Embed Size (px)
Citation preview

LocalFoodPrices,SNAPPurchasingPower,andChildHealth*
ErinT.BronchettiDepartmentofEconomics,SwarthmoreCollege
GarretChristensenBerkeleyInstituteforDataScience,UCBerkeley
HilaryW.HoynesDepartmentofEconomicsandPublicPolicy,UCBerkeley
November26,2017Pleasecheckwebsiteforlatestdraft.
Abstract:
TheSupplementalNutritionAssistanceProgram(SNAP,formerlyfoodstamps)isoneofthemostimportantelementsofthesocialsafetynet.Unlikemostothersafetynetprograms,SNAPvarieslittleacrossstatesandovertime,whichcreateschallengesforquasi-experimentalevaluation.Notably,SNAPbenefitsarefixedacross48states;butlocalfoodpricesvary,leadingtogeographicvariationintherealvalueofSNAPbenefits.Inthisstudy,weprovidethefirstestimatesthatleveragevariationintherealvalueofSNAPbenefitsacrossmarketstoexamineeffectsofSNAPonchildhealth.WelinkpaneldataonregionalfoodpricestoNationalHealthInterviewSurveydataanduseafixedeffectsframeworktoestimatetherelationshipbetweenlocalpurchasingpowerofSNAPandchildren’shealthandhealthcareutilization.WefindthatchildreninmarketregionswithlowerSNAPpurchasingpowerutilizelesspreventivehealthcare.LowerrealSNAPbenefitsalsoleadtoanincreaseinschoolabsences.Wefindnoeffectonreportedhealthstatus.
*ThisprojectwassupportedwithagrantfromtheUniversityofKentuckyCenterforPovertyResearchthroughfundingbytheU.S.DepartmentofAgriculture,EconomicResearchServiceandtheFoodandNutritionService,AgreementNumber58-5000-3-0066.Theopinionsandconclusionsexpressedhereinaresolelythoseoftheauthor(s)andshouldnotbeconstruedasrepresentingtheopinionsorpoliciesofthesponsoringagencies.WethankseminarparticipantsatNYUWagner,Lausanne,andtheUCLARDCConference.KristaRuffiniprovidedexcellentresearchassistance.

1
1. Introduction
TheSupplementalNutritionAssistanceProgram(SNAP,formerlytheFoodStampprogram)
isthelargestfoodassistanceprogramandoneofthelargestsafetynetprogramsintheUnited
States.1SNAPplaysacrucialroleinreducingpovertyforchildrenintheU.S.,withonlytheEITC
(combinedwiththeChildTaxCredit)raisingmorechildrenabovepoverty(RenwickandFox
2016).Eligibilityfortheprogramisuniversalinthatitdependsonlyonafamily’sincomeand
assets;in2015,1in7AmericansreceivedSNAPbenefits(Ziliak2015).
SNAP’sprimarygoalsaretoimprovefoodsecurityamonglow-incomehouseholds,reduce
hunger,andincreaseaccesstoahealthfuldiet.2Theextantliteraturedemonstratesthatthe
programsucceedsinreducingfoodinsecurityamongrecipienthouseholds(see,e.g.,Yenetal.
2008;NordandGolla2009;MykereziandMills2010;Ratcliffe,McKernan,andZhang2011;
ShaeferandGutierrez2011;Schmidt,Shore-Sheppard,andWatson2016andtherecentreview
byHoynesandSchanzenbach2016).Nonetheless,ratesoffoodinsecurityamongSNAP
householdsremainquitehigh,raisingthequestionofwhetherSNAPbenefitsareadequateto
meetthenutritionalneedsofrecipients(Coleman-Jensenetal.2012).Indeed,evidence
regardinghowSNAPbenefitsimpactrecipients’nutritionismoremixed(see,e.g.,Yen2010;
Gregoryetal.2013;Bronchetti,Christensen,andHansen2017b).
Ourstudyprovidesuniqueandhighlypolicy-relevantevidenceontheimpactofvariationin
thegenerosityofSNAPbenefitlevelsonchildhealth.Estimatingthecausalrelationship
betweenSNAPandhealthisdifficultbecauseSNAPbenefitsandeligibilityrulesarelegislatedat
1SNAPbenefitspaidin2016amountedtomorethan66billiondollars.Theprogramhasalsogrowndramaticallyintheyearssince1996welfarereform,withbenefitspaidoutalmosttriplinginrealtermsovertheyearsinthisstudy(1999-2010).2See,forexample,themostrecentlyamendedauthorizinglegislation,theFoodandNutritionActof2008,availableathttps://fns-prod.azureedge.net/sites/default/files/snap/Food-And-Nutrition-Act-2008.pdf.

2
thefederallevelanddonotvaryacrossstates,leavingfewopportunitiesforquasi-experimental
analysis.Onesetofquasi-experimentalstudiesanalyzestherolloutofthefoodstampprogram
acrosscountiesinthe1960sand1970sandfindsthatfoodstampsleadstosignificant
improvementsinbirthoutcomes(CurrieandMoretti2008;Almond,Hoynes,andSchanzenbach
2011)andaccesstofoodstampsinearlychildhoodleadstosignificantimprovementsinadult
health(Hoynes,Schanzenbach,andAlmond2016).Asecondsetofstudiesusesrecentstate
changesinapplicationprocedures(e.g.allowingonlineapplications,whetherthereisafinger
printingrequirement)asinstrumentsforSNAPparticipation(Schmeiser2012,GregoryandDeb
2015),3thoughthesestatepolicieshadrelativelysmalleffectsonparticipation(Ziliak2015).A
thirdapproachistakenbyEast(2016),whousesvariationineligibilityforSNAPgeneratedby
welfarereformlegislationinthe1990s,andfindsthatSNAPinearlychildhoodleadsto
improvementsinhealthstatusatages6-16.Noneofthesestudies,however,isabletoshed
lightonhowchangestolegislatedSNAPbenefitlevelsmightimpacthealthoutcomes.
OurapproachleveragesplausiblyexogenousgeographicvariationintherealvalueofSNAP
benefitstoidentifytheeffectsofvariationinSNAPgenerosityonhealthforasampleofchildren
inSNAPhouseholds.Importantly,theSNAPbenefitformulaisfixedacross48states(benefits
arehigherinAlaskaandHawaii)eventhoughthepriceoffoodvariessignificantlyacrossthe
country(Toddetal.2010;Todd,Leibtag,andPenberthy2011).4AcrossthecontinentalU.S.,
maximumbenefitsvaryonlywithfamilysize.So,in2016afamilyofthreewouldbeeligiblefor
amaximumbenefitof$511/monthregardlessofthelocalcostofliving.ThoughSNAPbenefits
3GregoryandDeb(2015)usetheMedicalExpenditurePanelSurveyandstatepolicyvariablesandfindthatSNAPparticipantshavefewersickdaysandfewerdoctor’svisits,butmorecheckupvisits.4StudyingdatafromtheQuarterlyFoodatHomePriceDatabase(QFAHPD),theauthorsfindthatregionalfoodpricesvaryfrom70to90percentofthenationalaverageatthelowendto120to140percentatthehighend.

3
areimplicitlyadjustedforvariationinthecostoflivingthroughalloweddeductions(e.g.,for
housing,andchildcare)inthecalculationofnetincome,thelimitedavailableevidence
indicatestheseadjustmentsarenotsufficienttoequalizerealbenefits,particularlyinhighcost
areas(Breenetal.2011).Gundersenetal.(2011)andtheInstituteofMedicine(2013)propose
thisasanareaforfutureresearch.
Higherareafoodprices,andconsequentlylowerSNAPpurchasingpower,mayimpact
children’shealthbyreducingnutritionifhouseholdsrespondbypurchasingandconsuming
lowerquantitiesoffood,oriftheypurchaselessexpensivefoodsoflowernutritionalquality.
ButlowerSNAPpurchasingpowermayalsoimpacthealthindirectly,withhigherfoodprices
causinghouseholdstoreduceconsumptionofotherinputsintothehealthproductionfunction,
likehealthcare.
Linkingnationallyrepresentativedatafromthe1999-2010NationalHealthInterview
Surveys(NHIS)toinformationonregionalfoodpricesfromtheQuarterlyFood-at-homePrice
Database(QFAHPD),westudytheeffectofvariationinrealSNAPbenefits(or“SNAPpurchasing
power”)onchildren’shealthcareutilizationandhealth.Ourmeasureofregionalfoodpricesis
thecostoftheThriftyFoodPlan(TFP),anutritionplanconstructedbytheUSDAtorepresenta
nutritiousdietatminimalcostandthebasisformaximumlegislatedSNAPbenefits(i.e.,
maximumbenefitsaresettotheTFPnationalaveragecost).TheQFAHPDincludesinformation
onfoodpricesthatallowsustoconstructanestimatedTFPpriceforeachof30designated
“marketgroup”geographicareaacrosstheU.S.Werelatevariouschildhealthoutcomestothe
realvalueofSNAPbenefits(i.e.,theratioofthenationalSNAPmaximumbenefittothemarket
group-levelTFPpricefacedbyahousehold)inafixedeffectsframeworkthatcontrolsfora

4
numberofindividual-levelandregioncharacteristics(includingnon-foodpricesinthearea)and
statepolicyvariables.Identificationcomesfromdifferencesacrossthe30marketareasin
trendsinthepriceoftheTFP.
OurstudycontributestothegrowingbodyofevidenceontheSNAPprogramanditseffects
inafewkeyways.First,weprovidenewevidenceontherelationshipbetweenSNAPbenefit
generosityandthehealthandwellbeingoftheSNAPpopulation.Ourfindingsconsistently
indicatethatchildreninmarketregionswithhigherfoodprices(lowerpurchasingpowerof
SNAP)utilizelesspreventive/ambulatoryhealthcare.Wefindthata10percentincreasein
SNAPpurchasingpowerraisesthelikelihoodachildhasanannualcheckupby6.3percentage
points(8.1percent)andthelikelihoodofanydoctor’svisitby3.1percentagepoints(3.4
percent).WhilelowerrealSNAPbenefitsdonotresultinsignificantdeclinesinreportedhealth
status,wedocumentsignificantdetrimentalimpactsonsomehealthindicators,likethe
numberofschooldaysmissedduetoillness,aswellasonchildren’sfoodsecurity.Summary
indicescontributeadditionalevidencetotheexistenceofeffectsonhealthcareutilization,but
nothealthoutcomesgenerally.Weconfirmthattheseeffectsarenotdrivenbyrelationships
betweengeographicvariationinfoodpricesandSNAPparticipationorhealthinsurance
coverage,noraretheypresentinaplacebosampleofsomewhathigher-incomechildren.
Asecondcontributionismethodological,inthatourapproachhighlightsanew
identificationstrategyforestimatingeffectsofproposedchangesinSNAPgenerosityonother
outcomesofinterest.Toourknowledge,oursisthefirststudytoutilizevariationinthereal
valueofSNAP(duetogeographicalvariationinfoodprices)asasourceofidentification.This
variationcouldbeleveragedtoexamineSNAP’simpactsonnutrition,foodconsumptionand

