-
8/4/2019 Locomotor Training Using Body-SCI
1/10
Locomotor Training Using Body-
Weight Support on a Treadmill inConjunction With Ongoing
PhysicalTherapy in a Child With SevereCerebellar AtaxiaKristin
Cernak, Vicki Stevens, Robert Price, Anne Shumway-Cook
Background and PurposeThis case report describes the effects of
locomotor training using body-weight
support (BWS) on a treadmill and during overground walking on
mobility in a child with severe cerebellar ataxia who was
nonambulatory. To date, no studies haveexamined the efficacy of
this intervention in people with cerebellar ataxia.
Case DescriptionThe patient was a 13-year-old girl who had a
cerebellar/brainstem infarct 16 monthsbefore the intervention. Her
long-term goal was to walk independently in her home
with a walker.
InterventionLocomotor training using a BWS system both on the
treadmill and during overground
walking was implemented 5 days a week for 4 weeks in a clinic.
Locomotor training
using BWS on a treadmill was continued 5 days a week for 4
months at home.
OutcomesPrior to training, she was able to take steps on her own
with the help of anotherperson, but did not take full weight on her
feet or walk on a regular basis. At 6months, she walked for
household distances. Prior to training, her Pediatric Func-tional
Independence Measure scores were 3 (moderate assistance) for all
transfers, 2(maximal assistance) for walking, and 1 (total
assistance) for stairs. At 6 months, herscores were 6 (modified
independence) for transfers, 5 (supervision) for walking, and4
(minimal assistance) for stairs. Prior to training, she was unable
to take independentsteps during treadmill walking; at 6 months, all
of her steps were unassisted.
Discussion and ConclusionLocomotor training using BWS on a
treadmill in conjunction with overground gaittraining may be an
effective way to improve ambulatory function in individuals
withsevere cerebellar ataxia, but the intensity and duration of
training required forfunctionally significant improvements may be
prolonged.
K Cernak, PT, DPT, MPH, is Phys-
ical Therapist, Division of PhysicalTherapy, Department of
Rehabili-tation Medicine, University ofWashington Medical Center,
1959NE Pacific St, Seattle, WA 98195(USA). Address all
correspon-dence to Dr Cernak at: [email protected].
V Stevens, PT, is Physical Thera-pist, Division of Physical
Ther-apy, Department of RehabilitationMedicine, University of
Washing-ton Medical Center.
R Price, MSME, is Research Scien-tist, Department of
RehabilitationMedicine, University of Washing-ton Medical
Center.
A Shumway-Cook, PT, PhD,FAPTA, is Professor, Division ofPhysical
Therapy, Department ofRehabilitation Medicine, Univer-sity of
Washington Medical Center.
[Cernak K, Stevens V, Price R,Shumway-Cook A. Locomotortraining
using body-weight sup-port on a treadmill in conjunctionwith
ongoing physical therapy in a
child with severe cerebellar ataxia.Phys Ther.
2008;88:8897.]
2008 American Physical TherapyAssociation
Case Report
Post a Rapid Response orfind The Bottom
Line:www.ptjournal.org
88 f Physical Therapy Volume 88 Number 1 January 2008
-
8/4/2019 Locomotor Training Using Body-SCI
2/10
One of the most commonlystated goals in the rehabilita-tion of
populations with neu-
rologic problems is the recovery ofwalking capacity.14 Although
there
is no consensus currently on the bestway to train safe,
efficient, and inde-pendent walking, evidence existsthat
task-specific gait training canhave more beneficial effects on
func-tional gait outcomes than nonspe-cific rehabilitation
approaches.5,6 Lo-
comotor training using body-weightsupport on a treadmill (BWST)
is anexample of task-specific gait trainingthat uses a harness to
provide partialbody-weight support in conjunction
with a motorized treadmill. Re-
searchers examining locomotortraining have suggested that
trainingusing BWST has several advantages:
(1) the body-weight support harnessallows a progressive increase
in thedemands for postural control, (2) thetreadmill allows
systematic controland progression of the speed at
which walking is performed, and (3)the repetitive training of a
completegait cycle enables a more appropri-ate pattern of sensory
input associ-
ated with the different phases of gaitto stimulate the locomotor
pat-tern.79 In addition, locomotor train-ing using BWST allows the
therapistto provide manual assistance to helpthe patient simulate a
more normal
walking pattern.
Previous research has presented
mixed results regarding the efficacyof locomotor training using
BWST inpatients with a variety of diagnoses,including stroke,1,5,10
spinal cord in-
jury,11,12 and cerebral palsy.13 A Co-chrane review by Moseley
et al10 in-
vestigated the results of gait trainingusing BWST after stroke
in 11 ran-domized controlled trials involving
458 participants and reported no sta-tistically significant
differences be-tween gait training using a treadmill
with or without body-weight sup-port and other interventions
for
walking speed and dependency.
