiichi-Sankyo J Kuramatsu reports no conflicts of
interest related to manuscript Unrelated potential conflicts of interest
travel grants from EMCools Otsuka and Boehringer Ingelheim and
speaker honoraria from Otsuka H Huttner reports no conflicts of inter-
est related to manuscript Unrelated potential conflicts of interest consul-
ting speaker honoraria and research support from Boehringer Ingelheim
Pfizer Biogen Medtronic and Novartis J Fang reports no disclosures
relevant to the manuscript S Schulman reports no conflicts of interest
related to manuscript Unrelated potential conflicts of interest honoraria
research support from Baxter Bayer Boehringer Ingelheim Daichii
694 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Sankyo Octapharma and Sanofi J Martiacute-Fagravebregas C Gathier
A Viswanathan A Biffi D Poli C Weimar and U Malzahn report
no disclosures relevant to the manuscript P Heuschmann research
grants from BMBF European Union Chariteacute Berlin Chamber of Physi-
cians German Parkinson Society University Hospital Wuumlrzburg
Robert-Koch-Institute German Heart Foundation Chariteacutendash
Universitaumltsmedizin Berlin (MonDAFIS unrestricted research grant to
Chariteacute from Bayer) University Goumlttingen (FIND-AFrandomized
unrestricted research grant to University Goumlttingen from Boehringer
Ingelheim) and University Hospital Heidelberg (RASUNOA-prime
unrestricted research grant to University Hospital Heidelberg from Bayer
BMS Boehringer Daiichi Sankyo) R Veltkamp consulting speaker
honoraria research support from Bayer Boehringer Daiichi Sankyo
BMS Pfizer Portola Biogen Amgen Morphosys Medtronic and
Apoplex Medical Technologies Go to Neurologyorg for full disclosures
Received December 29 2016 Accepted in final form May 23 2017
REFERENCES1 Camm AJ Lip GY De Caterina R et al 2012 Focused
update of the ESC guidelines for the management of atrial
fibrillation an update of the 2010 ESC guidelines for the
management of atrial fibrillation developed with the spe-
cial contribution of the European Heart Rhythm Associa-
tion Eur Heart J 2012332719ndash2747
2 Olesen JB Lip GY Hansen ML et al Validation of risk
stratification schemes for predicting stroke and thrombo-
embolism in patients with atrial fibrillation nationwide
cohort study BMJ 2011342d124
3 Flynn RW MacDonald TM Murray GD Doney AS
Systematic review of observational research studying the
long-term use of antithrombotic medicines following
intracerebral hemorrhage Cardiovasc Ther 201028
177ndash184
4 Poon MT Fonville AF Al-Shahi Salman R Long-term
prognosis after intracerebral haemorrhage systematic
review and meta-analysis J Neurol Neurosurg Psychiatry
201485660ndash667
5 Pisters R Lane DA Nieuwlaat R de Vos CB Crijns HJ
Lip GY A novel user-friendly score (HAS-BLED) to assess
1-year risk of major bleeding in patients with atrial fibrilla-
tion the Euro Heart Survey Chest 20101381093ndash1100
6 Hemphill JC III Greenberg SM Anderson CS et al
Guidelines for the management of spontaneous intracere-
bral hemorrhage a guideline for healthcare professionals
from the American Heart AssociationAmerican Stroke
Association Stroke 2015462032ndash2060
7 Steiner T Al-Shahi Salman R Beer R et al European
Stroke Organisation (ESO) guidelines for the management
of spontaneous intracerebral hemorrhage Int J Stroke
20149840ndash855
8 Liberati A Altman DG Tetzlaff J et al The PRISMA state-
ment for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions explanation
and elaboration J Clin Epidemiol 200962e1ndashe34
9 Nielsen PB Larsen TB Skjoth F Gorst-Rasmussen A
Rasmussen LH Lip GY Restarting anticoagulant treat-
ment after intracranial haemorrhage in patients with atrial
fibrillation and the impact on recurrent stroke mortality
and bleeding a nationwide cohort study Circulation
2015132517ndash525
10 Higgins JPT Altman DG Assessing Risk of Bias in
