Embed Size (px)
Citation preview
Local Professional Networks - PharmacyAgenda
• How do we work as a group? – agreements from telecon
• Call to action – update and key emerging key themes . Discussion about how LPN chairs engaged with the “Call to action” and a discussion about emerging themes and next steps
• Consultation Skills for Pharmacy Practice• Summary care record – update from SCR national
team• LPN chair development needs – Jane Brown to
lead. David Geddes to join.
1

Terms of Reference• Agreed to two national Pharmacy days and two afternoon
slots at national LPN assembly events per year.
• We will feed back to central support team after each event with a short report.
• Regional Pharmacists will have a role in supporting LPN chairs in each region.
• Purpose of national days will be
To share national strategy
To hear from LPN Chairs on progress
To support LPN Chairs in their development in the role.
To provide a network
2

IMPROVING HEALTH AND PATIENT CARE THROUGH COMMUNITY PHARMACY–A CALL TO ACTION
NHS England
December 2013

Purpose of the Call to Action
Every year in England, 438 million visits are made to community pharmacy for health related reasons. This is more that any other NHS care setting.
NHS England is, through this call to action, seeking to secure community pharmacy services that deliver great outcomes cost effectively, reaching into every community and which make the most the expertise of Pharmacists and of Pharmacy’s unique accessibility for patients in England.
The main purpose of this community pharmacy Call to Action is to stimulate debate in local communities, to shape local strategies for community pharmacy and to inform NHS England’s strategic framework for commissioning community pharmacy.
4

Some personal reflections• Area Teams did an amazing job at short notice
• People responded positively and it wasn’t a wish list for community pharmacy. The focus was patients, medicines and services.
• National stakeholder event went well.
• Patient engagement. Seldom heard voices work in train.
5
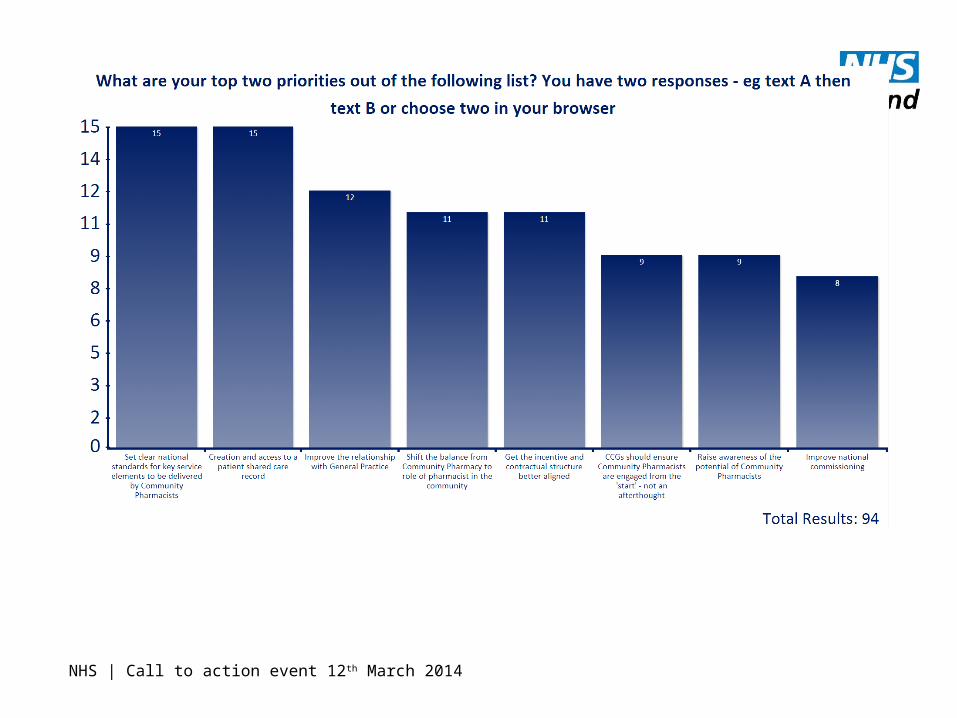
NHS | Call to action event 12th March 2014
6
So, emerging themes from your events• How did you organise them?
• What was your role?
• What did you hear?
• How will you progress the work locally?
7