5
otherspendingpatterns,birthoutcomes,andadulthealth.5Whilethispaperusesdataon
regionalfoodpricesfromtheQFAHPD,othersourcesoffoodpricedatamightalsoprove
fruitfulforresearchersinterestedinthesequestions.AnexampleistheUSDA’sNational
HouseholdFoodAcquisitionandPurchaseSurvey(FoodAPS),arelativelynew,nationally
representativesurveythatgatheredinformationonhouseholds’foodacquisitionandtheirlocal
shoppingenvironments.
Morebroadly,ourfindingspointtosizeable,beneficialimpactsofSNAP(andofincreasing
thegenerosityofSNAPbenefits)forchildren’shealthcareutilization,foodsecurity,andsome
measuresoftheirhealth,benefitswhichshouldbeweighedcarefullyagainstthecostsavingsof
anyproposedcutstotheSNAPprogram.Theseresultsalsoshedlightontheexpectedimpact
ofadjustingbenefitlevelstoaccountforgeographicvariationinfoodpricesacrossmarket
regions.Suchadjustmentswouldlikelyreducedisparitiesinpreventive/ambulatorycare,school
absenteeism,andfoodsecurityamonglow-incomechildren,butmaynotleadtoimmediate,
contemporaneousimprovementsinotherhealthoutcomes.
Thepaperproceedsasfollows.Thenextsectiondescribesourmultiplesourcesofdataon
regionalfoodprices,childhealth,foodsecurity,andSNAPparticipation,andSection3laysout
ourempiricalapproach.Section4presentsourmainresultsregardingtheimpactofSNAP
purchasingpoweronchildren’shealthcareutilizationandhealth,Section5explores
mechanismsandseveralrobustnesschecks,andSection6concludes.
2.Data5Bronchetti,Christensen,andHansen(2017b)linkFoodAPSdataonSNAPrecipients’dietstolocaldataonthecostoftheTFPtostudytheeffectsofvariationinSNAPpurchasingpoweronnutritionamongtheSNAPpopulation.

6
Inthisstudy,wecombinethreesetsofdatatoestimatetheeffectofSNAPonchildren’s
health.BelowwedescribethedataonthepriceoftheTFP,theNationalHealthInterview
Survey,andthestateandcountycontrolvariables.Additionally,wesupplementourmain
analysiswithadministrativedataonSNAPcaseloadsandhousehold-leveldataonfood
insecurityfromtheDecemberCurrentPopulationSurvey(CPS).
2.1RegionalCostoftheThriftyFoodPlan(TFP)
TheThriftyFoodPlan(TFP)isafoodplanconstructedbytheUSDA,specifyingfoodsand
amountsoffoodsthatrepresentanutritiousdietataminimalcost.TheTFPisusedasthebasis
forlegislatedmaximumSNAPbenefitlevels.In2016,theU.S.averageweeklyTFPcostwas
$146.90forafamilyoffourwithtwoadultsandtwochildren(ages6-8and9-11).6
ToassignfoodpricestooursampleofhouseholdsintheNHIS,weconstructdataonthe
regionalpriceoftheTFPusingtheQuarterlyFood-at-HomePriceDatabase(QFAHPD)(Toddet
al.2010)fortheyearsfrom1999through2010.TheQFAHPD,createdbytheUSDA’sEconomic
ResearchService,usesNielsenscannerdatatocomputequarterlyestimatesofthepriceof52
foodcategories(e.g.threecategoriesoffruit:freshorfrozenfruit,cannedfruit,fruitjuices;
ninecategoriesofvegetables,etc.)for35regionalmarketgroups.The35marketgroups
coveredintheQFAHPDinclude26metropolitanareasand9nonmetropolitanareas,thoughfor
1999-2001only4nonmetropolitanareasarecaptured.7Eachmarketareaconsistsofa
6Seehttps://www.cnpp.usda.gov/sites/default/files/CostofFoodNov2016.pdf.(Accessed1/28/17)7In1999-2001,theQFAHPDidentifiedonenonmetropolitanareaforeachofthe4censusregions(east,central,southandwest).In2002andlater,theyexpandedtoincludenonmetropolitanareasineachofthe9censusdivisions:NewEngland,MiddleAtlantic,EastNorthCentral,WestNorthCentral,SouthAtlantic,EastSouthCentral,WestSouthCentral,MountainandPacific.Forcomparabilityweusethefournonmetropolitanareasthroughout.

7
combinationofcounties.Wemapthe52QFAHPDfoodcategoriestothe29TFPfoodcategories
tocreateasinglepriceestimatefortheTFPforeachmarketareaandyearduringthefull1999-
2010periodcoveredbytheQFAHPD,followingthemethodsinGregoryandColeman-Jensen
(2013).8,9
TomaptheQFAHPDfoodgrouppricestotheTFPfoodgrouppricesinthemarketbasket,
weuseanexpenditure-weightedaverageofthepricesfortheQFAHPDfoods,wherethe
weightsaretheexpendituresharesfortheQFAHPDfoodswithineachTFPcategory(mostTFP
foodcategoriesconsistofmultipleQFAHPDfoodgroups).Weconstructnationalexpenditure
sharesbyaveragingthesharesacrossallmarketgroups.Toavoidconfoundingregional
variationinfoodpriceswithregionalvariationinconsumptionofdifferentfoodcategories,we
applythesenationalexpendituresharestoeachmarketarea’spriceswhenconstructingthe
marketgroup-levelcostoftheTFP.10,11Weusethe2006specificationoftheTFP,which
featuresfoodcategoriesthatarerelativelycloselyalignedwiththefoodcategoriesinthe
QFAHPDdata(Carlsonetal.2007).
8Wecomeveryclosetoreproducingtheirestimates.Asinthisearlierwork,wecancleanlylinktheQFAHPDcategoriesto23ofthe29TFPcategorieswithoutduplicationoroverlapofQFAHPDprices.TheremainingsixTFPcategoriescontainfoodsthatareaccountedforinotherpartsoftheQFAHPDTFPbasket.FordetailsontheconstructionoftheTFPitself,seeCarlsonetal.(2007).9TherearetwoversionsoftheQFAHPD:QFAHPD-1,whichprovidespricedataon52foodgroupsfor1999-2006,andQFAHPD-2,whichincludespricesfor54foodgroupsfor2004-2010.WebridgethetwoseriesbyestimatingtheaverageratioofQFAHPD-1toQFAHPD-2foryears2004through2006foreachmarketgroup.Wethendividethepricedatafor1999-2003(i.e.theyearswithinformationononly52foodgroups)bythisratiotoputeverythinginconsistentunits.10WehavealsoconstructedmeasuresofTFPcostusingtotalnationalexpenditureshares(asopposedtoaveragingtheweightsacrossmarketgroups)andobtainverysimilarestimatesoftheTFPandeffectsizes.11Anexample(borrowedfromGregoryandColeman-Jensen(2013))isillustrative.TheTFPfoodcategory“wholefruit”consistsoftwoQFAHPDfoodgroups:“fresh/frozenfruit”and“cannedfruit.”InHartford(marketgroup1)inthefirstquarterof2002,expendituresonfresh/frozenfruitwere$35.7million,andexpendituresoncannedfruitwere$5.8million.Thisyieldsexpenditureweightsforwholefruit(inHartfordinquarter12002)of0.86and0.13,respectively.Wethenaveragetheseexpendituresharesacrossallmarketgroupstogeneratethenationalexpenditureshares(foreachitemandperiod).In2002,thesenationalexpenditureweightsare0.84and0.16forfreshfruitandcannedfruit,respectively.Weapplythesesharestothefirst-quarter2002pricesoffresh/frozenandcannedfruitintheHartfordmarketgroup($0.218and$0.244per100grams,respectively)tocomputeapriceforwholefruitinHartfordforthefirstquarterof2002(0.84×$0.218+0.16×$0.244=$0.222per100grams).

8
WeassigneachhouseholdintheNHIStoamarketgroup-levelTFPpricebasedonthe
countyofresidenceandtheyearofinterview.Whenestimatingtherelationshipbetweenthe
realvalueofSNAPbenefitsandhealth,wemeasurethepurchasingpowerofSNAPusingthe
ratioofthemaximumSNAPbenefittotheTFPpricefacedbythehousehold.Ourmain
regressionmodelsusethenaturallogofthisratioasthekeyindependentvariableforeaseof
interpretation;however,resultsarequalitativelyverysimilarwhentheleveloftheratiois
employedinstead.12
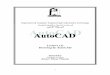
Figure1illustratesthevariationacrossregionsandovertimeintherealvalueofSNAP,
equaltothemaximumSNAPbenefitforafamilyof4dividedbytheregionalcostoftheTFP.13
PanelAdisplaysthevalueofthisratioin1999,PanelBshowsitsvaluein2008,andPanelC
showsitsvaluein2010.Ineachcase,adarkershadingrepresentsahigherSNAP/TFPratio,or
greaterSNAPpurchasingpower.ThemapsindicatethattherealvalueofSNAPislowerinthe
westandnortheast(astendstogenerallybethecase),butalsothattherearenoticeable
changesinSNAPpurchasingpowerwithinregionsoverthistimeperiod.Thechangesin2010
reflect,inpart,theincreaseinSNAPbenefitsaspartofthestimuluspackage(ARRA);thisraised
themaximumSNAPbenefitsinthesecondhalfof2009andthroughout2010.AppendixFigure
1ashowsthetrendsintherealTFPcostforeachofthemarketgroupareas.Thefigure
demonstratesthegeneralpatternofrisingTFPpricesin2005-2009followedbyadeclinein
2010.AppendixFigure1bshowsSNAPpurchasingpowerforthemarketgroupareas;this
illustratesthevariationintrendsacrossareasandshowsclearlytheeffectoftheARRA.
12Theseresultsareavailableuponrequest.13Aninteractiveversionofthisfigureisavailableonlineathttp://garretchristensen.shinyapps.io/Food_Price_Maps.

9
2.2NationalHealthInterviewSurvey(NHIS)DataonSNAPChildren
Weuserestricted-accessmicrodatafromtheNationalHealthInterviewSurvey(NHIS)for
theyears1999-2010toexamineeffectsonchildhealthandhealthcareutilization.14TheNHIS
surveysapproximately35,000householdsperyear.Bygainingrestricted-useaccesstothisdata
wecanobservethecountyofresidenceforeachhouseholdinthesurvey.Thisallowsustolink
respondentstoregionalareafoodpricesandaccessdetailedinformationonchildren’shealth
andthecharacteristicsoftheirparentsandhouseholdsforalargeandrepresentativenational
sample.Fromeachhouseholdwithchildren,thesurveyselectsonechildatrandom(the
“samplechild”)andcollectsmoreextensiveanddetailedinformationonthischild’shealthand
healthcareutilization.SeveraloftheoutcomeswestudyareonlyavailableintheseSample
Childfiles,whileothers(e.g.,parent-reportedhealthstatus)areavailableforallNHIS
respondentsinthePerson-levelfile.
Ourprimarysampleincludeschildrenages17andunderwhoarecitizensoftheUnited
States.Weimposethecitizenshiprestrictionbecausethepost-welfarereformerawitnessed
dramaticchangestorulesregardingnon-citizens’eligibilityformanysocialsafetynetprograms,
includingSNAP.15Weconductourmainanalysesonthesampleofchildreninhouseholdswho
reporthavingreceivedSNAPbenefitsinatleastoneofthepast12months.Fortheyearsfrom
1999through2010,thereare44,627suchchildren;18,299ofthemarealsointerviewedas
SampleChildren.WhiletheadvantageoflimitingouranalysistotheSNAPrecipientsisclear
(thisisthegroupmostaffectedbySNAP),non-randomselectionintoSNAPparticipationwould
14StateandcountyidentifiersaremaskedinthepublicuseNHISdata.ResearchersinterestedinaccessingtherestrictedgeocodedatashouldcontactPeterMeyeratrdca@cdc.gov.15Wetesttherobustnessofourresultstotheinclusionofnon-citizenchildren;theseresultsareverysimilartoourmainresults.SeeAppendixTables1–2.