Included Studies Chichester Wiley 2008
11 DerSimonian R Laird N Meta-analysis in clinical trials
Control Clin Trials 19867177ndash188
12 Stamplecoski M Fang J Kapral MK Silver FL Long-term
outcomes of elderly patients with intracerebral hemorrhage
and atrial fibrillation Stroke 201445(s1)ATMP103
13 Viswanathan A Rakich SM Engel C et al Antiplatelet use
after intracerebral hemorrhage Neurology 200666206ndash209
14 Gathier CS Algra A Rinkel GJ van der Worp HB Long-
term outcome after anticoagulation-associated intracerebral
haemorrhage with or without restarting antithrombotic
therapy Cerebrovasc Dis 20133633ndash37
15 Kuramatsu JB Gerner ST Schellinger PD et al Antico-
agulant reversal blood pressure levels and anticoagulant
resumption in patients with anticoagulation-related intra-
cerebral hemorrhage JAMA 2015313824ndash836
16 Majeed A Kim YK Roberts RS Holmstrom M Schulman
S Optimal timing of resumption of warfarin after intracranial
hemorrhage Stroke 2010412860ndash2866
17 Vidal-Jordana A Barroeta-Espar I Sainz Pelayo MP
Mateo J Delgado-Mederos R Marti-Fabregas J Intracerebral
hemorrhage in anticoagulated patients what do we do after-
wards [in Spanish] Neurologia 201227136ndash142
18 Horstmann S Rizos T Jenetzky E Gumbinger C Hacke W
Veltkamp R Prevalence of atrial fibrillation in intracerebral
hemorrhage Eur J Neurol 201421570ndash576
19 Andersen KK Olsen TS Dehlendorff C Kammersgaard LP
Hemorrhagic and ischemic strokes compared stroke severity
mortality and risk factors Stroke 2009402068ndash2072
20 Paciaroni M Agnelli G Should oral anticoagulants be
restarted after warfarin-associated cerebral haemorrhage
in patients with atrial fibrillation Thromb Haemost
201411114ndash18
21 Eckman MH Rosand J Knudsen KA Singer DE
Greenberg SM Can patients be anticoagulated after
intracerebral hemorrhage A decision analysis Stroke
2004341710ndash1716
22 Lip GY Andreotti F Fauchier L et al Bleeding risk assess-
ment and management in atrial fibrillation patients a position
document from the European Heart Rhythm Association
endorsed by the European Society of Cardiology Working
Group on Thrombosis Europace 201113723ndash746
23 Goldstein JN Greenberg SM Should anticoagulation be
resumed after intracerebral hemorrhage Cleve Clin J Med
201077791ndash799
24 Molina CA Selim MH The dilemma of resuming anti-
coagulation after intracranial hemorrhage little evidence
facing big fears Stroke 2011423665ndash3666
25 Pasquini M Charidimou A van Asch CJ et al Variation in
restarting antithrombotic drugs at hospital discharge after
intracerebral hemorrhage Stroke 2014452643ndash2648
26 Maeda K Koga M Okada Y et al Nationwide survey of
neuro-specialistsrsquo opinions on anticoagulant therapy after
intracerebral hemorrhage in patients with atrial fibrillation
J Neurol Sci 201231282ndash85
27 Hart RG Pearce LA Aguilar MI Meta-analysis antith-
rombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation Ann Intern Med 2007146
857ndash867
28 Chao TF Liu CJ Liao JN et al Use of oral anticoagulants
for stroke prevention in patients with atrial fibrillation who
have a history of intracranial hemorrhage Circulation
20161331540ndash1547
29 Pennlert J Overholser R Asplund K et al Optimal timing
of anticoagulant treatment after intracerebral hemorrhage
in patients with atrial fibrillation Stroke 201748
314ndash320
Neurology 89 August 15 2017 695
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