Next steps• Submissions to this address [email protected]
• We will work through the submissions
• Agree with the overall primary care at scale group what the priorities are.
• There will be some overlaps with UECR
• A strategic outline will be produced in 2014.
8

Launch of Consultation Skills for Pharmacy Practice
9
Educational solutions for the NHS pharmacy workforce
Consultation skills for pharmacy practice
10
Cross organisation project
Wide range of skill set throughout the profession
Phase 1 launched 18th March 2014

Educational solutions for the NHS pharmacy workforce
Achieving the patient-centred approach
True partner: Shared decision making
Give options (rather than
recommen-dations)
Listen (rather than
telling)
Respect their
beliefs, knowledge
and concerns
11

Educational solutions for the NHS pharmacy workforce
A range of learning, tools, resources and signposting
12
Online learning, forms, videos, hints and tips, employers information, trainers support, social media
www.consultationskillsforpharmacy.com

Educational solutions for the NHS pharmacy workforce
Six step model to improvement
Why?
What standard?
Where am I?
How do I improve?
Check my learning?
Ongoing improvement?
13
Summary Care Record• Sharon Wilson and Mohammed Hussain
14

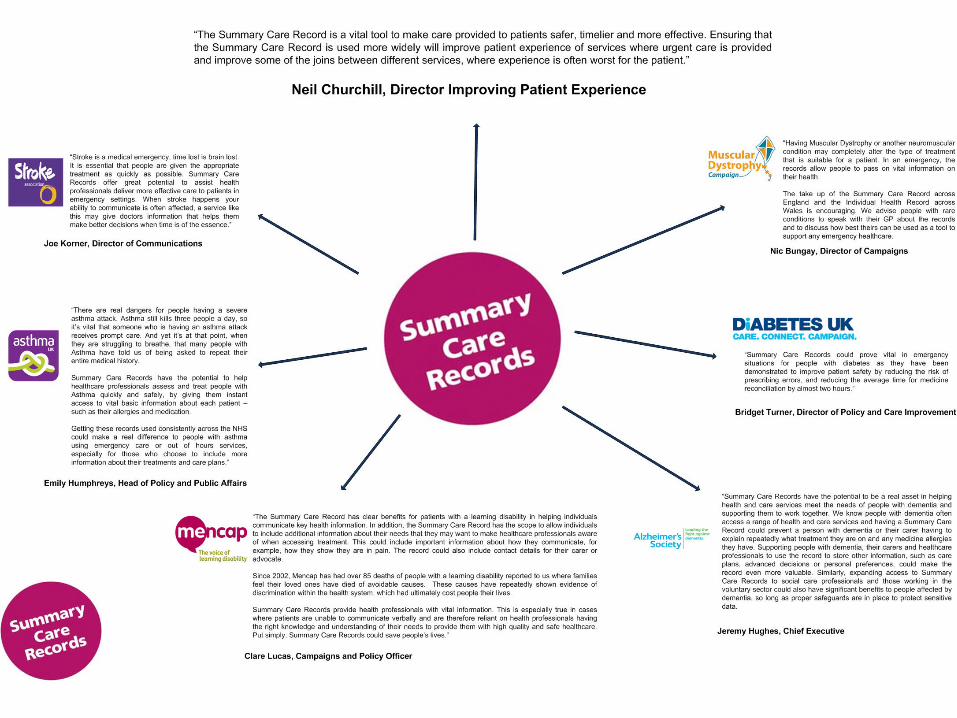
The Summary Care Record
Delivering vital information to the heart of urgent and emergency care
15
Mohammed Hussain MRPharmS, SCR Pharmacy LeadSharon Wilson, Senior Implementation Manager
What is the SCR?
• The SCR is an electronic summary of key health information.
• It will hold limited essential information – extracted electronically from the patient’s GP record and held securely on the National Spine.
• Core data – Medications, Allergies and Adverse Reactions
• Additional information can be included at the request of, or with the explicit consent of, the patient.
• Patients will be asked for ‘Permission to View’ their SCR before it is accessed.