10
callintoquestionacausalinterpretationofourestimates.InSection4.1,weanalyzethe
impactofSNAPpurchasingpoweronSNAPparticipationatthecountylevelanddocumentno
significantrelationshipbetweentherealvalueofSNAPbenefitsandtheper-capitaSNAP
caseload.AsarobustnesscheckinSection5,wealsotestthesensitivityofourresultsusingan
alternativesamplewithahighlikelihoodofbeingonSNAP—childrenlivingwithlow-educated,
unmarriedparent(s).
Familieswithlimitedresourcesmayrespondtohigherfoodpricesbyreducingconsumption
ofothergoodsthatimpacthealth,likeambulatoryorpreventivehealthcare.Ourprimary
measuresofhealthcareutilizationareindicatorsforwhetherthechildhashadacheck-upin
thepast12monthsandwhetherthechildhashadanydoctor’svisitinthepast12months.
AccordingtoguidelinesfromtheAmericanAcademyofPediatrics(AAP),childrenshouldhave
6-7preventivevisitsbeforeage1,3visitsperyearas1-yearolds,2visitsas2-yearolds,andat
leastonevisitperyearforages3through17.WealsoanalyzetherelationshipbetweenSNAP
purchasingpowerandwhether(theparentreportsthat)achildhasdelayedorforgonecare
duetocostinthepast12months.Finally,westudywhetherthechildhasvisitedtheERinthe
pastyear;iflowerSNAPpurchasingpowerreducestheuseofpreventive/ambulatorycare,we
mightexpecthigherareafoodpricestoincreaseutilizationofERcare.
WealsoanalyzetheeffectsofSNAPpurchasingpoweronseveraldirectmeasuresofchild
healththatmightrespondtoreducednutrition,ortoreducedconsumptionofotherinputsin
thehealthproductionfunction(e.g.,healthcare).Parentalrespondentsreportthechild’s
healthstatusona5-pointscale(1—excellent,2—verygood,3—good,4—fair,and5—poor);we
usethismeasuretoconstructanindicatorforwhetherthechildisinexcellentorverygood

11
health.Asmeasuresofcontemporaneoushealth,wealsostudywhetherthechildwas
hospitalizedoverthepast12months,thenumberofschooldaysmissedduetoillnessinthe
past12months(forthesub-sampleofschoolagedchildren),andanindicatorforwhetherthe
childmissed5ormoredaysofschoolduetoillness.Inaddition,weestimatetherelationship
betweenSNAPpurchasingpowerandtwolonger-termhealthoutcomesthatmayrespondto
reducednutritionortofoodinsecurity:anindicatorforobesitybasedonheightandweight
data(forthesubsampleofchildrenages12-17),andwhetherthechildhasemotionalproblems
(definedfortheuniverseofchildrenages4andolder).
Wealsotestbothofthesegroupsofoutcomes(preventativehealthcareutilization,health
outcomes)usingsummaryindexmethodsasinKling,Liebman,andKatz(2007).16
Table1displayssummarystatisticsforSNAPrecipientchildrenandfortheentirepopulation
ofchildren.Asexpected,SNAPchildrenarelikelytobepoor,liveinsingle-parenthouseholds
(onlyathirdlivewithbothparents),andaredisproportionatelylikelytobeblackorHispanic.
Becausesuchahighfraction(72percent)ofSNAPchildrenreceiveMedicaid,therateof
uninsuranceamongthissampleislow,atabout7percent.Healthcareutilizationandhealth
outcomesaresomewhatsimilarforSNAPcitizenchildrencomparedtothegeneralpopulation
ofchildrenintheU.S.Nearlyone-quarterofSNAPchildrenwentwithoutacheck-upinthepast
year,but90percenthadatleastsomesortofdoctor’svisitduringthattime,andmorethan5
percentreporthavingdelayedorgonewithoutcareduetoitscost.However,ERutilizationis
high,atover30percent,comparedto21percentamongtheentirepopulation.Intermsof
16Wecreatesummaryindicesbysubtractingthemeananddividingbythestandarddeviationofeachvariable,thensummingacrossvariableswithinanoutcomefamily.Typically,themeanandstandarddeviationofacontrolgroupareused,butlackingthat,weusethefullsample.Notethatthesampleintheseregressionsislimitedtothosewithfulldatafromallincludedmeasures.Forthehealthoutcomesindexthisimpliesschoolagechildrenonly.Anderson(2008)explainssimilarindicesclearly,andHoynes,Schanzenbach,andAlmond(2016)usethetechniquewhenevaluatinglong-runimpactsofSNAP.

12
healthitself,SNAPchildrenhavesimilarhealthstatus,butmissmoreschooldays(5,on
average,butone-thirdofSNAPchildrenmissed5ormoreinthepastyear),andmore
commonlyhaveemotionalproblems(46percentofSNAPchildren4oroldercomparedto27
percentinthegeneralpopulation).
2.3StateandCountyControlVariables
Weincludeseveralvariablestocontrolforregionalpoliciesandpricesthatmightaffect
childhealthandbecorrelatedwithlocalfoodprices.First,wecontrolforlocallabormarket
conditionswiththecountyunemploymentrate.Second,weincludeasummaryindexofstate-
levelSNAPpoliciesdevelopedbyGanongandLiebman(2015),whichincorporatesmeasuresfor
simplifiedreporting,recertificationlengths,interviewformat(e.g.inpersonornot),call
centers,onlineapplications,SupplementalSecurityIncomeCombinedApplicationProject,
vehicleexemptionsforassetrequirement,andbroad-basedcategoricaleligibility.Third,we
controlforotherstatepoliciesincludingtheminimumwage,stateEITC,TANFmaximumbenefit
guaranteeamounts,andMedicaid/StateChildren’sHealthInsuranceProgram(CHIP)income
eligibilitylimits.Finally,andperhapsmostimportantly,wecontrolforpricesofothergoodsby
includingHUD’sfairmarketrent(measuredbycountyasthe“40thpercentileofgrossrentsfor
typical,non-substandardrentalunitsoccupiedbyrecentmoversinalocalhousingmarket”17)
andregionalConsumerPriceIndices(CPIs)fornon-food,non-housingcategories(apparel,
commodities,education,medical,recreation,services,transportationandothergoodsand
services).Theseareavailablefor26metroareas;fortheremainingareas,theCPIiscalculated
17Morespecifically,HUDestimatesFMRsfor530metropolitanareasand2,045nonmetropolitancountyFMRareas.

13
withineachofthefourcensusregionsandforfourcountypopulationsizes(<50,000,50,000-
1.5million,>1.5million).
2.4SupplementalDataonSNAPCaseloadsandFoodInsecurity
WeinvestigatetherelationshipbetweenSNAPpurchasingpowerandSNAPparticipationin
Section4.1,usingadministrativedataoncounty-levelSNAPcaseloadsfromtheU.S.
DepartmentofAgriculture(USDA),fortheyearsfrom1999through2010.Wematcheach
county-yearobservationtothatyear’sTFPpriceforthemarketgrouptowhichthecounty
belongs.
Tofurtherprobemechanismswherebyvariationinregionalfoodpricesmayimpactchild
health,wesupplementourmainanalysisbystudyingtherelationshipbetweenSNAP
purchasingpowerandfoodinsecurity.18ForthisanalysisweusedatafromtheDecember
CurrentPopulationSurveyFoodSecuritySupplement(CPS-FSS)fortheyearsfrom2001-2010.19
Weidentifyasampleof37,277citizenchildren,ages0to17,wholiveinhouseholdsthatreport
receivingSNAP,andlinkthemtomarketareaTFPpricesaccordingtolocationofresidence.20
18Foodinsecurityisahousehold-levelmeasureofwell-being,definedasbeingunabletoobtain,oruncertainofobtaining,anadequatequantityandqualityoffoodduetomoneyorresources.Very-lowfoodinsecurityisdefinedasfoodinsecuritythatincludesdisruptedorrestricteddietarypatterns.Priorto2006,very-lowfoodinsecuritywaslabeled“foodinsecuritywithhunger”.19TheDecemberfoodsecuritysupplementwasnotcollectedin1999and2000.20Thepublic-usefoodsecuritysupplementfilesreportsgeographicinformationonallstates,217counties,69primarymetropolitanstatisticalareas,173metropolitanstatisticalareas(MSA),40combinedstatisticalareas(CSA),and278core-basedstatisticalareas(CBSA)duringourperiodofanalysis.InordertoassignCPSobservationstoamarketgroup,wefirstidentifystatesthatincludeasinglemarketgroupandassignallobservationsinthatstatetothecorrespondingmarketgroup.Continuingwiththenextmostgeneralgeography(CSA),werepeatthisprocessatincreasinglymoredetailedgeographieslevelstothecountyidentifiers.Afterthisstep,wethenassignobservationslivinginanon-metropolitanareatotheruralmarketgroupbasedontheirstateofresidence(forstateswithruralareasinasinglemarketgroup).Wematch83.7percentofCPSobservationstoamarketgroupusingthisiterativeprocess.