Matching the type of locomotortraining to specific patient
character-istics, such as gait speed, may be
required to optimize outcomes. Forexample, patients who have had
a
stroke and walk slower than 0.4 m/sbenefited most from
body-weightsupport and treadmill training,
whereas those who walked fasterthan 0.4 m/s required the
addition ofoverground training to training usingBWST.1
Guidelines regarding optimal waysto combine overground training
andtraining using BWST in specific pa-tient subgroups are still
being devel-oped. Helbostad14 suggested that,
despite the mixed evidence for theefficacy of training using
BWST forimproving gait in patients who are
ambulatory, it may be the only alter-native for ambulation
training in peo-ple who are unable or require signif-icant
assistance to walk.
Disordered or ataxic gait is a definingcharacteristic of
cerebellar pathol-ogy. Ataxic gait has been character-ized by a
widened or alternatively
variable base of support, inappropri-ate timing of foot
placement and re-duced step frequency, increasedstep width, and
prolonged time indouble-limb support.15 Both im-paired postural
stability and decom-position of multijoint leg movementsappear to
be factors in cerebellar gaitataxia.16,17 This combination of
im-
paired balance and dyscoordinationin lower-limb dynamics
suggests astrong rationale for the use of loco-motor training using
BWST in people
with ataxic gait. However, BWSTuses unweighting during
locomotortraining, and this unweighting is incontrast to previous
authors18 whohave recommended the use of
weights on the trunk and limbs todecrease ataxic movements in
pa-tients with cerebellar pathology.
In addition to their role in the con-trol of balance and gait,
cerebellar
structures also are important inpractice-dependent motor
adapta-tion and learning in many different
systems, including those controllinglocomotion.16,17 Damage to
the cer-
ebellum affects the extent and rate atwhich individuals adapt
locomotionto new contexts.16 This suggests thatthe training of
individuals with cere-bellar pathology may require alonger duration
or intensity of prac-tice to improve locomotor function
regardless of the type of training.
The purpose of this case report is todescribe the effect of
locomotortraining using BWST in conjunction
with overground walking training on
mobility function in a 13-year-old pa-tient with severe
cerebellar ataxia.
Case DescriptionPatient DescriptionThe patient was a 13-year-old
girl
who had been healthy previouslyand who had a spontaneous
poste-rior fossa hemorrhage with resultantcerebellar and brainstem
infarcts.She was initially unresponsive andon a ventilator. She
regained con-
sciousness after approximately 11 weeks. In addition to
rendering hernonambulatory, initial sequelae fromthe hemorrhage
included ataxia, de-creased coordination, weakness, andmultiple
cranial nerve palsies.
This individual was selected for thecase report involving
locomotor
training using BWST for several rea-sons: one of her goals for
therapy
was to improve her ability to walkindependently, she was limited
inher ability to participate in mobilitytraining because she
required maxi-mum assistance of 2 people to walk,she had a brief
exposure (less than10% of total treatment time) to loco-
motor training using BWST duringher inpatient rehabilitation
stay and
was receptive to it, and her family was very supportive and
willing totransport her to the clinic for physi-cal therapy every
day. In addition,
Locomotor Training in a Child With Cerebellar Ataxia
January 2008 Volume 88 Number 1 Physical Therapy f 89
-
8/4/2019 Locomotor Training Using Body-SCI
3/10
during her inpatient stay, weights were tried on both limbs and
the
trunk to reduce ataxic movements,with no appreciable gains in
eitherfunctional limb movements or im-
proved postural stability in sitting,standing, or walking. The
patient be-gan the intervention outlined in thiscase report 16
months after herinjury.
Examination A physical therapist performed thetests and measures
before the begin-
ning of clinic training, immediatelyafter completion of clinic
training, 1month after completion of clinictraining, and after the
completion of4 months of home training. At thebeginning of the
intervention, (16months after the hemorrhage), ourpatient required
a tracheotomy andfeeding tube, she was dependent in
all activities of daily living, and sheused a wheelchair for
in-home andcommunity mobility.
Table 1 summarizes her physical im-pairments at the initiation
of train-ing. She exhibited significant ataxiaduring both upper-
and lower-extremity movements, including dys-
metria when reaching for objects,dysdiadochokinesia when
perform-ing rapid alternating movements,
weakness (4 out of 5 on the manualmuscle test),19 spasticity
greater onthe right side (score of 2 on the Mod-
ified Ashworth Scale),20 clonus, anda tight Achilles tendon on
the right
lower extremity. She also demon-strated multiple cranial nerve
palsies(left vocal cord paresis, facial nerve
palsies, and swallowing dysfunction)and sensory and perceptual
deficitsprimarily on the left side, includingdecreased vision,
decreased proprio-ception, and impaired hearing.