truly new events or just an extension of the initialbleeding site9 The included studies are highly proneto selection bias and confounding by indicationbecause treating physicians may have avoided theuse of VKAs in patients perceived to be at higher riskof recurrence Hence unmeasured selection bias islikely in that we were unable to calculate adjustedincidence RRs because individual patient data werenot available in all studies We summarized aggre-gated treatment group differences (baseline character-istics and comorbidities) (table e-5) for each studythat may facilitate the interpretation of the results(table e-6) As previously shown baseline adjustmentin the setting of time-dependent exposure of treat-ment regimens only marginally affects outcomes asso-ciated with treatment9 This may indicate that otherreasons (besides the measure and included variables)have affected the decision of resuming OAC treat-ment This highlights the importance of meticulousinterpretation of the associations because indicationbias was likely present in all of the included studiesAnother limitation is that we did not have informationon either the time in therapeutic range for patientstaking VKAs or the quality of blood pressure control39
We also did not have data on dropout and rates anddirections of switch between different antithrombotictreatment strategies The number of studies includedin the meta-analysis was small therefore meta-regression and publication bias assessments may havebeen underpowered and should be interpreted withcaution Our study focused on IS and ICH as the mainoutcome events This approach may not provide thefull picture of outcome events and other factors affect-ing the net clinical benefit The 2 largest includedstudies showed a significant decrease of mortality inpatients treated with VKAs915 Because we censoredpatients after either IS or ICH we did not capturepotential multiple outcome events in individual pa-tients although ICH and IS are competing riskAnother limitation is that further subgroup analysesin terms of risk factors for ICH recurrence such aslobar vs deep hemorrhage topography leukoaraiosisand cerebral microbleed burden were not feasiblebecause this information was missing in several studiesIn addition comorbidities apart from AF (eg coro-nary artery disease) indicating the use of antiplateletswere not addressed
This meta-analysis of antithrombotic treatment inVKA-associated ICH survivors with AF suggests thatanticoagulation with VKA is associated with a lowerrate of IS compared to other or no antithromboticswithout causing a major increase of the risk of ICHrecurrence whereas antiplatelets fail to prevent ISBecause of the limitations of observational studiesa randomized controlled trial of antithrombotictherapy preferably with DOACs used as the
anticoagulants is needed to better guide decision mak-ing for antithrombotic therapy in patients with ICHand AF
AUTHOR CONTRIBUTIONSEleni Korompoki study concept data collection drafting and critical revi-
sion of manuscript Filippos T Filippidis study concept statistical analysis
data collection drafting and critical revision of manuscript Peter B Nielsen
study concept data collection and critical revision of manuscript
Angela Del Giudice Gregory Y Lip Joji Kuramatsu Hagen Huttner
Jiming Fang Sam Schulman Joan Martiacute-Fagravebregas Celine S Gathier
Anand Viswanathan Alessandro Biffi Daniela Poli and Christian
Weimar data collection and critical revision of manuscript Uwe
Malzahn and Peter Heuschmann critical review of manuscript Roland
Veltkamp study concept and financial support drafting and critical
revision of manuscript All authors have read and approved the final form
of the manuscript and have agreed to conditions noted on the authorship
agreement The principal author has taken full responsibility for the data
the analyses and the interpretation and the conduct of the research The
statistical analysis has been contacted by Dr Filippidis (Department of
Primary Care and Public Health Imperial College London UK) All
authors had full access to all the data in the study and had final respon-
sibility for the decision to submit for publication Contributor Torben
Bjerregaard Larsen his institution has received payment for enrolling trial
participants from Janssen Scientific Affairs LLC and Boehringer Ingelheim