14
3.EmpiricalMethods
WeestimatethecausalimpactofvariationintherealvalueofSNAPbenefitsonmeasures
ofchildhealthandhealthcareutilizationforchildreninhouseholdswhoreportreceivingSNAP
benefitsduringthepast12months.Throughout,ourregressionstakethefollowingform:
(1) 𝑦"#$ = 𝛼 + 𝛽 ln +,-./-0123.41
+ 𝑋"#$𝜃 + 𝑍#$𝛾 + 𝛿$ + 𝜆# + 𝜀"#$
where𝑦"#$isthehealthoutcomeofindividualiwhoresidesinregionrintimet.Thekey
independentvariableisthenaturallogoftheratioofmaximumSNAPbenefitsforafamilyof
four(whichvarybyyear,butisconstantacrossregions)totheregionalTFPprice.ThevectorXirt
containsasetofcontrolsforthechild’scharacteristics,includinghis/herage(anditssquare),
race,Hispanicethnicity,familysize,indicatorsforthepresenceofthemother(and/orfather)in
thehousehold,andinteractionsbetweenindicatorsforthemother's(father's)presenceand
themother's(father's)education,maritalstatus,age,andcitizenship.Thestatepolicyvariables
describedinSection2.3areincludedinZrt,asareasetofregionalCPIsinnon-food,non-
housingconsumptioncategories.Allmodelsalsoincludeafullsetoffixedeffectsfortheyear
(δt)andmarketgroup(lr).Thestandarderrorsareclusteredatthemarketgrouplevel.
Wehavealsotestedmodelswithadditionalcontrolsincludingincome,parent-reported
healthstatus,andanindicatorforinsurancecoverage,butduetoendogeneityconcerns,wedo
notincludetheseinourmainspecification.Theresultsaregenerallysimilar,however,andwe
reporttheseestimatesinthesupplementaryappendix(AppendixTables3and4).
IdentificationinthismodelcomesfromvariationintrendsinthepriceoftheThriftyFood
Planacrossmarketareas.AsweshowedearlierinFigure1,thereissubstantialvariationacross
geographicareasinthepurchasingpowerofSNAPbenefits.Inlower-costareastheSNAP

15
benefitcoversupto80percentofthecostoftheTFP,whileinhighercostareasthisfallstoless
than65percent.21Moreimportantlyforouridentificationstrategy,theseregionaldifferences
changeovertime,withsomeareasexperiencinglargerincreasesinSNAPpurchasingpower
from1999to2010,andothersexperiencingsmallerincreases(e.g.,purchasingpowerinsome
southernmetropolitanareasincreasednearly17percent,butonlyabout4.5percentinurban
NewYork).22
4.Results
4.1SNAPParticipation
WebeginbyanalyzingtheeffectsofSNAPpurchasingpowerontheSNAPcaseload.If
variationintherealvalueofSNAPleadstochangesinSNAPparticipation,thenselectionmay
biasourestimatesoftheeffectofSNAPpurchasingpoweronchildhealth.
UsingdatafromUSDA,weconstructacountypanelforannualSNAPcaseloadscovering
1999-2010.Weestimateequation(1)wherethedependentvariableisSNAPcaseloadsdivided
bycountypopulation.Table2displaystheresultsofsixdifferentspecificationsofthemodel.
Eachincludesyearandmarketgroupfixedeffects,aswellasthenaturallogoftheratioof
maximumSNAPbenefitstothemarketgroupTFPprice.Inthesecondcolumnweaddacontrol
forthecountyunemploymentrate,whichisasignificantdeterminantofSNAPcaseloads(Bitler
21NotethatsincethestatutoryTFPisconstructedusinganationalaverage,someareasare,bydefinition,likelytohaveSNAPbenefitsthatmorethancoverthecostoftheTFP.However,ourconstructionofmarketgroupTFPisunlikelytobeexactlyidenticaltothestatutorydefinition.Forouridentificationstrategytobevalidhowever,allthatmattersistherelativegenerosityacrossmarketgroupsandtrendsacrossmarketgroups.22SNAPbenefitsin2010and6monthsof2009includeincreasedbenefitsprovidedthroughtheAmericanRecoveryandReinvestmentAct(ARRA).ARRAbenefitsamountedto$62,orabouta13.6percentincreaseabovethebase2009levels.ChangesinSNAPpurchasingpowerrangedfromadecreaseof5.8percentinSanFranciscoto4.3percentincreaseinmetropolitanareasinArkansasandOklahomaoverthe1999-2008period.

16
andHoynes2016)andpossiblycorrelatedwithregionalprices.Incolumn3weaddcontrolsfor
statepolicyvariables,includingforSNAP,EITC,minimumwages,TANFgenerosity,and
Medicaid.Incolumn4weaddcontrolsforregionalprices,includingthecountyHUDfairmarket
rentandregionalCPIsforgoodsotherthanfood.
Whenonlyyearandmarketgroupfixedeffectsareincluded,theestimatedcoefficienton
SNAPpurchasingpowerispositiveandsignificant,consistentwiththeSNAPcaseloadpercapita
risingwhentheTFPdecreases(andtherealvalueofSNAPincreases).However,onceany
additionalcontrolsareadded(e.g.,evenjustthecountyunemploymentrate,incolumn2),the
coefficientdropssubstantiallyinmagnitudeandisnolongerstatisticallydifferentfromzero.
Theadditionofthestatepolicycontrols(column3)andtheregionalprices(column4)resultin
anestimatethatisevensmallerinmagnitude.Incolumns5,weextendthespecificationby
includingamarketgrouplineartimetrendwhichleadstolittlechangeintheestimated
coefficientonSNAPpurchasingpower.Fromthisweconcludethatthereisnosignificant
relationshipbetweentherealvalueofSNAPandSNAPcaseloads,andthusweinterpretour
mainresultsfreeofconcernsaboutselection.
4.2SNAPPurchasingPowerandHealthCareUtilization
Theprimarygoalofourstudyistoanalyzetheimpactsofvariationinthepurchasingpower
ofSNAPbenefitsonoutcomesrelatedtochildhealth.Webeginbyexaminingevidencefor
measuresofhealthcareutilization,recognizingthatfamiliesfacinghigherfoodpricesmay
respondtothelowerrealvalueoftheirSNAPbenefitsbyreducingout-of-pocketspendingon
othergoods,includinghealthcare.

17
WepresenttheresultsofthisanalysisinTable3.Ourprimarymeasureofhealthcare
utilizationisanindicatorforwhetherthechildhashadacheck-upinthepast12months
(column1),whichisobservedonlyforchildrenintheSampleChildfile.Wealsoexamine
indicatorsforwhetherthechildhashadanydoctor’svisitinthepast12months(column2),
whetherthechildhasdelayedorgonewithoutcareinthepast12monthsduetocost(column
3),andwhetherachildhasvisitedanERinthepast12months(column4).Whetherachildhas
delayedorforgonecareisreportedinthePersonfileoftheNHISsoisobservedforallNHIS
childrenunderage18;wereportthisestimateincolumn5.Themodelincludesfixedeffectsfor
marketgroup,year,individualcontrols,andregionalcontrolsforunemploymentrate,non-food
prices,andstatesafetynetpolicies(similartocolumn4ofTable2).23Thekeyindependent
variable,representingtherealvalueofSNAP,isln(SNAPMAX/TFP).
AmongSNAP-recipientchildren,wefindthatincreasedpurchasingpowerofSNAP
significantlyraisesthelikelihoodachildhashadacheckupinthepast12months.Aten
percentincreaseintheratio(SNAPMAX/TFP)leadstoa6.3percentagepoint(or8.1percent)
increaseinthelikelihoodofacheckup.Wealsodocumentasmaller,butsignificantimpactof
increasedSNAPpurchasingpowerontheprobabilityachildhashadanydoctor’svisitoverthe
past12months.AtenpercentincreaseinthepurchasingpowerofSNAPlowersthelikelihood
ofdelaying/forgoingcareby3.1percentagepoints,or3.4percent.
Theresultsincolumns3through5indicatethatSNAPpurchasingpowerhasnostatistically
significanteffectonwhetherchildrenarereportedtohavedelayedorforgonecareduetocost
23Individual-levelcontrolsincludethechild'sage(anditssquare),whetherthechildisblackorHispanic,thechild'sfamilysize,indicatorsforthepresenceofthemother(and/orfather)inthehousehold,andinteractionsbetweenindicatorsforthemother's(father's)presenceandthemother's(father's)education,maritalstatus,age,andcitizenship.

18
(amongallchildrenorintheSampleChildsample),oronwhethertheyhavevisitedtheERin
thepast12months.However,thecoefficientsareallnegative,suggestingaprotectiveeffectof
SNAP.
Toaddressconcernsofmultiplehypothesistesting,weconductacollectivetestofthese
healthcareutilizationoutcomesbyconstructingsummaryindexestimatesasinKling,Liebman,
andKatz(2007).Wenormalizeandcombine(andchangesignswhennecessarysothatall
positiveoutcomesmeanmorepreventativecare)thevariablesforcheckups,anydoctorvisits,
delayseekinghealthcare,ERvisit,andnohealthinsurance(seebelowformoreonthis
outcome).ResultsareshowninAppendixTable6.Wefindthata10%increaseinSNAP
purchasingpowerleadstoastatisticallysignificant0.4standarddeviationincreaseinhealth
careutilization.Broadly,weinterprettheseresultsassuggestingthatchildreninhouseholds
facinghigherfoodprices(andthus,lowerSNAPpurchasingpower)receivelesspreventiveand
ambulatorycare.
4.3SNAPPurchasingPowerandHealthOutcomes
Table4presentsevidenceontheextenttowhichvariationinSNAPpurchasingpower
affectschildhealthoutcomes.Theregressionspecificationsincludethesamesetofcontrolsas
inTable3.Notethatseveraloftheoutcomesaredefinedonlyforsub-samplesofchildren,
leadingtodifferentnumbersofobservationsacrossthecolumnsofTable4.Specifically,
obesityismeasuredonlyforchildrenages12through17,24emotionalproblemsareidentified
24TheindicatorforobesityisbasedonBMIcalculations,whichareaffectedbysomeoutlyingheightandweightmeasurements.WetrimthetopandbottomoftheBMIdistributiontoexcludethetopandbottompercentile.Inaddition,

19
forchildrenages4andolder,andthenumberofschooldaysmissedisrecordedonlyfor
childrenage5andolderwhoareinschool.Parent-reportedhealthstatusandhospitalizationin
thepast12monthsarereportedforallchildren,buttheotherhealthoutcomesareonly
providedforchildrenintheSampleChildfile.
WefindnostatisticallysignificantrelationshipbetweenSNAPpurchasingpowerandan
indicatorforthechild’s(parent-reported)healthstatusbeingexcellentorverygood,northe
likelihoodofhavingbeenhospitalizedinthepastyear.However,wedocumentastrong
negativeandrobustrelationshipbetweentherealvalueofSNAPandthenumberofschool
dayschildrenmissedduetoillness.ForSNAPrecipientchildren,atenpercentincreaseinSNAP
purchasingpowerisassociatedwithadecreaseinmissedschooldaysofjustover1day(ora22
percentdecreaserelativetothemeanofapproximately5daysmissed).
WefindnostatisticallysignificanteffectsofrealSNAPbenefitsonobesitynorthe
propensitytohaveemotionalproblems,althoughwenotethatthesearelongertermhealth
problemsthatoftendevelopovertimeandmaybelesslikelytorespondcontemporaneouslyto
higherareafoodprices.Itispossiblethattheseoutcomeswouldbelikelytorespondonlyafter
alonger,cumulativeperiodoffoodinsecurity,poornutrition,orreducedhealthcare.
Weagaincreateanormalizedsummaryindexandtestoveralleffectsofhealthoutcomes
(healthstatus,hospitalization,andschooldaysmissed).Wefindpositivebutnotsignificant
estimatesforSNAPchildren;a10%increaseinSNAPpurchasingpowerleadstoa0.12standard
deviationincreaseofthehealthmeasure.Theestimateislargerandmarginallysignificantfor
lowereducationunmarriedhouseholds.Weinterprettheseresultsassuggestingthatvariation
heightandweightinformationwasonlycollectedforchildrenages12andolderinyears2008through2010.Wethereforelimitthesampletochildrenages12-17.