At the beginning of the intervention,she required the assistance
of 2 peo-ple to ambulate because of an inabil-
ity to maintain upright posture andto produce an appropriate
locomo-tor pattern in her legs. During gait,she exhibited poorly
coordinated legmovements, which resulted in ab-normal and variable
swing foot tra-
jectories and foot placement, in-creased variability in length
andtiming of steps, slow walking speed,
profound trunk sway, and an incon-sistent base of support
(alternatingtoo narrow or too wide). Because ofthe severity of her
gait impairment,locomotor training using BWST wasconsidered the
only feasible methodfor this patient to safely and consis-tently
practice walking. In addition,body-weight support allowed the
therapists to provide manual assis-tance with stepping rather
than hav-ing to assist with weight support andpostural
stability.
Her physical therapy diagnosis wasImpaired Motor Function and
Sen-
sory Integrity Associated With Non-progressive Disorders of the
CentralNervous SystemAcquired in Ado-
lescence or Adulthood (PreferredPhysical Therapist Practice
Pattern5D).21
Two measures of mobility were usedas outcome measures: the
PediatricFunctional Independence Measure(WeeFIM), specifically the
transfersand locomotion subscales,22,23 and
the Gillette Functional WalkingScale.24 The WeeFIM is a
modified
version of the Functional Indepen-dence Measure designed to
indicateseverity of disability based on theconcept of burden of
care, whichrefers to the amount of assistancerequired to perform a
given activity.The WeeFIM has 18 items in 6 sub-
scales; however, only the transfersand locomotion subscales were
con-sidered as outcome measures for thiscase report. We chose this
test for itsability to monitor change over timein children with
chronic disabilities.Ottenbacher et al23 found the re-sponsiveness
of the WeeFIM to bestatistically significant (P.05) for
detecting change in functional abili-ties in 174 children with
chronicdisabilities over a 1-year period.Interrater reliability is
high (intra-class correlation coefficient [ICC].90.99), as is
test-retest reliability
Table 1.Impairments in Body Structure and Function as Measured
at Baseline
Impairment Tests and Measures Finding
Spasticity Resistance to passive stretch measuring
using the modified Ashworth Scale
Right lower extremity: 2
Left lower extremity: 1
Strength Manual muscle test (05) 4/5 in bilateral lower
extremities, except
for hip extension and hip abduction
bilaterally (3/5)
Dysmetria Past pointing
Finger to nose
Heel to shin
Moderate impairment on all tests
Right heel cord tightness Goniometry 2 of neutral
Clonus Quick stretch 2 beats of clonus on right
Locomotor Training in a Child With Cerebellar Ataxia
90 f Physical Therapy Volume 88 Number 1 January 2008
-
8/4/2019 Locomotor Training Using Body-SCI
4/10
(ICC.98.99).22 Ottenbacher etal22 also demonstrated that the
ICC
was the highest (.99) for the trans-
fers and locomotion subscales thatwe used with our patient.
The Gillette Functional WalkingScale (the walking-scale portion
ofthe Gillette Functional Assessment)is a 10-level scale that
includes theentire range of walking abilities fromnonambulatory to
completely inde-
pendent ambulation in all commu-nity settings and terrains. This
scale
was chosen for its ability to help doc-ument current functional
status andfor its ability to evaluate change as aresult of
interventions, specifically to
track an individuals progress in es-tablishing more independent
gait. Itis a reliable tool both between and
within raters for a range of commu-nity ambulation over a time
frame of1 to 6 months.24 Good test-retest(ICC.92), intrarater
(ICC.92),and interrater (ICC.81) reliabilityhave been demonstrated,
and con-tent and concurrent validity (as-sessed using Pearson
correlations)also are significant at the .01 level.24
Mobility function also was measuredduring overground walking and
dur-ing treadmill walking. Distance andlevel of assistance required
wereused to evaluate overground mobil-ity function. In addition,
the numberof independent steps the patient wasable to take while
walking on the
treadmill was measured weekly dur-ing the clinic training and
then againat 1 and 5 months after completionof the clinic
training.
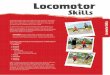
InterventionThe patient received locomotortraining using BWST on
a LiteGaitsystem (model LGI 500)25,* (Fig. 1) inconjunction with
practice in over-ground walking, 5 times a week for 4
weeks in the clinic. This was fol-
lowed by 4 months of training usingBWST in the home. At the
conclu-sion of the 4-week intervention inthe clinic, the patient
had no loco-motor training using BWST for 1
month because of a delay in locating
a suitable in-home treadmill system.Factors that affected the
selection ofa home unit included limited spacethat required a
treadmill that couldbe folded up and a treadmill thatcould be used
at a speed of0.2 m/s.
