Embed Size (px)
Citation preview

Locoregional management Locoregional management and and
neoadjuvant systemic treatmentneoadjuvant systemic treatment
Birgit Carly MD
Breast Unit Isala Breast Cancer Prevention Center
CHU Saint PierreBrussels
Inoperable Breast CancerInoperable Breast Cancer(LABC and IBC)(LABC and IBC)
- Standard of care
- Clinical downstaging T and N status
- Makes surgery possible
- Allows BCT
- Complete Pathologic response of primary T and axillary N is a prognostic factor
- Better overall survival
Machiavelli MR, Cancer J Sci Am 1998 / Ferriere JP, Am J Clin Oncol 1998 / Cance WG, Ann Surg 2002
Neoadjuvant CT

Operable Breast CancerOperable Breast CancerNeoadjuvant CT vs adjuvant CTNeoadjuvant CT vs adjuvant CT
n chimio OS chir conserv(%)
NSABP -B18 152360%T2, 13%T3
AC (4) id 67 vs 60
EORTC 10902 698 FEC (4) id 37 vs 21
ABCSG trial 7 423 CMF (3)
+ CMF or EC adj
id
Scholl 390 FAC (4) id 82 vs 77
- BCT possible without compromising survival;- Pathologic Complete Response better outcome;- Can be used to study Breast Cancer Biology;- Same DFS and OS.

Questions NAC and Locoregional treatment
• Optimal Method for Staging at Diagnosis and Evaluation Clinical Response after NAC?
•Use Sentinel Node?
• How to mark the tumorbed?
• Which Surgery in the Breast and the Axilla?
• Which Chemotherapy
•Timing of Surgery?
Staging at diagnosis and after NAC: optimal method
At diagnosis: Size, Unifocality, Type, Grading, Hormone Receptor status, Neu / HER2, Ki67, Contralateral breast, Nodal Status.
Tools: - Breast: Physical Examination, Mammography, Ultrasound, Microbiopsy. MRI?
- Axilla: Physical Examination, US, FNA, SN?
After NAC: Clinical Response Tumor through Change Size, Change Nodal Status
Tools: - Breast: Physical Examination, Mammography, Ultrasound, MRI - Axilla: Physical examination, US, SN?
Correct cTNM to establish first treatment: surgery or systemic treatment
Correct yTNM to establish surgery : Conservatice surgery vs mastectomy
Which staging we use after NAC for completing treatment, cTNM and / or yTNM:implications in surgery and RT

Staging at diagnosis and after NAC: optimal Imaging method
Breast?
NAC: degeneration, necrosis, fibrosis, sclerosis, inflammation of the Tumor
Chagpar AB, Ann Surg 2006
No NAC After NAC

Staging Breast Tumor after NAC
Peintinger F, Ann Surg Oncol 2006
Schott A, Breast Cancer Research and Treatment, 2005
Multidetector-row CT, PET, H MR spectroscopy
162 pat, retrosp. Accuracy
Phys Ex 53%
Mx + US 67%
PE + Mx + US 63%
43 pat, retrosp. Accuracy pCR
Phys Ex 75%
Mx 89%
US 82%
MRI 89%
Good overall correlation between MRI and Overall response, but very bad correlation when pCR.
Biopsy after NAC remains absolutely necessary to determine pCR
Type of Tumor important in measurement of residual tumor: lobular underestimated, poorly differentiated overestimated.