20
intherealvalueofSNAPmayhavesomemodestimpactsonchildren’scontemporaneous
health.Aweaknessofmeasuringhealthusingthenumberofschooldaysmissedduetoillness
isthatitmaydependontheparent’sevaluationofthechild’shealth;however,parent-reported
healthstatus,whichisalsoasubjectivemeasure,doesnotappeartorespondtovariationinthe
realvalueofSNAP.Ontheotherhand,thenumberofmissedschooldaysisperhapstheonly
healthoutcomeweanalyzethatmightbeexpectedtorespondcontemporaneouslytoreduced
nutritionorlimiteduseofpreventive/ambulatoryhealthcare.
5.MechanismsandRobustnessChecks
5.1SNAPPurchasingPowerandFoodInsecurity
Oneavenuethroughwhichhigherareafoodpricesmayimpactchildhealthisbyreducing
households’consumptionofpreventiveandambulatoryhealthcarefortheirchildren.The
resultsinSection4,whichpointtoasignificantreductioninyearlycheck-upsanddoctor’svisits
forthosewithlowerSNAPpurchasingpower,areconsistentwithsuchamechanism.
However,variationinSNAPpurchasingpowermayalsoaffecthealthmoredirectly,if
childrenfacinghigherareafoodpricesareabletoconsumeless(orlessnutritious)food.
BecausetheNHISdidnotprovideinformationonfoodsecurityornutritionalintakeintheyears
ofdataweanalyze,weturntodatafromtheDecemberfoodsecuritysupplementtotheCPSto
estimatetheimpactofSNAPpurchasingpoweronfoodinsecurityamongSNAP-recipient
children.
WedisplaytheseresultsinTable5.Theregressionspecificationsincludethesamesetof
controlsasinTables3and4.WefindthatahigherrealvalueofSNAPbenefitsisassociated

21
withanimprovementinchildren’sfoodsecurity:A10percentincreaseinSNAPpurchasing
powerreducesthelikelihoodachildisfoodinsecureby6.7percentagepoints(a21.8percent
decreaserelativetothemean).OurresultsarequalitativelyquitesimilartothoseinGregory
andColeman-Jensen(2013),whichusedfeweryearsofthesamedataandaslightlydifferent
estimationstrategy.
Theresultforverylowfoodsecurityisnotstatisticallysignificant;however,wenotethat
verylowfoodsecurityisafairlyrareoutcomeevenforSNAPchildren(only4percentofthe
childreninoursampleareveryfoodinsecurewhilealmost30percentarefoodinsecure).In
particular,verylowfoodsecurityrequiresnotonlythathouseholdsareuncertainofobtaining
anadequatequantityandqualityoffoodduetomoneyorresources,butthattheyalsorestrict
ordisruptfoodintakebecauseoflackofresources.Itisperhapsnotsurprising,then,thatthis
moreextremeoutcomeisnotsignificantlyresponsivetomarginalvariationinareafoodprices.
5.2SNAPPurchasingPowerandHealthInsuranceCoverage
InTable6weinvestigatewhetherthedocumentedimpactsofSNAPpurchasingpoweron
healthcareutilizationandhealthcouldbeexplainedbyarelationshipbetweenregionalfood
pricesandhealthinsurancecoverage.Sucharelationshipwouldbeunexpectedforthis
sample,giventhatSNAPrecipientchildrenarealllikelytobeincome-eligibleforMedicaidor
CHIP.ReturningtooursampleofNHISchildren,weestimateequation(1),wherethe
dependentvariableisnowanindicatorforwhetherthechildisuninsured.Reassuringly,for
bothchildrenintheSampleChildfileandallNHISchildren,wefindnostatisticallysignificant
effectofSNAPpurchasingpoweronthelikelihoodachildhasnohealthinsurance.

22
5.3RobustnessChecks
Anaturalcheckofourmainresultsistoestimateourmodelsforhealthcareutilizationand
healthoutcomesona“placebo”sampleofchildrenthatshouldnotbedirectlyaffectedby
SNAPpurchasingpower(i.e.,whoarenotimpactedbySNAPbenefitsandwhosehealthand
healthcareshouldnotbeasvulnerabletohigherareafoodprices).
InTable7wepresentregressionresultsanalogoustothoseinTables3and4,butfora
sampleofNHISchildrenlivinginhouseholdswithincomesbetween300and450percentofthe
federalpovertyline.25Estimatedcoefficientsforourkeyoutcomes(i.e.,hadcheck-up,hadany
doctor’svisit,andnumberofschooldaysmissed)aresmallandstatisticallyinsignificant.Thisis
trueformostotheroutcomes,aswell.Twoexceptionsarethatwefindastatisticallysignificant
effectofSNAPpurchasingpoweronwhetherachildinthisplacebosamplevisitedtheERinthe
pastyearandonwhetherachildisobese.Recallthatneitheroftheseoutcomeswasfoundto
respondsignificantlytoSNAPpurchasingpoweramongSNAPrecipientchildren.
Table8displaystheresultsofaseriesofrobustnesscheckstoourmainfindingsregarding
theimpactsofSNAPpurchasingpoweronhealthcareutilizationandhealth.InpanelA,were-
estimatethemodelsincludingaleadtermthatusesthet+1marketareaTFPprice.Thislead
specificationprovidesatestforthevalidityofourfixedeffectsdesign.Ifwefindsignificant
effectsoffutureprices(whilecontrollingforcurrentprices)wemightbeconcernedthatweare
capturingtheeffectsofsomeothertrendintheregions.Thatis,weestimate:
(2) 𝑦"#$ = 𝛼 + 𝛽< ln/-0+,-.123.41
+ 𝛽= ln/-0+,-.1>?23.4,1>?
𝑋"#$𝜃 + 𝑍#$𝛾 + 𝛿$ + 𝜆# + 𝜀"#$
25Asbefore,thissampleislimitedtochildrenages0through17whoarecitizensoftheUnitedStates.

23
In11ofthe13specifications,theleadofSNAPpurchasingpowerisinsignificant.
Additionally,ourresultsforthecontemporaneouseffectofSNAPpurchasingpowerarelargely
unchanged:Themagnitudesoftheestimatedcoefficientsfor“hadcheckup”and“schooldays
missed”arequitesimilartothoseinTables3and4.Oneexceptionisthattheestimatedimpact
ofcurrent-periodSNAPpurchasingpoweronwhetherachildhadanydoctor’svisitinthepast
12monthsisathirdaslargeandisnolongerstatisticallysignificant.
ThesecondpanelofTable8containsresultsfromamodelthatincludesasetofmarket
grouplineartimetrends.Thisapproachplacesseriousdemandsonthedatainthat
identificationnowmustcomefromdeparturesinmarketgroups’TFPpricesfromtheirtrends
(assumedtobelinear).Whilethemainestimatesforhealthcareutilization(hadcheckup,had
anydoctor’svisit)arequalitativelysimilartothoseinTable3,theyaresmallerinmagnitude
andnolongerstatisticallysignificant.TheestimatedimpactofSNAPpurchasingpoweron
missedschooldays,however,remainsnearlyidenticalinmagnitudeandsignificancetothatin
Table4.
Finally,toaddressconcernsthatinclusioninourSNAPrecipientsamplemaybeendogenous
toSNAPpurchasingpower,weestimatetheimpactsofvariationinSNAPpurchasingpoweron
healthcareutilizationandhealthforahighintent-to-treatpopulation.Inparticular,weidentify
asampleofchildrenlivingwithunmarriedparent(s)withlessthanacollegeeducation.26Again,
theestimatedimpactsonthelikelihoodofacheckupandonthenumberofmissedschooldays
arequitesimilarinmagnitudetothoseforourmainsample(althoughthep-valueonthe
coefficientformissedschooldaysrisesto0.141).TheestimatedrelationshipbetweenSNAP
26Eventhoughthisisahigh-ITTgroup,observablecharacteristicsshowthatitismoreadvantaged,onaverage,thantheSNAPpopulation.

24
purchasingpowerandhavinghadanydoctor’svisitissmallerandnolongerstatistically
significant.Interestingly,wedocumentanegativeeffectofincreasedSNAPpurchasingpower
onERutilizationforthissomewhathigher-incomesample:a10percentincreaseintheratio
(SNAPMAX/TFP)reducesthelikelihoodofanERvisitby4.8percentagepoints.
6.DiscussionandConclusion
InthispaperweprovidethefirstdirectevidenceonhowvariationintherealvalueofSNAP
benefitsaffectschildren’shealthcareutilizationandhealthoutcomes.Wefindevidence
consistentwithfamiliesadjustingtohigherareafoodprices(andthus,lowerSNAPpurchasing
power)byreducingutilizationofpreventive/ambulatorymedicalcare.Inparticular,we
documentthata10percentincreaseinSNAPpurchasingpowerincreasesthelikelihoodachild
hadacheck-upinthepastyearby8.1percentandincreasesthelikelihoodthatchildrenhad
anydoctor’svisitinthepast12monthsby3.4percent.
Wedonotfindmuchevidencethatthesehigherpricescausedetrimentalimpactsonhealth
status,thelikelihoodofahospitalization,orothermeasuresofphysical(e.g.,obesity)and
mentalhealth(e.g.,childhasemotionalproblems).Oneexceptionisthatchildrenfacinghigher
foodprices(andthus,lowerSNAPpurchasingpower)misssignificantlymoredaysofschooldue
toillness(22percentmore,relativetoabaselinemeanof5misseddays,whenSNAP
purchasingpowerisreducedby10percent).Wealsofindthatlowerpurchasingpowerof
SNAPbenefitsresultsinagreaterlikelihoodoffoodinsecurity.
Onepossibleexplanationforourfindingstrongereffectsonutilizationthanonhealthitself
isthatmostofthehealthmeasuresweconsideraremorechronicandcumulativeinnature

25
(e.g.,obesity).However,wealsofindnoevidenceofarelationshipbetweenSNAPpurchasing
powerandcaregiver-reportedhealthstatus,anoutcomewhichcouldbelesslikelytosuffer
fromthesameproblem.Asecondpossibleinterpretationofourfindingsisthatwhilelower
SNAPpurchasingpowercausesreducedhealthcareutilizationamongchildrenandnegatively
affectsfoodsecurity,neithertranslatesintosubstantialdetrimentalimpactsonchildren’s
healthstatus.
Wealsonotethatourmeasureofvariationinthepriceoffoodisconstructedusing30
marketregionsthatperhapsmaskvariationinurbanandruralcustomerswhoareinfactpaying
differentprices,thusmaskingwhycertainSNAPrecipientsareabletobuyrelatively
inexpensivefoodandstayrelativelyhealthy.Inrelatedwork,Bronchetti,Christensen,and
Hansen(2017a)usefoodpricesmeasuredatamuchfinerlevelfromtheFoodAcquisitionand
PurchaseSurvey(FoodAPS)anddemonstratethatthesizeofthegeographicradiususedto
measurewhetherSNAPbenefitsweresufficienttobuytheTFP(atastoreinsidetheradius)
matteredrelativelylittle.Whatmatteredfarmoreiswhetherrecipientswereabletoidentify
andtraveltoalowcoststoreinthearea.Still,weareoptimisticthatusingdatasetswithfiner
geographicvariationinfoodpricesmaybeafruitfulresearchareainthefuture.
Finally,ourresultsspeaktowhetheradjustingbenefitlevelstoaccountforgeographic
variationinfoodpricesacrossmarketregions(30nationally)wouldhelpimprovechildhealth
andwellbeing.Weconcludethatsuchadjustmentwouldreducedisparitiesinchildhealthcare
utilizationandschoolabsenteeisminlow-incomehouseholds,butmaynotleadtosignificant
improvementsincontemporaneoushealthstatus.