and he has been on the speaker bureaus for Bayer BMSPfizer Roche
Diagnostics Boehringer Ingelheim and Takeda Pharma
ACKNOWLEDGMENTContributor Torben Bjerregaard Larsen Aalborg University Hospital
Department of Cardiology Aalborg Thrombosis Research Unit Denmark
(data collection)
STUDY FUNDINGSupported by Imperial College London St Maryrsquos development fund
and National Institute for Health Research Imperial Biomedical Research
Centre The sponsor of the study had no role in study design data
collection data analysis data interpretation or writing of the report
Celine S Gathier was supported by the Dutch Heart Foundation grant
2009B046 Joan Martiacute-Fagravebregas was supported by the Spanish Ministry
of Health-Instituto de Salud Carlos III Redes temaacuteticas de Investigacioacuten
Cooperativa INVICTUS RD01200140002 and Fondo Europeo de
Desarrollo Regional Jiming Fang the Ontario Stroke Registry is funded
by the Canadian Stroke Network (CSN) and the Ontario Ministry of
Health and Long-Term Care (MOHLTC) This study was supported by
the Institute for Clinical Evaluative Sciences (ICES) which is funded by
an annual grant from the Ontario MOHLTC The opinions results and
conclusions reported in this paper are those of the authors and are inde-
pendent from the funding sources No endorsement by ICES or the
Ontario MOHLTC is intended or should be inferred
DISCLOSUREE Korompoki and F Filippidis report no disclosures relevant to the man-
uscript P Nielsen speaker for Boehringer Ingelheim consultant for
Bayer Pharma AS and BMSPfizer unrestricted research grant from
BMSPfizer A Del Giudice reports no disclosures relevant to the man-
uscript G Lip consultant for BayerJanssen BMSPfizer Biotronik
Medtronic Boehringer Ingelheim Microlife and Daiichi-Sankyo
speaker for Bayer BMSPfizer Medtronic Boehringer Ingelheim Micro-
life Roche and Daiichi-Sankyo J Kuramatsu reports no conflicts of
interest related to manuscript Unrelated potential conflicts of interest
travel grants from EMCools Otsuka and Boehringer Ingelheim and
speaker honoraria from Otsuka H Huttner reports no conflicts of inter-
est related to manuscript Unrelated potential conflicts of interest consul-
ting speaker honoraria and research support from Boehringer Ingelheim
Pfizer Biogen Medtronic and Novartis J Fang reports no disclosures
relevant to the manuscript S Schulman reports no conflicts of interest
related to manuscript Unrelated potential conflicts of interest honoraria
research support from Baxter Bayer Boehringer Ingelheim Daichii
694 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Sankyo Octapharma and Sanofi J Martiacute-Fagravebregas C Gathier
A Viswanathan A Biffi D Poli C Weimar and U Malzahn report
no disclosures relevant to the manuscript P Heuschmann research
grants from BMBF European Union Chariteacute Berlin Chamber of Physi-
cians German Parkinson Society University Hospital Wuumlrzburg
Robert-Koch-Institute German Heart Foundation Chariteacutendash
Universitaumltsmedizin Berlin (MonDAFIS unrestricted research grant to
Chariteacute from Bayer) University Goumlttingen (FIND-AFrandomized
unrestricted research grant to University Goumlttingen from Boehringer
Ingelheim) and University Hospital Heidelberg (RASUNOA-prime
unrestricted research grant to University Hospital Heidelberg from Bayer
BMS Boehringer Daiichi Sankyo) R Veltkamp consulting speaker
honoraria research support from Bayer Boehringer Daiichi Sankyo
BMS Pfizer Portola Biogen Amgen Morphosys Medtronic and
Apoplex Medical Technologies Go to Neurologyorg for full disclosures
Received December 29 2016 Accepted in final form May 23 2017
REFERENCES1 Camm AJ Lip GY De Caterina R et al 2012 Focused
update of the ESC guidelines for the management of atrial
fibrillation an update of the 2010 ESC guidelines for the
management of atrial fibrillation developed with the spe-