How to mark the tumorbed?
-Titanium clip in the center of the tumor before NAC
- Tattoo with black coal in center or at 4 poles of tumor

Neoadjuvant CT for Early Breast CancerNeoadjuvant CT for Early Breast Cancer
B.C.
n chimio cCR (%)
pCR (%)
BCR (%)
NSAPB-B27 2411 AC (4) 40 9,8 61
AC (4), DOC (4) 65 18,7 63
GEPARDUO (GABG)
913 A Pacl (4) / 2w 32,5 7,7 65
AC (4), DOC (4) 57,4 16,1 75
Penault-Llorca (France)
200 AC 6 45
A Pacl 15 56
Buzdar (Houston) 174 FAC (4) 24 18 35
Pacl (4) 27 6 46
Smith (Scottish) 104 CVAP (8) 33 15,4 48
CVAP (4), DOC (4)
56 30,8 67

Operable Breast CancerOperable Breast CancerNeoadjuvant CT and BCTNeoadjuvant CT and BCT
Breast conservation after NAC yields no higher incidence of positive margins than primary surgical treatment.
Soucy G J Am Coll Surg 2007
NAC equivalent to adjuvant CT for survival and DFS.
NAC increased risk of locoregional recurrence when RT without surgery was adopted.
Mauri D J Natl Cancer Inst 2005

Operable Breast CancerOperable Breast CancerNeoadjuvant CT and BCTNeoadjuvant CT and BCT
340 patients NAC, Stage I 4%, Stage II 58%, Stage III 38%Medium FU 60 months29 (95%)Local regional recurrence with 16 (91%) ipsilateral breast tumor recurrence
Chen AM J Clin Oncol 2004
Variables positive correlation:
- Clinical N2 or N3
- Pathological residual tumor larger then 2 cm
- Multifocal pattern
- Lymphovascular space invasion

Role of type of surgery on LR, risk factors
1772 women, breast cancer stade I-II,
randomised (EORTC et DBCG), retrospective
Voogd A, J Clin Oncol 2001
BCT:
Age < 35 yrs
Extended DCIS
Local recurrence10% at 10 yrs 9% at 10 yrs
Tumor size
Nodal Status
High histological grade
Vascular Invasion
BCT + MRM
Vascular Invasion
Distant metastasis
BCT + MRM

Axilla: Staging at diagnosis.
Khan A Surg Oncol 2005; Kilbride KE Ann Surg Oncol 2008; Grube BJ Arch Surg 2008;

Which Surgery to the Axilla. Optimal integration of SNB into
neoadjuvant chemotherapy program
Kilbride KE Ann Surg Oncol 2008; Khan A Ann Surg Oncol 2005; Grube BJ Arch Surg 2008;

Which Surgery to the Axilla. SN as definitive treatment before
NAC when SN negative?
Schrenk P Am J Surg 2008
Feasibility of SN mapping before NAC in cN0?
Feasibility of FU lymphatic mapping after NAC?
Can patients be spared Axillary Clearance post NAC?

Which Surgery to the Axilla. SN as definitive treatment before
NAC when SN negative?
Schrenk P Am J Surg 2008
45 cT2T3N0 (PE, US)
Pre NAC: SN IR 100%; 19 SN0, 26 SN+ ( 6/26 micromet)
After NAC all axillary cleareance:
SN IR 64%: - 80% SN0 or micromet pre NAC
- 45% SN+ pre NAC
FNR 0% N0 pre NAC
50% N+ pre NAC

Which Surgery to the Axilla. SN as definitive treatment before
NAC when SN negative?
Grube BJ Arch Surg 2008