SCR benefits – high level
• Improved patient safetyreducing the risk of prescribing errors and adverse reactions to prescribed medication.
• Increased efficiency and effectiveness reducing time, effort and resource required to share information across different NHS organisations.
• Increased quality of patient careenabling the most appropriate care to be delivered
in the most appropriate setting.
The SCR – main ‘selling points’ . . .
• 60% - 70% of patients presenting for urgent or emergency care are not able to provide an accurate medication history.
• Contacting the GP surgery to obtain that information is time consuming and depends on the GP surgery being open - so cannot be undertaken out of hours, at weekends or bank holidays, but has to wait until the next working day – sometimes three or four days away.
• SCR – instantly available – 24/7

The SCR – main ‘selling points’ . . .
• SCR viewing is cheap and easy to implement
• Key clinical information - for urgent care
• Single source of data – GP record
• Data Security/IG processes assured
• A national (England) record - not a local record
• Political, professional and patient backing
• Commissioned by NHS England

Areas Viewing the SCR currently
More than 15,000 SCRs are being viewed each week in the following care settings (more than one a minute!):
• 179 GP Out of Hours care settings
• Pharmacists in 127 hospitals
• 20 hospital Emergency Departments
• Acute admissions wards in 37 hospitals
• 110 Community & Intermediate Care teams
• 58 Walk in Centres/Minor Injuries Units