cial contribution of the European Heart Rhythm Associa-
tion Eur Heart J 2012332719ndash2747
2 Olesen JB Lip GY Hansen ML et al Validation of risk
stratification schemes for predicting stroke and thrombo-
embolism in patients with atrial fibrillation nationwide
cohort study BMJ 2011342d124
3 Flynn RW MacDonald TM Murray GD Doney AS
Systematic review of observational research studying the
long-term use of antithrombotic medicines following
intracerebral hemorrhage Cardiovasc Ther 201028
177ndash184
4 Poon MT Fonville AF Al-Shahi Salman R Long-term
prognosis after intracerebral haemorrhage systematic
review and meta-analysis J Neurol Neurosurg Psychiatry
201485660ndash667
5 Pisters R Lane DA Nieuwlaat R de Vos CB Crijns HJ
Lip GY A novel user-friendly score (HAS-BLED) to assess
1-year risk of major bleeding in patients with atrial fibrilla-
tion the Euro Heart Survey Chest 20101381093ndash1100
6 Hemphill JC III Greenberg SM Anderson CS et al
Guidelines for the management of spontaneous intracere-
bral hemorrhage a guideline for healthcare professionals
from the American Heart AssociationAmerican Stroke
Association Stroke 2015462032ndash2060
7 Steiner T Al-Shahi Salman R Beer R et al European
Stroke Organisation (ESO) guidelines for the management
of spontaneous intracerebral hemorrhage Int J Stroke
20149840ndash855
8 Liberati A Altman DG Tetzlaff J et al The PRISMA state-
ment for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions explanation
and elaboration J Clin Epidemiol 200962e1ndashe34
9 Nielsen PB Larsen TB Skjoth F Gorst-Rasmussen A
Rasmussen LH Lip GY Restarting anticoagulant treat-
ment after intracranial haemorrhage in patients with atrial
fibrillation and the impact on recurrent stroke mortality
and bleeding a nationwide cohort study Circulation
2015132517ndash525
10 Higgins JPT Altman DG Assessing Risk of Bias in
Included Studies Chichester Wiley 2008
11 DerSimonian R Laird N Meta-analysis in clinical trials
Control Clin Trials 19867177ndash188
12 Stamplecoski M Fang J Kapral MK Silver FL Long-term
outcomes of elderly patients with intracerebral hemorrhage
and atrial fibrillation Stroke 201445(s1)ATMP103
13 Viswanathan A Rakich SM Engel C et al Antiplatelet use
after intracerebral hemorrhage Neurology 200666206ndash209
14 Gathier CS Algra A Rinkel GJ van der Worp HB Long-
term outcome after anticoagulation-associated intracerebral
haemorrhage with or without restarting antithrombotic
therapy Cerebrovasc Dis 20133633ndash37
15 Kuramatsu JB Gerner ST Schellinger PD et al Antico-
agulant reversal blood pressure levels and anticoagulant
resumption in patients with anticoagulation-related intra-
cerebral hemorrhage JAMA 2015313824ndash836
16 Majeed A Kim YK Roberts RS Holmstrom M Schulman
S Optimal timing of resumption of warfarin after intracranial
hemorrhage Stroke 2010412860ndash2866
17 Vidal-Jordana A Barroeta-Espar I Sainz Pelayo MP
Mateo J Delgado-Mederos R Marti-Fabregas J Intracerebral
hemorrhage in anticoagulated patients what do we do after-
wards [in Spanish] Neurologia 201227136ndash142
18 Horstmann S Rizos T Jenetzky E Gumbinger C Hacke W
Veltkamp R Prevalence of atrial fibrillation in intracerebral
hemorrhage Eur J Neurol 201421570ndash576
19 Andersen KK Olsen TS Dehlendorff C Kammersgaard LP
Hemorrhagic and ischemic strokes compared stroke severity
mortality and risk factors Stroke 2009402068ndash2072
20 Paciaroni M Agnelli G Should oral anticoagulants be
restarted after warfarin-associated cerebral haemorrhage
in patients with atrial fibrillation Thromb Haemost
201411114ndash18
21 Eckman MH Rosand J Knudsen KA Singer DE
Greenberg SM Can patients be anticoagulated after
intracerebral hemorrhage A decision analysis Stroke
2004341710ndash1716
22 Lip GY Andreotti F Fauchier L et al Bleeding risk assess-
ment and management in atrial fibrillation patients a position