The family purchased a Vision Fit-
ness treadmill, and a Pneumex over-head frame and harness
(model07PW-1). The Pneumex harnessneeded to be altered because of
thepatients discomfort with the leg at-tachments to the support
harness. Agroin piece was ordered from Lite-Gait and altered to fit
the Pneumexharness to achieve the desired un-
weighting needed for training. Onceher home treadmill system was
in-stalled (Fig. 2), she continued her
locomotor training with BWST andoverground training for 30
minutes aday, 5 days per week, with the assis-tance of a home care
physical thera-pist or a trained rehabilitation aide.
In the clinic, each 1-hour treatmentsession consisted of 15
minutes oflocomotor training using BWST, fol-lowed by 15 to 20
minutes of over-ground walking training using theBWS harness. She
was seen for a totalof 19 sessions, and missed one treat-ment for
surgical revision of her
feeding tube. At the beginning ofeach session, the patient
donned aharness with assistance and wasbrought into the standing
positionand assisted onto the treadmill.
Training Parameters andProgressionThe parameters of training
that were
progressed with treatment are de-scribed below and summarized
inTable 2.
Training time. Initially, the pa-tient attempted to ambulate on
thetreadmill for 20 minutes with 2 rest
* Mobility Research, PO Box 3141, Tempe, AZ85280.
Vision Fitness, 500 South CP Ave, PO Box280, Lake Mills, WI
53551-0280. Pneumex Inc, 2605 N Boyer Ave, Sandpoint,ID 83864.
Figure 1.Body-weightsupported treadmill training system used in
the clinic.
Locomotor Training in a Child With Cerebellar Ataxia
January 2008 Volume 88 Number 1 Physical Therapy f 91
-
8/4/2019 Locomotor Training Using Body-SCI
5/10
breaks. As she fatigued, her step con-trol deteriorated and she
requiredgreater assistance; therefore, 15 min-utes was set as the
maximum time
for treadmill walking for the remain-ing sessions. The gait
training recom-mendations issued by the manufac-turer of the
body-weightsupportedtreadmill training system25 were fol-lowed,
including keeping each tread-mill training session to 15 minutes
orless, ensuring that the patient tookmost of the steps with
correct pat-
terns, and ending each session whenthe therapist or patient
fatigued orthe patients gait deteriorated. By theend of training,
this patient was ableto walk on the treadmill for 15 min-utes with
no rests. She was initially
able to tolerate only 5 minutes ofoverground walking with
body-
weight support but progressed to 15to 20 minutes with gradually
de-
creasing percentage of support.
Body-weight support. The levelof body-weight support
(determinedby using a scale to measure body
weight while standing on the tread-mill in the harness) was
adjustedacross sessions to maximize uprightposture and independent
stepping.
Initially, the harness provided ap-proximately 30% of
body-weightsupport for walking on the treadmilland during
overground walkingpractice. This was progressively de-creased to
10% of body-weight sup-
port by the second month of training.
Manual assistance. Amount andtype of manual assistance was
de-
creased across training sessions. Ini-tially, 3 physical
therapists were re-quired to provide manual assistanceto the
patient while walking on thetreadmill in the support harness.One
physical therapist assisted witheach lower leg by placing one
hand
at the top of each foot to facilitatetoe clearance at swing
phase andheel-strike at initial stance and theother hand behind the
knees to pre-
vent knee hyperextension. As shownin Figure 1, the therapists
providing
manual assistance to control lower-limb placement either
squatted orsat on the edge of the treadmill ap-
paratus or on a low stool. A thirdassistant stabilized the
patient at thehips and manually assisted with pel-
vic rotation. The patient was initiallyinstructed to hold
lightly onto hand-rails to provide additional supportand upright
posture on the treadmillas needed. Upper-extremity support
was discontinued 2 months after the
start of training, when the patientwas able to maintain a
vertical trunkposition without the assistance ofher arms; however,
she still requiredmanual assistance from the therapistat the hips.
This assistance at thehips was maintained for almost 4months
because of her severe ataxiaof the trunk.
Training speed. Based on re-search with a stroke population
thatshowed the efficacy of increasedtraining speed on locomotor
out-comes,26 our goal was to train gait atthe fastest speed
manageable by thepatient. However, Hidler27 sug-gested that
training speeds need to
be set according to each personsability to retain adequate motor
con-trol of his or her legs. At the begin-ning of training, our
patient required3 people to help her walk at a tread-mill speed of
0.18 m/s with approx-
Figure 2.Body-weightsupported treadmill training system used in
the home.