Optimal integration of SNB into neoadjuvant chemotherapy
program.SN Post NAC
Grube BJ Arch Surg 2008
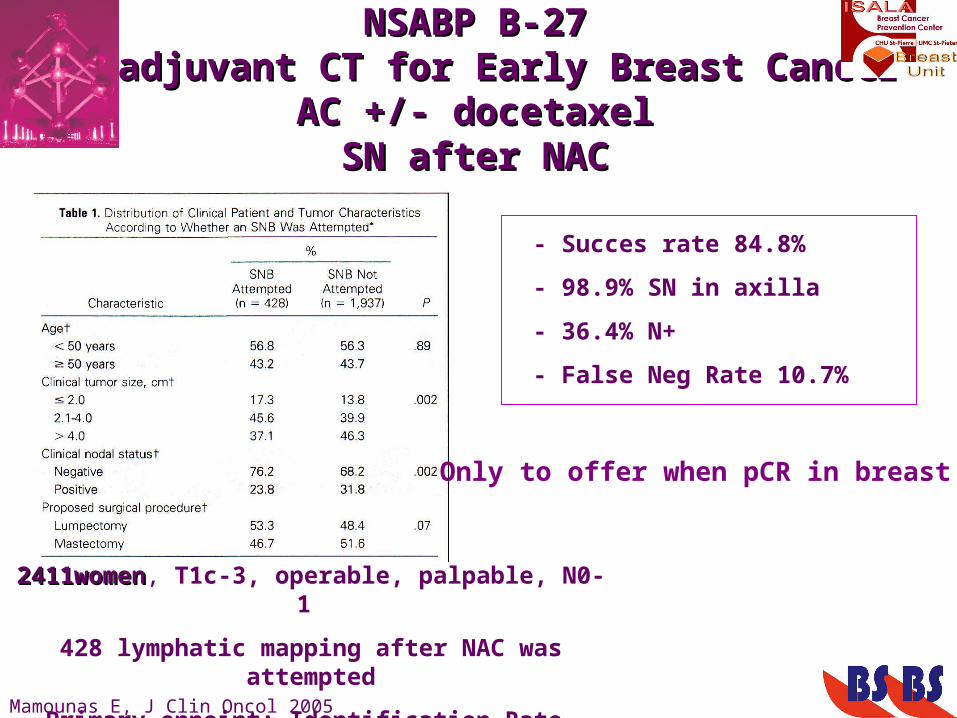
NSABP B-27NSABP B-27Neoadjuvant CT for Early Breast CancerNeoadjuvant CT for Early Breast Cancer
AC +/- docetaxelAC +/- docetaxelSN after NACSN after NAC
2411women2411women, T1c-3, operable, palpable, N0-1
428 lymphatic mapping after NAC was attempted
Primary enpoint: Identification Rate, False Neg. Rate
Mamounas E, J Clin Oncol 2005
- Succes rate 84.8%
- 98.9% SN in axilla
- 36.4% N+
- False Neg Rate 10.7%
Only to offer when pCR in breast

Optimal integration of SNB into neoadjuvant chemotherapy
program
33/104 patients Lymphoscintigraphy before and after NAC: same image on
lymphoscintigraphy
Kinoshita T, Breast Cancer 2007
Questions:
•Does tumour response to NAC causes lymphatic scarring that could affect drainage pattern?
•Does NAC has the same effect on involved SN as it does on non-involved SN

SNB after NAC in N + patients at diagnosis.SNB after NAC in N + patients at diagnosis.Can downstaging prevent Axillary dissection?Can downstaging prevent Axillary dissection?
Retrospective, 69patients, N+ at diagnosis by US FNA, mean T 4 cm
IR 92.8%, FN 25%
Shen J, Cancer 2007
Retrospective, 54 patients, N+ at diagnosis by US FNS or SNB, mean T 3 cm;
IR 98%, FN 8.6%
Newman E, Annals of Surgical Oncology 2006

Optimal integration of SNB into neoadjuvant chemotherapy
program
It is prognostically valuable to differentiate patients who presented as node negative from those who were
downstaged by chemotherapy
Which systemic neoadjuvant treatment ?
Chemotherapy or Endocrine treatment.
Same treatment that reflects state of the art in adjuvant regimens.

Timing of Surgery All CT upfront or Split CT by Surgery?
- The ideal timing of surgery, when NAC is given, is not known. - Treatment plan should be devised at the start and should
not be altered until there is clear evidence of disease progression.
- Patients with disease progression during initial course of treatment should be switched to alternate regimen or offered local therapy. - Use of additional CT after standard course of CT with residual tumour has no proven benefit.

Questions NAC and Locoregional treatment
• Optimal Method for Staging at Diagnosis and Evaluation Clinical Response after NAC?
•Use Sentinel Node?• How to mark the tumorbed?
• Which Surgery in the Breast and the Axilla?• Which Chemotherapy
•Timing of Surgery?





