• 35.5 million people in England now have a SCR –that’s over 60% of the population.
• 4,880 GP practices have created records.
• The opt out rate is just 1.4%.
• As at March 14th 2014
National roll-out of the SCR
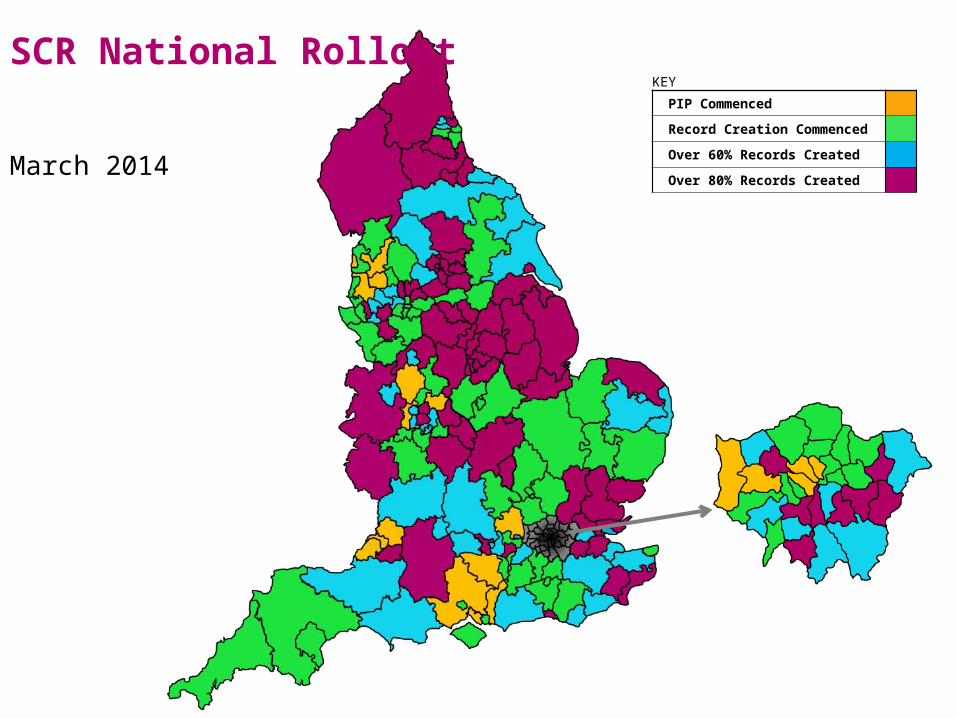
SCR National Rollout
March 2014
KEY
PIP Commenced
Record Creation Commenced
Over 60% Records Created
Over 80% Records Created
Viewing Summary Care
Records
Enabling SCR viewing is easy . . .• NHS Smartcards for authorised staff, and readers on
computers
• Secure N3 connection
• Some training (mainly on Information Governance)
• The organisation needs to identify a Privacy Officer who can audit emergency access and any self-claimed access to ensure that there is no malicious or inappropriate viewing.
• Patients need to be asked for Permission to View their SCR. If they are unable to give permission (because not mentally competent, confused or unconscious) staff should use emergency access in the patient’s best interest.
. . .That’s it!
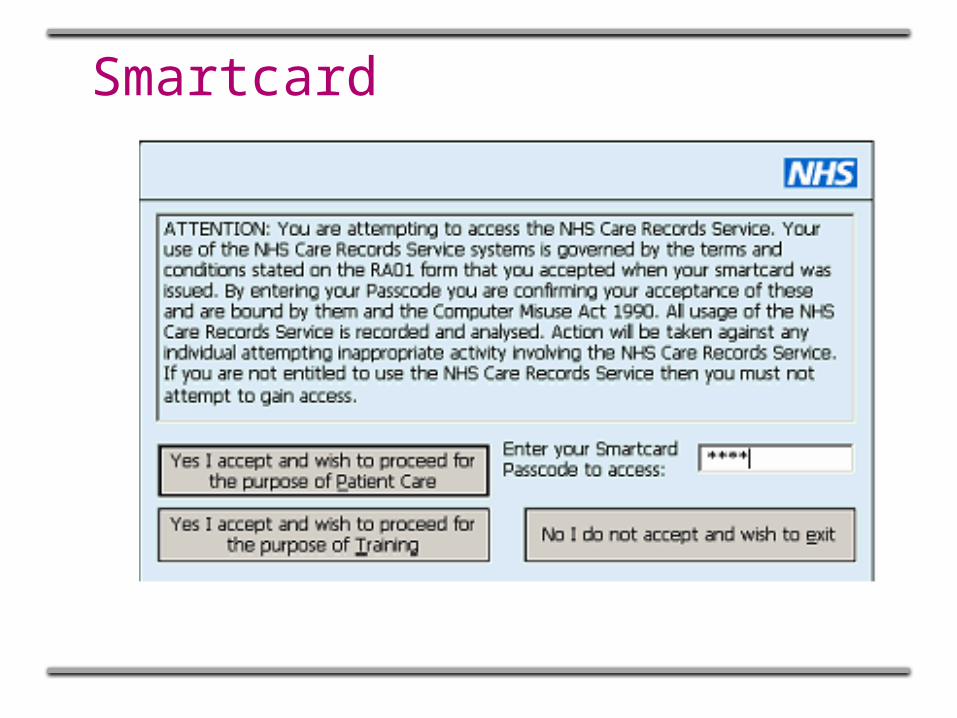
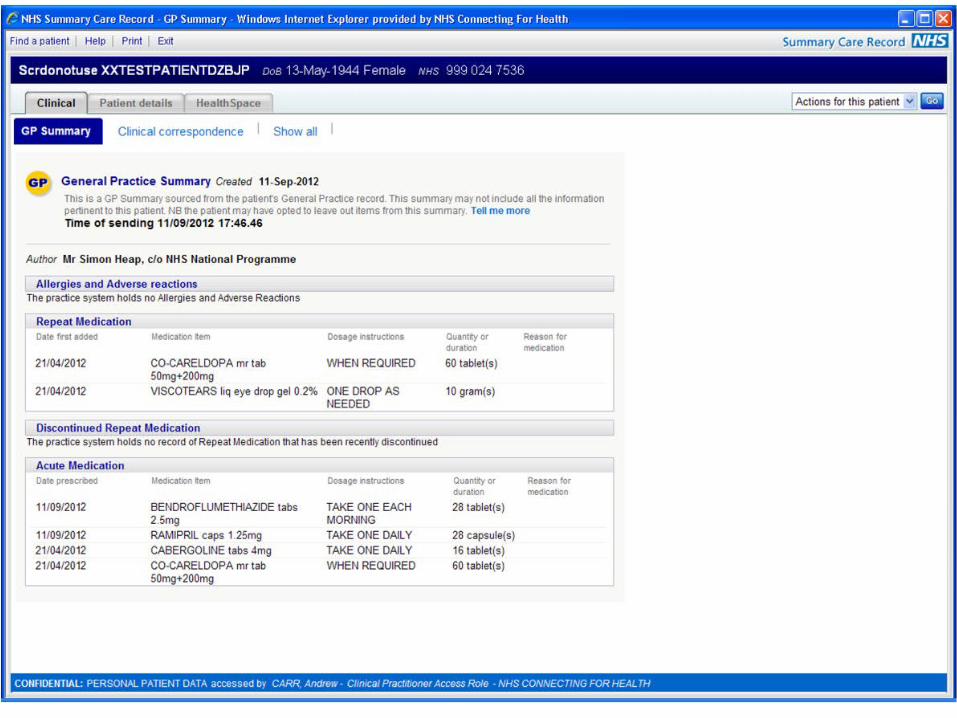
Smartcard