Locomotor Training in a Child With Cerebellar Ataxia
92 f Physical Therapy Volume 88 Number 1 January 2008
-
8/4/2019 Locomotor Training Using Body-SCI
6/10
imately 30% of body-weight support. We tried to increase her
trainingspeed, but found that if we at-
tempted to increase treadmill speedfaster than 0.31 m/s, our
patient wasnot able to retain adequate motorcontrol and stepping
ability. We
were not able to increase speed afterthe second week in the
clinic, andthe patient consistently trained at ap-proximately 0.3
m/s.
Visual cues for foot placement.Because of impaired
lower-extremityproprioception, the patient used vi-sual cues to
guide foot placementduring walking; however, this led toa forward
head and trunk posture
that decreased her postural stability. We alternated practicing
stepping with visual guidance (eg, looking at
her feet while walking) with lookingstraight ahead (increased
use of pro-prioceptive and kinesthetic cues forfoot placement). The
amount of timespent in visually guided foot place-ment was
gradually decreased, al-lowing the patient to gradually in-crease
the number of steps she wasable to take independently without
visual guidance for foot placement.
Progression of training parametersinvolved first reducing the
amount ofmanual assistance of the legs pro-
vided by therapists to improve step-
ping ability, then reducing body- weight support while
maintainingindependent stepping ability, and fi-
nally increasing speed of trainingwhile maintaining both
postural sta-bility and independent stepping abil-ity. Concomitant
to the progressionof treadmill training parameters, weincreased the
time and duration ofoverground walking training, pro-gressively
decreased body-weightsupport in the harness, and in-
creased gait speed during over-ground walking. The decision to
pri-oritize independent stepping ability(decreased manual
assistance) overpostural stability (decreased body
weight in the harness) was twofold:
Table 2.Parameters for Training on a Treadmill and Overground
Training With Body-Weight Support a
Clinic Training (1 mo) NoTraining(1 mo)
Home Training (4 mo)
Week 1(Pretest)
Week 2 Week 3 Week 4(Posttest)
1-MonthRetentionTest
Months 34 Months 56
Treadmill time
(min)
15 15 15 15 15 15 15
Treadmill
speed (m/s)
0.18 0.31 0.31 0.31 0.36 0.54 0.54
Body-weight
support
30% 25% 20% 15% 15% 10% 10%
No. of rest
breaks
required
2 1 0 0 0 0 0
Amount ofassistance 3 people 3 people 3 people 13 people 1
person 1 person CG/SBA
Overground
walking time
with BWS
(min)
5 12 15 15 15 N/A N/A
Distance
walked
overground
with BWS
(m)
50 91 125 157 188 N/A N/A
Distance
walked
overground
without BWS
(m)
8 with 4WW 152 with U-Stepb
a BWSbody-weight support, N/Anot applicable, CG/SBAcontact guard
or standby assist, 4WW4-wheeled walker.b In-Step Mobility Products
Corp, 8027 N Monticello Ave, Skokie, IL 60076.
Locomotor Training in a Child With Cerebellar Ataxia
January 2008 Volume 88 Number 1 Physical Therapy f 93
-
8/4/2019 Locomotor Training Using Body-SCI
7/10
first and foremost, the patient herselfwas strongly committed to
moving
her limbs independently, and, sec-ond, manually advancing the
limbs
was physically taxing and fatiguingto the therapists. As the
patient be-gan to master independent stepping,body-weight support
was reduced.Each session she attempted to ambu-late by loading the
maximum weightshe was able to support and still
maintain adequate stepping ability.Training time on the
treadmill wasconsistently set at 15 minutes, buttime spent on
walking overground
was increased as the patient devel-oped stepping ability and
tolerancefor physical activity.
Vital signs were monitored daily in
her home by a registered nurse andwere stable, so they were not
takenin the clinic. Oxygen saturation lev-els were taken when the
patientshowed any signs of respiratory dis-tress, and they did not
go below90%.
Our patient also received in-home
physical therapy twice a week for90-minute sessions from the
time ofher discharge home from the reha-bilitation center 6 months
prior tothe clinic intervention, during the4-week session of
training using
BWST in the clinic, and for at least ayear afterward. The goals
of her in-
home physical therapy program were to increase strength and
coor-dination, to improve her ability tomaintain balance in sitting
and stand-ing, and to increase independence intransfers. Specific
interventions aresummarized in the Appendix.
Outcomes
Table 3 compares scores on the 3primary outcome measures over
thecourse of the intervention. Prior totraining, her score on the
GilletteFunctional Walking Scale was 2 (cando some stepping on her
own withthe help of another person, but doesnot take full weight on
her feet or
walk on a regular basis) and re-
mained at 2 at the 4-week mark (ie, when the clinic training was
com-pleted) and at retention test 1 monthafter completion of the
clinic train-ing. Six months after initiation of theintervention,
her score improved to6 (walks for household distances).