document from the European Heart Rhythm Association
endorsed by the European Society of Cardiology Working
Group on Thrombosis Europace 201113723ndash746
23 Goldstein JN Greenberg SM Should anticoagulation be
resumed after intracerebral hemorrhage Cleve Clin J Med
201077791ndash799
24 Molina CA Selim MH The dilemma of resuming anti-
coagulation after intracranial hemorrhage little evidence
facing big fears Stroke 2011423665ndash3666
25 Pasquini M Charidimou A van Asch CJ et al Variation in
restarting antithrombotic drugs at hospital discharge after
intracerebral hemorrhage Stroke 2014452643ndash2648
26 Maeda K Koga M Okada Y et al Nationwide survey of
neuro-specialistsrsquo opinions on anticoagulant therapy after
intracerebral hemorrhage in patients with atrial fibrillation
J Neurol Sci 201231282ndash85
27 Hart RG Pearce LA Aguilar MI Meta-analysis antith-
rombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation Ann Intern Med 2007146
857ndash867
28 Chao TF Liu CJ Liao JN et al Use of oral anticoagulants
for stroke prevention in patients with atrial fibrillation who
have a history of intracranial hemorrhage Circulation
20161331540ndash1547
29 Pennlert J Overholser R Asplund K et al Optimal timing
of anticoagulant treatment after intracerebral hemorrhage
in patients with atrial fibrillation Stroke 201748
314ndash320
Neurology 89 August 15 2017 695
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Sankyo Octapharma and Sanofi J Martiacute-Fagravebregas C Gathier
A Viswanathan A Biffi D Poli C Weimar and U Malzahn report
no disclosures relevant to the manuscript P Heuschmann research
grants from BMBF European Union Chariteacute Berlin Chamber of Physi-
cians German Parkinson Society University Hospital Wuumlrzburg
Robert-Koch-Institute German Heart Foundation Chariteacutendash
Universitaumltsmedizin Berlin (MonDAFIS unrestricted research grant to
Chariteacute from Bayer) University Goumlttingen (FIND-AFrandomized
unrestricted research grant to University Goumlttingen from Boehringer
Ingelheim) and University Hospital Heidelberg (RASUNOA-prime
unrestricted research grant to University Hospital Heidelberg from Bayer
BMS Boehringer Daiichi Sankyo) R Veltkamp consulting speaker
honoraria research support from Bayer Boehringer Daiichi Sankyo
BMS Pfizer Portola Biogen Amgen Morphosys Medtronic and
Apoplex Medical Technologies Go to Neurologyorg for full disclosures
Received December 29 2016 Accepted in final form May 23 2017
REFERENCES1 Camm AJ Lip GY De Caterina R et al 2012 Focused
update of the ESC guidelines for the management of atrial
fibrillation an update of the 2010 ESC guidelines for the
management of atrial fibrillation developed with the spe-
cial contribution of the European Heart Rhythm Associa-
tion Eur Heart J 2012332719ndash2747
2 Olesen JB Lip GY Hansen ML et al Validation of risk
stratification schemes for predicting stroke and thrombo-
embolism in patients with atrial fibrillation nationwide
cohort study BMJ 2011342d124
3 Flynn RW MacDonald TM Murray GD Doney AS
Systematic review of observational research studying the
long-term use of antithrombotic medicines following
intracerebral hemorrhage Cardiovasc Ther 201028
177ndash184
4 Poon MT Fonville AF Al-Shahi Salman R Long-term
prognosis after intracerebral haemorrhage systematic
review and meta-analysis J Neurol Neurosurg Psychiatry
201485660ndash667
5 Pisters R Lane DA Nieuwlaat R de Vos CB Crijns HJ
Lip GY A novel user-friendly score (HAS-BLED) to assess
1-year risk of major bleeding in patients with atrial fibrilla-
tion the Euro Heart Survey Chest 20101381093ndash1100
6 Hemphill JC III Greenberg SM Anderson CS et al
Guidelines for the management of spontaneous intracere-
bral hemorrhage a guideline for healthcare professionals
from the American Heart AssociationAmerican Stroke
Association Stroke 2015462032ndash2060