Open spine portal

Find patient

Confirm patient details
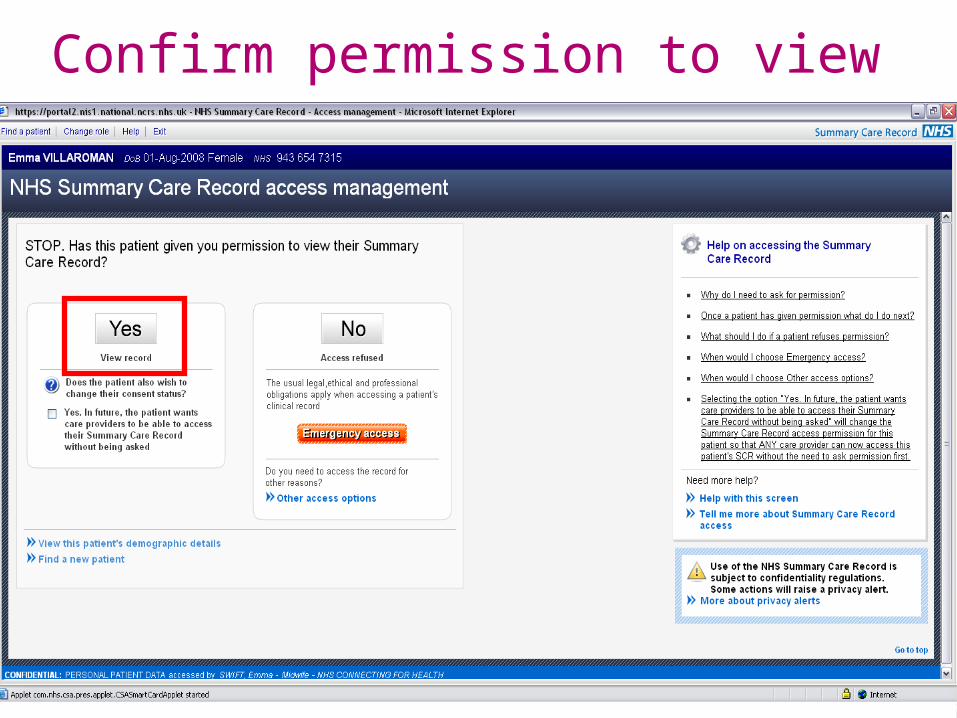
Confirm permission to view