Prior to training, her score on the
WeeFIM was 3 (moderate assistance)for transfers and 2 (maximum
assis-tance) for walking. At 4 weeks and atthe retention test 1
month after thecompletion of the clinic training, hertransfer score
improved to 4 (mini-
mal assistance), but her walkingscore did not change. Six
months
after the initiation of the interven-tion, her score was 6
(modified inde-pendence) for transfers and 5 (super-
vision) for walking.
The number of independent stepstaken during treadmill walking
was 0prior to training, and improved
weekly to 128 steps at 4 weeks and
to 200 steps at the1-month follow-upafter completion of the
clinic train-ing. Six months after initiation of theintervention,
all steps on the tread-mill were unassisted.
As noted in Table 2, there was asteady improvement in all
trainingparameters for the training using
BWST, including: an increase in gaitspeed from 0.18 to 0.31 m/s
on thetreadmill, increased endurance asshown by fewer rest breaks
duringthe 15-minute treadmill sessions, de-creased body-weight
support fromapproximately 30% to 15%, and de-creased level of
assistance requiredfor walking on the treadmill from 3
people to 1 person.
The body-weight support harnesswas used during overground
walkingtraining during the first 4 weeks oftraining. In the home
setting, how-
Table 3.Intervention Outcomes
Pretest Week 2 Week 3 Posttest 1-MonthRetention
TrialWithoutTraining
6-MonthFollow-up
Gillette Functional
Walking Scalea2 NTb NT 2 2 6
WeeFIMc transfers
subscale
3 NT NT 4 4 6
WeeFIM mobility
subscale
2 NT NT 2 2 5
No. of unassisted
steps
0 10 84 128 200 All
a Range of scores: 110.b NTnot tested.cWeeFIMPediatric
Functional Independence Measure (range of scores: 17).
Locomotor Training in a Child With Cerebellar Ataxia
94 f Physical Therapy Volume 88 Number 1 January 2008
-
8/4/2019 Locomotor Training Using Body-SCI
8/10
ever, the harness was anchored tothe ceiling and, therefore, was
notavailable for overground walking
training. At 2 weeks, the assistivegait device was changed from
a rear
support walker, which she wasnever able to successfully control,
toa front 4-wheeled walker. A U-Step
walker was introduced at home 2months into her home training.
Asshown in Table 2, there was steadyimprovement in overground
walk-
ing, as indicated by a gradual in-crease in the distance walked
from50 m at 1 week to 152 m at thecompletion of training, and a
reduc-tion in the personal assistance re-quired from maximum
assistance
from 3 people to supervision by 1person.
DiscussionThis case report examined the effect
of locomotor training using BWST inconjunction with home
physicaltherapy on mobility function in a 13-
year-old girl with severe cerebellarataxia. After 5 months of
this train-ing, our patient progressed from be-ing nonambulatory at
the start of
training to being able to walk 152 m with supervision using a
U-Step
walker. Other functional improve-ments included improved
indepen-dence in transfers. She continued touse her wheelchair for
long dis-tances in the community and for in-dependent mobility in
the home.Her increased independence in step-ping on the treadmill
after 4 weeksof training with BWST in the clinic
encouraged the family to purchase a
BWST system for the home so thattraining could be continued 5
days a week for 4 months. She continuedto make slow, but steady,
gainsthroughout her 5 months of training,despite the fact that
training was be-gun 16 months after her injury.
Previous research28,29 suggests that,following a neurologic
injury such asstroke, physical improvements pla-
teau after 6 months. However, re-cent studies examining the
effect of
constraint-induced therapy in people with stroke have suggested
thatgains can be made with intensivetherapy several years after the
inju-ry.30 Consistent with this research,our patient, whose injury
occurred16 months previously, made signifi-
cant functional gains with intensivephysical therapy (5 days per
weekfor 5 months) that included locomo-tor training using BWST in
conjunc-tion with overground walking.
Our results are similar to those of thecase report by Day et
al13 on a 9-year-old boy with cerebral palsy who was
nonambulatory but was able to com-plete up to 60 independent
steps onthe treadmill with body-weight sup-port after 44 sessions
of training anddemonstrated carryover to over-ground walking by
walking short dis-tances with a rolling walker withminimal
assistance 4 months aftertraining. In our patient, functional
independence in walking wasachieved only after 5 months
(ap-proximately 99 training sessions us-ing BWST). This suggests
that, in ad-dition to intensity, duration is acritical factor in
determining out-comes. Although walking on thetreadmill improved
steadily over thefirst month, significant improve-
ments in overground walking werenot seen until after 5 months
oftraining.