7 Steiner T Al-Shahi Salman R Beer R et al European
Stroke Organisation (ESO) guidelines for the management
of spontaneous intracerebral hemorrhage Int J Stroke
20149840ndash855
8 Liberati A Altman DG Tetzlaff J et al The PRISMA state-
ment for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions explanation
and elaboration J Clin Epidemiol 200962e1ndashe34
9 Nielsen PB Larsen TB Skjoth F Gorst-Rasmussen A
Rasmussen LH Lip GY Restarting anticoagulant treat-
ment after intracranial haemorrhage in patients with atrial
fibrillation and the impact on recurrent stroke mortality
and bleeding a nationwide cohort study Circulation
2015132517ndash525
10 Higgins JPT Altman DG Assessing Risk of Bias in
Included Studies Chichester Wiley 2008
11 DerSimonian R Laird N Meta-analysis in clinical trials
Control Clin Trials 19867177ndash188
12 Stamplecoski M Fang J Kapral MK Silver FL Long-term
outcomes of elderly patients with intracerebral hemorrhage
and atrial fibrillation Stroke 201445(s1)ATMP103
13 Viswanathan A Rakich SM Engel C et al Antiplatelet use
after intracerebral hemorrhage Neurology 200666206ndash209
14 Gathier CS Algra A Rinkel GJ van der Worp HB Long-
term outcome after anticoagulation-associated intracerebral
haemorrhage with or without restarting antithrombotic
therapy Cerebrovasc Dis 20133633ndash37
15 Kuramatsu JB Gerner ST Schellinger PD et al Antico-
agulant reversal blood pressure levels and anticoagulant
resumption in patients with anticoagulation-related intra-
cerebral hemorrhage JAMA 2015313824ndash836
16 Majeed A Kim YK Roberts RS Holmstrom M Schulman
S Optimal timing of resumption of warfarin after intracranial
hemorrhage Stroke 2010412860ndash2866
17 Vidal-Jordana A Barroeta-Espar I Sainz Pelayo MP
Mateo J Delgado-Mederos R Marti-Fabregas J Intracerebral
hemorrhage in anticoagulated patients what do we do after-
wards [in Spanish] Neurologia 201227136ndash142
18 Horstmann S Rizos T Jenetzky E Gumbinger C Hacke W
Veltkamp R Prevalence of atrial fibrillation in intracerebral
hemorrhage Eur J Neurol 201421570ndash576
19 Andersen KK Olsen TS Dehlendorff C Kammersgaard LP
Hemorrhagic and ischemic strokes compared stroke severity
mortality and risk factors Stroke 2009402068ndash2072
20 Paciaroni M Agnelli G Should oral anticoagulants be
restarted after warfarin-associated cerebral haemorrhage
in patients with atrial fibrillation Thromb Haemost
201411114ndash18
21 Eckman MH Rosand J Knudsen KA Singer DE
Greenberg SM Can patients be anticoagulated after
intracerebral hemorrhage A decision analysis Stroke
2004341710ndash1716
22 Lip GY Andreotti F Fauchier L et al Bleeding risk assess-
ment and management in atrial fibrillation patients a position
document from the European Heart Rhythm Association
endorsed by the European Society of Cardiology Working
Group on Thrombosis Europace 201113723ndash746
23 Goldstein JN Greenberg SM Should anticoagulation be
resumed after intracerebral hemorrhage Cleve Clin J Med
201077791ndash799
24 Molina CA Selim MH The dilemma of resuming anti-
coagulation after intracranial hemorrhage little evidence
facing big fears Stroke 2011423665ndash3666
25 Pasquini M Charidimou A van Asch CJ et al Variation in
restarting antithrombotic drugs at hospital discharge after
intracerebral hemorrhage Stroke 2014452643ndash2648
26 Maeda K Koga M Okada Y et al Nationwide survey of
neuro-specialistsrsquo opinions on anticoagulant therapy after
intracerebral hemorrhage in patients with atrial fibrillation
J Neurol Sci 201231282ndash85
27 Hart RG Pearce LA Aguilar MI Meta-analysis antith-
rombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation Ann Intern Med 2007146
857ndash867
28 Chao TF Liu CJ Liao JN et al Use of oral anticoagulants
for stroke prevention in patients with atrial fibrillation who
have a history of intracranial hemorrhage Circulation
20161331540ndash1547