26

27
References
Almond, Douglas, Hilary W. Hoynes, and Diane Whitmore Schanzenbach. 2011. “Inside the War on Poverty: The Impact of Food Stamps on Birth Outcomes.” Review of Economics and Statistics 93 (2):387–403. https://doi.org/10.1162/REST_a_00089.
Anderson, Michael L. 2008. “Multiple Inference and Gender Differences in the Effects of Early Intervention: A Reevaluation of the Abecedarian, Perry Preschool, and Early Training Projects.” Journal of the American Statistical Association 103 (484):1481–95. https://doi.org/10.1198/016214508000000841.
Bitler, Marianne, and Hilary Hoynes. 2016. “The More Things Change, the More They Stay the Same? The Safety Net and Poverty in the Great Recession.” Journal of Labor Economics 34 (S1):S403–44. https://doi.org/10.1086/683096.
Breen, Amanda B., Rachel Cahill, Stephanie Ettinger de Cuba, John Cook, and Mariana Chilton. 2011. “Real Cost of a Healthy Diet: 2011.” Children’s Health Watch. http://www.childrenshealthwatch.org/publication/real-cost-of-a-healthy-diet-2011/.
Bronchetti, Erin, Garret Christensen, and Benjamin Hansen. 2017a. “Are SNAP Benefits Adequate for Purchasing a Healthy Diet? Evidence on Geographic Variation in Food Prices and the Purchasing Power of SNAP.” http://www.ocf.berkeley.edu/~garret.
———. 2017b. “USDA Food Assistance Programs and Healthy Food Choices: Quasi Experimental Evidence from Geographic Variation in Food Prices.” presented at the APPAM Fall Research Conference, Chicago, IL, November 3. https://github.com/garretchristensen/FoodAPSAPPAM2017.
Carlson, Andrea, Mark Lino, Wen Yen Juan, Kenneth Hanson, and P. Peter Basiotis. 2007. “Thrifty Food Plan, 2006.” CNPP-19. US Department of Agriculture, Center for Nutrition Policy and Promotion. http://www.cnpp.usda.gov/sites/default/files/usda_food_plans_cost_of_food/TFP2006Report.pdf.
Coleman-Jensen, Alisha, Mark Nord, Margaret Andrews, and Steven Carlson. 2012. “Household Food Security in the United States in 2011.” United States Department of Agriculture, Economic Research Service. https://www.ers.usda.gov/webdocs/publications/45020/30967_err141.pdf?v=41165.
Currie, Janet, and Enrico Moretti. 2008. “Short and Long-Run Effects of the Introduction of Food Stamps on Birth Outcomes in California.” In Making Americans Healthier: Social and Economic Policy as Health Policy. New York: Russel Sage.
East, Chloe N. 2016. “The Effect of Food Stamps on Children’s Health: Evidence from Immigrants’ Changing Eligibility.” University of Colorado Denver. http://cneast.weebly.com/uploads/8/9/9/7/8997263/east_jmp.pdf.
Ganong, Peter, and Jeffrey Liebman. 2015. “The Decline, Rebound, and Further Rise in SNAP Enrollment: Disentangling Business Cycle Fluctuations and Policy Changes.” Harvard University. http://scholar.harvard.edu/files/ganong/files/draftapr07manuscript.pdf.
Gregory, Christian A., and Alisha Coleman-Jensen. 2013. “Do High Food Prices Increase Food Insecurity in the United States?” Applied Economic Perspectives and Policy 35 (4):679–707. https://doi.org/10.1093/aepp/ppt024.
Gregory, Christian A., and Partha Deb. 2015. “Does SNAP Improve Your Health?” Food Policy 50 (January):11–19. https://doi.org/10.1016/j.foodpol.2014.09.010.

28
Gregory, Christian A., Michele Ver Ploeg, Margaret Andrews, and Alisha Coleman-Jensen. 2013. “Supplemental Nutrition Assistance Program (SNAP) Participation Leads to Modest Changes in Diet Quality.” 147. Economic Research Report. USDA Economic Research Service. https://www.ers.usda.gov/webdocs/publications/err147/36939_err147.pdf.
Gundersen, Craig, Brent Kreider, and John Pepper. 2011. “The Economics of Food Insecurity in the United States.” Applied Economic Perspectives and Policy 33 (3):281–303.
Hoynes, Hilary, and Diane Whitmore Schanzenbach. 2016. “US Food and Nutrition Programs.” In Economics of Means-Tested Transfer Programs in the United States, Volume I. University Of Chicago Press. http://www.press.uchicago.edu/ucp/books/book/chicago/E/bo23520704.html.
Hoynes, Hilary, Diane Whitmore Schanzenbach, and Douglas Almond. 2016. “Long-Run Impacts of Childhood Access to the Safety Net.” American Economic Review 106 (4):903–34. https://doi.org/10.1257/aer.20130375.
Kling, Jeffrey R, Jeffrey B Liebman, and Lawrence F Katz. 2007. “Experimental Analysis of Neighborhood Effects.” Econometrica 75 (1):83–119. https://doi.org/10.1111/j.1468-0262.2007.00733.x.
Mykerezi, Elton, and Bradford Mills. 2010. “The Impact of Food Stamp Program Participation on Household Food Insecurity.” American Journal of Agricultural Economics 92 (5):1379–1391.
Nord, M., and M. Golla. 2009. “Does SNAP Decrease Food Insecurity? Untangling the Self-Selection Effect. USDA.” United States Department of Agriculture, Economic Research Service.
Ratcliffe, Caroline, Signe-Mary McKernan, and Sisi Zhang. 2011. “How Much Does the Supplemental Nutrition Assistance Program Reduce Food Insecurity?” American Journal of Agricultural Economics 93 (4):1082–98. https://doi.org/10.1093/ajae/aar026.
Renwick, Trudi, and Liana Fox. 2016. “The Research Supplemental Poverty Measure: 2011 - P60-258.Pdf.” Current Population Reports. US Census Bureau. https://www.census.gov/content/dam/Census/library/publications/2016/demo/p60-258.pdf.
Schmeiser, Maximilian D. 2012. “The Impact of Long-Term Participation in the Supplemental Nutrition Assistance Program on Child Obesity.” Health Economics 21 (4):386–404. https://doi.org/10.1002/hec.1714.
Schmidt, Lucie, Lara Shore-Sheppard, and Tara Watson. 2016. “The Effect of Safety-Net Programs on Food Insecurity.” Journal of Human Resources 51 (3):589–614. https://doi.org/10.3368/jhr.51.3.1013-5987R1.
Shaefer, H Luke, and Italo Gutierrez. 2011. “The Effects of Participation in the Supplemental Nutrition Assistance Program on the Material Hardship of Low-Income Families with Children.” Ann Arbor, MI: National Poverty Center, Gerald R. Ford School of Public Policy, University of Michigan.
“Supplemental Nutrition Assistance Program: Examining the Evidence to Define Benefit Adequacy.” 2013. Institute of Medicine and National Research Council. http://www.iom.edu/Reports/2013/Supplemental-Nutrition-Assistance-Program-Examining-the-Evidence-to-Define-Benefit-Adequacy.aspx.
Todd, Jessica E., Ephraim Leibtag, and Corttney Penberthy. 2011. “Geographic Differences in the Relative Price of Healthy Foods.” United States Department of Agriculture,

29
Economic Research Service. http://books.google.com/books?hl=en&lr=&id=4qm5sgn3u20C&oi=fnd&pg=PP5&dq=todd+qfahpd&ots=UPHWMF7gnM&sig=6wOvjI4JceZtjJ-d7S111pPJm2w.
Todd, Jessica E., Lisa Mancino, Ephraim S. Leibtag, and Christina Tripodo. 2010. “Methodology behind the Quarterly Food-at-Home Price Database.” United States Department of Agriculture, Economic Research Service. http://ideas.repec.org/p/ags/uerstb/97799.html.
Yen, Steven T. 2010. “The Effects of SNAP and WIC Programs on Nutrient Intakes of Children.” Food Policy 35 (6):576–83. https://doi.org/10.1016/j.foodpol.2010.05.010.
Yen, Steven T., Margaret Andrews, Zhuo Chen, and David B. Eastwood. 2008. “Food Stamp Program Participation and Food Insecurity: An Instrumental Variables Approach.” American Journal of Agricultural Economics 90 (1):117–132.
Ziliak, James. 2015. “Temporary Assistance for Needy Families.” In SNAP Matters: How Food Stamps Affect Health and Well-Being. Stanford University Press.
Ziliak, James P. 2015. “Why Are So Many Americans on Food Stamps?” In SNAP Matters: How Food Stamps Affect Health and Well-Being, 18-. Stanford University Press.

30
Figure1:PurchasingPowerofSNAPbyMarketGroupPanelA:1999
PanelB:2008
PanelC:2010
Notes:MapsplotSNAPMAX/TFPforeachofthe30marketareasidentifiedconsistentlyintheQuarterlyFoodatHomePriceDatabase(QFAHPD).

31

32
Table 1
Summary Statistics for Children in NHIS
SNAP All
SNAP All
Citizen Children
Sample Sample
Child/Household Characteristics Children
Health Care Utilization Children Children
TFP price 203 205
Any check-up (12m) 0.77 0.74
(14) (14.18)
(0.421) (0.44)
Max SNAP benefit 143 141
Any doctor's visit (12m) 0.90 0.88
(12) (10.17)
(0.299) (0.32)
Income to poverty ratio 0.90 3.06
Any ER visit (12m) 0.32 0.21
(0.738) (2.237)
(0.465) (0.41)
Child's age 7.5 8.5
Delay/forgo care (12m) 0.06 0.05
(5.1) (5.192)
(0.234) (0.220)
Child is male 0.51 0.51
(0.500) (0.500)
Health Outcomes
Child is black 0.34 0.16
Health status exc. or v. good 0.71 0.70
(0.473) (0.362)
(0.453) (0.458)
Child is Hispanic 0.26 0.19
Hospitalized overnight (12m) 0.09 0.08
(0.439) (0.395)
(0.280) (0.263)
Mother is present 0.94 0.95
School days missed, illness (12m) 4.96 3.53
(0.238) (0.226)
(9.36) (6.43)
Father is present 0.39 0.75
5+ school days missed (12m) 0.33 0.25
(0.488) (0.435)
(0.471) (0.43)
Both parents 0.36 0.71
Obese 0.20 0.13
(0.480) (0.453)
(0.399) (0.336)
Child receives Medicaid 0.72 0.21
Emotional problem 0.46 0.27
(0.448) (0.406)
(0.763) (0.59)
Child has no health insurance 0.07 0.10
(0.250) (0.297)
Number of observations 44,627
296,779 Number of observations 18,299 139,268
Notes: Tables contains estimates of means of US citizen children in household receiving SNAP, weighted to account for complex survey design. Standard errors in parentheses. Left panel are children from the person-file dataset (i.e. all children in household, separately for SNAP and all households) while right panel shows only children from sample child file (i.e. one child per household.)