We believe that a number of factorscontributed to the outcomes,
includ-ing the motivation of the patient andthe support and
dedication of herfamily. This family was able to afford
a home BWST system and was will-ing to work with her 5 days
per
week. In addition, she received in-home physical therapy and
occupa-tional therapy several times a weekas well as benefiting
from additional
time from a trained rehabilitationaide. The relative
contribution of lo-comotor training using BWST to the
outcomes in light of the fact that shereceived additional
interventions
cannot be determined. It is notewor-thy, however, that she was
nonam-bulatory after 1 year of in-home ther-apy, but achieved
independentambulation with the addition of 5months of intensive
locomotor train-ing using BWST.
Results from this case report suggestthat locomotor training
using BWSTis a promising intervention for im-proving gait in
patients with severecerebellar ataxia who are nonambu-
latory. Functional gains in walking,however, may require months
ofconsistent practice and training.
Findings from this case report pro- vide possible support for
researchdemonstrating the importance ofcerebellar structures in
locomotor ad-aptation and in practice-dependentmotor learning.16,17
It also supportsfindings that the rate of locomotor ad-aptation and
thus motor recoverymay be slower in the presence of
cerebellar pathology compared withother brain regions.16,17 The
inten-sity and duration of locomotor train-ing using BWST required
to achievefunctional gains in patients withlesser severity of
injury is notknown. In addition, it is not clearhow much additional
therapy isneeded to achieve these outcomes.
Studies are needed to determine theoptimal intensity and
duration of lo-comotor training to optimize func-tional walking
outcomes followingcerebellar pathology.
Dr Shumway-Cook provided concept/idea/research design. Dr
Cernak, Ms Stevens, andDr Shumway-Cook provided writing,
dataanalysis, and project management. All au-thors provided data
collection. Ms Stevensprovided the subject. Mr Price provided
fa-cilities/equipment. Mr Price, Ms Stevens, DrShumway-Cook,
Valerie Kelly, and StaciaLee, PT, provided consultation (including
re-view of manuscript before submission).
In-Step Mobility Products Corp, 8027 N Mon-ticello Ave, Skokie,
IL 60076.
Locomotor Training in a Child With Cerebellar Ataxia
January 2008 Volume 88 Number 1 Physical Therapy f 95
-
8/4/2019 Locomotor Training Using Body-SCI
9/10
This manuscript was received May 3, 2007,and was accepted August
7, 2007.
DOI: 10.2522/ptj.20070134
References
1 Barbeau H, Visintin M. Optimal outcomesobtained with
body-weight support com-bined with treadmill training in stroke
sub-
jects. Arch Phys Med Rehabil. 2003;84:14581465.
2 Latham NK, Jette DU, Slavin M, et al. Phys-ical therapy during
stroke rehabilitationfor people with different walking
abilities.Arch Phys Med Rehabil. 2005;86(12 suppl2):S41S50.
3 Lord SE, McPherson K, McNaughton HK,et al. Community
ambulation after stroke:how important and obtainable is it and
what measures appear predictive? ArchPhys Med Rehabil.
2004;85:234239.
4 Schenkman M, Cutson TM, Zhu CW, Whetten-Goldstein K. A
longitudinal eval-
uation of patients perceptions of Parkin-sons disease.
Gerontologist. 2002;42:790798.
5 Hesse S, Bertelt C, Jahnke MT, et al. Tread-mill training with
partial body weight sup-port compared with physiotherapy
innonambulatory hemiparetic patients.Stroke. 1995;16:976 981.
6 Laufer Y, Dickstein R, Chefez Y, MarcovitzE. The effect of
treadmill training on theambulation of stroke survivors in the
earlystages of rehabilitation: a randomizedstudy. J Rehabil Res
Dev. 2001;38:69 78.
7 Barbeau H. Locomotor training in neuro-rehabilitation:
emerging rehabilitationconcepts. Neurorehabil Neural
Repair.2003;17:311.
8 Behrman AL, Lawless-Dixon AR, Davis SB,et al. Locomotor
training progression andoutcomes after incomplete spinal cord
in-
jury. Phys Ther. 2005;85:13561371.
9 Behrman AL, Bowden MG, Nair PM. Neu-roplasticity after spinal
cord injury andtraining: an emerging paradigm shift in
re-habilitation and walking recovery. PhysTher. 2006;86:1406
1425.
10 Moseley AM, Stark A, Cameron ID, PollockA. Treadmill training
and body weight sup-port for walking after stroke. CochraneDatabase
Syst Rev. 2005;(4):CD002840.
11 Wernig A, Muller S, Nanassy A, Cagol E.Laufband therapy based
on rules of spinallocomotion is effective in spinal cordinjured
persons. Eur J Neurosci. 1995;7:1429.
12 Dietz V, Harkema S. Locomotor activity inspinal cord-injured
persons. J Appl Physiol.2004;96:19541960.