Create a legitimate relationship
View SCR

Alternatively, 1 person in the pharmacy can “register the patient”


And then someone else views it

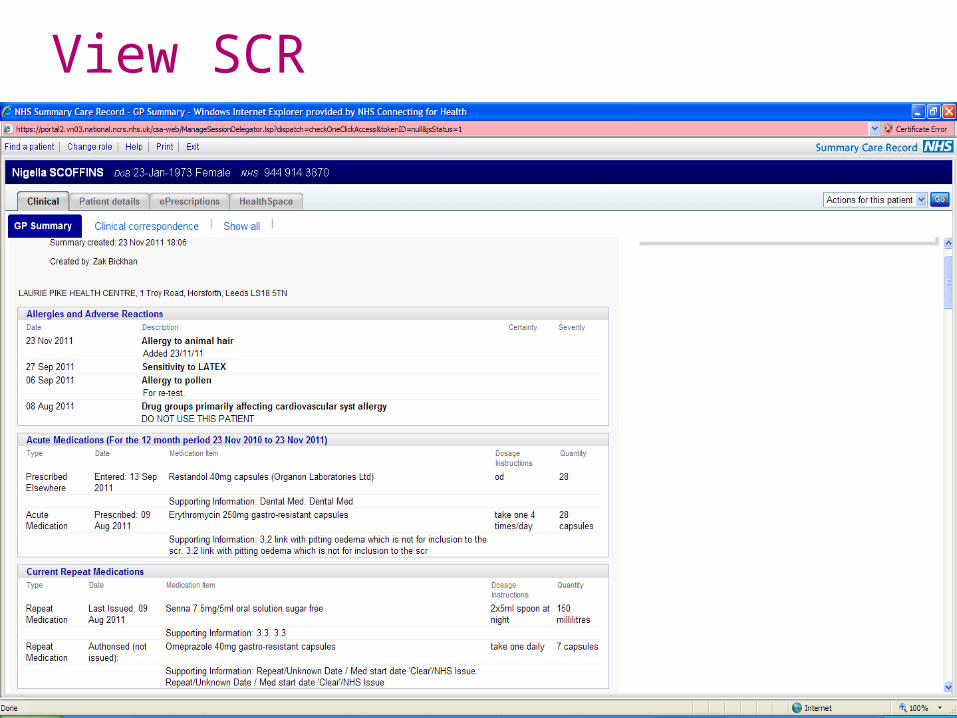
Some records though will look slightly different……

Old SCR view

SCR use by hospital pharmacists
• Sheffield: SCR use has reduced the average time for medicines reconciliation from 2 hrs 9 mins to just 19 mins.
• Leeds: Using SCRs reduced the time taken to complete medicines reconciliation by 55%. It currently takes only 19 minutes. The team is now meeting the 24 hr target 87% of the time (it was previously 57%).
“Pharmacists love the SCR because it makes their life a lot easier. This translates into a better service for patients, more accurate patient notes and as a result improved patient safety.” Una Laverty, Medicines Risk Manager – Leeds TH