33
Outcome = SNAP CASELOAD / POPULATION (1) (2) (3) (4) (5)
log(SNAPMax/TFPt ) 0.091** 0.024 0.003 -0.004 0.010(0.036) (0.089) (0.088) (0.079) (0.085)
log(SNAPMax/TFPt+1 )
Observations 37,277 37,277 37,277 37,177 37,177R-squared 0.299 0.497 0.514 0.539 0.544Mean 0.111 0.111 0.111 0.111 0.111Effect of a 10% increase in SNAP purchasing power 0.0088 0.0023 0.0003 -0.0004 0.0010
Fixed effect for year, county X X X X XCounty UR X X X XState SNAP and other policy controls X X XRegional price controls X XLinear time trend No No No No Yes
Notes: Data consists of county by year panel for 1999-2010. Results are weighted using county population. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include fixed effects for market group and year. Columns (2)-(6) add controls for local economic and policy variables: the county unemployment rate, an index of state SNAP policies (Ganong and Liebman, 2015), the state minimum wage, EITC, and Medicaid/SCHIP income eligibility limits, TANF generosity, as well as controls for HUD’s fair market rent, and regional CPIs for non-food, non-housing categories (apparel, commodities, education, medical, recreation, services, transportation and other goods and services).
Table 2Effect of SNAP Purchasing Power on Per-Capita SNAP Caseload

34
(1) (2) (3) (4) (5)Had a Doctor's Delay or Any ER Delay or
checkup visit forgo care visit forgo carepast 12m past 12m past 12m past 12m past 12m
log(SNAPMAX/TFP) 0.656*** 0.323** -0.117 -0.178 -0.089(0.225) (0.147) (0.099) (0.215) (0.092)
Mean of dep. var. 0.77 0.901 0.053 0.315 0.051Effect of 10% increase in SNAP purchasing power 0.063 0.031 -0.011 -0.017 -0.009As a % of mean of dep. var. 8.1% 3.4% -20.9% -5.4% -16.6%N 18,169 18,108 18,296 18,217 44,626R2 0.077 0.038 0.024 0.046 0.022Notes : Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include controls for the child's age (and its square), whether the child is black or Hispanic, the child's family size, indicators for the presence of the mother (and/or father) in the household, and interactions between indicators for the mother's (father's) presence and the mother's (father's) education, marital status, age, and citizenship. All regressions also include controls for local economic and policy variables: the county unemployment rate, an index of state SNAP policies (Ganong and Liebman, 2015), the state minimum wage, EITC, and Medicaid/CHIP income eligibility limits, TANF generosity, as well as controls for HUD’s fair market rent, and regional CPIs for non-food, non-housing categories (apparel, commodities, education, medical, recreation, services, transportation and other goods and services). Finally, all models include year and market group fixed effects. Outcomes in columns 1, 2, and 4 are observed only for children in the Sample Child files.
Table 3 Effects of Variation in SNAP Purchasing Power on Children's Health Care Utilization
Children in Sample Child File All Children
Sample: SNAP Recipient U.S. Citizen Children in the NHIS, 1999-2010

35
(1) (2) (3) (4) (5) (6) (7) (8)Health status Hospitalized School days 5 or more Obese Emotional Health status Hospitalizedexcellent or overnight missed due school days problem excellent or overnightvery good past 12m to illness missed very good past 12m
log(SNAPMAX/TFP) -0.069 0.028 -11.43** -0.148 -0.24 0.055 -0.121 0.02(0.208) (0.124) (5.374) (0.272) (0.374) (0.468) (0.199) (0.065)
Mean of dep. var. 0.701 0.0769 4.955 0.332 0.199 0.464 0.700 0.075Effect of 10% increase in SNAP purch power -0.007 0.003 -1.090 -0.014 -0.023 0.005 -0.012 0.002As a % of mean of dep. var. -0.9% 3.4% -22.0% -4.2% -11.5% 1.1% -1.6% 2.6%N 18299 18291 11420 11420 4471 10779 44,627 44,620R2 0.033 0.151 0.033 0.041 0.035 0.055 0.032 0.150Notes : Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include the same controls as in Table 3. Outcomes in columns (3)-(6) are observed only for children in the Sample Child files. Missed school days is defined only for children ages 5 and older who attend school; information on obesity is consistently available for children ages 12-17, trimmed to exclude the top and bottom percentile of the BMI distribution; and emotional problem defined for the universe of children ages 4 and older.
Table 4 Effects of Variation in SNAP Purchasing Power on Children's Health Outcomes
Children in Sample Child File All NHIS Children 0-17
Sample: SNAP Recipient U.S. Citizen Children in the NHIS, 1999-2010

36
(1) (2)Child is food Child is very
insecure food insecurelog(SNAPMax/TFPt ) -0.670* 0.0856
[0.330] [0.107]
Mean of dep. var. 0.293 0.041Effect of 10% increase in SNAP purchasing power -0.0639 0.00816As a % of mean of dep. var. -21.8% 19.9%N 29,324 29,324R2 0.033 0.021
Table 5Effects of SNAP Purchasing Power on Food Insecurity
Sample: SNAP Recipient U.S. Citizen Children in the December CPS, 2001-2010
Notes: Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include controls for the child's age (and its square), whether the child is b lack or Hispanic, the child's family size, indicators for the presence of the mother (and/or father) in the household, and interactions between indicators for the mother's (father's) presence and the mother's (father's) education, marital status, age, and citizenship. All regressions also include controls for local economic and policy variab les: the state unemployment rate, an index of state SNAP policies (Ganong and Liebman, 2015), the state minimum wage, EITC, and Medicaid/CHIP income eligib ility limits, and TANF generosity. Finally, all models include year and market group fixed effects.

37
Children in Sample Child File Children 0-17
(1) (2)No Insurance No Insurance
log(SNAPMax/TFPt ) -0.136 -0.071(0.146) (0.136)
Mean of dep. var. 0.068 0.067Effect of 10% increase in SNAP purchasing power -0.013 -0.007As a % of mean of dep. var. -19.0% -10.1%N 18,259 44,540R2 0.036 0.033
Notes: Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include controls for the child's age (and its square), whether the child is b lack or Hispanic, the child's family size, indicators for the presence of the mother (and/or father) in the household, and interactions between indicators for the mother's (father's) presence and the mother's (father's) education, marital status, age, and citizenship. All regressions also include controls for local economic and policy variab les: the county unemployment rate, an index of state SNAP policies (Ganong and Liebman, 2015), the state minimum wage, EITC, and Medicaid/CHIP income eligib ility limits, TANF generosity, as well as controls for HUD’s fair market rent, and regional CPIs for non-food, non-housing categories (apparel, commodities, education, medical, recreation, services, transportation and other) goods and services. Finally, all models include year and market group fixed effects.
Effects of SNAP Purchasing Power on Health Insurance CoverageTable 6
Sample: SNAP Recipient U.S. Citizen Children in the NHIS, 1999-2010
All NHIS

38
All Children
(1) (2) (3) (4) (5) (1) (2) (3) (4) (5) (6) (7) (8)Had Doctor's Delay or Any ER Delay or Health status Hosp. School 5+ school Obese Emotional Health status Hosp.
checkup visit forgo care visit forgo care exc or v good overnight days misseddays missed problem exc or v good overnightlog(SNAPMax/TFPt ) 0.232 0.190 -0.049 -0.300** -0.058 -0.026 -0.051 2.07 -0.095 0.420** 0.285 0.012 -0.013
(0.208) (0.125) (0.049) (0.116) (0.044) (0.107) (0.053) (3.14) (0.151) (0.159) (0.275) (0.104) (0.045)
Mean of dep. var. 0.756 0.911 0.030 0.175 0.030 0.889 0.051 3.360 0.241 0.113 0.239 0.886 0.054Effect of 10% increase in SNAP PP 0.022 0.018 -0.005 -0.029 -0.006 -0.002 -0.005 0.197 -0.009 0.040 0.027 0.001 -0.001As a % of mean of dep. var. 2.9% 2.0% -15.3% -16.3% -18.6% -0.3% -9.6% 5.9% -3.7% 35.4% 11.3% 0.1% -2.3%N 24,898 24,887 25,117 25,025 48,616 25,125 25,123 18,189 18,189 8,879 15,644 48,637 48,607R2 0.092 0.035 0.008 0.02 0.01 0.023 0.168 0.022 0.020 0.042 0.030 0.023 0.176Notes: Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include controls for the child's age (and its square), whether the child is b lack or Hispanic, the child's family size, indicators for the presence of the mother (and/or father) in the household, and interactions between indicators for the mother's (father's) presence and the mother's (father's) education, marital status, age, and citizenship. Insurance coverage not included as control in columns 1 and 5. All regressions also include controls for local economic and policy variab les: the county unemployment rate, an index of state SNAP policies (Ganong and Liebman, 2015), the state minimum wage, EITC, TANF generosity and Medicaid/CHIP income eligib ility limits, as well as controls for HUD’s fair market rent, and regional CPIs for non-food, non-housing categories (apparel, commodities, education, medical, recreation, services, transportation and other goods and services). Finally, all models include year and market group fixed effects. Outcomes in Panel A, columns 1,2, and 4, and outcomes on Panel B, columns 3-6 are observed only for children in the Sample Child files.
Table 7 Effects of SNAP Purchasing Power on Health Care Utilization and Health: Robustness Checks
Sample: U.S. Citizen Children in NHIS with Household Incomes between 300 and 450 Percent of Federal Poverty Line, 1999-2010
A. Health Care Utilization B. Health Outcomes
Chldren in Sample Child File Chldren in Sample Child File All Children