13 Day JA, Fox EJ, Lowe J, et al. Locomotortraining with partial
body weight supporton a treadmill in a nonambulatory child
with spastic tetraplegic cerebral palsy: acase report. Pediatr
Phys Ther. 2004;16:106113.
14 Helbostad JL. Treadmill training and/or
body weight support may not improve walking ability following
stroke. Aust JPhysiother. 2003;49:278.
15 Stolze H, Klebe S, Petersen G, et al. Typi-cal features of
cerebellar ataxic gait. J Neu-rol Neurosurg Psychiatry.
2002;73:310312.
16 Morton SM, Bastian AJ. Cerebellar controlof balance and
locomotion. Neuroscien-tist. 2004;10:247259.
17 Morton SM, Bastian AJ. Mechanisms of cer-ebellar ataxia.
Cerebellum. 2007;6:7986.
18 Morgan MH. Ataxia and weights. Physio-therapy.
1975;61:332334.
19 Kendall FP, McCreary EK. Muscles: Testingand Function. 3rd
ed. Baltimore, Md: Wil-
liams & Wilkins; 1983.20 Bohannon RW, Smith MB. Interrater
reli-
ability of a modified Ashworth scale ofmuscle spasticity. Phys
Ther. 1987;67:206207.
21 Guide to Physical Therapist Practice. Rev2nd ed. Alexandria,
Va: American PhysicalTherapy Association; 2003.
22 Ottenbacher KJ, Taylor ET, Msall ME, et al.The stability and
equivalence reliability ofthe Functional Independence Measure
forChildren (WeeFIM). Dev Med Child Neu-rol. 1996;38:907916.
23 Ottenbacher KJ, Msall ME, Lyon N, et al.The WeeFIM
instrument: its utility in de-tecting change in children with
develop-mental disabilities. Arch Phys Med Reha-bil.
2000;81:823829.
24 Novacheck TF, Stout JL, Tervo R. Reliabil-ity and validity of
the Gillette Functional
Assessment Questionnaire as an outcomemeasure in children with
walking disabil-ities. J Pediatr Orthop. 2000;20:7581.
25 Partial Weight Bearing Gait Training Pro-tocol using
LiteGait. Available at: http://
www.litegait.com/protocols.htm. Ac-cessed September 22,
2005.
26 Sullivan KJ, Knowlton BJ, Dobkin DH.Step training with body
weight support:
effect of treadmill speed and practice par-adigms on poststroke
locomotor recovery. Arch Phys Med Rehabil. 2002;83:683691.
27 Hidler JM. What is next for locomotor-based studies? [Guest
editorial.] J Rehabil Res Dev. 2005;42:xixiv.
28 Duncan PW, Goldstein LB, Matchar D,et al. Measurement of
motor recovery af-ter stroke: outcome assessment and sam-ple size
requirements. Stroke. 1992;23:10841089.
29 Duncan PW, Lai SM, Keighley J. Definingpost-stroke recovery:
implications for de-sign and interpretation of drug trials.
Neu-ropharmacology. 2000;39:835841.
30 Wolf SL, Winstein CJ, Miller JP, et al; EX-CITE
Investigators. Effect of constraint-induced movement therapy on
upper ex-tremity function 3 to 9 months afterstroke: the EXCITE
randomized clinical tri-al. JAMA. 2006;296:20952104.
Locomotor Training in a Child With Cerebellar Ataxia
96 f Physical Therapy Volume 88 Number 1 January 2008
-
8/4/2019 Locomotor Training Using Body-SCI
10/10
Appendix.Summary of Home Physical Therapy Interventions
Balance
1. Sitting unsupported with light beam target
2. High kneeling with bench for upper-extremity support3. Knee
walking with walker and without walker
4. Standing balance: Feet apart Feet together Split stance
Weight shifting Stepping without assistive device
Mobility1. Crawling on forearms
On extended arms2. Transfers
Wheel to chair and back Wheelchair to floor Floor to wheelchair
Sit to stand and back to sitting
3. Gait
Treadmill with harness
Gait with 4-wheeled walker
Gait with U-Step walkera
Strength1. Progressive resistive exercises for core and
extremities2. NuStep (model TRS4000)b with resistance
a In-Step Mobility Products Corp, 8027 N Monticello Ave, Skokie,
IL 60076.b NuStep Inc, 5111 Venture Dr, Ste 1, Ann Arbor, MI
48108.
Locomotor Training in a Child With Cerebellar Ataxia
January 2008 Volume 88 Number 1 Physical Therapy f 97




![[T] Locomotor training with partial body weight support in ... · the keywords: body weight-supported, treadmill trai-ning, spinal cord injury, gait training, robotic-assisted, treino](https://img.pdfslide.us/doc/110x75/5d1ca8c088c993fc268d8a5b/t-locomotor-training-with-partial-body-weight-support-in-the-keywords.jpg)