“From 1 April 2014 GP practices will be contractually required to:
• provide an automated upload of their summary information on at least a daily basis to the Summary Care Record, or have a published plan in place to achieve this by 31 March 2015.”
Outcome of the contract negotiations between the BMA’s General Practitioners Committee (GPC) and NHS Employers (on behalf of NHS England) on amendments that will apply to GMS contractual arrangements in England from April 2014.
15th November 2013
The Future of the SCR
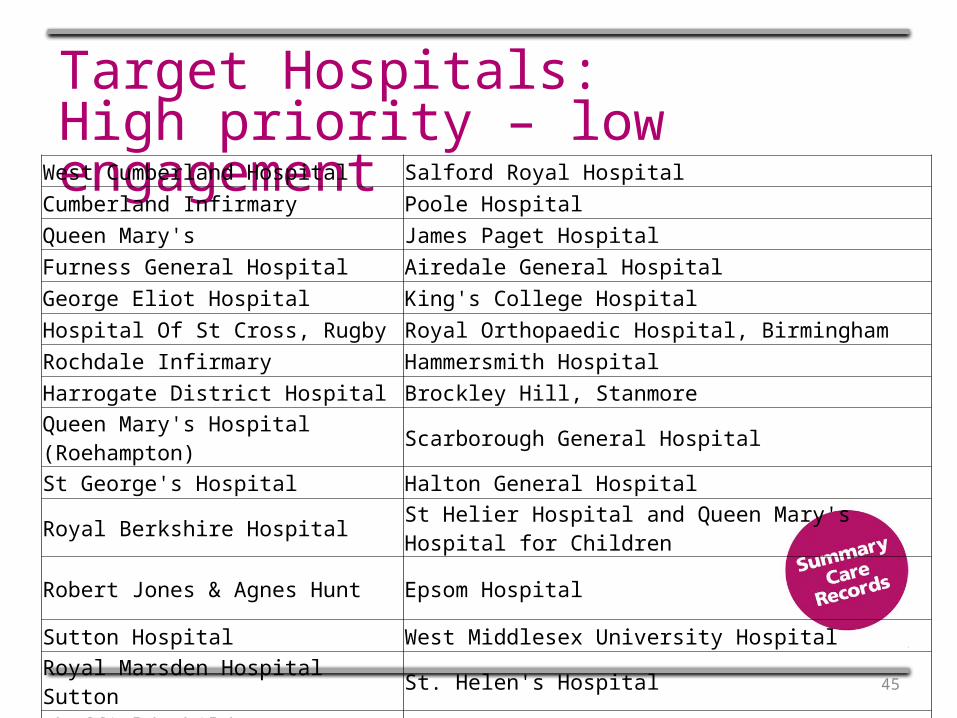
Target Hospitals:High priority – low engagement
45
West Cumberland Hospital Salford Royal HospitalCumberland Infirmary Poole HospitalQueen Mary's James Paget HospitalFurness General Hospital Airedale General HospitalGeorge Eliot Hospital King's College HospitalHospital Of St Cross, Rugby Royal Orthopaedic Hospital, BirminghamRochdale Infirmary Hammersmith HospitalHarrogate District Hospital Brockley Hill, StanmoreQueen Mary's Hospital (Roehampton) Scarborough General HospitalSt George's Hospital Halton General HospitalRoyal Berkshire Hospital St Helier Hospital and Queen Mary's Hospital for Children
Robert Jones & Agnes Hunt Epsom Hospital
Sutton Hospital West Middlesex University HospitalRoyal Marsden Hospital Sutton St. Helen's HospitalSheffield Children's Hospital Tameside General Hospital
Useful linksSCR website:www.hscic.gov.uk/scrwww.nhscarerecords.nhs.uk
SCR case studies:http://systems.hscic.gov.uk/scr/staff/aboutscr/comms/case
SCR deployment map:http://systems.hscic.gov.uk/scr/staff/impguidpm/deploy
Subscribe to our newsletter:http://systems.hscic.gov.uk/scr/staff/bulletin/maillist
Follow us on Twitter:www.twitter.com/NHSSCR

Thank you very much –
Happy to take questions . . .(Don’t forget to find out if your GP Practice has created a Summary Care Record for you and for each member of your family . . .)
47
Urgent an emergency care reviewAreas where the Community Pharmacy work programme will help delivery.
• Better support for self care/ advance care planning
• Right advice, right place, first time, NHS 111, referral rights through UEC system. Directory of services
• Highly responsive out of hospital care
• Specialist centres to maximise care
• Connecting services so the system is more than the sum of its parts
• NHS choices digital platform
48
LPN Chair development needs.• What would be in your wish list?
• Think leadership, influencing skills, negotiation etc
49
Issues for future agendas• Co- commissioning
• LETBEs ( including prescribing pharmacists0
• UECR
• Network – how do we have a closed network.
• Healthwatch
• Delayed discharge
50





