39
Robustness Check All Children
(1) (2) (3) (4) (5) (1) (2) (3) (4) (5) (6) (7) (8)Had Doctor's Delay or Any ER Delay or Health status Hosp. School 5+ school Obese Emotional Health status Hosp.
checkup visit forgo care visit forgo care exc or v good overnight days missed days missed problem exc or v good overnightlog(SNAPMax/TFPt ) 0.517* 0.111 0.023 0.011 0.040 -0.013 -0.094 -13.48** -0.161 -0.273 0.003 -0.065 0.043
(0.278) (0.161) (0.113) (0.308) (0.089) (0.328) (0.115) (5.90) (0.327) (0.535) (0.774) (0.305) (0.060)log(SNAPMax/TFPt+1 ) 0.194 0.260 -0.252** -0.386 -0.185* -0.214 0.116 -4.756 -0.303 0.0717 0.266 -0.155 -0.076
(0.247) (0.192) (0.118) (0.238) (0.097) (0.307) (0.092) (4.02) (0.295) (0.473) (0.792) (0.316) (0.089)
Mean of dep. var. 0.764 0.900 0.055 0.312 0.054 0.700 0.076 4.981 0.333 0.201 0.459 0.697 0.075Effect of 10% increase in SNAP PP 0.049 0.011 0.002 0.001 0.004 -0.001 -0.009 -1.284 -0.015 -0.026 0.000 -0.006 0.004As a % of mean of dep. var. 6.5% 1.2% 4.0% 0.3% 7.1% -0.2% -11.8% -25.8% -4.6% -13.0% 0.1% -0.9% 5.5%
B. Include market group-level linear time trends (1) (2) (3) (4) (5) (1) (2) (3) (4) (5) (6) (7) (6)Had Doctor's Delay or Any ER Delay or Health status Hosp. School 5+ school Obese Emotional Health status Emotional
checkup visit forgo care visit forgo care exc or v good overnight days missed days missed problem exc or v good problemlog(SNAPMax/TFPt ) 0.268 0.148 -0.0602 0.0724 -0.0316 -0.282 0.060 -12.53* -0.018 -0.351 -0.098 -0.228 0.0775
(0.272) (0.196) (0.153) (0.315) (0.116) (0.270) (0.142) (6.82) (0.289) (0.433) (0.671) [0.248] [0.0637]
Mean of dep. var. 0.770 0.901 0.053 0.315 0.051 0.701 0.077 4.955 0.332 0.199 0.464 0.70 0.07Effect of 10% increase in SNAP PP 0.026 0.014 -0.006 0.007 -0.003 -0.027 0.006 -1.194 -0.002 -0.034 -0.009 -0.02 0.01As a % of mean of dep. var. 3.3% 1.6% -10.8% 2.2% -5.9% -3.8% 7.4% -24.1% -0.5% -16.8% -2.0% -3.1% 9.9%
C. Alternate Sample: Children of Low-Educated, (1) (2) (3) (4) (5) (1) (2) (3) (4) (5) (6) (7) (6) Unmarried Parents Had Doctor's Delay or Any ER Delay or Health status Hosp. School 5+ school Obese Emotional Health status Emotional
checkup visit forgo care visit forgo care exc or v good overnight days missed days missed problem exc or v good problemlog(SNAPMax/TFPt ) 0.640** 0.100 -0.690 -0.505** 0.013 0.186 -0.065 -11.68 -0.011 0.210 -0.305 0.058 -0.047
(0.255) (0.161) (0.130) (0.184) (0.086) (0.195) (0.097) (7.93) (0.194) (0.344) (0.427) (0.195) (0.053)
Mean of dep. var. 0.726 0.867 0.061 0.279 0.057 0.708 0.061 4.323 0.305 0.181 0.396 0.705 0.062Effect of 10% increase in SNAP PP 0.061 0.010 -0.007 -0.048 0.001 0.018 -0.006 -1.113 -0.001 0.020 -0.029 0.006 -0.005As a % of mean of dep. var. 8.4% 1.1% -10.9% -17.3% 2.1% 2.5% -10.2% -25.7% -0.3% 11.0% -7.3% 0.8% -7.2%
Table 8Effects of SNAP Purchasing Power on Health Care Utilization and Health: Robustness Checks
Sample: SNAP-Recipient U.S. Citizen Children, 1999-2010
A. Include lead term using future TFP price
Notes: Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include controls for the child's age (and its square), whether the child is b lack or Hispanic, the child's family size, indicators for the presence of the mother (and/or father) in the household, and interactions between indicators for the mother's (father's) presence and the mother's (father's) education, marital status, age, and citizenship. Insurance coverage not included as control in columns 1 and 5. All regressions also include controls for local economic and policy variab les: the county unemployment rate, an index of state SNAP policies (Ganong and Liebman, 2015), the state minimum wage, EITC, TANF generosity, and Medicaid/CHIP income eligib ility limits, as well as controls for HUD’s fair market rent, and regional CPIs for non-food, non-housing categories (apparel, commodities, education, medical, recreation, services, transportation and other). Finally, all models include year and market group fixed effects. Outcomes in Panel A, columns 1,2, and 4, and outcomes on Panel B, columns 3-6 are observed only for children in the Sample Child files.
Chldren in Sample Child File All ChildrenChldren in Sample Child File
A. Health Care Utilization B. Health Outcomes

40

41
AppendixFigure1
VariationacrossMarketGroupAreas,1999-2010(a)RealTFPCost1999-2010
(b)SNAPPurchasingPower

42
Notes:Figureshows(a)theTFPinconstant2010dollarsand(b)theratioofmaximumSNAPbenefitstomarketregionTFP.Highlightedregionsarethosewiththelargestincreaseovertheperiod(NorthFlorida,NewYork,SanFrancisco)andthelargestdecrease(Chicago,MetroSouth:LittleRock,MetroOklahoma).
(1) (2) (3) (4) (5)Had a Doctor's Delay or Any ER Delay or
checkup visit forgo care visit forgo carepast 12m past 12m past 12m past 12m past 12m
log(SNAPMAX/TFP) 0.641*** 0.288* -0.126 -0.158 -0.094(0.227) (0.151) (0.098) (0.223) (0.089)
Mean of dep. var. 0.764 0.896 0.055 0.311 0.053Effect of 10% increase in SNAP purchasing power 0.061 0.028 -0.012 -0.015 -0.009As a % of mean of dep. var. 8.0% 3.1% -21.8% -4.8% -17.0%N 18,765 18,699 18,894 18,815 46,358R2 0.082 0.044 0.024 0.047 0.021Notes : Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include same controls as in Table 3 of the paper. Outcomes in columns 1-4 are observed only for children in the Sample Child files.
Appendix Table 1Effects of Variation in SNAP Purchasing Power on Children's Health Care Utilization
Sample: SNAP Recipient Children Ages 0-17 in the NHIS, 1999-2010
Children in Sample Child File All Children
(1) (2) (3) (4) (5) (6) (7) (8)Health status Hospitalized School days 5 or more Obese Emotional Health status Hospitalizedexcellent or overnight missed due school days problem excellent or overnightvery good past 12m to illness missed very good past 12m
log(SNAPMAX/TFP) -0.126 0.023 -11.10** -0.157 -0.190 0.048 -0.152 0.021(0.205) (0.121) (5.23) (0.263) (0.341) (0.455) (0.193) (0.062)
Mean of dep. var. 0.701 0.076 4.87 0.326 0.196 0.452 0.699 0.073Effect of 10% increase in SNAP purch power -0.012 0.002 -1.60 -0.015 -0.018 -0.005 -0.015 0.002As a % of mean of dep. var. -1.7% 2.6% -32.9% -4.6% -9.2% -1.1% -2.1% 2.7%N 18,897 18,890 11,953 11,953 4,740 11,252 46,359 46,354R2 0.033 0.148 0.034 0.044 0.034 0.058 0.031 0.148Notes : Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include the same controls as in Table 4 of paper. Missed school days is defined only for children ages 5 and older who attend school; information on obesity is consistently available for children ages 12-17, trimmed to exclude the top and bottom percentile of the BMI distribution; and emotional problem defined for the universe of children ages 4 and older.
Appendix Table 2Effects of Variation in SNAP Purchasing Power on Children's Health Outcomes
Sample: SNAP Recipient Children Ages 0-17 in the NHIS, 1999-2010
Children in Sample Child File All NHIS Children 0-17

43
(1) (2) (3) (4) (5)Had a Doctor's Delay or Any ER Delay or
checkup visit forgo care visit forgo carepast 12m past 12m past 12m past 12m past 12m
log(SNAPMAX/TFP) 0.648*** 0.301** -0.100 -0.230 -0.084(0.223) (0.146) (0.094) (0.207) (0.085)
Mean of dep. var. 0.770 0.901 0.053 0.315 0.051Effect of 10% increase in SNAP purchasing power 0.062 0.029 -0.010 -0.022 -0.008As a % of mean of dep. var. 8.1% 3.2% -18.9% -7.0% -15.7%N 18,126 18,065 18,249 18,171 44,504R2 0.087 0.052 0.100 0.063 0.097Notes : Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include the same controls as in Table 3 of paper but also add controls for family income, whether child has health insurance coverage, and child's health status (1-5). Finally, all models include year and market group fixed effects. Outcomes in columns 1, 2, and 4 are observed only for children in the Sample Child files.
Appendix Table 3 Effects of Variation in SNAP Purchasing Power on Children's Health Care Utilization
Sample: SNAP Recipient U.S. Citizen Children in the NHIS, 1999-2010
Children in Sample Child File All Children
(1) (2) (3) (4) (5) (6) (7) (8)Health status Hospitalized School days 5 or more Obese Emotional Health status Hospitalizedexcellent or overnight missed due school days problem excellent or overnightvery good past 12m to illness missed very good past 12m
log(SNAPMAX/TFP) -0.074 0.005 -12.16** -0.179 -0.338 -0.008 -0.140 0.021(0.205) (0.127) (5.57) (0.257) (0.380) (0.436) (0.196) (0.065)
Mean of dep. var. 0.701 0.077 4.96 0.332 0.199 0.463 0.700 0.075Effect of 10% increase in SNAP purch power -0.007 0.0005 -1.16 -0.017 -0.032 -0.001 -0.013 0.002As a % of mean of dep. var. -1.0% 0.6% -23.4% -5.1% -16.1% -0.2% -1.9% 2.7%N 18299 18291 11420 11420 4471 10779 44,627 44,620R2 0.033 0.151 0.033 0.041 0.035 0.055 0.034 0.150Notes : Results from weighted OLS regressions. Standard errors in parentheses are corrected for clustering at the market group level; *** p<0.01, ** p<0.05, * p<0.1. All regressions include the same controls as in Table 4 of paper but also add controls for family income, whether child has health insurance coverage, and child's health status (1-5) when health status is not the outcome of interest. Outcomes in columns (3)-(6) are observed only for children in the Sample Child files.. Outcomes in columns (3)-(6) are observed only for children in the Sample Child files. Missed school days is defined only for children ages 5 and older who attend school; information on obesity is consistently available for children ages 12-17, trimmed to exclude the top and bottom percentile of the BMI distribution; and emotional problem defined for the universe of children ages 4 and older.
Appendix Table 4 Effects of Variation in SNAP Purchasing Power on Children's Health Outcomes
Sample: SNAP Recipient U.S. Citizen Children in the NHIS, 1999-2010
Children in Sample Child File All NHIS Children 0-17

44
Appendix Table 5 Summary Index Estimates
(1) (3) (4) (5)
Utilization Utilization Outcomes Outcomes
VARIABLESSNAPCitizen
Low-EdUnmarried
SNAPCitizen
Low-EdUnmarried
log(SNAPMax/TFPYRM) 4.229** 4.469*** 1.336 2.345*
[1.542] [1.264] [0.847] [1.155]
Observations 17,985 17,560 11,413 12,371R-squared 0.052 0.060 0.027 0.023Meanofdep.variable -0.00484 0.00247 0.167 0.174Effectof10%increase 0.403 0.426 0.127 0.223
Notes:Tablefeaturescoefficientsfromsummaryindexestimatesforhealthcareutilizationvariable(checkups,anydoctorvisits,delayseekinghealthcare,ERvisit,andnohealthinsurance)orforhealthoutcomevariables(healthstatus,hospitalization,andschooldaysmissed).Variablesarestandardnormalizedandsums,socoefficientrepresentsstandarddeviationunits.AllobservationsarefromtheSampleChildfile,andtheexactsampleiseithercitizenSNAPchildrenorchildrenwithlow-educationunmarriedparents.