29 Pennlert J Overholser R Asplund K et al Optimal timing
of anticoagulant treatment after intracerebral hemorrhage
in patients with atrial fibrillation Stroke 201748
314ndash320
Neurology 89 August 15 2017 695
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

30 Friberg L Rosenqvist M Lip GYH Net clinical benefit of
warfarin in patients with atrial fibrillation a report from
the Swedish atrial fibrillation cohort study Circulation
20121252298ndash2307
31 Ruff CT Giugliano RP Braunwald E et al Comparison
of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation a meta-analysis
of randomised trials Lancet 2014383955ndash962
32 Chatterjee S Sardar P Biondi-Zoccai G Kumbhani DJ New
oral anticoagulants and the risk of intracranial hemorrhage
traditional and bayesian meta-analysis and mixed treatment
comparison of randomized trials of new oral anticoagulants in
atrial fibrillation JAMA Neurol 2013701486ndash1490
33 Ottosen TP Grijota M Hansen ML et al Use of antith-
rombotic therapy and long-term clinical outcome among
patients surviving intracerebral hemorrhage Stroke 2016
471837ndash1843
34 Connolly SJ Eikelboom J Joyner C et al Apixaban in
patients with atrial fibrillation New Engl J Med 2011
364806ndash817
35 Heidbuchel H Verhamme P Alings M et al EHRA
practical guide on the use of new oral anticoagulants in
patients with non-valvular atrial fibrillation executive
summary Eur Heart J 2013342094ndash2106
36 Horstmann S Zugck C Krumsdorf U et al Left atrial
appendage occlusion in atrial fibrillation after intracranial
hemorrhage Neurology 201482135ndash138
37 Hart RG Benavente O McBride R Pearce LA Antith-
rombotic therapy to prevent stroke in patients with atrial
fibrillation a meta-analysis Ann Intern Med 1999131
492ndash501
38 Mant J Hobbs FD Fletcher K et al Warfarin versus
aspirin for stroke prevention in an elderly community
population with atrial fibrillation (the Birmingham
Atrial Fibrillation Treatment of the Aged Study
BAFTA) a randomised controlled trial Lancet 2007
370493ndash503
39 Biffi A Anderson CD Battey TW et al Association
between blood pressure control and risk of recurrent intra-
cerebral hemorrhage JAMA 2015314904ndash912
Visit the Neurologyreg Website at Neurologyorgbull Enhanced navigation format
bull Increased search capability
bull Highlighted articles
bull Detailed podcast descriptions
bull RSS Feeds of current issue and podcasts
bull Personal folders for articles and searches
bull Mobile device download link
bull AAN Web page links
bull Links to Neurology Nowreg Neurology Todayreg and Continuumreg
bull Resident amp Fellow subsite
Find Neurologyreg on Facebook httptinyurlcomneurologyfan
Follow Neurologyreg on Twitter httpstwittercomGreenJournal
696 Neurology 89 August 15 2017
ordf 2017 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

DOI 101212WNL0000000000004235201789687-696 Published Online before print July 19 2017Neurology
Eleni Korompoki Filippos T Filippidis Peter B Nielsen et al fibrillation
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial
This information is current as of July 19 2017
ServicesUpdated Information amp
httpwwwneurologyorgcontent897687fullhtmlincluding high resolution figures can be found at
Supplementary Material
004235DC1httpwwwneurologyorgcontentsuppl20170719WNL0000000000Supplementary material can be found at
References httpwwwneurologyorgcontent897687fullhtmlref-list-1
This article cites 38 articles 15 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionstroke_preventionStroke prevention
httpwwwneurologyorgcgicollectionintracerebral_hemorrhageIntracerebral hemorrhage
httpwwwneurologyorgcgicollectionembolismEmbolism
httpwwwneurologyorgcgicollectioncardiacCardiac
strokehttpwwwneurologyorgcgicollectionall_cerebrovascular_disease_All Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2017 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology